Autologous solution protects bovine cartilage explants from IL-1α- and TNFα-induced cartilage...
7
Autologous Solution Protects Bovine Cartilage Explants From IL-1a- and TNFa-Induced Cartilage Degradation Andrea Matuska, Krista O’shaughnessey, William King, Jennifer Woodell-May Biomet Biologics, 56 East Bell Drive, Warsaw, 46581, Indiana Received 28 February 2013; accepted 16 July 2013 Published online 21 August 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/jor.22464 ABSTRACT: Osteoarthritis (OA) is characterized by deterioration of articular cartilage driven by an imbalance of pro- and anti- inflammatory cytokines. To address the cartilage deterioration observed in OA, an autologous protein solution (APS) has been developed which has been shown to inhibit the production of destructive proteases and inflammatory cytokines from chondrocytes and monocytes, respectively. The purpose of this study was to determine the chondroprotective effect of APS on IL-1a- or TNFa-challenged bovine articular cartilage explants. Cartilage explants were cultured in the presence or absence of recombinant inflammatory cytokines, IL-1a and TNFa. Explants under equivalent inflammatory conditions were pretreated with recombinant antagonists IL-1ra, sTNF-RI, or APS to measure their inhibition of matrix degradation. Explants were further evaluated with Safranin-O, Masson’s Trichrome, and Hematoxylin and Eosin histological staining. APS was more effective than recombinant antagonists in preventing cartilage matrix degradation and inhibited any measurable IL-1a-induced collagen release over a 21-day culture period. APS treatment reduced the degree of Safranin-O staining loss when cartilage explants were cultured with IL-1a or TNFa. Micrographs of APS treated cartilage explants showed an increase in observed cellularity and apparent cell division. APS may have the potential to prevent cartilage loss associated with early OA. ß 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res 31:1929–1935, 2013 Keywords: IRAP; IL-1ra; platelet rich plasma; autologous protein solution; osteoarthritis Osteoarthritis (OA) is characterized by deterioration of articular cartilage driven by an imbalance of pro- and anti-inflammatory cytokines. Proinflammatory cytokines, specifically interleukin-1 (IL-1) and tumor necrosis factor alpha (TNFa), are upregulated in OA. 1 Chondrocytes respond to these proinflammatory cytokines by increas- ing production of matrix metalloproteinases (MMPs), aggrecanases (ADAMTS), prostaglandins, and nitric ox- ide (NO). 2 Aggrecanases mediate glycosaminoglycan (GAG) release, which is one of the first extracellular matrix (ECM) components to undergo a measurable loss during OA. 3 This loss is considered reversible, however, since GAGs can be resynthesized. Alternatively, collagen release is slower and is considered irreversible. 4 The MMPs together (collagenases, gelatinases, and stromely- sins) degrade both type II collagen and proteoglycans. 5 As these components of the ECM are lost, strength and elasticity in the joint are irreversibly lost as well. 6 The destructive consequence of OA on patients’ everyday lives has motivated the development of new therapeutic approaches. Several approaches have been pursued to inhibit inflammatory cytokine signaling in OA. One attempted approach has been the use of recombinant protein antagonists of IL-1 or TNFa. For example, recombi- nant IL-1ra (Anakinra, Amgen, Thousand Oaks, CA) is currently FDA approved for treatment of rheuma- toid arthritis. However, recombinant IL-1ra failed to show statistical improvement in clinical assessment for knee OA. 7 Similarly, recombinant soluble tumor necrosis factor- receptor (sTNF-R) was evaluated suc- cessfully in clinical trials for rheumatoid arthritis 8 and inconclusively for the treatment OA. 9 These results suggest that targeting multiple inflammatory signal- ing pathways may be necessary to effectively treat OA. Autologous-derived products represent a potentially useful approach to deliver multiple therapeutic mole- cules simultaneously. For example, intra-articular injections of platelet-rich plasma (PRP) have been explored to treat OA. PRP has been characterized to contain high concentrations of anabolic growth fac- tors. 10 In a recent OA clinical trial, patients with bilateral OA were treated with a single PRP injection, two PRP injections separated by 3 weeks, or a single saline injection. Patients treated with single or double PRP injections had significantly improved Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores 2–3 weeks post-injection that lasted until the end of the study at 6 months. There were no significant differences between the single or double PRP injection groups. 11 In a separate study, patients were treated with three PRP or hyaluronic acid intra- articular injections. After 2, 6, and 12 months post- injection, both groups showed improved clinical scores, but there were no significant differences between the treatment groups evaluated. However, there was a trend toward more significant improvements in patients treated with PRP with less severe OA (Kellg- ren Lawrence Score < III). 12 These studies highlight the need for autologous products with well-character- ized compositions to treat OA. An autologous protein solution (APS) has been developed which can be prepared in less than 30min at the patient’s point-of-care and contains high concen- trations of anti-inflammatory cytokines and anabolic growth factors. 13 Previous research has demonstrated that APS inhibits the inflammatory responses of mono- cytes and chondrocytes to IL-1 and/or TNFa in vitro. Correspondence to: Jennifer Woodell-May (T: þ1-574-372-1757; F: þ1-574-371-1187; E-mail: [email protected]) # 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013 1929
Transcript of Autologous solution protects bovine cartilage explants from IL-1α- and TNFα-induced cartilage...

Autologous Solution Protects Bovine Cartilage Explants FromIL-1a- and TNFa-Induced Cartilage Degradation
Andrea Matuska, Krista O’shaughnessey, William King, Jennifer Woodell-May
Biomet Biologics, 56 East Bell Drive, Warsaw, 46581, Indiana
Received 28 February 2013; accepted 16 July 2013
Published online 21 August 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/jor.22464
ABSTRACT: Osteoarthritis (OA) is characterized by deterioration of articular cartilage driven by an imbalance of pro- and anti-inflammatory cytokines. To address the cartilage deterioration observed in OA, an autologous protein solution (APS) has been developedwhich has been shown to inhibit the production of destructive proteases and inflammatory cytokines from chondrocytes and monocytes,respectively. The purpose of this study was to determine the chondroprotective effect of APS on IL-1a- or TNFa-challenged bovinearticular cartilage explants. Cartilage explants were cultured in the presence or absence of recombinant inflammatory cytokines, IL-1aand TNFa. Explants under equivalent inflammatory conditions were pretreated with recombinant antagonists IL-1ra, sTNF-RI, or APSto measure their inhibition of matrix degradation. Explants were further evaluated with Safranin-O, Masson’s Trichrome, andHematoxylin and Eosin histological staining. APS was more effective than recombinant antagonists in preventing cartilage matrixdegradation and inhibited any measurable IL-1a-induced collagen release over a 21-day culture period. APS treatment reduced thedegree of Safranin-O staining loss when cartilage explants were cultured with IL-1a or TNFa. Micrographs of APS treated cartilageexplants showed an increase in observed cellularity and apparent cell division. APS may have the potential to prevent cartilage lossassociated with early OA. � 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res 31:1929–1935, 2013
Keywords: IRAP; IL-1ra; platelet rich plasma; autologous protein solution; osteoarthritis
Osteoarthritis (OA) is characterized by deteriorationof articular cartilage driven by an imbalance of pro- andanti-inflammatory cytokines. Proinflammatory cytokines,specifically interleukin-1 (IL-1) and tumor necrosis factoralpha (TNFa), are upregulated in OA.1 Chondrocytesrespond to these proinflammatory cytokines by increas-ing production of matrix metalloproteinases (MMPs),aggrecanases (ADAMTS), prostaglandins, and nitric ox-ide (NO).2 Aggrecanases mediate glycosaminoglycan(GAG) release, which is one of the first extracellularmatrix (ECM) components to undergo a measurable lossduring OA.3 This loss is considered reversible, however,since GAGs can be resynthesized. Alternatively, collagenrelease is slower and is considered irreversible.4 TheMMPs together (collagenases, gelatinases, and stromely-sins) degrade both type II collagen and proteoglycans.5
As these components of the ECM are lost, strength andelasticity in the joint are irreversibly lost as well.6 Thedestructive consequence of OA on patients’ everyday liveshas motivated the development of new therapeuticapproaches.
Several approaches have been pursued to inhibitinflammatory cytokine signaling in OA. One attemptedapproach has been the use of recombinant proteinantagonists of IL-1 or TNFa. For example, recombi-nant IL-1ra (Anakinra, Amgen, Thousand Oaks, CA)is currently FDA approved for treatment of rheuma-toid arthritis. However, recombinant IL-1ra failed toshow statistical improvement in clinical assessmentfor knee OA.7 Similarly, recombinant soluble tumornecrosis factor- receptor (sTNF-R) was evaluated suc-cessfully in clinical trials for rheumatoid arthritis8 and
inconclusively for the treatment OA.9 These resultssuggest that targeting multiple inflammatory signal-ing pathways may be necessary to effectively treat OA.
Autologous-derived products represent a potentiallyuseful approach to deliver multiple therapeutic mole-cules simultaneously. For example, intra-articularinjections of platelet-rich plasma (PRP) have beenexplored to treat OA. PRP has been characterized tocontain high concentrations of anabolic growth fac-tors.10 In a recent OA clinical trial, patients withbilateral OA were treated with a single PRP injection,two PRP injections separated by 3 weeks, or a singlesaline injection. Patients treated with single or doublePRP injections had significantly improved WesternOntario and McMaster Universities Arthritis Index(WOMAC) scores 2–3 weeks post-injection that lasteduntil the end of the study at 6 months. There were nosignificant differences between the single or doublePRP injection groups.11 In a separate study, patientswere treated with three PRP or hyaluronic acid intra-articular injections. After 2, 6, and 12 months post-injection, both groups showed improved clinical scores,but there were no significant differences between thetreatment groups evaluated. However, there was atrend toward more significant improvements inpatients treated with PRP with less severe OA (Kellg-ren Lawrence Score< III).12 These studies highlightthe need for autologous products with well-character-ized compositions to treat OA.
An autologous protein solution (APS) has beendeveloped which can be prepared in less than 30min atthe patient’s point-of-care and contains high concen-trations of anti-inflammatory cytokines and anabolicgrowth factors.13 Previous research has demonstratedthat APS inhibits the inflammatory responses of mono-cytes and chondrocytes to IL-1 and/or TNFa in vitro.
Correspondence to: Jennifer Woodell-May (T: þ1-574-372-1757;F: þ1-574-371-1187; E-mail: [email protected])
# 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013 1929

The outcome measures of those studies, IL-8 andMMP-13 concentrations produced by the cultured cells,indicated that APS may act to inhibit cartilage degra-dation.13,14 APS also has demonstrated improved gatebiomechanics, lameness, and pain in a prospective anddouble-blinded clinical trial to treat equine OA.15 Thepurpose of this study was to demonstrate the ability ofAPS to inhibit cartilage explant degeneration. Specifi-cally, GAG and hydroxyproline were assessed as ameasure of proteoglycan and collagen release, respec-tively. If APS inhibited cartilage explant degradation,this result could suggest this product could affect OAprogression.
MATERIALS AND METHODSPreparation of Autologous Protein Solution (APS)From consenting human donors (IRB #1115097), 55ml wholeblood was drawn into 5ml ACD-A (Citra Labs, Braintree,MA). The blood was processed in a disposable device, theAPS Separator, according to manufacturer’s instructionusing a 15-min centrifugation step (Biomet Biologics, War-saw, IN) to produce a cell solution containing platelets andwhite blood cells. The cell solution was collected andprocessed in an APS Concentrator device containing poly-acrylamide beads which desiccate the cell solution. Followingcentrifugation for 2min, approximately 2ml APS werecollected. The cells in the APS were lysed at 4˚C in a celldisrupter (Scientific Industries, Bohemia, NY), centrifuged,and the lysate was stored (�50˚C) until assayed.
Cartilage Explant CultureSlices of articular cartilage were harvested from bovine stiflejoints acquired from 24-month-old animals at Lemler Locker(Bourbon, IN). A disposable 4mm biopsy punch (Miltex, York,PA) was used to aseptically obtain uniform diameter cartilageexplants from the slices. Explants were washed and placed 1per well of a 24-well plate or 2 per well of a 12-well plate.Plates were incubated for 1–4 days at 37˚C and 5% CO2 inhumidified air in order to equilibrate explants. Media werereplaced with fresh media before beginning each assay.
Cartilage Explant Assay With Recombinant ProteinsEither rhIL-1a (PeproTech, Rocky Hill, NJ) or rhTNFa(Prospec Protein Specialists, Rehovot, Isreal) were added tothe explant cultures with or without a 1-h preincubation ofantagonists rhIL-1ra (Prospec Protein Specialists) or sTNF-RI (R&D Systems, Minneapolis, MN), respectively. Theplates were incubated for 3–21 days with both the inflamma-tory and anti-inflammatory cytokines in the media. Thesupernatants were collected and stored at �50˚C untilanalysis. Concentrations of test reagents were replaced every7 days when required.
Autologous Protein Solution in Cartilage Explant AssayIn a 12-well plate, media were exchanged with 1.5ml mediaand transwell inserts (Corning, Inc., Corning, NY) wereplaced in the wells. For the control samples, 500ml mediawere added to the inserts, but for the APS-treated samples250ml APS mixed with 250ml media were added to theinserts above the explants. After 1h, rhIL-1a or rhTNFa wasadded to the control and treatment wells. The explants wereincubated for 3–21 days, and the supernatants were collected
in microcentrifuge tubes. Fresh media, concentrations of testreagents, and APS treatment were replaced every 7 days.
GAG Release as a Measure of Proteoglycan DegradationFollowing culture, explants were collected into 1ml of papainbuffer (1.1mM ethylenediaminetetraacetic acid [EDTA], Sig-ma–Aldrich, St. Louis, MO), 5.5mM N-acetyl cysteine (Sig-ma–Aldrich), 0.067mM b-mercaptoethanol (Gibco, GrandIsland, NY), 1.5mg/ml papain (Worthington Biochemical,Lakewood, NJ) in PBS and incubated 1h at 60˚C fordigestion. GAG release testing using a dimethyl-methyleneblue (DMMB) assay was performed on collected supernatantsand digested cartilage samples in a 96-well round-bottommicroplate (Corning, Inc.) following previously describedmethods.16
Hydroxyproline Assay as a Measure of Collagen DegradationHydroxyproline release was assayed as a measure of collagendegradation using a previously described method17 which isbased off of the change in absorbance produced when freeamino acids undergo oxidation and decarboxylation and thesubsequent condensation reaction with dimethylaminoben-zaldehyde (DMBA, Sigma–Aldrich). Percent collagen releasewas calculated by dividing hydroxyproline detected in thesupernatant by the sum of hydroxyproline detected in thesupernatants and digested samples.
HistologyAfter 3 days (for Safranin-O analysis), 7, 14, 21 days (forTrichrome analysis), and 28 days (for Hematoxylin and Eosinanalysis) explants were collected, fixed in 10% formalinneutral buffered solution (Sigma–Aldrich) and processed forhistological evaluation (Toxikon, Bedford, MA). Explantswere sectioned, stained with Safranin-O, Masson’s Tri-chrome, or Hematoxylin and Eosin stain. Fixed slides wereanalyzed using an AxioCam MRc digital camera fitted to aninverted microscope (Axio Observer A1, Carl Zeiss, Thorn-wood, NY).
Statistical AnalysisData are presented as mean� standard deviation. Statisticalsignificance was determined with statistical software (Mini-tab, Inc., State College, PA). Parametric data were analyzedusing a student’s t-test where appropriate or with a singlefactor ANOVA and post hoc Tukey test, assuming a¼ 0.05 tobe significant. For non-parametric data, a Kruskal–Wallismultiple comparison test was used.
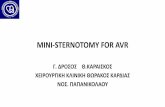
RESULTSCartilage Explant Assay With Recombinant ProteinsTreatment with recombinant inflammatory cytokinesrhIL-1a and rhTNFa induced a statistically significantincrease in the percentage of total GAGs released overthe 21-day culture period (p<0.05, Fig. 1A). After7 days, rhIL-1a and rhTNFa induced 79.6�5.0% and69.7�5.4% release of total GAG content, respectively.After 21 days, explants exposed to rhIL-1a released95.1�2.6% of their GAG content and explants exposedto rhTNFa released 94.7� 2.2% of their GAG content.Alternatively, rhIL-1a and rhTNFa induced 0.9�1.4%and 0.7� 0.7% release of total collagen content by day7, respectively (Fig. 1B). A statistically significantincrease in percent collagen released from the explants
1930 MATUSKA ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013
was induced by rhIL-1a after 14 (p¼0.007) and21 days (p¼0.002), with an average of 37.8�18.8%collagen released after 21 days. The release of7.0�1.6% of the explants’ collagen was induced byrhTNFa by day 21, which was not significantly differ-ent than the percent collagen released from explantsmaintained in media without exogenous inflammatorycytokines (p>0.05).
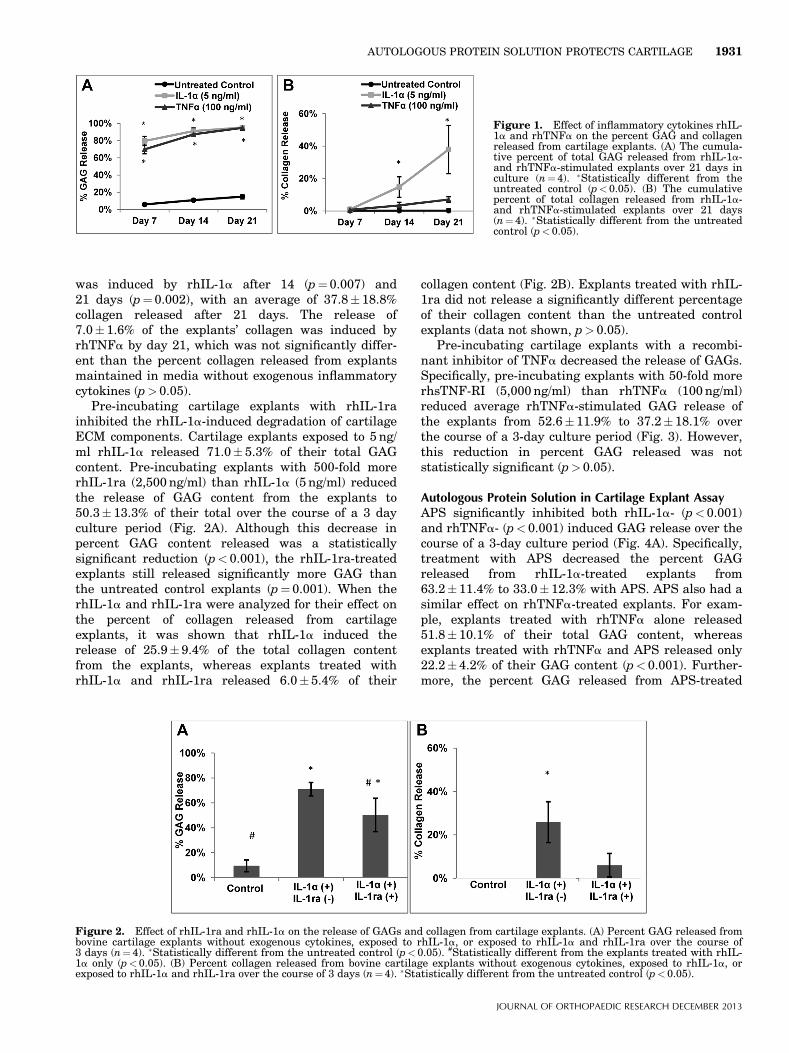
Pre-incubating cartilage explants with rhIL-1rainhibited the rhIL-1a-induced degradation of cartilageECM components. Cartilage explants exposed to 5ng/ml rhIL-1a released 71.0� 5.3% of their total GAGcontent. Pre-incubating explants with 500-fold morerhIL-1ra (2,500ng/ml) than rhIL-1a (5 ng/ml) reducedthe release of GAG content from the explants to50.3� 13.3% of their total over the course of a 3 dayculture period (Fig. 2A). Although this decrease inpercent GAG content released was a statisticallysignificant reduction (p< 0.001), the rhIL-1ra-treatedexplants still released significantly more GAG thanthe untreated control explants (p¼0.001). When therhIL-1a and rhIL-1ra were analyzed for their effect onthe percent of collagen released from cartilageexplants, it was shown that rhIL-1a induced therelease of 25.9�9.4% of the total collagen contentfrom the explants, whereas explants treated withrhIL-1a and rhIL-1ra released 6.0�5.4% of their
collagen content (Fig. 2B). Explants treated with rhIL-1ra did not release a significantly different percentageof their collagen content than the untreated controlexplants (data not shown, p> 0.05).
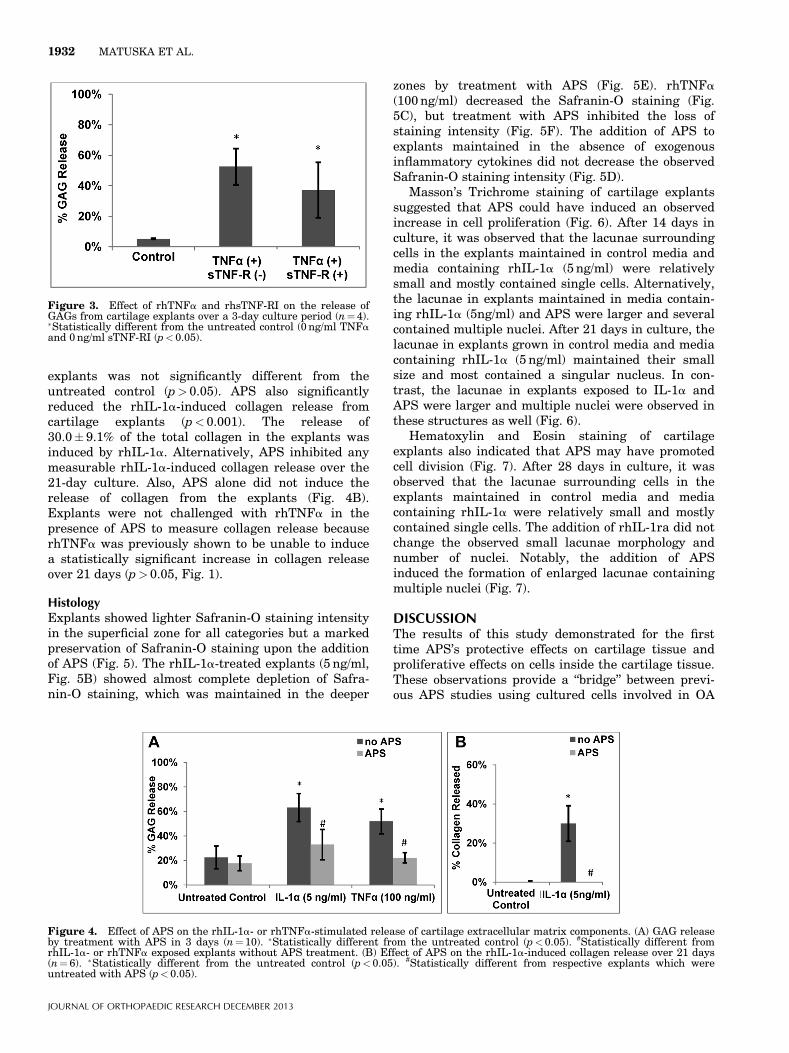
Pre-incubating cartilage explants with a recombi-nant inhibitor of TNFa decreased the release of GAGs.Specifically, pre-incubating explants with 50-fold morerhsTNF-RI (5,000ng/ml) than rhTNFa (100ng/ml)reduced average rhTNFa-stimulated GAG release ofthe explants from 52.6�11.9% to 37.2�18.1% overthe course of a 3-day culture period (Fig. 3). However,this reduction in percent GAG released was notstatistically significant (p>0.05).
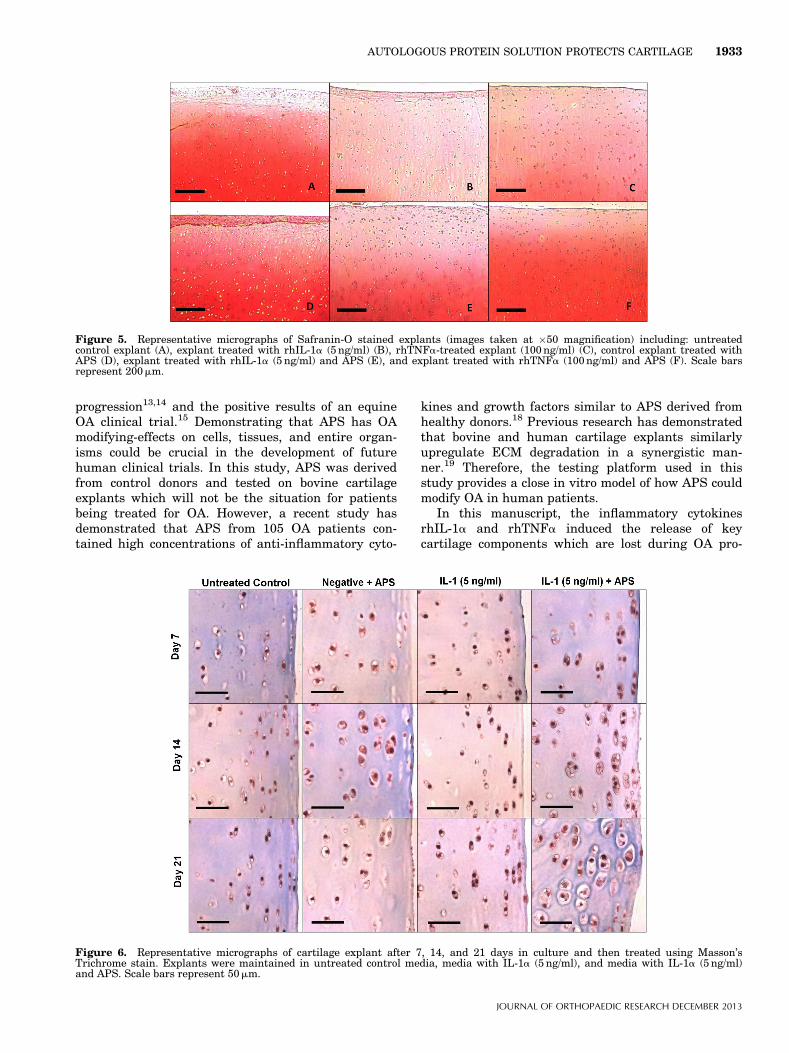
Autologous Protein Solution in Cartilage Explant AssayAPS significantly inhibited both rhIL-1a- (p<0.001)and rhTNFa- (p< 0.001) induced GAG release over thecourse of a 3-day culture period (Fig. 4A). Specifically,treatment with APS decreased the percent GAGreleased from rhIL-1a-treated explants from63.2� 11.4% to 33.0� 12.3% with APS. APS also had asimilar effect on rhTNFa-treated explants. For exam-ple, explants treated with rhTNFa alone released51.8� 10.1% of their total GAG content, whereasexplants treated with rhTNFa and APS released only22.2� 4.2% of their GAG content (p<0.001). Further-more, the percent GAG released from APS-treated
Figure 1. Effect of inflammatory cytokines rhIL-1a and rhTNFa on the percent GAG and collagenreleased from cartilage explants. (A) The cumula-tive percent of total GAG released from rhIL-1a-and rhTNFa-stimulated explants over 21 days inculture (n¼4). �Statistically different from theuntreated control (p<0.05). (B) The cumulativepercent of total collagen released from rhIL-1a-and rhTNFa-stimulated explants over 21 days(n¼ 4). �Statistically different from the untreatedcontrol (p< 0.05).
Figure 2. Effect of rhIL-1ra and rhIL-1a on the release of GAGs and collagen from cartilage explants. (A) Percent GAG released frombovine cartilage explants without exogenous cytokines, exposed to rhIL-1a, or exposed to rhIL-1a and rhIL-1ra over the course of3 days (n¼ 4). �Statistically different from the untreated control (p<0.05). #Statistically different from the explants treated with rhIL-1a only (p<0.05). (B) Percent collagen released from bovine cartilage explants without exogenous cytokines, exposed to rhIL-1a, orexposed to rhIL-1a and rhIL-1ra over the course of 3 days (n¼4). �Statistically different from the untreated control (p<0.05).
AUTOLOGOUS PROTEIN SOLUTION PROTECTS CARTILAGE 1931
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013
explants was not significantly different from theuntreated control (p>0.05). APS also significantlyreduced the rhIL-1a-induced collagen release fromcartilage explants (p<0.001). The release of30.0� 9.1% of the total collagen in the explants wasinduced by rhIL-1a. Alternatively, APS inhibited anymeasurable rhIL-1a-induced collagen release over the21-day culture. Also, APS alone did not induce therelease of collagen from the explants (Fig. 4B).Explants were not challenged with rhTNFa in thepresence of APS to measure collagen release becauserhTNFa was previously shown to be unable to inducea statistically significant increase in collagen releaseover 21 days (p>0.05, Fig. 1).
HistologyExplants showed lighter Safranin-O staining intensityin the superficial zone for all categories but a markedpreservation of Safranin-O staining upon the additionof APS (Fig. 5). The rhIL-1a-treated explants (5 ng/ml,Fig. 5B) showed almost complete depletion of Safra-nin-O staining, which was maintained in the deeper
zones by treatment with APS (Fig. 5E). rhTNFa(100ng/ml) decreased the Safranin-O staining (Fig.5C), but treatment with APS inhibited the loss ofstaining intensity (Fig. 5F). The addition of APS toexplants maintained in the absence of exogenousinflammatory cytokines did not decrease the observedSafranin-O staining intensity (Fig. 5D).
Masson’s Trichrome staining of cartilage explantssuggested that APS could have induced an observedincrease in cell proliferation (Fig. 6). After 14 days inculture, it was observed that the lacunae surroundingcells in the explants maintained in control media andmedia containing rhIL-1a (5 ng/ml) were relativelysmall and mostly contained single cells. Alternatively,the lacunae in explants maintained in media contain-ing rhIL-1a (5ng/ml) and APS were larger and severalcontained multiple nuclei. After 21 days in culture, thelacunae in explants grown in control media and mediacontaining rhIL-1a (5 ng/ml) maintained their smallsize and most contained a singular nucleus. In con-trast, the lacunae in explants exposed to IL-1a andAPS were larger and multiple nuclei were observed inthese structures as well (Fig. 6).
Hematoxylin and Eosin staining of cartilageexplants also indicated that APS may have promotedcell division (Fig. 7). After 28 days in culture, it wasobserved that the lacunae surrounding cells in theexplants maintained in control media and mediacontaining rhIL-1a were relatively small and mostlycontained single cells. The addition of rhIL-1ra did notchange the observed small lacunae morphology andnumber of nuclei. Notably, the addition of APSinduced the formation of enlarged lacunae containingmultiple nuclei (Fig. 7).
DISCUSSIONThe results of this study demonstrated for the firsttime APS’s protective effects on cartilage tissue andproliferative effects on cells inside the cartilage tissue.These observations provide a “bridge” between previ-ous APS studies using cultured cells involved in OA
Figure 4. Effect of APS on the rhIL-1a- or rhTNFa-stimulated release of cartilage extracellular matrix components. (A) GAG releaseby treatment with APS in 3 days (n¼10). �Statistically different from the untreated control (p<0.05). #Statistically different fromrhIL-1a- or rhTNFa exposed explants without APS treatment. (B) Effect of APS on the rhIL-1a-induced collagen release over 21 days(n¼ 6). �Statistically different from the untreated control (p< 0.05). #Statistically different from respective explants which wereuntreated with APS (p< 0.05).
Figure 3. Effect of rhTNFa and rhsTNF-RI on the release ofGAGs from cartilage explants over a 3-day culture period (n¼ 4).�Statistically different from the untreated control (0 ng/ml TNFaand 0ng/ml sTNF-RI (p< 0.05).
1932 MATUSKA ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013
progression13,14 and the positive results of an equineOA clinical trial.15 Demonstrating that APS has OAmodifying-effects on cells, tissues, and entire organ-isms could be crucial in the development of futurehuman clinical trials. In this study, APS was derivedfrom control donors and tested on bovine cartilageexplants which will not be the situation for patientsbeing treated for OA. However, a recent study hasdemonstrated that APS from 105 OA patients con-tained high concentrations of anti-inflammatory cyto-
kines and growth factors similar to APS derived fromhealthy donors.18 Previous research has demonstratedthat bovine and human cartilage explants similarlyupregulate ECM degradation in a synergistic man-ner.19 Therefore, the testing platform used in thisstudy provides a close in vitro model of how APS couldmodify OA in human patients.
In this manuscript, the inflammatory cytokinesrhIL-1a and rhTNFa induced the release of keycartilage components which are lost during OA pro-
Figure 5. Representative micrographs of Safranin-O stained explants (images taken at �50 magnification) including: untreatedcontrol explant (A), explant treated with rhIL-1a (5 ng/ml) (B), rhTNFa-treated explant (100ng/ml) (C), control explant treated withAPS (D), explant treated with rhIL-1a (5 ng/ml) and APS (E), and explant treated with rhTNFa (100ng/ml) and APS (F). Scale barsrepresent 200mm.
Figure 6. Representative micrographs of cartilage explant after 7, 14, and 21 days in culture and then treated using Masson’sTrichrome stain. Explants were maintained in untreated control media, media with IL-1a (5 ng/ml), and media with IL-1a (5 ng/ml)and APS. Scale bars represent 50mm.
AUTOLOGOUS PROTEIN SOLUTION PROTECTS CARTILAGE 1933
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013

gression (Fig. 1) and resulted in prominent decreasesin Safranin-O staining in the superficial layers of thecartilage explants (Fig. 5). Previous research hasdemonstrated that explants of human knees from OApatients showed co-localization of chondrocyte apopto-sis and a loss of Safranin-O staining,20 which maysuggest APS could have a chondroprotective effect bypreventing cell death and the loss of proteoglycancontent in the explants. Further research is planned todelineate the effect of APS on cell viability.
The anti-inflammatory cytokines in APS may haveprovided one of the key mechanisms driving itschondroprotective effects. Literature has estimatedthat 10–1,000-fold excesses of rhIL-1ra and 300-foldexcess rhsTNF-R have been required to block theeffects of IL-1 and TNFa by 80% or more.21,22 Previousanalysis has shown that APS contains 6,000 timesmore IL-1ra than IL-1 (a and b) and 3,500 times moresTNF-R (I and II) than TNFa.13 Furthermore, the250ml doses used to treat IL-1a- or TNFa-dosedexplants contained approximately 7.7 ng IL-1ra and3ng sTNF-R, which was well below the doses ofrecombinant IL-1ra and sTNF-R used to inhibit matrixdegradation (Figs. 2–3). Therefore, APS may haveinhibited the additional inflammatory pathways initi-ated by IL-1 or TNFa when the effect of IL-1ra orsTNF-R alone was rendered ineffective.
Anabolic growth factors may also have contributed tothe observed proliferative effects of APS. Notably, rhIL-1ra did not induce observed proliferative effects (Fig. 7).APS contains a statistically significant concentrationincrease of the following anabolic cytokines over base-line blood: EGF, IGF-I, PDGF-AB and -BB, VEGF, andTGF-b1.13 Furthermore, a recent study has measuredelevated anabolic growth factor concentrations in theAPS derived from 105 OA patients.18 The importance ofsynergistic growth factors on chondrocyte metabolismand subsequent cartilage growth has been previouslydemonstrated.23 IGF-I and TGF-b1 or -b2 has beenshown to induce aggrecan and type II collagen produc-
tion from articular chondrocytes when neither aloneinduced a cellular response.24 These results suggestthat autologous solutions containing multiple anti-in-flammatory and anabolic growth factors could enablesynergistic effects to drive the treatment of OA.
The two primary mechanisms of action a diseasemodifying osteoarthritis drug (DMOAD) would beexpected to utilize include anti-catabolic agents to slowOA progression and anabolic agents to induce cartilageregeneration.25 In this assay, APS reduced or eliminatedboth IL-1a- or TNFa-induced GAG and collagen releasefrom cartilage explants (Figs. 4–5). Furthermore, APSincreased the size of chondrocytes’ lacunae and in-creased the number of lacunae with multiple nuclei(Figs. 6–7). Similar histology has been observed whensupraphysiologic concentrations of fibroblast growthfactor-2 (FGF2) have been used to induce cartilageregeneration in vivo which suggests that APS mayinstruct cartilage repair.26 Future studies will enablethe further characterization of the proliferative effectsof APS on chondrocytes to ensure APS induces healthycartilage repair. Given that APS contains both anti-inflammatory and anabolic factors, has been shown toinhibit collagen degradation and may induce chondro-cyte proliferation, the potential for APS as an effectivetreatment for OA is promising. Further studies arewarranted to determine the efficacy and long-termoutcome of APS for the treatment of human OA.
ACKNOWLEDGMENTSBiomet Biologics provided funding for this research. K.O., W.-K., and J.W.M. are current employees of Biomet Biologics. A.-M. was employed by Biomet Biologics at the timeexperiments were performed.
REFERENCES1. Goldring MB. 2001. Anticytokine therapy for osteoarthritis.
Expert Opin Biol Ther 1:817–829.2. Sandell LJ, Aigner T. 2001. Articular cartilage and changes
in arthritis. An introduction: cell biology of osteoarthritis.Arthritis Res 3:107–113.
Figure 7. Representative micrographs of cartilage explant after 28 days in culture and then treated using Hematoxylin and Eosinstain. Explants were maintained in untreated control media, media with IL-1a, media with IL-1a and IL-1ra, and media with IL-1aand APS. Scale bars represent 200mm.
1934 MATUSKA ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013
3. Pratta MA, Yao W, Decicco C, et al. 2003. Aggrecan protectscartilage collagen from proteolytic cleavage. J Biol Chem278:45539–45545.
4. Ellis AJ, Curry VA, Powell EK, et al. 1994. The preventionof collagen breakdown in bovine nasal cartilage by TIMP,TIMP-2 and a low molecular weight synthetic inhibitor.Biochem Biophys Res Commun 201:94–101.
5. Billinghurst RC, Dahlberg L, Ionescu M, et al. 1997.Enhanced cleavage of type II collagen by collagenases inosteoarthritic articular cartilage. J Clin Invest 99:1534–1545.
6. Silver FH, Bradica G, Tria A. 2001. Relationship amongbiomechanical, biochemical, and cellular changes associatedwith osteoarthritis. Crit Rev Biomed Eng 29:373–391.
7. Chevalier X, Goupille P, Beaulieu AD, et al. 2009. Intraartic-ular injection of anakinra in osteoarthritis of the knee: amulticenter, randomized, double-blind, placebo-controlledstudy. Arthritis Rheum 61:344–352.
8. Keystone EC, Kavanaugh AF, Sharp JT, et al. 2004.Radiographic, clinical, and functional outcomes of treatmentwith adalimumab (a human anti-tumor necrosis factormonoclonal antibody) in patients with active rheumatoidarthritis receiving concomitant methotrexate therapy: arandomized, placebo-controlled, 52-week trial. ArthritisRheum 50:1400–1411.
9. Magnano MD, Chakravarty EF, Broudy C, et al. 2007. Apilot study of tumor necrosis factor inhibition in erosive/inflammatory osteoarthritis of the hands. J Rheumatol 34:1323–1327.
10. Eppley BL, Pietrzak WS, Blanton M. 2006. Platelet-richplasma: a review of biology and applications in plasticsurgery. Plast Reconstr Surg 118:147e–159e.
11. Patel S, Dhillon MS, Aggarwal S, et al. 2013. Treatmentwith platelet-rich plasma is more effective than placebo forknee osteoarthritis: a prospective, double-blind, randomizedtrial. Am J Sports Med 41:356–364.
12. Filardo G, Kon E, Di MA, et al. 2012. Platelet-rich plasma vshyaluronic acid to treat knee degenerative pathology: studydesign and preliminary results of a randomized controlledtrial. BMC Musculoskelet Disord 13:229.
13. Woodell-May J, Matuska A, Oyster M, et al. 2011. Autolo-gous protein solution inhibits MMP-13 production by IL-1beta and TNFalpha-stimulated human articular chondro-cytes. J Orthop Res 29:1320–1336.
14. O’Shaughnessey KM, Panitch A, Woodell-May JE. 2011.Blood-derived anti-inflammatory protein solution blocks theeffect of IL-1beta on human macrophages in vitro. InflammRes 60:929–936.
15. Bertone AL, Ishihara A, Zekas L, et al. 2012. Intra-articularuse of autologous protein solution for the treatment ofequine osteoarthritis. Abstract. ACVS Veterinary Sympo-sium, November 1–3, National Harbor, MD.
16. Mort JS, Roughley PJ. 2007. Measurement of glycosamino-glycan release from cartilage explants. Methods Mol Med135:201–209.
17. Creemers LB, Jansen DC, van Veen-Reurings A, et al. 1997.Microassay for the assessment of low levels of hydroxypro-line. Biotechniques 22:656–658.
18. O’Shaughnessey KM, Matuska A, Hoeppner J, et al. AnAutologous Protein Solution prepared from the blood ofosteoarthritic patients contains an enhanced profile of anti-inflammatory cytokines and anabolic growth factors. InSubmission.
19. Patwari P, Cook MN, DiMicco MA, et al. 2003. Proteoglycandegradation after injurious compression of bovine andhuman articular cartilage in vitro: interaction with exoge-nous cytokines. Arthritis Rheum 48:1292–1301.
20. Hashimoto S, Ochs RL, Komiya S, et al. 1998. Linkage ofchondrocyte apoptosis and cartilage degradation in humanosteoarthritis. Arthritis Rheum 41:1632–1638.
21. Wehling P, Moser C, Frisbie D, et al. 2007. Autologousconditioned serum in the treatment of orthopedic diseases:the orthokine therapy. BioDrugs 21:323–332.
22. Van Zee KJ, Kohno T, Fischer E, et al. 1992. Tumor necrosisfactor soluble receptors circulate during experimental andclinical inflammation and can protect against excessivetumor necrosis factor alpha in vitro and in vivo. Proc NatlAcad Sci USA 89:4845–4849.
23. Asanbaeva A, Masuda K, Thonar EJ, et al. 2008. Regulationof immature cartilage growth by IGF-I, TGF-beta1, BMP-7,and PDGF-AB: role of metabolic balance between fixedcharge and collagen network. Biomech Model Mechanobiol7:263–276.
24. Yaeger PC, Masi TL, de Ortiz JL, et al. 1997. Synergisticaction of transforming growth factor-beta and insulin-likegrowth factor-I induces expression of type II collagen andaggrecan genes in adult human articular chondrocytes. ExpCell Res 237:318–325.
25. Le Graverand-Gastineau MP. 2010. Disease modifying osteo-arthritis drugs: facing development challenges and choosingmolecular targets. Curr Drug Targets 11:528–535.
26. Henson FM, Bowe EA, Davies ME. 2005. Promotion of theintrinsic damage-repair response in articular cartilage byfibroblastic growth factor-2. Osteoarthritis Cartilage 13:537–544.
AUTOLOGOUS PROTEIN SOLUTION PROTECTS CARTILAGE 1935
JOURNAL OF ORTHOPAEDIC RESEARCH DECEMBER 2013