







γλώσσες
Σελίδες
Νομικός


1
CVI05513-11 REVISED VERSION (2) 1
Performance of the QuantiFERON®-cytomegalovirus (CMV) Assay for Detecting 2
and Estimating the Magnitude and Functionality of the CMV-Specific IFN-γ CD8+ 3
T-Cell Response in Allogeneic Stem Cell Transplant Recipients 4
María Ángeles Clari,1† Beatriz Muñoz-Cobo,1† Carlos Solano,2,3 Isabel Benet,2,3 Elisa 5
Costa,1 María José Remigia,2 Dayana Bravo,1 Paula Amat,2 and David Navarro1,4* 6
7
1Microbiology Service Hospital Clínico Universitario, Valencia, Spain; 2Hematology 8
and Medical Oncology Service, Hospital Clínico Universitario, Valencia, Spain; 9
3Department of Medicine, School of Medicine, University of Valencia, Valencia, Spain; 10
4Department of Microbiology, School of Medicine, University of Valencia, Valencia, 11
Spain. 12
*Correspondence: David Navarro, Microbiology Service, Hospital Clínico 13
Universitario, and Department of Microbiology, School of Medicine, Av. Blasco Ibáñez 14
17, 46010 Valencia, Spain. Phone: 34(96)3864657; Fax: 34(96)3864173; E-mail: 15
david.navarro@uv. 16
†These authors contributed equally to the present work 17
RUNNING TITLE: QuantiFERON®-CMV assay for evaluating CMV-specific CD8+ 18
T-cell immunity 19
20
21
22
23
Copyright © 2012, American Society for Microbiology. All Rights Reserved.Clin. Vaccine Immunol. doi:10.1128/CVI.05633-11 CVI Accepts, published online ahead of print on 29 February 2012
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

2
ABSTRACT 24
The performance of the QuantiFERON®-cytomegalovirus (CMV) assay was compared 25
to that of a flow-cytometry intracellular cytokine staining method (ICS) for detecting 26
CMV-specific IFN-γ-producing CD8+ T-cell responses in allogeneic stem cell 27
transplant recipients (allo-SCT) and for estimating their magnitude and functionality. A 28
total of 90 whole blood specimens from 23 allo-SCT recipients was analyzed by both 29
methods. Overall, the percentage of specimens that yielded concordant results by both 30
methods was 68.8% (κ=0.691; 95% CI 0.548-0.835), and the sensitivity of the 31
QuantiFERON®-CMV assay for detecting positive IFN-γ T-cell responses (>0.2 32
UI/mL), taking the ICS method as the reference, was 76.3%. The magnitude of IFN-γ 33
CD8+ T-cell responses to CMV-specific peptides measured with the QuantiFERON®-34
CMV assay correlated significantly (σ=0.695; P=<0.001) with that of the total IFN-γ 35
CD8+ T cells, functional dual (IFN-γ/TNF-α, σ=0.652; P=<0.001, and IFN-γ/CD107a, 36
σ=0.690; P=<0.001) and trifunctional (IFN-γ/TNF-α/CD107a; σ=0.679; P=>0.001) 37
CMV-specific CD8+ T-cell responses as quantitated by ICS. In summary, the data 38
indicated that the QuantiFERON®-CMV assay is less sensitive than the ICS method for 39
detecting CMV-specific IFN-γ CD8+ T-cell responses in the allo-SCT setting; 40
Nevertheless, it allowed the estimation of the total and polyfunctional CMV-specific 41
IFN-γ CD8+ T-cell responses in specimens testing positive by both methods. 42
43
KEY WORDS: Cytomegalovirus, QuantiFERON®-CMV assay, Intracellular cytokine 44
staining, CMV-specific IFN-γ-producing CD8+ T-cell response, allogeneic stem cell 45
transplantation. 46
47
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

3
INTRODUCTION 48
The assessment of the magnitude and the functionality of T-cell immunity against 49
cytomegalovirus (CMV) is emerging as a clinically useful tool for the therapeutic 50
management of CMV infection in the allogeneic stem cell transplantation setting (allo-51
SCT) (7,13). Monitoring CMV-specific CD8+ or CD4+ T-cell responses may allow for 52
the optimization of pre-emptive antiviral therapy regimens on an individual basis and 53
the identification of patients who may benefit from prophylactic antiviral or adoptive T-54
cell transfer therapeutic strategies (1,7,13). In recent years, several methods have been 55
developed for the ex vivo quantitation and functional characterization of T-cell 56
responses, among which flow cytometry for surface immunophenotyping and 57
intracellular cytokine staining (ICS) is currently considered the “gold standard” (13). 58
The QuantiFERON®-CMV assay (Cellestis Ltd., Melbourne, Australia) is a 59
commercially available test that allows the inference of the size of the CMV-specific T-60
cell response by quantitating the level of IFN-γ, mostly produced by CMV-specific 61
CD8+ T cells, upon the stimulation of whole blood with a number of immunogenic 62
peptides mapped within IE-1, IE-2, pp65, pp50, and gB and restricted by several 63
widespread HLA-I haplotypes (17). The performance of the QuantiFERON®-CMV 64
assay has been mostly assessed in the solid organ transplant (SOT) setting (see 4 for 65
review). Recently published data, although preliminary, lend support to the suitability of 66
the QuantiFERON®-CMV assay for monitoring the CMV-specific IFN-γ-producing 67
CD8+ T-cell response in allo-SCT recipients (2). Nevertheless, it is largely unknown 68
how this method compares to ICS assays for such purpose. In previous studies we 69
reported on the development and clinical utility of an ICS assay for the quantitation of 70
CMV-specific IFN-γ-producing CD8+ and CD4+ T cells (11,12,14-16). The assay was 71
found to reliably predict protection from the development of CMV DNAemia in allo-72
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

4
SCT recipients, and it has recently been used in the setting of a novel strategy for the 73
guidance of pre-emptive antiviral therapy based on combined virological and 74
immunological monitoring (12). In the current study, we compared the performance of 75
the QuantiFERON®-CMV assay with that of our ICS method for detecting and 76
quantitating CMV-specific IFN-γ-producing CD8+ T-cell responses in allo-SCT 77
recipients. 78
MATERIAL AND METHODS 79
Patients and specimens. A total of 90 whole blood samples obtained from 23 non-80
consecutive patients (median age, 53 years; range, 20 to 71 years old; 16 males and 7 81
females) who underwent peripheral blood (n=20) or umbilical cord blood (n=3) allo-82
SCT at the Hospital Clínico Universitario of Valencia between February 2010 and June 83
2011 were analyzed in this study. The underlying diseases of the patients were myeloid 84
acute leukemia (n=10), non-Hodgkin’s lymphoma (n=7), chronic lymphocytic leukemia 85
(n=2), multiple myeloma (n=2), or myelodysplastic syndrome (n=1). The types of 86
transplant were related/matched (n=10), unrelated/matched (n=9), 87
unrelated/mismatched (n=3), and related/mismatched (n=1). The conditioning regimen 88
was non-myeloablative (n=17) or myeloablative (n=6), and the paired CMV serostatus 89
of the donors (D) and recipients R) was: D+/R+ (n=9), D-/R+ (n=9), D+/R- (n=2) and 90
D-/R- (n=3). The study was approved by the Ethics Committees. All patients gave their 91
informed consent to participate in the study. 92
CMV serology. The CMV serological testing of the donors and recipients was 93
performed using the DiaSorin LIAISON® CMV IgG assay (DiaSorin, Saluggia, Italy), 94
following the recommendations of the manufacturer. 95
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

5
CMV plasma DNAemia quantitation. The CMV DNA load in the plasma was 96
quantitated by real-time PCR (Abbott CMV PCR Kit, produced by Qiagen GmbH, 97
Hilde, Germany for Abbott diagnostics, DesPlaines, Illinois, USA). The PCR reactions 98
were performed using the m2000RT system (Abbott Molecular, Illinois, USA), as 99
previously described (3). The DNA extractions were performed using 500 µL of plasma 100
on the m24 SP instrument (Abbott Diagnostics, Illinois, USA). 101
Enumeration of CMV-specific IFN-γ-producing CD8+ T-cells. Quantitation of the 102
total number of CMV-specific IFN-γ-producing CD8+ T cells, and selectively 103
bifunctional (IFN-γ/TNF-α, IFN-γ/CD107a) and trifunctional (IFN-γ/TNF-α/CD107a) 104
CMV-specific IFN-γ-producing CD8+ T cells was performed by ICS. Whole blood (0.5 105
mL) was simultaneously stimulated with two sets of 15-mer overlapping peptides 106
encompassing the sequence of the pp65 and IE-1 CMV proteins (1 μg/mL/peptide), 107
obtained from JPT peptide Technologies GmbH (Berlin, Germany), in the presence of 1 108
μg/mL of co-stimulatory mAbs to CD28 and CD49d, an anti-CD107a mAb coupled 109
with APC, brefeldin (5 µg/mL), and monensin (1 µM) for 6 h at 37 ºC. The cells were 110
washed in PBS-2% FCS, lysed in BD FACS lysis solution, stained with surface markers 111
(anti-CD8-PerCP-Cy5-5 and anti-CD3-APC-Cy7), permeabilized (BD FACS 112
Permeabilizing solution 2), washed, and finally stained for intracellular cytokines (anti-113
IFN-γ-FITC and anti-TNF-α-PE). All antibodies and solutions were purchased from 114
Becton Dickinson (San Jose, CA, USA). The cells were stored at 4 ºC in PBS-1% 115
formaldehyde, acquired within 4 h in a BD FCSCantoII flow cytometer (BD 116
Biosciences Immunocytometry Systems, San Jose, CA) and analyzed with the software 117
program Infinicyt (Cytognos, Salamanca, Spain). The negative controls (absence of 118
peptide stimulation) were processed in parallel for all experiments. The total number of 119
each CD8+ T-cell subpopulation was calculated by multiplying the corresponding 120
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

6
percentage of CMV-specific T cells (after background subtraction) by the absolute 121
number of CD8+ T cells. Specific responses were considered as those that were >0.1% 122
for each population. The CMV-specific IFN-γ-producing CD8+ T cells were enumerated 123
in parallel using the BD Fastimmune kit (BD-Beckton Dickinson and Company-124
Biosciences, San Jose, CA, USA) as previously described (11,12,14-16), but employing 125
the BD FCSCantoII flow cytometer and the software program Infinicyt for the analyses. 126
The levels of IFN-γ-producing CD8+ T cells (total number) measured by the two 127
abovementioned procedures were comparable (data not shown). 128
QuantiFERON®-CMV assay. The QuantiFERON®-CMV assay (Cellestis Ltd. 129
Melboure Australia) was performed according to the manufacturer’s instructions. 130
Briefly, 1 mL aliquots of heparinized whole blood were collected in three 131
QuantiFERON® CMV collection tubes, one containing a number of CMV 132
immunogenic peptides (CMV antigen), another with no peptides (nil control), and the 133
other one containing a polyclonal stimulating antigen (phytohemagglutinin) (mitogen 134
control). The tubes were shaken vigorously for 5 s and then incubated for 18-24 h at 37 135
ºC. The supernatants were then harvested and the levels of IFN-γ were measured by 136
ELISA. A standard curve was generated in each run. The results of the assay were 137
interpreted according to the criteria established by the manufacturers: (i) <0.2 IU/mL 138
(CMV minus Nil) and ≥0.5 IU/mL (mitogen minus nil)-non-reactive-; (ii) ≥0.2 IU/mL 139
(CMV minus nil) and any value of mitogen minus nil-reactive-; (iii) <0.2 IU/mL (CMV 140
minus nil) and <0.5 IU/mL (mitogen minus nil)-indeterminate. According to the 141
manufacturer, indeterminate results are not interpretable. 142
Statistical analysis. The data were analyzed with the aid of the statistical package 143
SPSS version 17.0 (SPSS, North Chicago, IL). Differences between the medians were 144
compared using the Mann-Whitney U test. The Spearman’s rank test was used to 145
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

7
analyze correlations between continuous variables. Two-sided exact P values are 146
reported. A P value < 0.05 was considered statistically significant. 147
RESULTS 148
A total of 90 blood samples from 23 allo-SCT recipients were analyzed by ICS and by 149
the QuantiFERON®-CMV assay. The data are summarized in Table 1. Fifty-five 150
samples (61.1%) from 17 patients had detectable CMV-specific IFN-γ-producing CD8+ 151
T-cell responses by ICS; of these, 42 (76.3%) from 13 patients were reactive (>0.2 152
UI/mL), and 13 (from 4 patients) yielded negative (n=10) or indeterminate (n=3) 153
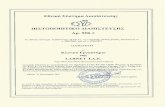
results in the QuantiFERON®-CMV assay. As shown in Figure 1, specimens testing 154
positive in the QuantiFERON®-CMV assay displayed significantly higher (P=0.001) 155
numbers of CMV-specific IFN-γ-producing CD8+ T cells, as measured by ICS, than 156
those that tested negative or indeterminate. As shown in Table 1, 35 specimens from six 157
patients lacked detectable CMV-specific IFN-γ-producing CD8+ T-cell responses, as 158
determined by ICS. Of these, only one sample yielded a positive result in the 159
QuantiFERON®-CMV assay (2.5 IU/mL). All patients (and/or their donors) with 160
negative results in the QuantiFERON®-CMV assays throughout the study period 161
displayed at least one HLA-I specificity able to present one of the immunogenic 162
peptides included in the QuantiFERON®-CMV assay pool (data not shown). A large 163
number of specimens gave indeterminate results in the QuantiFERON®-CMV assay 164
(n=17; 18.8%); most of these samples (n=14) had no detectable CMV-specific IFN-γ-165
producing CD8+ T-cell responses, as measured by ICS. Overall, the percentage of 166
specimens that yielded concordant results by both methods was 68.8% (κ=0.691; 95% 167
CI 0.548-0.835), and the sensitivity of the QuantiFERON®-CMV assay for detecting 168
positive IFN-γ T-cell responses, as determined by ICS, was 76.3%. Three specimens 169
that tested positive in the ICS assay displayed IFN-γ levels within the range of >0.1-170
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

8
<0.2 IU/mL in the QuantiFERON®-CMV assay. Thus, decreasing the cut-off level for a 171
positive result to >0.1 IU/mL resulted in a slight increase in the sensitivity of the 172
QuantiFERON®-CMV assay (81.8%). Of note was the fact that 15 out of the 42 173
specimens that tested positive in the QuantiFERON®-CMV assay gave optical density 174
values above the upper limit of quantification of the assay, and thus had to be further 175
diluted in order to determine precisely the levels of IFN-γ. 176
We next assessed to what extent the QuantiFERON®-CMV assay allowed the size 177
and functional diversity estimation of CMV-specific IFN-γ-producing CD8+ T-cell 178
responses as determined by ICS. For this, we performed a correlation analysis of the 179
levels of IFN-γ measured in the QuantiFERON®-CMV assay with the number of 180
different functional populations of IFN-γ-producing CD8+ T cells quantitated in the ICS 181
assay for 42 specimens that showed detectable responses by both methods. It is of note 182
that 20 out of these 42 specimens were obtained during episodes of non-treated (n=11 183
from 3 patients) or ganciclovir-treated (n=9 from 2 patients) CMV plasma DNAemia. In 184
addition, the remaining 22 specimens were obtained from eight patients who had a prior 185
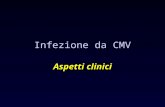
episode of CMV DNAemia. As shown in Figure 2, the magnitude of IFN-γ responses to 186
the CMV-specific peptides measured with the QuantiFERON®-CMV assay significantly 187
correlated (σ=0.695; P=<0.0001) with that quantitated by ICS for the total IFN-γ-188
producing CD8+ T cells. Furthermore, the IFN-γ levels determined by the 189
QuantiFERON®-CMV assay also significantly correlated with the number of functional 190
dual (IFN-γ/TNF-α, σ=0.652; P=<0.001, and IFN-γ/CD107a, σ=0.690; P=<0.0001) and 191
trifunctional (IFN-γ/TNF-α/CD107a; σ=0.679; P=<0.0001) CMV-specific CD8+ T cells. 192
193
194
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

9
DISCUSSION 195
The QuantiFERON®-CMV assay is the only commercially available method for 196
measuring CMV-specific IFN-γ-producing CD8+ T-cell responses. This assay has 197
previously been evaluated in SOT and allo-SCT recipients (2,4,5,8,10,17,18). 198
Preliminary data supported the clinical utility of this method for assessing the risk of 199
late-onset CMV end-organ disease in SOT recipients (5) and for predicting the 200
occurrence of CMV DNAemia in allo-SCT patients (2). Nevertheless, information on 201
how the QuantiFERON®-CMV assay correlates with ICS methods for estimating the 202
magnitude and assessing the functionality of CMV-specific CD8+ T-cell responses in 203
transplant recipients is still scarce. In the current study, we compared the performance 204
of the QuantiFERON®-CMV assay with that of an ICS method developed by our group 205
that has been proven to be clinically useful in the management of active CMV infection 206
in the allo-SCT setting (11,12,14-16). Overall, we found both methods to yield 207
concordant qualitative results in around 70% of specimens. This finding was not 208
entirely unexpected as 18 out of the 21 peptides included in the CMV tube of the 209
QuantiFERON®-CMV assay map within pp65 (n=15) and IE-1 (n=3). When the results 210
in QuantiFERON®-CMV assay were interpreted as indicated by the manufacturers 211
(positive responses if IFN-γ levels >0.2 UI/mL), the sensitivity of the assay, considering 212
the ICS method as the reference assay, was 76.37%. The sensitivity of the assay slightly 213
improved (81.8%) when the cut-off threshold for positive IFN-γ responses was lowered 214
to 0.1 UI/mL, as previously suggested (5). All patients (and/or their donors) who tested 215
negative in the QuantiFERON®-CMV assay throughout the study period displayed at 216
least one HLA-I variant included among the specificities covered by the test. The 217
specificity of the QuantiFERON®-CMV assay approached 100%. In fact, there was only 218
one specimen that gave a positive result in the QuantiFERON®-CMV assay (2.5 IU/mL) 219
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

10
but which tested negative using the ICS method; this could have been a false positive 220
result, since a follow-up specimen of the same patient obtained 3 days later tested 221
negative in both assays. The QuantiFERON®-CMV assay gave a large number of 222
indeterminate results. This observation is in keeping with previously published data (2). 223
Most of the specimens that yielded indeterminate results (14 out of 17), and those that 224
tested negative, had undetectable CMV-specific IFN-γ-producing CD8+ T-cell 225
responses as measured by ICS. 226
The levels of IFN-γ measured in the QuantiFERON®-CMV assay were found to 227
correlate significantly with the total number of CMV-specific IFN-γ-producing CD8+ T 228
cells quantitated in the ICS assay. This observation is in accordance with the data 229
reported in a recently published study in which the QuantiFERON®-CMV assay was 230
compared to an ICS method using a library of CMV peptides mapped within pp65 as 231
the stimulating antigen (2). 232
Recent data seem to favor the idea that polyfunctional rather than monofunctional 233
CMV-specific CD8+ T cells, in particular those with the ability to produce cytokines 234
with antiviral properties such as IFN-γ and TNF-α and to simultaneously display 235
cytotoxic activity (cells expressing CD107a), are crucial in the protection from and 236
resolution of episodes of active CMV infection in the allo-SCT setting (6,10,19). The 237
QuantiFERON®-CMV assay cannot distinguish between different functional CD8+ T-238
cell populations producing IFN-γ in response to CMV replication. In this context, we 239
were interested to assess to what extent the QuantiFERON®-CMV assay could allow 240
the estimation of levels of CMV-specific polyfunctional IFN-γ-producing CD8+ T cells. 241
We found that IFN-γ levels determined by the QuantiFERON®-CMV assay 242
significantly correlated with the number of CMV-specific functional dual (IFN-γ/TNF-243
α, and IFN-γ/CD107a) and trifunctional (IFN-γ/TNF-α/CD107a) CD8+ T cells. It should 244
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

11
be stressed that the above correlations were observed in a very precise virological 245
setting, i.e., in patients with an ongoing episode of active CMV infection or in patients 246
who had recently resolved an episode of CMV DNAemia. In this context, we observed 247
that the expansion and contraction of monofunctional and polyfunctional CMV-specific 248
IFN-γ-producing CD8+ T-cell responses elicited by CMV replication followed different 249
kinetic patterns and also showed wide variations on an individual basis (9). It is thus 250
likely that the ability of the QuantiFERON®-CMV assay to accurately estimate the size 251
of CMV-specific polyfunctional IFN-γ-producing CD8+ T-cell responses may 252
ultimately depend upon the past and current status of CMV replication. The current 253
study has two main limitations; First, both assays are not entirely comparable, as they 254
are of distinct nature and, most importantly, employ different stimulating antigens (see 255
Table 2); Second, the ICS method taken as the reference standard for measuring CMV-256
specific CD8+ T-cell responses in the current study lacked extensive inter-laboratory 257
validation. Despite these limitations, we are convinced that studies comparing the 258
performance of QuantiFERON®-CMV assay with that of ICS methods with proven 259
reliability to assess and quantitate CMV-specific IFN-γ-producing CD8+ T-cell 260
responses conferring protection against CMV infection are of major clinical interest. 261
Table 2 summarizes the characteristics, advantages and limitations of the 262
QuantiFERON®-CMV assay and the ICS method developed by our group. In summary, 263
the data presented herein indicated that the QuantiFERON®-CMV assay, although less 264
sensitive than our ICS method, allowed the estimation of total and polyfunctional CMV-265
specific IFN-γ-producing CD8+ T-cell-responses in specimens testing positive by both 266
methods. We wonder whether the use of overlapping pp65 and IE-1 peptide pools in the 267
QuantiFERON®-CMV assay instead of a mix of immunogenic CMV peptides would 268
increase the sensitivity of the method. Further studies should be undertaken to confirm 269
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

12
our observations, and most importantly to assess the clinical utility of the 270
QuantiFERON®-CMV assay in this setting; In this context, it seems essential to 271
establish threshold levels of IFN-γ associated with protection from or the resolution of 272
episodes of active CMV infection and CMV end-organ disease. 273
ACKNOWLEDGMENTS 274
We thank Matilde Pastor and Amanda Mataix for their technical assistance. This 275
research study was supported by a grant (09/1117) from FIS (Fondo de Investigaciones 276
Sanitarias, Ministerio de Sanidad y Consumo, Spain). The QuantiFERON®-CMV assay 277
reagents were kindly provided by Alere (Barcelona, Spain). 278
REFERENCES 279
1. Avetisyan, G., J. Aschan, H. Hägglund, O. Ringdén, and P. Ljungman. 280
2007. Evaluation of intervention strategy based on CMV-specific immune 281
responses after allogeneic SCT. Bone Marrow Transplant. 40:865-869. 282
2. Fleming, T., J. Dunne, and B. Crowley. 2010. Ex vivo monitoring of human 283
cytomegalovirus-specific CD8(+) T-Cell responses using the QuantiFERON-284
CMV assay in allogeneic hematopoietic stem cell transplant recipients attending 285
an Irish hospital. J. Med. Virol. 82:433-440 286
3. Gimeno, C., C. Solano, J.C. Latorre, J.C. Hernández-Boluda, M.A. Clari, 287
M.J. Remigia, S. Furió, M. Calabuig, N. Tormo, and D. Navarro. 2008. 288
Quantification of DNA in plasma by an automated real-time PCR assay 289
(cytomegalovirus PCR kit) for surveillance of active cytomegalovirus infection 290
and guidance of preemptive therapy for allogeneic hematopoietic stem cell 291
transplant recipients. J. Clin. Microbiol. 46:3311-3318. 292
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

13
4. Giulieri, S., and O. Manuel. 2011. QuantiFERON®-CMV assay for the 293
assessment of cytomegalovirus cell-mediated immunity. Expert Rev. Mol. 294
Diagn. 11:17-25. 295
5. Kumar, D., S. Chernenko, G. Moussa, I. Cobos, O. Manuel, J. Preiksaitis, S. 296
Venkataraman, and A. Humar. 2009. A. Cell-mediated immunity to predict 297
cytomegalovirus disease in high-risk solid organ transplant recipients. Am. J. 298
Transplant. 9:1214-1222. 299
6. Lacey, S., C. La Rosa, W. Zhou, M.C. Sharma, J. Martinez, A. Krishnan, G. 300
Gallez-Hawkins, L. Thao, J. Longmate, R. Spielberger, S.J. Forman, A. 301
Limaye, J.A. Zaia, and D.J. Diamond. 2006. Functional comparison of T cells 302
recognizing cytomegalovirus pp65 and immediate-early antigen polypeptides in 303
hematopoietic stem-cell transplant and solid organ transplant recipients. J. Infect. 304
Dis. 194:1410-1421. 305
7. Ljungman P. 2006. Would monitoring CMV immune responses allow 306
improved control of CMV in stem cell transplant patients. J. Clin. Virol. 307
35:493-495. 308
8. Lochmanova, A., I. Lochman, H. Tomaskova, P. Marsalkova, J. Raszka, J. 309
Mrazek, J. Dedochova, A. Martinek, and H. Brozmanova. 2010. 310
Quantiferon-CMV test in prediction of cytomegalovirus infection after kidney 311
transplantation. Transplant. Proc. 42:3574-3577. 312
9. Muñoz-Cobo, B., C. Solano, I. Benet, E. Costa, M.J. Remigia, R. de la 313
Cámara, J. Nieto, J. López, P. Amat, A. Garcia-Noblejas, D. Bravo, M.A. 314
Clari, and D. Navarro. 2011. Functional profile of cytomegalovirus (CMV)-315
specific CD8+ T cells and kinetics of NKG2C+ NK cells associated with the 316
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

14
resolution of CMV DNAemia in allogeneic stem cell transplant recipients.317
J.Med.Virol., in press. 318
10. Nebbia, G., F.M. Mattes, C. Smith, E. Hainsworth, J. Kopycinski, A. 319
Burroughs, P.D. Griffiths, P. Klenerman, and V.C. Emery. 2008. 320
Polyfunctional cytomegalovirus-specific CD4+ and pp65 CD8+ T cells protect 321
against high-level replication after liver transplantation. Am. J. Transplant. 322
8:2590-2599. 323
11. Solano, C., I. Benet, M.A. Clari, J. Nieto, R. de la Cámara, J. López, J.C. 324
Hernández-Boluda, M.J. Remigia, I. Jarque, M.L. Calabuig, A. Garcia-325
Noblejas, J. Alberola, A. Tamarit, C. Gimeno, and D. Navarro. 2008. 326
Enumeration of cytomegalovirus-specific interferongamma CD8+ and CD4+ T 327
cells early after allogeneic stem cell transplantation may identify patients at risk 328
of active cytomegalovirus infection. Haematologica. 93:1434-1436. 329
12. Solano, C., I. Benet, M.J. Remigia, R. de la Cámara, B. Muñoz-Cobo, E. 330
Costa, M.A. Clari, D. Bravo, P. Amat, and D. Navarro. 2011. Immunological 331
monitoring for guidance of preemptive antiviral therapy for active 332
cytomegalovirus infection in allogeneic stem-cell transplant recipients: a pilot 333
experience. Transplantation. 92:e17-20 334
13. Solano, C., and D. Navarro. 2010. Clinical virology of cytomegalovirus 335
infection following hematopoietic transplantation. Future Virol. 5:111-24. 336
14. Tormo, N., C. Solano, I. Benet, J. Nieto, R. de la Cámara, J. López, A. 337
Garcia-Noblejas, B. Muñoz-Cobo, E. Costa, M.A. Clari, J.C. Hernández-338
Boluda, M.J. Remigia, and D. Navarro. 2011. Reconstitution of CMV pp65 339
and IE-1-specific IFN-γ CD8(+) and CD4(+) T-cell responses affording 340
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

15
protection from CMV DNAemia following allogeneic hematopoietic SCT. Bone 341
Marrow Transplant. Jan 17. [Epub ahead of print]. 342
15. Tormo, N., C. Solano, I. Benet, M.A. Clari, J. Nieto, R. de la Cámara, J. 343
López, N. López-Aldeguer, J.C. Hernández-Boluda, M.J. Remigia, A. 344
Garcia-Noblejas, C. Gimeno, and D. Navarro. 2010. Lack of prompt 345
expansion of cytomegalovirus pp65 and IE-1-specific IFNgamma CD8+ and 346
CD4+ T cells is associated with rising levels of pp65 antigenemia and DNAemia 347
during pre-emptive therapy in allogeneic hematopoietic stem cell transplant 348
recipients. Bone Marrow Transplant. 45:543-549. 349
16. Tormo, N., C. Solano, I. Benet, J. Nieto, R. de la Cámara, A. Garcia-350
Noblejas, M.A. Clari, M. Chilet, J. López, J.C. Hernández-Boluda, M.J. 351
Remigia, and D. Navarro. 2010. Kinetics of cytomegalovirus (CMV) pp65 and 352
IE-1-specific IFNgamma CD8+ and CD4+ T cells during episodes of viral 353
DNAemia in allogeneic stem cell transplant recipients: potential implications for 354
the management of active CMV infection. J. Med. Virol. 82:1208-1215. 355
17. Walker, S., C. Fazou, T. Crough, R. Holdsworth. P. Kiely, M. Veale, S. Bell, 356
A. Gailbraith, K. McNeil, S. Jones, and R. Khanna. 2007. Ex vivo monitoring 357
of human cytomegalovirus-specific CD8+ T-cell responses using 358
QuantiFERON-CMV. Transpl. Infect. Dis. 9:165-170. 359
18. Westall, G.P., N.A. Mifsud, and T. Kotsimbos. 2008. Linking CMV serostatus 360
to episodes of CMV reactivation following lung transplantation by measuring 361
CMV-specific CD8+ T-cell immunity. Am. J. Transplant. 8:1749-1754. 362
19. Zhou, W., J. Longmate, S.F. Lacey, J.M. Palmer, G.Gallez-Hawkins, 363
L.Thao, R. Spielberger, R. Nakamura, S.J. Forman, J.A. Zaia, and D.J. 364
Diamond. 2009. Impact of donor CMV status on viral infection and 365
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

16
reconstitution of multifunction CMV-specific T cells in CMV-positive transplant 366
recipients. Blood. 113:6465-6476. 367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

17
FIGURE LEGENDS 389
390
FIGURE 1. The number of cytomegalovirus pp65/IE-1-specific IFN-γ-producing 391
CD8+ T cells (total) enumerated by flow cytometry for intracellular cytokine staining 392
(ICS) in the specimens that tested positive, negative or intermediate in the 393
QuantiFERON®-CMV assay. The data are given as log10 values, each dot represents a 394
single measurement and the bars represent median values. 395
FIGURE 2. Correlation between the number (log10) of pp65/IE-1-specific IFN-γ-396
producing CD8+ T cells enumerated by flow cytometry for intracellular cytokine 397
staining (ICS) and IFN-γ levels (log10) measured in the QuantiFERON®-CMV assay. 398
The data of 42 whole blood specimens (from 13 allogeneic stem cell transplant 399
recipients) testing tested positive in both methods are depicted. (A) Total number of 400
IFN-γ-producing CD8+ T cells; (B) dual IFN-γ/TNF-α CD8+ T cells; (C) dual IFN-401
γ/CD107a CD8+ T cells; (D) trifunctional (IFN-γ/TNF-α/CD107a) CD8+ T cells. 402
403
404
. 405
406
407
408
409
410
411
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

18
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

FIGURE 1.
g 10
cells
/μl)
1
2
CD
8+ T ce
lls (l
og
0
MV
-spe
cific
IFN
-γ
-1
QuatiFERON® CMV assay result
Indeterminate Non-reactive Reactive
CM
-2
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

A B
FIGURE 2.
T ce
lls (l
og10
cel
ls/μ
l)
1,5
2,0
2,5
3,0
D8+
T ce
lls (l
og10
cel
ls/ μ
l) 1
2
CM
V-s
peci
fic IF
N-γ
CD
8+ T
0,0
0,5
1,0
1,5-s
peci
fic IF
N- γ
/TN
F-α
CD
-1
0
IFN-γ level (log10 UI/ml)
-2 -1 0 1 2 3
C
QuatiFERON® CMV assay result
-3 -2 -1 0 1 2 3
CM
V-
IFN-γ level (log10 UI/ml)
QuatiFERON® CMV assay result
C D
T ce
lls (l
og10
cel
ls/μ
l)
1
2
T ce
lls (l
og10
cel
ls/μ
l)
1
2
ecifi
c IF
N-γ
/CD
107
CD
8+ T
-1
0
-spe
cific
trifu
nctio
nal C
D8+
-1
0
-3 -2 -1 0 1 2 3
CM
V-s
p
-2
IFN-γ level (log10 UI/ml)
QuatiFERON® CMV assay result
-3 -2 -1 0 1 2 3
CM
V-
IFN-γ level (log10 UI/ml)
QuatiFERON® CMV assay result
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

TABLE 1. Detection of cytomegalovirus-specific IFN-γ-producing CD8+ T cells by
intracelullar cytokine staining (ICS) and the QuantiFERON®-CMV assay in whole
blood specimens from allogeneic stem cell transplant recipients
______________________________________________________________________
Result of the ICS method Result of the QuantiFERON®-CMV
(no. of specimens) (no. of specimens)
______________________________________
Positive Negative Indeterminate
______________________________________________________________________
Positive (55) 42 10 3
Negative (35) 1 20 14
______________________________________________________________________
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

TABLE 2. Characteristics, advantages and limitations of the intracelular cytokine
staining method (ICS) used in the current study and the QuantiFERON®-
cytomegalovirus (CMV) Assay for evaluation of CMV-specific T-cell immunity
Method ICS (Intracellular cytokine
staining)
QuantiFERON®-cytomegalovirus
(CMV) Assay
Specimen/
volume
Whole blood/1 mL Whole blood/3 mL
Results
available within
8-10 h. 24-48 h.
CMV antigen Two peptide pools consisting
15 mer overlapping peptides
spanning the entire sequences
of pp65 and IE-1
21 peptides mapped within IE-1, IE-
2, pp65, pp50, and gB, and restricted
by several widespread HLA-I
variants (HLA A1,A2,A3,A24,
HLAB7, B8, B27,B35,B44,B52)
Knowledge of
HLA genotype
Not necessary Not necessary
Allows
differentiation
between CD8+
and CD4+ T
cells
Yes No (mostly detects CD8+ T cells)
Allows Yes Yes (IFN-γ only)
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from

functional
analysis of T
cells
Allows
phenotypic
analysis of T
cells
Yes No
Major
advantages
High sensitivity/ Precise
enumeration of CMV-specific
T cells/ Proven clinical utility
Highly standardized/Can be
performed in any center/ Simple to
perform
Major
limitations
Lack of standardization/Need
access to a flow cytometer
Suboptimal sensitivity (76% taking
ICS as the reference procedure and a
threshold of 0.2 UI/mL, as
recommended by the manufacturers)/
High percentage (~20%) of
indeterminate specimens/ Need to
dilute ~30% of positive samples for
precise quantitation/Lack of studies
demonstrating clinical utility in the
Allo-SCT setting
on March 28, 2020 by guest
http://cvi.asm.org/
Dow
nloaded from
Top Related