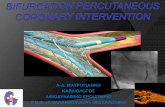
A pilot study of chronic, low-dose epoetin-β following percutaneous coronary intervention suggests...
9
..................................................................................................................................................................................... ..................................................................................................................................................................................... A pilot study of chronic, low-dose epoetin- b following percutaneous coronary intervention suggests safety, feasibility, and efficacy in patients with symptomatic ischaemic heart failure Martin W. Bergmann 1,2 * † , Sven Haufe 2 , Florian von Knobelsdorff-Brenkenhoff 1 , Heidrun Mehling 2 , Ralf Waßmuth 1 , Ines Mu ¨ nch 3 , Andreas Busjahn 3 , Jeanette Schulz-Menger 1 , Jens Jordan 2 , Friedrich C. Luft 1,2 , and Rainer Dietz 4 1 Franz-Volhard Clinic, Charite ´ Campus Buch, Berlin, Germany; 2 Franz-Volhard Clinical Research Center, Experimental and Clinical Research Center, Charite ´ Campus Buch, Berlin, Germany; 3 HealthTwist GmbH, Berlin, Germany; and 4 Department of Cardiology, Charite ´ Campus Buch & Campus Virchow, Berlin, Germany Received 19 August 2010; revised 4 November 2010; accepted 8 November 2010 Aims Low-dose epoetin-b improved neo-angiogenesis and cardiac regeneration in experimental models of ischaemic car- diomyopathy without raising haemoglobin. No clinical study has tested this approach to date. Methods and results We performed a randomized, placebo-controlled, double-blind, single-centre study of 35 IU/kg body weight epoetin-b given subcutaneously once weekly for 6 months started within 3 weeks after successful percutaneous coronary intervention (PCI). Patients were included if they presented with a lesion within the proximal segment of the left anterior descending artery, the right coronary artery, or circumflex and had symptomatic heart failure. Patients with ST-segment elevation due to an acute myocardial infarct were excluded. The outcome variables were measured at baseline and at 6 months. Primary outcome measure was individual change in ejection fraction; secondary outcome was safety, change in N-terminal pro-brain natriuretic peptide, and peak VO 2 . Twenty-four patients completed the 6-month treatment course. No adverse event related to the treatment occurred. Low-dose epoetin-b following PCI significantly improved global ejection fraction as measured by echocardiogra- phy (EPO: DEF 5.2 + 2.0%, P ¼ 0.013; placebo: DEF 0.3 + 1.6%, P ¼ 0.851; P ¼ 0.019 for the inter-group differ- ence) and cardiac magnetic resonance (EPO: DEF 3.1 + 1.6%, P ¼ 0.124; placebo: 21.9 + 1.2%, P ¼ 0.167; P ¼ 0.042 for the inter-group difference). N-terminal pro-brain natriuretic peptide levels decreased in both groups without significant inter-group differences. Peak VO 2 levels increased significantly by 3.9 + 1.1% (P , 0.05) in the EPO group, whereas in the placebo group the increase did not reach statistical significance (Dpeak VO 2 3.0 + 1.6, P ¼ ns). No significant difference regarding peak VO 2 was observed between the EPO and placebo groups. Conclusions Low-dose epoetin-b treatment following PCI is safe and feasible, and has possible beneficial effects on global ejection fraction and measures of exercise capacity. Extended low-dose epoetin-b treatment warrants further mechanistic studies as well as larger clinical trials. Clinical Trial Registration Information: NCT00568542 ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Heart failure † Growth substances † Ischaemia * Corresponding author. Tel: +49 40 1818852309, Fax: +49 40 181885 4444, Email: [email protected] † Present address. Department of Cardiology, ASKLEPIOS Klinik St Georg, Lohmu ¨hlenstr. 5, 20099 Hamburg, Germany. Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected]. European Journal of Heart Failure (2011) 13, 560–568 doi:10.1093/eurjhf/hfr002
Transcript of A pilot study of chronic, low-dose epoetin-β following percutaneous coronary intervention suggests...

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
A pilot study of chronic, low-dose epoetin-bfollowing percutaneous coronary interventionsuggests safety, feasibility, and efficacy in patientswith symptomatic ischaemic heart failureMartin W. Bergmann 1,2*†, Sven Haufe2, Florian von Knobelsdorff-Brenkenhoff 1,Heidrun Mehling2, Ralf Waßmuth1, Ines Munch3, Andreas Busjahn3,Jeanette Schulz-Menger 1, Jens Jordan2, Friedrich C. Luft1,2, and Rainer Dietz4
1Franz-Volhard Clinic, Charite Campus Buch, Berlin, Germany; 2Franz-Volhard Clinical Research Center, Experimental and Clinical Research Center, Charite Campus Buch, Berlin,Germany; 3HealthTwist GmbH, Berlin, Germany; and 4Department of Cardiology, Charite Campus Buch & Campus Virchow, Berlin, Germany
Received 19 August 2010; revised 4 November 2010; accepted 8 November 2010
Aims Low-dose epoetin-b improved neo-angiogenesis and cardiac regeneration in experimental models of ischaemic car-diomyopathy without raising haemoglobin. No clinical study has tested this approach to date.
Methodsand results
We performed a randomized, placebo-controlled, double-blind, single-centre study of 35 IU/kg body weightepoetin-b given subcutaneously once weekly for 6 months started within 3 weeks after successful percutaneouscoronary intervention (PCI). Patients were included if they presented with a lesion within the proximal segmentof the left anterior descending artery, the right coronary artery, or circumflex and had symptomatic heart failure.Patients with ST-segment elevation due to an acute myocardial infarct were excluded. The outcome variableswere measured at baseline and at 6 months. Primary outcome measure was individual change in ejection fraction;secondary outcome was safety, change in N-terminal pro-brain natriuretic peptide, and peak VO2. Twenty-fourpatients completed the 6-month treatment course. No adverse event related to the treatment occurred.Low-dose epoetin-b following PCI significantly improved global ejection fraction as measured by echocardiogra-phy (EPO: DEF 5.2+2.0%, P ¼ 0.013; placebo: DEF 0.3+1.6%, P ¼ 0.851; P ¼ 0.019 for the inter-group differ-ence) and cardiac magnetic resonance (EPO: DEF 3.1+ 1.6%, P ¼ 0.124; placebo: 21.9+1.2%, P ¼ 0.167;P ¼ 0.042 for the inter-group difference). N-terminal pro-brain natriuretic peptide levels decreased in bothgroups without significant inter-group differences. Peak VO2 levels increased significantly by 3.9+1.1%(P , 0.05) in the EPO group, whereas in the placebo group the increase did not reach statistical significance(Dpeak VO2 3.0+1.6, P ¼ ns). No significant difference regarding peak VO2 was observed between the EPOand placebo groups.
Conclusions Low-dose epoetin-b treatment following PCI is safe and feasible, and has possible beneficial effects on global ejectionfraction and measures of exercise capacity. Extended low-dose epoetin-b treatment warrants further mechanisticstudies as well as larger clinical trials.
Clinical Trial Registration Information: NCT00568542- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Heart failure † Growth substances † Ischaemia
* Corresponding author. Tel: +49 40 1818852309, Fax: +49 40 181885 4444, Email: [email protected]† Present address. Department of Cardiology, ASKLEPIOS Klinik St Georg, Lohmuhlenstr. 5, 20099 Hamburg, Germany.
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected].
European Journal of Heart Failure (2011) 13, 560–568doi:10.1093/eurjhf/hfr002

IntroductionTreatment options and prognosis for patients with heart failurehave improved because of revascularization by percutaneous cor-onary intervention (PCI) or surgical means, drug therapy, and noveldevice-based treatments. Nevertheless, mortality and morbidityremain high. Heart failure currently accounts for 5% of hospitaladmissions in Western Europe, making heart failure the common-est cause for emergency department care.1 Cardiac regenerationcould be a future treatment option. Experimental studies and clini-cal trials suggest that neo-angiogenesis and cardiomyocyte regen-eration are feasible.2 Intra-coronary cell therapy andintra-myocardial bone marrow cell injections have accrued interestin open-label studies; however, randomized trials have shownmixed results.3,4
The use of growth factors has also been promulgated. However,clinical studies of single high doses of granulocyte-colony-stimulating factor (G-CSF) or erythropoietin following acute myo-cardial infarct were disappointing.5 Recently, the HEBE III trialinvestigated the use of a single high dose of epoetin following anacute myocardial infarct. No significant effect on left ventricular(LV) ejection fraction, the primary endpoint, was observed.However, adverse cardiac events, a secondary endpoint, were sig-nificantly reduced in the EPO group.6 Erythropoietin has beenstudied extensively in patients with anaemia and heart failure.But, aside from smaller surrogate-parameter studies,7,8 no largerandomized trial has confirmed a benefit in raising haemoglobinlevels to .12 mg/dL. In fact, studies aimed at increasing haemo-globin to 14 mg/dL rather than the 12 mg/dL recommended incurrent guidelines in pre-dialysis patients yielded a neutral heartfailure-related outcome.9– 11
However, low-dose, long-term epoetin not aimed at increasinghaemoglobin could have beneficial effects on cardiac remodellingby several mechanisms, including the promotion of angiogen-esis.12– 14 Epoetin-b, administered at doses as low as 30 IU/kgper week, mobilized endothelial progenitor cells from the bonemarrow and increased functionally active endothelial progenitorcells in peripheral blood.15 Interestingly, epoetin increases circulat-ing endothelial progenitor cell levels by itself; however, improvedmicrovascularization depends on the additional presence of localischaemia.16 Thus, chronic, low-dose epoetin-b treatment follow-ing PCI for macrovascular ischaemia may exert beneficial effectson LV function beyond the effects of PCI alone.
Methods
Patient populationPatients were eligible if they presented with symptomatic heart failureNYHA ≥II, elevated N-terminal pro-brain natriuretic peptide(NT-proBNP) levels (.2× upper norm) and a significant stenosis inthe proximal segment of the right coronary artery, the left anteriordescending artery, or the circumflex artery. Patients were screenedafter successful revascularization by PCI for the stenotic lesion. Thepatients were required to demonstrate globally reduced ejection frac-tion or at least a regional wall motion defect in the area of the stenoticlesion. During screening, wall motion defects were detected byLV angiography, echocardiography, or cardiac magnetic resonance
imaging (cardiac MRI) at the time of PCI. Patients with acuteST-segment elevated infarct or unprotected left main were excluded.Patients with elevated troponin T as a marker of an acute coronarysyndrome were allowed to enter the trial if they did not presentwith any other exclusion criteria.
These inclusion criteria resulted in a heterogeneous group ofpatients in terms of ejection fraction. However, all patients alsodemonstrated elevated LV end-diastolic pressure .15 mmHg. Allpatients received an angiotensin-converting enzyme (ACE) inhibitoror angiotensin receptor blocker and a b-blocker if not intolerant tothe drugs. Within 3 weeks following successful PCI of a major coron-ary vessel, patients were asked for informed consent if they fulfilled theinclusion criteria and did not exhibit any of the following exclusion cri-teria: valvular heart disease, contraindication for cardiac MRI (pace-maker, implantable cardioverter, metal implants, and claustrophobia),uncontrolled hypertension (resting blood pressure .180/100 mmHg), haemoglobin .16 mg/dL, or thrombocytosis. Patientsaged .75 years and pre-menopausal women were not included.Patients with active malignancy, severe renal dysfunction (serum crea-tinine .3.0 mg/dL), chronic liver disease, or indication for open-labelepoetin treatment were also excluded. We excluded patients withiron deficiency (ferritin ,50 mg/mL and/or transferrin saturation,20%) or anaemia (Hb ,12 mg/dL) and patients with neurologicaldiseases, including a prior stroke. Serum vitamin B12 levels wererequired to be within the normal range. We also excluded patientswith earlier in-stent restenosis or stent thrombosis.
The ethics committee of Berlin as well as the BfArM (Bundesamt furArzneimittel und Medizinprodukte) regulatory agency approved thestudy and written informed consent was obtained (Eudra-CT2004-002646-35; ClinicalTrials.gov NCT00568542).
Study protocolFollowing informed consent, patients underwent measurement of LVfunction, laboratory values including NT-proBNP, and exercisecapacity. The measurements were performed around day 13.4+3.2after PCI. No measurement was made within the first 7 days orlater than 21 days after PCI. Subjects received either weight-adjustedsubcutaneous epoetin-b (35 IU/kg) or placebo once a week for 6months by self-injecting with a pen (NeoRecormonw). The clinicaltrials unit at Charite Campus Virchow randomized the patients andprovided them with vials for loading the injection pen. Patients weretrained to self-inject epoetin-b or placebo. Patients, doctors, andstudy nurses were blinded to the investigational product; compliancewas checked by inspecting the vial when patients returned forexchange. Data were entered on-site into a centralized databasewith regular external monitoring (Figure 1). The primary endpointwas change from baseline to 6 months in cardiac MRI and echocardio-graphically determined global ejection fraction. Secondary endpointswere changes in exercise capacity, NT-proBNP, and regional wallmotion. Safety endpoints were adverse events, laboratory values,blood pressure, and repeat revascularization.
MeasurementsStudy visits were undertaken after 4 weeks, 3 months, and 6 months.Assessments performed at baseline and at 6 months included echocar-diography, cardiac MRI, serum erythropoietin levels, and NT-proBNP.Haemoglobin, haematocrit, serum creatinine, oscillometric seatedblood pressure, and heart rate were assessed at every visit. Echocar-diography was performed according to current guidelines; we usedthe American Society of Echocardiography 16-segment model toassess regional wall motion. Endocardial borders were manually
Epoetin-b in ischaemic heart failure 561

traced from the apical four- and two-chamber views to calculate percent ejection fraction using the biplane summation-of-discs methodincluded in current ultrasound machines (Accuson Sequoia, Siemensand Vivid 7, GE Healthcare, Munchen, Germany). Experts, blinded tothe treatment, performed the studies and entered the values into theonline database. Cardiac MRI regional wall motion was determined bythe 17-segment model according to international guidelines. Left ventri-cular ejection fraction was measured using contiguous short-axis slicesaccording to the validated cardiac MRI laboratory standards. Expertsblinded to the treatment allocation performed the image analysis. Alldata were entered into the central database and regularly monitored.
All patients performed an incremental exercise test until volitionalexhaustion on a motorized treadmill (h/p Cosmos Mercury 4.0, Traun-stein, Germany) to assess oxygen uptake capacity and power output.Patients breathed through a disposable pneumotach. Exercise wasbegun at 0 W and increased by 25 W every 3 min until reaching themaximally tolerated workload (Vmax spectra 229D, Sensor Medics,Munchen, Germany).
Statistical analysisNo formal sample size calculation was performed as the trial was con-ceived as exploratory. All analysed subjects received the treatment towhich they were randomly assigned and were retained in the groupuntil endpoint. After completion of the study and final external moni-toring, the database was closed and the treatment code opened toperform the statistical analysis. As pre-specified, intra-individual
changes in ejection fraction and other endpoints were comparedbetween the two groups with either epoetin-b or placebo treatment.Categorical data were analysed by x2 tests. The Kolmogorov–Smirnovtest was applied to detect deviations from normal distribution. Weused Levene’s test, which is an inferential statistic used to assess theequality of variance in different samples. Intra-group differences werecompared by a one-sided paired t-test and inter-group differences byunpaired t-testing. For variables that were not normally distributed(NT-proBNP), the Mann–Whitney test was applied. A P , 0.05 wasconsidered statistically significant; nominal P-values are presented. Allresults are reported as mean+ SEM.
Results
Enrolment and baseline characteristicsWe recruited 32 patients. Four patients withdrew consent orpresented with exclusion criteria during the screening phaseafter providing informed consent. Of the remaining 28 patients,14 were assigned to receive placebo and 14 to receiveepoetin-b. In the EPO group, one patient dropped out of thestudy after receiving a cardiac resynchronization device. In thecontrol group, three patients did not finish the 6-month treat-ment course: two patients withdrew consent for personalreasons and one other patient received an intra-cardiac defibril-lator with cardiac resynchronization therapy. The two groups
Figure 1 Study algorithm and patient numbers. Haemoglobin and serum erythropoietin were measured to assess any haematopoietic effectsof the treatment. Ejection fraction was analysed by both echocardiography and cardiac magnetic resonance imaging at baseline and after com-pletion of the study at 6 months as primary outcome measures. Secondary outcome measures were change in N-terminal pro-brain natriureticpeptide levels, peak VO2, and diastolic E/E′ between these time points.
M.W. Bergmann et al.562

were well matched in terms of baseline characteristics (Table 1).The EPO group presented with lower end-diastolic pressure atthe time of PCI (placebo: 24+2.2 mmHg; epoetin-b: 17.6+2.3 mmHg) as well as reduced LV end-diastolic diameter index(placebo: 115+12.4 mL/m2; epoetin-b: 85+6 mL/m2;Table 1). We considered that a multivariate analysis of theresults was not feasible given the low patient numbers in bothgroups. It is possible that this deviation may have influencedthe overall results; however, other parameters such as peak
VO2 showed some discrepancy in favour of the placebo group(placebo: 22+2.9; epoetin-b: 18.8+ 1.8) and ejection fractionwas distributed normally in both groups.
In the placebo group, more patients received a drug-elutingstent; however, the lesion type according to the AmericanCollege of Cardiology classification was not different. The patientspresented with moderate heart failure as judged by ejection frac-tion, NT-proBNP levels, and peak VO2 at baseline. All patientsalso had diastolic dysfunction as shown by elevated LV
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Baseline characteristics and details of the percutaneous coronary intervention procedure (fiducial limits,mean+++++SEM)
Placebo EPO group Significance (P)
Clinical features
Age (years) (mean+ SEM) 61.8+3.0 61.0+1.7 ns, P ¼ 0.25
Male/female (n) 9/2 12/1 ns, P ¼ 0.56
Risk factorsa (no. of patients with 1/2/3/4/5 risk factors) 1/5/3/2/0 0/5/4/2/2 ns, P ¼ 0.21
Body mass index 29.3+1.2 28.3+0.8 ns, P ¼ 0.66
Prior myocardial infarction [n (%)] 6 (54) 4 (31) ns, P ¼ 0.49
Acute coronary syndrome (%) 4 (36) 5 (38) ns, P ¼ 0.36
Vessels with .50% stenosis 2.1+0.3 1.9+0.2 ns, P ¼ 0.38
Drug eluting stent (%) 55% 31%
Medication
ACE [n (%)] 10 (91) 11 (84) ns, P ¼ 0.56
AT1 [n (%)] 2 (18) 3 (23) ns, P ¼ 0.59
Clopidogrel [n (%)] 11 (100) 13 (100) ns, P ¼ 0.71
Aspirin [n (%)] 10 (91) 12 (92) ns, P ¼ 0.72
Ca-antagonist [n (%)] 3 (27) 2 (15) ns, P ¼ 0.63
Statins [n (%)] 10 (91) 13 (100) ns, P ¼ 0.46
b-Blockers [n (%)] 11 (100) 13 (100) ns, P ¼ 0.78
Diuretics [n (%)] 4 (36) 2 (15) ns, P ¼ 0.42
Baseline measurements
Haemoglobin (mg/dL) 13.9+0.3 14.1+0.3 ns, P ¼ 0.68
Haematocrit (%) 42.1+1.1 42.3+3.4 ns, P ¼ 0.93
Leucocytes (×103/dL) 7.19+0.53 8.3+0.87 ns, P ¼ 0.3
Thrombocytes (×106/dL) 237+27.4 267+21.7 ns, P ¼ 0.41
NT-proBNP (pg/mL) 732+266 856+391 ns, P ¼ 0.80
Creatinine (mmol/L) 76+12 81+9 ns, P ¼ 0.91
HbA1c (%) 6.0+0.3 6.4+0.3 ns, P ¼ 0.35
Cholesterol (mmol/L) 3.93+0.36 3.97+0.12 ns, P ¼ 0.94
LDL-cholesterol (mmol/L) 2.4+1.01 2.5+0.9 ns, P ¼ 0.81
Erythropoietin (U/L, norm: 8–22 U/L) 8.4+1.2 14.7+2.6 P ¼ 0.06
Systolic/diastolic blood pressure (mmHg) 121+5.3/68+1.7 122+5.4/70+3.4 ns, P ¼ 0.85
Left ventricular end-diastolic pressure mmHg (normal ,12 mmHg) 24+2.2 17.6+2.3 P ¼ 0.06
E/E′ by echocardiography 15.2+5.1 13.9+2.6 ns, P ¼ 0.25
Ejection fraction (%; echocardiography) 46.4+3.3 48.4+2.5 ns, P ¼ 0.29
Left ventricular end-diastolic diameter index (mm/m2; echocardiography) 27.7+0.9 25.1+0.7 P ¼ 0.03
Ejection fraction (short-axis measurement cardiac MRI) (%) 47.4+5.7 49.6+3.7 ns, P ¼ 0.35
Left ventricular end-diastolic volume index by cardiac MRI (mL/m2) 115.4+12.4 85.2+6 P ¼ 0.03
Peak VO2 (mL/kg/min) 22+2.9 18.8+1.8 ns, P ¼ 0.46
NT-proBNP (pg/mL) 732+266 856+392 ns, P ¼ 0.82
aRisk factors: hypertension, hyperlipidaemia, adiposity (BMI .35), smoking, diabetes.
Epoetin-b in ischaemic heart failure 563

end-diastolic pressure and an elevated E/E′ ratio at baseline (seeTable 1 for details).
The patients were not anaemic; the baseline haemoglobin andhaematocrit values were normal, as were the iron-related values.By chance, the EPO group included two patients with relativelyelevated erythropoietin blood levels prior to treatment; thisresulted in a borderline higher average level of erythropoietin atbaseline (P ¼ 0.06) in that group. These two patients presentedwith haemoglobin values of 14.6 and 14.3 mg/dL and NT-proBNPlevels of 210 and 1623 pg/mL, respectively.
Epoetin-b treatmentPatients in the EPO group had significantly increased levels of ery-thropoietin at 6 months, compared with the placebo group (P ¼0.009, Figure 2A). No significant change in blood pressure, haema-tocrit, or haemoglobin was observed in either group (Figure 2B,Table 2). Pharmacological treatment of patients was in accordancewith current guidelines; in both groups, .95% of patients receiveda b-blocker, ACE-inhibitor or AT1-antagonist, statin, and aspirinplus clopidogrel during every planned visit (Table 1). During thestudy, no stent thrombosis or uncontrolled hypertension wasobserved. All patients were on dual-antiplatelet therapy through-out the study. One patient of the control group was re-admittedto the hospital for decompensated heart failure that resolvedwith nitroglycerin and furosemide; this was the only serious
adverse effect reported in the study. The episode was judged unre-lated to study treatment.
Quantitative measurement of leftventricular functionThe individual change in ejection fraction between baseline and6-month follow-up measured by echocardiography and cardiacMRI was greater in the EPO group than in the placebo group.Both methods of LV function measurement performed in thetrial, namely cardiac MRI and echocardiography, are reported ina combined fashion due to the low patient numbers. Epoetin-btreatment led to a significant increase (Figure 3A) in echocardio-graphic ejection fraction (DEF 5.7+ 1.9%, P , 0.05). Percutaneouscoronary intervention treatment alone plus placebo brought aboutno change in ejection fraction (DEF 0.3+1.6%, P ¼ ns). The EPOgroup had slightly higher ejection fractions, compared with placeboat baseline; the difference was not statistically significant. Thecardiac MRI measurements (Figure 3B) revealed an upward trendin ejection fraction in the EPO group (DEF ¼ 3.1+1.6%, P ¼ns), whereas the reverse was the case in the placebo group(DEF ¼ 21.9+1.2%, P ¼ ns). As a result, the comparisons ofthe intra-individual DEF baseline vs. 6-month follow-up betweenthe groups reached statistical significance (P , 0.05). Due tothe low patient numbers, we did not perform a multivariateanalysis. No difference in pharmacological treatment, blood
Figure 2 Levels of (A) erythropoietin and (B) haemoglobin in both study groups. Following treatment for 6 months, only the EPO treatmentgroup demonstrated increased erythropoietin levels compared with baseline levels. The EPO group by chance had two patients with elevatedlevels at baseline. No significant increase in haemoglobin was observed in either group.
M.W. Bergmann et al.564

pressure, or further interventions was observed. No significantchange in LV end-diastolic volume was detected. The DLVEDVover the 6 months was ,20 mL in both groups (DLVEDVplacebo group: +15+ 12.5 mL, P ¼ ns; EPO group: 0.1+8.4 mL, P ¼ ns). If anything, further ventricular dilation occurredin the placebo group, whereas the EPO group remained stablein terms of diameters and volume. No significant change in recov-ery of the regional wall motion defect at study entry could bedocumented by echo or cardiac MRI, probably due to the lowpatient numbers.
Heart failure assessmentWe also analysed other parameters of heart failure, namely bloodlevels of NT-proBNP and exercise tests. Both parametersimproved over the course of the study following PCI, without sig-nificant differences between EPO and placebo (Figure 4A and B).Peak VO2 levels increased significantly by 3.9+1.1%, P , 0.05 inthe EPO group. In the placebo group, we detected no significantchange (Dpeak VO2 3.0+1.6, P ¼ ns). No difference in thenumber of hospital admissions due to heart failure related to
Figure 3 Increase in ejection fraction following percutaneous coronary intervention plus low-dose epoetin-b over 6 months compared withpercutaneous coronary intervention plus placebo treatment. (A) Echocardiographic data from patients with complete measurements both atbaseline and at 6-month follow-up. The comparison between the groups revealed a significant change favouring the EPO treatment arm.(B) Cardiac magnetic resonance imaging data from all patients with complete analysis both at baseline and at 6-month follow-up. The compari-son between the groups revealed a significant change favouring the EPO treatment arm.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Safety data concerning haemoglobin levels and blood pressure (fiducial limits, mean+++++SEM)
Placebo EPO group Significance (P)
Haemoglobin (mg/dL)
Baseline 13.9+0.3 14.1+0.3 ns, P ¼ 0.68
4 weeks 13.8+0.3 14.5+0.3 ns, P ¼ 0.18
3 months 14.1+0.2 15.1+0.3 ns, P ¼ 0.59
6 months 14.3+0.2 14.9+0.4 ns, P ¼ 0.52
Blood pressure (mmHg)
Baseline 121+5.3/67+1.7 122+5.4/70+3.4 ns, P ¼ 0.85
4 weeks 116+5.4/65+2.4 126+5.8/70+3.3 ns, P ¼ 0.27
3 months 122+4.1/68+2.6 123+3.8/71+3.4 ns, P ¼ 0.80
6 months 123+3.6/65+2.2 117+3.8/66+2.6 ns, P ¼ 0.25
Epoetin-b in ischaemic heart failure 565

study drug assignment was observed during the 6-monthfollow-up.
The study population was quite heterogeneous regarding indi-vidual NT-proBNP levels at study entry, and the reductionduring the follow-up period possibly precluded any statistically rel-evant effects (Table 1, Figure 4B). However, the data on exercisecapacity revealed some interesting insights. Patients in bothgroups had a numerically increased aerobic capacity (EPO:16.4+1.8 to 20.3+ 1.9 mL/min/kg, P , 0.05; placebo: 19.3+1.8 to 22.3+3.4 mL/min/kg, P ¼ ns) and power output (EPO:120+ 16 to 152+17 W, P , 0.05; placebo: 129+21 to 140+27 W, P ¼ ns). The EPO group achieved significance, while theplacebo group did not. Moreover, maximum oxygen pulse wasenhanced more in the EPO group (25.4%, P , 0.05) than in theplacebo group (15.7%, P ¼ ns). These data suggest that epoetin-bmight have indeed improved cardiac function.
At the individual anaerobic threshold, we observed numericalincreases for oxygen pulse (EPO: 10.9+1 to 13.3+1.1, P ,
0.05; placebo: 12.7+ 0.9 to 13.7+ 1.1, P ¼ ns) and poweroutput (EPO: 70.3+10.7 to 80.7+ 10.1, P , 0.05; placebo: 0.656+10.7 to 68.7+ 11.4, P ¼ ns) with only slight changes inoxygen uptake. Again, the EPO group achieved significance, whilethe placebo group did not. No significant alterations wereobserved for lactate concentrations, either at individual anaerobic
threshold or at volitional exhaustion. The more pronounced adap-tations in patients who received EPO compared with the placebogroup suggested that improved cardiac function was responsiblefor these findings rather than metabolic adjustments.
DiscussionWe performed a double-blind, placebo-controlled pilot study toevaluate the effects of low-dose epoetin-b administered subcu-taneously, once a week for 6 months, on cardiac function inheart failure patients following PCI for significant coronarydisease. Heart failure was defined by dyspnoea, elevatedNT-proBNP levels, and measures of diastolic dysfunction (LV end-diastolic pressure and E/E′). We used epoetin-b doses that did notinfluence haemoglobin or haematocrit in these non-anaemicpatients. All patients had a regional wall motion defect in the ter-ritory of the coronary artery subjected to PCI. This pilot studyfound low-dose epoetin-b treatment to be feasible. Furthermore,we found evidence of improved LV function following epoetin-btreatment by means of two different imaging techniques, withintra-individual changes in ejection fraction analysed by expertreaders blinded to the treatment allocation. Furthermore, wefound evidence of improved cardiac performance with exercisefollowing epoetin-b treatment over 6 months. This is therefore
Figure 4 Peak VO2 and N-terminal pro-brain natriuretic peptide levels improved in both patient groups when all patients with complete dataat baseline and at follow-up were analysed. (A) Patients performed an exercise test at baseline and at the 6-month follow-up. There was nostatistical difference between the two groups. (B) N-terminal pro-brain natriuretic peptide levels were measured at baseline and after6 months. N-terminal pro-brain natriuretic peptide levels decreased in both groups with no significant differences between the groups.
M.W. Bergmann et al.566

the first study to provide evidence of improved LV remodellingafter chronic low-dose epoetin-b treatment. While this studywas only small and comes with all the limitations of a single-centrestudy, the double-blind, placebo-controlled nature of the study atleast encourages the design of larger randomized trials based onthis protocol. In addition, the study supports experimentalanimal data demonstrating improved LV remodelling throughepoetin-b-induced mobilization of functional endothelial progeni-tor cells.12,17
Erythropoietin has been tested in anaemic patients with heartfailure leading to an ongoing, multi-centre, randomized trial of dar-bepoetin in heart failure (RED-HF).18 This trial is aimed at correct-ing the anaemia often observed in association with severe heartfailure. Anaemia is associated with increased mortality in heartfailure but a causal relationship has not been established.19 Largestudies in pre-dialysis patients have failed to show a benefit of nor-malizing haemoglobin levels to .14 mg/dL, compared with a lowertarget of 12 mg/dL. Earlier studies of erythropoietin in heart failuresolely identified significant changes of exercise capacity rather thanparameters of LV remodelling. While in our study no significantdifferences in peak VO2 were observed between the groups, echo-cardiography and cardiac MRI both confirmed attenuation of LVremodelling. The exercise test revealed no significant effect onpeak VO2, but a significant effect on power output, which is afinding also in line with improved cardiac function rather thanmetabolic adjustments by oxygen uptake.
We found that low-dose epoetin-b treatment for 6 months wassafe. Larger doses of erythropoietin to avoid blood transfusions inpatients with chronic kidney disease or malignant disease may beharmful.20 Some studies suggest that erythropoietin treatmentcould be an option to reduce in-stent restenosis by acceleratingre-endothelialization of the injured endothelium. However, otherstudies have implied thrombocyte activation.21,22 Our study wassmall, but we nonetheless observed no stent thrombosis. Recentstudies have reached the same conclusion regarding single high-dose darbepoetin, a longer-acting erythropoietin analogue, follow-ing PCI after acute myocardial infarction.23 The HEBE III trial con-firmed this finding regarding safety and reported less cardiac eventsincluding stent thrombosis.6 Here, we excluded patients with anacute myocardial infarction. In addition, darbepoetin administered.26 weeks in patients with anaemia and chronic heart diseaseaimed at a target haemoglobin of 14+1.0 g/dL has also beenshown to be safe.7
Several small studies have supported the idea that erythro-poietin could exert pro-angiogenic effects by mobilizing endo-thelial progenitor cells even at low doses.13,15,16 In addition,the functional capacity of these endothelial progenitor cells, asmeasured by their migration capacity, is enhanced especiallywith chronic treatment.24 Improving endothelial function andneo-angiogenesis in ischaemic myocardial tissue has beenshown to be a valid strategy to attenuate LV remodelling bypreventing a mismatch between perfusion and cardiac hypertro-phy.25,26 Interestingly, ischaemia is necessary for erythropoietinto increase myocardial expression of vascular, endothelialgrowth factor, thereby stimulating homing and local proliferationof endothelial progenitor cells.13,16 This effect is specific to ery-thropoietin, while in principle mobilization of endothelial
progenitor cells is also achieved by other growth factors suchas G-CSF.27 However, G-CSF lacks any effects on homing andlocal proliferation of endothelial progenitor cells. Therefore,the negative results of recent clinical trials analysing the effectof G-CSF in patients following myocardial infarction cannot beextrapolated to erythropoietin treatment.28
Our pilot study is limited by its small sample size, the lack of apower calculation, and variations in patient baseline data. Nonethe-less, the patient characteristics were similar in both treatment arms,and treatment as well as data acquisition and analyses were con-ducted in a strict double-blind fashion. Retrospectively, differencesin LV end-diastolic pressure at the time of PCI as well as LV end-diastolic diameter index were observed. This may have influencedthe outcome over the 6-month treatment course, although dimen-sions did not change significantly over the treatment course.
We believe that the reported findings provide an improved per-spective for heart failure patients after coronary intervention. Per-cutaneous coronary intervention alone in elective patients withsymptoms of heart failure does not necessarily improve heart func-tion. Once-weekly low-dose epoetin-b treatment in addition toPCI is feasible, and the data suggest that the treatment may beeffective. Larger trials confirming this approach are warranted toreproduce this result and possibly to introduce this concept intoclinical practice in heart failure patients undergoing macrovascularrevascularization.
AcknowledgementsThe authors thank the Franz-Volhard Clinical Research Centerteam at Charite Campus Buch and the Pharmacy at ChariteCampus Virchow for expert help throughout the study.
FundingThis study was supported by a grant from the Roche Foundation ofAnemia Research (RoFAR). The study was solely investigator initiated;the granting agency played no role in the study or in the reportpreparation.
Conflict of interest: none declared.
References1. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P,
Poole-Wilson PA, Stromberg A, van Veldhuisen DJ, Atar D, Hoes AW,Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K, Vahanian A,Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C,Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M,Widimsky P, Zamorano JL. ESC Guidelines for the diagnosis and treatment ofacute and chronic heart failure 2008. Eur Heart J 2008;29:2388–2442.
2. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: the scientific foun-dations of cardiac repair. J Clin Invest 2005;115:572–583.
3. Schachinger V, Erbs S, Elsasser A, Haberbosch W, Hambrecht R,Holschermann H, Yu J, Corti R, Mathey DG, Hamm CW, Suselbeck T,Assmus B, Tonn T, Dimmeler S, Zeiher AM, the R-AMII. Intracoronary bonemarrow-derived progenitor cells in acute myocardial infarction. N Engl J Med2006;355:1210–1221.
4. Tendera M, Wojakowski W, Ruzyllo W, Chojnowska L, Kepka C, Tracz W,Musialek P, Piwowarska W, Nessler J, Buszman P, Grajek S, Breborowicz P,Majka M, Ratajczak MZ. Intracoronary infusion of bone marrow-derived selectedCD34+CXCR4+ cells and non-selected mononuclear cells in patients withacute STEMI and reduced left ventricular ejection fraction: results of randomized,multicentre Myocardial Regeneration by Intracoronary Infusion of Selected Popu-lation of Stem Cells in Acute Myocardial Infarction (REGENT) trial. Eur Heart J2009;30:1313–1321.
Epoetin-b in ischaemic heart failure 567

5. Zohlnhofer D, Dibra A, Koppara T, de Waha A, Ripa RS, Kastrup J, Valgimigli M,Schomig A, Kastrati A. Stem cell mobilization by granulocyte colony-stimulatingfactor for myocardial recovery after acute myocardial infarction: a meta-analysis.J Am Coll Cardiol 2008;51:1429–1437.
6. Voors AA, Belonje AM, Zijlstra F, Hillege HL, Anker SD, Slart RH, Tio RA, van’tHof A, Jukema JW, Peels HO, Henriques JP, Ten Berg JM, Vos J, van Gilst WH, vanVeldhuisen DJ. A single dose of erythropoietin in ST-elevation myocardial infarc-tion. Eur Heart J 2010;31:2593–2600.
7. Ponikowski P, Anker SD, Szachniewicz J, Okonko D, Ledwidge M, Zymlinski R,Ryan E, Wasserman SM, Baker N, Rosser D, Rosen SD, Poole-Wilson PA,Banasiak W, Coats AJ, McDonald K. Effect of darbepoetin alfa on exercise toler-ance in anemic patients with symptomatic chronic heart failure: a randomized,double-blind, placebo-controlled trial. J Am Coll Cardiol 2007;49:753–762.
8. Palazzuoli A, Silverberg D, Iovine F, Capobianco S, Giannotti G, Calabro A,Campagna SM, Nuti R. Erythropoietin improves anemia exercise tolerance andrenal function and reduces B-type natriuretic peptide and hospitalization inpatients with heart failure and anemia. Am Heart J 2006;152:1096 e9–1096 e15.
9. Drueke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC, Tsakiris D,Burger HU, Scherhag A. Normalization of hemoglobin level in patients withchronic kidney disease and anemia. N Engl J Med 2006;355:2071–2084.
10. Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, Reddan D, the CI.Correction of anemia with Epoetin alfa in chronic kidney disease. N Engl J Med2006;355:2085–2098.
11. Szczech LA, Barnhart HX, Sapp S, Felker GM, Hernandez A, Reddan D, Califf RM,Inrig JK, Patel UD, Singh AK. A secondary analysis of the CHOIR trial shows thatcomorbid conditions differentially affect outcomes during anemia treatment.Kidney Int 2010;77:239–246.
12. Lipsic E, Westenbrink BD, van der Meer P, van der Harst P, Voors AA, vanVeldhuisen DJ, Schoemaker RG, van Gilst WH. Low-dose erythropoietinimproves cardiac function in experimental heart failure without increasing haema-tocrit. Eur J Heart Fail 2008;10:22–29.
13. Westenbrink BD, Lipsic E, van der Meer P, van der Harst P, Oeseburg H, DuMarchie Sarvaas GJ, Koster J, Voors AA, van Veldhuisen DJ, van Gilst WH,Schoemaker RG. Erythropoietin improves cardiac function through endothelialprogenitor cell and vascular endothelial growth factor mediated neovasculariza-tion. Eur Heart J 2007;28:2018–2027.
14. Kleijn L, de Boer RA, Voors AA. Should erythropoietin treatment in chronic heartfailure be haemoglobin targeted? Eur J Heart Fail 2010;12:215–216.
15. Bahlmann FH, De Groot K, Spandau JM, Landry AL, Hertel B, Duckert T,Boehm SM, Menne J, Haller H, Fliser D. Erythropoietin regulates endothelial pro-genitor cells. Blood 2004;103:921–926.
16. Westenbrink BD, Oeseburg H, Kleijn L, van der Harst P, Belonje AM, Voors AA,Schoemaker RG, de Boer RA, van Veldhuisen DJ, van Gilst WH. Erythropoietinstimulates normal endothelial progenitor cell-mediated endothelial turnover,
but attributes to neovascularization only in the presence of local ischemia. Cardi-ovasc Drugs Ther 2008;22:265–274.
17. Gabel R, Klopsch C, Furlani D, Yerebakan C, Li W, Ugurlucan M, Ma N,Steinhoff G. Single high-dose intramyocardial administration of erythropoietinpromotes early intracardiac proliferation, proves safety and restores cardiac per-formance after myocardial infarction in rats. Interact Cardiovasc Thorac Surg 2009;9:20–25; discussion 25.
18. McMurray JJ, Anand IS, Diaz R, Maggioni AP, O’Connor C, Pfeffer MA, Polu KR,Solomon SD, Sun Y, Swedberg K, Tendera M, van Veldhuisen DJ,Wasserman SM, Young JB. Design of the Reduction of Events with Darbepoetinalfa in Heart Failure (RED-HF): a Phase III, anaemia correction, morbidity-mortality trial. Eur J Heart Fail 2009;11:795–801.
19. Lindenfeld J. Prevalence of anemia and effects on mortality in patients with heartfailure. Am Heart J 2005;149:391–401.
20. Timmer SAJ, De Boer K, Knaapen P, Gtte MJW, Van Rossum AC. The potentialrole of erythropoietin in chronic heart failure: from the correction of anemia toimproved perfusion and reduced apoptosis? J Card Fail 2009;15:353–361.
21. Prunier F, Pottier P, Clairand R, Mercier A, Hajjar RJ, Planchon B, Furber A.Chronic erythropoietin treatment decreases post-infarct myocardial damage inrats without venous thrombogenic effect. Cardiology 2009;112:129–134.
22. Urbich C, Dimmeler S. Endothelial progenitor cells: characterization and role invascular biology. Circ Res 2004;95:343–353.
23. Lipsic E, van der Meer P, Voors AA, Westenbrink BD, van den Heuvel AFM, deBoer HC, van Zonneveld AJ, Schoemaker RG, van Gilst WH, Zijlstra F, vanVeldhuisen DJ. A single bolus of a long-acting erythropoietin analogue darbepoe-tin alfa in patients with acute myocardial infarction: a randomized feasibility andsafety study. Cardiovasc Drugs Ther 2006;20:135–141.
24. Hamed S, Barshack I, Luboshits G, Wexler D, Deutsch V, Keren G, George J. Ery-thropoietin improves myocardial performance in doxorubicin-induced cardio-myopathy. Eur Heart J 2006;27:1876–1883.
25. Muller P, Kazakov A, Semenov A, Bohm M, Laufs U. Pressure-induced cardiacoverload induces upregulation of endothelial and myocardial progenitor cells. Car-diovasc Res 2008;77:151–159.
26. Shiojima I, Sato K, Izumiya Y, Schiekofer S, Ito M, Liao R, Colucci WS, Walsh K.Disruption of coordinated cardiac hypertrophy and angiogenesis contributes tothe transition to heart failure. J Clin Invest 2005;115:2108–2118.
27. Pitchford SC, Furze RC, Jones CP, Wengner AM, Rankin SM. Differential mobil-ization of subsets of progenitor cells from the bone marrow. Cell Stem Cell2009;4:62–72.
28. Zohlnhofer D, Ott I, Mehilli J, Schomig K, Michalk F, Ibrahim T, Meisetschlager G,von Wedel J, Bollwein H, Seyfarth M, Dirschinger J, Schmitt C, Schwaiger M,Kastrati A, Schomig A. Stem cell mobilization by granulocyte colony-stimulatingfactor in patients with acute myocardial infarction: a randomized controlledtrial. JAMA 2006;295:1003–1010.
M.W. Bergmann et al.568