Effect of the examination stress on periodontal health status and salivary IL-1β among Iraqi dental...
133
Effect of the examination stress on periodontal health status and salivary IL-1β among Iraqi dental students A thesis submitted to the council of the College of Dentistry at the University of Baghdad, in partial fulfillment of the requirements for the degree of Master of Science in Periodontics By Athraa Ali Mahmood B.D.S. Supervised by Prof. Dr. Leka'a M. Ibrahim B.D.S., M. Sc. October/ 2013 Dhu al-Hijjah / 1434
-
Upload
hashim-moeen -
Category
Health & Medicine
-
view
34 -
download
11
Transcript of Effect of the examination stress on periodontal health status and salivary IL-1β among Iraqi dental...

Effect of the examination stress on
periodontal health status and salivary
IL-1β among Iraqi dental students
A thesis submitted to the council of the College of Dentistry at
the University of Baghdad, in partial fulfillment of the
requirements for the degree of Master of Science in
Periodontics
By
Athraa Ali Mahmood
B.D.S.
Supervised by
Prof. Dr. Leka'a M. Ibrahim
B.D.S., M. Sc.
October/ 2013 Dhu al-Hijjah / 1434



Approved by the council of the college of Dentistry/ University of Baghdad.
Prof. Dr. Nabeel abdul-Fatah
B.D.S., M.Sc. (Prosthodontics) UK
Dean of the college of Dentistry
University of Baghdad
Committee Certification
We, the members of the examining committee, certify that we
have read this thesis and examined the graduate student “Athraa Ali
Mahmood“ in its contents and in our opinion, it meets the standard of thesis
for the degree of Master of Science in Periodontics.
Assist. Prof. Dr. Maha Abdul Aziz Ahmed
B.D.S., M.Sc.
(The Chairman)
Assist. Prof. Dr. Batool Hassan Al-Ghurabei
B.S.C., M.Sc., Ph.D.
Member
B.D.S M.Sc.
Member
Assist. Prof. Dr. Kadhim Jawad Hanau
B.D.S., M.Sc.
Member

To my precious mother
& father
To my lovely Hashim
Dedication
Athraa…
To my sweet daughters
Retaj & Fatima
To my dear sisters &
brothers

I
Acknowledgement
First of all, I would like to thank almighty “ALLAH” for inspiring me the
energy, patience and strength to accomplish this work. A special peace to our
messenger Mohammed (peace be upon him).
My sincere appreciation to Prof. Dr. Nabeel abdul-Fatah, Dean of the
College of Dentistry, University of Baghdad, for continuously supporting the
postgraduate students.
My deepest thanks and admiration goes to Prof. Dr. Leka'a M. Ibrahim,
Head of Department of Periodontology and my supervisor, for her guidance, kindness,
high ethics, scientific support and continuous helpful advices throughout my study.
I would like to express my deep thanks and respect to the members of the
Department of Periodontology, Baghdad University; Dr. Maha Shukri, Dr. Basima
Ghafori, Dr. Maha Abdul Aziz, Dr. Saif Siham, Dr. Alaa Umran for their help and
encouragement through the study period.
I am highly indebted to the members of Department of Periodontology,
Almustansiriyah University; Dr. Kadhim Jawad, Dr. Ra'ad Aziz, Dr. Hussein Owaid,
Dr. Enas Razzoqi, for their valuable advices, support and continuous assistance.
Much thanks to Assistant Prof. Dr. Batool Hassan in Department of basic
science, Baghdad University, for her generous helpful throughout my study.
My mellifluous appreciation and gratitude to all medical staff of Department
of Immunology in Teaching Laboratories of Baghdad Medical City, especially Dr.
Nahla and Mr. Amjad, for their help in facilitating the performing of this work.
My thanks and appreciation to all the postgraduate colleagues in the
Department of Periodontology, for their cooperation throughout my study.
I gratefully acknowledge to the cooperation and participation of dental
students in this study.
Finally, I am unable to express my sincere gratitude, appreciations and love
to my dear husband (Dr. Hashim) and mother for their unlimited support and love.

II
Abstract
Background: Periodontal diseases are common chronic inflammatory diseases caused
by pathogenic microorganisms colonizing the gingival area and inducing local and
systemic elevations of pro-inflammatory cytokines resulting in tissue destruction by a
destructive inflammatory process affecting tooth-supporting tissues. Many local or
systemic risk factors contribute to development of periodontal disease, stress was
considered as one of the important factors that causes many inflammatory diseases
including periodontal disease. When the stress increase for long period, it may
influence inflammatory process leading to systemic or local diseases such as
periodontal disease.
Interleukin-1beta is a highly pro-inflammatory cytokine strongly associated
with periodontal disease. In addition, interleukin-1beta is a critical mediator of adaptive
stress responses as well as stress-associated neuropathology and psychopathology.
Aims of the study: To determine and compare clinical periodontal parameters (plaque
index, gingival index and bleeding on probing), stress level and salivary interleukin-
1beta level among dental students before, during and after mid-year exam periods. In
addition, to find the correlation among stress, salivary interleukin-1beta and clinical
periodontal parameters.
Materials and methods: The sample was consisted of twenty-four dental students;
twelve male and twelve female aged (21-23) years, they were examined in this follow
up study at three main periods:
First period at least one month before mid-year exam (Period I).
Second period during mid-year exam (Period II).
Third period at least one month after mid-year exam (Period III).
Depression Anxiety Stress Scale (DASS-21) was used to measure stress level
in all periods. Saliva samples were collected to determine the salivary interleukin-1beta
level by enzyme-linked immunosorbent assay (ELISA). Clinical periodontal

III
parameters were recorded at four sites per tooth including plaque index, gingival index
and bleeding on probing.
Results: The results showed that the means of all clinical periodontal parameters were
higher in the period II than in the periods I and III with highly significant differences
at (P ≤ 0.01). As well as, the means concentrations of salivary interleukin-1beta were
higher in the period II than in the periods I and III with highly significant differences
at (P ≤ 0.01). Also, by using Pearson's Correlation Coefficient, stress shows highly
significant strong positive correlation with the immunological parameter (salivary
interleukin-1beta) and clinical periodontal parameters at (P ≤ 0.01).
Conclusions: The results of this study provided strong evidence of association between
examination stress and periodontal disease, where dental students during mid-year
exam have higher levels of stress, clinical periodontal parameters and salivary
interleukin-1beta as compared with before and after mid-year exam periods. Also, there
were strong correlation among stress, salivary interleukin-1β and clinical periodontal
parameters.

IV
List of Contents
Page
No.
Subject
I Acknowledgement
II Abstract
IV List of Contents
VII List of Tables
VIII List of Figures
IX List of Abbreviations
1 Introduction
3 Aims of the study
Chapter One-Review of Literature
4 1.1. Periodontal diseases
4 1.1.1. Definition
5 1.1.2. Epidemiology
5 1.1.3. Pathogenesis of periodontitis
5 1.1.3.1. Bacterial factors
7 1.1.3.2. Host responses factors
8 I- Innate immune response
9 II-Adaptive immune response
10 1.1.3.3. Viral factors
10 1.1.3.4. Other risk factors
12 1.2. Stress
14 1.2.1. Stress scales
18 1.2.2. Molecular and endocrine mechanisms of the stress response
22 1.2.3. Behavioral changes of stress response
23 1.2.4. Stress and microbiology of periodontal disease
24 1.2.5. Role of stress on gingivitis
25 1.2.6. Role of stress on periodontitis
26 1.2.7. Role of stress on periodontal treatment
27 1.3. Saliva
28 1.3.1. Functions of saliva
29 1.3.2. Salivary composition
30 1.3.3. Saliva and diagnosis

V
31 1.3.4. Saliva and stress
32 1.4. Cytokines
34 1.4.1. Interleukin-1β
35 1.4.1.1. Interleukin-1β regulation of the periodontal ligament
36 1.4.1.2. Interleukin-1β and its role in periodontal disease
37 1.4.1.3. Stress-induced interleukin-1β production
Chapter Two-Materials and Methods
41 2.1. Materials
41 2.1.1. Instruments and Equipment
42 2.1.2. Test kit
42 2.2. Methods
42 2.2.1. Sample description
43 2.2.2. Exclusion criteria
43 2.2.3. Study design
44 2.2.4. Depression anxiety and stress scale
45 2.3. Clinical periodontal parameters examination
45 2.3.1. Plaque index
46 2.3.2. Gingival index
46 2.3.3. Bleeding on probing
46 2.4. Saliva sample collection and preparation
47 2.5. Detection of interleukin-1β
47 2.5.1. Test principle
48 2.5.2. Reagent preparation
49 2.5.3. Procedure
50 2.5.4. Calculations of interleukin-1β
50 2.6. Calibration
51 2.7. Statistical analysis
Chapter Three-Results
56 3.1. Descriptive statistical analysis of demographic data
56 3.2. Clinical periodontal parameters analysis
56 3.2.1. Plaque index
58 3.2.2. Gingival index
60 3.2.3. Bleeding on probing
62 3.3. Stress analysis
63 3.4. Salivary interleukin-1β statistical analysis

VI
65 3.5.Correlations between clinical periodontal parameters with
immunological marker (salivary interleukin-1β) and stress
Chapter Four-Discussion
67 4.1. Demographic data
68 4.2. Periodontal health status
68 4.2.1. Plaque index
69 4.2.2. Gingival index
69 4.2.3. Bleeding on probing
70 4.3. Stress data
71 4.4. Salivary interleukin-1β level
73 4.5. Correlations between stress, interleukin-1β and clinical periodontal
parameters
Chapter Five-Conclusions and Suggestions
74 5.1. Conclusions
75 5.2. Suggestions for further studies
References
76 References
Appendices
106 Appendices
الخالصة

VII
List of Tables
Page
No.
Table title Table
No.
15 DASS severity-rating index 1-1
15 DASS 42-item questionnaire version 1-2
17 DASS 21-item questionnaire version 1-3
29 Functions of saliva components 1-4
33 Effects attributed to cytokines identified in periodontal disease 1-5
45 Stress questionnaires of DASS 21-item version 2-1
45 DASS severity-rating index 2-2
56 Descriptive statistical results of students' ages 3-1
56 Descriptive statistical results of plaque index for each period 3-2
57 ANOVA test for plaque index 3-3
58 LSD test to compare the means of plaque index between each two
periods
3-4
58 Descriptive statistical results of gingival index for each period 3-5
59 ANOVA test for gingival index 3-6
60 LSD test to compare the means of gingival index between each
two periods
3-7
61 Percentages and numbers of scores of bleeding on probing for
each period and comparison among periods
3-8
61 Inter-period comparisons for bleeding on probing among periods 3-9
62 Percentages and numbers of stress range and comparison among
periods
3-10
63 Descriptive statistical results of interleukin-1β for each period 3-11
64 ANOVA test of interleukin-1β 3-12
64 LSD to compare the means of interleukin-1β between each two
periods
3-13
65 Person correlation coefficient of salivary interleukin-1β with
plaque index, gingival index, bleeding on probing score (1 and 0)
and stress levels among periods
3-14
66 Person correlation coefficient of stress with salivary interleukin-
1β and plaque index, gingival index, bleeding on probing score (1
and 0) among periods
3-15

VIII
List of Figures
Page
No.
Title Figure
No.
7 Schematic illustration of the pathogenesis of periodontitis 1-1
21 Effects of stress on hypothalamic pituitary adrenal axis 1-2
21 Physiological model of effects of stress on periodontal disease 1-3
23 Psychosocial stress and its effect on behavior as manifested
by alterations in periodontal disease
1-4
40 Interleukin 1 mediates stress-induced activation of the
hypothalamic pituitary adrenal axis. Immunological and
psychological stressors increase the levels of interleukin 1
1-5
52 Salimetrics salivary interleukin-1β kit 2-1
52 A. Adjustable micropipettes and pipettes yellow tips
B. Adjustable micro multichannel pipettes
2-2
52 Centrifuge (Kokusan Corporation –Japan) 2-3
53 Auto vortex mixer (Frost instrument LTD, Great Britain) 2-4
53 A. Rotatest shaker (R 100 Luck ham, England)
B. Microtitre plate of interleukin-1β kit
2-5
53 Microplate ELISA washer device (Human, Germany) 2-6
54 Microtitre plate of interleukin-1β kit after adding stop solution 2-7
54 Microplate ELISA reader device (Human, Germany) 2-8
55 Quadratic parameter curve fit of software program 2-9
57 Bar chart graph for means of plaque index for each period 3-1
59 Bar chart graph for means of gingival index for each period 3-2
61 Bar chart graph for percentages of scores of bleeding on
probing for each period
3-3
63 Bar chart graph for means of interleukin-1β for each period 3-4
65 Bar chart graph for correlations of interleukin-1β with (plaque
index, gingival index, bleeding on probing score (1)) and
stress
3-5
66 Bar chart graph for correlations of stress with (plaque index,
gingival index, bleeding on probing score (1)) and interleukin-
1β
3-6

IX
List of Abbreviations
Aggregatibacter actinomycetemcomitans A. actinomycetemcomitans
Adrenocorticotropic hormone ACTH
Analysis of variance ANOVA
Acute necrotizing ulcerative gingivitis ANUG
Bleeding on probing BOP
Degree of centigrade ºc
Cluster of differentiation CD
Central nervous system CNS
Chronic periodontitis CP
Corticotropin releasing hormone CRH
Depression anxiety stress scale DASS
example e.g.
Enzyme-linked immunosorbent assay ELISA
Glucocorticoids GC
Gingival crevicular fluid GCF
Gingival index GI
Interleukine-1 receptor antagonist IL-1ra
Human cytomegalovirus HCMV
Hypothalamic pituitary adrenal HPA
Horseradish peroxidase HRP
Highly significant HS
Interferon IFN
Immunoglobulin Ig
Interleukin-1 IL-1
Interleukin-1beta IL-1β
Interleukin-10 IL-10
Lipopolysaccharide LPS
Least significant differences LSD
Maximum Max.
Membrane Cluster of differentiation mCD
Minimum Min.
Milliliter ml
Matrix metalloproteinases MMPs

X
Natural killer cell NK
Nanometer nm
Number No.
Non-significant NS
Optical density OD
Pathogen associated molecular pattern PAMPs
Periodontal diseases PD
Periodontal ligament PDL
Prostaglandin E2 PgE2
Porphyromonas gingivalis P. gingivalis
Prevotella intermedia P. intermedia
Picogram per milliliter pg/ml
Plaque index PLI
Polymorphonuclear leukocyte PMN
Picomole per liter pmol/L
Probability value P-value
Person's correlation coefficient R
Revolution per minute rpm
Significant S
Soluble cluster of differentiation sCD
Suprachiasmatic nuclei SCN
Standard deviation SD
Standard error SE
Significance Sig.
Substance P SP
Statistical package for social science SPSS
Transforming growth factor beta TGF-β
T helper Th
T helper type 1 Th1
T helper type 2 Th2
Tetramethylbenzidine TMB
Tumor necrosis factor TNF
Microliter μL

Introduction
&
Aims of the study

1
Introduction
Periodontal diseases are one of the most wide spread diseases of humankind,
no nation and no region of the world being free from them (Buatongsri et al., 2002).
The extent, severity and course of periodontal diseases are affected by several factors
such as personal oral hygiene, diet, genetics, public preventive services as well as
personal dental preventive, diagnostic and therapeutic services (Brown et al., 2002).
Such diseases may be found in every age group, but is more commonly found in adult
population regardless of the sex, race, education, residence, or socioeconomic status
(El-Qadri and Taani, 2004).
Periodontal diseases are multifactorial infection characterized by destructive
inflammatory process affecting tooth-supporting tissues caused by pathogenic
microorganisms, which induce elevations of pro-inflammatory cytokines resulting in
tissue destruction. Evolution of periodontal diseases is influenced by many local or
systemic risk factors (Cazalis et al., 2009; Malathi and Sabale, 2013). Dental plaque,
which harbours specific periodontal pathogens, its primary etiologic factor. Where host
tissue damage in periodontal disease is mainly due to the action of oral microbes and
associated host immune-inflammatory responses (Van Dyke and Serhan 2003; Van
Dyke, 2007). In addition, several risks and susceptibilities have been associated with
periodontal disease, like systemic diseases, socioeconomic or educational status,
smoking and psychological stress. Several clinical studies have investigated the
possible relationship between psychological stress and periodontal disease and have
suggested that stress may play a role in development of periodontal disease (Elter et
al., 1999; Hamissi et al., 2010; Vered et al., 2011; Akcali et al., 2013).
Stress is defined as the reactions of the body to forces of a deleterious nature,
infections and various abnormal states that tend to disturb its normal physiological
equilibrium (Lathrop and Thomas, 2008). It's nevertheless a confirmed and important
factor in the etiology and maintenance of many inflammatory diseases, including
periodontal disease (Keshava and Sangeeta, 2013). Stress results in delayed healing

2
of the connective tissues and bone, apical migration of the junctional epithelium and
formation of periodontal pocket (Chandna and Bathla, 2010). It's said to influence
the host defenses, exerting an immunosuppressive effect, increasing one's vulnerability
to disease (Ishisaka et al., 2008; Goyal et al., 2011). Cytokines and other humoral
mediators of inflammation are potent activators of the central stress response, and the
glucocorticoids released via this mechanism might regulate the recruitment of immune
cells into inflamed tissues, in order to cope with the psychological stress and depression
(Breivik and Thrane, 2001). When the inflammatory action is sufficiently long and
profound, the systemic manifestations of the disease may become evident, as could
happen with periodontal disease.
Many physiopathological processes are involved in periodontal destruction
in terms of the inflammatory and immune host response, especially proinflammatory
cytokines or matrix metalloproteinase (Dahan et al., 2001; Kiecolt-Glaser et al.,
2003; Van Dyke and Kornman, 2008). Interleukin-1β is a highly pro-inflammatory
cytokine strongly associated with periodontal breakdown (Dayan et al., 2004). In
addition, interleukin-1, produced following exposure to immunological and
psychological challenges, plays an important role in the neuroendocrine and
neurobehavioral stress responses (Goshen and Yirmiya, 2009; Debnath et al., 2011).
Saliva is a mirror to the general health condition that reflects various
systemic changes in the body (Nagler et al., 2002; Chiappelli et al., 2006; Nagler,
2008). So its' interest as a diagnostic fluid has grown exponentially in recent years.
Where the composition of saliva immediately reflects the sympathetic and
parasympathetic nervous systems, hypothalamic-pituitary-adrenal axis and immune
system response to stress (Khaustova et al., 2010). In addition, salivary levels of
various biochemical parameters have been measured in infectious diseases,
autoimmune diseases and psychiatric disorders (Streckfus and Bigler, 2002).

3
Aims of the study
1. To determine and compare the periodontal parameters (plaque index, gingival index
and bleeding on probing) among dental students before, during and after mid-year
exam period by clinical examination.
2. To determine and compare the stress level among dental students before, during and
after mid-year exam period by using DASS-21.
3. To estimate and compare the level of salivary interleukin-1β among dental students
before, during and after mid-year exam period by using ELISA.
4. To correlate the stress with the immunological parameter (salivary interleukin-1β)
and clinical periodontal parameters (plaque index, gingival index and bleeding on
probing).

Chapter One
Review of Literature

Review of Literature Chapter One
4
Review of Literatures
1.1. Periodontal diseases
1.1.1. Definition
Periodontal diseases (PD) are group of inflammatory diseases caused by
pathogenic microflora organized in biofilms surrounding the teeth and divided into two
main forms, gingivitis is a superficial and reversible affection of gingiva without
destruction of alveolar bone and periodontitis corresponding to profound disease
associated with destruction of teeth-supporting tissues that can lead to tooth loss
(Pihlstrom et al., 2005).
Periodontal diseases begins when bacteria in plaque causes the gingiva to
become inflamed (American Academy of Periodontology, 2004). As a rule, PD
develops through gingivitis, an inflammation of the marginal periodontium. However,
not every gingivitis develops further into periodontitis; both the amount and virulence
of the microorganisms and the resistance factors of the host (risk factors and immune
status) are crucial for the progression of the periodontal destruction (Saini et al., 2009).
There is equilibrium that exists between microbial challenge and host's
immune response; any alteration to that with the addition of other modifying factors is
responsible for clinical manifestation of PD. The oral cavity works as a continuous
source of infectious agents, and its condition often reflects progression of systemic
pathologies (Saini et al., 2009; Soory, 2010).
Studies showed the essential role of bacteria in periodontitis but bacteria
alone seem to be insufficient to explain occurrence or progression of the disease
(Leininger et al., 2010). Age, tobacco use, systemic diseases and psychological stress
have been identified as important risk factors for periodontitis (Peruzzo et al., 2007;
Cronin et al., 2008).
Several studies have demonstrated a relationship between psychological
stress and inflammatory diseases such as rheumatoid arthritis and periodontitis

Review of Literature Chapter One
5
(Walker et al., 1999; Hilgert et al., 2006; Saini et al., 2010; Goyal et al., 2011;
Reddy et al., 2012; Rivera et al., 2012; Refulio et al., 2013).
1.1.2. Epidemiology
The PD are highly prevalent and can affect in the initial and acute phases up
to 90% of the population worldwide. The disease affects a relatively high percentage
of the adult population in developed and developing countries (Zadik et al., 2008).
Periodontal disease is widely regarded as the second most common disease
worldwide, after dental decay, and in the United States has a prevalence of 30-50% of
the population, but only about 10% have sever forms. Like other conditions that are
intimately related to access to hygiene and basic medical monitoring and care,
periodontitis tends to be more common in economically disadvantaged populations or
regions (Pihlstrom et al., 2005). Generally, in Yemenite, North-African, South Asian,
or Mediterranean origin have higher prevalence of PD than individuals from European
descent individuals living in East Asia (e.g. Japan, South Korea and Taiwan) have the
lowest incident of PD in the world. This could be attributed to genetic predisposition
as well as environmental and behavioral differences (e.g. smoking, oral hygiene, stress
and access to dental treatment) between populations (Zadik et al., 2008).
1.1.3. Pathogenesis of periodontitis
There are a number (No.) of models by which pathogenesis of periodontitis
can be explained. One suggests continuous progression of disease where the loss of
attachment occurs slowly over time and then another suggests progression of
attachment loss occurs rapidly over short period of time, or in an episodic burst manner.
It appears that, depending on the patient and the sites, both these models could occur
together (Jepsen, 1996).
1.1.3.1. Bacterial factors
Periodontitis is a common, chronic and complex inflammatory disease
caused by bacterial biofilms that accumulate on the tooth surface and gingival sulcus,

Review of Literature Chapter One
6
and it is characterized by progressive destruction of the structures that support teeth
(Van Dyke, 2007; Kornman, 2008).
Microbial plaque accumulation on teeth surfaces adjacent to the gingival
tissues brings the oral sulcular and junctional epithelial cells into contact with the waste
product, enzymes and surface components of colonizing bacteria. As the bacterial load
increases, so does the irritation of the host tissues by these substances. The microbial
substances that can direct its action against vasculature and leukocytes, causing
vasodilation, increased gingival crevicular fluid (GCF) flow and migration of
neutrophils. In addition, these components interact with host systems involved in
inflammatory responses that lead to produce proinflammatory cytokines and other
chemical mediators of inflammation. These mediators begin an inflammatory response
within the tissues, which follows the classical inflammatory response. The tissues
become swollen as fluid accumulates and cell infiltrate is recruited into the lesion that
secretes proinflammatory mediators, including prostaglandin E2 (PGE2), interleukin
1(IL-1), IL-6 and tumor necrosis factor alpha (TNF-α), and clinical gingivitis develops
(Ranney, 1991; Ebersole and Cappelli, 2000). Many physiopathological processes
are involved in periodontal destruction in terms of the inflammatory and immune host
response, especially proinflammatory cytokines or matrix metalloproteinase (MMP)
(Dahan et al., 2001; Kiecolt-Glaser et al., 2003; Van Dyke et al., 2008). MMPs
participate in the destruction of the extracellular matrix (Teba et al., 2005).
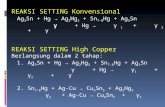
Etiology of PD is highly related to periodontal bacteria such as
Porphyromonas gingivalis (P. gingivalis), Prevotella intermedia (P. intermedia) or
Aggregatibacter actinomycetemcomitans (A. actinomycetemcomitans) (Castillo et al.,
2011). These bacteria induce the destruction of periodontal tissues with their numerous
virulence factors such as fimbriae and lipopolysaccharide (LPS) that cause activation
of monocytes and subsequent production of tissue destruction can lead to connective
tissue attachment loss and bone loss. Cytokines can cause tissue destruction by
allowing the secretion of tissue MMPs, thus further contributing to the pathogenesis of
PD (Curtis et al., 2005) (Fig. 1-1).

Review of Literature Chapter One
7
Fig. 1-1: Schematic illustration of the pathogenesis of periodontitis (Carranza et al., 2006).
In healthy periodontium, neutrophils can form a wall and fend back bacteria,
keeping their virulent factors away from the tissues. The neutrophils get the assistance
of opsonizing antibodies from reservoirs of the GCF. In the diseased state, GCF
is an inflammatory exudate that flows through the junctional epithelium into the
gingival crevice. It contains many molecules such as locally produced antibodies, host
cell derived products, endotoxin, amines, enzymes, bacterial collagenase and immune
response product such as cytokines (Embery and Waddington, 1994; Delima and
Van Dyke, 2003). The antibodies in the GCF allow neutrophils to recognize, ingest,
and degrade bacteria. When bacteria have invaded the periodontal tissues, host-
mediated destruction occurs and host cells release cytokines into the environment,
which provide the signals to other cells to begin affecting their function (Liu et al.,
1996; Rawlinson et al., 2000).
1.1.3.2. Host responses factors
Although bacteria initiate PD, the host response is believed to play an
essential role in the breakdown of connective tissue and bone. Microbial antigens and

Review of Literature Chapter One
8
virulence factors elicit an inflammatory and immune reaction, in which both innate and
adaptive immune responses are involved (Van Dyke and Kormman, 2008). The
response varies among individuals, depending on potential variations in cytokine and
other antimicrobial responses, environmental factors and the subjects' genetics
(Gemmell et al., 2007; Kinane et al., 2007).
I. Innate immune response:
The first line of defense in infectious diseases, the innate immunity, is
challenged to detect pathogens and mount a rapid defensive response, which requires
no prior immune learning or experience. It is responsible for the defense during the
initial hours and days of the infection (Kirkwood et al., 2006; Kinane et al., 2007).
It acts through the recruitment of immune cells, activation of complement system,
identification and removal of foreign substances and activation of the adaptive immune
system (Vandyke and Kormman, 2008).
Periodontal disease may in most cases be considered a localized infection.
However, it is speculated that the inflamed and ulcerated subgingival pocket epithelium
could form an easy port of entry for dental plaque bacteria to disperse systemically
(Hujoel et al., 2001; Moutsopoulos and Madianos, 2006). Neutrophils
(polymorphonuclear leukocytes (PMNs)) are the first cells to encounter pathogens,
soon reinforced by the recruitment of monocytes/macrophages (Janeway et al., 2005).
Neutrophil infiltration takes place in the periodontal tissue (Dixon et al., 2004).
Inflammatory cell infiltrate in gingival tissue and GCF is predominantly formed by
neutrophils, B-cells and plasma cells are also present (Ebersole, 2003).
The complement system is a part of innate response, composed of 30 proteins
that participate in tissue destruction and in inflammatory processes, it can be activated
by the alternative pathway (LPS or other bacterial products) or by the classical pathway
(detection of antigen antibody complexes), giving rise to bacterial opsonisation
(Bascones and Gonzalez-Moles, 2003).
The innate immune system recognizes common pathogen associated
molecular patterns (PAMPs) that are expressed on microorganisms, but not on host

Review of Literature Chapter One
9
cells, by extra- and intracellular receptors like cluster of differentiation 14 (CD14). The
CD 14 proteins found in two distinct forms: membrane CD14 (mCD14), expressed
primarily on the surface of monocytes/ macrophages and neutrophils, and a soluble
form (sCD14) (Le Van et al., 2001; Bas et al., 2004). Activation of the CD14 receptor
activates monocytes and endothelia cells for secretion of proinflammatory molecules
such as IL-1β, TNF-α, PGE2 and IL-6 (Dixon et al., 2004; Martinez et al., 2009).
II. Adaptive immune response:
The innate immunity system is closely linked to the adaptive immune
response; it acts the second defense line that helps clear the infection and builds specific
immunity with a memory component. Activation of the adaptive response occurs
through cytokine secretion, antigenic processing and presentation and differentiation
of effector cells (Hornef et al., 2002).
The primary cells involved in the adaptive immune response are
lymphocytes, B-cells and T-cells. B-cells are mainly antibody producers, while T-cells
are functionally divided into two main classes. One class differentiates on activation
into cytotoxic T-cells, which kill cells infected with viruses and express CD8 molecule
on their cell surfaces. T helper (Th) cells, on the other hand, are marked by the
expression of the cell surface molecule CD4, and play an important role in the initiation
of immune responses by providing help to other cells (Janeway et al., 2005).
T-cells are considered to have a central role in controlling the progression of
PD, and different types of T cell clones have been demonstrated to play destructive
roles (Taubman and Kawai, 2001). The early periodontal lesion (gingivitis)
characterized by increased Nos. of T-cells, but there is only limited consensus
regarding the nature of Th cells that predominate in inflamed gingival tissue. Most of
the studies support the notion that T helper type 1 (Th1) cells and their cytokines are
associated with early /stable periodontal lesions, while T helper type 2 (Th2) response
in periodontium predispose to susceptibility to disease progression (Gemmell et al.,
2007). Although T-cells act as the main regulatory group of cells in periodontitis
lesions, B-cells have several critical roles. After encounter with antigen, B-cells

Review of Literature Chapter One
10
differentiate into antibody secreting plasma cells, the production of antibodies involves
the response to foreign antigens as well as to self-antigens, plasma cells that have the
property of specifically binding to the antigen (Bascones and Gonzalez-Moles, 2003;
Berglundh et al., 2007).
Periodontal pathogens give rise to a marked humeral immune response such
as production of immunoglobulin (Ig) that can be measured locally in saliva or GCF or
systemically in serum (Korn et al., 2007; Pussinen et al., 2007; Gaffen and
Hajishengallis, 2008).
1.1.3.3. Viral factors
In addition to bacteria and host response factors, viruses also play a role in
the pathogenesis of periodontitis (Slots and Contreras 2000; Slots, 2005).
Herpes virus infections can induce pro-inflammatory cytokine release as a
response from the immune system. Cytokines normally play a positive role in the
immune system by exerting antiviral activity to fight off infection or invasion by
pathogens (Alcami and Koszinowski, 2000). However, herpes viruses can interfere
with these functions and cause paradoxical effects leading to tissue damage. In
particular, the viruses can change the cytokine production and prevent antiviral
responses (Tortorella et al., 2000).
The over production of pro-inflammatory cytokines such as IL-1β, 1L-6, IL-
12 and TNF-α are often evident in human cytomegalovirus (HCMV) infections and
can lead to detrimental effects (Mogensen et al., 2004). A productive herpes virus
infection can exacerbate periodontal tissue destruction through a virus-induced
impairment of the periodontal immune defense, leading to a more virulent population
of resident bacteria (Slots and Contreras, 2000; Mogensen et al., 2004; Slots, 2005).
1.1.3.4. Other risk factors
Although oral microorganism seem to play a predominant role in etiology of
chronic periodontitis (CP), other risk indicators have been identified. Risk factors are
important in periodontopathy as they affect the severity and prevalence of periodontal
diseases among population. The assessment of risk factor is essential and necessary in

Review of Literature Chapter One
11
order to limit and control the disease and treatment for subjects with increased risk
(Tanner et al., 1997). CP has been considered more common in people aged more than
30, having systemic disease, inadequate oral hygiene and /or high levels of stress and
low socioeconomic status (Akhter et al., 2005).
Oral hygiene, a considerable No. of studies have suggested an important role
of oral hygiene in periodontal health status such as (Hirschfeld and Wasserman in
1978; Konig et al., in 2001), during their classical investigations with optimal
individual hygiene procedures, resulted in improvement of periodontitis and stable
periodontal health status (under highly standardized conditions).
Smoking is one of the most significant risk factor for the initiation and
progression of PD and associated with increased prevalence and severity of destruction
of PD in term of periodontal pocketing and attachment loss. Additionally, smoking can
lower the chances for successful treatment (AL-Ghamdi and Anil, 2007).
Genetic factors influence susceptibility to the different forms of early onset
periodontitis. However, it is unlikely that a specific gene will be identified as causing
enhanced disease susceptibility. It is more likely that the genetic influences are as
multifactorial as the diseases themselves, and a complex interplay between genetically
determined host responses and environmental challenges may determine whether
disease is present (Jindal, 2009).
Alcohol consumption as well as alcohol sensitivity may be a risk factor for
periodontitis progression (Shimazaki et al., 2005; Nishida et al., 2010).
Psychological factors, many studies have demonstrated that individuals
under psychological stress are more likely to develop clinical attachment loss, loss of
alveolar bone and increased the periodontitis (Mawhorter and Lauer, 2001; Pistorius
et al., 2002; Wimmer et al., 2002).

Review of Literature Chapter One
12
1.2. Stress
Stress originates from a Latin word: 'stringere', which means 'tight', 'strained'.
In 1935, Cannon described stress as the result of the homeostasis and showed the
influence of the sympathetic system. In 1950, Selye published a book known as (Relief
from stress) which had over 1000 pages and more than 5000 references. He elaborated
stress as a response state of the organism to forces acting simultaneously on the body
which if excessive that is straining the capacity of adaptive process beyond their limits
leads to disease of adaptation and eventually disease of exhaustion and death. He
defined forces that have the potential to challenge the adaptive capacity of the organism
as stressor (LeResche and Dworkin, 2002; Sateesh et al., 2010).
The stressors are all situations that can constitute aggressions or feel like that.
Various origins can take place such as physical or psychological (mental) (Sateesh et
al., 2010). When any type of stressor exceeds the threshold, the stress system mediates
the generalized stress response. Selye recognized that stressor acting to produce
changes in the body could be positive (e.g. exciting, pleasurable), leading to a response
state known as eustress, or stressor could be negative, threatening homeostasis with
pain, discomfort and physical pathology which is known as distress (LeResche and
Dworkin, 2002).
A subject exhibits stress response or not depends upon the factors, including
coping behaviors, genetic predisposition, concomitant stressors, level of social support
and their lifestyle factors. Potential effects of stress response that may be observed or
even measured, includes anxiety, depression, impaired cognition and altered self-
esteem (Boyapati and Wang, 2007). The coping is the effort to try to reduce, control
or tolerate the state of stress. It needs adjustment, adaptation and confrontation
strategies (Sateesh et al., 2010).
Reners and Breex in 2007 defined stress as physiological and metabolic
perturbations caused by various aggressive agents and psychophysiological response
of an organism facing the perception of a challenge or a threat.

Review of Literature Chapter One
13
Different kinds of stress have been defined, such as work related, negative
life experiences and socioeconomic status (Genco et al., 1998; Mead et al., 2001;
Soares et al., 2007).Stress is often classified as acute and chronic. Acute stress lasts
for a period of minutes to hours, whereas chronic stress persists for several hours, a
day, weeks or even months. In case of acute stress, stress response may prepare the
immune system for challenges such as infection that may be imposed by the stressor
(Dhabbar, 2002). When stress becomes chronic, it may influence inflammatory
processes leading to development of systemic or local diseases such as rheumatoid
arthritis (Culshaw et al., 2011), diabetes (Chida and Hamer, 2008), cardiovascular
diseases (Backe et al., 2012) or PD (Stabholz et al., 2010). So stress can be mediates
disease and illness, LeResche distinguished between disease and illness in that the
maladaptation of organs or organ systems manifests itself as the pathological states that
we call disease, such as inflammatory disease, malignancy and genetic malformations.
While people have an illness, which is typically based on the self-attribution or belief
that a disease is present. Illness behaviors may become maladaptive, such as excessive
worry about poor outcomes, depression, anxiety, overzealous health-care seeking and
interruption of normal behaviors such as work, eating and social activities (LeResche
and Dworkin, 2002).The magnitude of stress is measure according to the peak levels
of stress hormones, neurotransmitters and other physiological changes, including
increased levels in heart rate and blood pressure and by the duration of time during
which these changes linger during and after exposure to a stressor. Therefore, the
combination of intensity and duration comprise the magnitude of stress (Dhabbar,
2002).
An academic exam can be considered as a psychological stressor, consisting
of a period of preparation, anticipation and then the exam itself. Furthermore, an
academic exam plays an important role in evaluating student learning outcomes and
their mastery of a subject. Recent studies have reported high levels of anxiety among
dental and medical students (Omigbodun et al., 2006; Smith et al., 2007). Students
who participated in a major exam had significantly more dental plaque and more

Review of Literature Chapter One
14
gingival inflammation compared with students who didn't participate in any exam
(Deinzer et al., 2005). Academic stress appears to affect periodontal health status
(Deinzer, 2001; Johannsen et al., 2010). In addition, some studies have shown that
the levels of pro-inflammatory cytokines, IL-1β, IL-6 and IL10 in serum and GCF, are
increase in patients with depression and academic stress (Deinzer, 1998; Maes et al.,
1998; Paik et al., 2000; Waschul et al., 2003; Johannsen et al., 2006; Johannsen et
al., 2007; Von Kanel et al., 2007; Johannsen et al., 2010).
1.2.1. Stress scales
There are many types of stress scales such as holme rahe stress scale (HRSS),
college undergraduate stress scale (CUSS), traditional college student stress scale
(TCSS) and two versions of depression anxiety stress scale (DASS); DASS versions
are a 42-item questionnaire version and a 21-item questionnaire version, Table (1-2)
and (1-3), which includes three self-report scales designed to measure the negative
emotional states of depression, anxiety and stress. Each of the three scales contains 14
items in a 42-item questionnaire version and 7 items in a 21-item questionnaire version.
The depression scale assesses dysphoria, hopelessness, devaluation of life, self-
deprecation, lack of interest, anhedonia and inertia. The anxiety scale assesses
autonomic arousal, skeletal muscle effects, situational anxiety and subjective
experience of anxious affect. The stress scale is sensitive to levels of chronic non-
specific arousal. It assesses difficulty relaxing, nervous arousal and being easily
agitated, over-reactive and impatient. Respondents are asked to use 4-point severity
scales to rate the extent to which they have experienced each state over the past week.
Scores of depression, anxiety and stress calculated by summing the scores for the
relevant items. The depression scale items are 3, 5, 10, 13, 16, 17, 21, 24, 26, 31, 34,
37, 38 and 42 in a 42-item questionnaire version and in a 21-item questionnaire version
include 3,5,10, 13, 16,17and 21. The anxiety scale items are 2, 4, 7, 9, 15, 19, 20, 23,
25, 28, 30, 36, 40 and 41 in a 42-item questionnaire version and in a 21-item
questionnaire version include 2, 4,7,9,15,19 and 20. The stress scale items are 1, 6, 8,

Review of Literature Chapter One
15
11, 12, 14, 18, 22, 27, 29, 32, 33, 35 and 39 in a 42-item questionnaire version and in
a 21-item questionnaire version include 1, 6, 8,11,12,14 and 18. The score for each of
the respondents over each of the sub-scales then evaluated as per the severity-rating
index, Table (1-1) (Lovibond and Lovibond, 1995).
Table (1-1): DASS severity-rating index (Lovibond and Lovibond, 1995).
Table (1-2): DASS 42-item questionnaire version (Lovibond and Lovibond, 1995).
1 I found myself getting upset by quite trivial things 0 1 2 3
2 I was aware of dryness of my mouth 0 1 2 3
3 I couldn't seem to experience any positive feeling at all 0 1 2 3
4 I experienced breathing difficulty (e.g. excessively rapid breathing,
breathlessness in the absence of physical exertion)
0 1 2 3
5 I just couldn't seem to get going 0 1 2 3
6 I tended to over-react to situations 0 1 2 3
7 I had a feeling of shakiness (e.g. legs going to give way) 0 1 2 3
8 I found it difficult to relax 0 1 2 3
9 I found myself in situations that made me so anxious I was most
relieved when they ended
0 1 2 3
10 I felt that I had nothing to look forward to 0 1 2 3

Review of Literature Chapter One
16
11 I found myself getting upset rather easily 0 1 2 3
12 I felt that I was using a lot of nervous energy 0 1 2 3
13 I felt sad and depressed 0 1 2 3
14 I found myself getting impatient when I was delayed in any way (e.g.
lifts, traffic lights, being kept waiting)
0 1 2 3
15 I had a feeling of faintness 0 1 2 3
16 I felt that I had lost interest in just about everything 0 1 2 3
17 I felt I wasn't worth much as a person 0 1 2 3
18 I felt that I was rather touchy 0 1 2 3
19 I perspired noticeably (e.g. hands sweaty) in the absence of high
temperatures or physical exertion
0 1 2 3
20 I felt scared without any good reason 0 1 2 3
21 I felt that life wasn't worthwhile 0 1 2 3
22 I found it hard to wind down 0 1 2 3
23 I had difficulty in swallowing 0 1 2 3
24 I couldn't seem to get any enjoyment out of the things I did 0 1 2 3
25 I was aware of the action of my heart in the absence of physical
exertion (e.g. sense of heart rate increase, heart missing a beat)
0 1 2 3
26 I felt down-hearted and blue 0 1 2 3
27 I found that I was very irritable 0 1 2 3
28 I felt I was close to panic 0 1 2 3
29 I found it hard to calm down after something upset me 0 1 2 3
30 I feared that I would be "thrown" by some trivial but unfamiliar task 0 1 2 3
31 I was unable to become enthusiastic about anything 0 1 2 3
32 I found it difficult to tolerate interruptions to what I was doing 0 1 2 3
33 I was in a state of nervous tension 0 1 2 3
34 I felt I was pretty worthless 0 1 2 3

Review of Literature Chapter One
17
35 I was intolerant of anything that kept me from getting on with what
I was doing
0 1 2 3
36 I felt terrified 0 1 2 3
37 I could see nothing in the future to be hopeful about 0 1 2 3
38 I felt that life was meaningless 0 1 2 3
39 I found myself getting agitated 0 1 2 3
40 I was worried about situations in which I might panic and make fool
of myself
0 1 2 3
41 I experienced trembling (e.g. in the hands) 0 1 2 3
42 I found it difficult to work up the initiative to do things 0 1 2 3
Table (1-3): DASS 21-item questionnaire version (Lovibond and Lovibond, 1995).
1 I found it hard to wind down 0 1 2 3
2 I was aware of dryness of my mouth 0 1 2 3
3 I couldn't seem to experience any positive feeling at all 0 1 2 3
4 I experienced breathing difficulty (e.g. excessively rapid breathing) 0 1 2 3
5 I found it difficult to work up the initiative to do things 0 1 2 3
6 I tended to over-react to situations 0 1 2 3
7 I experienced trembling (e.g. in the hands) 0 1 2 3
8 I felt that I was using a lot of nervous energy 0 1 2 3
9 I was worried about situations in which I might panic and make
a fool of myself
0 1 2 3
10 I felt that I had nothing to look forward to 0 1 2 3
11 I found myself getting agitated 0 1 2 3
12 I found it difficult to relax 0 1 2 3
13 I felt down-hearted and blue 0 1 2 3
14 I was intolerant of anything that kept me from getting on with
what I was doing
0 1 2 3

Review of Literature Chapter One
18
15 I felt I was close to panic 0 1 2 3
16 I was unable to become enthusiastic about anything 0 1 2 3
17 I felt I wasn't worth much as a person 0 1 2 3
18 I felt that I was rather touchy 0 1 2 3
19 I was aware of the action of my heart in the absence of physical
exertion (e.g. sense of heart rate increase, heart missing a beat)
0 1 2 3
20 I felt scared without any good reason 0 1 2 3
21 I felt that life was meaningless 0 1 2 3
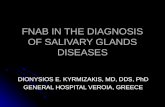
1.2.2. Molecular and endocrine mechanisms of the stress response
The immune response doesn't operate autonomously but in close cooperation
with the neuroendocrine systems. When the body is in stress, there is an increase of
stress markers and immune cells in the plasma mobilized from lymphoid organs. A
negative feedback, with the activation of the immune system that is associated with the
increase of circulating cytokines, increases the activity of the corticotropin releasing
hormone (CRH) and activates the hypothalamic pituitary adrenal (HPA), causing an
elevation of the levels of cortisol (Fig. 1-2). When the inflammatory action is
sufficiently long and profound, systemic manifestations of the disease might become
evident, as could happen with periodontitis (LeResche and Dworkin, 2002).
Where stress can result in the degeneration of the immune system, mediated
primarily through HPA axis and sympathetic adrenal medullary axis (Fig. 1-3). Stress
perceived by the brain stimulates the hypothalamus to produce CRH, which is release
into the hypophyseal portal system, activating the pituitary gland to release
adrenocorticotropic hormone (ACTH), which in turn induces release of glucocorticoids
(GC) from the adrenal cortex (Boyapati and Wang, 2007). Cortisol, known more
formally as hydrocortisone, is a steroid hormone, more specifically is the main adrenal
GC hormone, and it is released in response to stress and a low level of blood GC
(Marieb et al., 2013).

Review of Literature Chapter One
19
Glucocorticoids, including cortisol, exert major suppressive effects through
highly specific mechanisms at multiple levels. For example, in vivo GC reduce the No.
of circulating lymphocytes, monocytes and eosinophil. They also inhibit the
accumulation of eosinophil, macrophages and neutrophils at inflammatory sites. At the
molecular level, GC profoundly inhibit important functions of inflammatory cells
including macrophages, neutrophils, eosinophil and mast cells in functions such as
chemotaxis, secretion and degranulation. GC also inhibit the cascade of the immune
response by inhibiting macrophage-antigen presentation, lymphocyte proliferation and
lymphocyte differentiation to effector cell types such as helper lymphocytes, cytotoxic
lymphocytes, natural killer cells and antibody-forming B cells. Corticosteroids also
inhibit production of cytokines including IL-1, IL-2, IL-3, IL-6, TNF, interferon-
gamma (IFN-γ), granulocyte and monocyte colony stimulating factors. GC inhibit
arachidonic acid-derived proinflammatory mediators such as PG. Hence, the stress-
related stimulation of the HPA axis with the production of GC such as cortisol has
major suppressive actions on immune and inflammatory responses. This represents the
major effector arm of the CNS-hormonal axis. There is also an afferent or feedback
arm consisting of stimulation of the HPA axis by cytokines (Kunz-Ebrecht et al.,
2003; Boyapati and Wang, 2007; Groer et al., 2010; Papacosta and Nassis, 2011).
Glucocorticosteroids, including cortisol, then depresses immunity including
secretory IgA, IgG and neutrophil functions, all of which may be important in
protection against infection by periodontal organisms. Secretory IgA antibodies may
protect by reducing initial colonization of periodontal pathogens. IgG antibodies may
exert protection by opsonizing periodontal organisms for phagocytosis and killing by
neutrophils. This then gives rise to increased susceptibility, which leads to the
establishment of periodontal infection, which, in turn, results in destructive
periodontitis. Periodontitis is brought about by tissue destroying factors such as IL-1
and MMPs activated by the periodontal pathogens, as well as by the direct effects of
pathogenic bacteria (Grossi et al., 1998).

Review of Literature Chapter One
20
The second major pathway to be activated is the sympathetic nervous system
called ‘flight or fight’ response to potentially harmful stimuli. Stress activates the nerve
fibers of the autonomic nervous system, which innervate the tissues of the immune
system, results in the release of catecholamine from the adrenal medulla that lead to
the development of hyperglycemia by directly stimulating glucose production and
interfering with the tissue disposal of glucose. Catecholamines are alter the blood flow.
Peripheral vasoconstriction may affect important oxygen–dependent healing
mechanisms, such as angiogenesis, collagen synthesis and epitheliazation (Boyapati
and Wang, 2007). In addition, catecholamines are the most important molecules to
relay information from the CNS to the immune system (Marketon and Glaser, 2008).
The release of catecholamine results in hormonal secretion of
norepinephrine/ epinephrine (noradrenaline/adrenaline) by adrenal medulla and
sensory nerve fibers, which results in a range of immune functions including cell
proliferation (Sanders and Straub, 2002; Hamaguchi et al., 2008), inhibition of pro-
inflammatory cytokines such as IFN-γ, IL-2, IL-6, IL-12 and TNF-α (Hansel et al.,
2010), suppression of lymphocyte proliferation, Natural killer (NK) cell activity (Ben-
Eliyahu et al., 2000), antibody production and cytolysis activity (Padgett and Glaser,
2003).
Increased sympathetic stimulation can also act to decrease salivary
secretions typically experienced as anxiety induced dry mouth. Stress that is associated
with immune challenge has been called immune stress or inflammatory stress
(Boyapati and Wang, 2007).
Autonomous nervous system can also moderate the HPA axis by stimulating
CNS and sensory nerve fibers leading to secretion of neuropeptides such as substance
P (SP) (Rosenkranz, 2007). Neuropeptides are generated primarily in the CNS and
play important roles in neurogenic inflammation, including vasodilatation, plasma
extravasation and recruitment of immune cells (Kabashima et al., 2002; Lundy and
Linden, 2004). SP is important in initiating and sustaining inflammation, increasing

Review of Literature Chapter One
21
proinflammatory cytokine production and by limiting the production of transforming
growth factor beta (TGF-β) and IFN-γ activated macrophages (Pradeep et al., 2009).
Fig. 1-2: Effects of stress on hypothalamic pituitary adrenal axis (Genco et al., 1998).
Fig. 1-3: Physiological model of effects of stress on periodontal disease (Boyapati and Wang,
2007).

Review of Literature Chapter One
22
1.2.3. Behavioral changes of stress response
It is hypothesized that the main effects of stress occur through behavioral
changes which affect at risk health behaviours such as smoking, poor oral hygiene and
poor compliance with dental care. There is also a possibility that stress leads to other
behavioral changes such as overeating, especially a high-fat diet, which then can lead
to immunosuppression through increased cortisol production (Fig. 1-4) (Grossi et al.,
1998).
There are certainly much other possible behavior that could be affected by
stress, inadequate coping and distress, such as depression, which would have
significant effects on PD. Croucher et al., in 1997 studied the relationship between
life events and PD and found that both negative life events leading to oral health risk
behaviours such as poor oral hygiene and smoking as important determinants of PD.
Stress, distress and inadequate coping may influence a multitude of
behaviors, for example depression, thus considerably affecting PD. Health risk
behaviors must be evaluated to reveal the extent to which they contribute to the
interaction between stress and PD (Genco et al., 1998).
Klages et al., in 2005 discovered that mental stress could influence life-style
and dental hygiene habits. This influence wasn't only decreases the frequency as well
as the quality of the dental hygiene but also it increases tobacco use and alcohol
consumption, changes in food habits leading to a diminution of the general health. This
was in agreement with the study conducted by Suchday et al., in 2006.
Deinzer et al., in 2005 have discussed that plaque is a valid indicator of oral
hygiene behavior even under academic stress conditions, there seems to be good
evidence to add oral hygiene behavior to the list of health behavior's which gets
adversely affected by stress. These results confirm the findings of Deinzer et al., in
2001 on stress associated alterations in oral health behavior. It further extends by
demonstrating an increase of gingivitis in exam going students as compared with
controls 4 weeks after the exams. Gingivitis rates of posterior sextants of exam going
students nearly doubled those of control participants.

Review of Literature Chapter One
23
Fig. 1-4: Psychosocial stress and its effect on behavior as manifested by alterations in
periodontal disease (Grossi et al., 1998).
1.2.4. Stress and microbiology of periodontal disease
Periodontitis is mainly related to changes in the composition of oral biofilms
especially colonizing species such as P. gingivalis, P. intermedia or A.
actinomycetemcomitans (Socransky and Haffajee, 2005). Stress induced by
psychosocial factors could influence periodontal ecology. Where several
microorganisms have the ability to recognize the hormones that are found within the
host and use them effectively to adapt to their environment and to promote bacterial
growth and infectious diseases. This supports the idea bacterial infections may develop
in response to stress. In an in vitro study done by Roberts et al., in 2002 to determine
whether noradrenaline and adrenaline, which are, released during human stress
responses, signals to alter the growth of 43 microorganisms found within subgingival
microbial complexes. The researchers found that 20 species within the subgingival
biofilm significantly grew from inoculation with noradrenaline and 27 species
significantly grew when adrenaline was introduced. There was also marked difference

Review of Literature Chapter One
24
in the growth response within bacterial species and within or between microbial
complexes. They concluded that this variation might influence in the vivo composition
of the subgingival biofilm in response to stress-induced changes in local catecholamine
levels and thus play a vital role in the etiology and pathogenesis of PD.
Shortly after this research published, another research also discovered that
chronic psychological stress has a marked impact on the localized immune response to
P. gingivalis (Houri-Haddad et al., 2003).
These observations indicate that stress-induced hormones may have specific
effects depending on species of bacteria. Periodontal destruction is the result of an
imbalance between bacterial aggression and host response. Stress-related hormones are
likely to favor the infection by increasing bacterial growth, thereby inducing a
breakdown in oral biofilms. Specific mechanisms underlying these effects on
periodontal microbiota remain unknown, and further studies are required to evaluate
possible effects of these hormones, especially on triggering of virulence factors
(Roberts et al., 2005).
1.2.5. Role of stress on gingivitis
Stress has shown to reduce the saliva flow and it increases the formation of
plaque. A study has shown that responses to emotional or psychological stress may
influence immune activities directly via nerve messenger substances
(neurotransmitters and neuropeptides) and/or indirectly via neuroendocrine (hormone)
substances and may modulate the immune response to bacteria, thus be expected to
influence the progression and course of gingivitis and periodontitis (Breivik et al.,
1996). Another study has shown that emotional stress modifies pH and its IgA secretion
(Reners and Breex, 2007). A series of studies done by Deinzer et al., examine the role
of academic stress during their examination period on periodontal health status.
Academic stress as shown to be a risk factor for gingival inflammation with increasing
crevicular IL-1β levels and a decrease in the quality of the oral hygiene (Deinzer et
al., 1998; Deinzer et al., 1999; Deinzer et al., 2000; Deinzer et al., 2001).

Review of Literature Chapter One
25
In a pilot study done by Axtelius et al., in 1998 showed the presence of
cortisol in GCF. A study conducted by Johannsen et al., in 2006 also confirmed that
persons with depressive signs show an elevation in cortisol levels in GCF.
Over the past decade, it has become more apparent that stress can negatively
influence the oral health status, which can lead to increased amounts of dental plaque
and gingival inflammation (Klages et al., 2005; Johannsen et al., 2007). In addition,
Deinzer et al., in 2005 and Johannsen et al., in 2010, who found increased dental
plaque and gingival inflammation in students who experienced academic stress.
Academic stress appears to affect periodontal health status, shown by more
plaque accumulation, gingival inflammation and increased amounts of IL-6, IL-10 in
GCF and cortisol in saliva. Therefore, the clinical implication should be to inform
individuals about stress as a possible risk factor for gingivitis and periodontitis and to
introduce additional preventive strategies in these individuals (Johannsen et al.,
2010).
1.2.6. Role of stress on periodontitis
Psychosocial factors are predisposing factors for the development of necrotic
PD. The first studies showing this influence were done by Giddon et al., in 1963;
Giddon et al., in 1964 (more necrotic PD in college during examination period). Many
of the main risk factors for necrotic PD such as past episode of necrotic PD, bad oral
hygiene, unusual emotional stress, bad sleep, tobacco, alcohol and recent illness are
often related to stress (Sateesh et al., 2010).
In addition, Stress linked with acute necrotizing ulcerative gingivitis
(ANUG) since early study evaluated the association between PD and psychosocial
stress (Murayama et al., 1994). Compared to other times, college students experience
an increase in the incidence of ANUG during examinations (Genco et al., 1998).
One study by Monteiro da Silva et al., in 1996 showed that people with
aggressive periodontitis were more depressed and socially isolated people than people

Review of Literature Chapter One
26
with CP or the control group. These studies show the interconnection that exists
between aggressive periodontitis and psychosocial stress.
Several clinical studies have investigated the possible relationship between
psychological stress and periodontitis; have suggested that stress may play an
important role in the development of PD and increase severity of PD (Hilgert et al.,
2006; Saini et al., 2010; Doyle and Bartold, 2012). Where, in a longitudinal study by
Linden et al., in 1996 predicted the future attachment loss depending on occupational
stress. In addition, the subjects who felt stress were more prone to develop PD than
subjects without stress (Akhter, 2005).
In contrary, Castro et al., in 2006 couldn't show any association between
life events, anxiety and depression with periodontitis. The association between
psychosocial factors and periodontitis is derived mainly from cross-sectional studies
(Linden et al., 1996; Genco et al., 1999; Johannsen et al., 2005; Klages et al., 2005).
1.2.7. Role of stress on periodontal treatment
A study conducted by Axtelius et al., in 1998 showed that patients with
psychosocial strain and passive dependent traits didn't respond to treatment when
compared to patients with less stressful psychosocial situation and a rigid personality.
Another study done by Kamma and Baehni showed that supportive
periodontal care was more effective in less stressful patients with aggressive
periodontitis (Kamma and Baehni, 2003).
Wimmer et al., in 2005; Reners and Brecx in 2007 explained the influence
of coping with stress on periodontal therapy and concluded that patients who had
maladaptive coping strategies have more advanced disease and those patients showed
a poor response to non-surgical periodontal treatment. In addition, Gamboa et al., in
2005 showed the influence of emotional intelligence which was used as a measure of
the coping mechanism in patients with CP on the initial responses to periodontal
treatment. The results of this study showed a decrease in plaque formation and
reduction in bleeding on probing (BOP) in patients with active coping strategy.

Review of Literature Chapter One
27
1.3. Saliva
Saliva is a unique complex, important body fluid and contains a No. of
systems, which serves a wide spectrum of physiological needs to protect the oral
mucosa and the whole body from infection (Harris and Godoy, 2004; Nanci, 2003;
Peter, 2004). It's produced from three-paired major salivary glands (parotid,
submandibular and sublingual), plus that from 200-400 minor salivary glands which
scattered throughout the oral cavity (Nanci, 2003; Costanzo, 2010). When the fluids
from all major and minor glands mix with each other, this secretion become known as
whole saliva or mixed saliva. Whole saliva is further altered by the presence of particles
of food, tissue fluid, lysed bacteria, sloughed epithelial cells and inclusion of living
cells and their metabolic products (Lawrence, 2002; Harris and Godoy, 2004).
Unstimulated (resting) saliva is a mixture of secretions, which enter the
mouth in the absence of exogenous stimuli (Ship et al., 1991; Thylstrup and
Fejerskov, 1994). Several factors affecting unstimulated salivary flow rate as the
degree of hydration, body position, exposure to light, previous stimulation, circadian
rhythms (peak during late afternoon), circannual rhythms (peak during winter) and
medications (Leone and Oppenheim, 2001; Thie et al., 2002; Guggenheimer, 2003).
Stimulated saliva is secreted in response to either masticatory or gustatory
stimulation and to lesser extent by activation of the vomiting center (Ghezzi et al.,
2000; Stooky, 2008). Stimulated salivary flow rate is affected by nature of the
stimulus, vomiting, smoking, gland size, gag reflex, olfaction and food intake
(Sreebny, 2000; Chausau et al., 2002; Inoue et al., 2009).
A loss or reduction of saliva results in significant problems such as dental
caries, PD, difficulties with eating, talking, altered taste sensation, as well as higher
risks of candidiasis and mucositis, which result in an overall reduction in the quality of
life (Buhlink et al., 2002; Hujoel et al., 2002; Thomson and Spencer, 2002).

Review of Literature Chapter One
28
1.3.1. Functions of saliva
De Almeida et al., in 2008; Greabu et al., in 2009 stated the functions of
saliva as follow:
1. Taste: The hypotonicity of saliva (low levels of glucose, sodium, chloride, and urea)
and its capacity to provide the dissolution of substances allows the gustatory buds
to perceive different flavors. Gustin, a salivary protein appears to be necessary for
the growth and maturation of these buds.
2. Buffer Capacity: Saliva behaves as a buffer system to protect the mouth as follows:
a) It prevents colonization by potentially pathogenic microorganisms by denying
them optimization of environmental conditions.
b) Saliva buffers (neutralizes) and cleans the acids produced by acidogenic
microorganisms, thus, prevent enamel demineralization.
3. Protection and Lubrication: Saliva forms a seromucosal covering that lubricates and
protects the oral tissues against irritating agents.
4. Dilution and cleaning: In addition to diluting substances, its fluid consistency
provides mechanical cleansing of the residues present in the mouth such as
nonadherent bacteria, cellular and food debris.
5. Integrity of tooth enamel: Saliva plays a fundamental role in maintaining the
physical-chemical integrity of tooth enamel by modulating remineralization and
demineralization.
6. Digestion: Saliva is responsible for the initial digestion of food, favoring the
formation of the food bolus, this action occurs mainly by the presence of the
digestive enzyme in the composition of saliva.
7. Tissue repair: A tissue repair function attributed to saliva since clinically the
bleeding time of oral tissues appears to be shorter than other tissues.
8. Defense such as spiting and oxidative stress.
9. Excretion, speaking, water balance, drug testing and denture retention.
10. Antibacterial, antifungal and antiviral: Saliva contains spectrum proteins with
antibacterial properties.

Review of Literature Chapter One
29
1.3.2. Salivary composition
Salivary gland secretion is mainly under autonomic nervous control, but
various hormones may also modulate salivary composition (Turner and Sugiya,
2002). Saliva consists of two component that are secreted by independent mechanisms
first component includes ions (inorganic), which is produced mainly by
parasympathetic stimulation and second component include protein (organic), which
is released mainly in response to the sympathetic stimulation (Scully, 2003).
Saliva possesses a multiplicity of immunological and nonimmunological
defense systems against toxins, fungi, viruses and bacteria (Dean and Simon, 2003;
Surdacka et al., 2007).
Saliva is principally a mixture of water and electrolytes such as sodium,
potassium, chloride and bicarbonate ions (Guyton and Hall, 2000; Johnson, 2003).
Saliva also contains organic compounds. These organic products are mostly proteins
or peptides, including enzymes, mucins, lactoferrin, lysozyme, cystatins and histatins
(Nieuw et al., 2004). The organic and inorganic components of saliva serve a wide
range of functions. Some of the more important of these are summarized in the Table
(1- 4) (Nieuw, 2007).
Table (1-4): Functions of saliva components (Nieuw, 2007).
Mucins Lubricate food
Protect teeth against acid
Help protect against bacteria, viruses, fungi
Digestive enzymes α-Amylase – digests starches
Lipase – digests fats
Protease – digests proteins
Lysozyme
Peroxidases
Lactoferrin
Histatins
Anti-bacterial agents

Review of Literature Chapter One
30
Cystatins
Secretory IgA
Histatins
Cystatins
Anti-fungal, anti-viral agents
Bicarbonate ions
Phosphate ions
Proteins
Help protect teeth and soft tissues against
acidic conditions
Calcium ions
Phosphate ions
Proline-rich proteins
Help maintain mineral content of tooth enamel
Concentrations of some components in whole saliva can be altered because
of differing flow rates from the principal glands. While in the unstimulated rest state,
the parotid glands contribute only a relatively small proportion of the total mix, and the
viscous, mucin-rich saliva from the minor, sublingual and submandibular glands
predominates. When stimulated, however, the parotid glands disproportionately
increase their output of watery saliva, effectively lowering the concentration of mucins
in the mixed saliva (Nieuw, 2007).
1.3.3. Saliva and diagnosis
Local and systemic disorders may disturb and interrupt the complex balanced
functions of saliva, which can lead to mucosal and tooth damages. In other cases,
systemic disorders induce salivary changes without any significant local effects. Many
such changes are of high diagnostic interest because they can be rather specific to the
causing conditions and can be used for screening and early diagnosis of several local
and systemic disorders (Fabian et al., 2007).
Interest in saliva as a diagnostic fluid has grown exponentially in recent
years. Saliva is a unique diagnostic fluid, the composition of which immediately
reflects the sympathetic nervous system, parasympathetic nervous system, HPA axis

Review of Literature Chapter One
31
and immune system response to stress (Khaustova et al., 2010). In addition, salivary
levels of various biochemical parameters have been measured in infectious diseases,
autoimmune diseases, cancers and psychiatric disorders (Edgar, 1992; Boyle et al.,
1994; Streckfus and Bigler, 2002).
Saliva collection is rapid, painless, non-invasive, economically, by
individuals with limited training, no special equipment is needed for the collection of
saliva and yields findings that are reproducible (Akcali et al., 2013).
1.3.4. Saliva and stress
Saliva can be used to monitor the systemic as well as the oral health status
(Buduneli et al., 2011). Furthermore, stress is also a factor that can be followed by
analysis of saliva, especially by determining the levels of stress-related markers (Pani
et al., 2011). These markers have biological properties that influence genesis and
development of PD. There are numerous stress-related molecules involved in different
aspects of stress response (Cortisol, Catecholamines, Chromogranin A, α-amylase,
Neuropeptides) (Akcali et al., 2013).
Physical and psychological stress have been shown to affect the secretion of
salivary proteins (Bosch et al., 2001; Allgrove et al., 2008). Recent investigations
have explored the use of salivary α-amylase as a biomarker of stress and there has been
much interest in its ability to serve as a convenient and non-invasive measure of
sympathetic nervous activity (Van Stegeren et al., 2006; Granger et al., 2007; Davis
and Granger, 2009; Nater and Rohleder, 2009; Spinrad et al., 2009; Fisher et al.,
2010; Strahler et al., 2010; Rudolph et al., 2011). However, due to the role that the
parasympathetic nervous system also plays in the control of protein secretion, a recent
study has questioned the ability of salivary α-amylase to serve exclusively as a
sympathetic marker (Bosch et al., 2011).

Review of Literature Chapter One
32
1.4. Cytokines
Cytokines are soluble proteins, secreted by cells in both the innate and
adaptive host response, act as messenger molecules that transmit signals to other cells,
cytokines have many overlapping functions, they interlinked to form an active network,
which controls the host response, and the responses caused by these substances are
varied and interrelated. In general, cytokines control growth, mobility and
differentiation of lymphocytes, but they also exert a similar effect on other leukocytes
and some non-immune cells (Greenwold et al., 2007).
Between the important members of the cytokine group is interleukins
involved in communication between leukocytes and other cells, such as epithelial cells
and fibroblasts engaged in the inflammatory process, they play role in cell-mediated
immune responses (Lindhe et al., 2008).
In other words cytokines are biologically an active nucleus released by
specific cells that elicit a particular response from other cells on which they act,
cytokines are effective in very low concentrations, are produced transiently, act locally
in the tissue where they are produced (Page et at, 1997). It also has systemic effects
(Okada and Murakami, 1998). They are often self-regulatory and able to induce their
own expression in an autocrine (affecting the behavior of the cell that releases the
cytokine) or paracrine fashion (affecting the behavior of adjacent or even distant cells).
Cytokines act on their target cells by binding to specific receptors and
initiating intracellular second messengers resulting in phenotypic changes (physical
characteristics) in the cell via altered gene regulation (Taylor et al., 2004). There is a
significant overlap and redundancy between the function of individual cytokines. They
don't act in isolation, but rather as a complex network, bringing together element of
both innate and adaptive immunity (Banyer et al., 2000).
Cytokines play an important role in a No. of different processes, but if
expressed inappropriately, they also induce pathology. An inflammatory cytokine is
defined as a cytokine, which is induced during the course of an inflammatory response
and is closely associated with its onset and/or progression. IL1α, IL-1 ß, IL-6, IL-8 and

Review of Literature Chapter One
33
TNF-α are generally classified as pro-inflammatory cytokines (Okada and
Murakami, 1998). Pro-inflammatory cytokines enhance the bactericidal capacity of
phagocytes, recruit additional innate cell populations to sites of infection, induce
dendritic cell maturation and direct the ensuing specific immune response to the
invading microbes (Hornef et al., 2002). Anti-inflammatory cytokines block this
process or at least suppress the intensity of the cascade. Cytokines such as IL4, IL-10,
IL-13 and TGF-β suppress the production of IL1, TNF, chemokine such as IL8, and
vascular adhesion molecules (Dinarello, 2000).
Under pathologic conditions such as those that occur in PD, the balance
between pro- and anti-inflammation is directed towards proinflammatory activity
(Graves and Cochran, 2003). In periodontal tissue destruction three proinflammatory
cytokines, IL-1, IL-6 and TNF-α, appear to have a central role (Nikolopoulos et al.,
2008). Some of the effects attributed to cytokines identified in PD are listed in Table
(1-5) (Ranney, 1991).
Table (1-5): Effects attributed to cytokines identified in periodontal disease (Ranney, 1991).
Function induced or facilitated Cytokine
Antigen presentation IL-1
Attachment of PMN and monocytes to epithelium IL-1, TNF
T-cell growth and proliferation IL-2, IL-6, IL-7
TNF production IL-2
B-cell maturation to plasma cell IL-6
Cytoxicity TNF
Metalloproteinase synthesis IL-2, INF-γ
Bone resorption IL-1, IL-6, TNF, INF-γ

Review of Literature Chapter One
34
1.4.1. Interleukin-1β
Interleukin-1 is a key mediator of the host response to various infectious,
inflammatory and immunologic challenges two distinct polypeptides of IL-1 are
found (IL-lα and IL-lβ), which mediate IL-1 biological activities and bind to the same
cell surface receptor (Dinarello, 2000).
The primary sources of IL-1 are blood monocytes and tissue macrophages,
other specialized cells such as T and B-lymphocytes, various epithelial such as mucosal
epithelial cells ,dendritic cells, endothelial, keratinocytes and fibroblasts cells also
produce IL-1, IL-1β represent the major form described in plasma and other biological
fluids (Maruyama et al., 2005; Nikolopoulos et al., 2008). IL-1β is also present in
the saliva of both healthy and diseased individuals (Perrier et al., 2002). IL-1β also
found to be synthesize and release from acinar and ductal cells in mouse salivary
glands, which may be present as components of whole saliva (Tanda et al., 1998; Seil
et al., 2012). Human tear fluid and GCF also contain IL-1β (Solomon et al. 2001;
Miller et al., 2010).
The relationship between salivary and circulating levels of IL-1β is not clear.
Studies involving antigenic challenge by injection of LPS in mice produced increases
in salivary levels of IL-1β similar to that seen in the circulation in response to LPS
challenge (Yao et al., 2005; Yao et al., 2006; Reinhardt et al., 2012). Another study
that examined both plasma and salivary cytokine responses to LPS injections in pigs
found that plasma levels of TNF-α, but not IL-1β, were increased following injection
of a low dose of LPS. Levels of both cytokines found to be elevated in the pigs’ saliva,
which were higher than those found in plasma (Kakizaki et al., 1999). IL-1β levels are
generally higher in saliva than in plasma or serum, and serum/plasma levels are often
below the limit of detection (Llamas Moya et al., 2006; Brailo et al., 2012; Aliefendic
et al., 2013). One study has reported that the correlation between human passive drool
saliva samples and plasma for IL-1β isn't statistically significant (Williamson et al.,
2012).

Review of Literature Chapter One
35
Interleukin-1 has essential role in T-cell activation, providing one of the
necessary signals for IL-2 production, it's the main mediator of inflammatory processes
by acting on the nervous system (fever, sleep, anorexia), bone marrow derived cells
(chemotaxis and or activation of neutrophils, monocyte and lymphocyte) and on
various tissues (fibroblast proliferation, resorption of cartilage and bone matrices and
stimulation of endothelial cell) (Gourin, 1997; Dinarello, 2009). Most of these
activities are directly attributable to IL-β, but others are mediate in collaboration with
other cytokines such as IL6, IFN and TNF. IL-1 stimulates the production or acts
synergistically with these cytokines and the final biological activity in thus the result
of network of interaction between these various mediators and the biological properties
of IL-1 (Aboyoussef et al., 1998).
1.4.1.1. Interleukin-1β regulation of the periodontal ligament
In periodontal tissues, IL-1 known to stimulate the proliferation of
keratinocytes, fibroblasts and endothelial cells to enhance fibroblast synthesis of type
I procollagen, collagenase, hyaluronate, fibronectin and PGE2. IL-1 is therefore a
critical competent in the homeostasis of periodontal tissues, and its unrestricted
production may lead to tissue damage (Okada and Murakami, 1998), and it's also a
potent stimulator of bone resorption (Shirodaria et al., 2000).
Agarwal et al., in 1998 examined how IL-1β regulates periodontal ligament
(PDL) cell functions that are maintain the attachment between the tooth and alveolar
bone and are constantly challenged during infections by bacterial by-products. In
addition, he demonstrated that IL-1β down-regulates or inhibits the osteoblast-like
characteristics of PDL cells (that can grow new bone in periodontal defects under
certain conditions) and become unable to produce TGF-β1 and proteins needed for
bone mineralization, such as alkaline phosphatase and osteocalcin. In other words, IL-
1β changes the phenotype of the PDL cells, so that they are now able to respond to LPS
and subsequently produce proinflammatory cytokines.
Agarwal et al., in 1998 proposed that proinflammatory cytokines regulate
homeostasis in PDL, a role that may be central to maintaining the stability of both the

Review of Literature Chapter One
36
PDL and the host immune response during inflammation. The potent
immunostimulatory agent, LPS and proinflammatory cytokines are the most significant
factors regulating tissue destruction and remodeling.
1.4.1.2. Interleukin-1β and its role in periodontal disease
Interleukin-1β is a proinflammatory cytokine that is consistently associated
with patients of PD. It is assists inflammatory cells at the site of infection, promotes
bone resorption and stimulates the release of MMPs then degrades the extracellular
matrix (Dinarello, 1997; Aboyoussef et al., 1998; Barksby et al., 2007).
Interleukin-1β is considered the most potent osteoclast-activating factor
within the mammalian organism (Nguyen et al., 1991). In addition, it is the most
important single agent that responsible for periodontal bone destruction at sites of
periodontal inflammation (Cavanaugh et al., 1998; Rasmussen et al., 2000). Not only
within the periodontium but also within the whole organism, the margin between IL-1
induced clinical benefit and IL-1 induced clinical destruction and toxicity seems to be
extremely small (Dinarello, 1998). Other destructive inflammatory diseases like
cardiovascular disease, arthritis, colitis and multiple sclerosis have been associated
with exceeding IL-1 concentrations. Even septic shock itself seems to be a consequence
of an endotoxin induced IL-1 overflow and the cascade of bodily responses there by
set off (Quan et al., 2001; Apostolakis et al., 2008; Bhaskar et al., 2011).
Rawlinson et al., in 2000 investigated cytokine IL-1β and its receptor
antagonist (IL-1ra) in GCF, in patients with adult periodontitis. The cytokine levels
were highest for bleeding periodontitis sites, lower for non-bleeding periodontitis sites
and lowest for periodontal healthy sites. IL-1ra levels were highest in the periodontal
healthy sites, lower for non-bleeding periodontitis sites and lowest for bleeding
periodontitis sites. Rawlinson et al. concluded that a significant relationship exists
between the severity of adult periodontitis and the higher GCF levels of IL and lower
levels of IL antagonist.
In addition, patients suffering from periodontitis who are under stressful
conditions have increased levels of IL-6 and IL-1β in GCF (Giannopoulou et al.,

Review of Literature Chapter One
37
2003; Kamma et al., 2004; Johannsen et al., 2007); similarly, patients with
aggressive forms of periodontitis have elevated levels of IL-6 and IL-1β in serum. On
contrary, another study failed to find any correlation between IL-6, IL-1β and cortisol
levels in peripheral blood of aggressive periodontitis patients (Mengel et al., 2002).
Serum level of pro-inflammatory cytokine IL-lβ was significantly higher in
patients with CP as compared with healthy control (Bodet et al., 2006; Guzeldemir et
al., 2011). Moreover, levels of IL-1β in saliva and GCF have been studied in relation
to gingival and PD and significant correlation to the presence of PD has been found
(Miller et al., 2006; Fitzsimmons et al., 2010; Han and Reynolds, 2012; Lee et al.,
2012). In addition, several reports have been demonstrated that a significant correlation
exists between IL-1β levels in GCF and periodontal parameters such as probing pocket
depth and attachment level (Figueredo et al., 1999; Engebretson et al., 2002; Orozco
et al., 2006). In other clinical study conducted by Guzeldemir et al., in 2011 noticed
that increased serum levels of IL-1β in CP patients have been associated with
inflammation in periodontitis and levels decrease after therapy.
Correspondingly, Gorska et al., in 2003 studied twenty-five patients with
CP in Poland, and found that the concentrations of IL-1β were significantly higher in
serum and gingival tissue biopsies samples in those patients as compared to healthy
control. In contrast, other reports mentioned that there were no differences in the
concentrations of IL-1β between CP patients and healthy control (Queiroz et al., 2008;
Yucel et al., 2008; Elkhouli, 2011).
1.4.1.3. Stress-induced interleukin-1β production
Interleukin-1 is a main mediator of the acute phase inflammatory responses
characterized by alteration in metabolic, endocrinlogic and immunologic functions
(Maruyama et al., 2005). IL-1β levels in the circulation change in response to stress.
(Glaser and Kiecolt-Glaser, 2005; Calcagni and Elenkov, 2006). IL-1β is a critical
mediator of adaptive stress responses as well as stress-associated neuropathology and
psychopathology (Goshen and Yirmiya, 2009; Debnath et al., 2011). IL-1β and its
associated signaling systems may play a role in mediating the response of the circadian

Review of Literature Chapter One
38
timing system to immune challenge as well as the basal functioning of the SCN
(suprachiasmatic nuclei of the anterior hypothalamus of the brain) (Beynon and
Coogan, 2010).
Where psychological and immunological stressors activate the IL-1 system
(brain and peripheral) and elevation in circulation by activated cells of the innate
immune system such as monocytes, macrophages and brainmicroglia then IL-1
activates the HPA axis not only during sickness, but also in response to various
psychological stressors. Interestingly, the physiological and behavioral outcomes of
both immune activation and exposure to other stressors are very similar, including
sympathetic and HPA axis activation, fever and a variety of sickness behavior like
symptoms, such as increased sleep and reduced exploratory, social and sexual
behavior. The interaction between IL-1 and the HPA axis is bi-directional. On the one
hand, IL-1 activates the HPA axis and on the other hand, GCs suppress the production
of IL-1 then brain IL-1 is also involved in the feedback regulation of the HPA axis (Fig.
1-5). This regulation is considered to involve inhibitory actions of GCs via GC
receptors (Goshen and Yirmiya, 2009).
The Levels of IL-1β in saliva and GCF have been observed to change in
response to various types of physical and psychological stressors, similar to the
response seen in the circulation (Ilardo et al., 2001; Deinzer et al., 2004; Zefferino
et al., 2006). Where it's accepted that stress and psychological tension can negatively
influence the immune system and function. The manner in which the host immune
system responds to periodontal pathogenic microorganisms appears to play a
significant role in PD. Of late, IL-1ß has become an important focal point for
periodontal researchers such as Deinzer et al., in 2000 found that supragingival plaque
stimulated the secretion of crevicular IL-1ß, and stress further increased the level of
IL-1ß. IL-1ß is consider the most powerful osteoclast-activating factor in humans. It
increases bone resorption and inhibits bone formation. Increased levels of IL-1β have
been noted in areas experiencing periodontal inflammation. Not only do studies show
that it is associated with future loss of alveolar bone, but the IL-1ß levels decrease

Review of Literature Chapter One
39
following periodontal treatment. Thus, it postulated that IL-1ß has a significant
function in the deterioration of periodontal tissues.
The first study to prove the effects of stress on the levels of IL-1β secretion
in GCF was done by Deinzer et al., in 1999. They conducted clinical oral examinations
during and after a major stressful academic examination on students. Experimentally
induced gingivitis was begun 7 days before the last exam. Increased levels of IL-1β
due to stress were noted at gingivitis sites with no oral hygiene for 21 days as well as
the perfect oral hygiene sites. Deinzer et al., in 2000 published another study, with a
modified experimental design to advance their understanding of the relationship
between stress and immune system relative to periodontal research. In this study, the
period of experimental gingivitis began immediately after stress was terminated, rather
than during the stress period as in 1999 study. Thus, the subjects were exposed to stress
before gingivitis and plaque accumulation were experimentally induced. Stress and
gingivitis weren't concurrently present. After termination of the stress, they wanted to
determine if the after-effects of stress on the plaque-induced IL-1ß secretion would still
be measurable. Eighteen medical students took a major academic examination prior to
the inception of the study, and thirteen students who were controls didn't take any
academic examinations 4 weeks before or after the study. No students in this study
smoked. The results revealed that pre-exposure to academic stress did increase levels
of IL-1β secreted at sites where plaque was allow accumulating in the study group, but
it didn't increase IL-1β levels at sites where perfect oral hygiene was maintained in the
control group. The levels of IL-1β secretion in GCF were most obvious 2 weeks after
stressful examinations. By this time, IL levels in control subjects had already achieved
their maximum (Max.), but the levels in the study subjects continued to rise.
In the first study in 1999, they weren't certain if the after-effects of stress
were cause by the exposure to plaque and stress that were both present at the same
time. Their second study confirmed that plaque and stress needn't be present
concomitantly to induce stress aftereffects. Pre-exposure to a protracted period of
academic stress was sufficient in itself to alter the consequent crevicular IL-1β response

Review of Literature Chapter One
40
to microbial plaque. However, the results indicate that a concomitant exposure to stress
and plaque leads to secretion of a larger level of crevicular IL-1β than successive
exposure to stress and plaque. They also established that after termination of stress, the
effects of stress on IL-1β could persist for at least two weeks (Deinzer et al., 2000).
Furthermore, academic stress has been associated with increased levels of
IL-1β, IL-6 and IL-10 in serum and GCF (Maes et al., 1998; Paik et al., 2000;
Waschul et al., 2003), but the data regarding IL-1β alterations have been inconsistent
with (Dugue et al., 1993; Lacey et al., 2000), Marques-Deak et al., in 2007 and
Johannsen et al., in 2010 reported similarities between IL-1β and IL-6 in both stressed
and non-stressed students.
Fig. 1-5: Interleukin 1 mediates stress-induced activation of the hypothalamic pituitary adrenal
axis. Immunological and psychological stressors increase the levels of interleukin 1 (Goshen and
Yirmiya, 2009).

Chapter Two
Materials and Methods

Materials and Methods Chapter Two
41
Materials and Methods
2.1. Materials
2.1.1. Instruments and Equipment
1. Dental mirrors.
2. Periodontal probes (the University of Michigan O probe, with William’s
markings at (1, 2, 3, 5, 7, 8, 9 and 10mm).
3. Dental tweezers
4. Cotton wool.
5. Gloves and masks.
6. Kidney dish.
7. Pan for sterilized instruments and sterilizer.
8. Disposable test tubes.
9. Case sheets form.
10. Disposable plastic cups.
11. Cooling box and freezer.
12. Marker pen.
13. Adjustable micro pipettes (Fig. 2-2).
14. Pipettes yellow tips (Fig. 2-2).
15. Adjustable micro multichannel pipettes (Fig. 2-2).
16. Water bath (Grant Instruments LTD, Barrington, England).
17. Centrifuge (Kokusan Corporation –Japan) (Fig. 2-3).
18. Filter papers.
19. Test tube racks.
20. Can tubes (Fig. 2-2).
21. Auto vortex mixer (Frost instrument LTD, Great Britain) (Fig. 2-4).
22. Rotatest shaker (R 100 Luck ham, England) (Fig. 2-5).
23. Microplate ELISA washer device (Human, Germany) (Fig. 2-6).

Materials and Methods Chapter Two
42
24. Microplate ELISA reader device (Human, Germany) (Fig. 2-8).
25. Digital timer.
2.1.2. Test Kit
Test kit, salivary IL-1β ELISA kit for research use only; for quantitative
determination of IL-1β in saliva from Salimetrics, USA. Catalog No. 1-3902, 96-well
kit order No. 1302502. Expiry date: 12.Oct.2013 (Fig. 2-1).
Materials Supplied with IL-1β kit are:
1. IL-1β microtitre plate with 96 mouse IL-1β antibodies coated wells.
2. IL-1β standard in a saliva-like matrix 200 pg/ml.
3. IL-1β controls high and low.
4. Wash buffer concentrate.
5. IL-1β assay diluent ready to use.
6. IL-1β sample diluent ready to use.
7. IL-1β antibody conjugate: biotin conjugated to antibody to human IL-1β.
8. Streptavidin conjugated to horseradish peroxidase (HRP).
9. Tetramethylbenzidine (TMB) substrate solution (non-toxic).
10. Three molar stop solution contains sulfuric acid (caustic).
2.2. Methods
2.2.1. Sample description
The original sample was consisted of fifty-four dental students, twenty-three
male and thirty-one female aged (21-23) years were randomly recruited in this follow
up study. They were fifth class students from the collage dentistry in University of
Baghdad and Almustansiriyah. Eleven male and nineteen female were excluded from
this study in the second and third periods because they were not fit for the criteria of
study. Therefore, the final sample was twenty-four students, twelve male and twelve
female continue to follow in this study at three main periods.
The students enrolled voluntarily in the study after a well explanation of
purpose of the investigation and consented to its protocol in period from November
2012 to March 2013.

Materials and Methods Chapter Two
43
All students in this study were systemically healthy, males and females in
the fifth class, cooperative, nonsmoker and not taking any antibiotics during the last
three months (Johannsen et al., 2010).
2.2.2. Exclusion criteria
Pregnant and in menstrual cycle women.
Any student had history of chronic systemic diseases with known associations
with PD (e.g. cardiovascular diseases and diabetes mellitus).
Any student taking psychotropic medication (e.g. prednisone).
Any student with retentive factor of plaque (e.g. orthodontic appliance and
partial denture).
2.2.3. Study design
In this follow up study, clinical periodontal parameters were measured and
stress questionnaire were recorded at three main periods:
1. The first period at least one month before mid-year exam: In this period, the
students were in the normal range of stress scale of DASS criteria and all students
given motivation and instructions about brushing technique and the use of dental
aids to reduce accumulation of dental plaque and gingival inflammation. This
period represents period I, which used as a base line for this study.
2. The second period during mid-year exam: In this period, the students subjected
to stress, also all students given motivation and instructions about brushing
technique and the use of dental aids to reduce accumulation of dental plaque and
gingival inflammation. This period represents period II.
3. The third period at least one month after mid-year exam: In this period, students
were in the normal range of stress scale of DASS criteria. This period represents
period III.
The students were subjected to questionnaire about name, age, full medical
history, periodontal health status and clinical examination of periodontal parameters in
each period by measuring plaque index (PI), gingival index (GI) and BOP for all teeth
except third molars. Clinical examinations were performed after recording the stress

Materials and Methods Chapter Two
44
questionnaires that include 7-items of DASS 21-item questionnaire version (a copy of
case sheet and DASS stress questionnaires are provided in appendices).
Two milliliter (ml) of saliva sample was collected from students one month
before mid-year exam period, during mid-year exam and one month after mid-year
exam period and stored at (-70ºc) for later centrifuged and analysis by ELISA for
determination of IL-1β. The laboratory test done in the Teaching Laboratories of
Baghdad Medical City.
2.2.4. Depression Anxiety and Stress Scale
The DASS 21 version was used in this study, which included three self-
report scales designed to measure the negative emotional states of depression, anxiety
and stress. Each of the three scales contains 7 items. Students were answered about
stress questionnaires during the three periods before the examination of clinical
periodontal parameters; Table (2-1). The items of stress scale are sensitive to levels of
chronic non-specific arousal. It assesses difficulty relaxing, nervous arousal, being
easily agitated, over-reactive and impatient.
Respondents were asked to use 4-points of severity scales to rate the extent
to which they have experienced each state over the past week. Scores of stress
calculated by summing the scores for the relevant items (1, 6, 8, 11, 12, 14 and 18).
Then, the sum for stress scores evaluated by the severity-rating index, Table (2-2)
(Lovibond and Lovibond, 1995).
The DASS case sheet include name of subject, date of questionnaire then
instruct the subject to understand each statement and refer a suitable No. either 0, 1, 2
or 3, which indicates how much the statement applied to his or her over the past week.
There are no right or wrong answers and don't spend too much time on any statement.
The rating scale is as follows:
0 Didn't apply to me at all.
1 Applied to me to some degree, or some of the time.
2 Applied to me to a considerable degree, or a good part of time.
3 Applied to me very much, or most of the time.

Materials and Methods Chapter Two
45
Table (2-1): Stress questionnaires of DASS 21-item version (Lovibond and Lovibond, 1995).
1. I found it hard to wind down 0 1 2 3
2. I tended to over-react to situations 0 1 2 3
3. I felt that I was using a lot of nervous energy 0 1 2 3
4. I found myself getting agitated 0 1 2 3
5. I found it difficult to relax 0 1 2 3
6. I was intolerant of anything that kept me from
getting on with what I was doing
0
1
2
3
7. I felt that I was rather touchy 0 1 2 3
Table (2-2): DASS severity-rating index (Lovibond and Lovibond, 1995).
2.3. Clinical periodontal parameters examination
Clinical Periodontal examination was performed by using the University of
Michigan O probe according to the following criteria:
2.3.1. Plaque index
The four surfaces of each tooth except 3rd molar were examined and scored
according to PI by (Silness and Loe, 1964).
The scores and criteria for this system as proposed by authors:
Score 0: No plaque in the gingival area.

Materials and Methods Chapter Two
46
Score 1: A film of plaque adhering to the free gingival margin and adjacent area
of the tooth surface, the plaque may be recognized only by running a probe
across the tooth surface.
Score 2: Moderate accumulation of soft deposits within the gingival pocket, on
the gingival margin and or adjacent tooth surface, which can be seen by naked
eye.
Score 3: Abundance of soft matter within the gingival pocket and or on the
gingival margin and adjacent tooth surface.
2.3.2. Gingival index
The gingival inflammation at the four surfaces of each tooth except 3rd molar
was assessed using the criteria of the GI (Loe and Silness, 1963). The criteria of this
index then modified by Loe in 1967 as the following:
Score 0: Absence of inflammation/normal gingival.
Score 1: Mild inflammation, slight change in color, slight edema, no BOP.
Score 2: Moderate inflammation, moderate redness, glazing and edema, BOP.
Score 3: Sever inflammation, marked redness and ulceration, tendency to
spontaneous bleeding.
2.3.3. Bleeding on probing
A periodontal probe was inserted to the bottom of the periodontal pocket and
was moved gently along the tooth (root) surface. If bleeding occurs within 30 seconds
after probing, the site was given as positive score (1) and a negative score (0) for the
non-bleeding site (Carranza et al., 2006).
2.4. Saliva sample collection and preparation
The students were instructed not eat or drink (except water) for at least 60
minutes before collection of the samples. Acidic or high sugar foods can compromise
assay performance by lowering saliva PH and influencing bacterial growth. To
minimize the effect of these factors, the student was rinsed his/her mouth thoroughly
with water then waited 2 minutes for water clearance before the sample was collected.

Materials and Methods Chapter Two
47
The subject was sat in a relax position then the whole unstimulated mixed
saliva was collected by tilting the head forward, allowing the saliva to pool on the floor
of the mouth, and then drop his/her saliva into the polyethylene tube until 2ml was
collected, a standardized method according to (Thylstrup and Fejerskov, 1994).
The tube was labeled with the No. of the subject that was previously written
on the case sheet and record the time and date of sample collection. Samples visibly
contaminated with blood were discarded (Schwartz and Granger, 2003; Kivlighan
et al., 2004). Saliva was collected between 8-12 a.m. and before clinical periodontal
examination.
After sample collection, it was put in a small cooling box to keep sample
cold within 30 minutes and freezing at (-70ºC) within 4 hours of collection until
assayed, in order to prevent bacterial growth and minimize loss of IL-1β in the sample.
Freezing saliva samples were precipitate mucins. On day of assay, thaw
completely by putting in the water bath at 37ºC then centrifuge at 3000 rpm for 15
minutes. Centrifuging removes mucins and other particulate matter, which may
interfere with antibody binding, leading to false elevated results, the clear supernatant
was separated by micropipette into can tubes then all samples were diluted 15 times in
IL-1β sample diluent before adding to assay plate.
2.5. Detection of IL-1β
2.5.1. Test principle
The ELISA test kit provides quantitative in vitro assay for the determination
of IL-1β in saliva. The test kit contains a microtitre plate that was coated with mouse
antibodies to IL-1β. IL-1β in standards and unknowns attach to the antibody binding
sites. After incubation, unbound components were washed away. Biotin conjugated to
goat antibodies to human IL-1β were added and attached to the bound IL-1β. After
incubation, unbound components were washed away. Streptavidin conjugated to HRP
was added and binds to the biotin conjugated to the goat antibodies. Bound
streptavidin-HRP was measured by the reaction of the HRP enzyme on the substrate
TMB. This reaction produces a blue color. A yellow color was formed after stopping

Materials and Methods Chapter Two
48
the reaction with 3-molar sulfuric acid (Fig. 2-7). Optical density (OD) was read on a
standard plate reader at 450 nm. The amount of streptavidin-HRP detected is
proportional to the amount of IL-1β present (Chard, 1990).
2.5.2. Reagent preparation
All reagents and microtitre plate were bring in sealed foil pouch to room
temperature. A minimum of 1.5 hours is for the 14ml of IL-1β assay diluent
used in steps 7 and 10 to come to room temperature. It was important to keep
the foil pouch with the plate strips closed until warmed to room temperature (as
humidity may have an effect on the coated wells).
All reagents were mixed before use.
Each control vial was reconstituted with 1.0ml of deionized water then let it to
sit 20 minutes at room temperature before using. It was mixed well immediately
before use.
IL-1β standard was reconstitute with deionized water according to the volume
on the standard vial label then let it to sit 20 minutes at room temperature before
using. It was mixed well immediately before use.
Prepared serial dilutions of the IL-1β standard as follows:
1. Labeled 6 can tubes 2 through 7.
2. 300μL of IL-1β assay diluent was pipetted into tubes 2 through 7.
3. Serially diluted the IL-1β standard by adding 300μL of the 200pg/ml standard
(tube 1) to tube 2 and mixed well. After changing pipette tips, removed 300μL
from tube 2 to tube 3 and mixed well then continue for tubes 4, 5, 6 and 7.
The final concentrations of standards for tubes 1 through 7, respectively, were
200pg/ml, 100pg/ml, 50pg/ml, 25pg/ml, 12.5pg/ml, 6.25pg/ml and
3.13pg/ml. Standard concentrations in pmol/L were 11.8, 6.0, 3.0, 1.5, 0.7,
0.4 and 0.2.
Prepared the wash buffer solution by diluting wash buffer concentrate 10-fold
with room-temperature deionized water (100ml of wash buffer concentrate to
900ml of deionized water).

Materials and Methods Chapter Two
49
2.5.3. Procedure
Step 1: The plate layout was determined.
Step 2: 14ml of IL-1β assay diluent was pipette into each of two different disposable
tubes and cap. They were set aside for 7 and 10 steps.
Step 3: Saliva was diluted 15 times in IL-1β sample diluent by using 20μL of saliva to
280μL of IL-1β sample diluent.
Step 4:
• 100μL of each standard, control and unknown (diluted) sample was pipette into
appropriate wells. Standards, controls and unknown samples were assayed in duplicate.
• 100μL of IL-1β assay diluent was pipetted into the duplicate zero wells.
Step 5: The plate was covered with adhesive cover provided then it was incubated at
room temperature for 1 hour on a horizontal shaker set at 500 rpm.
Step 6: The plate was washed 4 times with wash buffer solution; washing was done by
pipetting 300μL of wash buffer into each well and then decanting the liquid into a sink.
After each wash, the plate was blotted on paper towels but didn't let the wells dry out.
Step 7: The antibody conjugate was diluted 1:500 by adding 28μL of the antibody
conjugate to the 14ml of IL-1β assay diluent prepared in step 2 (antibody conjugate
tube was centrifuged for a few minutes to bring the liquid down to the tube bottom).
Immediately mixed the diluted antibody solution and added 100μL to each well by
using a multichannel pipette.
Step 8: The plate was covered with adhesive cover provided then it was incubated at
room temperature for 2 hour on a horizontal shaker set at 500 rpm.
Step 9: Repeated the washing procedure at step 6.
Step 10: The streptavidin-HRP was diluted 1:200 by adding 70μL of the streptavidin-
HRP to the 14ml of IL-1β assay diluent prepared in step 2 (Streptavidin-HRP tube was
centrifuged for a few minutes to bring the liquid down to the tube bottom). Immediately
mixed the diluted solution and added 100μL to each well using a multichannel pipette.
Step 11: The microtiter plate was incubated at room temperature for 20 minutes and
mixed constantly at 500 rpm.

Materials and Methods Chapter Two
50
Step 12: Repeated wash procedure from step 6.
Step 13: Added 100μL of TMB solution to each well with a multichannel pipette.
Step 14: The plate was incubated in the dark at room temperature for 20 minutes on a
horizontal shaker set at 500 rpm and avoided direct sunlight.
Step 15: Added 50μL of stop solution with a multichannel pipette into each well.
Step 16:
• The plate was mixed at room temperature for 3minutes on a horizontal shaker that set
at 500 rpm. All wells were turned yellow.
• The absorbencies were read in a plate reader at 450nm within 10 minutes of adding
stop solution. (It was corrected at 630nm).
2.5.4. Calculations of IL-1β
1. The average OD was computed for all duplicate wells.
2. The concentrations of the controls and unknowns were determined by using a
quadratic parameter curve fit of software program (Fig. 2-9).
3. All results for unknown samples were multiplied by the dilution factor of 15.
2.6. Calibration
The purpose of calibration, training and testing the design of the study,
calibration was carried out about three weeks before the conduction of the actual work,
for accurate calibration of the examiner for the clinical periodontal parameters was
assessed by:
(1) Inter examiner calibration: Four sites of all teeth except third molars were examined
by the examiner and supervisor for five subjects.
(2) Intra examiner calibration: Four sites of all teeth except third molars were examined
twice by the same examiner with interval of one week between the two examinations.
Measurements obtained by the inter- and intra-examiner calibrations were
computed and the results were with non-significant (NS) differences (P ≥ 0.05), when
student t-test was applied.

Materials and Methods Chapter Two
51
2.7. Statistical analysis
Data were processed and analyzed using (IBM® SPSS® Statistics version 21,
2012). Both descriptive and inferential analysis were used in order to analyze and
assess the results of the study.
1. Descriptive statistics:
a) Tables (Frequencies and percentages).
b) Ratio
c) Arithmetic mean (Mean).
d) Standard deviation (SD).
e) Standard error (SE).
f) Two extreme values (Min. and Max.).
g) Graphical presentation by Bar charts.
2. Inferential statistics:
These used to accept or reject the statistical hypotheses, which included:
a) Chi-square test.
b) student t-test
c) Analysis of variance (ANOVA) with least significant differences (LSD).
d) Pearson's correlations coefficient (R) was used for testing the correlation
between the two independent variables: the clinical and immunological
parameters.
The level of NS was P ≥ 0.05, the level of significant (S*) was at P ≤ 0.05,
the level of highly significant (HS**) when P ≤ 0.01.

Materials and Methods Chapter Two
52
Fig. 2-1: Salimetrics salivary interleukin-1β kit.
Fig. 2-2: A. Adjustable micropipettes and pipettes yellow tips.
B. Adjustable micro multichannel pipettes.
Fig. 2-3: Centrifuge (Kokusan Corporation–Japan).

Materials and Methods Chapter Two
53
Fig. 2-4: Auto vortex mixer (Frost instrument LTD, Great Britain).
Fig. 2-5: A. Rotatest shaker (R 100 Luck ham, England).
B. Microtitre plate of interleukin-1β kit.
Fig. 2-6: Microplate ELISA washer device (Human, Germany).

Materials and Methods Chapter Two
54
Fig. 2-7: Microtitre plate of interleukin-1β kit after adding stopper solution.
Fig. 2-8: Microplate ELISA reader device (Human, Germany).

Materials and Methods Chapter Two
55
Fig. 2-9: Quadratic parameter curve fit of software program.

Chapter Three
Results

Results Chapter Three
56
Results
3.1. Descriptive statistical analysis of demographic data
During this study, twenty-four dental students were involved; they were
continuous to followed up during three main periods (1st period/before examination
was called period I, 2nd period/during examination was called period II, 3rd period/after
examination was called period III). The ages of students ranged between (21-23) years
with a mean age of 22 and SD of 0.624 as shown in table (3-1). Furthermore, 50% of
students were female and 50% of students were male. Female to male ratio in this study
was 1:1.
Table (3-1): Descriptive statistical results of students' ages.
Number Min. Max. Mean SD
Age 24 21 23 22 0.62409
3.2. Clinical periodontal parameters analysis
3.2.1. Plaque index
The descriptive statistical results of PLI for each period were shown in table
(3-2); it was shown that the mean of PLI was elevated in period II in comparison with
I and III periods as shown in figure (3-1). Mean ± SD of PLI were 1.0283 ± 0.24701
in period II, while mean ± SD of PLI were 0.6375 ± 0.25674 and 0.2300 ± 0.22733
respectively in periods I and III.
Table (3-2): Descriptive statistical results of plaque index for each period.
Periods No. Min. Max. Mean SD SE
Period I 24 0.23 1.14 0.6375 0.25674 0.05241
Period II 24 0.56 1.40 1.0283 0.24701 0.05042
Period III 24 0.01 0.73 0.2300 0.22733 0.04640

Results Chapter Three
57
Fig. 3-1: Bar chart graph for means of plaque index for each period.
For comparisons among periods, ANOVA test was used in this study; the
results showed that there were HS difference at P-value ≤ 0.01 among and within
periods, Table (3-3).
Least significant difference test (LSD) was performed for multiple
comparisons between each two periods; the results showed that there were HS
differences at P-value ≤ 0.01, Table (3-4).
Table (3-3): ANOVA test for plaque index.
ANOVA Sum of Squares
(SS)
Degree of
freedom
(df)
Mean Square
(MS)
F-test P-value Sig.
Among periods 7.649 2 3.825
64.240
0.000
**
Within periods 4.108 69 0.060
Total 11.757 71
P ≤ 0.01 High significant (HS) **

Results Chapter Three
58
Table (3-4): LSD test to compare the means of plaque index between each two periods.
P ≤ 0.01 High significant (HS) **
3.2.2. Gingival index
The descriptive statistical results of GI for each period were shown in table
(3-5); it was shown that the mean of GI was elevated in the period II in comparison
with the periods I and III as shown in figure (3-2). Where mean ± SD of GI were 0.6004
± 0.27085 in the period II, while mean ± SD of GI were 0.2029 ± 0.16843 and 0.1054±
0.08444 respectively in the periods I and III.
Table (3-5): Descriptive statistical results of gingival index for each period.
Periods Mean Difference (MD) SE P- value Sig.
Period I
Period II -0.39083 0.07044 0.000 **
Period III 0.40750 0.07044 0.000 **
Period II Period III 0.79833 0.07044 0.000 **
SE SD Mean Max. Min. No. Periods
0.03438 0.16843 0.2029 0.56 0.03 24 Period I
0.05529 0.27085 0.6004 1.17 0.20 24 Period II
0.01724 0.08444 0.1054 0.31 0.02 24 Period III

Results Chapter Three
59
Fig. 3-2: Bar chart graph for means of gingival index for each period.
For comparison among periods, ANOVA test was used in this study; the
results showed that there were HS difference at P-value ≤ 0.01 among and within
periods, Table (3-6).
For multiple comparisons between each two periods, LSD test was
performed. The results showed that there were HS differences at P-value ≤ 0.01
between periods I and II; II and III, while there was NS difference at P-value ≥ 0.05
between periods I and III as shown in Table (3-7).
Table (3-6): ANOVA test for gingival index.
ANOVA SS df MS F-test P-value Sig.
Among periods 3.300 2 1.650
45.475
0.000
** Within periods 2.504 69 0.036
Total 5.804 71
P ≤ 0.01 High significant (HS) **

Results Chapter Three
60
Table (3-7): LSD test to compare the means of gingival index between each two periods.
P ≥ 0.05 Non-significant (NS)
P ≤ 0.01 High significant (HS) **
3.2.3. Bleeding on probing
Descriptive statistical results for BOP were described in table (3-8); it was
clearly shown that the No. and percentage of bleeding sites in the period II was higher
than the periods I and III.
Where in the period II the No. and percentage of healthy sites were 2508
(93.3 %), whereas the bleeding sites were 180 (6.7 %). While in the period I the No.
and percentage of healthy sites were 2624 (97.6 %), whereas the bleeding sites were
64 (2.4 %). While in the period III the No. and percentage of healthy sites were 2657
(98.8 %), whereas the bleeding sites were 31 (1.2 %) as shown in figure (3-3).
For comparison of all periods, chi-square test was used; the results showed
that there was HS difference at P-value ≤ 0.01 among periods as shown in table (3-8).
Inter-period comparisons for BOP was shown in table (3-9); the results showed that
there were HS differences at P-value ≤ 0.01 of the comparison between each two
periods.
Periods MD SE P-value Sig.
Period I
Period II -0.39750 0.05499 0.000 **
Period III 0.09750 0.05499 0.081 NS
Period II Period III 0.49500 0.05499 0.000 **

Results Chapter Three
61
Table (3-8): Percentages and numbers of scores of bleeding on probing for each period and
comparison among periods.
Scores of BOP
Period I Period II Period III
No. % No. % No. % Chi-
square
df P-value Sig.
0 (no bleeding) 2624 97.6% 2508 93.3% 2657 98.8%
138.339
2
0.000
**
1(bleeding sites) 64 2.4% 180 6.7% 31 1.2%
P ≤ 0.01 High significant (HS) **
Table (3-9): Inter-period comparisons for bleeding on probing between each two periods.
Sig. P-value df Chi-square Periods
** 0.000 1 57.770 Between period I and II
** 0.001 1 11.669 Between period I and III
** 0.000 1 109.516 Between period II and III
P ≤ 0.01 High significant (HS) **
Fig. 3-3: Bar chart graph for percentages of scores of bleeding on probing for each period.

Results Chapter Three
62
3.3. Stress analysis
Descriptive statistical results for stress were shown in table (3-10); it was
clearly appeared that all students in the period II were within mild to severe range of
stress, while in the period I and III were within normal range of stress.
In the period II, the Nos. and percentages of students in the mild, moderate
and sever ranges were 4 students (16.7 %), 15 students (62.5 %) and 5 students (20.8
%) respectively. Whereas in the periods I and III, Nos. and percentages of students in
normal range were 24 students (100 %) while in the other ranges were zero (0.0 %).
For comparison among periods, chi-square test was used; the results showed
that there was HS difference at P-value ≤ 0.01 among periods as shown in table (3-10).
Table (3-10): Percentage and number of stress range and comparison among periods.
P ≤ 0.01 High significant (HS) **
Scores of
Stress
Period I Period II Period III
No % No % No % Chi-square df P-value Sig.
Normal
(0-14)
24 100.0% 0 0.0% 24 100.0%
72.000
6
0.000
**
Mild
(15-18)
0 0.0% 4 16.7% 0 0.0%
Moderate
(19-25)
0 0.0% 15 62.5% 0 0.0%
Sever
(26-33)
0 0.0% 5 20.8% 0 0.0%
Extremely
sever (34)
0 0.0% 0 0.0% 0 0.0%

Results Chapter Three
63
3.4. Salivary interleukin-1β statistical analysis
The descriptive statistical results of IL-1β for each period were shown in
table (3-11); it was shown that the mean of IL1β was elevated in the period II in
comparison with the periods I and III as shown in figure (3-4). Where mean ± SD of
IL-1β were 552.5669 ± 275.62299 pg/ml in the period II, while mean ± SD of IL-1β
were 269.9206 ± 158.79005 pg/ml and 114.0194 ± 72.51898 pg/ml respectively in the
periods I and III.
Table (3-11): Descriptive statistical results of interleukin-1β for each period.
Fig. 3-4: Bar chart graph for means of interleukin-1β for each period.
SE SD Mean Max. Min. No. Periods
32.41288 158.79005 269.9206 674.85 60.39 24 Period I
56.26131 275.62299 552.5669 1228.07 122.04 24 Period II
14.80287 72.51898 114.0194 263.96 39.72 24 Period III

Results Chapter Three
64
For comparison among periods, ANOVA test was used in this study; the
results were showed that there was HS difference at P-value ≤ 0.01 among and within
periods, Table (3-12).
Least significant difference test (LSD) was performed for multiple
comparisons between each two periods; the results showed that there were HS
differences at P-value ≤ 0.01, Table (3-13).
Table (3-12): ANOVA test for interleukin-1β level.
ANOVA SS df MS F P-value Sig.
Among periods 2372144.097 2 1186072.049
33.429
0.000
** Within periods 2448150.213 69 35480.438
Total 4820294.310 71
P ≤ 0.01 High significant (HS) **
Table (3-13): LSD to compare the means of interleukin-1β between each two periods.
Periods
MD SE P- value Sig.
Period I
Period II -282.64625 54.37557 0.000 **
Period III 155.90125 54.37557 0.005 **
Period II Period III 438.54750 54.37557 0.000 **
P ≤ 0.01 High significant (HS) **

Results Chapter Three
65
3.5 Correlations between clinical periodontal parameters with
immunological marker (salivary interleukin-1β) and stress
Pearson's correlation coefficient (R) of immunological marker (salivary IL-
1β) with clinical periodontal parameters (PLI, GI and BOP) and stress were strong
(positive) correlations and HS differences at P-value ≤ 0.01 in all parameters, except
BOP score (0) the correlation was inverse (negative) correlation and NS difference at
P-value ≥ 0.05 as shown in table (3-14) and figure (3-5).
Table (3-14): Pearson's correlation coefficient of salivary interleukin-1β with plaque index,
gingival index, bleeding on probing score (1 and 0) and stress level among periods.
Salivary IL-1β
R P-value Sig.
PLI 0.543 0.000 **
GI 0.504 0.000 **
BOP score (1) 0.411 0.000 **
BOP score (0) -0.090 0.450 NS
Stress 0.661 0.000 **
P ≥ 0.05 Non-significant (NS) P ≤ 0.01 High significant (HS) **
Fig. 3-5: Bar chart graph for correlations of interleukin-1β with (plaque index, gingival
index, bleeding on probing score (1)) and stress.

Results Chapter Three
66
Pearson's correlation coefficient of stress with immunological parameter
(salivary IL-1β) and clinical periodontal parameters (PLI, GI and BOP) were strong
(positive) correlations and HS differences at P-value ≤0.01 in all parameters, except
BOP score (0) the correlation was inverse (negative) correlation and NS difference at
P-value ≥ 0.05 as shown in table (3-15) and figure (3-6).
Table (3-15): Pearson's correlation coefficient of stress with salivary interleukin-1β and
plaque index, gingival index, bleeding on probing score (1 and 0) among periods.
P ≥ 0.05 Non-significant (NS) P ≤ 0.01 High significant (HS) **
Fig. 3-6: Bar chart graph for correlations of stress with (plaque index, gingival index,
bleeding on probing score (1)) and interleukin-1β.
Stress
R P-value Sig.
PLI 0.715 0.000 **
GI 0.684 0.000 **
BOP score (1) 0.545 0.000 **
BOP score (0) -0.016 0.450 NS
Salivary IL-1β 0.661 0.000 **

Chapter Four
Discussion

Discussion Chapter Four
67
Discussion
Periodontal disease is a multifactorial disease and research promoting the
identification of risk factors are gaining importance for treatment and prevention. It's
suggested that stress, depression and ineffective coping may contribute to development
of PD (Rosania et al., 2009). Stress is term refers to physiological and psychological
reactions that mobilize an organism’s defense against external or internal threats to
stressors. Different kinds of stress have been defined, such as work related, negative
life experiences and socioeconomic status (Genco et al., 1999; Mead et al., 2001;
Soares et al., 2007). Chronic stress may tend to have a negative effect on
immunological response of body, which represents an important example of mind-
body interaction that leading to an imbalance between host and parasites and further
resulting in periodontal breakdown (Reners and Brecx, 2007; Johannsen et al.,
2010).
Interleukin-1 is one of the most critical molecules involved in
neuroendocrine and neurobehavioral stress responses (Goshen and Yirmiya,
2009). In addition, IL-1 is important pro-inflammatory cytokine in pathogenesis of PD
(Dayan et al., 2004). Therefore, the current study is the first of its kind in Iraq that
reflect the association between examination stress, salivary IL-1β and periodontal
health status.
4.1. Demographic data
The results of this study involving dental students because recent studies
have reported high levels of stress among dental and medical students (Omigbodun et
al., 2006; Smith et al., 2007; Johannsen et al., 2010), aged 21-23 years of the fifth
class, we selected this class because final class represent the more stress class, they
follow up in three main periods:
1. The first period (period I) before mid-year exam: It was used as a base line for this
study to assess periodontal health status and salivary IL-1β at least one month before

Discussion Chapter Four
68
mid-year exam to avoid the effect of examination stress on students because an
academic exam can be considered a psychological stressor, consisting of a period
of preparation, anticipation and then the exam itself (Deinzer et al., 1999;
Johannsen et al., 2010).
2. The second period (period II) during mid-year exam: in this period the students
during the stress at the third weeks of examination because IL-1β reach to the peak
level with gingival inflammation at this time (Deinzer et al., 1999). Students who
participated in a major exam had significantly more dental plaque and more gingival
inflammation compared with students who didn't participate in any exam (Deinzer
et al., 2005; Johannsen et al., 2010). Furthermore, academic stress has been
associated with increased levels of IL-1β, IL-6 and IL-10 in serum and GCF (Maes
et al., 1998; Paik et al., 2000; Waschul et al., 2003).
3. The third period (period III) at least one month after mid-year exam to avoid any
after-effects of stress on periodontal health status and IL-1β (Deinzer et al., 2000;
Johannsen et al., 2010).
4.2. Periodontal health status
4.2.1. Plaque index
The mean value of PLI of period II was significantly higher than that of
periods I and III. This result could be related to the effect of stress to achieve good oral
hygiene among the second period. The changes occurring in behavioral of stressful
students, as inattention leads to improper oral hygiene mechanism, have been
considered as a reason for association between stress and gingivitis.
Over the past decade, it has become more apparent that stress can negatively
influence oral health status, which can lead to increased amounts of dental plaque,
gingival inflammation and more severe periodontitis (Klages et al., 2005; Johannsen
et al., 2007). In the present study, students were found to have more plaque
accumulation and gingival inflammation during an exam period, suggesting that
examination stress might influence periodontal health status. This result is in

Discussion Chapter Four
69
conformity with Deinzer et al., in 2001; Deinzer et al., in 2005 and Johannsen et al.,
in 2010, who found increased dental plaque and gingival inflammation in students who
experienced examination stress. The increased levels of dental plaque and gingival
inflammation in the present study may be explained by behavioral changes in the
stressed students, for example, oral hygiene might be less effective and ⁄ or reduced in
frequency during this time of stress. After the exam period, a reduced amount of dental
plaque was found and this may partly be explained by the Hawthorne effect (Adair,
1984), meaning that panelists involved in clinical trials might be affected because of
attention and interest.
4.2.2. Gingival index
There is a significant difference in the mean values of GI among periods.
This elevation of GI reflects a higher inflammation in the period II than periods I and
III. This result is agrees with Deinzer et al., in 1999; Deinzer et al., in 2005 and
Johannsen et al., in 2010.
Regarding gingival inflammation during examination stress, two possible
explanations may be considered, either by the direct influence of stress on immune
system (biologic model), through release of stress hormones or by an influence of
increase plaque accumulation during the exam period leading to gingival inflammation,
as the plaque is the causative factor of gingival inflammation (behavioral model), both
resulting in increased susceptibility to PD (Genco et al., 1998; Boyapati and Wang,
2007).
4.2.3. Bleeding on probing
The percentage of sites with BOP was significantly higher in period II than
periods I and III. The potential altered abilities of period II to perform effective oral
hygiene could result in an increased BOP that exacerbates the risk for enhanced tissue
destruction in PD. Moreover, interesting observations regarding the complexity of the
oral and systemic challenge provide unique mechanisms by which dysregulation of
host responses could occur due to immunologic and behavioral changes, related to
examination stress may be lead to PD. Where examination stress appears to affect

Discussion Chapter Four
70
periodontal health status, shown by more plaque accumulation, gingival inflammation
and increased amounts of proinflammatory cytokine salivary IL-1β therefore
examination stress appears as a possible risk factor for gingivitis and periodontitis. This
result is in agreement with Deinzer et al., in 1999; Deinzer et al., in 2005 and
Johannsen et al., in 2010.
4.3. Stress data
The students registered their perceived stress on DASS-21. The DASS is a
simple-to-administer, reliable and a valid measurement tool for evaluating stress
(Lovibond and Lovibond, 1995). The DASS summarized magnitude of psychological
derangement by summing the scores obtained from stress domain only from this scale,
that ranged from no stress at all, to the extremely sever stress imagined. Where students
were asked how stressed they felt on a 4-points scale before, during and after mid-year
exam to compare between them. According to the results of this study, the percentage
of stress was significantly higher in period II than period I and III. Where the DASS
scores were significantly higher during the exam period compared with before and after
the mid-year exam.
This result is agrees with Johannsen et al., in 2010, which used a visual
analogue scale (VAS) to register the perceived stress of students during the exam
period compared with after the exams, Michael et al., in 2011, which used DASS to
psychological distress in diurnal variations, Singh et al., in 2012, which used DASS in
measuring stress and it's effect on cortisol level in medical student and Premkumar et
al., in 2013, which used DASS in measuring changes in mood and assessed the
correlation with cortisol. The proper explanation for this result was dental students who
participated in the exam had significantly more stress compared with students who
didn't participate in any exam.

Discussion Chapter Four
71
4.4. Salivary interleukin-1β level
Salivary IL-1β was used in this study instead of serum IL-1β because saliva
has been used as a diagnostic biofluid to measure host responses to a variety of
triggering factors in systemic and oral diseases (Forde et al., 2006). Saliva analyses
have advantages of quick and easy sample collection not requiring specialized
equipment or personnel. Moreover, its sampling is painless and noninvasive, therefore,
saliva sampling doesn’t cause stress to students. It's one of the most promising
mediums for its diagnostic potential for various diseases including stress-related
diseases, and it's readily available any time and for repeated samplings (Wolff et al.,
2004). If the relationship between stress and PD can be verified in saliva samples,
diagnosing stress by means of saliva analysis can be helpful for differential diagnosis
from the evidence-based point of view in various medical fields (Akcali et al., 2013).
In addition, IL-1β levels are generally higher in saliva than in plasma or serum, and
serum/plasma levels are often below the limit of detection (Llamas Moya et al., 2006;
Brailo et al., 2012; Aliefendic et al., 2013).
Interleukin-1 is important pro-inflammatory cytokine in the pathogenesis
of PD (Dayan et al., 2004). It induces widespread gene expression of
cyclooxygenase-2, inducible nitric oxide synthesis and MMP, which results in
activation of osteoclasts, bone resorption and downregulation of type I collagen
expression in bone (Okada and Murakami, 1998; Graves and Cochran, 2003).
Although both isoforms of IL-1 (1L-1α and IL-1β) have similar biological activities
and appear to be contributory, but IL-lβ is more potent in stimulating bone
resorption and is the form more frequently occurring in periodontitis (Stashenko et
al., 1987). In addition IL-1β is a critical mediator of adaptive stress responses as well
as stress-associated neuropathology and psychopathology (Goshen and Yirmiya,
2009; Debnath et al., 2011). For all these reasons, salivary IL-1β was used in this
study.

Discussion Chapter Four
72
In the present study, salivary level of IL-1β inflammatory related cytokine
was assessed; the mean value of IL-1β of period II was significantly higher than that
of the period I and III. Where IL-1β stimulates the HPA axis activity and associated
with immune system and inflammation response during stress (Goshen and Yirmiya,
2009).
This result is agrees with Deinzer et al., in 1999 and Deinzer et al., in 2000,
who found higher amounts of IL-1β in GCF during academic examination stress and
Brydon et al., in 2005, who found higher amounts of IL-1β in human mononuclear
cells during psychological stress and disagrees with Marques-Deak et al., in 2007,
who reported similarities of IL-1β level in both stressed and non-stressed individuals
and Johannsen et al., in 2010, who reported non-significant difference of IL-1β level
between during and after exam. One problem in stress studies in general could be the
difficulty to know when the influence on the biomarkers by a stress period is over. An
explanation to why Marques-Deak et al., in 2007 and Johannsen et al., in 2010 didn't
find high IL-1β levels in GCF, despite a high degree of inflammation could be that
hormonal stress inhibits IL-1β response to stress (feedback regulation of IL-1β)
(Williams and Yarwood, 1990; Chrousos, 1995; Genco et al., 1998; Nguyen et al.,
2000). In addition, some studies have shown that the levels of pro-inflammatory
cytokine, IL-1β, are increased in patients with depression (Johannsen et al., 2006;
Johannsen et al., 2007; Von Kanel et al., 2007); however, contradictory results have
also been described (Rothermundt et al., 2001).
Interleukin-1β level is a sensitive and reliable marker of chronic
inflammatory disease activity and IL-1β elevation may demonstrate tissue destruction
(Lacopino et al., 1997; Keles et al., 2005). Thus, in this study the detection of elevated
levels of IL-1β in the saliva of subjects with stress was consistent with the cytokine's
role in inflammation and suggests that salivary lL-1β may be a good marker of
periodontal inflammation.

Discussion Chapter Four
73
4.5. Correlations between stress, interleukin-1β and clinical periodontal
parameters
There was a strong positive correlations between stress, pro-inflammatory
cytokine(IL-1β) and clinical periodontal parameters, when stress increase pro-
inflammatory cytokine IL-1β level, plaque accumulation, gingival inflammation and
bleeding sites will be increase. These results of present study were in agreement with
Maes et al., in 1998; Paik et al., in 2000; Waschul et al., in 2003 where stress alters
immune function and affects different immune cells, hence increase production of pro-
inflammatory cytokine (humoral immunity) and decrease cellular immunity that lead
to periodontal inflammation. In addition, stress was related to PD because
psychological stress can directly affect periodontal health status by various biological
(physiological) mechanisms; also, it can have indirect effects through the behavioral
(psychological) changes in lifestyle such as ignoring oral-hygiene measures that lead
to increased levels of dental plaque, smoking more heavily and consuming more fat
and sugar in diet (LeResche and Dworkin, 2000).
Periodontal disease is develop during stressful condition by tissue destroying
factors such as IL-1β and MMPs activated by periodontal pathogens, as well as by the
direct effects of pathogenic bacteria in dental plaque (Grossi et al., 1998). Where
etiology of PD is highly related to periodontal pathogenic bacteria such as P. gingivalis,
P. intermedia or A. actinomycetemcomitans (Castillo et al., 2011). These bacteria
induce the destruction of periodontal tissues by their numerous virulence factors such
as LPS, fimbriae etc. (Curtis et al., 2005). In addition, many physiopathological
processes are involved in periodontal destruction in terms of the inflammatory and
immune host response, especially proinflammatory cytokines or MMPs (Dahan et al.,
2001; Kiecolt-Glaser et al., 2003; Van Dyke and Kornman, 2008).
All these factors lead to strong correlation among salivary IL-1β, dental
plaque, gingival inflammation, BOP and stress during examination period. This result
is in agreement with Deinzer et al., in 1999 and Deinzer et al., in 2000.

Chapter Five
Conclusions and
Suggestions

Conclusions and Suggestions Chapter Five
74
Conclusions and Suggestions
5.1. Conclusions
1. Highly significant differences in the immunological parameter (salivary
interleukin-1β) level and clinical periodontal parameters (plaque index, gingival
index and bleeding on probing) in different periods at P-values ≤ 0.01.
2. Psychological examination stress affected on periodontal health status by more
plaque accumulation, gingival inflammation and increased amounts of interleukin-
1β in saliva. Thus, examination stress appears as a possible risk factor for gingivitis.
3. Strong positive correlations between salivary interleukin-1β level, clinical
periodontal parameters and examination stress at P-value ≤ 0.01.
4. Salivary interleukin-1β can be used as indicator for examination stress that lead to
periodontal diseases.

Conclusions and Suggestions Chapter Five
75
5.2. Suggestions for further studies
1. Further studies in larger populations are required to explore the relationship
between stress and periodontal diseases.
2. Use another stress questionnaires such as Perceived Stress Scale (PSS) with another
stress markers such as salivary and serum cortisol, C-reactive protein, tumor
necrosis factor-alpha, and matrix metalloproteinase.
3. Further studies may include stress managements for the stressful patients such as
coping styles or medications and their relation with periodontal diseases.
4. Determine the relationship between periodontal diseases and other types of
psychological stress such as occupational stress (athletes); involuntary stress
(soldiers) and voluntary stress (musicians).
5. Compare the effects of any type of stress differences with the periodontal diseases
between males and females.

References

References
76
References
A
Aboyoussef H, Carter C, Jandinski J, Panagakos F. Detection of Prostaglandin E2
and Matrix Metalloproteinase in implant crevicular fluid. Int J Oral Maxillofac
Implants. 1998; 13(5):689-696.
Adair JG. The Hawthorne effect: a reconsideration of the methodological artefact. J
Appl Psychol. 1984; 69(2):334-345.
Agarwal S, Chandra CS, Piesco NP, Langkamp HH, Bowen L, Baran C.
Regulation of periodontal ligament cell functions by interleukin-1beta. Infect Immun.
1998; 66(3):932-937.
Akcali A, Huck O, Tenenbaum H, Davideau JL, Buduneli N. Periodontal diseases
and stress: a brief review. J Oral Rehabil. 2013; 40(1):60-68.
Akhter R, Hannan M, Okhuba R, Morita M. Relationship between stress factor and
periodontal disease in a rural area population in Japan. Eur J Med Res. 2005;
10(8):352-357.
Alcami A, Koszinowski HU. Viral mechanisms of immune evasion. Trends
Microbiol. 2000; 8(9):410-418.
AL-Ghamidi H, Anil S. Serum antibody levels in smoker and non-smoker Saudi
subjects with chronic periodontitis. J Periodontol. 2007; 78(6):1043-1050.
Aliefendic A, Zimmerer R, Meyrat B, Muhney K, Rivera-Hidalgo F, Al-Hashimi
I. Serum and salivary CTX, ICTP, IL-1b in periodontal diseases. IADR. 2013.
Allgrove JE, Gomes E, Hough J, Gleeson M. Effects of exercise intensity on salivary
antimicrobial proteins and markers of stress in active men. J Sports Sci. 2008; 26(6):
653-661.

References
77
American Academy of Periodontology: Drug-associated gingival enlargement.
Informational paper. J Periodontol. 2004; 75(10):1424-1431.
Apostolakis S, Vogiatzi K, Krambovitis E, Spandidos D. IL-1 cytokines in
cardiovascular disease: diagnostic, prognostic and therapeutic implications.
Cardiovasc Hematol Agents Med Chem. 2008; 6(2):150-158.
Axtellius B, Edwardsson S, Theodorsson E, Svensater G, Attstrom R. Presence of
cortisol in gingivalcrevicular fluid. A pilot study. J Clin Periodontol. 1998; 25(11):929-
932. (www.ivsl.org).
B
Backe EM, Seidler A, Latza U, Rossnagel K, Schumann B. The role of psychosocial
stress at work for the development of cardiovascular diseases: a systematic review. Int
Arch Occup Environ Health. 2012; 85(1):67-79.
Banyer J, Hamilton N, Ramshaw I, Ramsay A. Cytokines in innate and adaptive
immunity. Rev Immunogenet. 2000; 2(3):359-473.
Barksby H, Lea S, Preshaw P, Taylor J. The expanding family of interleukin-1
cytokines and their role in destructive inflammatory disorders. Clin Exp Immunol.
2007; 149(2):217-225.
Bascones A, Gonzalez-Moles MA. Immunological mechanisms of periodontal and
peri-implant diseases. Av Period Implant. 2003; 15:121-138.
Bas S, Gauthier B, Spenato U, Stingelin S, Gabay C. CD14 is an acute-phase
protein. J Immunol. 2004; 172(7):4470-4479.
Ben-Eliyahu S, Shakhar G, Page GG, Stefanski V, Shakhar K. Suppression of NK
cell activity and of resistance to metastasis by stress: a role for adrenal catecholamines
and betaadrenoceptors. Neuroimmunomodulation. 2000; 8(3):154-164.
Berglundh T, Donati M, Zitzmann N. B cells in periodontitis: friends or enemies.
Periodontol 2000. 2007; 45(1):51-66. (www.ivsl.org).

References
78
Beynon AL, Coogan AN. Diurnal, age and immune regulation of interleukin-1 and
interleukin-1 type1 receptor in the mouse suprachiasmatic nucleus. Chronobiol Int.
2010; 27(8):1546-1563.
Bhaskar V, Yin J, Mirza A, Vanegas S, Issafras H, Michelson K, Hunter J,
Kantak S. Monoclonal antibodies targeting IL-beta reduce biomarkers of
atherosclerosis in vitro and inhibit atherosclerotic plaque formation in Apo lipoprotein
E-deficient mice. Atherosclerosis. 2011; 216(2):313-333.
Bodet C; Chandad F, Grenier D. Porphyromonas gingivalis induced inflammatory
mediator profile in an ex vivo human whole blood model. Clin Exp Immunol. 2006;
143(1):50-57.
Bosch JA, De Geus EJ, Kelder A, Veerman EC, Hoogstraten J, Nieuw Amerongen
AV. Differential effects of active versus passive coping on secretory immunity.
Psychophysiol. 2001; 38(5):836-846.
Bosch JA, Veerman EC, de Geus EJ, Proctor GB. α-Amylase as a reliable and
convenient measure of sympathetic activity: Don’t start salivating just yet.
Psychoneuroendocrinology. 2011; 36(4):449-453.
Boyapati L, Wang HL. The role of stress in periodontal disease and wound healing.
Periodontol 2000. 2007; 44(1):195-210. (www.ivsl.org).
Boyle JO, Mao L, Brennan JA. Gene mutations in saliva as molecular markers for
head and neck squamous cell carcinoma. Am J Surg. 1994; 168(5):429-432.
Brailo V, Vucicevic-Boras V, Lukac J, Biocina-Lukenda D, Zilic- Alajbeg I,
Milenovic A, Balija M. Salivary and serum interleukin 1 beta, interleukin 6 and tumor
necrosis factor alpha in patients with leukoplakia and oral cancer. Med Oral Patol Oral
Cir Bucal. 2012; 17(1):10-15.
Breivik T, Thrane PS, Murison R, Gjermo P. Emotional stress effects on immunity,
gingivitis and periodontitis. Eur J Oral Sci. 1996; 104(4):327-334.

References
79
Breivik T, Thrane PS. Psychoneuroimmune interaction in periodontal disease. In:
Psychoneuroimmunology. In: Ader R, Fetten DL, Cohen N. 3rd ed. San Diego:
Academic Press; 2001; 627-644.
Brown LJ, Johns BA, Wall TP. The economics of periodontal diseases. Periodontol
2000. 2002; 29(1):223-234.
Brydon L, Edwards S, Jia H, Mohamed-Ali V, Zachary I, Martin JF, Steptoe A.
Psychological stress activates interleukin-1beta gene expression in human
mononuclear cells. Brain Behav Immun. 2005; 19(6):540-456.
Buatongsri V, Songpaison Y, Hong prasong N, Phantumvanti P, Clark N. The
distribution of severe periodontitis in urban (Bankok) and rural (payao province) high
risk to stress group of this population. Cu Dent J. 2002; 25:1-4.
Buduneli N, zcaka O, Nalbantsoy A. Salivary and plasma levels of Toll-like receptor
2 and Toll-like receptor 4 in chronic periodontitis. J Periodontol. 2011; 82(6):878-884.
Buhlink K, Gustafsson A, Hakansson J, Klinque B. Oral health and cardiovascular
disease in Sweden. J Clin Periodontal. 2002; 29(3):254-259. (www.ivsl.org).
C
Calcagni E, Elenkov I. Stress system activity, innate and T helper cytokines and
susceptibility to immune-related diseases. Ann N Y Acad Sci. 2006; 1069:62-76 .
Carranza FA, Newman MG, Takei HH, Perry R. Carranza's Clinical
Periodontology, 10th ed. WB Saunders Company, 2006.
Castillo DM, Sanchez-Beltran MC, Castellanos JE, Sanz I, Mayorga-Fayad I,
Sanz M, Lafaurie GI. Detection of specific periodontal microorganisms from
bacteraemia samples after periodontal therapy using molecular-based diagnostics. J
Clin Periodontol. 2011; 38(5):418-427. (www.ivsl.org).

References
80
Castro GDC, Oppermann RV, Haas AN, Winter R, Alchieri JC. Association
between Psychosocial factors and Periodontitis. J Clin Periodontol. 2006; 33(2):109-
114.
Cavanaugh PF, Meredith MP, Buchanan W, Doyle MJ, Reddy MS, Jeffcoat MK.
Coordinate production of PGE2 and Il-1b in the gingival crevicular fluid of adults with
periodontitis: its relationship to alveolar bone loss and disruption by twice daily
treatment with ketorolac tromethamine oral rinse. J Periodontol Res. 1998; 33(2):75-
82. (www.ivsl.org).
Cazalis J, Tanabe S, Gagnon G, Sorsa T, Grenier D. Tetracyclines and chemically
modified tetracycline-3 (CMT-3) modulate cytokine secretion by lipopolysaccharide-
stimulated whole blood. Inflammation. 2009; 32(2)130-137.
Chandna S, Bathla M. Stress and periodontium: A review of concepts. J Oral Health
Comm Dent. 2010; 4(1):17-22.
Chard T. An introduction to radioimmunoassay and related techniques, 4th ed.
Amsterdam: Elsevier, 1990.
Chausau S, Becker A, Chausau G, Sharpiro J. Stimulated parotid salivary flow rates
in patients with Down syndrome. Spec Care Dentist. 2002; 22(1):41-44.
Chiappelli F, Iribarren F, Prolo P. Salivary biomarkers in psychobiological
medicine. Bioinformation. 2006; 8(1):331-334.
Chida Y, Hamer M. An association of adverse psychosocial factors with diabetes
mellitus: a meta-analytic review of longitudinal cohort studies. Diabetologia. 2008;
51(12):2168-2178.
Chrousos GP. The hypothalamic-pituitary-adrenal axis and immune-mediated
inflammation. N Engl J Med. 1995; 332(20):1351-1362.
Costanzo LS. Physiology, 4th ed. Saunders, Elsevier, ISBN, 2010.

References
81
Cronin AJ, Claffey N, Stassen LF. Who is at risk? Periodontal disease risk analysis
made accessible for the general dental practitioner. Br Dent J. 2008; 205(3):131-137.
Croucher R, Marcenes WS, Torres MC, Hughes F, Sheiham A. The relationship
between life-events and periodontitis. A case-control study. J Clin Periodontol. 1997;
24(1):39-43. (www.ivsl.org).
Culshaw S, Mcinnes IB, Liew FY. What can the periodontal community learn from
the pathophysiology of rheumatoid arthritis. J Clin Periodontol. 2011; 38(11):106-113.
Curtis MA, Slaney JM, Aduse-Opoku J. Critical pathways in microbial virulence. J
Clin Periodontol. 2005; 32(6):28-38.
D
Dahan M, Nawrocki B, Elkaam R et al. Expression of matrix metalloproteinases in
healthy and diseased human gingiva. J Clin Periodontol. 2001; 28(2):128-136.
Davis EP, Granger DA. Developmental differences in infant salivary alpha-amylase
and cortisol responses to stress. Psychoneuroendocrinology. 2009; 34(6):795-804.
Dayan S, Stashenko P, Niederman R, Kupander T. Oral epithelial overexpression
of IL-1 alpha causes periodontal disease. J Dent Res. 2004; 83(10):786-90.
(www.ivsl.org).
De Almeida Pdel V, Gregio AM, Machado MA. Saliva composition and functions:
a comprehensive review. J Contemp Dent Pract. 2008; 9(3):72-80.
Dean VS, Simon CL. Periodontal disease is associated with lower antioxidant
capacity in whole saliva and evidence of increased protein oxidation. Clin Sci. 2003;
105(2):167-172.
Debnath M, Doyle KM, Langan C, McDonald C, Leonard B, Cannon DM. Recent
advances in psychoneuroimmunology: Inflammation in psychiatric disorders. Translat
Neurosci. 2011; 2(2):121-37.

References
82
Deinzer R, Ruttermen S, Mobes O, Herforth A. Increase in gingival inflammation
under academic stress. J Clin Periodontol. 1998; 25(5):431-433.
Deinzer R, Forster P, Fuck L, Herforth A, Stiller-Winkler R, Idel H. Increase of
crevicular interleukin-1 beta under academic stress at experimental gingivitis sites and
at sites of perfect oral hygiene. J Clin Periodontol. 1999; 26(1):1-8.
Deinzer R, Kottman W, Foster P, Herforth A, Stiller-Winkler R, Idel H. After-
effects of stress on crevicular interleukin-1ß. J Clin Periodontol. 2000; 27(1):74-77.
Deinzer R, Hilpert D, Bach K, Schawacht M, Herforth A. Effects of academic stress
on oral hygiene–a potential link between stress and plaque-associated disease. J Clin
Periodontol. 2001; 28(5):459-464. (www.ivsl.org).
Deinzer R, Granrath N, Stuhl H, Twork L, Idel H, Waschul B, Herforth A. Acute
stress effects on local IL-1 responses to pathogens in a human in vivo model. Brain
Behav Immun. 2004; 18(5):458-467.
Deinzer R, Granrath N, Spahl M, Linz S, Waschul B, Herforth A. Stress, oral
health behavior and clinical outcome. Br J Health Psychol. 2005; 10(2):269-283.
Delima AJ, Van Dyke TE. Origin and function of the cellular components in gingival
crevice fluid. Periodontol 2000. 2003; 31(1):55-76. (www.ivsl.org).
Dhabbar FS. Stress-induced augmentation of immune function-the role of stress
hormones, leukocyte trafficking, and cytokines. Brain Behav Immun. 2002; 16(6):785-
798.
Dinarello CA. Interleukin-1. Cytokine Growth Factor Rev. 1997; 8(4):253-265.
Dinarello CA. Interleukin-1, interleukin - 1 receptors and interleukin-1 receptor
antagonist. Int Rev Immunol. 1998; 16(5-6):457-499.
Dinarello CA. The Role of the interleukin-1-receptor antagonist in blocking
inflammation mediated by interleukin-1. N Engl J Med. 2000; 343(10):732-734.

References
83
Dinarello CA. Immunological and inflammatory functions of the interleukin-1
family. Ann Rev Immunol. 2009; 27:519-550.
Dixon D, Bainbridge B, Darveau R. Modulation of the innate immune response
within the periodontium. Periodontol 2000. 2004; 35(1):53-74.
Doyle CJ, Bartold PM. How dose stress influence periodontitis. J Int Acad
Periodontol. 2012; 14(2):42-49.
Dugue B, Leppanen EA, Teppo AM, Fyhrquist F, Grasbeck R. Effects of
psychological stress on plasma interleukins-1 beta and 6, C-reactive protein, tumour
necrosis factor alpha, anti-diuretic hormone and serum cortisol. Scand J Clin Lab
Invest. 1993; 53(6):555-561.
E
Ebersole J. Humeral immune responses in gingival crevicular fluid: local and systemic
implications. Periodontol 2000. 2003; 31:135-166.
Ebersole JL, Cappelli D. Acute phase reactants in infectious and inflammatory
diseases. Periodontol 2000. 2000; 23(1):19-49.
Edgar WM. Saliva: Its secretion, composition and functions. Br Dent J. 1992; 172(8):
305-312.
Elkhouli A. The efficacy of host response modulation therapy (omega-3 plus low-dose
aspirin) as an adjunctive treatment of chronic periodontitis (clinical and biochemical
study). J Periodontol Res. 2011; 46(2):261-268. (www.ivsl.org).
El-Qadri SS, Taani DQ. Assessment of periodontal knowledge and periodontal status
of an adult population in Jordan. Int J Dent Hygiene. 2004; 2(3):132-136.
(www.ivsl.org).
Elter JR, Beck JD, Slade GD, Offenbacher S. Etiologic models for incident
periodontal attachment loss in older adults. J Clin Periodontol. 1999; 26(2):113-123.

References
84
Embery G, Waddington R. Gingival crevicular fluid: Biomarkers of periodontal
tissue activity. Adv Dent Res. 1994; 8(2):329-336.
Engebretson S, Grbic J, Singer R, Lamster I. GCF IL-1beta profiles in periodontal
disease. J Clin Periodontol. 2002; 29(1):48-53.
F
Fabian TK, Fejerdy P, Nguyen MT, Soti C, Csermely P. Potential immunological
functions of the salivary chaperone, Hsp70 in the mucosal and periodontal defense
mechanisms. Arch Immunol Ther Exp. 2007; 55(2):1-8.
Figueredo CM, Ribeiro MS, Fischer RG, Gustafsson A. Increased interleukin-1beta
concentration in gingival crevicular fluid as a characteristic of periodontitis. J
Periodontol. 1999; 70(12):1457-1463.
Fisher AJ, Granger DA, Newman MG. Sympathetic arousal moderates self-reported
physiological arousal symptoms at baseline and physiological flexibility in response
to a stressor in generalized anxiety disorder. Biol Psych. 2010; 83(3):191-200.
Fitzsimmons TR, Sanders AE, Bartold PM, Slade GD. Local and systemic
biomarkers in gingival crevicular fluid increase odds of periodontitis. J Clin
Periodontol. 2010; 37(1):30-36.
Forde MD, Koka S, Eckert SE, Carr AB, Wong DT. Systemic assessments utilizing
saliva: Part 1. General considerations and current assessments. Int J Prosthodont. 2006;
19(1):43-52.
G
Gaffen S, Hajishengallis G. A new inflammatory cytokine on the block: rethinking
periodontal disease and the Thl/Th2 paradigm in the context of Thl7 cells and IL-17. J
Dent Res. 2008; 87(9):817-818. (www.ivsl.org).

References
85
Gamboa ABO, Hughes FJ, Marcenes W. The relationship between emotional
intelligence and initial response to a standardized periodontal treatment: a pilot study.
J Clin Periodontol. 2005; 32(7):702-707.
Gemmell E, Yamazaki K, Seymour G. The role of T cells in periodontal disease:
homeostasis and autoimmunity. Periodontol 2000. 2007; 43(1):14-40.
Genco RJ, Alex WHO, Jeffrey K, Grossi SG, Dunford RG, Tedesco LA. Models
to evaluate the role of stress in periodontal disease. Ann Periodontol. 1998; 3(1):288-
302.
Genco RJ, Alex WHO, Grossi SG, Dunford RG, Jeffrey K, Tedesco LA.
Relationship of stress, distress and inadequate coping behaviors to periodontal disease.
J Periodontol. 1999; 70(7):711-723.
Ghezzi E, Lange L, Ship J. Determination of variation of stimulated salivary flow
rates. J Dent Res. 2000; 79(11):1874-1878.
Giannopoulou C, Kamma JJ, Mombelli A. Effect of inflammation, smoking and
stress on gingival crevicular fluid cytokine level. J Clin Periodontol. 2003; 30(2):145-
153. (www.ivsl.org).
Giddon DB, Goldhaber P, Dunning JM. Prevalence of reported cases of acute
necrotizing ulcerative gingivitis in a university population. J Periodontol. 1963; 34(4):
66-70.
Giddon DB, Zackin SJ, Goldhaber P. Acute necrotizing ulcerative gingivitis in
college students. J Am Dent Assoc. 1964; 68:381-386.
Glaser R, Kiecolt-Glaser JK. Stress-induced immune dysfunction: Implications for
health. Nature Rev Immunol. 2005; 5(3):243-251.
Gorska R, Gregorek H, Kowalski J, Laskus-Perendyk A, Syczewska M,
Madalinski K. Relationship between clinical parameters and cytokine profiles in

References
86
inflamed gingival tissue and serum samples from patients with chronic periodontitis. J
Clin Periodontol. 2003; 30(12):1046-1052.
Goshen I, Yirmiya R. Interleukin-1 (IL-1): A central regulator of stress responses.
Front Neuroendocrinol. 2009; 30(1):30-45.
Gourin C. Production of tumor necrosis factor and interleukin-1b by human cerebral
microvascular endothelium after percussive trauma. J Trauma. 1997; 42(6):1101-1107.
Goyal S, Jajoo S, Nagappa G, Rao G. Estimation of relationship between
psychosocial stress and periodontal status using serum cortisol level: a clinico-
biochemical study. Indian J Dent Res. 2011; 22(1):6-9.
Granger DA, Kivlighan KT, El-Sheikh M, Gordis EB, Stroud LR. Salivary α-
amylase in biobehavioral research: Recent developments and applications. Ann N Y
Acad Sci. 2007; 1098(1):122-144.
Graves D, Cochran D. The contribution of interleukin 1 and tumor necrosis factor to
periodontal tissue destruction. J Periodontol. 2003; 74(3):391-401.
Greabu M, Maurizio Battino, Maria Mohora, Alexandra Totan, Andreea
Didilescu, Tudor Spino, Cosmin Totan, Daniela Miricescu, Radu Radulescu.
Saliva-diagnostic window to the body, both in health and disease. J of Medicine and
Life. 2009; 2(2):124-132.
Greenwold D, Slack R, Pesterer J, Barer M. Medical Microbiology. A guide to
microbial infection, pathogenesis, immunity, laboratory diagnosis and control, 17th ed.
Edinburgh, UK: Elsevier Limited; 2007; 107-133.
Groer M, Murphy R, Bunnell W, Salomon K, Van Eepoel J, Rankin B et al.
Salivary measures of stress and immunity in police officers engaged in simulated
critical incident scenarios. J Occup Environ Med. 2010; 52(6):595-602.
Grossi SG, Dunford RG, Tedesco LA. Models to evaluate the role of stress in
periodontal disease. Ann Periodontol. 1998; 3(1):288-302.

References
87
Guggenheimer J. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc.
2003; 134(1):61-69.
Guyton AC, Hall JE. Textbook of medical physiology, 10th ed. Philadelphia, PA,
London: WB Saunders; 2000; 739-742.
Guzeldemir E, Cetinkaya B, Bulut S. Cytokine profiles in patients with rheumatoid
arthritis and chronic periodontitis. International Association for dental research.
2011.
H
Hamaguchi T, Fukudo S, Kanazawa M, Tomiie T, Shimizu K, Oyama M. Changes
in salivary physiological stress markers induced by muscle stretching in patients with
irritable bowel syndrome. Biopsychosoc Med. 2008; 2(20):1751-0759.
Hamissi J, Kakaei S, Hamissi H. Psychological stress and periodontal disease. Pak
Oral Dental J. 2010; 30(2):464-467.
Han JY, Reynolds MA. Effect of anti-rheumatic agents on periodontal parameters
and biomarkers of inflammation: A systematic review and meta-amalysis. J
Periodontal Implant Sci. 2012; 42(1):3-12.
Hansel A, Hong S, Camara RJ, Von Kanel R. Inflammation as a
psychophysiological biomarker in chronic psychosocial stress. Neurosci Biobehav
Rev. 2010; 35(1):115-121.
Harris N, Godoy F. Primary preventive dentistry. 6th ed. Upper Saddle River, New
Jersey; 2004.
Hilgert JB, Hugo FN, Bandeira DR, Bozzetti MC. Stress, cortisol, and periodontitis
in a population aged 50 years and over. J Dent Res. 2006; 85(4):324-328.
(www.ivsl.org).
Hirschfeld L, Wasserman B. A long-term survey of tooth loss in 600 treated
periodontal patients. J Periodontol. 1978; 49(5):225-237.

References
88
Hornef M, Wick M, Rhen M, Normark S. Bacterial strategies for overcoming host
innate and adaptive immune responses. Nat Immunol. 2002; 3(11):1033-1040.
Houri-Haddad Y, Itzchaki O, Ben-Nathan D, Shapira L. The effect of chronic
emotional stress on the humeral immune response to porphyromonas gingivalis in
mice. J Periodontol Res. 2003; 38(2):204-209. (www.ivsl.org).
Hujoel P, White B, Garcia R, Listgarten M. The dentogingival epithelial surface
area revisited. J Periodontol Res. 2001; 36(1):48-55.
Hujoel P, Drangsholt M, Spiekerman C. Periodontal disease and coronary heart
disease risk. JAMA. 2002; 284(11):1406-1410.
I
Ilardo C, Toniolo AM, Aimone-Gastin I, Abdelmouttaleb I, Gueant JL, Desor D.
Effects of psycho-physical stress (competitive rafting) on saliva interleukin-1 beta.
Stress Health. 2001; 17(1):9-15.
Inoue H, Ono K, Masuda W, Morimoto Y, Tanaka T, Yokota M, Inenaya K.
Gender difference in unstimulated whole salivary flow rate and salivary gland size.
Arch Oral Biol. 2009; 51(12):1055-1060.
Ishisaka A, Ansai T, Soh I, Inenaga K, Awano S, Yoshida A, Hamasaki T, Sonoki
K, Takata Y, Nishihara T, Takehara T. Association of cortisol and
dehydroepiandrosterone sulphate levels in serum with periodontal status in older
Japanese adults. J Clin Periodontol. 2008; 35(10):853-861.
J
James MJ, Proudman SM, Cleland LG. Dietary n-3 fats as adjunctive therapy in a
prototypic inflammatory disease: issues and obstacles for use in rheumatoid arthritis.
Prostaglandins Leukot Essent Fatty Acids. 2003; 68(6):399-405.

References
89
Janeway CA, Travers P, Walport MJ, Shlomchik M. Immunobiology. The immune
system in health and disease, 6th ed. Taylor & Francis Group, Garland Science; 2005;
1-95.
Jepsen R. Progressive periimplantitis. Incidence and prediction of periimplant
attachment loss. Clin Oral Impl Res. 1996; 7(2):133-142.
Jindal V. An overview for physicians oral-systemic relation. 2009; 1(1):31-33
Johnson LR. Essential Medical Physiology, 3rd ed. San Diego, CA: Elsevier Academic
Press; 2003; 499-502.
Johannsen A, Asberg M, Soder PO, Soder B. Anxiety, gingival inflammation and
periodontal disease in non-smokers and smokers. J Clin Periodontol. 2005; 32(5):488-
491.
Johannsen A, Rylander G, Soder B, Asberg M. Dental plaque, gingival
inflammation, and elevated levels of interleukin-6 and cortisol in gingival crevicular
fluid from women with stress-related depression and exhaustion. J Periodontol. 2006;
77(8):1403-1409.
Johannsen A, Rydmark I, Soder B, Asberg M. Gingival inflammation, increased
periodontal pocket depth and elevated interleukin-6 in gingival crevicular fluid of
depressed women on long-term sick leave. J Periodontal Res. 2007; 42(6):546-552.
Johannsen A, Bjurshammar N, Gustafsson A. The influence of academic stress on
gingival inflammation. Int J Dent Hy. 2010; 8(1):22-27. (www.ivsl.org).
K
Kabashima H, Nagata K, Maeda K, Lijima T. Involvement of substance P, mast
cells, TNF-alpha and ICAM-1 in the infiltration of inflammatory cells in human
periapical granulomas. J Oral Pathol Med. 2002; 31(3):175-180.
Kakizaki Y, Watanobe H, Kohsaka A, Suda T. Temporal profiles of interleukin-
1beta, interleukin-6, and tumor necrosis factor-alpha in the plasma and hypothalamic

References
90
paraventricular nucleus after intravenous or intraperitoneal administration of
lipopolysaccharide in the rat: Estimation by push-pull perfusion. Endocr J. 1999;
46(4):487-96.
Kamma JJ, Baehni PC. Five-year maintenance follow-up of early- onset periodontitis
patients. J Clin Periodontol. 2003; 30(6):562-572.
Kamma JJ, Giannopoulou C, Vasdekis VG, Mombelli A. Cytokine profile in
gingival crevicular fluid of aggressive periodontitis: influence of smoking and stress.
J Clin Periodontol. 2004; 31(10):894-902.
Keshava PK, Sangeeta NU. Stressing the stress in periodontal disease. J Pharm
Biomed Sci. 2013; 26(26): 345-348.
Keles G, Acikgoz G, Ayas B, Sakallioglu E, Firatli E. Determination of systemically
and locally induced periodontal defects in rats. Indian J Med Res. 2005; 121(3):176-
184.
Khaustova S, Shkurnikov M, Tonevitsky E, Artyushenko V, Tonevitsky A.
Noninvasive biochemical monitoring of physiological stress by Fourier transform
infrared saliva spectroscopy. Analyst. 2010; 135(12):3183-3192.
Kiecolt-Glaser JK, Preacher KJ, MacCallum RC, Atkinson C, Malarkey WB,
Glaser R. Chronic stress and age-related increases in the proinflammatory cytokine
IL-6. Proc Natl Acad Sci USA. 2003; 100(15):9090-9095.
Kinane D, Demuth D, Gorr S, Hajishengallis G, Martin M. Human variability in
innate immunity. Periodontol 2000. 2007; 45(1):14-34. (www.ivsl.org).
Kirkwood K, Nisengard R, Haake S, Miyasaki K. Immunity and inflammation:
basic concepts. In: Newman MG, Takej H, Klokkewold P, Carranza F. Carranza's
Clinical Periodontology, 10th ed. St. Louis, Missouri: Saunders, Elsevier; 2006; 209-
227.

References
91
Kivlighan KT, Granger DA, Schwartz EB, Nelson V, Curran M, Shirtcliff EA.
Quantifying blood leakage into the oral mucosa and its effects on the measurement of
cortisol, dehydroepiandrosterone, and testosterone in saliva. Horm Behav. 2004;
46(1):39-46.
Klages U, Weber AG, Wehrbein H. Approximal plaque and gingival sulcus bleeding
in routine dental care patients. Relations to life stress, somatization and depression. J
Clin Periodontol. 2005; 32(6):575-582.
Konig J, Plagmann H, Langenfeld N, Kocher T. Retrospective comparison of
clinical variables between compliant and non-compliant patients. J Clin Periodontol.
2001; 28(3):227-232.
Kornman K. Mapping the pathogenesis of periodontitis: a new look. J Periodontol.
2008; 79(8):1560-1568.
Korn T, Oukka M, Kuchroo V, Bettelli E. Thl7 cells: effector T cells with
inflammatory properties. Semin Immunol. 2007; 19(6):362-371.
Kunz-Ebrecht SR, Mohamed-Ali V, Feldman PJ, Kirschbaum C, Steptoe A.
Cortisol responses to mild psychological stress are inversely associated with
proinflammatory cytokines. Brain Behav Immun. 2003; 17(5):373-383.
L
Lacey K, Zaharia MD, Griffiths J, Ravindran AV, Merali Z, Anisman H. A
prospective study of neuroendocrine and immune alterations associated with the stress
of an oral academic examination among graduate students.
Psychoneuroendocrinology. 2000; 25(4):339-356.
Lacopino A, Doxey D, Cutler C, Nares S, Stoever K, Fojt J, Gonzales A, Dill R.
Phenytoin and cyclosporine A specifically regulate macrophage phenotype and
expression of platelet derived growth factor and interleukin-1 in vitro and in vivo:

References
92
possible molecular mechanism of drug-induced gingival hyperplasia. J Periodontol.
1997; 68(l):73-83.
Lathrop, Thomas. Stedman's medical dictionary, 28th ed. Philadelphia: Hubsta Ltd;
2008.
Lawrence HP. Salivary markers of systemic disease, Non-invasive diagnosis of
disease and monitoring of general health. J Cand Dent Assoc. 2002; 68(3):170-174.
Lee A, Ghaname CB, Braun TM, Sugai JV, Teles RP, Loesche WJ, Kornman KS,
Giannobile WV, Kinney JS. Bacterial and salivary biomarkers predict the gingival
inflammatory profile. J Periodontol. 2012; 83(1):79-89.
Leininger M, Tenenbaum H, Davideau JL. Modified periodontal risk assessment
score: long-term predictive value of treatment outcomes. A retrospective study. J Clin
Periodontol. 2010; 37(5):427-435. (www.ivsl.org).
Leone C, Oppenheim F. Physical and chemical aspects of saliva as indicators of risk
for dental caries in humans. J Dent Educ. 2001; 65(10):1054-1062.
LeResche L, Dworkin SF. The role of stress in inflammatory diseases, including
periodontal disease: review of concepts and current findings. Periodontol 2000. 2002;
30(1):91-103.
LeVan T, Bloom J, Bailey T, Karp C, Halonen M, Martinez F, Vercelli D. A
common single nucleotide polymorphism in the CD14 promoter decreases the affinity
of Sp protein binding and enhances transcriptional activity. J Immunol. 2001; 167(10):
5838-5844.
Linden GJ, Mullally BH, Freeman R. Stress and the progression of periodontal
disease. J Clin Periodontol. 1996; 23(7):675-680.
Lindhe J, Lang NP, Karring T. Clinical periodontology and implant dentistry, 5th ed.
Blackwell Munksgaard, Blackwell Publishing company; 2008.

References
93
Liu C, Hou L, Wong M, Rossomando E. Relationships between clinical parameters,
Interleukin 1b and histopathology findings of gingival tissue in periodontitis patients.
Cytokine. 1996; 8(2):161-167.
Llamas Moya S, Boyle LA, Lynch PB, Arkins S. Pro-inflammatory cytokine and
acute phase protein responses to low-dose lipopolysaccharide (LPS) challenge in pigs.
Animal Sci. 2006. 82(4):527-534.
Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta
Odontol Scand. 1963; 21:533-551.
Loe H. The gingival index, the plaque index and the retention index system. J
periodontol. 1967; 38(6):610-616.
Lovibond SH, Lovibond PF. Manual for the depression anxiety stress scales, 2nd ed.
Psychology Foundation of Australia; 1995.
Lundy FT, Linden GJ. Neuropeptides and neurogenic mechanisms in oral and
periodontal inflammation. Crit Rev Oral Biol Med. 2004; 15(2):82-98.
M
Maes M, Song C, Lin A, De Jongh R, Van Gastel A, Kenis G, Bosmans E, De
Meester I, Benoy I, Neels H, Demedts P, Janca A, Scharpe S, Smith RS. The effects
of psychological stress on humans: increased production of pro-inflammatory
cytokines and a Th1-like response in stress-induced anxiety. Cytokine. 1998;
10(4):313-318.
Malathi K, Sabale D. Stress and periodontitis: A review. DMS. 2013; 9(4):54-57.
Marieb EN, Hoehn K, Hutchinson M. Human anatomy and physiology, 9th ed. San
Francisco: Pearson Education/Benjamin Cummings; 2013.
Marketon WJI, Glaser R. Stress hormones and immune function. Cell Immunol.
2008; 252(1-2):16-26.

References
94
Marques-Deak AH, Neto FL, Dominguez WV et al. Cytokine profiles in women
with different subtypes of major depressive disorder. J Psychiatr Res. 2007; 41(1-
2):152-159.
Martinez A, Corcuera, M, Noronha S, Mota P, Ilundain C and Trapero J. Host
defense mechanisms against bacterial aggression in periodontal disease: Basic
mechanisms. Med Oral Patol Oral Cir Bucal. 2009; 14(12):680-685.
Maruyama Y, Stenvinkel P, Lindholm B. Role of interleukin-l beta in the
development of malnutrition in chronic renal failure patients. Blood Purif. 2005; 23
(4):275-281.
Mawhorter S, Lauer M. Is atherosclerosis an infectious disease. Cleveland Clinic
Journal of Medicine. 2001; 68(5):449-458.
Mead H, Witkowski K, Gault B, Hartmann H. The influence of income, education,
and work status on women’s well being. Women’s Health Issue. 2001; 11(3):160-172
Mengel R, Bacher M, Flores-De-Jacoby L. Interactions between stress, interleukin-
1beta, interleukin-6 and cortisol in periodontally diseased patients. J Clin Periodontol.
2002; 29(11):1012-1022. (www.ivsl.org).
Michael D; Liam D; Peter D; Malcolm M. The role of awakening cortisol and
psychological distress in diurnal variations in affect: a day reconstruction study
University College Dublin. Geary Institute. 2011; 11(3):524-532.
Miller CS, King CP, Langub MC, Kryscio RJ, Thomas MV. Salivary biomarkers
of existing periodontal disease: A cross-sectional study. J Am Dent Assoc. 2006;
137(3):322-329.
Miller CS, Foley JD, Bailey AL, Campell CL, Humphries RL, Christodoulides N,
Floriano PN, Simmons G, Bhagwandin B, Jacobson JW, Redding SW, Ebersole
JL, McDevitt JT. Current developments in salivary diagnostics. Biomark. 2010;
4(1):171-189.

References
95
Mogensen T, Malmgaard L, Melchjorsen J, Casola A, Paludan S. Suppression of
Proinflammatory cytokine expression by herpes simplex type 1. J Virol. 2004; 78(11):
5883-5890.
Monteiro da Silva AM, Oakley DA, Newman HN, Nohl FS, Lloyd HM.
Psychosocial factors and adult onset rapidly progressive periodontitis. J Clin
Periodontol. 1996; 23(8):789-794.
Moutsopoulos N, Madianos P. Low-grade inflammation in chronic infectious
diseases: paradigm of periodontal infections. Ann N Y Acad Sci. 2006; 1088(1):251-
264.
Murayama Y, Kurihara H, Nagai A, Dompkowski D, Van Dyke TE. Acute
necrotizing ulcerative gingivitis: Risk factors involving host defense mechanisms.
Periodontol 2000. 1994; 6(1):116-124.
N
Nanci A. Ten cate's oral histology: Development, structure, and function, 6th ed. USA,
Mosby; 2003; 229-231.
Nater UM, Roulade N. Salivary alpha-amylase as a non-invasive biomarker for the
sympathetic nervous system: Current state of research. Psychoneuroendocrinology.
2009; 34(4):486-496.
Nagler RM, Hershkovich O, Lischinsky S, Diamond E, Reznick AZ. Saliva
analysis in clinical setting: revisiting an underused diagnostic tool. J Investig Med.
2002; 50(2):214-225.
Nagler R. Saliva analysis for monitoring dialysis and renal function. Clinical
Chemistry. 2008; 54(9)1415-1417.
Nguyen L, Dewhirst FE, Hauschka PV, Stashenko P. Interleukin-1b stimulates bone
resorption and inhibits bone formation in vivo. Lymphokine Cytokine Res. 1991; 10(1-
2):15-21.

References
96
Nguyen KT, Deak T, Will MJ, Hansen MK, Hunsaker BN, Fleshner M, Watkins
LR, Maier SF. Timecourse and corticosterone sensitivity of the brain, pituitary, and
serum interleukin-1beta protein response to acute stress. Brain Res 2000; 859(2):193-
201.
Nieuw AAV, Bolscher JGM, Veerman EC. Salivary proteins: Protective and
diagnostic value in cariology. Caries Res. 2004; 38(3):247-253.
Nieuw AAV, Ligtenberg AJ, Veerman, EC. Implications for diagnostics in the
biochemistry and physiology of saliva. Ann N Y Acad Sci. 2007; 1098:1-6.
Nikolopoulos G, Dimou N, Hamodrakas S, Bagos P. Cytokine gene polymorphisms
in periodontal disease: a met analysis of 53 studies including 4178 cases and 4590
controls. J Clin Periodontol. 2008; 35(9):754-767. (www.ivsl.org).
Nishida N, Tanaka M, Sekine S, Takeshita T, Nakayama K, Morimoto K,
Shizukuishi S. Association of ALDH2 genotypes with periodontitis progression. J
Dent Res. 2010; 89(2):138-142.
O
Okada H, Murakami S. Cytokine expression in periodontal health and disease. Crit
Rev Oral Biol Med. 1998; 9(3):248-266.
Omigbodun OO, Odukogbe AT, Omigbodun AO, Yusuf OB, Bella TT, Olayemi
O. Stressors and psychological symptoms in students of medicine and allied health
professions in Nigeria. Soc Psychiatry Psychiatr Epidemiol. 2006; 41(5):415-421.
Orozco A, Gemmell E, Bickel M, Seymour G. Interleukin-l beta, interleukin-12 and
interleukin-18 levels in gingival fluid and serum of patients with gingivitis and
periodontitis. Molecular Oral Microbiology. 2006; 21(4):256-260.
P
Padgett DA, Glaser R. How stress influences the immune response. Trends Immunol.
2003; 24(8):444-448.

References
97
Paik IH, Toh KY, Lee C, Kim JJ, Lee SJ. Psychological stress may induce increased
humoral and decreased cellular immunity. Behav Med. 2000; 26(3):139-341.
Page R, Offenbacher S, Schroeder H, Seymour G, Kornman K. Advances in the
pathogenesis of periodontitis: summary of developments, clinical implications and
future directions. Periodontol 2000. 1997; 14(1):216-248. (www.ivsl.org).
Pani SC, Al Askar AM, Al Mohrij SI, Al Ohali TA. Evaluation of stress in final-
year Saudi dental students using salivary cortisol as a biomarker. J Dent Educ. 2011;
75(3):377-384.
Papacosta E, Nassis GP. Saliva as a tool for monitoring steroid, peptide and immune
markers in sport and exercise science. J Sci Med Sport. 2011; 14(5):424-434.
Perrier S, Kherratia B, Deschaumes C, Ughetto S, Kemeny JL, Baudet-Pommel
M, Sauvezie B. IL-1ra and IL-1 production in human oral mucosal epithelial cells in
culture: Differential modulation by TGF-β1 and IL-4. Clin Exp Immunol. 2002;
127(1):53-59.
Peruzzo DC, Benatti BB, Ambrosano GM et al. A systematic review of stress and
psychological factors as possible risk factors for periodontal disease. J Periodontol.
2007; 78(8):1491-1504.
Peter S. Essential of preventive community dentistry, 2nd ed. New Delhi, Arya (Medi)
Publishing House; 2004; 250-255.
Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005;
366(9499):1809-1820.
Pistorius A, Krahwinkel T, Willerhausen B, Bockstegen C. Relationship between
stress factors and periodontal disease. Eur J Med Res. 2002; 7(9):393-398.
Potter R. Genetic studies of juvenile periodontitis. J Den Res. 1990; 69(1):94-95.

References
98
Pradeep AR, Raj S, Aruna G, Chowdhry S. Gingival crevicular fluid and plasma
levels of neuropeptide Substance-P in periodontal health, disease and after nonsurgical
therapy. J Periodontol Res. 2009; 44(2):232-237. (www.ivsl.org).
Premkumar M, Sable T Dhanwal D, Dewan R. Circadian levels of serum melatonin
and cortisol in relation to changes in mood, sleep, and neurocognitive performance,
spanning a year of residence in Antarctica. Neuroscience Journal. 2013;1-10.
Pussinen P, Mantyla P, Sorsa T. Serum microbial- and host-derived markers of
periodontal diseases: a review. Curr Med Chem. 2007; 14(22):2402-2412.
Q
Quan N, Avitsur R, Stark JL, He L, Shah M, Caligiuri M, Padgett DA, Marucha
PT, Sheridan JF. Social stress increases the susceptibility to endotoxic shock. J
Neuroimmunol. 2001; 115(1-2):36-45.
Queiroz A, Mario T, O'Connell P, Nobrega P, Costa P. Inflammation markers in
healthy and periodontitis patients. A data screening. Br Dent J. 2008; 19(l):333-338.
R
Ranney RR. Immunologic mechanisms of pathogenesis in periodontal disease: An
assessment. J Periodontal Res. 1991; 26(3):243-254. (www.ivsl.org).
Rasmussen L, Hanstrom L, Lerner UH. Characterization of bone resorbing activity
in gingival crevicular fluid from patients with periodontitis. J Clin Periodontol. 2000;
27(1):41-52.
Rawlinson A, Dalati M, Rahman S, Walsh T, Fairlough A. Interleukin-1 and IL-1
receptor antagonist in gingival crevicular fluid. J Clin Periodontol. 2000; 27(10):738-
743.
Reddy S, Kaul S, Prasad MGS, Agnihotri J, Amudha D, Vinayak. Interlink
between stress and periodontal disease. Health Renaissance. 2012; 10(2):126-131.

References
99
Refulio Z, Rocafuerte M, Rosa M, Mendoza G, Chambrone L. Association among
stress, salivary cortisol levels, and chronic periodontitis. J Periodontal Implant Sci.
2013; 43(2):96-100.
Reinhardt EL, Fernandes PA, Markus RP, Fischer FM. Daily rhythm of salivary
IL-1β, cortisol and melatonin in day and night workers. Work. 2012; 41(1):5788-5790.
Reners M, Breex M. Stress and periodontal disease. Int J Dent Hyg. 2007; 5(4):199-
204. (www.ivsl.org).
Rivera C, Monsalve F, Suazo I, Becerra J. Stress increases periodontal
inflammation. Exp Ther Med. 2012; 4(5):883-888.
Roberts A, Matthews JB, Socransky SS, Freestone PP, Williams PH, Chapple IL.
Stress and periodontal diseases: effects of catecholamine on the growth of periodontal
bacteria in vitro. Molecular Oral Microbiology. 2002; 17(5):296-303.
Roberts A, Matthews JB, Socransky SS, Freestone PP, Williams PH, Chapple IL.
Stress and the periodontal diseases: growth responses of periodontal bacteria to
Escherichia coli stress-associated autoinducer and exogenous Fe. Molecular Oral
Microbiology. 2005; 20(3):147-153. (www.ivsl.org).
Rosania AE, Low KG, McCormick CM, Rosania DA. Stress, depression, cortisol
and periodontal disease. J Periodontol. 2009; 80(2):260-266.
Rosenkranz MA. Substance P at the nexus of mind and body in chronic inflammation
and affective disorders. Psychol Bull. 2007; 133(6):1007-1037.
Rothermundt M, Arolt V, Peters M, Gutbrodt H, Fenker J, Kersting A, Kirchner
H. Inflammatory markers in major depression and melancholia. J Affect Disord. 2001;
63(1-3):93-102.
Rudolph KD, Troop-Gordon W, Granger DA. Individual differences in biological
stress responses moderate the contribution of early peer victimization to subsequent
depressive symptoms. Psychopharmacology. 2011; 214(1):209-219.

References
100
S
Saini R, Marawar PP, Shete S. Periodontitis a true infection. J Global Infect Dis.
2009; 1(2):149-150.
Saini R, Saini S, Saini SR. Periodontitis and psychological stress: A dental view. Ind
Psychiatry J. 2010; 19(1):66-67.
Sanders VM, Straub RH. Norepinephrine, the beta-adrenergic receptor, and
ımmunity: review. Brain Behav Immun. 2002; 16(4):290-332.
Sateesh CP, Santosh KR, Pushpalatha G. Relationship between stress and
periodontal disease. J Dent Sci Res. 2010; 1(1):54-61.
Schroder N, Meister D, Wolff V, Christan C, Kaner D, Haban V, Purucker P,
Hermann C, Moter A, Gobel U, Schumann R. Chronic periodontal disease is
associated with single nucleotide polymorphisms of the human TLR-4 gene. Genes
Immun. 2005; 6(5):448-451.
Schwartz E, Granger DA. Transferrin enzyme immunoassay for quantitative
monitoring of blood contamination in saliva. Clin Chem. 2004; 50(3):654-656.
Scully CBE. Salivary glands and saliva, drug effects on salivary glands: dry mouth.
Oral Dis. 2003; 9(4):165-176.
Seil M, El Ouaaliti M, Abdou Foumekoye S, Pochet S, Dehaye JP. Distinct
regulation by lipopolysaccharides of the expression of interleukin-1 by murine
macrophages and salivary glands. Innate Immun. 2012; 18(1):14-24.
Shimazaki Y, Saito T, Kiyohara Y, Kato I, Kubo M, lida M. Relationship between
drinking and periodontitis: the Hisayama Study. J Periodontol. 2005; 76(9):1534-1541.
Ship J, Fox P, Baum B: How much saliva is enough. J Am Dent Assoc. 1991; 122(3):
63-69.

References
101
Shirodaria S, Smith J, McKay I, Kennett C, Hughes F. Polymorphisms in the IL-
1A gene are correlated with levels of interleukin - alpha protein in gingival crevicular
fluid of teeth with severe periodontal disease. J Dent Res. 2000; 79(11):1864-1869.
Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral
hygiene and periodontal condition. Acta Odontol Scand. 1964; 22:121-135.
Singh R, Goyal M, Tiwari S, Ghildiyal A, Nattu S, Das S. Effect of examination
stress on mood, performance and cortisol levels in medical students. Indian J Physiol
Pharmacol. 2012; 56(1):48-55.
Slots J, Contreras A. Herpes viruses: a unifying causative factor in periodontitis.
Molecular Oral Microbiology. 2000; 15(5):277-280. (www.ivsl.org).
Slots J. Herpes viruses in periodontal diseases. Periodontol 2000. 2005; 38(1):33-62.
Smith CK, Peterson DF, Degenhardt BF, Johnson JC. Depression, anxiety, and
perceived hassles among entering medical students. Psychol Health Med. 2007;
12(1):31-39.
Soares JJ, Grossi G, Sundin O. Burnout among women: associations with
demographic ⁄ socio-economic, work, life-style and health factors. Arch Womens Ment
Health. 2007; 10(2):61-71.
Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontol 2000. 2005;
38(1):135-187.
Solomon A, Dursun D, Liu Z, Xie Y, Macri A, Pflugfelder SC. Pro- and anti-
inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with
dry-eye disease. Invest Ophthalmol Vis Sci. 2001. 42(10):2283-2292.
Soory M. Association of periodontitis with rheumatoid arthritis and atherosclerosis:
novel paradigms in etiopathogeneses and management. Open Access Rheumatol Res
Rev. 2010; 2:1-16.

References
102
Spinrad T, Eisenberg N, Granger DA, Eggum ND, Sallquist J, Haugen RG,
Kupfer A, Hofer C. Individual differences in preschoolers’ salivary cortisol and
alpha-amylase reactivity: Relations to temperament and maladjustment. Horm Behav.
2009; 56(1):133-139.
Sreebny LM. Saliva in health and disease: an appraisal and update. Int Dent J. 2000;
50(3):140-161.
Stabholz A, Soskolne WA, Shapira L. Genetic and environmental risk factors for
chronic periodontitis and aggressive periodontitis. Periodontol 2000. 2010; 53(1):138-
153.
Stashenko P, Dewhirst FE, Peros WJ, Kent RL, Ago JM. Synergistic interactions
between interleukin 1, tumor necrosis factor, and lymphotoxin in bone resorption. J
Immunol. 1987; 1;138(5):1464-1468.
Stooky G. The effect of saliva on dental caries. J Am Dent Assoc. 2008; 139(2):11-
17.
Strahler J, Mueller A, Rosenloecher F, Kirschbaum C, Rohleder N. Salivary α-
amylase stress reactivity across different age groups. Psychophysiology. 2010; 47(3):
587-595.
Streckfus CF, Bigler LR. Saliva as a diagnostic fluid. Oral Dis. 2002; 8(2):69-76.
Suchday S, Kapur S, Ewart CK, Friedberg JP. Urban stress and health in
developing countries: development and validation of a neighborhood stress index for
India. Behav Med. 2006; 32(3):77-86.
Surdacka A, Strzykata K, Rydzews-ka A. Changeability of oral cavity en-
vironment. Eur J Dent. 2007; 1(1):14-17.
T
Taba M Jr, Kinney J, Kim AS, Giannobile WV. Diagnostic biomarkers for oral and
periodontal diseases. Dent Clin North Am. 2005; 49(3):551-571.

References
103
Tanda N, Ohyama H, Yamakawa M, Ericsson M, Tsuji T, McBride J, Elovic A,
Wong DT, Login GR. IL-1 beta and IL-6 in mouse parotid acinar cells:
Characterization of synthesis, storage, and release. Am J Physiol. 1998; 274(1):47-56.
Tanner A, Maiden M, Lee K, Shulman L, Weber H. Dental implant infections. Clin
Infect Dis. 1997; 25(2):213-217.
Taubman M, Kawai T. Involvement of T-lymphocytes in periodontal disease and in
direct and indirect induction of bone resorption. Crit Rev Oral Biol Med. 2001; 12(2):
125-135.
Taylor J, Preshaw P, Donaldson P. Cytokine gene polymorphism and
immunoregulation in periodontal disease. Periodontol 2000. 2004; 35(9):158-182.
Thie N, Kato T, Boder G, Montplaisir J, Lavigne G. The significance of saliva
during sleep and the relevance of motor movements. Sleep Med Rev. 2002; 6(3):213-
227.
Thomson W, Spencer A. Is medication a risk factor for dental caries. Community
Dent Oral Epidemiol. 2002; 30(3):224-232.
Thylstrup A, Fejerskov O. Textbook of clinical cariology, 2nd ed. Copenhagen,
Munksgaard, 1994; 17-43.
Tortorella D, Gewurz B, Furman M, Schust D, Ploegh H. Viral subversion of the
immune system. Annu Rev Immunol. 2000; 18(1):861-926.
Turner RJ, Sugiya H. Understanding salivary fluid and protein secretion. Oral Dis.
2002; 8(1):3-11.
V
Van Dyke TE. Cellular and molecular susceptibility determinants for periodontitis.
Periodontol 2000. 2007; 45(1):10-13. (www.ivsl.org).
Van Dyke TC, Serhan CN. Resultion of inflammation: a new paradigm for the
pathogenesis of periodontal diseases. J Dent Res. 2003; 82(2):82-90.

References
104
Van Dyke TE, Kornman KS. Inflammation and factors that may regulate
inflammatory response. Review. J Clin Periodontol. 2008; 79(8):1503-1507.
Van Stegeren A, Rohleder N, Everaerd W, Wolf OT. Salivary alpha amylase as
marker for adrenergic activity during stress: Effect of beta blockade.
Psychoneuroendocrinology. 2006; 31(1):137-141.
Vered Y, Soskolne V, Zini A, Livny A, Sgan-Cohen HD. Psychological distress and
social support are determinants of changing oral health status among an immigrant
population from Ethiopia. Community Dent Oral Epidemiol. 2011; 39(2):145-153.
Von Kanel R, Hepp U, Kraemer B, Traber R, Keel M, Mica L, Schnyder U.
Evidens for low-grade systemic proinflammatory activity in patients with
posttraumatic stress disorder. J Psychiatr Res. 2007; 41(9):744-752.
W
Walker JG, Littlejohn GO, McMurray NE, Cutolo M. Stress system response and
rheumatoid arthritis: a multilevel approach. Rheumatology. 1999; 38(11):1050-1057.
Marketon JIW, Glaser R. Stress hormones and immune function. Cell Immunol.
2008; 252(1-2):16-26.
Waschul B, Herforth A, Stiller-Winkler R, Idel H, Granrath N. Effects of plaque,
psychological stress and gender on crevicular IL-1beta and IL-1ra secretion. J Clin
Periodontol. 2003; 30(3):238-248. (www.ivsl.org).
Williamson S, Munro C, Pickler R, Grap MJ, Elswich RK. Comparison of
biomarkers in blood and saliva in healthy adults. Nurs Res Pract. 2012; 246178:1-4.
Williams TJ, Yarwood H. Effect of glucocorticosteroids on microvascular
permeability. Am Rev Respir Dis. 1990; 141(2):39-43.
Wimmer G, Janda M, Wieselmann K, Jakse N, Polansky R, Pert C. Coping with
stress: its influence on periodontal disease. J Periodontol. 2002; 73(11):1343-1351.

References
105
Wimmer G, Kohldorfer G, Mischak I, Lorenzoni M, Kallus KW. Coping with
stress: its influence on periodontal therapy. J Periodontol. 2005; 76(1):90-98.
Wolff A, Ofer S, Raviv M, Helft M, Cardash HS. The flow rate of whole and
submandibular/sublingual gland saliva in patients receiving replacement complete
dentures. J Oral Rehabil. 2004; 31(4):340-343.
Y
Yao C, Li X, Murdiastuti K, Kosugi-Tanaka C, Akamatsu T, Kanamori N, Hosoi
K. Lipopolysaccharide-induced elevation and secretion of interleukin-1β in the
submandibular gland of male mice. Immunol. 2005; 116(2):213-222.
Yao C, Karabasil MR, Purwanti N, Li X, Akamatsu T, Kanamori N, Hosoi K.
Tissue kallikrein mK13 is a candidate processing enzyme for the precursor of
interleukin-1β in the submandibular gland of mice. J Biol Chem. 2006; 281(12):7968-
7976.
Yucel OO, Berker E, Gariboglu S, Otlu H. Interleukin-11, interleukin-1beta,
interleukin-12 and the pathogenesis of inflammatory periodontal diseases. J Clin
Periodontol. 2008; 35(5):365-370. (www.ivsl.org).
Z
Zadik Y, Bechor R, Shockat Z, Galor S. Ethnic origin and alveolar bone loss in
Israeli adults in Hebrew. Refuat Hpeh vehashinayim. 2008; 25(2):19-22.
Zefferino R, Facciorusso A, Lasalvia M, Narciso M, Nuzzaco A, Lucchini R,
L’Abbate N. Salivary markers of work stress in an emergency team of urban police
(1degree step). G Ital Med Lav Ergon. 2006; 28(4):472-477.

Appendices

106
Appendices
Appendix I: DASS-21 case sheet
Name: Date:
Please read each statement and circle a number 0, 1, 2 or 3, which indicates how much
the statement applied to you over the past week.
There is no right or wrong answers. Do not spend too much time on any statement.
The rating scale is as follows:
0 Did not apply to me at all.
1 Applied to me to some degree, or some of the time.
2 Applied to me to a considerable degree, or a good part of time.
3 Applied to me very much, or most of the time.
1. I found it hard to wind down 0 1 2 3
2. I tended to over-react to situations 0 1 2 3
3. I felt that I was using a lot of nervous energy 0 1 2 3
4. I found myself getting agitated 0 1 2 3
5. I found it difficult to relax 0 1 2 3
6. I was intolerant of anything that kept me from
getting on with What I was doing
0
1
2
3
7. I felt that I was rather touchy 0 1 2 3

107
Appendix II: Case sheet
Patient name: No: Age:
Telephone No: Date: Time:
Previous medical history and medication:
Periodontal health status:
Smoking:
Plaque index:
Mean PLI =
Gingival index:
Mean GI =
Bleeding on probing:
Percent BOP =

الخالصة
عمر تست تسببها كائنات حية دقيقه ممرضه شائعه مزمنة هلتهابيإ أمراض هي ما حول األسنان أمراض الخلفية:
تدمير إلى يؤدي مما لاللتهاباتؤدية الم المدورات الخلوية في عامةو وضعيةم رتفاعاتإ على تحفزو منطقه اللثة
ةلخطرا عواملال من العديدهنالك لإلسنان.الداعمة األنسجة على تؤثر التيالمدمر لتهاباأل عملية بواسطة األنسجة
همةالم العوامل أهم من واحدك اإلجهاد يعتبرو األسنان،ما حول أمراض تطوير في تساهم لعامة التيا أو ةموضعيال
،ه طويلهلفتر اإلجهادزداد ي ما عندف .ما حول األسنان أمراض ذلك في بما هلتهابياأل األمراض من لعديدا التي تسبب
.ما حول األسنانأمراض مثلوضعية الم أو عامةال األمراض إلى ؤديي مما لتهاباأل عملية على ؤثري قد فإنه
إلى باإلضافة .ما حول األسنانيرتبط بقوة مع أمراض مؤدي لاللتهاب مدور خلويبيتا هو 1البين ابيضاضي
مراضلأل المصاحب اإلجهاد وكذلك األجهاد المتكيف ستجاباتحرج في إ وسيطهو بيتا 1ابيضاضي البين ذلك،
.النفسيةو لعصبيةا
ما حول األسنان )مؤشر الصفيحة الجرثومية، مؤشر إلتهاب اللثة، ؤشراتم لتحديد ومقارنة أهداف الدراسة:
اللعابي بين طالب طب األسنان قبل، بيتا 1ابيضاضي البينمستوى األجهاد ومستوى ، مؤشر النزف عند الجس(
بيتا 1ابيضاضي البين ،اإلجهاد العالقة بينيجاد إل ذلك، إلى وباإلضافة. خالل وبعد فترة إمتحان نصف السنة
حول األسنان. لما السريرية المؤشراتواللعابي
راوحتت أنثى عشر اثنإوذكرا عشر اثنإ ; األسنان طبل الباط عشرينو أربعة من تكونت عينةال المواد والطرق:
:رئيسية فترات ثالث فيالمتتابعه في هذه الدراسة فحصهم تمالذين ،عاما( 12-11) بين أعمارهم
فترةال) نصف السنة متحانإ قبلاألقل على واحد بشهر األولى الفترة (I.
نصف السنة متحانالثانية خالل إ الفترة (فترةال II).
نصف السنة بعد إمتحان األقل على واحد بشهر الثالثة الفترة (فترةال III).
عينات جمع تم .المجموعات كل في اإلجهاد مستوى لقياس( DASS-21) اإلجهادو والقلق اإلكتئاب مقياس استخدم
تم .بواسطة نظام مقايسة األنزيم المرتبط الممتز المناعي اللعابي بيتا 1ابيضاضي البين مستوى لتحديد اللعاب من
مؤشر الصفيحة الجرثومية، مؤشر إلتهاب سن تضمنت لكل واضعم أربعة فيتسجيل مؤشرات ما حول األسنان
.اللثة، مؤشر النزف عند الجس
فترةال يف أعلى تكان السريرية ؤشرات ما حول األسنانم جميعل المتوسطات الحسابية أن ائجالنت أظهرت النتائج:
وكذلك، .(P ≤ 0.01) عالية عند معنوية ختالفاتإ وجود مع والثالثة األولى فتراتال في عليه كانت مما الثانية
اتفترال في عليه كانت مما الثانية فترةال في أعلى تكان اللعابي بيتا 1ابيضاضي البين تركيزل االوساط الحسابي
يظهر بيرسون، رتباطإ معامل ستخدامإب ،كذلك .(P ≤ 0.01) عالية عند إختالفات معنوية وجود مع والثالثة األولى
ؤشرات لما حول والم( اللعابي بيتا 1ابيضاضي البين) المناعي مؤشرال مع قوية عالية عالقة معنوية وجود اإلجهاد
.(P ≤ 0.01) عند األسنان السريرية

يثح األسنان، وأمراض ما حول إجهاد اإلمتحان بين رتباطاإل على قويا دليال الدراسة هذه نتائج قدمت ستنتاج:اإل
و مؤشرات ما حول األسنانو جهادلإل يات أعلىمستو إمتلكوا إمتحان نصف السنة خالل طب األسنان طالبأن
قوي اطرتبإ هناك كان ،كذلك .نصف السنة متحانإ وبعد قبلفترات مع بالمقارنة اللعابي بيتا 1ابيضاضي البين
.والمؤشرات لما حول األسنان السريرية اللعابي بيتا 1ابيضاضي البين اإلجهاد، بين

لما صحيةال حالةال على متحاناإل إجهاد تأثير
بين اللعابيبيتا 1بيضاضيإالبين و حول األسنان
ينالعراق األسنان طب طالب
من كجزءجامعة بغداد / األسنان طب كلية مجلس الى مقدمة رسالة
أمراض وجراحة ما حول األسنان في الماجستير درجة نيل متطلبات
من قبل
عذراء علي محمود سنانواأل الفم وجراحة طب لوريوسابك
بأشراف
هيمرالق اء محمود إب أ. الدكتورة
مراض وجراحة ما حول األسنانماجستير أ
م2013 ين األولرتش / ه1434 الحجةذو /