Tissue Response to Biphasic Calcium Phosphate Ceramic With Different Ratios of HA/βTCP in...
7
729 Tissue Response to Biphasic Calcium Phosphate Ceramic With Different Ratios of HA/ßTCP in Periodontal Osseous Defects Edmundo . Nery, * Racquel Z. LeGeros,f Kenneth L. Lynch, * and Kelvin Lee% The purpose of this study was to determine the optimal ratio of calcium hydroxyapatite (HA) to beta tricalcium phosphate (ßTCP) in a biphasic porous calcium phosphate (BCP) ceramic for effective repair of periodontal osseous defects. Defects were surgically pro- duced in beagle dogs and made chronic for 4 months to simulate periodontal disease. Mucoperiosteal periodontal flaps were reflected, followed by osseous defect debridement and root planing. Specially prepared ceramic with different HA/ßTCP ratios were im- planted into the prepared defects. The sites were allowed to heal for 6 months, animals were euthanized, and site-blocks were removed for histological study. During the follow- up phase, scaling and polishing were done once a month, and standardized probing attachment levels were recorded pre- and 6-months postoperatively. The Duncan's mul- tiple range test showed that all the treatments produced statistically significant higher gain in probing attachment levels than the control group (OHA/OßTCP) ( <0.05). Among the 7 "active" treatment groups, 2 (65/35 and 85/15) had significantly higher gain in probing attachment levels than those in 3 groups (50/50, 100/0, and 0/100) (P < 0.05). Histologically, higher HA ratio (but not 100% HA) showed accelerated new bone formation and new attachment levels. Based on histological results, the 85HA/ 15 ßTCP ratio appears to demonstrate greater gain in attachment level and bone regen- eration in the treatment of periodontal osseous defects. /Periodontal 1992; 63:729-735. Key Words: Periodontal diseases/therapy; bone loss/therapy; beta tricalcium phosphate/ therapeutic use Calcium phosphate ceramics have long been investigated as applied to biological systems.1'2 The most widely used are the dense hydroxyapatite (HA) and the beta tricalcium phosphate (ßTCP) ceramics. Both are biologically com- patible and have been used in the treatment of periodontal osseous defects.3 7 Early reports have shown that HA par- ticles did not elicit an inflammatory response and that they provided a scaffold for the new bone to grow. However, it has been shown that HA failed to show evidence of new periodontal tissue attachment, Osteogenesis, or cemento- genesis in the treatment of periodontal osseous defects;810 'Clement J. Zablocki V.A. Medical Center, Dental Research Section Mil- waukee, WI. fNew York University Dental Center Office of Research Program, New York, NY. Medicai College of Wisconsin, Department of Orthopaedic Surgery, Mil- waukee, WI. §V.A. Medical Center, Cooperative Studies Program Coordinating Center, Palo Alto, CA. instead, it was believed that the material produced a re- sponse like a well-tolerated foreign body within the host connective tissue. While ßTCP was reported to form bone within the periodontal osseous defects,3,4 new periodontal attachment was questionable. The material was also found to resorb unpredictably in biologic fluids and in a variety of solvents.11,12 Therefore, ßTCP may not provide a pre- dictable scaffold for new bone to grow. The development of a 2-phased calcium phosphate or biphasic calcium phosphate ceramic (BCP) made it possible to control the resorbability of the material and at the same time maintain its osteoconductive property. X-ray powder diffraction of the material showed a ratio of approximately 60% hydroxyapatite to 40% beta tricalcium phosphate. Early studies have shown that this estimated ratio seems to pro- vide a bone conductive property.10'13 However, the opti- mum ratio of HA to ßTCP is still not known. The purpose of this study was to evaluate the tissue response to different ratios of each of these crystalline entities in combination
Transcript of Tissue Response to Biphasic Calcium Phosphate Ceramic With Different Ratios of HA/βTCP in...

729
Tissue Response to Biphasic CalciumPhosphate Ceramic With DifferentRatios of HA/ßTCP in PeriodontalOsseous DefectsEdmundo . Nery, * Racquel Z. LeGeros,f Kenneth L. Lynch, * and Kelvin Lee%
The purpose of this study was to determine the optimal ratio of calcium hydroxyapatite(HA) to beta tricalcium phosphate (ßTCP) in a biphasic porous calcium phosphate (BCP)ceramic for effective repair of periodontal osseous defects. Defects were surgically pro-duced in beagle dogs and made chronic for 4 months to simulate periodontal disease.Mucoperiosteal periodontal flaps were reflected, followed by osseous defect debridementand root planing. Specially prepared ceramic with different HA/ßTCP ratios were im-planted into the prepared defects. The sites were allowed to heal for 6 months, animalswere euthanized, and site-blocks were removed for histological study. During the follow-up phase, scaling and polishing were done once a month, and standardized probingattachment levels were recorded pre- and 6-months postoperatively. The Duncan's mul-tiple range test showed that all the treatments produced statistically significant highergain in probing attachment levels than the control group (OHA/OßTCP) ( <0.05).Among the 7 "active" treatment groups, 2 (65/35 and 85/15) had significantly highergain in probing attachment levels than those in 3 groups (50/50, 100/0, and 0/100) (P< 0.05). Histologically, higher HA ratio (but not 100% HA) showed accelerated newbone formation and new attachment levels. Based on histological results, the 85HA/15 ßTCP ratio appears to demonstrate greater gain in attachment level and bone regen-eration in the treatment of periodontal osseous defects. /Periodontal 1992; 63:729-735.
Key Words: Periodontal diseases/therapy; bone loss/therapy; beta tricalcium phosphate/therapeutic use
Calcium phosphate ceramics have long been investigatedas applied to biological systems.1'2 The most widely usedare the dense hydroxyapatite (HA) and the beta tricalciumphosphate (ßTCP) ceramics. Both are biologically com-
patible and have been used in the treatment of periodontalosseous defects.3 7 Early reports have shown that HA par-ticles did not elicit an inflammatory response and that theyprovided a scaffold for the new bone to grow. However, ithas been shown that HA failed to show evidence of new
periodontal tissue attachment, Osteogenesis, or cemento-genesis in the treatment of periodontal osseous defects;810
'Clement J. Zablocki V.A. Medical Center, Dental Research Section Mil-waukee, WI.fNew York University Dental Center Office of Research Program, NewYork, NY. Medicai College of Wisconsin, Department of Orthopaedic Surgery, Mil-waukee, WI.§V.A. Medical Center, Cooperative Studies Program Coordinating Center,Palo Alto, CA.
instead, it was believed that the material produced a re-
sponse like a well-tolerated foreign body within the hostconnective tissue. While ßTCP was reported to form bonewithin the periodontal osseous defects,3,4 new periodontalattachment was questionable. The material was also foundto resorb unpredictably in biologic fluids and in a varietyof solvents.11,12 Therefore, ßTCP may not provide a pre-dictable scaffold for new bone to grow.
The development of a 2-phased calcium phosphate or
biphasic calcium phosphate ceramic (BCP) made it possibleto control the resorbability of the material and at the sametime maintain its osteoconductive property. X-ray powderdiffraction of the material showed a ratio of approximately60% hydroxyapatite to 40% beta tricalcium phosphate. Earlystudies have shown that this estimated ratio seems to pro-vide a bone conductive property.10'13 However, the opti-mum ratio of HA to ßTCP is still not known. The purposeof this study was to evaluate the tissue response to differentratios of each of these crystalline entities in combination

730 BIPHASIC CALCIUM PHOSPHATE CERAMIC IN PERIODONTAL DEFECTSJ Periodontol
September 1992
Table 1. Treatment Groups With Corresponding Ratios of HA andßTCP
Ratio Number of TotalGroup (HA/ßTCP) Dogs (Sites) Sites1 100/0 2 (8) 162 85/15 3 (8) 243 65/35 3 (8) 244 50/50 3 (8) 245 35/65 3 (8) 246 15/85 3 (8) 247 0/100 2 (8) 16Control 0/0 2(8) 16
with each other so that the most desirable ratio could bedetermined for optimum bone conductivity and healing ofperiodontal tissue components.
MATERIALS AND METHODSBiphasic calcium phosphate ceramic was prepared by sin-tering apatitic calcium phosphates prepared under differentconditions.14"16 The HA/ßTCP ratio was determined fromthe x-ray diffraction patterns using the method previouslydescribed.14 Macroporosity was introduced by the additionof napthalene according to Hubbard.13
Twenty-one adult beagle dogs were used in this study.They were divided into 8 groups
-
3 dogs for 5 of the ratios,and 2 dogs for the other 3 (Table 1). This experiment was
approved by the V.A. Animal Studies Subcommittee inaccordance with established guidelines in the use of exper-imental animals.
Under sodium pentobarbital anesthesia (30mg/kg,IV) thefollowing teeth were extracted to provide space for the sur-
gical production of periodontal osseous defects: the rightand left maxillary and mandibular 4th premolar, and theright and left mandibular 3rd lateral incisor. Since a widediastema naturally exists between the maxillary canine andlateral incisors of dogs, no extraction was necessary. Afterextraction, 3-walled intrabony defects were surgically cre-ated at the mesial aspect of the maxillary and mandibular1st molars and canines. These defects were made chronicfor 16 weeks with stainless steel ligature wire and braidedsilk sutures as described in a previous report.17 The wireswere then removed, the surgical sites scaled and polished,and the areas were allowed to heal for 2 weeks.
Prior to implanting the ceramic, a "T" groove with ver-tical and horizontal grooves, was cut on the mesial aspectof each of the study teeth. The horizontal served as a ref-erence landmark for measuring the attachment level, whilethe vertical allowed the consistent alignment of the wireprobe with the osseous defect. Following placement of thegroove, the pre-implantation probing attachment level wasmeasured with a 0.016" diameter stainless steel orthodonticround wire, approximately 20 mm in length. The wire wasthen inserted into the defect with the use of a standardizedO'Neil spring gauge11 set at 25 ponds of force (1 pond = 1
"Instrument and Machine Shop, VAMC, Milwaukee, WI.
gram of force applied).18 While maintained in this position,the wire was clamped with a locking plier at the level ofthe apical part of the horizontal groove. This was then re-moved and immediately transposed to a millimeter ruler toobtain the measurement.
For the implantation procedure, mucoperiosteal peri-odontal flaps were reflected, followed by debridement andthorough root planing. The area was irrigated with normalsaline solution, then dried with 2x2 sponges. The ceramicwas mixed with normal saline solution in a sterile dappendish, and the excess was blotted out with sponges. Theceramic was then delivered into the defect with an amalgamcarrier and packed lightly with an amalgam plugger. Weattempted to approximate the buccal and lingual flaps witha resorbable suture material.
Postoperatively, the animals were given antibiotics (ce-fazolin 24mg/kg,IM) and a soft diet for 7 consecutive daysafter which an oral hygiene regimen was initiated underInnovar-Vet (0.1ml/kg,IM). This was repeated once a monthfor 6 months.
The same surgical procedure was accomplished in thecontrol group, except that no implant material was placedinto the defect.
At the 6-months post-implantation period, the probingattachment level was again measured. The animals werethen euthanized with an overdose of sodium pentobarbital.The experimental as well as the control sites were retrievedfor histologie evaluation. All specimens were fixed in 10%buffered formalin, decalcified with 10% Na2EDTA (pH 7.3),sectioned serially in mesiodistal direction at 8 µ thick-ness, and stained with hematoxylin and eosin. All histo-logical sections described in this text were representativesof the mid-section of the osseous defect.
Statistical AnalysisEight treatments were investigated, with 2 or 3 dogs as-
signed to each treatment. For each dog, 8 teeth were se-lected for measurement. However, some teeth were excluded,9 where the osseous defects had inadvertently extended intothe sinus cavity during chronic induction and 5 which wereretained for microdensitometric analysis and hence, un-available for results in this study. The probing attachmentlevel for each tooth was measured preoperatively as wellas 6 months postoperatively. Since measurements taken onteeth within the same dog will tend to correlate with eachother, we took into account this correlation by performinga repeated measures analysis of variance, using the generallinear model (GLM) procedure of SAS. Treatment com-
parisons were performed by using the Duncan's multiplerange test.19
RESULTSAll treatment and control sites healed uneventfully with noclinical evidence of inflammatory response to the ceramicimplant.
The analysis of variance showed that, for treatment com-

Volume 63Number 9
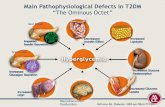
Figure 1. Section of the implant site with 85HA/I5ßTCP ceramic showingnew attachment level (NA) and accelerated new bone formation aroundthe ceramic particles (C); also shows old bone (B) indicating the originalbase of the pocket prior to implant procedure (H&E; original magnifi-cation, 10).
Table 2. Mean Preoperative Probing Attachment Level and 6Month Postoperative Gain
HA/BTCP Number of Dogs Preoperative GainRatio (total sites) Mean ± SE Mean ± SE
100/0 2 (16) 10.3 ±0.6 3.9 ±0.585/15 3 (22) 11.3 ±0.5 5.3 ±0.465/35 3 (20) 10.8±0.4 5.4±0.550/50 3 (21) 10.0 ±0.6 4.0 ±0.635/65 3 (20) 9.2 ±0.7 4.2 ±0.715/85 3 (23) 10.3 ±0.5 4.5 ±0.40/100 2 (16) 8.8 ±0.5 3.3 ±0.50/0 2(16) 10.6 ±0.8 1.8 ±0.3
NERY, LeGEROS, LYNCH, LEE 731
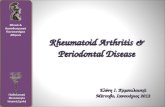
Figure 2. Higher magnification of Figure I showing new cementum (CE)with inserting collagen fibers (CF), vascularity (V), and new bone for-mation (B) enfolding the ceramic particles (C) (H&E; original magnifi-cation, X 160).
parisons, at least one of the treatment groups was differentfrom the others. The Duncan multiple range test showedthat all the treatments produced statistically significant highergain in probing attachment levels than did the control groups(OHA/OßTCP) ( <0.05). Among the "active" treatmentgroups, 2 of them (65/35 and 85/15) had significantly highergains in probing attachment levels than those in 3 groups(50/50, 100/0, and 0/100) (P <0.05). The preoperativeprobing attachment level and the 6-month postoperative gainare shown in Table 2.
Histologically, although no quantitative measurementswere made, the amount of bone regeneration and new at-tachment of periodontal tissues appear to be greater in spec-imens with a ratio of 85HA/15ßTCP as compared to othertreatments. This is shown in Figure 1 which depicts accel-erated new bone formation around the ceramic particles andnew attachment level as evidenced by cementum formationand inserting collagen fibers (Fig. 2). This new attachmentwas found at the same level as the ceramic implant materialindicating that the root surface of the tooth was denudedprior to implantation. Along the root surface of the toothsmall areas of ankylosis could also be found (Fig. 3). In

732 BIPHASIC CALCIUM PHOSPHATE CERAMIC IN PERIODONTAL DEFECTSJ Periodontol
September 1992
Figure 3. Higher magnification of Figure I showing ankylotic formation(A) on old cementum (CE). Note that the ankylosed bone appears to
originate from the same bone that was formed around the ceramicparticles(C) (H&E; original magnification, 50).
the lOOHA/OßTCP ratio group, a similar reaction of newbone formation and new attachment level was seen. How-ever, the tissue appears to demonstrate a decrease in osteo-blastic activity and some of the ceramic particles were simplysurrounded with fibrous connective tissue (Fig. 4). As theproportion of ßTCP increases, osteoclastic activity also in-creases with concomitant ceramic résorption as evidencedby the presence of numerous multinucleated giant cells (Fig.5) and fewer ceramic particles present in the implant site.The bone surrounding some of the unresorbed ceramic par-ticles showed an irregular inner surface indicating that ré-
sorption or dissolution process of the ceramic took placeprior to laying down of mineralized bone matrix (Fig. 6).This is in contrast with the relatively smooth appearinginner surface found in higher proportion of HA ceramic(Fig. 7). A collapse of underlying connective tissue, ac-
companied with a long junctional epithelium was a common
finding in defects treated with the OHA/lOOßTCP ratio, butnew attachment could still be demonstrated in some of thespecimens examined (Fig. 8). In the control group, markedrecession of the gingival tissue with a long junctional epi-thelium as in OHA/lOOßTCP group was also seen. The bone
Figure 4. Section of the implant site with 100HAI0ßTCP ceramic showingdecreased osteoblastic activity. Most of the ceramic particles (C) are
surrounded with fibrous connective tissue but some showed appositionalosteoid seams (O); and evidence of new cementum formation (CE) (H&E;original magnification, 50).
Figure 5. Higher magnification of a ceramic particle (C) with 65HAI35ßTCP ratio juxtaposed with multinucleated giant cells (G) (H&E; orig-inal magnification, x 400).

Volume 63Number 9 NERY, LeGEROS, LYNCH, LEE 733
Figure 6. Section of 15HAI85ßTCP ceramic particles (C) showing irreg-ular inner surface ofnew bone ( ) (H&E; original magnification, X 160).
showed large marrow spaces with no evidence of activebone formation (Fig. 9).
DISCUSSIONThe results of the study indicated that the ratio of HA toßTCP in the ceramic implant influenced periodontal woundhealing when used in the treatment of chronic osseous de-fects in dogs. Although the clinical probing attachment levelin this study showed no statistically significant differencebetween treatment groups (different ratios), they appear todemonstrate a pattern; i.e., higher HA ratio to ßTCP tendedto show greater gain in attachment level accompanied byaccelerated new bone formation as shown histologically.When ßTCP was removed from the ceramic component,using only 100% porous HA, the gain was found to be lessthan that of the groups that received ceramic containingßTCP. This may be due to the low dissolution rate of po-rous HA.15'16 Others have reported that porous HA has noosteoinductive capability20'21 and that it has been identifiedas having a "benign" reaction with tissues.22 It would seemthat the HA material evokes a mild cellular activity thatcould perhaps compromise repopulation of osteogenic cellsas well as the periodontal ligament cells needed for theproduction and attachment of new periodontal tissues to
Figure 7. Section of WOHA/OßTCP ceramic particles (C) showing rela-tively smooth inner surface of bone (B) (H&E; original magnification, x
160).
previously denuded root surfaces. Since this study showedthat the combination of HA and ßTCP has better new at-tachment level and bone regeneration, it would indicate thatßTCP plays an important role in cell proliferation, revas-
cularization, and Osteogenesis. However, when the oppositeend of the ratio was examined; i.e., OHA/lOOßTCP, prob-ing attachment level was also found to be less than thegroup that received the ceramic with HA. This may also bedue to the dissolution factor of the ceramic: ßTCP resorbsmore readily than HA in vitro23'24 or in vivo11'15,16'25"27which is consistent with the present study where most ofthe 100% ßTCP particles disappeared within a period of 6months. A collapse of the overlying connective tissues witha very minimal new periodontal attachment level and boneregeneration was also observed. This ceramic does not stayin the tissue long enough for cell differentiation, matura-tion, and a much needed revascularization. It is believedthat the sequence of events involve chemotactic attractionand activation of histiocyte and mononuclear cell macro-
phages, as well as multinucleated giant cells followed byrésorption. This rapid disappearance may then be the resultof cell mediated phagocytosis or biologic chemical disso-lution, or both.16 It is, therefore, not an ideal scaffolding

J Periodontol734 BIPHASIC CALCIUM PHOSPHATE CERAMIC IN PERIODONTAL DEFECTS September 1992
Figure 8. Section of an implant site with OHA/lOOßTCP ceramic showing Figure 9. A control section showing a collapse of overlying connectivemarked bone résorption with few remaining ceramic particles (C). Note tissues (arrow) with long functional epithelium (JE). The bone shows a
the long functional epithelium (JE), the parallel orientation of collagen large marrow space (M) with no evidence ofactive bone formation (H&E;fibers (CF), and the root résorption (arrow) (H&E; original magnifica- original magnification, x 10).tion, X 10).
material when used alone for the repair of periodontal os-seous defects. Although ßTCP is an important componentof ceramic implants, the higher proportion of ßTCP wouldtend to decrease its effectiveness for tissue regeneration.
The presence of small areas of ankylosis in some of thespecimens that we examined may not be regarded as a pos-itive result. However, as described in our previous report,17in fully erupted permanent dentition, ankylosis seldommanifests clinical symptoms and requires no treatment un-
less there is an underlying problem, such as pulp infec-tion.28 It is believed to be associated with excessivemasticatory pressure or trauma to periodontal tissues.29 Inthis study trauma may be the causative factor, but partici-pation of osteogenic cells originating from the surroundingbone during healing should not be ruled out.
Despite the limitation of this study because of small sam-
ple size, we nevertheless believe that the combination ofHA and ßTCP in the ceramic implant is essential in en-
hancing repopulation of cells, new periodontal tissue at-

Volume 63Number 9 NERY, LeGEROS, LYNCH, LEE 735
tachment, and bone regeneration within the space of a
periodontal osseous defect. It has been hypothesized thatthe biphasic nature of this ceramic provides two basic func-tions: 1) initiates cell growth and differentiation; and 2)acts as a scaffold for cell maturation and bone formation;i.e., having the property of osteoinductivity.30 It may alsobe hypothesized that adequate retention time (less résorp-tion time) of BCP ceramic material in the area may providea barrier for the apical migration of the dento-gingival ep-ithelial cells. This was evidenced by the short junctionalepithelium found in higher HA ratio to ßTCP.
Based on histological results the 85HA/15ßTCP ratio ap-pears to demonstrate greater gain in attachment level andbone regeneration. However, further experimentation withincreased sample size is needed.
AcknowledgmentsThis study was supported by the Zimmer Corporation, War-saw, IN; NIH/NIDR Research Grant DE04123; MedicalCollege of Wisconsin, Department of Orthopaedic Surgery;and Zablocki V.A. Medical Center. The authors are gratefulto Dr. R.L. Van Swol for his comments and criticism; Dr.Tsau Ho for performing the initial statistical processing;Dr. A.A. Rimar for his advice on statistical processing; Dr.Phil Anderson for making the ceramic porous; Inta Lacitisfor preparing the histological materials; Dave Wimmer forpreparing the illustrations; and Joe Nery for his technicalassistance.
REFERENCES1. Levitt SR, Grayton PH, Monroe EA, Condrate RA. Forming method
for apatite prosthesis. J Biomed Mater Res 1969; 3:683.2. Monroe EA, Votava W, Bass DB, McMullen J. New calcium phos-
phate ceramic material for bone and tooth implants. J Dent Res 1971;50:860.
3. Levin MP, Getter L, Adrian J, Cutright DE. Healing of periodontaldefects with ceramic implants. / Clin Periodontol 1974; 1:197.
4. Levin MP, Getter L, Cutright DE, Bhaskar SN. Biodegradable ce-ramic in periodontal defects. Oral Surg Oral Med Oral Pathol 1974;38:344.
5. Robalais ML Jr, Yukna RA, May ET. Evaluation of Durapatite ce-ramic as an alloplastic implant in periodontal osseous defect. I: Initialsix-month results. J Periodontol 1981, 52:680.
6. Yukna RA, Harrison BG, Caudill RF, Evans GH, Mayer ET, MillerS. Evaluation of Durapatite ceramic as an alloplastic implant in peri-odontal osseous defects. II: Twelve month reentry results. J Peri-odontol 1985; 56:540.
7. Yukna RA, Kossingham RJ, Caudill RF, et al. Six-month evaluationof calcitite (hydroxyapatite ceramic) in periodontal osseous defects.Int J Periodontics Restorative Dent 1986; 6(3):34.
8. Froum SJ, Kushner L, Scopp IW, Stahl SS. Human clinical andhistologie response to Durapatite implants and intraosseous lesions.Case report. / Periodontol 1982; 53:719.
9. Moskow BS, Lubarr A. Histologie assessment of human periodontaldefects after Durapatite ceramic implant. /Periodontol 1983; 54:455.
10. Ellinger RF, Nery EB, Lynch KL. Histological assessment of peri-odontal osseous defects following implantation of hydroxyapatite andbiphasic calcium phosphate ceramic. A case report. Int J PeriodonticsRestorative Dent 1986; 6(3):223.
11. Jarcho M. Calcium phosphate ceramics as hard-tissue prosthetics.Clin Ortho Rei Res 1981; 157:259.
12. Jarcho M. Biomaterial aspect of calcium phosphates (properties andapplications). Dent Clin Am 1986; 30:25.
13. Hubbard WG. Physiological calcium phosphate as orthopedic bio-materials. PhD Thesis, Marquette University, Milwaukee, 1974.
14. LeGeros, RZ. Variability of ßTCP/HA ratios in sintered 'apatite'. JDent Res 1986;65 (Spec. Issue):292 (Abstr. 1110).
15. LeGeros RZ, Daculsi G. In-vivo transformation of biphasic calciumphosphate ceramics. In: Yamamuro T, Hench L, Wilson-Hench J,eds. CRC Handbook of Bioactive Ceramic, Vol. 2. Boca Raton, FL:CRC Press; 1990: 17-28.
16. Daculsi G, LeGeros RZ, Nery EB, Lynch KL, Kerebel B. Transfor-mation of calcium phosphate ceramics in vivo: Ultrastructural andphysicochemical characterization. J Biomed Mat Res 1989; 23:883.
17. Nery EB, Eslami A, Van Swol RL. Biphasic calcium phosphate ce-
ramic combined with fibrillar collagen with and without citric acidconditioning in the treatment of periodontal osseous defects. / Per-iodontol 1990; 61:166.
18. Vitek RM, Robinson PJ, Lautenschlager EP. Development of a forcecontrolled periodontal probing instrument. JPeriodontol 1979; 14:93.
19. Duncan DB. T-test and intervals for comparisons suggested by thedata. Biometrics 1975; 31:339.
20. Piecuch JF. Extraskeletal implantation of a porous hydroxyapatiteceramic. / Dent Res 1982; 61:1458.
21. Itatani C, Marshall GJ. Cellular responses to implanted replamineformhydroxyapatite. Trans Orthoped Res Soc 1984; 9:123.
22. White E, Shors EC. Biomaterial aspects of Interpore-200 porous hy-droxyapatite. Dent Clin Am 1986; 30:49.
23. LeGeros RZ. Calcium phosphate materials in restorative dentistry: Areview. Adv Dent Res 1988; 2:164.
24. LeGeros RZ. Properties of commercial bone grafts compared to hu-man bone and new synthetic bond biomaterials. Proceedings of theNinth Annual Meeting of the Society for Biomaterials. Birmingham,AL. 1983:86.
25. DeGroot K. Bioceramic of Calcium Phosphate. Boca Raton FL: CRCPress; 1983:91.
26. Osbom JF. Implantatwerkstoff hydroxylapatit keramic grundlagen undklinische anwendung. Quintessenz Verlags GmbH, Berlin, 1985.
27. Metsger DS, Driskill TD, Paulsrad JR. Tricalcium phosphate ceramic
-
a resorbable bone implant: Review and current status. J Am DentAssoc 1982; 105:1035.
28. Shafer WB, Hine MK, Levy BM. Oral Pathology, 4th ed. Philadel-phia: W.B. Saunders Co.; 1983: 540-541.
29. Biederman WB. The problems of the ankylosed tooth. Dent Clin Am 1968; 12:409-429.
30. Lynch KL, Toth JM, Hamson KR, Ho KC, Hirthe WM. Osteoin-ductivity by subcutaneous implant of a fibrillar collagen and a calciumphosphate ceramic composite. Proceedings of Third InternationalSymposium on Ceramics in Medicine. Bioceramics 1992; 3:295-304.
Send reprint requests to: Dr. E.B. Nery, Dental Research Section, ClementJ. Zablocki V.A. Medical Center, Milwaukee, WI 53295
Accepted for publication March 24, 1992.