ΕΓΚΥΜΟΣΥΝΗ ΚΑΙ ΥΠΕΡΤΑΣΗ Ανδρέας Πιτταράς Καρδιολόγος Hypertension specialist ESH

ΥΠΕΡΤΑΣΗ ΣΤΟΥΣ
ΑΘΛΗΤΕΣ
Ανδρέας ΠιτταράςΚαρδιολόγος - Hypertension Specialist ESH
Ass. Prof. George Washington University USAΥπερτασικό ιατρείο Ασκληπιείο Βούλας
MEDITON

Disclosure of Relationships
Over the past 12 months
No relationships to disclose
on this lecture
A. Pittaras

Physical exercise is known to lower BP
and reduce cardiovascular risk
through a wide range of mechanisms.

Effects of Exercise/Physical Activity
• Antihypertensive
• Anti-atherogenic
• Anti-arrhythmic
• Lipid Metabolism
• CHO Metabolism
• LVH Regression
• Cardiac Function
• Endothelial Function
• Weight Control
• Bone Density
• Reduces Stress
• Increases Energy
• Induces Deep Sleep
• Improves Brain Function
• Free & Safe
• No Side-effects

Effects of Exercise/Physical Activity
• Lower risk of all-cause
mortality
• Lower risk of CVD
mortality
• Lower risk of CVD
(including stroke)
• Lower BP & risk of HTN
• Lower risk of T2DM
• Lower risk of adverse
lipid profile
• Lower risk cancers of the
bladder breast colon,
endometrium esophagus
kidney lung stomach
• Improved cognition
• Reduced risk dementia
• Improved quality of life
• Reduced anxiety
• Reduced risk depression
• Improved sleep
• Slowed-reduced weight gain
• Weight loss
• Prevention of weight regain
• Improved bone health
• Improved physical function
• Lower risk falls- injuries
older
JAMA
Nov 2018

Endothelial function
Coronary flow reserve
Tolerance of myocardial ischaemia
Myocardial capillary density
Ventricular fibrillation thresholds
Arterial blood pressure
Arterial stiffness
CV benefits of regular endurance training

EXERCISE
OBESITY
HTN
DYSLIPIDEMIADIABETES
CAD AFib
CKD

P.F.Kokkinos, A. Pittaras., et al. Cardiology Clinics 2001;19(3):507-516
Kokkinos P, Pittaras A., et al. New Eng J Med 1995;333:1462-7
P.Kokkinos, M. Doumas, A.Pittaras, A. Manolis et. Al. Hypertension 2009
Faselis C., Doumas M, Pittaras A, Kokkinos P. Hypertension 2014
P.Kokkinos, M. Doumas,A. Pittaras, Α. Manolis Am. J. of Hypertension 2009
P. Kokkinos, M. Doumas, A. Pittaras, A. Manolis , Blood Pressure 2009
A.Pittaras, M. Doumas, P. Kokkinos et. al. Top Scoring Abstract AHA & ACC Meeting
C. Faselis, A. Pittaras, P. Kokkinos et al Mayo Clin Proc. 2016
Kokkinos P. Pittaras A. et al. Diabetes Care 2009 32:623-28
A. Pittaras, C. Faselis, P. Kokkinos et al Am J Cardiol. 2013
Kokkinos P, Pittaras A., et al. Circulation 2008
Narayan P, Doumas M, Pittaras A, Kokkinos PF. Am J Cardiol. 2017
Lovic D, Narayan P, Pittaras A, Faselis C, Doumas M, Kokkinos P. J Clin Hypertens 2017

HTN IN ATHLETES
• HTN is the most prevalent CVD among athletes
and physically active subjects.
• The management of HTN in athletes can differ
from standard approaches, primarily due to the
potential side effects of some medications that
may impair training and performance.

“ATHLETS”
• Competitive athletes:
-Scholastic (high school)
-Club
-Collegiate
• Professional
• Recreational athletes
• Exercise for fitness and health

Hypertension in athletes: epidemiology
...the overall prevalence of high BP in athletes
is approximately 50% lower than in the general
population…
Fagard RH , Cardiol Clin 2007

HTN IN ATHLETS
• There was no evidence that BP was lower in athletes
than in controls.
• A number of studies showed a higher BP in athletes.
• The prevalence of HTN in athletes could not be
determined reliably because of different definitions of
HTN and poorly standardised methods of BP
measurement.
• A positive linear association between high BP and
LVH was observed in athletes, but confounding
factors may have played a role.
• Future studies should be designed to determine more
precisely the prevalence, determinants and
prognostic significance of HTN in athletes.

51 studies: 138.390 Athletes. H. Berge BMJ 2015

51 studies: 138 390 athletes. H. Berge BMJ 2015

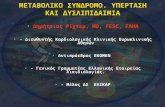
Prevalence of HTN in athletes. H. Berge BMJ 2015

Prevalence of HTN in athletes. H. Berge BMJ 2015

Prevalence of HTN in athletes. H. Berge BMJ 2015

• HTN was defined in 11 different ways in the 25 studies.
• The most often used criteria for HTN ranged from SBP
≥140 or DBP ≥90 mm Hg to BP>140/90 mm Hg.
• The lowest cut-off value for HTN was BP ≥130/85 mm Hg
and the highest cut-off value was ≥160/95 mm Hg.
• 3 studies used medication to define HTN.
• One accepted self-reported HTN
• One only included participants with BP≤120/80 mm Hg.
• The prevalence of HTN was lower in studies that were
restricted to athletes within the age range 18–40 years
• 6 studies excluded patients with high BP>140/90mm Hg.
Prevalence of HTN in Athletes studies

Method of BP measurement in athletes Ι
• Some descriptions of measurement methods in 21 studies
• BP was measured in the sitting position in 10 studies and in a
supine position in 6 studies.
• At least 5 min of rest prior to BP recordings was required in 11
studies, while only 4 informed about time from physical activity
to BP measurement.
• Athletes abstained from caffeine and/or smoking prior to BP
recordings in 2 studies, and no studies informed about the
physical environment where the BP measurements took place.
• Only 8 studies reported whether an appropriate cuff size was
used. In the 8 studies using a ‘standard’ mercury
sphygmomanometer, the method of measurement performance
was reported in 3 studies.
• Only the 3 studies that used an automated BP device reported
the device type and manufacturer.

Method of BP measurement in athletes ΙΙ
• A single measurement in 5 studies, but repeated in 3 of
these if BP was high. The lowest of these values was
registered in 2 studies, and the highest in one.
• BP was recorded 2 and 3 times in 6 and 4 studies,
respectively, and there was a significant difference in
SBP between one and two BP recordings (127±4.7 vs
118±4.0mm Hg, p<0.05).
• Choice of arm for measurement was presented in 5
studies and no study measured BP in both arms.
• 3 studies recommended repeated BP recordings on a
separate occasion if the BP was elevated.
• Only 1 study referred athletes with elevated office BP to
ambulatory BP measurement.

Children and adolescents
• Age-adjusted tables baseupon gender and height percentile
Power sport athletes
• Measurement of forearm circumference
Appropriately sized cuff
• Good luck finding one…
Establishing BP levels in young athletes or in power sports (boxing, wrestling, weight
lifting) athletes is not so simple…

Establish BP levels in Athletes
• 410 football players at the annual preventive check (age
16±4 years)
• 41 athletes out of 410 (10%) were detected as having
elevated SBP or DBP in the first measurement.
• 18 athletes out of 410 (4.4%) had BP above the accepted
normal levels after two or more BP measurements
• Only 2 athletes had elevated 24h-ABPM values!
• Be careful (as usual) in diagnosing hypertension before
starting treatments / restrain the activity of an athlete!
Kouidi E et al, Am J Hypert 1999


Screening for Secondary Causes
• Prevalence of 2nd HTN in athletes is expected to be the
same as in the general population.
• Certain special situations must also be considered.
• Wheelchair athletes with spinal cord injuries above T6
level may have severe episodic HTN in the case of self-
induced autonomic dysreflexia (commonly known as
boosting), which is a massive sympathetic discharge
induced by nociceptive stimuli, improving performance
time by 10% in elite wheelchair marathon racers during
simulated racing.

Drug-induced HTN in Athletes
• NSAIDs
• Oral contraceptive pills (commonly taken by female
athletes)
• Herbal and dietary supplements used to increase energy or
control weight, containing “natural” substances such as
Guarana, Ma huang, and Ephedra, which are stimulants.
• Performance-enhancing drugs, such as Androgen-anabolic
steroids, Growth hormone, Erythropoietin, or Stimulants
such as Amphetamines, Caffeine, Ephedrine and
Pseudoephedrine and Cocaine have negative
cardiovascular effects, including HTN.
• Doping substances, impair both lipid and glucose
homeostasis, may favor in direct prothrombotic effect
(erythropoietin), in vasospasm (cocaine) or arrhythmias
(cocaine and other stimulants).

Assessment of TOD in Athlets
• Urinalysis, including microalbuminuria, is among routine
laboratory investigations to be performed in HTNsive pts.
• In athletes false positive results are likely, since exercise-
induced proteinuria, a benign and reversible
phenomenon, may occur if vigorous physical activity is
performed in the 24 h before the test.
• Echocardiography and ETT (with ECG and BP
monitoring), which are not always included in evaluation
of the HTNsive pt, are warranted as routine tests in the
HTNsive athlete

Lovic D, Pittaras A, Faselis C, Doumas M, Kokkinos P. J Clin Hypertens 2017




Predominant Changes in Heart with Aerobic Training
Volume Load Increases
Diastolic Stress Increases
Chamber Size Increases
Eccentric LVH

• Inhaling and breath holding while engaging in
the actual lifting of a weight (i.e., Valsalva
maneuver) can result in extremely high BP
responses, dizziness and even fainting,
especially in hypertensive individuals.
• Thus, such practice must be avoided during
resistance training.
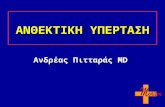
WEIGHT LIFTING

BP up to 345/245 mm
Hg have been recorded
during heavy lifts.
• Activation of central
sympathetic drive
• Size of muscle mass
• Intrathoracic and
intraabdominal
pressure associated
with Valsalva.
McDougall JD, et al. J Appl
Physiol ‘85 58:758-90
McDougall JD, et al. J Appl
Physiol ‘92 73:1590-97
Palatini et al. J Hypertension
1989 7(6)S72-S-73

Predominant Changes in Heart with Resistance/Anaerobic Training
Pressure Load Increases
Systolic Stress Increases
Wall Thickness Increases
Concentric LVH



10
20
30
40
50
60
70
80
90
100
<5 5 6 7 8 9 10 12 14 18 22
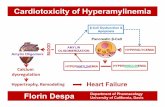
Schematic Representation of Exercise-
Related Health Benefits
Threshold
>16-22 METs
Athletes/
Marathoner, etc
Plateau
%
13-16 METs
Highly Active
METS
Most of these health
benefits are realized at
relatively low levels
of physical activity






Differential effect of prolonged intense exercise on RV & LV volumes.

Duration-dependent effect of endurance events on right ventricular EF.

hs-cTnT concentrations before, immediately after, and 24 and 72 hours after marathon

Mayo Clin Proc. 2012 Jun; 87(6): 587–595.

Proposed pathogenesis of cardiomyopathy in endurance athletes

long-term sustained vigorous aerobic ET increases the prevalence of AFib

Characteristics of endurance exercise speculated to promote AF
N. John Bosomworth et al Can Fam Physician 2015;61:1061-70

STUDIES IN ATHLETES

Potential association between dose of endurance sports and CV events

Lancet. 2011;378(9798):1244–1253
Relationship between dose of physical activity and
reduction in all-cause mortality. The mortality benefits of exercise appear with even small amounts of daily
exercise and peak at 50 to 60 minutes of vigorous exercise per day.

Nonpharmacological Treatment
• All HTNsives have to adhere to lifestyle changes.
• In athletes with grade 1–2 HTN at low/moderate added CVR,
it is possible to delay the initiation of treatment by several
weeks, in order to assess the efficacy of lifestyle changes.
• Athletes are often more motivated to comply with
nonpharmacological interventions.
• Reduction of high sodium, and increase foods rich in K+
(endurance athletes may tend to be hypokalemic).
• Weight loss for overweight athletes, under specialist
supervision.
• BP-raising substances, (NSAIDs etc).
• In patients with 2nd HTN, clinical evaluation for sports
participation is preferably postponed to after removal of the
cause of hypertension.

2007 , 2009, 2013, 2018 ESH/ESC GuidelinesCombinations between Some Classes of Antihypertensive Drugs
Thiazide diuretics
ACE-i
CCBs
ARBs
• Pronounced antihypertensive effect
• CV protection
• Optimal tolerability

• Antihypertensive drugs such as beta blockers and diuretics impair
the ability to regulate body temperature during exercise in hot and/or
humid environments and provoke hypoglycemia.
• People using these medications should be educated on the
signs/symptoms, adequate hydration, proper clothing, the optimal
times of the day, decreasing time and intensity during periods of
increased heat or humidity, and methods to prevent hypoglycemia.
• In addition, beta blockers can alter submaximal and maximal exercise
capacity, particularly in those without myocardial ischemia.
• Because antihypertensive agents such as alpha blockers, CCBs, and
vasodilators may provoke hypotensive episodes after abrupt
cessation of activity, extending the cool-down period is generally
recommended.

• In athletes two further aspects should be considered:
- Some drugs are considered doping substances and are banned
by several sports associations
- Others have a negative effect on exercise performance.
• RAAS blockers and dihydropiridine CCBs appear to be the first
choice antihypertensive agents particularly in endurance athletes,
since they have no major effects on energy metabolism or
cardiovascular adaptation to exercise.
• RAAS blockers are contraindicated in female athletes during the
reproductive age.
• α-blockers and centrally acting α-agonists can be used in association
as second- or third-choice drugs.
Pharmacological Treatment

• Diuretics usually not recommended, favoring the excretion or dilution
of illegal substances, rapid weight loss, in weight-related categories
(boxing),so they are considered doping substances in several sports.
• Diuretics impair exercise performance and capacity in the first weeks
of treatment, and appears to be restored during long-term treatment.
• Loop diuretics can also precipitate hypovolemia, orthostatic
hypotension, and electrolyte imbalance (loss of potassium,
magnesium), in pts exercising intensely or in warm weather.
• Diuretics are contraindicated in elite athletes requiring drug testing.
• As second- or third-choice drugs and at low dosage in physically
active patients with HTN and salt-sensitive HTNsive athletes (blacks).
• Potassium-sparing diuretics avoid electrolyte disturbances.
Pharmacological Treatment: Diuretics

• β-blockers are prohibited in certain competitive sports (shooting, ski
jumping, archery, diving) due to their antitremor and anxiolytic effect.
• β-blockers affect sports performance in endurance athletes, as a
consequence of their negative ino- and chrono-tropic effect and
impairment of muscle blood flow, thus increasing the perception of
greater exertion during exercise.
• Inhibition of lipolysis and glycogenolysis could impair energy
metabolism.
• β-blockers should be used in athletes only when it is mandatory, as in
the presence of coronary artery disease, rather than merely for their
antihypertensive effect.
• For mandatory cases, a combined α-β blocker may be the best choice,
since they are expected to provide a lesser impairment of muscle
blood flow and of maximum oxygen uptake.
Pharmacological Treatment: β-blockers

• Diuretics and beta blockers are not ideal drugs for
athletes in sports with high aerobic demands.
• If these are the optimal therapy, and are not
banned by the sport's governing body, consider
carefully the time doses.
• It is best to take diuretics at least 7-8 hours prior.
• Be aware of the risks of hypoK and hypoNa.
• Beta blockers is best to take them at least 3-4
hours prior to competition.
• It is unknown what if any adjustments are needed
for extreme endurance events (eg, marathon,
ironman). Take any new medication for at least
one week prior to any competitive event.

Athletes with exaggerated BP response to ETT
• Normal or Increased resting BP.
• This issue is particularly complex.
• No widely accepted definition of exertional HTN:
- Cut off the 90°–95° percentile
- Fixed number
- Peak values
- 3 min ETT
- BP in the recovery period or at a chosen heart rate
- Peak SBP >210 mmHg for men and >190 mmHg for women.
• Possible negative prognostic role (±) independently of resting BP.
• Such rises should not be a reason to restrict physical activity.
• Those Athletes are more prone to develop HTN.
• Reasonable to recommend to regularly check BP, either at home
or in a clinical setting, in order to promptly intervene if
hypertension develops.

Sports eligibility depends on the pt’s risk profile

CONCLUSION
• Incidence of HTN is low in athletes, but it can be more
frequent with advancing age
• It is important to exclude the intake of substances which
can increase BP values (and CV risk!!)
• Diagnostic procedures must include echocardiography
and exercise testing
• Sport activity can be permitted depending on the presence
of well controlled BP values and low CV risk
• Althoug compelling indications do not exist, preferred
pharmacological treatment should be based on RAS-
blockers and/or calcium antagonists
• While endurance sports reduce CV events, power sports
increase the risk of coronary artery disease