







γλώσσες
Σελίδες
Νομικός

©Copyright2012OregonStateUniversity.AllRightsReserved
DrugUseResearch&ManagementProgramOregonStateUniversity,500SummerStreetNE,E35Salem,Oregon97301-1079Phone503-947-5220|Fax503-947-1119
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
NewDrugEvaluation:patiromerpowderfororalsuspensionDateofReview:3/17/16 EndDateofLiteratureSearch:3/17/16GenericName: patiromer BrandName(Manufacturer):Veltassa®(Relypsa)PDLClass:PotassiumExchangers AMCPDossierReceived:YesResearchQuestions:• Ispatiromermoreeffectivethanplaceboatmaintainingnormalpotassiumlevelsinpatientswithchronickidneydisease(CKD)andpatientswithheart
failure(HF)whoarealsoonACEIs,ARBsorspironolactone?• Aretheresubgroupsofpatientsbasedondemographics(e.g.,age,racialgroups,gender),comorbidities(e.g.,drug-diseaseinteractions,obesity),orother
medications(drug-druginteractions)forwhichpatiromerismoreeffectiveorsafe?Conclusions:• Patiromerwasstudiedin1phase2trial,atwo-part,singleblind,phase3trial,anda52-week,open-labelrandomized,dose-findingphase2trial.Major
limitationsofthedataincludeahighriskofperformancebiasandselectionbias.GeneralizabilityislimitedbyrelativelyfewstudysiteswithintheU.S.,significantexclusioncriteria,difficultdosingschedules,andalackofdatacomparingpatiromertoothermeasurestoreducepotassium.Inaddition,intheprimaryefficacystudy,onlypatientswhoinitiallyrespondedtotreatmentwithpatiromerwererandomizedtotheprimarytrialperiod,increasingtheriskofbiasandpotentiallythebeneficialeffectofthedrugobserved.Lastly,thisstudywassponsoredanddesignedincollaborationbythepharmaceuticalcompany.
• Thereislowqualityevidencethatpatiromercandecreaseserumpotassiumlevelsfrom0.35mEq/Lto1.23mEq/Lover4weeksoftherapyinpatientswithCKDandhyperkalemiaonareninangiotensinaldosteronesystem(RAAS)inhibitor.Themagnitudeofpotassiumdecreaseismorepronouncedwithahigherbaselinepotassiumlevel.
• ThereislowqualityevidencethatinpatientswithCKDonaRAASinhibitorwithbaselinehyperkalemia,patiromerisassociatedinareductionintherecurrenceofhyperkalemia(60%vs.15%)through8weeksoftreatment.
• Thetrialswereshorttermandnotdesignedtodetectdifferencesinanylongtermcomplicationsofchronichyperkalemia(suddencardiacdeathorventriculararrhythmias).Thereisinsufficientevidencethatpatiromerpreventslongtermcomplications,includingarrhythmias.
• Themostcommonadverseeffectsseenshort-termaregastrointestinal(flatulence,diarrhea,constipation,vomiting,nausea),hypomagnesemia,chronicrenalfailure,andanemia.Thereisaboxedwarningtoadministerotheroralmedicationsatleast6hoursbeforeor6hoursafterpatiromer,duetothepotentialbindingofpatiromertoothermedications.
• Longerstudiesareneededtoassessthesafetyoflongtermuseandtoappropriatelydefineitsplaceintherapy.Itremainsunclear,ifpatiromerwillallowforthelongtermadministrationofRAAStherapyinpatientswithCKDorHFandhyperkalemia.ConsiderationoftheriskversusbenefitofRAASinhibitortherapyandadjustmentordiscontinuationofothermedicationsorherbaltreatmentsthatmaycontributetoserumpotassiumisnecessary.
• Duetotheslowonsetofpatiromer,thereiscurrentlynoplaceintheacutetreatmentofhyperkalemia(≥6.5mEq/L).
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
Recommendations:• DeferPDLdecisionsuntilareviewofsodiumpolystyrenesulfonateandzirconiumcyclosilicate(awaitingFDAapproval)atanupcomingP&Tmeeting.• RecommendclinicalPAcriteriatopreventuseintheemergentsettingorinscenariosnotsupportedbythemedicalliterature(Appendix2).Background:
Hyperkalemiaiscommoninpatientswithchronickidneydisease(CKD)orheartfailure(HF).Multipledefinitionsofhyperkalemiaexist,includingpotassiumlevelsover5.0,5.5,or6.0mEq/L.1Hyperkalemiaisduetoalteredpotassiumhandlingbythekidneys,aldosteroneresistanceleadingtodecreasedpotassiumexcretion,acidosisorlackofinsulin.2InHFwithreducedejectionfraction,(HFrEF),angiotensinconvertingenzymeinhibitors(ACEi,),angiotensinIIreceptorblockers(ARBs),andaldosteroneantagonistshavebeenshowntobeeffectiveinreducingmorbidityandmortalitybutcanalsocausehyperkalemia.ThesemedicationshavealsodemonstratedtheabilitytodecreaseprogressionofkidneydiseaseinpatientswithdiabetesandCKD.Therefore,theoptimizationoftreatmentwiththesemedicationsisoftenlimitedbythedevelopmentofhyperkalemia.
Hyperkalemiacanresultinflaccidityofmuscles,paralysis,andmoreseriouslycancauselife-threateningcardiacarrhythmiasandincreasedmortality.3Treatmentisindicatedinpatientswithpotassiumlevelsover6mEq/L,orwithrapidincreasesinpotassiumlevel.4,5Severalmedicationsareusedtotreathyperkalemiaintheemergentsetting(seeTable1).Mostofthesehaveafastonsetandworkeitherbyshiftingpotassiumintracellularlyorbyremovingpotassiumfromthebody.However,thereisnodatatosupporttheuseofthesetherapiesinthesettingofchronichyperkalemia.Althoughsometimesusedchronicallyinpatients,theprolongeduseofsodiumpolystyrenesulfonate(SPS)increasestheriskofdevelopingbowelnecrosisduetoitssorbitolcontainingformulation.Italsohasanunpleasanttaste,andcommonlycausesdiarrhea.ThelargeststudyevaluatingSPSinvolvedonly32patientswitheitheracuteorchronicrenaldisease;howeverthesepatientswereonlytreatedforuptosixdays.6Theonlyothercurrentoptiontolowerpotassiumlevelareloopdiuretics.ChronicuseofloopdiureticsislimitedbyelectrolyteimbalancesandtheymaynotbeaseffectiveinpatientswithCKD.Patiromer,acationexchangepolymer,wasdevelopedasapotentialoptionfortreatmentinchronichyperkalemia.Itisnoteffectivefortheemergencytreatmentoflifethreateninghyperkalemiabecauseofitsdelayedonsetofaction.7Inadditiontomedications,severalothermeasuresmaybeeffectivetopotentiallyreduceserumpotassium.Thisincludescounsellingonalowpotassiumdietandreviewofmedicationsthatcancontributetoanelevatedpotassiumlevel(NSAID,potassium-sparingdiuretic,potassiumorherbalsupplements).Patiromerisanonabsorbedpolymerthatbindspotassiuminexchangeforcalciumpredominantlyinthedistalcolon,increasingfecalpotassiumexcretion.Asitisnotabsorbed,theamountofcalciumabsorbedremainssmall.Table1.Acutetreatmentforhyperkalemia
Shiftpotassiumintracellularly RemovepotassiumInsulin(withglucose) Diuretics(i.e.loop,thiazide)Sodiumbicarbonate(formetabolicacidosis) Sodiumpolystyrenesulfonateβ-2adrenergicagonists(i.e.albuterol) SeeAppendix1forHighlightsofPrescribingInformationfromthemanufacturer,includingBlackBoxedWarningandRiskEvaluationMitigationStrategies(ifapplicable),indications,dosageandadministration,formulations,contraindications,warningsandprecautions,adversereactions,druginteractionsanduseinspecificpopulations.

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
ClinicalEfficacy:
Patiromerwasstudiedin1phaseIItrial,atwo-part,singleblind,phaseIIItrial,anda52-week,open-labelrandomized,dose-findingphaseIItrialforboththepreventionandtreatmentofhyperkalemia.Patientsincludedintheclinicaltrialshadeitherchronickidneydisease(CKD)orheartfailure(HF).
ThePEARL-HFtrialwasa4weekphaseIItrialevaluatingpatiromerforthepreventionofhyperkalemiawhichisanoff-labeluseinpatientstreatedwithstandardtherapyforHFwithserumpotassiumof4.3to5.1mEq/L.OverhalfofthepatientsincludedhadCKD,and36%hadahistoryofhyperkalemia(7.5%hadbothCKDandhistoryofhyperkalemia).OverallmorenormokalemiapatientswithHFrEFonstandardtherapywereabletotitrateuptospironolactone50mgdailyandavoidhyperkalemiathanpatientsonplacebo.8Thistrialfoundthatthechangeinpotassiumwithpatiromerusewas-0.45mEq/L(p<0.001).Theclinicalsignificanceofthisdifferenceinpotassiumisunclear,asevenintheplacebogrouppotassiumonlyincreasedby0.22mEq/l.Fewerpatientsonpatiromerexperiencedhyperkalemia(serumpotassium>5.5mEq/L)comparedtoplacebo(7.3%vs.24.5%).Ninety-onepercentofpatientsinthepatiromergroupand74%ofpatientsintheplacebogroupweresuccessfullyincreasedtothehigherspironolactonedose(p=0.019).However,itisunclearifthisincreasedspironolactonedosehasahighermortalitybenefitcomparedto25mg,asthemeanspironolactonedoseachievedinpreviousHFtrialswas26mg/day.9ThepatientsinthisstudyareagoodrepresentationoftheHFpatientswhocouldclinicallybenefitfrompatiromeruse,astheyhadotherrisksfordevelopinghyperkalemia,suchascomorbidCKDandmoreadvancedage.However,thisstudydidnotevaluatepatiromerforthetreatmentofhyperkalemiainpatientswithHF.
TheprimaryphaseIIItrial(OPAL-HK)evaluatedtheuseofpatiromerinpatientswithhyperkalemiaandCKDreceivingRAASinhibitors(n=243).12,13Afteraninitialdosetitrationperiodbasedonbaselinepotassiumlevel,onlypatientswhorespondedtotherapywererandomizedto8weeksofeithercontinuedpatiromertherapyorwithdrawal.Theprimaryoutcomewasreductioninserumpotassiumafter4weekscomparedtobaseline,andcomparedtoplaceboinan8-weekwithdrawalphase.Duringthefirstphase,62%ofpatientshadmoderate-to-severehyperkalemiaandtheremainderhadmild(38%),andthemeanchangeinserumpotassiumlevelsfrombaselinetoweek4was-1.01mmol/L(95%CI-1.07to-0.95)withalargerchangeinpatientswithmoderate-to-severehyperkalemia(-1.23mmol/L)comparedtothosewithmild(-0.65mmol/L).Onlypatientswhosepotassiumlevelhadbeenwell-controlledduringtheinitialphasewereincludedinthesecondphase,increasingtheriskofbiasandpotentiallythebeneficialeffectofthedrugobserved.Afterweek8inthewithdrawalphase,fifteenpercentofpatientsinthepatiromergroupand60%ofpatientsintheplacebogrouphadhyperkalemiawithpotassium>5.5mEq/L,and43%ofthepatiromerpatientsand91%oftheplacebopatientshadhyperkalemiawithpotassium>5.1mEq/L(bothp<0.001).Inanexploratoryanalysis,94%ofpatientsinthepatiromergroupwerestillreceivingRAASinhibitorsattheendofthestudy.However,riskofbiasinthisstudyishighandgeneralizabilityislowbecausetherun-inphaseresultedinonlyrespondersandthosewithmoderatehyperkalemiatoberandomizedinthe8weektrial.Apoorerresponseisexpectedintherealworldsetting.Thisstudywasfundedbythepharmaceuticalcompanyandwasdesignedincolloaborationwiththesponsor.
AMETHYST-DNtrialwasamulticenter,open-label,dose-ranging,phase2trialof324patientswithtype2diabetesmellitus(T2DM)andCKD.10,11Thistrialconsistedofthreephasesandapost-treatmentfollow-upphase:duringthe4-weekrun-in,patientswithserumpotassiumlessthan5.0mEq/LwererandomizedtocontinuethecurrentACEi/ARBtherapyorswitchtolosartan100mgdaily.After2weeks,ifbloodpressurewasuncontrolled,spironolactone25mgdailywasinitiated;thiscouldbeincreasedto50mgdailyforfurtherbloodpressurelowering.Duringthesecondphase,patientswithbaselinepotassiumof5.0-6.0mEq/Lwereincludedinathirdcohortthatskippedtherun-inphase;thisthirdcohortmadeupaboutthree-fourthsofthestudypopulation.Patientsfromallthreecohortswereagainrandomizedto8weeksoftreatmentwithpatiromeratvariousdoses(4.2-16.8gBID)basedonbaselinepotassiumlevel.Theprimaryendpointwasthemeancentrallabserumpotassiumlevelfrombaselinetoweek4ofthesecondphase.Overall,serumpotassiumleveldecreasedby0.35-0.97mEq/L,withahigherchangeinpotassiumlevelinthemoderatehyperkalemiagroup.Asignificantnumberofpatientswerenottreatedperprotocol;thereforetheeffectofpatiromeronpotassiumloweringmaybegreaterthanthatobserved.Ontheotherhand,giventheopenlabeldesignofthisstudyandhighnon-adherence,thereisanincreasedriskforbias.Thiscouldespeciallyhaveoccurredinpatientsathigherpotassiumlevels,whomayhavebeenmorecarefultoavoidothersourcesofpotassium,suchaspotassiumfoundinthediet.Itisthereforedifficulttosayifpatiromerwasthesolecauseofthelarger
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
potassiumchangeinthemoderatehyperkalemiagroup.Theproportionofpatientswithpotassiumlevelswithintargetrangeateachscheduledvisitofthemaintenancephasethroughweek52rangedfrom83.1%to92.7%inpatientswithmildhyperkalemia(n=180)andfrom77.4%to95.1%inpatientswithmoderatehyperkalemia(n=66).
Thereislowqualityevidencefromthesestudiestosupporttheuseofpatiromertolowerpotassiumlevelsfordurationof4weeks.However,theamountofpotassiumloweringmaydifferfromthatseeninthesingle-blindtrials,AMETHYST-DNandOPAL-HK.ClinicalSafety:
TheAMETHYST-DNtrialdemonstratedthatthemostcommonadversereactions(>1%)oflong-termpatiromeruseincludeworseningCKD(9.2%)orhypertension(7.9%),hypomagnesemia(8.6%),constipation(6.3%),diarrhea(5.6%),andhypoglycemia(3.3%).TheamountofCKDworseningwasnotdefined,althoughthisadverseeffectledto8patientsdiscontinuingtherapy.Althoughhypomagnesemiawasacommonadversereaction,nopatientsdiscontinuedtherapyduetohypomagnesemia,andnopatientsdevelopedseverehypomagnesemia(<1.0mg/dL).However,thisisapotentialconcern,aslowmagnesiumlevelsarealsoassociatedwithventriculararrhythmias,andmayincreasetheriskofdeathwhenincombinationwithlowpotassiumlevels.8
SeeTable2forcommonadverseeffectsseenwithshort-termuseofpatiromer,asseeninthePEARL-HFandOPAL-HKtrials.Themostcommonadverseeffectfoundinbothstudieswasgastrointestinal(GI)effects.Ingeneral,thiswasreportedtobemildtomoderate,withnopatientsexperiencingseriousGIeffects.InthePEARL-HFtrial,magnesiumdecreasedonanaverageof-0.22mg/dL.However,theincidenceofventriculararrhythmiaswasnodifferentthanplacebo.Similarly,magnesiumlevelsdecreasedby-0.1to-0.2mg/dLintheOPAL-HKtrial;thereseemedtobenocorrelationtomagnesiumdecreaseandpatiromerdose.Ninepatientsrequiredmagnesiumreplacementtherapy.AlthoughchronicrenalfailurewasreportedintheOPAL-HKtrial,therewasnosignificantchangeinrenalfunctionreportedineitherofthesetrials.Anemiawasnotdiscussed.
Anotherconcernisthestatedwarning/precautionthatpatiromerbindstomanyorallyadministeredmedicationsandallmedicationsshouldbeadministered6hoursbeforeorafterpatiromerduetotheriskofdecreasedabsorption.Thisdoesnotseemtobeaddressedinanyofthepatiromerstudies.Inpreviousratstudies,patiromerdidnotaffectdrugabsorptionformostdrugsthatarecommonlyusedinHFandCKD;howeverbioavailabilityofvalsartanandrosiglitazonewasdecreasedby30%.8
Thereislowevidence,providedbyAMETHYST-DN,thatpatiromerissafeandeffectiveforusefor52weeks.Overall,thecomplicationsofhyperkalemia(i.e.muscleweakness,arrhythmias)wereuncommon;furtherstudieswithalargerpatientpopulationwouldbeneededtodetermineifpatiromerisabletopreventthesecomplications.StudiesdidnotreportanysignificantdifferenceoranyclinicallysignificantchangesinECGparameters,howeverpatientsatriskforarrhythmiaswereexcludedfromtrials.Table2.Incidenceofcommonadverseeffectswithshort-termpatiromeruseAdverseEffect Patiromer(n=666) PlaceboConstipation 7.2% 0Hypomagnesemia 5.3% NADiarrhea 4.8% 0Nausea 2.3% 0Abdominaldiscomfort 2.0% NAFlatulence 2.0% NA

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
Look-alike/Sound-alikeErrorRiskPotential:NonePharmacologyandPharmacokineticProperties:14
Parameter
MechanismofActionIncreasesfecalpotassiumexcretionthroughbindingofpotassiuminthelumenofthegastrointestinaltract,resultinginareductionofserumpotassiumlevels.
Absorption NotsystemicallyabsorbedDistributionandProteinBinding N/A,notabsorbedMetabolism N/A,notabsorbedHalf-Life N/A,notabsorbedElimination FecallyAbbreviations:GI=gastrointestinal,N/A=notapplicableComparativeClinicalEfficacy:
ComparativeEvidenceTableRef./StudyDesign
DrugRegimens/Duration
PatientPopulation N EfficacyEndpoints
ARR/NNT
SafetyOutcomes
ARR/NNH
RiskofBias/Applicability
1.Pittetal.(PEARL-HF)8
Multicenter,double-blind,RCT,phase2study4weeks
1.Patiromer15gBID+spironolactone2.Placebo+spironolactone
Demographics:Age:68yearsMen:61%White:96.5%NYHAII:55%NYHAIII:42.5%LVEF:40+12%DM:32%CKD:56.5%Historyofhyperkalemia:36%CKDandhistoryofhyperkalemia:7.5%BaselineK:4.67
ITT:1.602.60mITT:1.552.49PP:1.562.49Attrition:1.5(8.3%)
PrimaryEndpoint:MeanchangeinserumKfrombaselineto28days:1.-0.22mEq/L2.+0.25mEq/LDifferencebetweengroups-0.45mEq/L,p<0.001SecondaryEndpoint:Proportionofpatientsincreasedtospironolactone50mg/d1.50/55(91%)
N/AARR48.6%NNT2
Outcome:GIdisorders1.21%2.6%Discontinuationsduetoadverseevents:1.4(7%)2.3(6%)
5 RiskofBias(moderate):SelectionBias:methodofrandomizationandallocationconcealmentisnotspecified.PatientsinthepatiromergrouphadmoreACEi/ARBuseandACEi/ARBplusBBusePerformanceBias:double-blinddesignindicatedbutblindingnotdescribed.DetectionBias:double-
ClinicallyRelevantEndpoints:1) Longtermmaintenanceofnormokalemia2) Complicationsofhyperkalemia3) Discontinuationsduetoadverseevents
PrimaryStudyEndpoint:1) MeandifferenceofchangeinserumKfrombaselineto28days(all
threestudies)2) DifferencebetweengroupsinserumKlevelafter4weeksof
patiromerdiscontinuation/continuation
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
KeyInclusionCriteria:-Age>18years-HistoryofchronicHFwithindicationtoinitiatespironolactone-K4.3-5.1mEq/L-CKD(eGFR<60mL/min)receivingatleast1HFtherapy,orhistoryofhyperkalemialeadingtoHFtherapydiscontinuationinthepast6monthsKeyExclusionCriteria:-SevereGIdisorders-MajorGIsurgery-Bowelobstruction-Swallowingdisorders-Significantprimaryvalvulardisease-Knownobstructive/restrictivecardiomyopathy-Unstableorstablearrhythmia-recentUA/ACS/TIA-QTc>500ms,BP>170/90mmHG,dialysis,elevatedLFTs>3xULN
2.11(18.3%) 2.36/49(74%)p=0.019
blinddesignindicatedbutblindingnotdescribed.NomentionwasmaderegardingblindingoftheoutcomeassessorsAttritionBias:Totalattritionrate13%(low),butdifferentialattritionrate10%ReportingBias:allendpointswerereportedApplicability:Patient:MainlywhitepatientswithHFNYHAIIandIII(97.5%)andCKD(56.5%).Significantexclusioncriteriareducegeneralizabilityofresults.Intervention:unclearifseparatedfromothermedicationsaccordingComparator:NodatacomparedtoothermeasurestomanagehyperkalemiaOutcomes:Primaryoutcomewasasurrogateoutcome.Shorttermstudynotdesignedtodetectdifferencesinlongtermcomplicationsofhyperkalemia.Setting:Patientswere
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
enrolledfrom38centersintheUS,Germany,CzechRepublic,Poland,Ukraine,Russia,andGeorgia
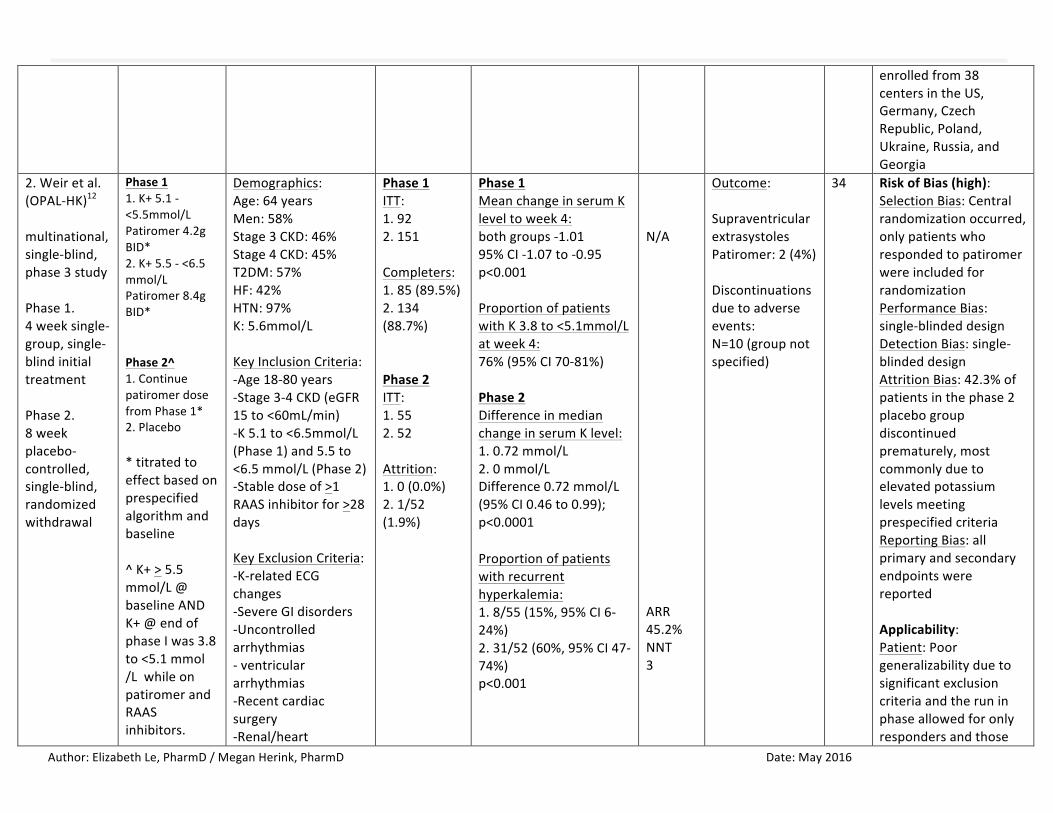
2.Weiretal.(OPAL-HK)12
multinational,single-blind,phase3studyPhase1.4weeksingle-group,single-blindinitialtreatmentPhase2.8weekplacebo-controlled,single-blind,randomizedwithdrawal
Phase11.K+5.1-<5.5mmol/LPatiromer4.2gBID*2.K+5.5-<6.5mmol/LPatiromer8.4gBID*Phase2^1.ContinuepatiromerdosefromPhase1*2.Placebo*titratedtoeffectbasedonprespecifiedalgorithmandbaseline^K+>5.5mmol/L@[email protected]<5.1mmol/LwhileonpatiromerandRAASinhibitors.
Demographics:Age:64yearsMen:58%Stage3CKD:46%Stage4CKD:45%T2DM:57%HF:42%HTN:97%K:5.6mmol/LKeyInclusionCriteria:-Age18-80years-Stage3-4CKD(eGFR15to<60mL/min)-K5.1to<6.5mmol/L(Phase1)and5.5to<6.5mmol/L(Phase2)-Stabledoseof>1RAASinhibitorfor>28daysKeyExclusionCriteria:-K-relatedECGchanges-SevereGIdisorders-Uncontrolledarrhythmias-ventriculararrhythmias-Recentcardiacsurgery-Renal/heart
Phase1ITT:1.922.151Completers:1.85(89.5%)2.134(88.7%)Phase2ITT:1.552.52Attrition:1.0(0.0%)2.1/52(1.9%)
Phase1MeanchangeinserumKleveltoweek4:bothgroups-1.0195%CI-1.07to-0.95p<0.001ProportionofpatientswithK3.8to<5.1mmol/Latweek4:76%(95%CI70-81%)Phase2DifferenceinmedianchangeinserumKlevel:1.0.72mmol/L2.0mmol/LDifference0.72mmol/L(95%CI0.46to0.99);p<0.0001 Proportionofpatientswithrecurrenthyperkalemia:1.8/55(15%,95%CI6-24%)2.31/52(60%,95%CI47-74%)p<0.001
N/AARR45.2%NNT3
Outcome:SupraventricularextrasystolesPatiromer:2(4%)Discontinuationsduetoadverseevents:N=10(groupnotspecified)
34 RiskofBias(high):SelectionBias:Centralrandomizationoccurred,onlypatientswhorespondedtopatiromerwereincludedforrandomizationPerformanceBias:single-blindeddesignDetectionBias:single-blindeddesignAttritionBias:42.3%ofpatientsinthephase2placebogroupdiscontinuedprematurely,mostcommonlyduetoelevatedpotassiumlevelsmeetingprespecifiedcriteriaReportingBias:allprimaryandsecondaryendpointswerereportedApplicability:Patient:Poorgeneralizabilityduetosignificantexclusioncriteriaandtheruninphaseallowedforonlyrespondersandthose
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
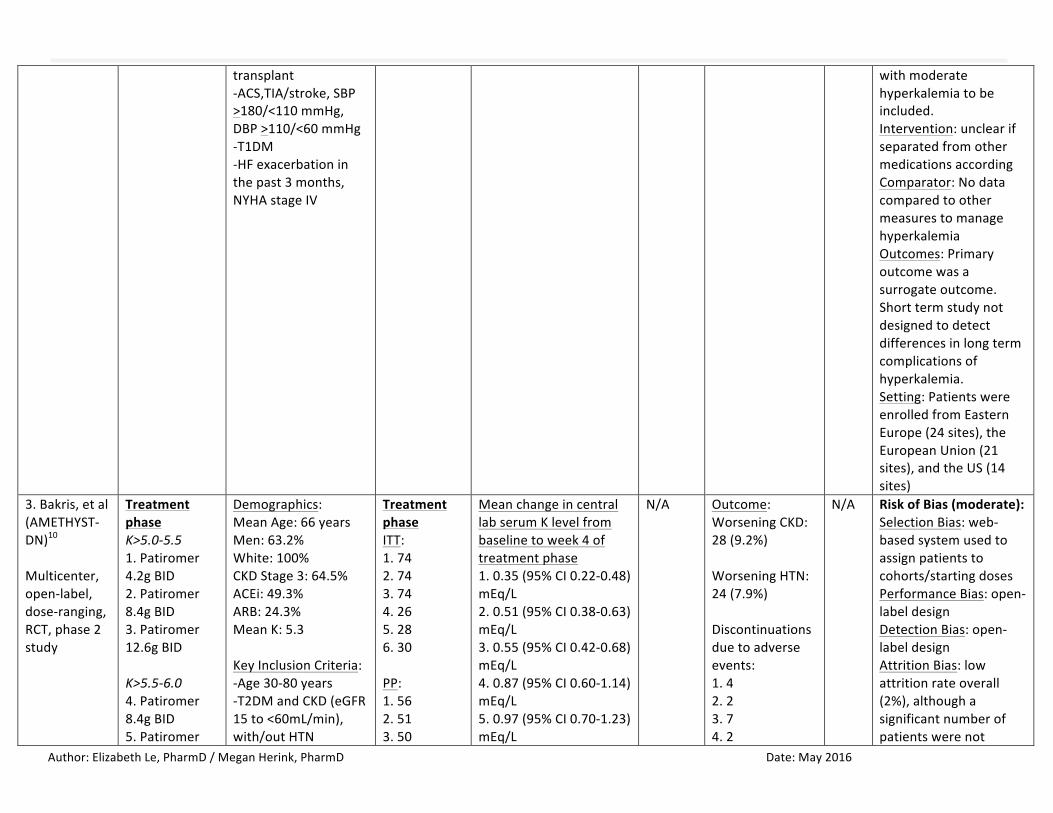
transplant-ACS,TIA/stroke,SBP>180/<110mmHg,DBP>110/<60mmHg-T1DM-HFexacerbationinthepast3months,NYHAstageIV
withmoderatehyperkalemiatobeincluded.Intervention:unclearifseparatedfromothermedicationsaccordingComparator:NodatacomparedtoothermeasurestomanagehyperkalemiaOutcomes:Primaryoutcomewasasurrogateoutcome.Shorttermstudynotdesignedtodetectdifferencesinlongtermcomplicationsofhyperkalemia.Setting:PatientswereenrolledfromEasternEurope(24sites),theEuropeanUnion(21sites),andtheUS(14sites)
3.Bakris,etal(AMETHYST-DN)10
Multicenter,open-label,dose-ranging,RCT,phase2study
TreatmentphaseK>5.0-5.51.Patiromer4.2gBID2.Patiromer8.4gBID3.Patiromer12.6gBIDK>5.5-6.04.Patiromer8.4gBID5.Patiromer
Demographics:MeanAge:66yearsMen:63.2%White:100%CKDStage3:64.5%ACEi:49.3%ARB:24.3%MeanK:5.3KeyInclusionCriteria:-Age30-80years-T2DMandCKD(eGFR15to<60mL/min),with/outHTN
TreatmentphaseITT:1.742.743.744.265.286.30PP:1.562.513.50
MeanchangeincentrallabserumKlevelfrombaselinetoweek4oftreatmentphase1.0.35(95%CI0.22-0.48)mEq/L2.0.51(95%CI0.38-0.63)mEq/L3.0.55(95%CI0.42-0.68)mEq/L4.0.87(95%CI0.60-1.14)mEq/L5.0.97(95%CI0.70-1.23)mEq/L
N/A Outcome:WorseningCKD:28(9.2%)WorseningHTN:24(7.9%)Discontinuationsduetoadverseevents:1.42.23.74.2
N/A RiskofBias(moderate):SelectionBias:web-basedsystemusedtoassignpatientstocohorts/startingdosesPerformanceBias:open-labeldesignDetectionBias:open-labeldesignAttritionBias:lowattritionrateoverall(2%),althoughasignificantnumberofpatientswerenot
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
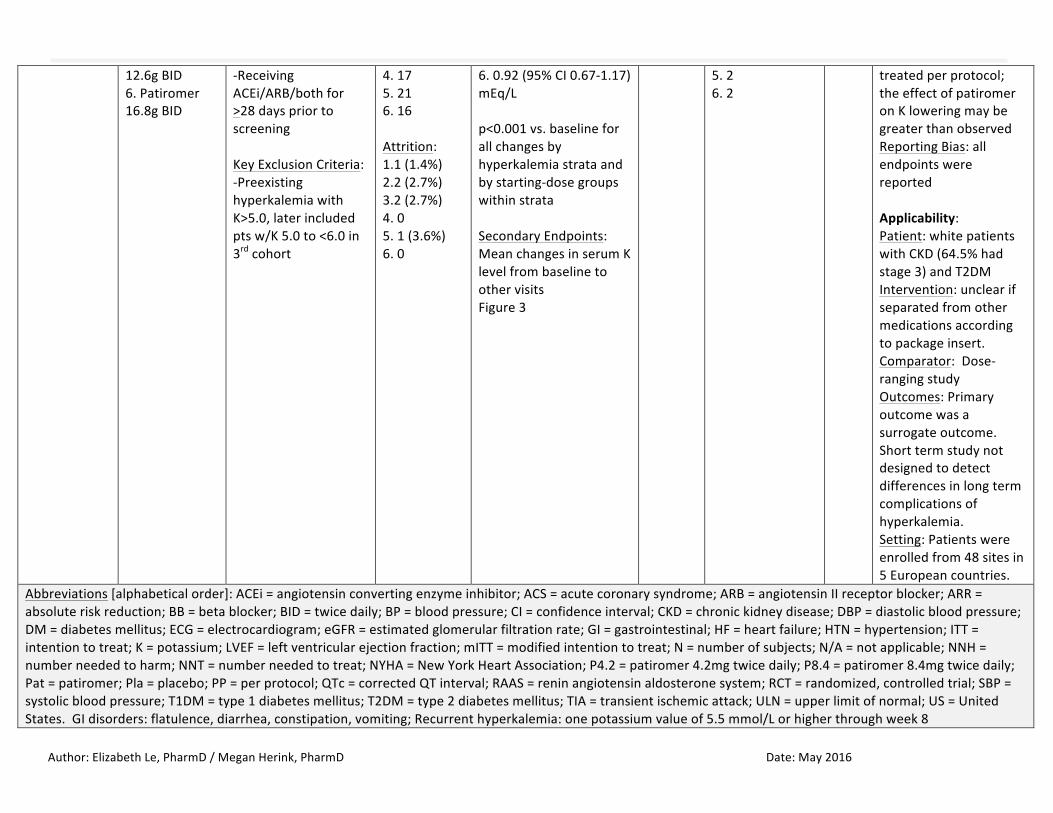
12.6gBID6.Patiromer16.8gBID
-ReceivingACEi/ARB/bothfor>28dayspriortoscreeningKeyExclusionCriteria:-PreexistinghyperkalemiawithK>5.0,laterincludedptsw/K5.0to<6.0in3rdcohort
4.175.216.16Attrition:1.1(1.4%)2.2(2.7%)3.2(2.7%)4.05.1(3.6%)6.0
6.0.92(95%CI0.67-1.17)mEq/Lp<0.001vs.baselineforallchangesbyhyperkalemiastrataandbystarting-dosegroupswithinstrataSecondaryEndpoints:MeanchangesinserumKlevelfrombaselinetoothervisitsFigure3
5.26.2
treatedperprotocol;theeffectofpatiromeronKloweringmaybegreaterthanobservedReportingBias:allendpointswerereportedApplicability:Patient:whitepatientswithCKD(64.5%hadstage3)andT2DMIntervention:unclearifseparatedfromothermedicationsaccordingtopackageinsert.Comparator:Dose-rangingstudyOutcomes:Primaryoutcomewasasurrogateoutcome.Shorttermstudynotdesignedtodetectdifferencesinlongtermcomplicationsofhyperkalemia.Setting:Patientswereenrolledfrom48sitesin5Europeancountries.
Abbreviations[alphabeticalorder]:ACEi=angiotensinconvertingenzymeinhibitor;ACS=acutecoronarysyndrome;ARB=angiotensinIIreceptorblocker;ARR=absoluteriskreduction;BB=betablocker;BID=twicedaily;BP=bloodpressure;CI=confidenceinterval;CKD=chronickidneydisease;DBP=diastolicbloodpressure;DM=diabetesmellitus;ECG=electrocardiogram;eGFR=estimatedglomerularfiltrationrate;GI=gastrointestinal;HF=heartfailure;HTN=hypertension;ITT=intentiontotreat;K=potassium;LVEF=leftventricularejectionfraction;mITT=modifiedintentiontotreat;N=numberofsubjects;N/A=notapplicable;NNH=numberneededtoharm;NNT=numberneededtotreat;NYHA=NewYorkHeartAssociation;P4.2=patiromer4.2mgtwicedaily;P8.4=patiromer8.4mgtwicedaily;Pat=patiromer;Pla=placebo;PP=perprotocol;QTc=correctedQTinterval;RAAS=reninangiotensinaldosteronesystem;RCT=randomized,controlledtrial;SBP=systolicbloodpressure;T1DM=type1diabetesmellitus;T2DM=type2diabetesmellitus;TIA=transientischemicattack;ULN=upperlimitofnormal;US=UnitedStates.GIdisorders:flatulence,diarrhea,constipation,vomiting;Recurrenthyperkalemia:onepotassiumvalueof5.5mmol/Lorhigherthroughweek8

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
References:
1. KovesdyCP.Managementofhyperkalemiainchronickidneydisease.NatRevNephrol.2014;10(11):653-662.2. IngelfingerJR.Aneweraforthetreatmentofhyperkalemia?NEnglJMed.2015;372:275-277.3. SegalA.PotassiumandDyskalemias.In:MountDB,SayeghMH,SinghAK,eds.CoreConceptsintheDisordersofFluid,ElectrolytesandAcid-Base
Balance.NewYork,NY:SpringerScience+BusinessMedia;2012.4. Hollander-RodriguezJC,CalvertJF.Hyperkalemia.AmFamPhysician.2006;73(2):283-290.5. UKRenalAssociation.Clinicalpracticeguidelines:Treatmentofacutehyperkalemiainadults.2014.Availableat:www.renal.org.6. ScherrL,OgdenDA,MeadAW,SpritzN,RubinAL.Managementofhyperkalemiawithacation-exchangeresin.NEnglJMed.1961;264:115-119.7. Veltassa®[packageinsert].RedwoodCity,CA:RelypsaInc;2015.8. PittB,AnkerSD,BushinskyDA,etal.EvaluationoftheefficacyandsafetyofRLY5016,apolymericpotassiumbinder,inadouble-blind,placebo-
controlledstudyinpatientswithchronicheartfailure(thePEARL-HF)trial.EurHeartJ.2011;32(7):820-828.doi:10.1093/eurheartj/ehq502.Epub2011Jan5.
9. YancyCW,JessupM,BozkurtB,etal.2013ACCF/AHAguidelineforthemanagementofheartfailure:areportoftheAmericanCollegeofCardiologyFoundation/AmericanHeartAssociationTaskForceonPracticeGuidelines.JAmCollCardiol.2013;62(16):e147-e239.
10. BakrisGL,PittB,WeirMR,etal.Effectofpatiromeronserumpotassiumlevelinpatientswithhyperkalemiaanddiabetickidneydisease:TheAMETHYST-DNrandomizedclinicaltrial.JAMA.2015;314(2):151-161.doi:10.1001/jama.2015.7446.
11. Supplementto:BakrisGL,PittB,WeirMR,etal.Effectofpatiromeronserumpotassiumlevelinpatientswithhyperkalemiaanddiabetickidneydisease:TheAMETHYST-DNrandomizedclinicaltrial.JAMA.2015;314(2):151-161.doi:10.1001/jama.2015.7446.
12. WeirMR,BakrisGL,BushinskyDAetal.PatiromerinpatientswithkidneydiseaseandhyperkalemiareceivingRAASinhibitors.NEnglJMed.2015;372(3):211-221.doi:10.1056/NEJMoa1410853.Epub2014Nov21.
13. Supplementto:WeirMR,BakrisGL,BushinskyDAetal.PatiromerinpatientswithkidneydiseaseandhyperkalemiareceivingRAASinhibitors.NEnglJMed.2015;372(3):211-221.doi:10.1056/NEJMoa1410853.Epub2014Nov21.
14. MicromedexHealthcareSeries[internetdatabase].GreenwoodVillage,CO:TruvenHealthAnalytics,Inc.UpdatedPeriodically.AccessedMarch17,2016.

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
Appendix1:HighlightsofPrescribingInformation7BlackBoxWarnings:NoneRiskEvaluationMitigationStrategies:NoneIndications:Hyperkalemia
- Limitations:Nottobeusedasanemergencytreatmentforlife-threateninghyperkalemiaduetoitsdelayedonsetofactionDosageandAdministration:Startingdose8.4gorallyoncedailywithfood
- Adjustdoseby8.4gdailyasneededatone-weekintervalstoobtaindesiredserumpotassiumtargetrange- Dosesofpatiromerinexcessof50.4g/dayhavenotbeentested.Excessivedosesofpatiromermayresultinhyperkalemia.Restoreserumpotassiumif
hypokalemiaoccursFormulations:Powderfororalsuspension(8.4,16.8,and25.2gpackets)
- ActiveIngredient:patiromersorbitexcalcium- InactiveIngredient:xanthangum
Contraindications:KnownhypersensitivitytopatiromeroranyofitscomponentsWarningsandPrecautions:
• Worseningofgastrointestinalmotility;useshouldbeavoidedinpatientswithsevereconstipation,bowelobstructionorimpaction,aspatiromermaybeineffectiveorworsengastrointenstinalmotility.
• Hypomagnesemia,;patiromerbindstomagnesiuminthecolonwhichcouldresultinhypomagnesmia.Thiswasreportedin5.4%ofpatientsinclinicaltrials.
• Bindingtootheroralmedications;patiromerbindstomanyorallyadministeredmedications,whichcoulddecreasetheirabsorptionandreducetheireffectiveness.Administerotheroralmedicationsatleast6hoursbeforeor6hoursafterpatiromer.
AdverseReactions:Common(incidence>2%):constipation,hypomagnesemia,diarrhea,nausea,abdominaldiscomfort,flatulenceDrugInteractions:Takeotherorallyadministereddrugsatleast6hoursbeforeorafterpatiromerUseinSpecificPopulations:
- Pregnancy:patiromerisnotabsorbedsystemicallyfollowingoraladministrationandmaternaluseisnotexpectedtoresultinfetalrisk.- Lactation:patiromerisnotabsorbedsystemicallybythemother,sobreastfeedingisnotexpectedtoresultinrisktotheinfant.- PediatricUse:safetyandefficacyinpediatricpatientshavenotbeenestablished
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
- GeriatricUse:ofthe666patientstreatedwithpatiromerinclinicalstudies,59.8%wereage65andover,and19.8%wereage75andover.Nooveralldifferencesineffectivenesswereobservedbetweenthesepatientsandyoungerpatients.Patientsage65andolderreportedmoregastrointestinaladversereactionsthanyoungerpatients.
- RenalImpairment:ofthe666patientstreatedwithpatiromerinclinicalstudies,93%hadchronickidneydisease(CKD).Nospecialdosingadjustmentsareneededforpatientswithrenalimpairment.
StorageandStability:Refrigerate.Mustbeusedwithin3monthsorbeingtakenoutoftherefrigerator
Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
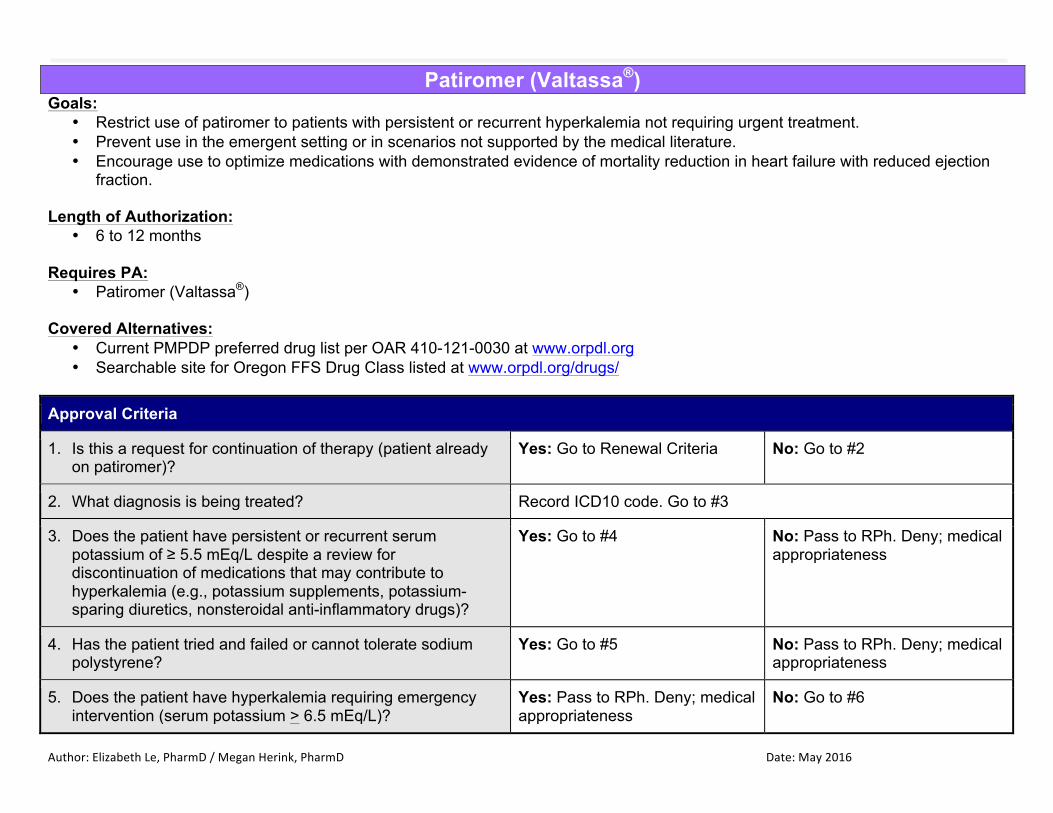
Patiromer (Valtassa®) Goals:
• Restrict use of patiromer to patients with persistent or recurrent hyperkalemia not requiring urgent treatment. • Prevent use in the emergent setting or in scenarios not supported by the medical literature. • Encourage use to optimize medications with demonstrated evidence of mortality reduction in heart failure with reduced ejection
fraction. Length of Authorization:
• 6 to 12 months Requires PA:
• Patiromer (Valtassa®) Covered Alternatives:
• Current PMPDP preferred drug list per OAR 410-121-0030 at www.orpdl.org • Searchable site for Oregon FFS Drug Class listed at www.orpdl.org/drugs/
Approval Criteria
1. Is this a request for continuation of therapy (patient already on patiromer)?
Yes: Go to Renewal Criteria No: Go to #2
2. What diagnosis is being treated? Record ICD10 code. Go to #3
3. Does the patient have persistent or recurrent serum potassium of ≥ 5.5 mEq/L despite a review for discontinuation of medications that may contribute to hyperkalemia (e.g., potassium supplements, potassium-sparing diuretics, nonsteroidal anti-inflammatory drugs)?
Yes: Go to #4 No: Pass to RPh. Deny; medical appropriateness
4. Has the patient tried and failed or cannot tolerate sodium polystyrene?
Yes: Go to #5 No: Pass to RPh. Deny; medical appropriateness
5. Does the patient have hyperkalemia requiring emergency intervention (serum potassium > 6.5 mEq/L)?
Yes: Pass to RPh. Deny; medical appropriateness
No: Go to #6

Author:ElizabethLe,PharmD/MeganHerink,PharmD Date:May2016
Approval Criteria
6. Does the patient have hypomagnesemia (serum magnesium < 1.4 mg/dL)?
Yes: Pass to RPh. Deny; medical appropriateness
No: Go to #7
7. Does the patient have a severe GI disorder (i.e., major GI surgery (e.g., large bowel resection), bowel obstruction/impaction, swallowing disorders, gastroparesis, severe constipation)?
Yes: Pass to RPh. Deny; medical appropriateness
No: Approve up to 6 months
Renewal Criteria
1. Is the patient’s potassium level < 5.1 mEq/L and has this decreased by at least 0.35 mEq/L from baseline?
Yes: Approve for up to 12 months
No: Pass to RPh. Deny; medical appropriateness
Clinical Considerations: -Monitoring
-Monitor potassium at baseline and at each dose titration (weekly for first 8 weeks, then monthly thereafter). -Hypomagnesemia was reported in 9% of patients in clinical trials. Monitor serum magnesium every 2 weeks for 2 months, then monthly thereafter. Consider magnesium supplementation or risk vs. benefit of continued treatment with patiromer.
-Administration -It is recommended to administer other oral medications at least 6 hours before or 6 hours after patiromer, due to the potential binding of patiromer to other orally administered medications.
-Administer patiromer with food. Do not heat or add heated foods/liquids. Do not take patiromer in its dry form -Prepare each dose immediately prior to administration following the steps below: -1): Add about 1 ounce (30 mL) of water to an empty glass or cup -2): Empty the entire contents of the packet(s) into the glass or cup -3): Stir the mixture thoroughly -4): Add an additional 2 ounces (60 mL) of water to the glass or cup -5): Stir the mixture thoroughly; the powder will not dissolve and the mixture will look cloudy
-6): Drink the mixture immediately. If some powder remains in the glass after drinking, add more water, stir, and drink immediately. Repeat as needed to ensure the entire dose is administered
P&T / DUR Review: 05/16 (EL/MH) Implementation: TBD
Top Related