





γλώσσες
Σελίδες
Νομικός


SURGICAL MANAGEMENT OF THE AXILLA
Stephane Zervoudis MD, PhD Gynecologist- Breast Surgeon
Assoc. Professor University Montpellier-Nimes France President of MANOSMED Mediterranean University of Mastology
REA Hospital Athens & University of Ioannina Greece
4TH SYMPOSIUM CLINICAL ONCOLOGY April 2016

Breast Cancer Surgery is targeting the:
-Primary tumor : Mastectomy or Conservative Surgery
-Axillary lymph nodes : dissectionlevel I-II or SNB
The status of the axillary lymph nodes remains one of the most important prognostic factors in women with early stage breast cancer. Histologic examination of excised lymph nodes is the most accurate method for assessing spread of disease to these nodes
Uptodate , March 2016

• Main:– drainage axillary ispilatéral 85%– drainage internal mammaire ispilatéral 15%
• Others:– Interpectoral (Rotter)– intra- ou para-mammary– sub-claviculaire direct– rétrosternal to controlatéral CMI– sub-cutaneous to the controlateral chain– rétrograde liver via CMI
Sappey 1843, Tanis 2001 ,Estourgie Ann Surg 2004
Drainage pathways of the breast

4
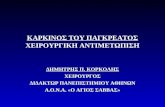
THE AXILLA AND THE LYMPH NODES• The axillary lymph nodes are divided to 3 levels:
– Level I: outside the minor pectoralis muscle– Level II: anterior and posterior to the minor pectoralis muscle– Level III: Inside the minor pectoralis muscle
• The axillary dissection extends normally only to levels I & II

Ultrasound Anatomy of the Axilla

Axillary`s nodes levels and locations
The axillary cross ( Clough 2012)The 3 levels of Berg
:87%
:: 11%
: 2%
:0%

Staging of Axilla: Difficult !!
• Clinical : no accurate• Ultrasound : difficult, in progress• MRI: SPIO technique: expansive, next future• CT : no specific• Nuclear Medicine : F-18 FDG : expansive , no micrometastasis Lymphoscintigraphy• Interventionnal: FNAC node
SLN Biopsy

SPIO-MR :Superparamagnetic iron oxide enhanced magnetic resonance imaging for the detection of metastases in sentinel nodes localized by computed tomography -lymphography (CT-LG) in patients with breast cancer
JNCI 2005 Kobayashi et al., Ann Surg Oncol 2011, Motomura K , Nakanishi K
Sentinel node biopsy for breast cancer: past, present, and future. Breast Cancer. 2015 May, Motomura K

2012-2017

SURGICAL MANAGEMENT OF AXILLA
• Maximum “Information” For prognosis & adjuvant treatment
• minimum “ Local Recurrence”
• Maximum “Survival”
• Maximum “Quality of Life”

SURGICAL MANAGEMENT OF AXILLA
.Sentinel node biopsy is the gold standard in 2016 as first procedure except Contra-indications
. Avoid axillary dissection as much as possible!!!

ADVICES after Axillary Dissection for the ipsilateral arm: The 10 Orders
• 1.NO CONSTRICTING WEAR, NO TIGHT JEWELERY• 2.AVOID CUTTING, PULLING CUTICLES, NAILS• 3.WEAR PADDED GLOVESWHEN
COOKING,GARDENING,HOUSEWORK• 4.AVOID CARRY HEAVY HANDBAGS,SUITCASES,PACKS• 5.AVOID SUNBURN,USE SUNCREAM• 6.WASH CUTS,SCRAPES,INSECT BITES WITH ANTISEPTIC• 7.TAKE BLOOD PRESSURE ON THE OTHER ARM• 8.MAKE INJECTIONS,BLOOD SAMPLING ON THE OTHER HAND• 9.TAKE ANTIBIOTICS AND CALL PHYSICIAN IF THE ARM IS
RED,HOT,TOUGHT,SWOLLEN• 10.KEEP THE ARM IN HIGH POSITION MORE OFTEN

Complications of Axillary Dissection
• Seroma• Lymphedema• Arm infection, septicemia• Paresthesia• Shoulder dyskinesia ,Chronic shoulder or arm pain• Angiosarcoma Stewart-Treves• Surgical complications: nerves injury, vessels injury

SEROMA ( Lymphocele)

Lymphedema : 13-27%


Complete Decongestive TherapyBandaging

Lymphedema Elephantiasis

ARM INFECTION : 2-5%

Axillary web syndrome Moskovitz : 8%
Paresthesia:-Numbness: 18%
Ann Surg. 1999 Aug; 230(2): 194.PMCID: PMC1420861Complications of Level I & II Axillary Dissection in the Treatment of Carcinoma of the BreastDaniel F. Roses MD,* Ari D. Brooks, MD,* Matthew N. Harris, MD,* Richard L. Shapiro, MD,* andJulie Mitnick, MD

WINGED SCAPULADisruption of the long thoracic nerve (Bell) results in
loss of serratus anterior function and a `` deformity with an unsightly posterior shoulder bony protrusion.

ANGIOSARCOMA STEWART TREVES : 0.03%

SENTINEL NODE
• Haldstedian concept < 1960: progression tumor growth and spread to regional lymph nodes
• Ramon,Cabanas 1960:``A specific lymph center…appears to be the primary site of metastasis
• Morton 1992:``Intaoperative Lymphatic mapping for malignant melanoma
• Krag 1993:``Surgical resection of radiolocalized sentinel node in breast cancer using a γ probe: HOT TECHNIQUE
• Giuliano 1994:``Lymphatic mapping and sentinel lymphadenectomy for breast cancer: BLUE TECHNIQUE
• Albertini 1996: HOT AND BLUE TECHNIQUE

Nieweg et al. Ann Surg Oncol 2004
DefinitionS Sentinel Node

JUNE 2015

CONTRA-INDICATIONS OF S.N• N+ Clinically palpable• T inflammatory• Performance of the surgeon if Detection rate < 90-95% , if False Negative >10%
• T> 4 cm : No more : Intra M , J Surg Oncol 2007• T multicentric : No more ?: Gentilini Eu j Surg Oncol 2006• Prior axillary surgery, mammoplasty No more? Rodriguez Fernandez Ann Surg Oncol 2009• Pregnancy : No more? Gentilini, Veronesi; Eur J Nucl Mrd Mol Imag 2010
• Neoadjuvant chemotherapy : No more? Veronesi 2010
• Male breast cancer: No more: Zurrida , Future Oncology 2010

IDENTIFICATION TECHNIQUES
• 1. RADIOACTIVE
• 2.COLORIMETRIC
• 3.COMBINED ( RADIOACTIVE AND COLOR )

SN IDENTIFICATION TECHNIQUES RADIOACTIVE TECHNIQUE
• Injection 3-24 hours before surgery, radioactive colloid Albumin filtered or no, Antimony, Rhenium , marked with Tc 99m
• Volume injected 0.2-0.5cc (0.5 mci) in the dermis in 4 points
• +- Lymphoscintigraphy follows with handheld γ probe
• Count node: rule of 10%: >7000counts and node with 700 counts removed too
• Mean number of nodes : 2,4 (1-7)
• Problem of ``Shine Through phenomena`` in Supero-ext Quadrant

Lymphoscintigraphy
Provides a road map and improves the intraoperative identification of SN. Localization of nodes with “hot” node on scan was higher than those without. (98% vs. 90%)
Goyal et al Eur J Cancer 2005;41:238-243



Macroaggregates of nanocolloid labeled with 12 MBq 99mTc, in 0.2 ml (ROLL)
SNOLL = Sentinel Node + ROLL
Sentinel node
Microaggregates of nanocolloid labeled with12 MBq 99mTc, in 0.2 ml (Lymphoscintigraphy)

SN IDENTIFICATION TECHNIQUES
COLORIMETRIC TECHNIQUE
INJECTION: 1-2 cc BLUE PATENTE, BLUE ISOSULFAN ,BLUE METHYLENE, INDOCYANINE GREEN
INTRATUMORAL or PERITUMORAL(91% ID) or SUBDERMAL SUBCUTANEOUS or SUBAREOLAR ( 96%ID)
Keshtgar etal: the sentinel node in surgical oncology Springer Verlag 1999
INTRA-NIPPLEZervoudis et al: intranipple injection EJGO 2012

COLORIMETRIC TECHNIQUE: INJECTION SITES
PERITUMORAL SUBAREOLAR

Sentinel lymph node detection by intra-nipple injection of patent blue dye in breast cancer: a preliminary report of a feasibility study
S.Zervoudis, G.Iatrakis, I.Navrozoglou, et al. Eur.J.Gynaec.Oncol XXXIII,n3, 2012
INTRANIPPLE INJECTION

Breast massage : 4-5 minutes

After 10 minutes a small incision < 2cm is performed in the lower part of the axilla

The Clavipectoralis aponevrosis is opened the blue sentinel node is recognized with the afferents and the efferents lymphatic vessels.
The node is grasped and removed

``HOT`` AND ``BLUE`` SENTINEL NODE

SNB procedures after excision
• Clips on sentinel node vessels
• Digital exploration of axilla
• Assessment background radioactivity
• Closure in 2 layers: subcutaneous ( vicryl 2/0 or PDS 3/0) intradermic (monocryl or nylon 4/0 )
• no drain is necessary

AXILLLARY LYMPH NODES LEVEL I-II
SENTINEL NODE

SN Internal Mammary : remove or no remove ? NO

SECOND STEP : LUMPECTOMY


> 95% < 10%

Allergic reactions : to the blue dye (isosulfan blue, patent blue). Within a few minutes to an hour, up to 2% present hemodynamic instability and anaphylaxis.
Skin coloration: resolve after 1-12 months
Skin necrosis: more with methylene blue
COMPLICATIONS OF SENTINEL NODE TECHNIQUES
Pregnancy: Blue dyes are contraindicated because the risk of teratogenicity is unknown.
Vitug AF, Newman LA. Complications in breast surgery. Surg Clin North Am 2007; 87:431-51

Data on long-term follow-up of patients who have undergone sentinel lymph node biopsy are revealing adverse sequelae in fewer than 10% of cases.
. axillary wound infections in 1%,
.axillary seroma in 7%,
.axillary hematoma in 1.4%.
.Lymphedema in 2-3.5% of cases.
Vitug AF, Newman LA. Complications in breast surgery. Surg Clin North Am 2007; 87:431-51
ACOZOG-ZOO11

How to increase identification rate ?
• Training curve of surgeon and pathologist
• Good technique of injection: timing, site
• Combined technique> single technique
• Digital palpation of the axilla
• Removing more SN decrease False negative : 10% 2SN, 7% 3 SN, 1% 5SN ( NSABP B32)
Krag et al - Lancet Oncol - 2007 Goyal et al - Breast Cancer Res Treat. 2006
Carmon et al - Breast J – 2006 Rodier et al – J Clin Oncol – 2007

5031 October 2015
NOMOGRAMS used multiple factors to predict the risk of invasion of non-SLN in the axilla:Tumor size,Grade,Number of positive
SLN,Estrogen statuspresence of lymphovascular invasion

51
TNM classification of Breast Cancer•pN0 : No regional lymph node metastasis identified histologically
Note: Isolated tumor cell clusters (ITC) are defined as small clusters of cells not greater than 0.2 mm, or single tumor cells, or a cluster of fewer than 200 cells in a single histologic cross-section. ITCs may be detected by routine histology or by immunohistochemical (IHC) methods.
pN0(i−) : No regional lymph node metastases histologically, negative IHC
pN0 (i+) : Malignant cells in regional lymph node(s) no greater than 0.2 mm (detected by H&E or IHC including ITC)
pN0(mol−) : No regional lymph node metastases histologically, negative molecular findings (RT-PCR)
pN0(mol+) : Positive molecular findings (RT-PCR)**, but no regional lymph node metastases detected by histology or IHC
THE AXILLARY INVOLVEMENT IN BREAST CANCER
31 October 2015

52
TNM classification of Breast Cancer• pN1 : Micrometastases, or metastases in 1–3 axillary lymph nodes; and/or in
internal mammary nodes with metastases detected by sentinel lymph node biopsy but not clinically detected pN1mi : Micrometastases (>0.2 mm and/or more than 200 cells, but < 2.0 mm) pN1a : Metastases in 1–3 axillary lymph nodes, at least one metastasis greater
than 2.0 mm pN1b : Metastases in internal mammary nodes with micrometastases or
macrometastases detected by sentinel lymph node biopsy but not clinically detected
pN1c: Metastases in 1–3 axillary lymph nodes and in internal mammary lymph nodes with micrometastases or macrometastases detected by sentinel lymph node biopsy but not clinically detected
THE AXILLARY INVOLVEMENT IN BREAST CANCER
31 October 2015

Axillary Metastasis; pN UICC (AJCC, 2002)
Type of Axillary Node`s metastasis pN
Isolated cells pNO(i+)Micrometastasis 0,2-2mm pN1miMacrometastasis > 2mm: 1-3 N+ pN1Macrometastasis >2mm : 4-9 N+ pN2
Isolated tumor cells
Micrometastasis

VALUE OF ITC and micrometastasis • Prognosis of ITC: Imoto S 2006 Europ J Surg Oncol Herbert GS 2007 Am J Surg : NO IMPACT
• Pronostic of μmeta controversy: μmeta possible nest of transient tumor cells ?
Hansen 2001 Ann Oncol Guenther 2003 Arch Surg : Kuijt: 2005 Eur J Surg Oncol : Cox 2008 J Am Coll Surg Lee.K.Tan 2009 J.Clinic.Oncol : μmeta : : IMPACT < DFS & OS
Chagpar 2005 Cancer, Langer 2005 Ann Surg, Nagashima 2006 Breast cancer,Kahn 2006 Breast J , Bulte EJSO 2008 Gobardhan , Van Dalen 2009 Ann. Oncol : NO IMPACT DFS OS Langer Ann Surg Oncol 2009 Maaskant-Braat AJ, Cancer Res Treat 2011 Truong PT , Europ J Cancer 2008 : number of sentinel nodes + with micrometas and ratio : impact on survival
Montagna E June 2009 Br Cancer Res Treat : 3158 patients p T12 pn0 pn1 minimal axillary lymph node involvement bad prognosis versus n- in AD, but prognosis differ according the stagging procedure: in SNB no difference
Rutgers E.J J Clin Oncol 2008: Findings pose difficulties to take clinical decision …

New Techniques for SNB

New Agents: Blue and Radioactive
Phillips W et al. 99 Tc Biotine labeled liposome encapsuled blue dye.
J Nucl Med (2001)
El-Tamer M et al. 99m Tc labeled phtalocyanine tetrasulfonate
Annals of Surgical Oncology (2003)

Non-Invasive Identification of Sentinel Lymph Nodes Using IndocyanineGreen Fluorescence
Imaging in Patients with Breast Cancer
Nobumi Tagaya*, Aya Nakagawa, Akihito Abe, Yoshimi Iwasaki and Keiichi Kubota Dokkyo Medical University, Mibu, Tochigi , Japan
The Open Surgical Oncology Journal, 2010
This method is safe, minimally invasive for intraoperative detection of SLN, allowing real-time observation


MANAGEMENT OF AXILLA
Early stage, cN0, Primary Surgery
SLNB
pNSLN- pNSLN+
Neoajvt chemo No further surgery No AD Axillary RT
Axillary dissection ( AD)

STUDIES Sentinel Node NSABP-B 32 :SN+AD VS SN
ACOSOGZOO11 (USA): SN + : AD VS 0
ALMANAC (UK) :SN+: AD VS 0
AMAROS (EORTC) :SN+: → AD VS RT
IBCSG23-01 SN mic+:AD VS 0
ACOSOG Z1071 (ALLIANCE) : SN after neoadjvt chemoth for N+
SENTINA SN before and after neoadjvt chemoth
FRANCENOD :SN /injection periareolar vs intratumoral
SENTIBRAS: Selective axillary clearance

The New Challenge

Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from
the NSABP B-32 trial
D.Krag, S.Anderson, T. Julian, A.Brown, S. Harlow, J. Costantino, T.Ashikaga, D. Weaver, E.Mamounas, L. Jalovec, T. G Frazier, R Noyes, A. Robidoux, H. Scarth, N. Wolmark
Lancet Oncol 2010 oct 11 (10)
• Methods NSABP B-32 was a randomised controlled phase 3 trial done at 80 centres in Canada and the USA between May 1, 1999, and Feb 29, 2004. Women with invasive breast cancer were randomly assigned to either SLN resection plus ALND (group 1) or to SLN resection alone with ALND only if the SLNs were positive (group 2)
• Overall survival, disease-free survival, and regional control were statistically equivalent between the 2 groups.
• When the SLN is negative, SLN surgery alone with no further ALND is an appropriate, safe, and effective therapy for breast cancer patients with clinically negative lymph nodes

NSABP B-32Occult Metastases Conclusions
At ten years, there is not a significant difference in OS and DFS despite the absolute difference of 3.1%.
A significant difference in DFS for occult metastases with an absolute difference of 4.7% is identified.
This downward trend is seen for both ITC and micro-metastatic disease.
However, the impact of occult metastatic nodal disease in this very large cohort of 5,611 patients with a OS HR of 1.09 and a DFS HR of 1.02 is clinically non significant.
OS, DFS, and Local-regional recurrence is not affected by the positive occult metastases in the SNR only group.
Ax Node dissection for occult metastases is of no benefit. The routine use of IHC analysis for SNB is not recommended.
San Antonio Breast Cancer Symposium, December 10-14, 2013

The NSABP B-32 showed that the rate of False-Negative in SLN biopsies is 9.8%.
These false-negative patients did not undergo ALND.
What happened to such patients ?


ACS Oncology Group Z0011 Randomized Trial
Annals of Surgery 2010

ACS Z0011 Results7 years of median follow-up
2 groups : pN+ patients with isolated SLN biopsy compared to pN+ patients treated by SLN biopsy + ALND
The 2 groups were comparable as to local and to regional recurrence
SLN alone SLN + ALND
Local Recurence 8 (1.8%) 15 (3.6%)
Regional recurrence 4 (0.9%) 2 (0.5%)

ACS Z0011 Results
The authors indicated that the results of this study do not apply to:
– Women with palpable nodal disease– Women with > 2 Sentinel nodes positive– Women undergoing mastectomy (because of
abstention to radiotherapy)– the subject of survival

IBCSG 23-1 Trial Veronesi
Lancet Oncology 2013 14(4)

70
IBCSG 23-01 TRIAL
BREAST EVENTSSLN SLN + ALND
Breast Cancer 10.6% 10.8%

IBCSG 23-01 TRIAL Conclusion
In Sentinel node micrometastasis ALND is not necessary
How to explain this observation, although 13% of non-sentinel lymph nodes in the SLN + ALND are metastatic ?
Adjuvant radiotherapy was used in 97% of cases in both arms Hormonotherapy was used in about 65% in both groups
Chemotherapy was used in about 8% in both groups

In retrospective studies (MD Anderson, Mayo Clinic), series of SLN positive patients did not undergo ALND because the lymph nodes contained limited extension of cancer (N1mi) or patients refused a second surgery: No axilary recurrence and no breast cancer related deaths were noted. All these patients received chemotherapy and (or) radiotherapy.
In a Swedish multicenter cohort study, (Bergkvist), 2246 women had a negative SLN and did not undergo ALND: the 5-year isolated axillary recurrence rate was 1.1%, compared to a 1% risk in cases of negative ALND
In a Dutsch study (Van der Ploeg), 755 women with negative SLN did not undergo ALND. The axillary recurrence rate at 5 years was 0.4%. The OS was 95.5% and the DFS was 89.7%.

Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer patients: final analysis of the EORTC AMAROS trial
By the EORTC Breast Cancer Group andRadiation Oncology Group In collaboration with the Dutch BOOG Group and ALMANAC Trialists’ Group
E. Rutgers The Netherlands Cancer Institute, Amsterdam
Axillary lymph node dissection and axillary radiotherapy after a positive sentinel node provide excellent and comparable axillary control for patients with T1-2 primary breast cancer and no palpable lymphadenopathy. Axillary radiotherapy results in significantly less morbidity.( lymphedema)

(SENTInal NeoAdjuvant)103 centers
n=1 737


STUDY SENTIBRAS
•December 2009 - December 201211 Centers ( 32 surgeons)
Ann Surg Oncol. 2007 Sep;14(9):2490-6. .Blue dye injection in the arm in order to conserve the lymphatic drainage of the arm in breast cancer patients requiring an axillary dissection.
Nos C, Lesieur B Clough KB, Lecuru F.

The ASCO Update Committee issued recommendations for clinical practice concerning
use of SLN Biopsy
Journal of clinical Oncology 2014

New Guidelines and Recommendations: ASCO Journal Clinical Oncology May 2014 J Anello; B Feinberg; R Lindsey; L Soler; C Wojdylo; O Wong, DO; N Dunford

CONSENSUS ST GALLEN 2015
Axillary dissection no longer indicates in: Negative sentinel node1 or isolated cells Sentinel node with micro-metastases ≤ 2mm
independently from type of surgery 1-2 metastatic sentinel nodes > 2mm when breast
conserving surgery 2
Still indicated in case of mastectomy or > 2 nodes positive or if no radiation therapy
Krag DN et al. Lancet Oncol 2010; 11:927-933Giuliano AE et al. JAMA 2011;305:569-575

CHINESE METANALYSIS 2015 ASCO Recommendations are consolidated by a Chinese
Meta-analysis reviewing all publications comparing SNB alone to ALND in Node positive breast cancer

81
CHINESE META-ANALYSIS 2015
31 October 2015
12 studies were found fulfilling the inclusion criteria. They include 26,870 patient undergoing SLN biopsies and 103,705 patients undergoing ALND

82
CHINESE META-ANALYSIS 2015
31 October 2015
No difference in Effect of Micrometastasis on Survival

83
CHINESE META-ANALYSIS 2015
31 October 2015
No difference in Locoregional Recurrence

84
CHINESE META-ANALYSIS 2015
31 October 2015
No difference in Disease Free Survival

85
CHINESE META-ANALYSIS 2015
31 October 2015
No difference in Overall survival

CONCLUSIONSThe management of axilla in breast cancer is changing!!!From « dissect all axilla when pN+ » to « do not more dissect axilla »We propose `` no dissect in pN- , no dissect in pNmic and may be no dissect in pN+ unless…………``

``L’analphabète d’aujourd’hui est celui qui ne sait pas désapprendre pour pouvoir apprendre à réapprendre``
Mahdi Elmandjra

THANK YOUΕΥΧΑΡΙΣΤΩ
Top Related