Total Quality Improvement Assessment Of Strep C β-Hemolytic Streptococci Treatment in a College...
71
Total Quality Total Quality Improvement Assessment Improvement Assessment Of Strep C Of Strep C β β -Hemolytic -Hemolytic Streptococci Treatment Streptococci Treatment in a College Population in a College Population Valerie Kiefer MS, APRN University Of Connecticut
Transcript of Total Quality Improvement Assessment Of Strep C β-Hemolytic Streptococci Treatment in a College...
Total Quality Total Quality Improvement Assessment Improvement Assessment
Of Strep C Of Strep C ββ-Hemolytic -Hemolytic Streptococci Treatment in Streptococci Treatment in
a College Populationa College PopulationValerie Kiefer MS, APRN
University Of Connecticut
24-Hour Care Fee for Service Departments:
◦ Primary Care ◦ Walk-In Clinic◦ Women’s Clinic◦ Allergy Clinic◦ Counseling & Mental Health◦ 9 Bed In-Patient◦ Laboratory◦ Radiology◦ Pharmacy
The University of Connecticut provides primary health care to approximately
20,000 students annually.
What is Group C Streptococcus?Gram positive anaerobe which produce
small or large coloniesUsually beta hemolytic
Share many clinical characteristics with GAS
Group C can cause isolated exudative or common source epidemic pharyngitis indistinguishable clinically from GAS
Large colony Small colony are not associated with
pharyngitis
Why Study Group C Strep?
Pharyngitis and Group C Streptococcus common in college health
Do You Treat or Test for Group C strep pharyngitis?
Unknown if the association of group C (BHS) pharyngitis in college students is
related to immunity issues, lifestyle or other factors
Review Of The Literature
Studies that have shown strong epidemiologic association between
group-C BHS and endemic pharyngitis in college students
Review Of The Literature
Turner et al, JAMA 1990Association of Group C β-Hemolytic Streptococci With Endemic Pharyngitis Among College StudentsPurpose: NGA BHS could be detected more commonly in the throats of students with symptomatic pharyngitis than among healthy controls of similar age.
Performed throughout 2 school yearsNGA BHS group, only those from group C
were isolated more often/compared with the control group (26% to 11%)
Established a strong epidemiologic association between group C BHS and endemic pharyngitis in college students
Group C BHS had fever, exudative tonsillitis and anterior cervical adenopathy more frequently than patients who were negative for group C
Turner et al, Journal Of Clinical Microbiology 1997Epidemiologic Evidence From Lancefield Group C Beta Hemolytic Streptococci As A Cause Of Exudative Pharyngitis In College Students
Compared the isolation rates of strains of group C BHS from throat swab cultures of patients with exudative pharyngitis, the common cold, and healthy controls
College health/chart review
Isolation of Lancefield group A and C beta-hemolytic streptococci from throat cultures was used as an outcome measurement
Lancefield Group C strep associated with purulent exudative pharyngitis in college students.
Broyles et al, Clinical Infectious Disease 2009Population-Based Study of Invasive Disease Due to β-Hemolytic Streptococci of Groups Other than A and BDifferent Species of non A, non B –hemolytic streptococci and their clinical significanceNABS Comprise multiple distinct species that cause infections. (G,B,H) Manifestations differ, specification may be warranted in clinical settings
Tiemstra et al, Journal American Board Family Medicine 2009Role of Non Group A Streptococci in Acute PharyngitisThe role of Non Group A strep as pathogens of pharyngitis is controversial. Data is limited and conflicting on whether these bacteria are true pathogens of pharyngitis and whether treatment is indicated in all or just select cases.
Objective: Determine whether in non-GAS identified on culture if the clinical signs and symptoms resemble group Aimplicating them as true pathogens or if they resemble culture negative pharyngitis suggesting they are viral in etiology
Retrospective case control studyMean age 26 yearsGAS by RAS or cultureNeg. RSA or culture
Results: Young, adult population with acute pharyngitis, non GAS was as common as GAS
Non GAS same clinical features typically associated with GAS
Suggests clinicians may want to consider treating patients with proven or presumptive non GAS pharyngitis who fail to respond to symptomatic therapy or who are at increased risk for sequelae
Further study needed/antibiotic treatment
Cooper et al, Annals Of Internal Medicine 2001, Principles of Appropriate Antibiotic Use For Acute Pharyngitis In Adults, Position PaperExamines the available evidence regarding the diagnosis and treatment of acute GABHS in adult patientsRecommendations made that balance concerns about the potential consequences of untreated GABHS and the goal of decreasing inappropriate antibiotic prescriptions
Group A strep is the causal agent in 10% of adult cases of pharyngitis.
Antibiotics are prescribed to 75% of adult patients with acute pharyngitis.
Incidence of complications regardless of treatment with antibiotics is low.
Antibiotic therapy instituted within 2-3 days of symptom onset hastens symptomatic
improvement by 1-2 days in patients/cultures grow GABHS.
Antibiotics do not have this effect with a negative culture.
Symptom duration is strongly related to patient satisfaction.
Antibiotic treatment benefits only those patients with GABHS.
Limit antibiotic prescriptions to patients who are most likely to have GABHS
infections.
Rutecki, Top Papers Of The Month, Does This Patient Have Group A Strep Pharyngitis?, Consultant 2012
This paper discussed pharyngitis and the Centor Criteria.
Include Centor Criteria in Management/approach to pharyngitis.
Shah, Centor and Jennings, Severe Acute Pharyngitis Caused by Group C Streptococcus, 2006 Case Report
Group C Strep. / Approx. 5% prevalencePresent Broad Spectrum of SeverityLess common cause of acute pharyngitis but has both similar microbiology and presentation to group A.Both cause exudative or epidemic pharyngitis which are indistinguishable clinically.
5 Important Considerations/Neg. RSA/ Worsening Symptoms
MonoAcute HIVGroup C
Peritonsillar AbscessLemierre’s Syndrome
(Fusobacterium necrophorum)Neg. RSA /possibly worsen over the next
week
Reasons We Treat Strep ThroatStrep A causal agent 10%
Reduce SymptomsPrevent the spread of StreptococciPrevent Infectious Complications
◦Tonsillar Abscesses ◦Sinusitis
Prevent Rheumatic Fever /2011 incidence of rheumatic fever in the US was 1 per 1 million strep throatsPrevent GlomerulonephritisMajority of adults have a self limited illness who do not need antibiotics
Group C Strep- Does not cause some of the
complications caused by Group AUncommon cause of pneumonia
Group C Strep sinusitis has been reportedRarely isolated from blood cultures/fewer
than 1% of all bacteremiaGroup C and G Strep meningitis have been
reported and are often associated with endocarditis
Group C Strep arthritis uncommon/occurs in joints with preexisting rheumatologic
abnormalities
Role of Non-Group A Streptococci
Conflicting and limited data◦Guidelines/Standards treat Strep A◦Controversy regarding management strategy
for adult pharyngitis◦Dr. Centor points out in the article: Pharyngitis
Management: Defining the Controversy JGIM (2007) ◦Randomized trial data suggests a symptomatic
benefit for treating Group C patients
Infectious Diseases Society of America (IDSA) 2012 Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal PharyngitisGroup C Strep common cause of acute pharyngitis among college students and adultsPrimary reason to identify GCS as the etiologic agent of acute pharyngitis is to initiate antibiotic therapy that may reduce the clinical impact of the illness
Currently, there is no convincing evidence from controlled studies of a clinical response to antibiotic therapy in patients with acute pharyngitis from GCS isolated from the throat
CDC recommends not treating GCS.
Community Vs. College Health Rapid Strep A testing (RSA)
◦Fever◦Exudative Tonsillitis◦Adenopathy◦No cough
◦A back up throat culture is not routinely performed
◦Community/Follow up visit
UCONN
RSABack Up Throat Culture
Treated by Clinical PresentationRSA Neg. Strep C No Improvement
AntibioticFollow up visit or antibiotic left at clinic for
pick up by studentTime period of antibiotic treatment could
range from 1-5 days post visit
OSOM
RSAUltra Strep A Test98.2% SensitiveSingle Swab CultureQuality of the test depends on the quality of the sample. Negative results can occur from inadequate specimen collectionDoes not differentiate between carriers and acute infectionUsed as an adjunct to other information available to the provider
Purpose of Study/Quality Issues Addressed
Quality Improvement Assessment
To determine if antibiotic use in the treatment of Group C BHS in the college population is appropriate in relationship to community standards/guidelines.
◦College Population DIFFERENT!!
To evaluate if the University of Connecticut’s quality of care and guidelines are appropriate in the treatment of Group C BHS
To assess the time frame of treatment or non treatment of Group C BHS .
Same day treatmentNext day treatment
Treatment within 2-5 days of visit
To evaluate key indicators in relationship to Group C BHS in the college population.◦Tonsillitis◦Mononucleosis
Collected data before & after an educational action for clinical staff
Performance Goals
Difficult to set/lack of guidelinesCollege Health taken into account75% adult pharyngitis patients treated with an antibiotic
Performance Goals
70% Total Patients Treated with antibiotic10% Patients Treated with antibiotic day 1
10% Patients Treated with antibiotic day 2- 5
Looked at:Under and over usage of antibiotics
Quality of care and outcome issues as well as practice guidelines
Data Description
Retrospective Chart Audit January/11 to March/11
786 Diagnosed With PharyngitisPeopleSoft#
Date of ExaminationPositive for Group C BHS
Negative treatment with an antibiotic Treated with an antibiotic/time frame
Tonsillitis or MononucleosisFollow up visit or phone call
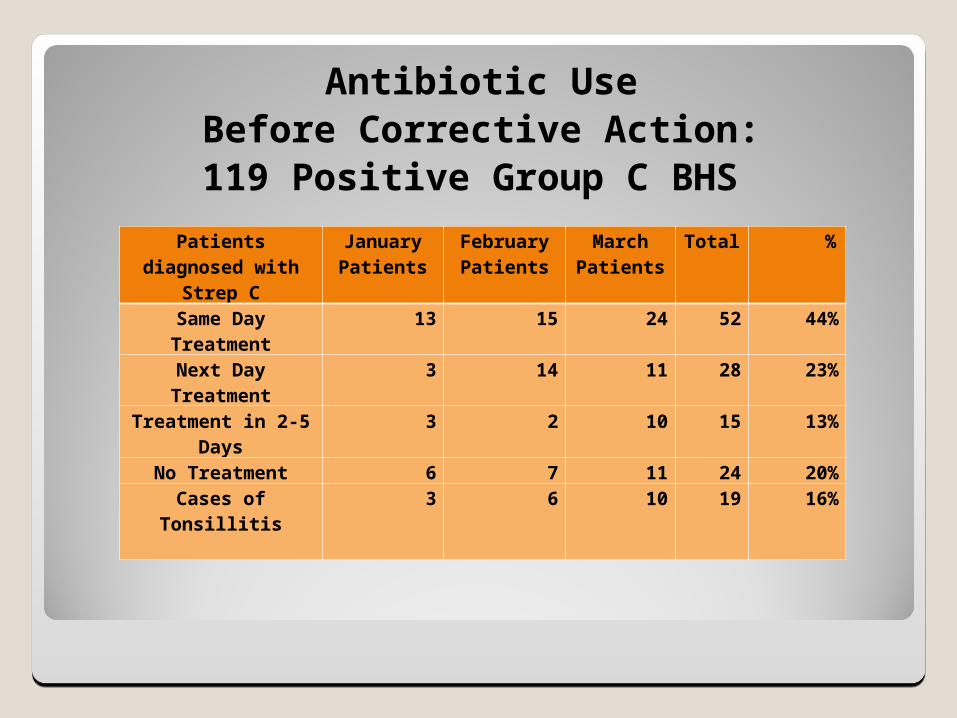
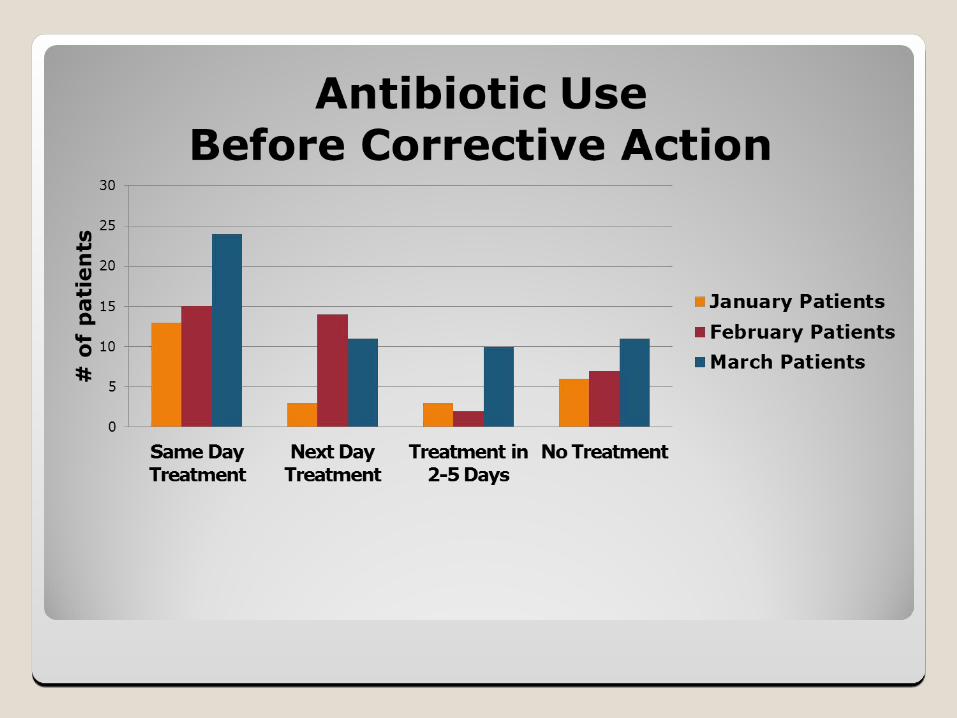
Antibiotic UseBefore Corrective Action:119 Positive Group C BHS
Patients diagnosed with
Strep C
January Patients
February Patients
March Patients
Total %
Same Day Treatment
13 15 24 52 44%
Next Day Treatment
3 14 11 28 23%
Treatment in 2-5 Days
3 2 10 15 13%
No Treatment 6 7 11 24 20%Cases of
Tonsillitis3 6 10 19 16%
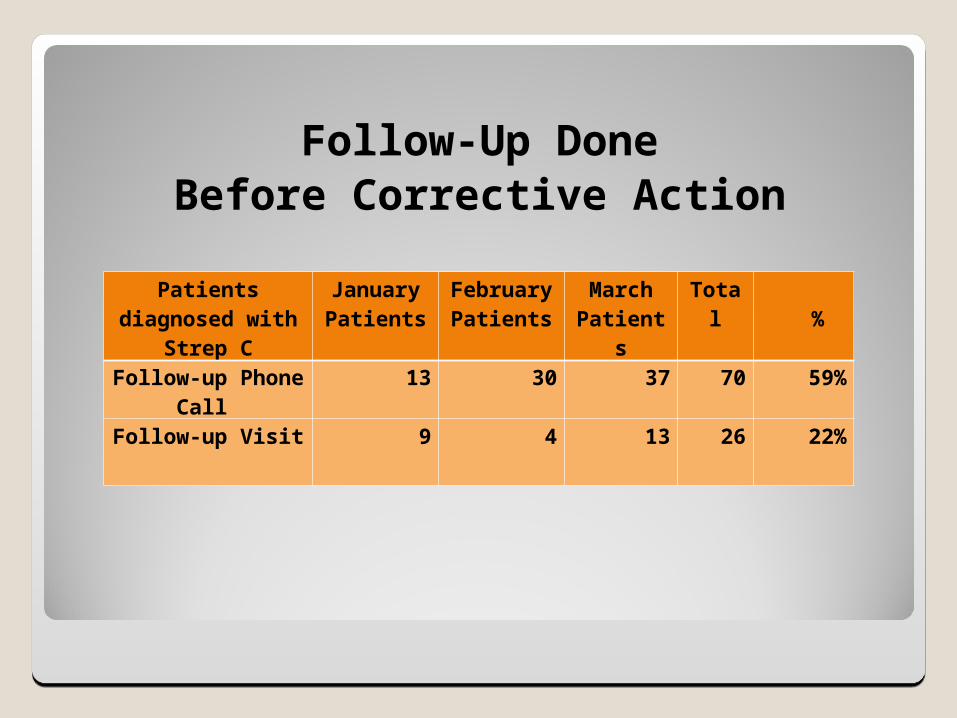
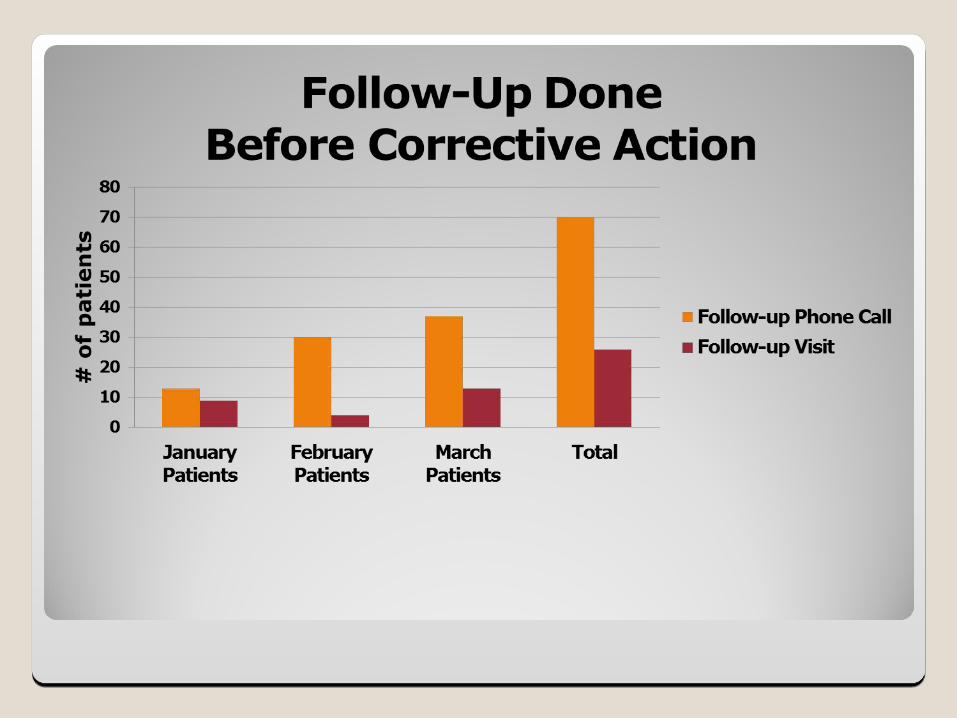
Follow-Up DoneBefore Corrective Action
Patients diagnosed with
Strep C
January Patients
February Patients
March Patient
s
Total %
Follow-up Phone Call
13 30 37 70 59%
Follow-up Visit 9 4 13 26 22%
Data AnalysisBefore Corrective Action:
80% Treated with an antibiotic44% Same Day23% Next Day13% Day 2-5
16% Tonsillitis6% Mononucleosis
59% Follow-up Phone Call22% Follow-up Visit
Antibiotics Used
Penicillin VK 500 mg TID Zithromax (Z-Pak)
Amoxicillin 875 mg BIDAugmentin 875 mg-125 mg BID
Clindamycin 300 mg TIDBiaxin 500 mg BID
IDSA Recommendations
PCN 500 MG BID
AMOXICILLIN 50 MG/KG QD(MAX = 1000 MG)
AZITHROMYCIN 12 MG/KG QD(MAX = 500 MG)

Performance Goals Comparison
Goal: 70% TreatedPerformance: 80% Treated
Goal: 10% Treated/Next DayPerformance: 24% Treated/Next Day
Goal: 10% Treated/Day 2-5Performance: 13% Treated/Day 2-5
Discussion
Community Standards/College Health Standards
Laboratory On Site/Depending on the time the student is seen, we will get a throat culture back the next day
2 Day Illness History/Average of 2 days of illness before they come in for an evaluation
Issues Of Concern
Antibiotic Offered Too Soon/Patient would have eventually improved and not needed to be treated with an antibiotic
80% Antibiotic Treatment for Strep C was too high in relation to community standards and we were prematurely over prescribing antibiotics
Laboratory Turnaround/Prompt turnaround of backup throat cultures contributed to our increased antibiotic usage. If the backup culture was returned 1 day post visit / probability of student still having a sore throat was high which in turn could influence the provider to prescribe an antibiotic
Issues Of Concern
Reevaluation Of Symptoms
Prescribing antibiotics without consistent reevaluation of patients was not
appropriate medical care or follow up and addressed quality of care issues
Corrective Actions
Positive Group C BHS results would not be reported until 3 days post visit/Address the quick turnaround time of cultures from our laboratory
Laboratory results available if needed/provider call the lab for a result if there was a clinical
concern
Provider would continue patient education/Issues or concerns call or make an appointment to be
seen
Comfort Measures/Treatment for Sore Throat
Corrective Actions
Clinical Judgment/Same day treatment would not be addressed due to the involvement of the providers judgment regarding antibiotic usage
Group C BHS reported to clinician
Student with continued symptoms/ follow –up visit/antibiotic would not be left at the clinic or
in the pharmacy
Original provider or back up clinician
Corrective Actions Implemented
January 2012
Re-Measuring Of Data
Chart Audit
January 2012 to March 2012
107 Charts Audited
773 With Pharyngitis Diagnosed
Same Criteria
PeopleSoft #Date Of ExaminationPositive For Group C BHS Negative Treatment With An AntibioticTreated With An AntibioticTime Frame of TreatmentSame Day, Next Day, Day 2-5Tonsillitis or Mononucleosis DiagnosedFollow Up Visit or Phone Call
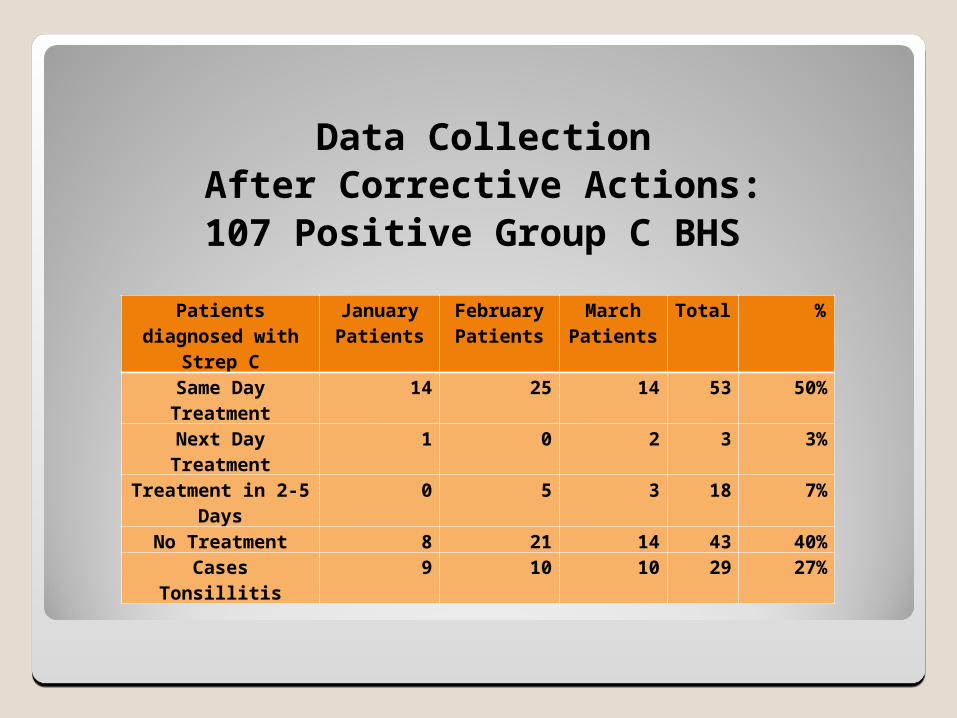
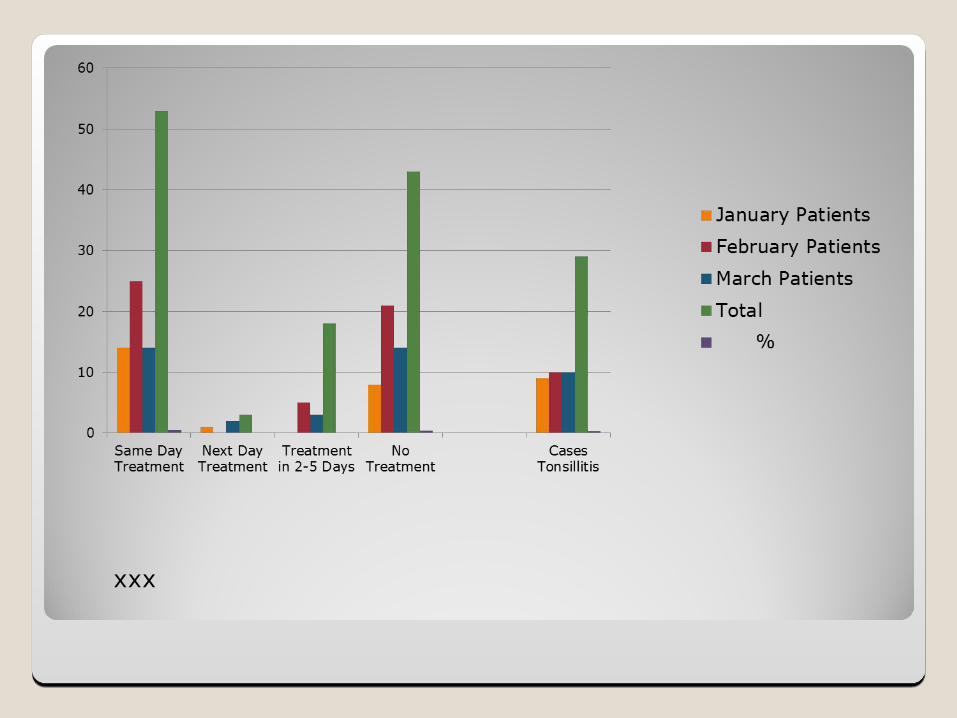
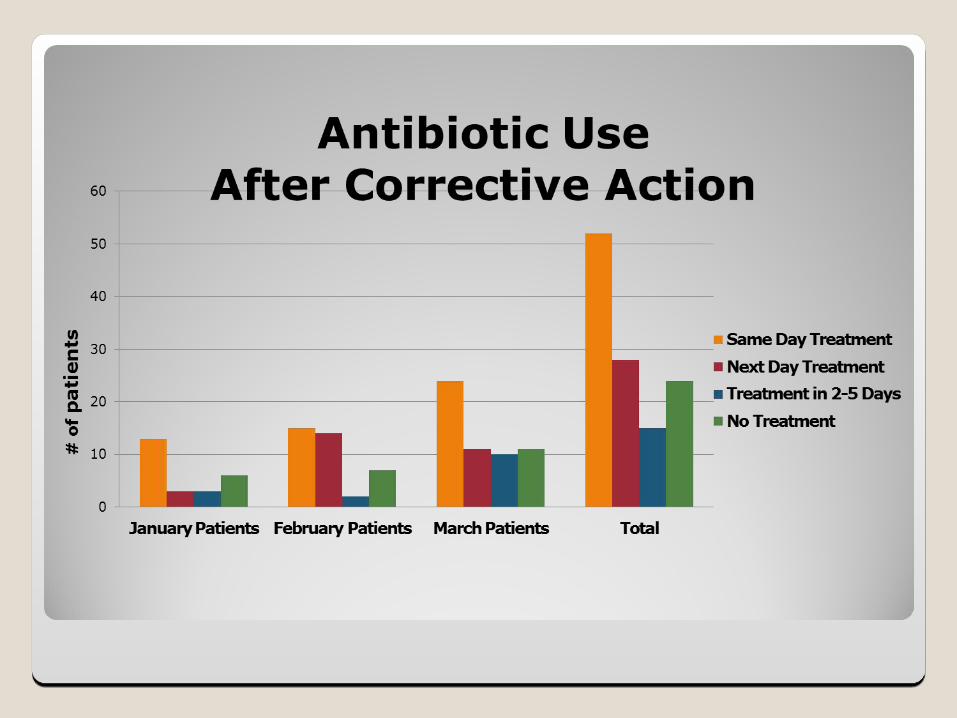
Data CollectionAfter Corrective Actions:
107 Positive Group C BHS
Patients diagnosed with
Strep C
January Patients
February Patients
March Patients
Total %
Same Day Treatment
14 25 14 53 50%
Next Day Treatment
1 0 2 3 3%
Treatment in 2-5 Days
0 5 3 18 7%
No Treatment 8 21 14 43 40%Cases Tonsillitis 9 10 10 29 27%
xxx
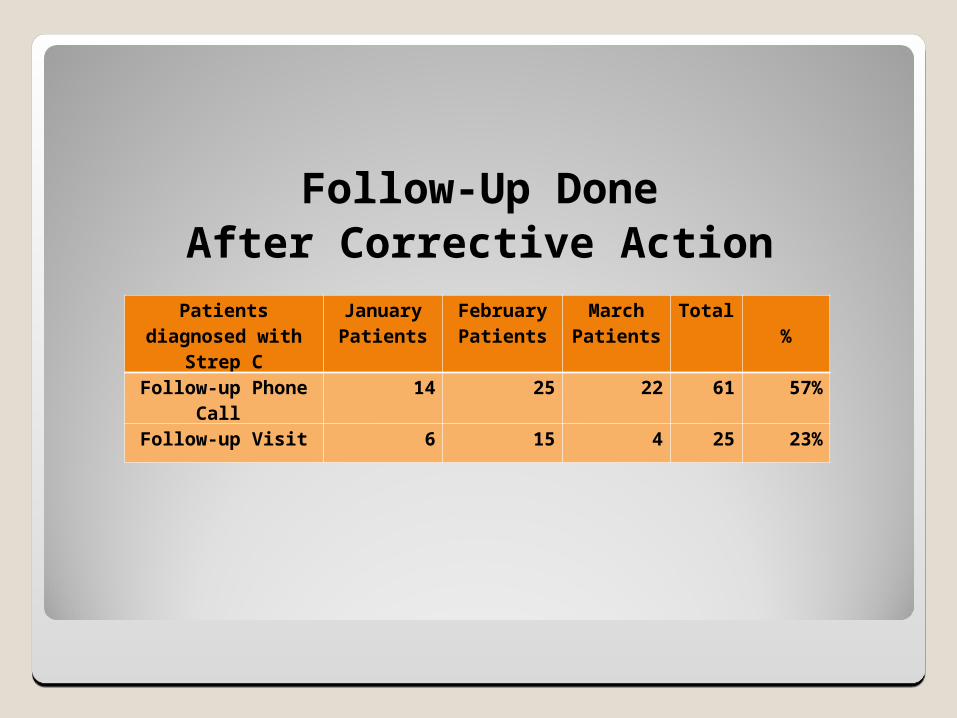
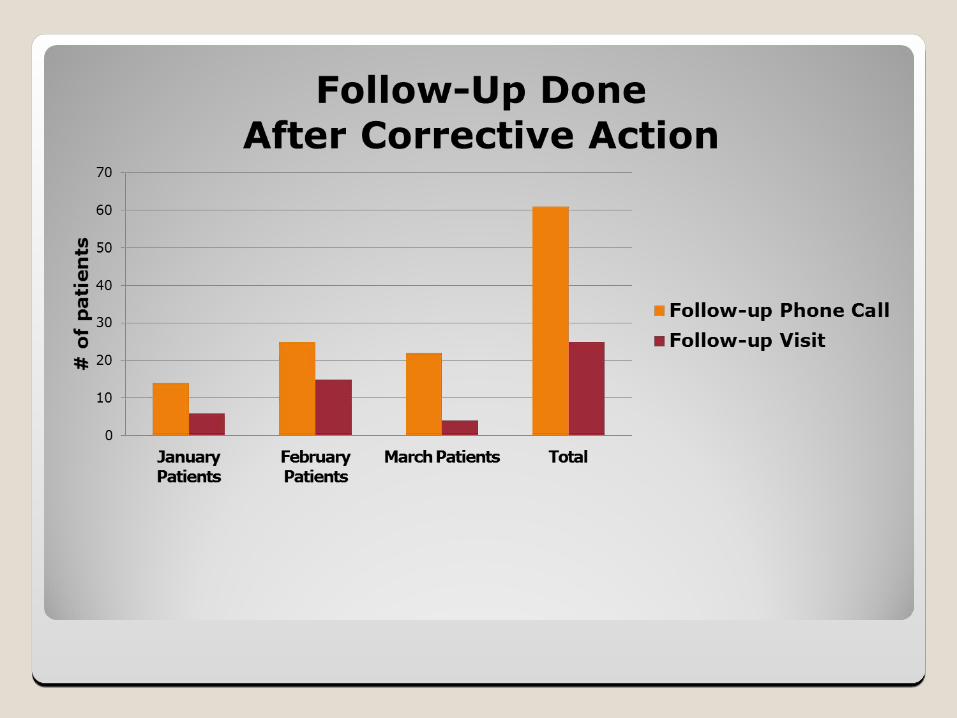
Follow-Up DoneAfter Corrective Action
Patients diagnosed with
Strep C
January Patients
February Patients
March Patients
Total %
Follow-up Phone Call
14 25 22 61 57%
Follow-up Visit 6 15 4 25 23%
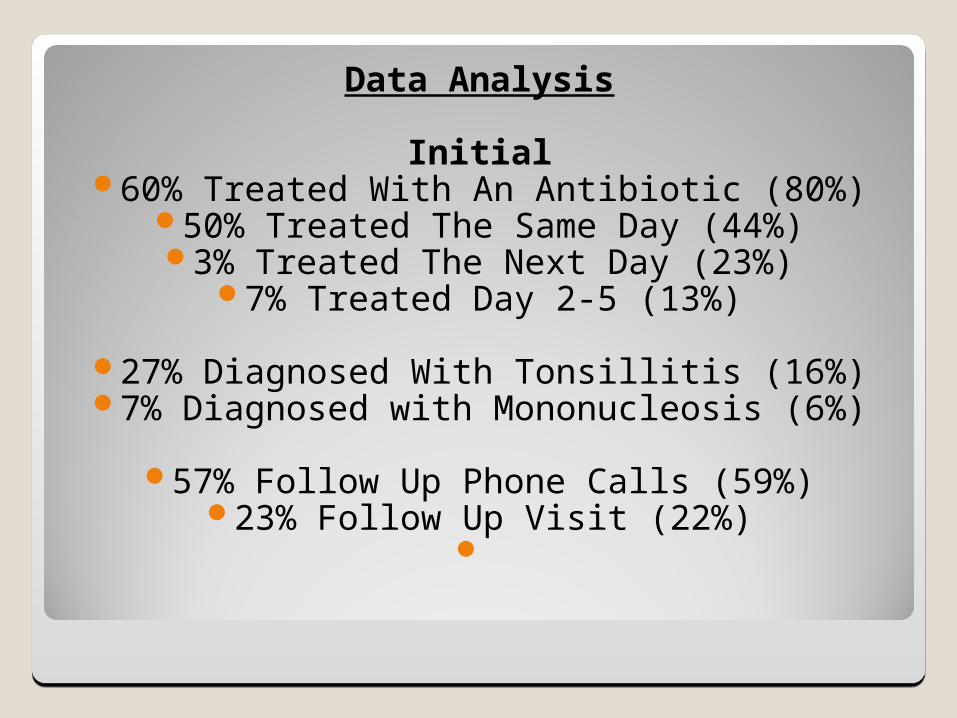
Data Analysis
Initial60% Treated With An Antibiotic (80%)
50% Treated The Same Day (44%)3% Treated The Next Day (23%)
7% Treated Day 2-5 (13%)
27% Diagnosed With Tonsillitis (16%)7% Diagnosed with Mononucleosis (6%)
57% Follow Up Phone Calls (59%)23% Follow Up Visit (22%)
%
Before Corrective
Action
After Corrective
Action
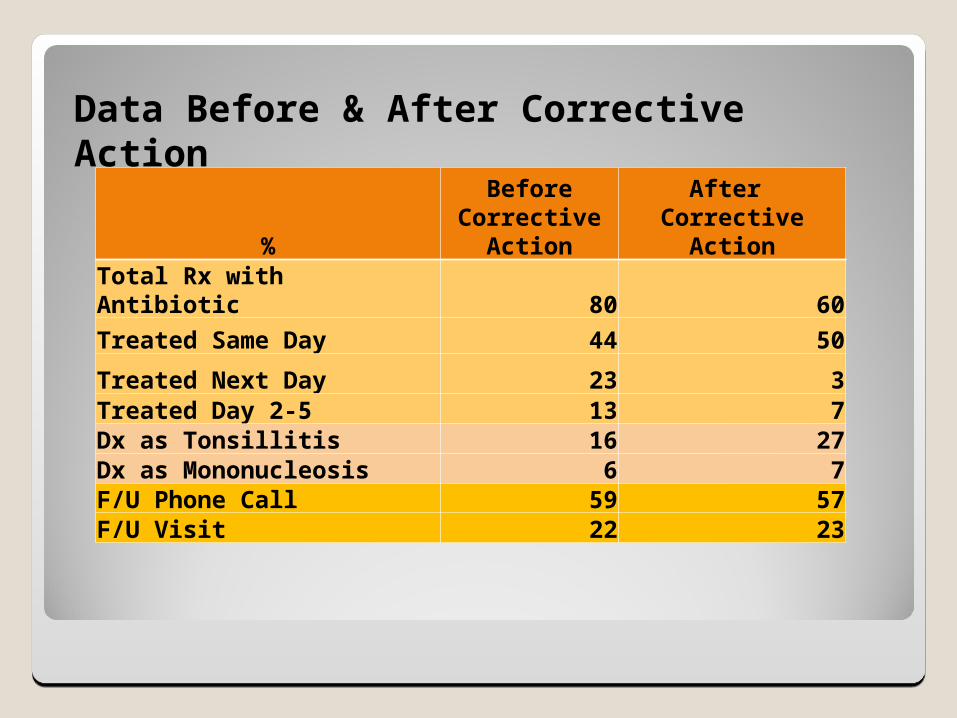
Total Rx with Antibiotic 80 60
Treated Same Day 44 50
Treated Next Day 23 3Treated Day 2-5 13 7Dx as Tonsillitis 16 27Dx as Mononucleosis 6 7F/U Phone Call 59 57F/U Visit 22 23
Data Before & After Corrective Action
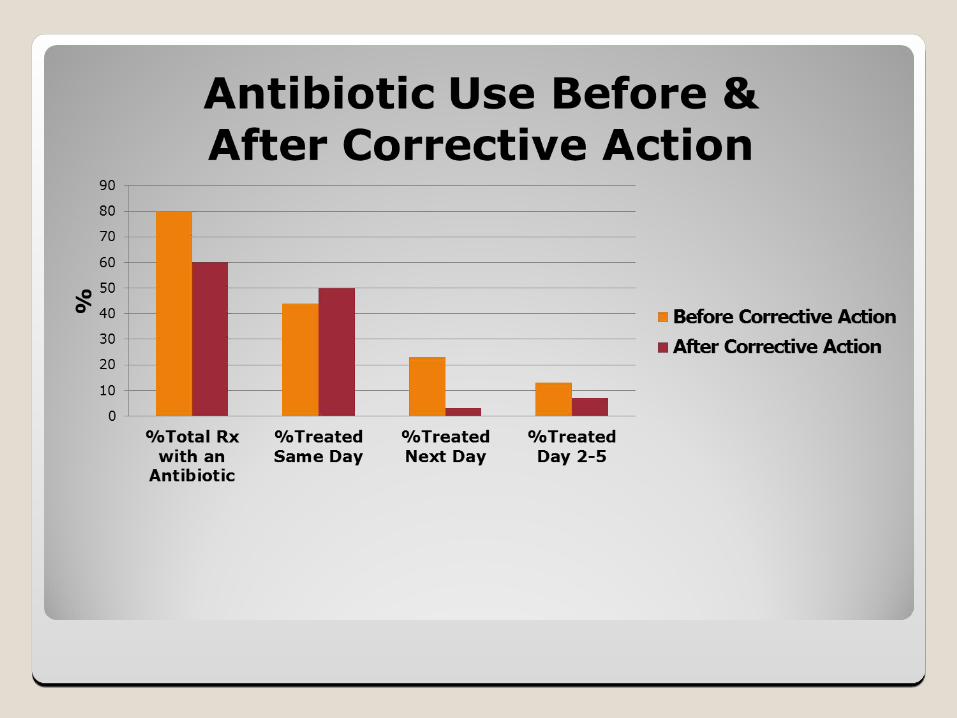
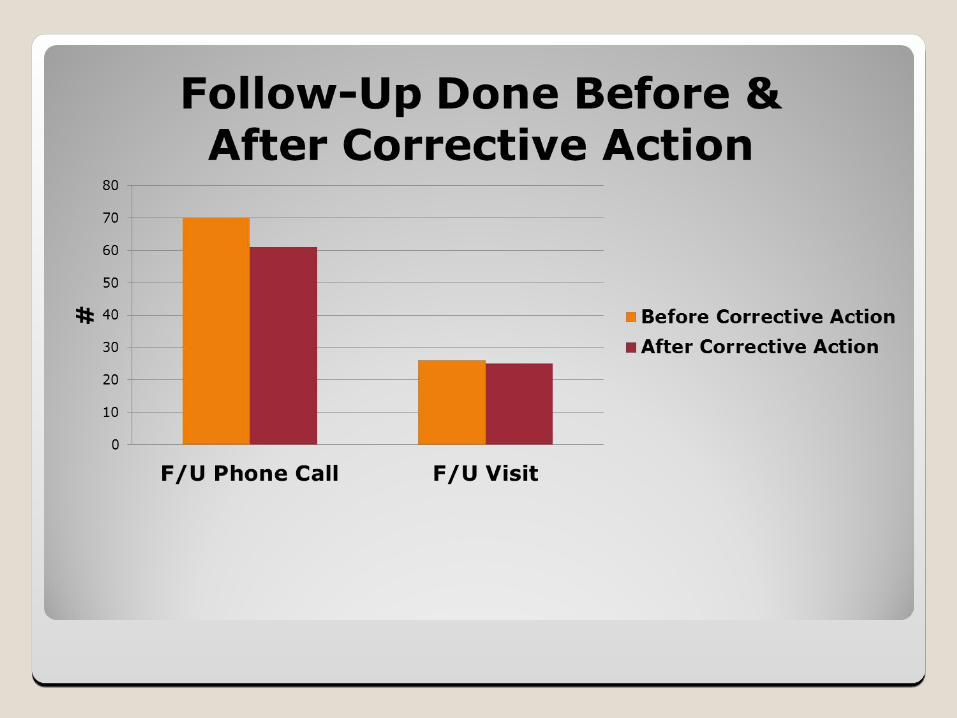
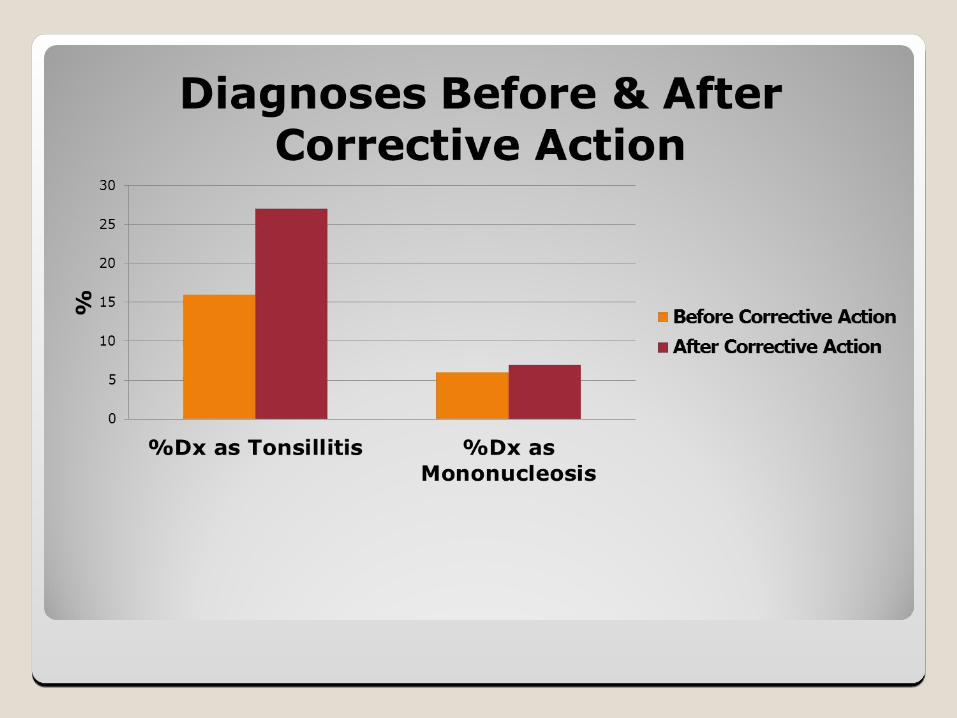
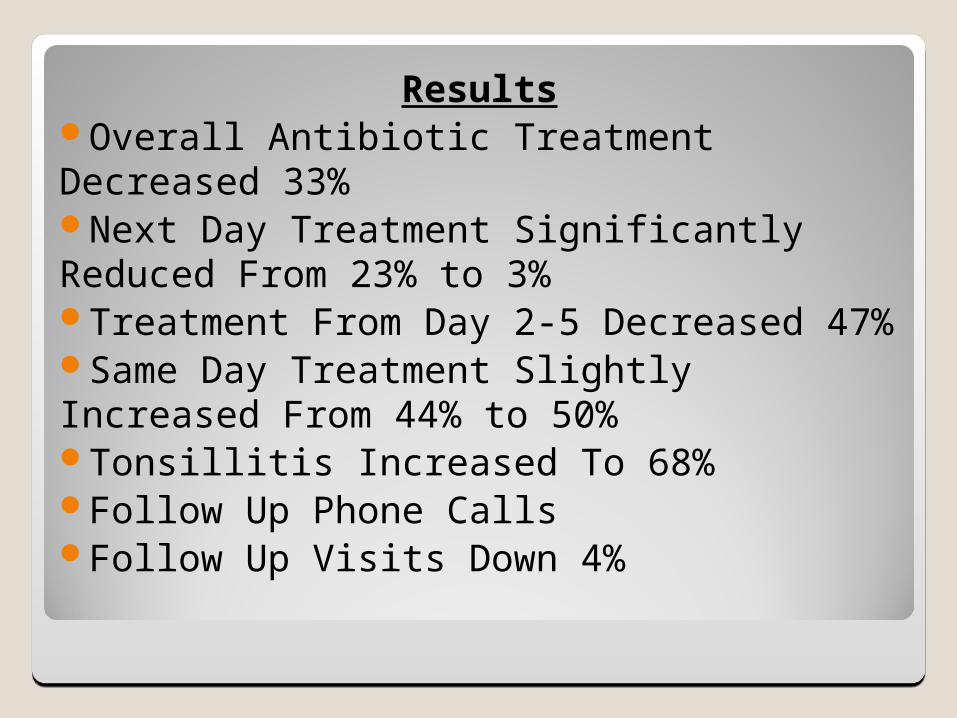
ResultsOverall Antibiotic Treatment Decreased 33%Next Day Treatment Significantly Reduced From 23% to 3%Treatment From Day 2-5 Decreased 47%Same Day Treatment Slightly Increased From 44% to 50%Tonsillitis Increased To 68%Follow Up Phone CallsFollow Up Visits Down 4%

Performance Goal Comparison
Goal: 70% TreatedPerformance: 60% Treated
Goal: 10% Treated/Next DayPerformance 3% Treated/Next Day
Goal: 10% Treated/Day2-5Performance 7% Treated/Day 2-5
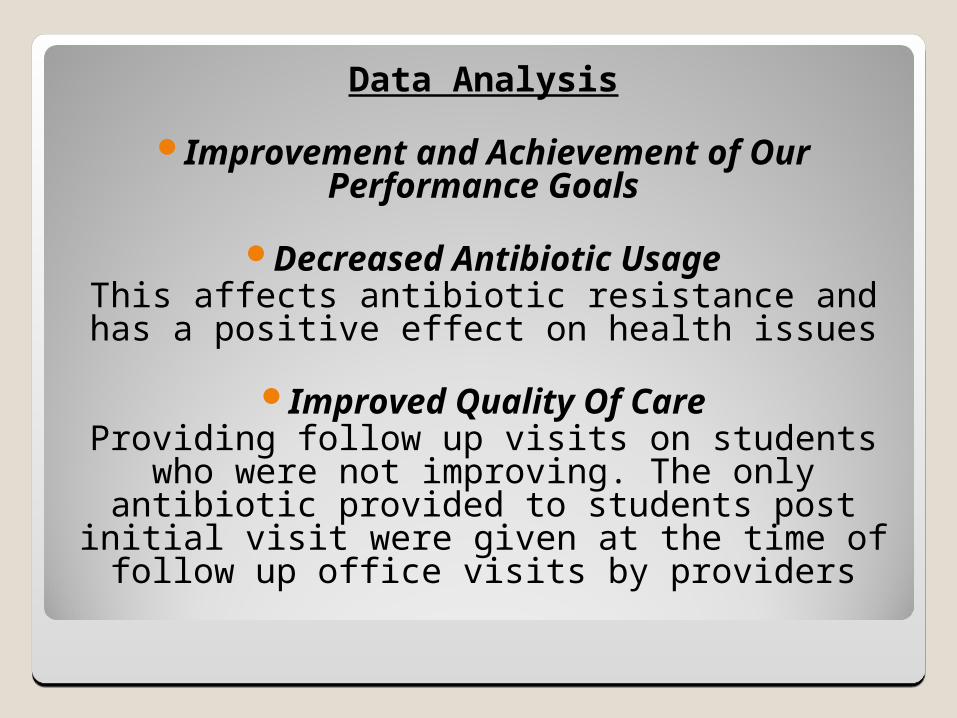
Data Analysis
Improvement and Achievement of Our Performance Goals
Decreased Antibiotic UsageThis affects antibiotic resistance and has a
positive effect on health issues
Improved Quality Of CareProviding follow up visits on students who were not improving. The only antibiotic provided to
students post initial visit were given at the time of follow up office visits by providers
Limitations Of Assessment
Strep C Only/QI Assessment
College Health
Clinical Judgment
Tonsillitis and Mononucleosis
FUTURE STUDY
Comparing Group A Clinical Presentation to Group C Presentation
Centor Criteria
Predictive Method to Diagnosis Strep A
Relationship In Predicting Strep C
Centor Criteria
Set of 4 criteria which may be used to identify the likelihood of a Group A Strep infection in patients complaining of pharyngitis.
It is a method that can be used to quickly diagnosis the probability of Strep A.
Based On 4 Criteria
Fever ≥100.5
Absence Of Cough
Tonsillar Exudate
Tender Anterior Cervical Adenopathy
Centor Criteria
Score 0-1: less than 10% ProbabilityNot worthwhile to test.
Score 2-3: Intermediate Probability
Score of 2, 15% Prob.Score of 3, 32% Prob.RSA test done.You can follow with a throat cx.
Score 4: 60% ProbabilityConsider empiric antibiotic Rx. Some perform a RSA.
Presence of all 4 criteria: 40-60% prob. of GAS present
Absence of all 4 criteria: negative predictive value of greater than 80% GAS not present
High predictive value – Better at ruling out rather than ruling in strep throat.

Centor Criteria/application to testing on students with pharyngitis and Group C BHS
Pharyngitis/ Centor Criteria EHR
Implementation of guidelines for treatment of Group C BHS in the college population
Throat Facts8/1/12-5/15/13
Point Of Care1,425
Rapid Strep In Lab53
Back Up Throat Cultures In Lab401








![Publication List: Professor Valerie Gibsongibson/pubs.pdf · 2017-08-31 · 66. “Amplitude analysis of B− → D+π−π− decays” R. Aaij et al. [LHCb Collaboration]. arXiv:1608.01289](https://static.fdocument.org/doc/165x107/5fb37c1f3e7ef127ed5f9cfc/publication-list-professor-valerie-gibson-gibsonpubspdf-2017-08-31-66-aoeamplitude.jpg)