Professor Autor-Inglês-Inglês Ι 9º Ano Ι Fundamental-Simple Past x Past Progressive

Journal of the Neurological Sciences 339 (2014) 210–213
Contents lists available at ScienceDirect
Journal of the Neurological Sciences
j ourna l homepage: www.e lsev ie r .com/ locate / jns
Short communication
A novel SCARB2mutation in progressivemyoclonus epilepsy indicated byreduced β-glucocerebrosidase activity
Marsha Zeigler a, Vardiella Meiner a, J.P. Newman b, Bettina Steiner-Birmanns c, Ruth Bargal a, Vivi Sury a,Getu Mengistu a, Or Kakhlon b, Ina Leykin b, Zohar Argov b, Oded Abramsky b, Alexander Lossos b,⁎a Department of Human Genetics, Hebrew University-Hadassah Medical Center, Jerusalem, Israelb Department of Neurology, The Agnes Ginges Center for Human Neurogenetics, Hebrew University-Hadassah Medical Center, Jerusalem, Israelc Department of Neurology, Shaare Zedek Medical Center, Jerusalem, Israel
⁎ Corresponding author at: Department of NeurologyMedical Center, Jerusalem 91120, Israel. Tel.: +972 2 677
E-mail address: [email protected] (A. Lossos).
0022-510X/$ – see front matter © 2014 Elsevier B.V. All rhttp://dx.doi.org/10.1016/j.jns.2014.01.022
a b s t r a c t
a r t i c l e i n f oArticle history:Received 2 May 2013Received in revised form 23 December 2013Accepted 14 January 2014Available online 23 January 2014
Keywords:Progressive myoclonus epilepsyLIMP2SCARB2Action myoclonus renal failure syndromeAtaxiaGaucher disease
Action myoclonus renal failure (AMRF) syndrome is a rare form of progressive myoclonus epilepsy with renaldysfunction related to mutations in the SCARB2 gene. This gene is involved in lysosomal mannose-6-phosphate-independent trafficking of β-glucocerebrosidase (GC), an enzyme deficient in Gaucher disease. Wereport a family with myoclonic epilepsy, ataxia and skeletal muscle atrophy but without cognitive impairmentor overt renal disease. A novel SCARB2 mutation was indicated by a striking discrepancy between lymphocyteand fibroblast GC activity in the proband evaluated for possible Gaucher disease. Our findings expand the geneticand phenotypic diversity of AMRF and suggest that lowGC activitymay present an important biochemical clue tothe diagnosis of AMRF.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Actionmyoclonus renal failure (AMRF) syndrome (MIM2549000) is arare autosomal recessive form of progressive myoclonus epilepsy (PME)associated with renal dysfunction [1]. Main neurological manifestationsinclude a variable combination of tremor, action myoclonus, ataxia andepilepsy but, in contrast to the other forms of PME, without cognitive im-pairment. Less typical features are peripheral neuropathy andhearing loss[2,3]. The disease presents between the ages of 15–25 yearswith protein-uria or with neurological symptoms and follows thereafter a relentlesslyprogressive course over a decade with the development of renal failureand disabling neurological deterioration.
Recently, loss-of-function mutations in the SCARB2 gene have beenidentified in AMRF families [4]. This gene encodes a lysosomal integralmembrane protein LIMP2 important for lysosomal/endosomal systembiogenesis and for lysosomal mannose-6-phosphate-independent traf-ficking of β-glucocerebrosidase (GC), an enzyme deficient in Gaucherdisease [5]. Since this discovery, more than 16 disease-causing non-sense, splice-site and missense mutations have been described inAMRF [2–4,6,7], and the reported clinical phenotype has been expanded
, Hebrew University-Hadassah6941; fax: +972 2 6437782.
ights reserved.
to include occasional patients with PME who show no signs of overtrenal disease [2,6].
We report a novel SCARB2mutation in a family with PME evaluatedfor possible Gaucher disease and describe additional phenotypic vari-ability in AMRF.
2. Subjects and methods
2.1. Case report
The proband (Fig. 1A) was a 17-year-old man of Arab origin firstevaluated for progressive unsteadiness of gait and repeated episodesof falling for one year duration. He was well until then, with normalmotor and higher-than-average school achievements. Initial hand trem-or was rapidly followed by involuntary jerky movements of fingers andhands on performing finemotor tasks, twitches in the facewhen speak-ing, and shaking of the legs on standing and walking. He lost the abilityto walk unaided and began using a wheelchair within a short time. Twoepisodes of generalized tonic–clonic seizures occurred a few monthslater but were thereafter controlled with a variable combination ofvalproic acid, clonazepam, lamotrigine and levetiracetam.
On examination, there was prominent action and intention-inducedmyoclonus involving fingers, hands, proximal arms and legs. Themyoc-lonus was reflex-sensitive to touch, particularly in the legs, and aggra-vated by excitement or stress without startle response. Dysarthria

I
II
1 2
4321 5 6
A
B ControlProband
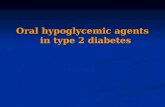
Fig. 1. (A) Pedigree of the family. Circles represent women and squares representmen. Filled symbols represent affected individuals, strikethroughs represent deceased, and arrow pointsto the proband. Double lines indicate consanguinity by descent. Subject II-1 was medically documented to be similarly affected from age 17, with normal renal functions at age 20.(B) SCARB2 sequencing in the proband showing c.1270CNT mutation (arrow) in exon 11 predicted to change arginine to a premature stop codon p.R424X.
211M. Zeigler et al. / Journal of the Neurological Sciences 339 (2014) 210–213
with perioral twitches appeared on speech attempts but there wasno palatal myoclonus. In spite of frequent myoclonic intrusions,mild limb and marked gait ataxia was observed. Although he ap-peared relaxed when in bed and reported quiet sleep, lying down andturning caused severe trunk contractions. Mild generalized skeletal mus-cle atrophywithout fasciculationswas noted early in the course of his dis-ease and remained unchanged thereafter. Muscle tone was slightlyreduced, deep tendon reflexes were normal and plantar response wasdowngoing. The formal ocular and neurocognitive evaluation revealedno abnormality.
The results of routine laboratory studieswere unremarkablewith nor-mal serumcreatinine andurinalysis. Tests for possible causes of PMEwerenegative and ruled out the appropriate forms of Unverricht–Lundborgdisease, myoclonic epilepsy with ragged red fibers (MERRF), Lafora's dis-ease, dentatorubral-pallidoluysian atrophy, celiac disease and subacutesclerosing panencephalitis. Screening for lysosomal storage disordersruled out sialidoses, neuronal ceroid lipofuscinosis, GM2 gangliosidosisand Niemann–Pick type A or C. In addition, bonemarrow, skeletal muscleand repeat skin biopsies were unremarkable and abdominal ultrasonog-raphy demonstrated no organomegaly or urogenital abnormality. Renalfunction testing at the age of 29 years, shortly after the diagnosis, showeda 24-hour urine protein excretion of 127 mg (normal range b150) andcreatinine clearance of 61 ml/min, consistentwith the chronic kidney dis-ease class II.
Although electroencephalogram during the early stages of his dis-ease showed no epileptiform activity, later studies demonstrated briefinterictal generalized runs of polyspike and wave complexes with neg-ative intermittent photic stimulation. Brainstem auditory evoked re-sponse (BAER) latencies and peripheral nerve conduction velocity(NCV) were normal with good compound motor action potentials, F-wave latencies and sensory conductions. Concentric needle electromy-ography (EMG) of the proximal and distal muscles showed widespreadloss of motor units without spontaneous activity. The remaining unitswere mostly of large-amplitude. Magnetic resonance imaging (MRI) ofthe brain showed only mild generalized atrophy.
Over 13 years of follow-up, he gradually continued to deteriorateneurologically but retained stable renal functions. Progressive bulbarmyoclonus caused difficulties swallowing and managing secretions,which eventually led to aspiration pneumonia and death.
Of the familymembers (Fig. 1A), only subject II-1 was reported to besimilarly affected from age 17withmultifocal myoclonus, ataxia and in-frequent generalized tonic–clonic seizures. Her cognitive status, renalfunctions BAER and NCV were documented as normal at age 20. Shedied of progressive disease 10 years after initial symptoms.
2.2. Methods
All studies were performed after formal genetic counseling, withinformed consent of the participants and after institutional reviewboard approval. Lymphocytes were extracted from peripheral bloodand cultured skin fibroblasts were propagated from skin biopsies bystandard methods [8]. Evaluation of GC activity was performed using4-methylumbelliferyl-β-glucopyranoside (Sigma-Aldrich) as previouslydescribed [9]. RNA was extracted from cultured skin fibroblasts usingthe high pure RNA isolation kit from Roche (Mannheim, Germany) ac-cording to manufacturer's instructions. First strand cDNA of the OpenReading Frame (ORF) of the GBA, PSAP and SCARB2 genes was synthe-sized with Superscript II (Invitrogen). PCR products were purified andsequenced with the BigDye terminator system on an ABI prism 3700 se-quencer (Applied Biosystems, Foster City, CA, USA).
To confirm the sequence data and examine familial segregation, thePCR products were analyzed by digestion with the restriction enzymeHinfI. The primers used were forward SCARB2int10F “CACACTGGATGTTTAGTCATC” and reverse EX11R “CCAAACCAAAGAACACACCC”.
To evaluate the fate of the SCARB2 mRNA, total RNA was obtainedfrom the culturedfibroblasts using the PureLink kit (Invitrogen, Carlsbad,CA, USA) and reverse-transcribed using theHigh-Capacity cDNAReverseTranscription kit (Applied Biosystems, Foster City, CA, USA). The SCARB2mRNA content, normalized to an endogenous HPRT control, was deter-mined by real-time RT-PCR using pre-designed SYBR Green GeneExpression system (Quanta Biosciences, Gaithersburg, MD, USA) andthe StepOnePlus thermocycler and analyzer (Applied Biosystems).
3. Results
Enzymatic GC activity was initially measured as part of screeningfor non-infantile neuropathic form of Gaucher disease rarely de-scribed with PME-like phenotype [10]. Proband's lymphocyte GC

0
0.2
0.4
0.6
0.8
1
1.2
SC
AR
B2
mR
NA
(rel
ativ
e un
its)
ProbandControl
*
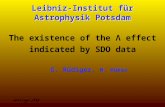
Fig. 3. Relative SCARB2 mRNA levels derived from control skin fibroblasts and from theproband. The results are means (±SD) of 3 experiments. T-test analysis demonstratedthat mRNA levels in the proband were significantly (p b 0.01) lower than the control's.
212 M. Zeigler et al. / Journal of the Neurological Sciences 339 (2014) 210–213
activity was 7 nmol/mg protein/h (control 15), suggesting that hemay be a carrier for Gaucher disease. In fibroblasts, a severe deficiencyof 6 nmol/mg protein/h (control 551) was found. Direct sequencingruled out mutations in the GBA or the GBA activator (PSAP) genes.Sequencing of the SCARB2 identified a novel homozygous nonsensemu-tation in exon 11 c.1270CNT (Fig. 1B) changing arginine to a prematurestop codon p.R424X. The segregation of thismutationwas confirmed byrestriction analysis (Fig. 2) showing the patient to be homozygous forthe mutation and his parents as carriers. Gene expression assays usingreal-time RT-PCR indicated N80% reduction in the SCARB2 expressionin the patient as compared to control (Fig. 3).
4. Discussion
After ruling out mutations in the GBA and PSAP, the striking discrep-ancy between lymphocyte and fibroblast GC activity in the proband in-dicated the possibility of a SCARB2-related disease [4,11–14]. Previously,SCARB2mutationswere identifiedmostly on the basis of clinical presen-tation, and this is the third report of a patient diagnosed as a result ofinitial testing for Gaucher disease [12,13,15]. Recently a patient withGaucher disease manifesting PME was found to have a heterozygouslyexpressed SCARB2 mutation. He presented with a more severe form ofGaucher disease then his affected brother [15], illustrating the influenceof this gene on GC activity.
LIMP2 is an abundant lysosomal membrane protein of 478 aminoacids with two cytosolic and transmembrane domains each and withone main luminal domain where GC-binding site is between residues145–288 [5,11]. The LIMP2-GC complex leaves endoplasmic reticulumand is targeted to the late endosomes and lysosomes [5]. The c.1270CNTmutation identified in this family leads to a premature stop codon atposition 424 and results in a significantly reduced SCARB2 expression,to explain low GC activity. These data support the hypothesis that themRNA is subjected to nonsense-mediated RNA decay. Additional tissue-specific factors possibly account for the observed discrepancy betweenlymphocytes and fibroblasts [11].
This family presented the typical neurological AMRF phenotype butwith a few notable features. Our patient and his sister did not manifestovert renal failure, and his serum creatinine and urinalysis remainednormal throughout the course of the disease. Still, because formal creat-inine clearance was tested once and was slightly reduced, it might havedeteriorated later. Similar observation originally reported in 6 patientssuggests distinct pathogenesis of the neurological and renal involve-ment [2,6]. Also, patients in this family did notmanifest peripheral neu-ropathy and hearing loss. Both features characterize SCARB2 knockoutmice [16] but have only recently been reported to expand the AMRFphenotype [2,3,7]. Because no obvious genotype–phenotype correlationhas so far emerged in this disease [2,6], additional genetic and environ-mental factors may be responsible for the observed clinical variability.
1353bp1078872603
310
234194
281/271
118
72
Fig. 2.Restriction analysiswithHinfI. Lanes: 1, unrestricted control; 2, the proband'smoth-er; 3, the proband's father; 4, the proband's DNA from blood, and 5, from fibroblasts; 6,normal control; and 7, HaeIII digest of φχ 174 DNA ladder. The mutant allele abolishes aHinfI site. The normal allele yields two fragments of 75 and 88 bp. The patient was con-firmed to be homozygous for the mutation and the parents were carriers.
Because GC-related LIMP2 activity alone is insufficient to produceAMRF, other functions of LIMP2 may play a role in its pathogenesis[4,11]. It is a recognized cellular receptor for enterovirus 71 (EV71),involved in a range of acute neurological disorders, clinically and path-ologically distinct from AMRF [17]. Yet, brainstem encephalitis withprominent myoclonus and anterior myelitis with acute flaccid paralysisare among the typical manifestations of EV71 infection [18]. Of note inthis respect is generalized muscle atrophy in the proband accompaniedby EMG pattern compatible with chronic or past anterior horn involve-ment, seemingly implying functional significance of SCARB2 in this neu-ral compartment.
In conclusion, our findings expand the genetic and phenotypic diver-sity of AMRF and confirm its worldwide geographic distribution. The ob-served clinical features in this family further imply the importance oftesting for SCARB2mutations in patientswith PMEwithout cognitive im-pairment even in the absence of overt renal dysfunction. LowGC activitymay present an important biochemical clue to the diagnosis of AMRF.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] Badhwar AP, Berkovic SF, Dowling JP, Gonzales M, Narayanan S, Brodtmann A, et al.Action myoclonus–renal failure syndrome: characterization of a unique cerebro-renal disorder. Brain 2004;127:2172–82.
[2] Dibbens LM, Karakis I, Bayly MA, Costello DJ, Cole AJ, Berkovic SF. Mutation ofSCARB2 in a patient with progressive myoclonus epilepsy and demyelinatingperipheral neuropathy. Arch Neurol 2011;68:812–3.
[3] Perandones C, Micheli FE, Pellene LA, Bayly MA, Berkovic SF, Dibbens LM. A case ofsevere hearing loss in action myoclonus renal failure syndrome resulting frommutation in SCARB2. Mov Disord 2012;27:1195–7.
[4] Berkovic SF, Dibbens LM, Oshlack A, Silver JD, KaterelosM, Vears DF, et al. Array-basedgene discoverywith three unrelated subjects shows SCARB2/LIMP-2 deficiency causesmyoclonus epilepsy and glomerulosclerosis. Am J Hum Genet 2008;82:673–84.
[5] Reczek D, SchwakeM, Schroder J, Hughes H, Blanz J, Jin X, et al. LIPM-2 is a receptor forlysosomalmannose-6-phosphate-independent targeting ofβ-glucocerebrosidase. Cell2007;131:770–83.
[6] Dibbens LM, Michelucci R, Gambardella A, Andermann F, Rubboli G, Bayly MA, et al.SCARB2 mutations in progressive myoclonus epilepsy (PME) without renal failure.Ann Neurol 2009;66:532–6.
[7] Hopfner F, Schormair B, Knauf F, Berthele A, Tolle TR, Baron R, et al. Novel SCARB2mutation in action myoclonus–renal failure syndrome and evaluation of SCARB2mutations in isolated AMRF features. BMC Neurol 2011;11:134.
[8] Wenger D, Williams C. Screening for lysosomal disorders. In: Homme FA, editor.Techniques in diagnostic human genetics. A laboratory manual. Wiley-Liss, Inc.;1991. p. 587–617.
[9] Raghavan SS, Topol J, Kolodny EH. Leukocyte beta-glucosidase in homozygotes andheterozygotes for Gaucher disease. Am J Hum Genet 1980;32:158–73.
[10] Park JK, Orvitsky E, TayebiN, Kaneski C, LamarcaME, Stubblefield BK, et al. Myoclonicepilepsy in Gaucher disease: genotype–phenotype insights from a rare patient sub-group. Pediatr Res 2003;53:387–94.
[11] Blanz J, Groth J, Zachos C,Wehling C, Saftig P, SchwakeM. Disease-causingmutationswithin the lysosomal integral membrane protein type 2 (LIMP-2) reveal the natureof binding to its ligand β-glucocerebrosidase. Hum Mol Genet 2010;19:563–72.
[12] Balreira A, Gaspar P, Caiola D, Chaves J, Beirao I, Lima JL, et al. A nonsensemutation inthe LIMP-2 gene associated with progressive myoclonic epilepsy and nephritic syn-drome. Hum Mol Genet 2008;17:2238–43.

213M. Zeigler et al. / Journal of the Neurological Sciences 339 (2014) 210–213
[13] Dardis A, FilocamoM, Grossi S, Ciana G, Francescheti S, Dominissini S, et al. Biochem-ical and molecular findings in a patient with myoclonic epilepsy due to a mistargetof the β-glucosidase enzyme. Mol Genet Metab 2009;97:309–11.
[14] Chaves J, Beirao I, Balreira A, Gaspar P, Caiola D, Sa-Miranda M, et al. Progressivemyoclonic epilepsywith nephropathyC1q due to SCARB2/LIMP-2deficiency: clinicalreport of two siblings. Seizure 2011;20:738–40.
[15] Velayati A, DePaolo J, Gupta N, Choi JH, Moaven N,WestbroekW, et al. A mutation inSCARB2 is a modifier in Gaucher disease. Hum Mutat 2011;32:1232–8.
[16] Gamp AC, Tanaka Y, Lullmann-Rauch R, Wittke D, D'Hooge R, De Deyn PP, et al.LIMP-2/LGP85 deficiency causes ureteric pelvic junction obstruction, deafness andperipheral neuropathy in mice. Hum Mol Genet 2003;12:631–46.
[17] Chen P, Song Z, Qi Y, Feng X, Xu N, Sun Y, et al. Molecular determinants of enterovi-rus 71 viral entry. Cleft around GLN-172 on VP1 protein interacts with variableregion on scavenger receptor B 2. J Biol Chem 2012;287:6406–20.
[18] Ooi MH,Wong SC, Lewthwaite P, Cardosa MJ, Solomon T. Clinical features, diagnosis,and management of enterovirus 71. Lancet Neurol 2010;9:1097–105.