
1 Central (intraosseous) mucoepidermoid carcinoma of 1 the ... · intermediate grade mucoepidermoid...
5
91 Σκοπός: Το βλεννοεπιδερμοειδές καρκίνωμα αποτελεί το 5-10% όλων των όγκων των σιελογόνων αδένων, και το 2- 4,3% όλων βλεννοεπιδερμοειδών καρκινωμάτων εντοπί- ζεται ενδοοστικά (κεντρικά) στις γνάθους. Από την ανασκόπηση της Αγγλόφωνης βιβλιογραφίας προκύπτει ότι μέχρι σήμερα έχουν αναφερθεί 135 περιπτώσεις κεν- τρικού βλεννοεπιδερμοειδούς καρκινώματος. Η προ- έλευση του όγκου είναι αμφιλεγόμενη. Η ριζική χειρουργική εκτομή συνδέεται με καλύτερο θεραπευτικό αποτέλεσμα, σε σχέση με συντηρητικές τεχνικές. Ωστόσο στις περισσότερες από τις περιπτώσεις που έχουν περι- γραφεί μέχρι σήμερα τα στοιχεία για τη μετεγχειρητική παρακολούθηση, τη βιολογική συμπεριφορά και την πρό- γνωση της νόσου είναι ελλιπή. Περιγραφή περίπτωσης: Στη παρούσα εργασία περιγρά- φεται περίπτωση κεντρικού βλεννοεπιδερμοειδούς καρ- κινώματος στην περιοχή της γωνίας της κάτω γνάθου δεξιά, σε άνδρα ηλικίας 62 ετών. Η πανοραμική ακτινο- γραφία έδειξε πολύχωρη διαύγαση και η ιστολογική εξέ- ταση βλεννοεπιδερμοειδές καρκίνωμα μέσης κακοήθειας. Έγινε τμηματική εκτομή του προσβεβλη- μένου οστού της κάτω γνάθου σε συνδυασμό με υπερω- μοειδικό λεμφαδενικό καθαρισμό. Ένα χρόνο μετά την αρχική επέμβαση ο ασθενής είναι ελεύθερος υποτροπής ή μεταστατική νόσου. Συμπέρασμα: Τα κεντρικά βλεννοεπιδερμοειδή καρκι- νώματα αποτελούν σπάνιους όγκους των σιαλογόνων αδένων, συνήθως είναι χαμηλής κακοήθειας βλάβες και η θεραπεία τους συνιστάται σε ευρεία εκτομή. Η μακρό- χρονη μετεγχειρητική παρακολούθηση είναι επιβεβλη- μένη δεδομένου ότι έχουν καταγραφεί περιπτώσεις τοπικών υποτροπών ή περιοχικών μεταστάσεων ακόμα και μετά από δεκαετίες. Λέξεις κλειδιά: Βλεννοεπιδερμοειδές καρκίνωμα, κεν- τρικό, ενδοοστικό, κάτω γνάθος Background: Mucoepidermoid carcinoma of the sali- vary glands is a well-defined entity, representing 5% to 8% of all salivary gland tumours. However the cen- tral (intraosseous) mucoepidermoid carcinoma of the jaws is extremely rare, comprising 2 to 4,3% of all mucoepidermoid carcinomas. A review of the Eng- lish literature revealed 135 reported cases. The ori- gin of the central mucoepidermoid carcinoma is controversial. The primary treatment modality is radical surgical resection that offers a better prog- nosis than do more conservative procedure. However, in most reported cases limited follow-up makes dif- ficult accurate prognostic comparisons and estab- lishment of the biological behavior of the tumor. Case report: We describe a case of central mucoepi- dermoid carcinoma in the right angle of the mandible in 62 year old male. A panoramic radiograph re- vealed a multilocular radiolucent lesion and a biopsy showed a medium grade of malignancy mucoepider- moid carcinoma. Conclusion: The central mucoepidermoid carcinomas are uncommon salivary gland tumours that are often low-grade lesions treated by wide local excision. Long- term follow-up is necessary, as some cases can develop late local recurrences and regional metastasis, even after decades. Key Words: Mucoepidermoid carcinoma, central, in- traosseous, mandible Περίληψη Abstract DD. Andressakis 1 A. Antoniadou 1 KI. Tosios 2 E. Ntokos 1 M. Archondaki 3 D. Balatsouras 4 A. Zissi Sermpetzoglou 5 1. Dental Department of “Tzaneio” General Hospital of Piraeus, Piraeus 2. Department of Oral Pathology, Dental School, University of Athens, Athens, Greece 3. Department of Head and Neck / Maxillofacial Surgery, Greek Anticancer Institute, St Savvas Hospital 4. ΕΝΤ Department of “Tzaneio” General Hospital of Piraeus, Piraeus 5. Histopathologic Department of “Tzaneio” General Hospital of Piraeus, Piraeus Hellenic Otorhinolaryngology - Head an Neck Surgery Volume 31 - Issue 2 ΔΔ. Ανδρεσάκης 1 Α. Αντωνιάδου 1 ΚΙ. Τόσιος 2 Ε. Ντόκος 1 Μ. Αρχοντάκη 3 Δ. Μπαλατσούρας 4 Α. Ζήσση Σερμπέτζογλου 5 1. Οδοντιατρικό Τμήμα Γ.Ν.Π. “Τζάνειο”, Πειραιάς 2. Εργαστήριο Στοματολογίας, Τομέας Παθολογίας και Χειρουργικής Στόματος, Οδοντιατρική Σχολή Πανεπιστημίου Αθηνών 3. Τμήμα Γναθοποροσωπικής Χειρουργικής ΑΟΝΑ “Ο Άγιος Σάββας” 4. Τμήμα ΩΡΛ, Γ.Ν.Π. “Τζάνειο”, Πειραιάς 5. Τμήμα Παθολογικής Ανατομικής, Γ.Ν.Π. “Τζάνειο”, Πειραιάς Ελληνική Ωτορινολαρυγγολογία Χειρουργική Κεφαλής & Τραχήλου Τόμος 31 - Τεύχος 2 Correspondence: D.D. Andressakis, Dental Department of “Tzaneio” General Hospital of Piraeus, Zanni & Afentouli 18536, e-mail: [email protected] Central (intraosseous) mucoepidermoid carcinoma of the mandible. Report of a case and review of literature Κεντρικό (ενδοοστικό) βλεννοεπιδερμοειδές καρκίνωμα της κάτω γνάθου. Αναφορά περίπτωσης και ανασκόπηση της βιβλιογραφίας. 00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:34 ΠΜ Page 91
Transcript of 1 Central (intraosseous) mucoepidermoid carcinoma of 1 the ... · intermediate grade mucoepidermoid...

91
Σκοπός: Το βλεννοεπιδερμοειδές καρκίνωμα αποτελεί το
5-10% όλων των όγκων των σιελογόνων αδένων, και το 2-
4,3% όλων βλεννοεπιδερμοειδών καρκινωμάτων εντοπί-
ζεται ενδοοστικά (κεντρικά) στις γνάθους. Από την
ανασκόπηση της Αγγλόφωνης βιβλιογραφίας προκύπτει
ότι μέχρι σήμερα έχουν αναφερθεί 135 περιπτώσεις κεν-
τρικού βλεννοεπιδερμοειδούς καρκινώματος. Η προ-
έλευση του όγκου είναι αμφιλεγόμενη. Η ριζική
χειρουργική εκτομή συνδέεται με καλύτερο θεραπευτικό
αποτέλεσμα, σε σχέση με συντηρητικές τεχνικές. Ωστόσο
στις περισσότερες από τις περιπτώσεις που έχουν περι-
γραφεί μέχρι σήμερα τα στοιχεία για τη μετεγχειρητική
παρακολούθηση, τη βιολογική συμπεριφορά και την πρό-
γνωση της νόσου είναι ελλιπή.
Περιγραφή περίπτωσης: Στη παρούσα εργασία περιγρά-
φεται περίπτωση κεντρικού βλεννοεπιδερμοειδούς καρ-
κινώματος στην περιοχή της γωνίας της κάτω γνάθου
δεξιά, σε άνδρα ηλικίας 62 ετών. Η πανοραμική ακτινο-
γραφία έδειξε πολύχωρη διαύγαση και η ιστολογική εξέ-
ταση βλεννοεπιδερμοειδές καρκίνωμα μέσης
κακοήθειας. Έγινε τμηματική εκτομή του προσβεβλη-
μένου οστού της κάτω γνάθου σε συνδυασμό με υπερω-
μοειδικό λεμφαδενικό καθαρισμό. Ένα χρόνο μετά την
αρχική επέμβαση ο ασθενής είναι ελεύθερος υποτροπής
ή μεταστατική νόσου.
Συμπέρασμα: Τα κεντρικά βλεννοεπιδερμοειδή καρκι-
νώματα αποτελούν σπάνιους όγκους των σιαλογόνων
αδένων, συνήθως είναι χαμηλής κακοήθειας βλάβες και
η θεραπεία τους συνιστάται σε ευρεία εκτομή. Η μακρό-
χρονη μετεγχειρητική παρακολούθηση είναι επιβεβλη-
μένη δεδομένου ότι έχουν καταγραφεί περιπτώσεις
τοπικών υποτροπών ή περιοχικών μεταστάσεων ακόμα
και μετά από δεκαετίες.
Λέξεις κλειδιά: Βλεννοεπιδερμοειδές καρκίνωμα, κεν-
τρικό, ενδοοστικό, κάτω γνάθος
Background: Mucoepidermoid carcinoma of the sali-
vary glands is a well-defined entity, representing 5%
to 8% of all salivary gland tumours. However the cen-
tral (intraosseous) mucoepidermoid carcinoma of
the jaws is extremely rare, comprising 2 to 4,3% of
all mucoepidermoid carcinomas. A review of the Eng-
lish literature revealed 135 reported cases. The ori-
gin of the central mucoepidermoid carcinoma is
controversial. The primary treatment modality is
radical surgical resection that offers a better prog-
nosis than do more conservative procedure. However,
in most reported cases limited follow-up makes dif-
ficult accurate prognostic comparisons and estab-
lishment of the biological behavior of the tumor.
Case report: We describe a case of central mucoepi-
dermoid carcinoma in the right angle of the mandible
in 62 year old male. A panoramic radiograph re-
vealed a multilocular radiolucent lesion and a biopsy
showed a medium grade of malignancy mucoepider-
moid carcinoma.
Conclusion: The central mucoepidermoid carcinomas
are uncommon salivary gland tumours that are often
low-grade lesions treated by wide local excision. Long-
term follow-up is necessary, as some cases can develop
late local recurrences and regional metastasis, even
after decades.
Key Words: Mucoepidermoid carcinoma, central, in-
traosseous, mandible
Περίληψη Abstract
DD. Andressakis1
A. Antoniadou1
KI. Tosios2
E. Ntokos1
M. Archondaki3
D. Balatsouras4
A. Zissi Sermpetzoglou5
1. Dental Department of “Tzaneio”
General Hospital of Piraeus, Piraeus
2. Department of Oral Pathology,
Dental School, University of Athens,
Athens, Greece
3. Department of Head and Neck /
Maxillofacial Surgery, Greek
Anticancer Institute, St Savvas
Hospital
4. ΕΝΤ Department of “Tzaneio”
General Hospital of Piraeus, Piraeus
5. Histopathologic Department of
“Tzaneio” General Hospital of
Piraeus, Piraeus
Hellenic Otorhinolaryngology -
Head an Neck Surgery
Volume 31 - Issue 2
ΔΔ. Ανδρεσάκης1
Α. Αντωνιάδου1
ΚΙ. Τόσιος2
Ε. Ντόκος1
Μ. Αρχοντάκη3
Δ. Μπαλατσούρας4
Α. Ζήσση Σερμπέτζογλου5
1. Οδοντιατρικό Τμήμα Γ.Ν.Π.
“Τζάνειο”, Πειραιάς
2. Εργαστήριο Στοματολογίας,
Τομέας Παθολογίας και
Χειρουργικής Στόματος,
Οδοντιατρική Σχολή
Πανεπιστημίου Αθηνών
3. Τμήμα Γναθοποροσωπικής
Χειρουργικής ΑΟΝΑ
“Ο Άγιος Σάββας”
4. Τμήμα ΩΡΛ, Γ.Ν.Π. “Τζάνειο”,
Πειραιάς
5. Τμήμα Παθολογικής Ανατομικής,
Γ.Ν.Π. “Τζάνειο”, Πειραιάς
Ελληνική Ωτορινολαρυγγολογία
Χειρουργική Κεφαλής & Τραχήλου
Τόμος 31 - Τεύχος 2
Correspondence: D.D. Andressakis,
Dental Department of “Tzaneio”
General Hospital of Piraeus, Zanni
& Afentouli 18536, e-mail:
Central (intraosseous) mucoepidermoid carcinoma of the mandible. Report of a case and review of literatureΚεντρικό (ενδοοστικό) βλεννοεπιδερμοειδές καρκίνωμα τηςκάτω γνάθου. Αναφορά περίπτωσης και ανασκόπηση τηςβιβλιογραφίας.
00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:34 ΠΜ Page 91

The purpose of this study is to describe a case of CMECof the mandible, discussing the clinical and radiographiccharacteristics, the pathogenesis, the histological featuresand differential diagnosis of the lesion, and the concernsthat exist in the literature regarding the prognostic factorsand the criteria for selection of therapeutic method.
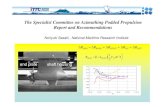
Case reportA 62-year-old man was referred to the Dental depar-tment of “Tzanio” General Hospital with an asympto-matic radiolucent multilocular lesion with distinctborders in the right angle of the mandible and ramus(Fig.1). The lesion has been discovered on a routinepanoramic radiograph. There was no history of pain orlip paraeshesia.
92
IntroductionMucoepidermoid carcinoma of the salivary glands is awell-defined entity, representing 5% to 8% of all sali-vary gland tumours.1,2,3 About 70% of these tumours arefound in the parotid gland, 15% to 20% in the oral ca-vity, affecting the minor salivary glands, and 6% to 10%in the submandibular gland.4,5 However the central (in-traosseous) mucoepidermoid carcinoma (CMEC) ofthe jaws is extremely rare, comprising 2 to 4,3% of allmucoepidermoid carcinomas.2,5,6,7 A thorough review ofthe English-language literature until 2008, revealed 135reported cases of CMEC.8 However, in most cases thereported data relatively the behavioural pattern, the ef-fectiveness of current therapeutic approaches and pro-gnosis of these tumours are insufficient.9
Fig. 4. Histologic microphotograph of the specimen showing a compactblast with epidermoid and mucous cells in equal proportion. (HE, original
magnification X400).
Fig. 3. Histologic microphotograph of the specimen showing wall of blast witchconsist of epidermoid and mucous cells. (HE, original magnification X200).
Fig. 2. The aspiration of showed the presence of liquid yellow colourwithin the lesion.
Fig.1. Panoramic radiograph showing multilocular osteolytic lesion of the right mandible with distinct borders.
00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:34 ΠΜ Page 92

93
Clinically there was slight swelling of the posterior lin-gual surface of the right mandible. During palpationof the cortical bone was intact. The lesion was aspira-ted, and the examination showed the presence of liquidyellow colour (Fig. 2). With the probable diagnosis ofodontogenic keratocyst performed partial biopsy. The microscopic examination of 5 μm thick sectionsstained with hematoxylin and eosin showed vascular fi-brous connective tissue infiltrated by solid and cystictumour epithelial cell blasts (Fig. 3). Tumour cells exh-ibited characteristics of epidermoid cells with abundantcytoplasm and large amphiphilic or dark-stainingfoamy nucleus or mucous cells with slightly basophiliccytoplasm and eccentric nucleus (Fig. 4). The mucouscells reacted positively with PAS staining and mucocar-min. Also recognized smaller cells with a slightly eosi-nophilus cytoplasm, compatible with intermediate cells.The proportion epidermoid-mucous cells was approxi-mately 1:1. The connective tissue showed infiltrationof inflammatory cells with the dominant lymphocytesand areas with interstitial bleeding. The diagnosis was,intermediate grade mucoepidermoid carcinoma. The patient was referred to a specialist Department ofOral and Maxillofacial Surgery, where he underwentsegmental mandibular resection of the affected bonewith homolateral suprahomohyoid neck dissection.One year after the initial surgery the patient is free ofrecurrent or metastatic disease.
DiscussionCentral salivary gland tumours are uncommon andCMEC is the most frequent representing 64% to 75%of the cases according to various series. 6,8,10,11,12
The criteria as proposed by Alexander et al13 andsubsequently modified by Browand and Waldron14
for the diagnosis of a central salivary adenocarci-noma are the following: (1) the presence of an intactcortical bone plate, (2) radiographic evidence ofbone destruction, (3) histologic features of salivaryadenocarcinoma, (4) evidence of mucin production,(5) absence of other primary salivary gland or odon-togenic tumor. Many authors believe that the firstcriterion should not be an essential feature in asses-sing the intaosseous origin of CMEC, since extensivetumours can penetrate the surrounding bone and ex-tend to surrounding tissues. 7,11,15 Our case fulfilledthe acceptance criteria described above except thatthe first of the rupture of the cortical plate.The CMEC has been reported in all ages with over-whelming majority occurring in 5th and 6th decades
of life.7,9,11,12 In teenagers and children occurred sel-dom and until today, 11 cases have been repor-ted.12,14,16,17,18,19,20 The younger patient was one yearold21 and most aged 85 years old.12 The male-femaleratio was 1:1,45 in favour of female.2,9.12 About 60%to 85 % of tumours affect the mandible, especiallythe premolar-molar region, angle andramus.5,7,11,12.14,15 Maxillary origin sometimes may bequestionable, because such tumours may actuallyarise from the submucosal mucus secreting glands inthe antrum, or representing intraosseous extensionof minor salivary glands tumours of the sinus mu-cosa.11 According to Pires et al7 this distinction is im-portant because CMEC identified in the maxilla haveworse prognosis than those in the mandible, althoughhave better prognosis than mucoepidermoid carci-nomas which derived from the sinus mucosa.12
Clinically, in most cases the lesion appears as apainless swelling covered by normal mucosa, 7,17,19,22
and rarely accompanied by pain, 23,24,25 trismus, 7.8
or paraesthesia.22, 26,27 In many reports the tumor isdescribed as an asymptomatic lesion that discoveredincidentally during on routine radiographic con-trol.2,12 Radiographically, the CMECs usually occursas multilocular9,16,23,28 and rarely as unilocular ra-diolucency.2,11,17 The borders are usually well-defi-ned. 9,15,17 Johnson and Velez24 describe an unusualcase of CMEC witch caused resorption of teethroots. In our case the tumour was painless and ra-diographic appearance was a well- circumscribedmultilocular radiolucency.
The pathogenesis of central adenocarcinomas is still un-known and four possible origin have been described2,6,13,29
(a) entrapment of retromolar mucous glands within themandible, witch subsequently undergo neoplastic tran-sformation, (b) developmentally included embryonic re-mnants of the submandibular gland within the mandible,(c) neoplastic transformation of the mucous secretingcells commonly found in the pluripotential epithelial li-ning of dentigerous cysts associated with impacted thirdmolars; and (d) neoplastic transformation and invasionfrom the lining of the maxillary sinus. More recently, in-traosseous salivary tissue was demon¬strated in 0.3% ofbone specimens of all jawbones studied by Bouquot etal,6 providing new evidences for the origin of intraosse-ous salivary carci¬nomas. In other studies described therelationship of CMECof the mandible with odontogeniccysts or impacted teeth at rates 32% to 50%,12.29 whichsupports the theory of the origin from the investing epi-thelium of cysts.
00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:35 ΠΜ Page 93

94
As its name implies the CMEC composed mainly ofthee types of cells, the epidermoid, the mucous-secre-ting, and the intermediate cells. 4,15,30 Other cells thatrarely occurred are the clear cells and the sebaceouscells.1,2,4,11 The three main cell types forming sheets orislands, which may be solid or contain cystic spaces, 11.22
which contain mucous material.9,18 The grading of tu-mour depends primarily on the relative mix of celltypes, although growth pattern and cellular atypia alsoply significant roles.15,30,31 Low grade tumours20,23,25
show prominent cyst formation, minimal cellular aty-pia, and a relatively high proportion of mucous cells.High grade tumours11,26 consist of solid islands of squa-mous and intermediate cells, witch can demonstrateconsiderable pleomorphism and mitotic activity. Mu-cous-producing cells may be infrequent. Intermediategrade32 tumours show features that fall between thoseof low grade and high grade neoplasms. Cyst formationoccurs but is less prominent than that observed in lowgrade tumours. All three major cell types are present,but the intermediate cells usually predominate. Cellu-lar atypia may or may not be observed. Most CMECclassified as low grade tumours .4,9,10, 11.33
The radiographic differential diagnosis of CMEC ismade by lesions that have a similar picture as amelo-blastoma, odontogenic keratocyst, dentigerous cyst,
central giantcell tumour and periapical cyst.10,11.25 John-son and Velez24 present an unusual case witch occurreda well circum-scribed and corticated radiolucent lesionshowing large dense radiopacities. The authors consi-dered the lesion associated with desmoplastic amelo-blastoma, early ossifying fibroma, and calcifyingepithelial odontogenic tumour.These central bony lesions cannot be clinically stagedby criteria already established by the AJCC for majorsalivary gland carcinomas, so Brookstone and Huvos12
alternatively proposed a three-graded classificationbased on condition of the overlying bone (Table 1). Thisgrading system seems to be useful, adjunctive to clinicalstage, localization and histological grade of the tumours,in establishing proper management and prognosis ofCMEC.10 However, one of the difficulties in evaluatingthe usefulness of this system is tha absence of large com-parative series of CMEC in the literature.8,26 Based onthis grading system our case is classified as grade III. Throughout the literature, surgery has been the predo-minant treatment for the central salivary gland jaw le-sions. For the purpose of this discussion, surgicaltreatment has been categorized broadly as conservative(enucleation, curettage, marsupialization) or radical(marginal resection, segmental resection). Conserva-tive approach is undesirable and associated with incre-ased rates of local recurrence11,12,33,34 or even distantmetastasis.28 The radical surgery, seems to be more ac-ceptable to treat CMEC and associated with better th-erapeutic results.7,12,17,19 Neck dissection has beenperformed by some surgeons16, 26,32,34 although the Bro-okstone and Huvos12 Support not offer significant the-rapeutic effect. Additionally a literature review reportscervical metastatic disease in rate 9%. Other authorspropose the implementation of postoperative radioth-erapy after radical surgery.7, 9,11,23 The indications forenforcement neck dissection and complementary ra-diotherapy appears to be the presence of clinically pal-pable cervical lymph nodes, close surgical limits, thepresence of perineural or perivascular neoplastic inva-sion and high-grade tumours.10, 23,33,34
The data of literature relatively current treatment ap-proaches and their effectiveness are limited.9 Additio-nally there are few series with long postoperativefollow-up.14,34 For these reasons, reliable conclusionsabout the prognosis of the disease is not can be derived.7
The relapse rates according to various surveys rangedfrom 10% to 50%, which correlated with both thebiological behaviour of the tumour and surgical ap-proach.7,9,12 CMEC regional metastasis are reportedTable 1. Clinical staging of CMEC.
Disease stage
Stage Ι
Stage ΙΙ
Stage ΙΙΙ
Characteristics
Intact cortical bone and overlying
periosteum without of signs of corti-
cal expansion
Lesion surrounded by intact cortical
bone that has undergone some de-
gree of expansion
Cortical perforation, breakdown of
the overlying periosteum or metasta-
tic nodal spread
00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:35 ΠΜ Page 94

95
in 10-15% of the cases, and these tumours rarelyshow distant metastasis.12,28 Two such cases of meta-stasis have been reported, one was the clavicle28 andthe other the lungs.35 As to the timing of metastaseshave been reported instances of the following 17 to20 years from initial treatment, which makes longmonitoring of these patients necesary.7 Approxima-tely 10% of patients with CMEC can evolve to deathand, in general, these tomours usually show a goodoverall prognosis.11,14,34
In conclusion, CMECs are uncommon salivary glandtumours that usually affect the posterior mandibleas uni- or multilocular irregularly bordered lesions.They are commonly low-grade tumours and trea-tment includes essen¬tially wide local excision. Long-term follow-up is necessary, as some cases candevelop late local recurrences and regional metasta-sis, even after decades.
1. Αγγελόπουλος�ΑΠ,�Παπανικολάου�Στ.,�Αγγελοπούλου�Ε.�Σύγχρονη�Στοματική�και
Γναθοπροσωπική�Παθολογία.�Αθήνα:�Ιατρικές�Εκδόσεις�Λίτσας,�2000:506-8.
2. Gingell�JC,�Beckerman�T,�Levy�BA,�Snider�LA.�Central�mucoepidermoid�carcinoma.
Review�of�the�literature�and�report�of�a�case�associated�with�an�apical�periodontal
cyst.�Oral�Surg�Oral�Med�Oral�Pathol�1984;57:436-40.
3. Eversole�LR.�Mucoepidermoid�Carcinoma:�Review�of�815�reported�cases.�Oral�Surg
Oral�Med�Oral�Pathol�1970;28:490–5.
4. Marx�RE,�Stern�D.�Oral�and�Maxillofacial�Pathology.�A�Rationale�for�Diagnosis�and�Treat-
ment.�Chicago-Berlin-Tokyo-London-Paris:�Quintessence�Publishing�Co,�2002:543-50.
5. Ellis�GL,�Auclair�PL,�Gnepp�DR.�Surgical�Pathology�of�the�Salivary�Glands.�Philadel-
phia�:�W.B.�Saunders,�1991:291-5.
6. Bouquot�JE,�Gnepp�DR,�Dardick�I,�Hietanen�JHP.�Intraosseous�salivary�tis¬sue:�jawbone
examples�of�choristomas,�hamartomas,�embryonic�rests,�and�inflammatory�entrap-
ment:�another�his-togenetic�source�for�intraosseous�adeno-carcinoma.�Oral�Surg�Oral
Med�Oral�Pathol�Oral�Radiol�Endod�2000;�90:205¬-17.
7. Pires�FR,�Paes�de�Almeida�O,�Lopes�MA,�Elias�da�Cruz�Perez�D,�Kowalski�LP.�Central
mucoepidermoid�carcinoma�of�the�mandible:�report�of�four�cases�with�long-term�fol-
low-up.�Int�J�Oral�Maxillofac�Surg�2003;32:378-82.
8. Li�Y,�Li�LJ,�Huang�J,�Han�B,�Pan�J.�Central�malignant�salivary�gland�tumors�of�the�jaw:
retrospective�clinical�analysis�of�22�cases.�J�Oral�Maxillofac�Surg�2008;�66:2247-53.
9. Kochaji�N,�Goossens�A,�Bottenberg�P.�Central�Mucoepidermoid�carcinoma:�case�report,
literature�review�for�missing�and�available�information�and�guideline�proposal�for
coming�case�reports.�Oral�Oncology�Extra�2004;40:95-105.
10. Martínez-Madrigal�F,�Pineda-Daboin�K,�Casiraghi�O,�Luna�MA.�Salivary�gland�tumors
of�the�mandible.�Ann�Diagn�Pathol�2000;4:347-53.
11. Waldron�CA,�Koh�ML.�Central�mucoepidermoid�carcinoma�of�the�jaws:�report�of�four
cases�with�analysis�of�the�literature�and�discussion�of�the�relationship�to�mucoepi-
dermoid,�sialodontogenic,�and�glandular�odontogenic�cysts.�J�Oral�Maxillofac�Surg
1990;48:871-7.�
12. Brookstone� MS,� Huvos� AG.� Central� salivary� gland� tumors� of� the� maxilla� and
mandible:�a�clinicopathologic�study�of�11�cases�with�an�analysis�of�the�literature.�J
Oral�Maxillofac�Surg�1992;50:229-36.
13. Alexander�RW,�Dupuis�RH,�Holton�H.�Central�mucoepidermoid�tumor�(carcinoma)
of�the�mandible.�J�Oral�Surg�1974;32:541-7.�
14. Browand�BC,�Waldron�CA.�Central�mucoepidermoid�tumors�of�the�jaws.�Report�of�nine
cases�and�review�of�the�literature.�Oral�Surg�Oral�Med�Oral�Pathol�1975;40:631-43.
15. Inagaki�M,�Yuasa�K,�Nakayama�E,�Kawazu�T,�Chikui�T,�Kanda�S,�et�al.�Mucoepidermoid
carcinoma�in�the�mandible:�findings�of�panoramic�radiography�and�computed�to-
mography.�Oral�Surg�Oral�Med�Oral�Pathol�Oral�Radiol�Endod�1998;85:613-8.
16. Ezsiás�A,�Sugar�AW,�Milling�MA,�Ashley�KF.�Central�mucoepidermoid�carcinoma�in
a�child.�J�Oral�Maxillofac�Surg�1994;52:512-5.�
17. Baj�A,�Bertolini�F,�Ferrari�S,�Sesenna�E.�Central�mucoepidermoid�carcinoma�of�the
jaw�in�a�teenager:�a�case�report.�J�Oral�Maxillofac�Surg�2002;60:207-11.�
18. Cohen-Kerem�R,�Campisi�P,�Ngan�BY,�Iera�D,�Sándor�GK,�Forte�V.�Central�mucoepi-
dermoid� carcinoma� of� the�mandible� in� a� child.� Int� J� Pediatr� Otorhinolaryngol
2004;68:1203-7.�
19. Namin�AK,�Moshref�M,�Shahoon�H,�Mashhadi�A,�Khojasteh�A.�Intraosseous�mucoepi-
dermoid�carcinoma�of�the�maxilla�in�a�teenager:�a�case�report�and�review�of�litera-
ture.�Oral�Surg�Oral�Med�Oral�Pathol�Oral�Radiol�Endod�2005;�100:e93-6.�
20. Moraes�P,�Pereira�C,�Almeida�O,�Perez�D,�Correa�ME,�Alves�F.�Paediatric�intraoral
mucoepidermoid� carcinoma� mimicking� a� bone� lesion.� Int� J� Paediatr� Dent
2007;17:151-4.
21. Bhaskar�SN:�Central�mucoepidermoid�tumors�of�the�mandible.�Cancer�1963;�16:721-6,�
22. Simon�D,�Somanathan�T,�Ramdas�K,�Pandey�M.�Central�Mucoepidermoid�carcinoma
of�mandible� -� A� case� report� and� review� of� the� literature.�World� J� Surg� Oncol
2003;25:1-5.
23. de�Mello-Filho�FV,�Brigato�RR,�Mamede�RC,�Ricz�HM,�Saggioro�FP,�Xavier�SP.�Cen-
tral�mucoepidermoid�carcinoma:� report�of�2�cases.�Br�J�Oral�Maxillofac�Surg
2008;46:239-41.�
24. Johnson�B,� Velez� I.� Central�mucoepidermoid� carcinoma�with� an� atypical� radi-
ographic� appearance.� Oral� Surg� Oral� Med� Oral� Pathol� Oral� Radiol� Endod
2008;106:e51-3.�
25. Sidoni�A,�D'Errico�P,�Simoncelli�C,�Bucciarelli�E.�Central�mucoepidermoid�carcinoma
of�the�mandible:�report�of�a�case�treated�13�years�after�first�radiographic�demon-
stration.�J�Oral�Maxillofac�Surg�1996;54:1242-5.�
26. Winkle�MR,�Harrington�PC,�Maronian�N.�Central�mucoepidermoid�carcinoma�of�the
mandible.�Am�J�Otolaryngol�1999;20:169-71.�
27. Zaharopoulos�P.�Primary�intraosseous�(central)�salivary�gland�neoplasms�in�jaw
bones:�report�of�a�mucoepidermoid�carcinoma�of�the�mandible�diagnosed�by�fine-
needle�aspiration�cytology.�Diagn�Cytopathol�2004;31:271-5.
28. Lebsack�JP,�Marrogi�AJ,�Martin�SA.�Central�mucoepidermoid�carcinoma�of�the�jaw
with�distant�metastasis:�a�case�report�and�review�of�the�literature.�J�Oral�Maxillofac
Surg�1990;48:518-22.�
29. Eversole�LR,�Sabes�WR,�Rovin�S:�Aggressive�growth�and�neo-plastic�potential�of
odontogenic�cysts�with�special�reference�to�central�epidermoid�and�mucoepidermoid
carcinomas.�Cancer�1975;35:270-82.�
30. Neville�BW,�Damm�DD,�Allen�CM,�Bouquot�JE.�Oral�and�Maxillofacial�Pathology.
2nd�ed,�Philadelphia-London-Toronto:�W.B.�Saunders�Co,�2002:�420-3.
31. Auclair�PL,�Goode�RK,�Ellis�GL.�Mucoepidermoid�carcinoma�of�intraoral�salivary
glands.� Evaluation� and� application� of� grading� criteria� in� 143� cases.� Cancer
1992;69:2021-30.
32. Freije�JE,�Campbell�BH,�Yousif�NJ,�Clowry�LJ�Jr.�Central�mucoepidermoid�carcinoma
of�the�mandible.�Otolaryngol�Head�Neck�Surg�1995;112:453-6.�
33. Caccamese�JF,�Ord�RA.�Paedi�atric�mucoepidermoid�carcinoma�of�the�palate.�Int�J
Oral�Maxillofac�Surg�2002;31:136-9.
34. Maremonti�P,�Califano�L,�Mangone�GM,�Zupi�A,�Guida�C.�Intraosseous�mucoepider-
moid�carcinoma.�Report�of�a�long-term�evolution�case.�Oral�Oncol�2001;37:110-3.
35. Dhawan�IK,�Bhargava�S,�Nayak�NC,�Gupta�RK.�Central�salivary�gland�tumors�of�jaws.
Cancer�1970;26:211-7.
ΒΙΒΛΙΟΓΡΑΦΙΑ
00_00_ANDRESSAKIS-5:MASTER ORL 16/07/2010 9:35 ΠΜ Page 95














![Contentspi.math.cornell.edu/~danielhl/dcts_2020_09_22.pdf · 2020. 10. 1. · sometimes referred to as \window categories." The mathematical physicists Hori, Herbst, and Page [HHP]](https://static.fdocument.org/doc/165x107/60acb1ddcaf81b42667a28e3/danielhldcts20200922pdf-2020-10-1-sometimes-referred-to-as-window-categories.jpg)
