THE ROLE OF PPAR-γ IN TROPHOBLAST LAYER … ROLE OF PPAR-γ IN TROPHOBLAST LAYER DYNAMICS BASED ON...
113
THE ROLE OF PPAR-γ IN TROPHOBLAST LAYER DYNAMICS Based on a Cell Model of Trophoblast Differentiation by Khrystyna Levytska A thesis submitted in conformity with the requirements for the degree of Master of Science Graduate Department of Laboratory Medicine and Pathobiology University of Toronto ©Copyright by Khrystyna Levytska (2013)
-
Upload
vuongnguyet -
Category
Documents
-
view
219 -
download
3
Transcript of THE ROLE OF PPAR-γ IN TROPHOBLAST LAYER … ROLE OF PPAR-γ IN TROPHOBLAST LAYER DYNAMICS BASED ON...

THE ROLE OF PPAR-γ IN TROPHOBLAST LAYER DYNAMICS
Based on a Cell Model of Trophoblast Differentiation
by
Khrystyna Levytska
A thesis submitted in conformity with the requirements
for the degree of Master of Science
Graduate Department of Laboratory Medicine and Pathobiology
University of Toronto
©Copyright by Khrystyna Levytska (2013)

ii
ABSTRACT
THE ROLE OF PPAR-γ IN TROPHOBLAST LAYER DYNAMICS BASED ON A CELL MODEL OF
TROPHOBLAST DIFFERENTIATION
Degree: Master of Science
Year of Convocation: 2013
Name: Khrystyna Levytska
Graduate Department: Laboratory Medicine and Pathobiology
University: University of Toronto
Severe pre-eclampsia (sPE) is a pregnancy disorder stemming from the placenta which
features abnormal trophoblast layer physiology. A transcription factor, glial cell missing-1 (GCM-1),
regulates differentiation of cytotrophoblast cells into syncytiotrophoblast (SCT) within the layer.
GCM-1 is regulated by PPAR-γ, a nuclear receptor controlling trophoblast differentiation in mice.
We have previously shown that activation of PPAR-γ ameliorates disease features in a rat model of
sPE via an upregulation of heme oxygenase-1 (HO-1), a cytoprotective enzyme. Here, we assessed
how manipulating PPAR-γ influences gene expression and alters proliferation/differentiation
balance in a human cell line, BeWo, which mimics SCT formation. PPAR-γ activation induced HO-1
expression and led to a transient upregulation of GCM-1 expression. Blocking PPAR-γ activity
increased cell proliferation and decreased differentiation, whereas PPAR-γ stimulation did not
change this balance. Since HO-1 and GCM-1 are downregulated in sPE, their upregulation via PPAR-
γ offers insights into a pathway relevant to sPE management.

iii
ACKNOWLEDGEMENTS
I would like to thank my supervisor Dr. John CP Kingdom for his guidance, support and contribution
to the project design throughout my Master’s degree. Furthermore, I would like to put forth my
gratitude to my committee members, Dr. Theodore Brown, Dr. Sarah Keating and Dr. S. Lee
Adamson, as well as my international advisor, Dr. Asif Ahmed, for their contribution and helpful
discussions.
A special thank you goes out to my outstanding mentors, Mrs. Dora Baczyk and Dr. Sascha Drewlo,
who were my inspiration figures and role models since the very beginning of my scientific career.
Without their support, encouragement and scientific input I would not have been who and where I
am now.
Many thanks go out to members of collaborating laboratories, such as Dr. Lye’s lab, for helping me
advance my project swiftly and efficiently. I would also like to thank various funding sources, such
as Mount Sinai Hospital, Faculty of Medicine and School of Graduate Studies at the University of
Toronto, for providing me with the opportunity and resources necessary for the completion of my
degree.
Most importantly, I would like to thank my dear friends and family for their help, understanding
and never-ceasing support throughout my graduate career and always.

iv
TABLE OF CONTENTS
ABSTRACT .................................................................................................................................................... ii
ACKNOWLEDGEMENTS ............................................................................................................................. iii
TABLE OF CONTENTS ................................................................................................................................ iv
LIST OF TABLES ........................................................................................................................................ vii
LIST OF FIGURES ...................................................................................................................................... viii
LIST OF ABBREVIATIONS ........................................................................................................................... x
LIST OF APPENDICES ................................................................................................................................ xii
INTRODUCTION ........................................................................................................................................... 1
1.1. Healthy pregnancy ....................................................................................................................... 2
1.2. Hypertensive disorders of pregnancy ........................................................................................ 2
1.3. Pre-eclampsia (PE) ...................................................................................................................... 3
1.3.1. Disease symptoms .............................................................................................................. 3
1.3.2. Current lack of treatment options for women suffering from PE.................................... 3
1.4. Placenta ........................................................................................................................................ 4
1.4.1. Function of the healthy placenta ........................................................................................ 4
1.4.2. Placental trophoblast lineages ........................................................................................... 4
1.4.2.1. Extravillous trophoblast (EVT) lineage ............................................................................ 5
1.4.2.2. Villous cytotrophoblast (VCT) lineage ............................................................................. 6
1.4.3. Pathological features of sPE ............................................................................................... 7
1.5. Glial cell missing-1 (GCM-1) ........................................................................................................ 9
1.5.1. GCM-1: transcription factor controlling differentiation ................................................... 9
1.5.2. Role of GCM-1 in placentation and trophoblast differentiation ...................................... 9
1.6. Peroxisome proliferator-activated receptors (PPARs) ........................................................... 11
1.6.1. Family of peroxisome proliferator-activated receptors ................................................. 11
1.6.2. PPAR-γ gene and protein structure ................................................................................. 12
1.6.3. Role of PPARs in development ......................................................................................... 14
1.6.4. Regulation of PPAR-γ activity .......................................................................................... 14
1.6.5. PPAR-γ expression in healthy pregnancy and pregnancy complications ..................... 18
1.6.6. Role of PPAR-γ in trophoblast physiology ....................................................................... 20
1.6.7. Modulation of PPAR-γ during pregnancy and models of PE .......................................... 21

v
1.6.8. PPAR-γ controls a cytoprotective enzyme, heme oxygenase-1 (HO-1) ........................ 22
1.7. Heme oxygenase-1 (HO-1) ........................................................................................................ 22
1.7.1. HO-1 expression during pregnancy ................................................................................. 23
1.7.2. Role of HO-1 in placentation ............................................................................................. 24
1.7.3. Studies of HO-1 in cell-based models............................................................................... 26
1.7.4. Molecular manipulation of HO-1 ...................................................................................... 27
1.8. Rationale of the project ............................................................................................................. 28
1.9. Models used in this study .......................................................................................................... 28
1.10. Hypotheses and specific aims ................................................................................................... 29
MATERIALS AND METHODS .................................................................................................................... 30
2.1. Mouse model .............................................................................................................................. 31
2.1.1. Tissue collection ................................................................................................................ 31
2.1.2. RNA extraction, reverse transcription and qRT-PCR ..................................................... 31
2.2. In vitro model ............................................................................................................................. 33
2.2.1. Evaluation of cell models .................................................................................................. 33
2.2.2. The BeWo cell line ............................................................................................................. 33
2.2.3. Drug treatments of BeWo cells ......................................................................................... 34
2.2.4. Transfection of cells .......................................................................................................... 36
2.2.5. RNA analysis ...................................................................................................................... 37
2.2.5.1. Primer design .................................................................................................................. 37
2.2.5.2. Housekeeping gene stability check ............................................................................... 38
2.2.5.3. RNA extraction ................................................................................................................ 39
2.2.5.4. Reverse transcription and quantitative real time-PCR (qRT-PCR) ............................ 39
2.2.6. Protein analysis ................................................................................................................. 39
2.2.6.1. Protein isolation .............................................................................................................. 39
2.2.6.2. Western blotting ............................................................................................................. 40
2.2.6.3. Enzyme-linked immunosorbent assay (ELISA) ............................................................ 41
2.2.6.3.1. Free β-hCG ELISA .................................................................................................... 41
2.2.6.3.2. HO-1 ELISA .............................................................................................................. 41
2.2.6.4. Fluorescent immunohistochemistry (F-IHC) ............................................................... 42
2.2.6.4.1. Validation of E-cadherin as a cell membrane marker ........................................... 43
2.2.7. Luciferase assay ................................................................................................................. 43

vi
2.2.8. Cell proliferation assay ..................................................................................................... 45
2.2.9. Cellular fractionation analysis .......................................................................................... 46
2.2.10. Statistical analysis ............................................................................................................. 46
RESULTS ..................................................................................................................................................... 47
3.1. Placental gene expression in Gcm-1 heterozygous mice ........................................................ 48
3.2. GCM-1 silencing does not affect HO-1 and PPAR-γ expression in the BeWo cell model ....... 49
3.3. Time- and dose- responses to drug treatments in BeWo cells .............................................. 50
3.3.1. Expression of HO-1 ............................................................................................................ 50
3.3.2. Expression of PPAR-γ ........................................................................................................ 51
3.3.3. Expression of GCM-1.......................................................................................................... 52
3.4. Effect of PPAR-γ activity-modulating drugs on HO-1 expression in BeWo cells .................. 53
3.4.1. PPAR-γ activation induces a rapid rise in HO-1 RNA levels ........................................... 54
3.4.2. Intracellular HO-1 protein expression increases following PPAR-γ activation ........... 54
3.4.3. HO-1 release from BeWo cells increases with PPAR-γ activation ................................. 56
3.5. PPAR-γ participates in a negative auto-regulatory feedback mechanism ............................ 57
3.5.1. PPAR-γ expression is inversely related to PPAR-γ activity ............................................ 57
3.5.2. PPAR-γ protein levels correlate with gene expression profiles .................................... 58
3.5.3. Phosphorylation of PPAR-γ protein is increased following rosiglitazone treatment .. 59
3.5.4. Fluorescent immunohistochemistry analysis of PPAR-γ localization ........................... 60
3.5.5. Nuclear and cytoplasmic (phospho-) PPAR-γ expression.............................................. 61
3.6. Role of PPAR-γ in proliferation/differentiation balance ........................................................ 63
3.6.1. PPAR-γ-mediated induction of GCM-1 expression is transient ...................................... 63
3.6.2. PPAR-γ activity in BeWo cells .......................................................................................... 64
3.6.3. Effect of PPAR-γ activity modulation on free β-hCG release .......................................... 65
3.6.4. Visualization of BeWo cell fusion using fluorescent immunohistochemistry .............. 66
3.6.5. Effect of PPAR-γ activity on BeWo cell proliferation ...................................................... 67
DISCUSSION ............................................................................................................................................... 68
4.1 Conclusion .................................................................................................................................. 76
FUTURE DIRECTIONS ............................................................................................................................... 77
REFERENCES ............................................................................................................................................. 81
APPENDIX .................................................................................................................................................. 90

vii
LIST OF TABLES
Chapter 1: Introduction
Table 1: Patient characteristics ................................................................................................................ 19
Chapter 2: Materials and Methods
Table 2: Mouse primers ............................................................................................................................ 32
Table 3: Drugs and concentrations .......................................................................................................... 35
Table 4: Human primers ........................................................................................................................... 37
Table 5: Antibodies and dilutions ............................................................................................................ 40

viii
LIST OF FIGURES
Chapter 1: Introduction
Figure 1: Schematic representation of a placental-decidual interaction in healthy pregnancy. .......... 5
Figure 2: Schematic representation of a healthy trophoblast turnover.................................................. 7
Figure 3: Schematic representation of a placental-decidual interaction in PE. ..................................... 8
Figure 4: Structure of the GCM-1 protein. ............................................................................................... 10
Figure 5: Schematic representation of the roles of three PPAR family members. ............................... 12
Figure 6: PPAR-γ isoforms and structure. ............................................................................................... 13
Figure 7: PPAR-γ ligands. .......................................................................................................................... 15
Figure 8: Transactivation model of PPAR-γ activity. .............................................................................. 16
Figure 9: Post-translational modifications of PPAR-γ. ........................................................................... 17
Figure 10: Placental expression of PPAR-γ in pathologies and controls. ............................................. 19
Figure 11: Schematic representation of heme breakdown by HO-1. .................................................... 23
Chapter 2: Materials and Methods
Figure 12: Gene expression in human pregnancy-related cell lines. .................................................... 33
Figure 13: Preliminary assessment of gene expression in BeWo cells across passages...................... 34
Figure 14: Effects of drugs on cell viability over time. ........................................................................... 35
Figure 15: Location of siRNA sequences in the human GCM-1 mRNA. ................................................. 36
Figure 16: Stability of individual housekeeping genes in BeWo cells under different treatments. .... 38
Figure 17: E-cadherin expression in response to different drug treatments. ...................................... 43
Figure 18: Gene map of the 1kb upstream region of the human GCM-1. .............................................. 44
Figure 19: Plasmid design and oligonucleotide sequences in the luciferase reporter assay. ............. 44
Chapter 3: Results
Figure 20: Placental Hmox-1, Hmox-2 or Ppar-γ expression is unaltered in Gcm-1+/- mice. ................ 48
Figure 21: Downregulation of GCM-1 in BeWo cells has no effect on HO-1 and PPAR-γ levels. .......... 49
Figure 22: Dose-dependent expression of HO-1 in BeWo cells over time. ........................................... 51
Figure 23: Dose-dependent expression of PPAR-γ in BeWo cells over time. ........................................ 52
Figure 24: Dose-dependent expression of GCM-1 in BeWo cells over time. ......................................... 53
Figure 25: HO-1 mRNA expression levels following modulation of PPAR-γ activity. .......................... 54
Figure 26: Expression of HO-1 protein in BeWo cells. ........................................................................... 55
Figure 27: HO-1 release from BeWo cells. ............................................................................................... 56
Figure 28: PPAR-γ mRNA expression levels following modulation of PPAR-γ activity. ...................... 57
Figure 29: Expression of PPAR-γ protein in BeWo cells. ....................................................................... 58
Figure 30: Expression of phosphorylated PPAR-γ protein in BeWo cells............................................. 59
Figure 31: Effect of PPAR-γ-modulating drugs on its localization in BeWo cells. ................................ 60

ix
Figure 32: Cellular fractionation analysis of PPAR-γ expression in BeWo cells................................... 61
Figure 33: Nuclear phosphorylated PPAR-γ expression in BeWo cells. ............................................... 62
Figure 34: GCM-1 mRNA expression levels following modulation of PPAR-γ activity. ........................ 63
Figure 35: PPAR-γ activity in BeWo cells. ............................................................................................... 64
Figure 36: Effect of PPAR-γ manipulation on free β-hCG release in BeWo cells. ................................. 65
Figure 37: Effect of PPAR-γ modulation on BeWo cell fusion. ............................................................... 66
Figure 38: Effect of PPAR-γ activity modulation on BeWo cell proliferation. ...................................... 67

x
LIST OF ABBREVIATIONS
Abbreviation Meaning
AF-1 Activation function-1
AF-2 Activation function-2
CO Carbon monoxide
CT Cytotrophoblast
DBD DNA-binding domain
DR-1 Direct repeat-1
ERK Extracellular-signal-regulated kinase
EVT Extravillous trophoblast
GCM-1 Glial cell missing-1
hCG Human chorionic gonadotrophin
HDACs Histone deacetylases
HELLP Hemolysis, elevated liver enzymes and low platelets
HMOX-1 Gene coding for heme oxygenase-1
HO-1 Heme oxygenase-1
HO-2 Heme oxygenase-2
HO-3 Heme oxygenase-3
HTR8 Extra-villous trophoblast cell line
HUVECs Human umbilical vein endothelial cells
IUGR Intra-uterine growth restriction
JEG-3 Human choriocarcinoma cell line
LBD Ligand-binding domain
LMWH Low molecular weight heparin
Nrf-2 Nuclear factor (erythroid-derived 2)-like 2
PE Pre-eclampsia
PlGF Placenta-like growth factor
PPAR-α Peroxisome proliferator-activated receptor-alpha
PPAR-β/δ Peroxisome proliferator-activated receptor-beta (or delta)
PPAR-γ Peroxisome proliferator-activated receptor-gamma
PPRE PPAR-γ response element
RUPP Reduced uterine perfusion pressure
RXR Retinoid X receptor

xi
sFLT-1 Soluble fms-like tyrosine kinase-1
SA Spontaneous abortion
sENG Soluble endoglin
sIUGR Severe intra-uterine growth restriction
SP Spongiotrophoblast
sPE Severe pre-eclampsia
TIMP Tissue inhibitor of metalloproteinase
Treg Regulatory T
TS Trophoblast stem
uNK Uterine natural killer
VEGF Vascular endothelial growth factor
VCT Villous cytotrophoblast cell
WT Wildtype

xii
LIST OF APPENDICES
Chapter 1: Introduction
1. Drewlo, S., K. Levytska, and J. Kingdom, Revisiting the housekeeping genes of human placental
development and insufficiency syndromes. Placenta, 2012. 33(11): p. 952-4.
2. Levytska, K., et al., Heme oxygenase-1 in placental development and pathology. Placenta,
2013. 34(4): p. 291-8.

1
INTRODUCTION
Chapter 1:

2
Successful pregnancy requires several adaptations by the mother aimed to ensure normal
fetal development and maternal tolerance of pregnancy. The placenta is a central player; its proper
function contributes to successful implantation and subsequent embryonic and fetal growth. The
epithelial trophoblast layer covering the placental villi is in direct contact with maternal blood and
is central to both maternal adaptation and fetal development. As will be outlined in this chapter,
molecular dysregulation of the trophoblast lineages may lead to perinatal complications with
adverse outcomes for both mother and baby.
1.1. Healthy pregnancy
Successful human pregnancy is accompanied by hemodynamic changes in the mother
including maternal cardiac output and blood volume increase by 30-45% [1, 2]. These changes,
accompanied by vasodilation of the uteroplacental arteries, produce an exponential rise in utero-
placental blood flow to support the demands of the growing fetus. Higher cardiac output and blood
volume would predict a significant elevation in blood pressure were it not for the substantial
reduction in systemic vascular resistance that occurs in the second trimester.
1.2. Hypertensive disorders of pregnancy
In the event that maternal hemodynamic adaptations are defective, pregnant women
develop hypertension which may co-exist with other conditions. Hypertensive disorders are a
group of the most common complications during pregnancy, affecting 5-10% of all pregnancies [3].
These disorders include chronic hypertension, gestational hypertension, pre-eclampsia and chronic
hypertension with superimposed pre-eclampsia. Pre-eclampsia, which affects 3-5% of pregnancies
worldwide, is a major contributor to maternal, fetal and infant mortality and morbidity due to its
downstream effects on the mother’s wellbeing and neonatal development [4].

3
1.3. Pre-eclampsia (PE)
1.3.1. Disease symptoms
Severe early-onset pre-eclampsia (sPE) manifests clinically in the second trimester (after 20
weeks) of gestation. Its key features are hypertension (>140/90 mmHg) and proteinuria (>0.3 g of
protein excreted in urine within 24 hours), possibly complicated by edema [5]. sPE is a syndrome
affecting multiple organ systems, namely the placenta, the kidneys, the liver, and the brain [6]. The
feto-maternal interface is thought to suffer from hypoxia and/or reperfusion injury; it exhibits
several morphological abnormalities including impaired placental development and differentiation,
placental infarcts, and signs of non-infarct-related maternal vascular underperfusion [7].
Endothelial dysfunction in the kidneys (glomerular endotheliosis) results in high protein levels in
the urine. Hepatic ischemia, another hallmark of the syndrome, may lead to the manifestation of the
hemolysis, elevated liver enzymes and low platelets (HELLP) syndrome. Lastly, if PE progresses to
the most serious stage, it develops into eclampsia. Eclampsia, complicated by cerebral ischemia,
poses the largest health risk for the mother and may lead to migraines, seizures, coma, and death.
To date, there is no cure for PE other than delivery of the placenta, which in most severe
cases necessitates delivery of the fetus prior to 34 weeks of gestation. Several factors have been
associated with increased incidence of sPE, such as advanced maternal age at first pregnancy, use of
assisted reproductive technologies, obesity and others [4]. Considering that these demographic
trends are on the rise, there is a pressing need for extensive research into disease etiology and
pathogenesis to alleviate the associated health care burden and improve maternal and neonatal
conditions post-partum.
1.3.2. Current lack of treatment options for women suffering from PE
As mentioned above, the only current effective treatment option for sPE is delivery of the
placenta, which has severe long-term morbidities for the mother and the newborn thereby
increasing the risk of neonatal mortality. Several treatment options have been examined for women
suffering from or at risk of developing PE. In most complicated sPE cases, women receive
magnesium sulfate treatment at the onset of labor and for the initial 24 hours post-partum, where
the drug is thought to contribute to vasorelaxation and prevent eclamptic seizures [8]. Several trials
have examined the possibility of managing sPE symptoms with mineral or vitamin
supplementation, some with little success. For example, calcium supplementation was shown to be
effective in preventing sPE symptoms possibly due to its vasodilatory effects [9], while vitamins C
and E and fish oil supplements did not change the risk of developing the disease [10, 11].

4
Low-dose aspirin (commenced prior to 16 weeks of gestation) was shown to decrease
severe but not mild PE incidence by inducing vasorelaxation and preventing excessive placental
coagulation; however, it was not able to decrease rates of maternal mortality [12]. More recently,
the use of low molecular weight heparin (LMWH) has been shown to have positive outcomes for
pregnancies complicated by placental insufficiencies via anti-coagulation independent mechanisms
[13-16]. Despite some of these studies showing a decrease in the occurrence of sPE, none of these
interventions have shown an improvement in function of the organ thought to be a key player in
disease development, namely, the placenta.
1.4. Placenta
1.4.1. Function of the healthy placenta
The placenta is a transient organ present only during pregnancy and its main function is the
maintenance of a nourishing environment for the developing fetus. Humans undergo hemochorial
placentation where maternal blood is separated from the fetus by the chorion, ensuring an efficient
transfer of nutrients and waste. The placenta has several functions, including fetal nutrition,
respiration, waste excretion and hormone secretion [17, 18]. The placenta is responsible for both
active and passive transport of glucose, amino acids and other nutrients to sustain metabolic
demands of the growing fetus. It also mediates the transport of oxygen into, and removal of carbon
dioxide out of, the fetal circulation. Furthermore, it acts to eliminate waste (such as urea) from the
fetal environment [19]. Importantly, the placenta becomes an endocrine organ which is capable of
synthesizing glycogen, cholesterol, fatty acids, and hormones (such as estrogen, progesterone,
placenta-like growth factor [PlGF] and human chorionic gonadotropin [hCG]) [20].
1.4.2. Placental trophoblast lineages
The key component of the placenta is the trophoblast, responsible for the establishment and
maintenance of proper placental physiology throughout gestation and towards term. Two
trophoblast lineages exist during human placentation, each with is specific role in proper
pregnancy progression and maintenance [20]. The first cell type is the extravillous trophoblast
(EVT) responsible for placental invasion into the decidua, spiral artery remodelling and the
suppression of maternal immune response. The second cell type is the villous cytotrophoblast
(VCT); it provides the epithelial lining of floating placental villi which project into the intervillous
space (Figure 1).

5
Figure 1: Schematic representation of a placental-decidual interaction in healthy pregnancy. Extravillous cytotrophoblasts from the anchoring villous columns proliferate and invade the maternal decidua and contribute to spiral artery remodeling. This results in high blood flow from maternal arteries to the intervillous space, ensuring low pressure blood flow and delivery of oxygen to the growing fetus. Placental villi are covered by the trophoblast layer composed of two compartments, the underlying cytotrophoblast cells which replenish the overlying syncytiotrophoblast (appears here with the permission of the publisher from Everett et al, Placenta, 33:893-901, 2012 [21]).
1.4.2.1. Extravillous trophoblast (EVT) lineage
The EVT cells, originating from the columns of the anchoring villi, proliferate and invade the
external layer of the uterus, the decidua [20]. EVT cells at the base of the anchoring villus column
are of the proliferative phenotype, while those more distal of the column acquire the invasive
phenotype and are divided into interstitial and endovascular subtypes. Interstitial subtype invades
the maternal decidua; the endovascular subtype migrates toward the lumina of maternal spiral
arteries and displaces the endothelial and smooth muscle lining in arterial walls, thus, contributing
to blood vessel enlargement and vasorelaxation. Proper invasion of endovascular EVTs is
instrumental in the establishment of a high flow/low pressure perfusion in the intervillous space,
ensuring minimal shear stress on the villus surface and maximizing delivery of nutrients and
oxygen to the fetus [22]. These cells invade maternal arteries as early as 4-6 weeks of gestation,
with a marked increase in invasion seen between 10 and 12 weeks [23]; before 8 weeks of
gestation, these cells occlude uterine capillaries to limit blood oxygen delivery to the placenta and
the fetus which do not yet possess defence mechanisms against oxidative stress [24]. This hypoxia,
in turn, serves as a trigger for placental angiogenesis and villous tree branching.

6
To adequately invade the maternal tissue, EVTs must undergo several changes. For
example, they must alter their expression of integrins and matrix metalloproteinases (MMPs) in
order to co-ordinate decidual degradation and cell migration within maternal tissue [25]. Of note, it
has been shown that a tissue inhibitor of metalloproteinase-4 (TIMP-4) is upregulated in sPE
placentas, suggesting that this molecule contributes to extracellular matrix degradation in normal
pregnancy [26]. Furthermore, invading EVTs must communicate with decidual immune cells
(primarily uterine natural killer (uNK) cells); this interaction is critical for proper placental
establishment especially during early stages of development (reviewed in [27]).
1.4.2.2. Villous cytotrophoblast (VCT) lineage
The second trophoblast lineage is the villous cytotrophoblast (VCT) which forms a
continuous layer covering floating villi and is in direct contact with the maternal blood, creating the
interface between maternal and fetal circulations [20]. The trophoblast layer is composed of two
compartments: the cytotrophoblast (CT) cells and the syncytiotrophoblast (SCT), or syncytium
(Figure 2) [28]. The layer grows throughout gestation to accommodate expansion of the villous
surface area which acts to maximize net nutrient and waste exchange across the placenta. The CT
cell population is heterogeneous: some cells retain their stem-like potential and divide
symmetrically in order to replenish the cytotrophoblast pool; others lose their mitotic potential and
differentiate. The plasma membrane of post-mitotic differentiated cells disintegrates and their
nuclei fuse with the overlying syncytium layer. Subsequently, as evidence suggests, nuclei which
have differentiated apoptose as they aggregate to form syncytial knots which are then shed into the
maternal blood stream (as much as 3g per day in healthy pregnancy) [29, 30]. The process of
proliferation, differentiation, fusion, apoptosis and shedding within the trophoblast layer is
referred to as the trophoblast turnover. It is thought that abnormal trophoblast turnover
contributes to placental insufficiency syndromes such as sPE and IUGR (Widdows et al, in
preparation).

7
Figure 2: Schematic representation of a healthy trophoblast turnover. Stem (progenitor) cytotrophoblast cells undergo two types of divisions: symmetric and asymmetric. Symmetric divisions produce identical daughter cells and maintain the pool of cytotrophoblast cells. Asymmetric divisions, orchestrated by factors such as the differentiation marker glial cell missing-1, produce one daughter cell with fusogenic potential. This cell moves on to differentiate, and fuse with and donate its nucleus to the overlying syncytiotrophoblast layer. Nuclei within the syncytium subsequently form syncytial knots, undergo apoptosis and shed into the maternal blood stream. The process of cytotrophoblast proliferation, differentiation and fusion into the overlying syncytium is termed as the trophoblast turnover (appears here with the permission of the publisher from Lanoix et al, Molecular and Cellular Endocrinology, 348: 1-11, 2012 [31]).
1.4.3. Pathological features of sPE
Key features of a proper placental establishment and development are defective in placental
insufficiency syndromes, such as sPE and intrauterine growth restriction (IUGR). sPE is thought to
be a two stage disease: 1) pre-clinical and 2) clinical. The current hypothesis holds that in early
stages of sPE, pregnancy is characterized by poor placentation where the infiltration of EVTs into
the maternal decidua, and subsequent remodeling of spiral arteries, are inadequate (Figure 3) [32,
33]. The resulting oxidative and nitrosative stress at the placental bed [34, 35] possibly results due
to hypoxia or ischemia-reperfusion injury following reduced or intermittent uteroplacental blood
flow, respectively [36]. At this stage of disease development, the effects are local and restricted to
the feto-maternal interface while the mother remains asymptomatic.
By contrast, the second stage of the disease is thought to be characterized by a systemic
maternal response leading to a clinical presentation of sPE. While hypoxia and oxidative stress are
important contributors to disease pathology, another factor is an exaggerated maternal immune
response seen by elevated pro-inflammatory cytokines found in sera of mothers suffering from sPE
[37]. The involvement of both hypoxia and inflammation in pathological placental responses has
been supported by several findings. For example, the expression of a marker of hypoxia, hypoxia-
inducible factor 1-α (HIF1-α), in placental explants increases in low oxygen conditions (reviewed in

8
[38]); interestingly, however, stimulation of explants with angiotensin II (Ang II), a pro-
inflammatory peptide, under normoxic conditions has the same effect, in addition to decreasing
EVT differentiation [39]. Furthermore, hypoxia induces the release of anti-angiogenic factors
(described below) into culture medium from placental explants [40, 41], an effect which is
analogous to that seen following stimulaiton of tissue with pro-inflammatory cytokines in normoxia
[42, 43]. These findings support the notion that hypoxia is one of several causes of systemic
vascular dysfunction, and is most likely complicated by other factors such as wide-spread
inflammation and impaired underlying molecular mechanisms.
On a microscopic level, villi from PE placentas exhibit excessive formation of structures
called syncytial knots which are shed into the maternal blood stream and contribute to wide-spread
endothelial cell damage. Interestingly, these syncytial knots are capable of protein synthesis
possibly contributing to high serum levels of anti-angiogenic factors in sPE [44-46]. One such factor
has been identified to be soluble fms-like tyrosine kinase-1 (sFLT-1), highly upregulated in
maternal serum even prior to the development of PE symptoms [47]. sFLT-1, the soluble variant of
the membrane-bound vascular endothelial growth factor (VEGF) receptor, acts as a decoy protein
for VEGF and PlGF; upon sFLT-1 binding to these factors, their downstream angiogenic functions on
the endothelium are disrupted [48]. sFLT-1, along with other anti-angiogenic factors, contributes to
maternal vasoconstriction, vascular dysfunction and overt hypertension.
Figure 3: Schematic representation of a placental-decidual interaction in PE. Invasion by the extravillous trophoblasts is shallow leading to the lack of spiral artery remodeling. This is believed to result in unsteady blood flow into the intervillous space, hypoxia or hypoxia-reperfusion injury and detrimental downstream effects on the trophoblast compartment. These contribute to local infarcts, tissue necrosis and excessive shedding of microparticles into maternal bloodstream (appears here with the permission of the publisher from Everett et al, Placenta, 33:893-901, 2012 [21]).

9
As has been discussed thus far, there is evidence implicating that dysregulation of the
trophoblast compartment contributes to the pathology seen in PE, leading to the overt
manifestation of symptoms, such as systemic endothelial cell damage, hypertentsion, and kidney
damage. Several factors contribute to pregnancy maintenance and proper placentation, including
glial cell missing-1, peroxisome proliferator-activated receptor-gamma, and heme oxygenase-1. The
functions of these have been shown to be altered in pathological placental tissue. Each of these
factors and the roles they play in placentation and PE pathophysiology will be discussed in detail in
the following sections.
1.5. Glial cell missing-1 (GCM-1)
1.5.1. GCM-1: transcription factor controlling differentiation
Control of the trophoblast turnover has been studied extensively in recent years and several
factors have been identified in this physiological process. One of such factors is glial cell missing-1
(Gcm-1), first discovered in Drosophila where it was shown to regulate neuroblast fate by inducing
differentiation of neural precursors into glial cells [49]. Further studies have characterized Gcm-1
as a member of the zinc-containing transcription factor family, possessing a nuclear localization
signal, a transactivation domain and a DNA-binding domain (Figure 4A) [50, 51].
1.5.2. Role of GCM-1 in placentation and trophoblast differentiation
The human GCM-1 gene has been localized to chromosome 6 and genetic studies have
shown that its peptide sequence shares homology across human and rodent species (Figure 4B)
[52]. Although first discovered in the brain, GCM-1 is prominently expressed in a few non-neuronal
tissues, including the placenta. The crucial role of Gcm-1 in proper placentation in mice was shown
by Anson-Cartwright and colleagues in 2000 [53]. First, the group showed that in a healthy
placenta, Gcm-1 is localized in a small subset of cells which corresponded to future branch points
within the chorioallantoic plate. By creating a double Gcm-1 knock-out mouse, they illustrated that
Gcm-1 is responsible for proper branching of the chorioallantoic surface and development of the
labyrinth area in the placenta (equivalent of the exchange zone in the human placenta). Due to a
defect in branching, mice lacking Gcm-1 died in utero before E10.5. Upon examination, Gcm-1-/-
placentas showed lack of differentiated trophoblast cells and did not show signs of cell fusion [53].
Other studies in mice have also identified Gcm-1 as a crucial factor in chorioallantoic interaction
during placental development [54].

10
Figure 4: Structure of the GCM-1 protein. (A) Diagrammatic representation of the GCM-1 protein, which contains the general transcription factor domains: DNA-binding domain, nuclear localization signal and transactivation domain. (B) Mouse and human GCM-1 peptide sequences exhibit close homology with highest homology seen in the DNA-binding domain. Dark- and light- shaded regions correspond to identical and similar amino acids, respectively (appears here with the permission of the publisher and adapted from Nait-Oumesmar et al, The Journal of Histochemistry & Cytochemistry, 48(7): 915-922, 2000 [52]).
Studies localizing GCM-1 expression within the human placenta have shown similar
expression pattern to the one seen in the mouse [55]. Using in situ hybridization, it was confirmed
that GCM-1 expression is restricted to cytotrophoblast subset of cells in the villous trophoblast
layer. Furthermore, manipulating GCM-1 expression in the human placenta – downregulating it
using siRNA or upregulating its expression with forskolin [56] – has identified GCM-1 as a key
regulator of the trophoblast turnover [57]. Downregulation of GCM-1 in placental villi resulted in
cytotrophoblast proliferation, whereas forskolin-mediated induction of its expression led to higher
levels of differentiation and syncytium formation. Furthermore, GCM-1 was shown to induce
differentiation of trophoblast cells along the EVT pathway as assessed by the Matrigel migration
assay [57].
Consistent with the role of GCM-1 in trophoblast cell invasion and implantation, as well as
in the development of the labyrinth layer in the mouse, evidence shows that GCM-1 protein
expression is reduced in placentas with developmental complications, such as in sPE, when

11
compared to age-matched controls [58, 59]. Consequently, a study examining the relationship
between Gcm-1 and murine placental morphology confirmed the importance of this transcription
factor in proper placental development, specifically villous branching [59]. Using a heterozygous
(het) Gcm-1 model (since a double Gcm-1 knockout is lethal in utero), the authors showed that
placentas from het conceptuses exhibited higher placental sFlt-1 levels than those from WT mice, as
well as abnormalities in the syncytiotrophoblast and thickened inter-hemal membrane separating
maternal and fetal circulations, indicating defective maternal-fetal transfer [59]. Complementing
the above studies, GCM-1 has been shown to induce the expression of syncytin-1, a fusogenic
protein expressed in the human placenta which mediates fusion of cytotrophoblast cells into the
overlying syncytiotrophoblast layer [60, 61]. Collectively, data indicate that GCM-1 plays a role in
trophoblast turnover and placental morphology and further development.
1.6. Peroxisome proliferator-activated receptors (PPARs)
1.6.1. Family of peroxisome proliferator-activated receptors
Another family of proteins implicated in proper placentation and trophoblast development
are peroxisome proliferator-activated receptors (PPARs). PPARs are a family of ligand-activated
nuclear receptors and transcription factors. Three members of the PPAR family have been
described: PPAR-α, PPAR-β/δ and PPAR-γ (isoforms γ1 and γ2), general functions of which are
outlined in Figure 5. Expression of all three members has been assessed in different tissues [62-64].
PPAR-α is mostly expressed in kidney, liver, heart, and muscle cells; PPAR-β/δ is widely expressed,
with highest levels found in skin, brain and adipose tissue; and PPAR-γ has been mostly localized to
adipocytes, pancreatic β-cells, vascular endothelium, cells of the immune system, and the placenta
(reviewed in detail in [65]). The PPAR-γ isoform has been of particular clinical interest, since it was
shown to be strongly activated with anti-diabetic glitazones, implying its role as a potential
therapeutic target in serious health conditions, such as obesity, metabolic syndrome, and type II
diabetes [66]. Initial research on PPARs has shown their prominent role in adipocyte and
macrophage differentiation as well as adipogenesis (lipid storage); recent studies have also
underlined their functions in processes such as atherosclerosis, cardiovascular disease and
inflammation [67].

12
Figure 5: Schematic representation of the roles of three PPAR family members. Roles of PPAR-α, PPAR-β/δ and PPAR-γ in development, inflammation, lipid metabolism and atherosclerosis are described (appears here with the permission of the publisher and adapted from Michalik and Wahli, Current Opinion in Biotechnology, 10: 564-570, 1999 [68]).
1.6.2. PPAR-γ gene and protein structure
Four splice variants of PPAR-γ have been identified: γ1, γ2, γ3 and γ4; when translated, these
result in two protein isoforms: PPAR-γ1 and PPAR-γ2 (due to alternative splicing, γ1, γ3 and γ4 all
produce the same peptide sequence, PPAR-γ1) (Figure 6A). Mouse, rat and bovine PPAR-γ1 and
PPAR-γ2 proteins are highly conserved (PPAR-γ1 and PPAR-γ2 share 97-98% and 95-96% homology
with humans, respectively) [69]. Functional studies of this nuclear receptor have identified the
following five domains within its structure: 1) the “A/B” [or activation function-1 (AF-1)] domain
which has ligand-independent activity; 2) the highly conserved “C” [or DNA-binding] domain which
possesses classical two zinc-finger-like motifs with α-helical elements that bind to the PPAR-γ
response element (PPRE); 3) the “D” [or hinge] domain which interacts with the extension site
outside of the PPRE; and 4) the “E/F” [or activation function-2 (AF-2)] domain, which is the ligand-
binding domain (Figure 6B). Domains D and E/F are involved in dimerization of PPAR-γ with its
transactivation partner and cofactor, retinoid X receptor (RXR) [70]. The PPRE response element to
which the heterodimer complex binds has been characterized as a direct repeat 1 (DR1) motif
consisting of two copies of the consensus AGGTCA sequence separated by one nucleotide (Figure
6C) [71].

13
Figure 6: PPAR-γ isoforms and structure. (A) Diagrammatic representation of PPAR-γ isoforms at the RNA and protein level. Due to alternative splicing, γ1, γ3 and γ4 all produce the same peptide sequence – PPAR-γ1 (a 477 amino acid protein), while γ2 isoform results in a 505 amino acid peptide (appears here with the permission of the publisher and adapted from Zieleniak et al, Arch. Immunol. Ther. Exp., 56: 331–345, 2008 [72]). (B) Schematic representation of PPAR-γ domains A/B, C, D, and E/F (appears here with the permission of the publisher and adapted from Gelman et al, Current Opinion in Cell Biology, 17:216-222, 2005 [73]). (C) Representation of the PPAR-γ response element (PPRE) which is a direct repeat 1 motif consisting of two repeats of AGGTCA separated by one nucleotide. Below is a computer generated model of how PPAR-γ interacts with its cofactor and binds to the DNA (appears here with the permission of the publisher from Chandra et al, Nature, 456(7220): 350-356, 2008 [70]).

14
1.6.3. Role of PPARs in development
While initially discovered in their involvement with lipid metabolism and adipogenesis,
PPAR-β/δ and PPAR-γ have been shown to be important in placentation and embryogenesis.
Although PPAR-δ null pups are viable, these pregnancies are characterized by lower litter sizes
when compared to wildtype (WT) matings, primarily due to their developmental abnormalities
[74]. To dissect the contributions of fetal vs maternal PPAR-δ expression to pregnancy outcomes,
Wang et al performed cross-implantation experiments by introducing WT or null blastocysts into
WT or PPAR-δ null mothers. These experiments allowed the group to conclude that maternal PPAR-
δ was critical for on-time implantation and decidual angiogenesis, while the embryonic copy was
essential for successful placental development (placentas of null pups showed impaired ecto-
placental trophoblast development and chorioallantoic fusion) [74].
Contrary to the outcomes from PPAR-δ null pregnancies, double PPAR-γ mutations resulted
in embryonic death at E10 [75]. Interestingly, Barak et al found that lethality of these embryos was
observed in two stages: an initial defect was seen in trophoblast differentiation and placental
vascularization (1), which subsequently contributed to a myocardial defect (2). To prove the
connection between placental malformation and improper subsequent heart development, the
group performed chimera experiments where PPAR-γ null embryos were supplemented with WT
placentas. Researchers found that although the cardiac defect could be rescued, pups surviving to
term exhibited other lethal complications and died shortly after birth (within one week). The study
reinforced the importance of PPAR-γ in placentation and embryo development.
1.6.4. Regulation of PPAR-γ activity
Being a ligand-activated nuclear receptor, PPAR-γ is a useful target for pharmacological
manipulation. Furthermore, regulation of PPAR-γ expression and activity can be achieved at many
levels, such as control of its gene transcription, pharmacologic control of its activity with receptor
agonists and antagonists, and post-translational modifications (ex. phosphorylation, sumoylation
and ubiquitination). This section will focus on control of PPAR-γ activity with several known drugs
(agonists and antagonists) and phosphorylation.
PPAR-γ is a member of a family of ligand-activated nuclear receptors and a number of its
natural and synthetic ligands have been described (Figure 7A, B) [68, 72, 76]. PPAR-γ can be
activated by peroxisome proliferators (ex. xenobiotics) as well as long-chain fatty acid and their
derivatives [77-79]. Compounds, such as arachidonic acid and its prostaglandin metabolites of D2
and J2 families (ex. 15-deoxy-Δ12,14-prostaglandin J2) have been identified as powerful natural PPAR-

15
γ ligands (Figure 7A) [78, 79]. In addition to known natural ligands of PPAR-γ, several synthetic
ligands have been described (Figure 7B) [66, 72]. Thiazolidinediones, a class of drugs used to treat
diabetes and insulin resistance, are well-characterized synthetic ligands highly specific for the
gamma member of the PPAR family (reviewed in [80]). The most common thiazolidinediones are
pioglitazone and rosiglitazone, both of which are approved for use in the USA [66, 81]. It has been
shown that upon binding to PPAR-γ, these agonists induce conformational and other changes of the
receptor [63, 70], leading to transactivation (a DNA-dependent process) or transrepression (a DNA-
independent process).
Figure 7: PPAR-γ ligands. Natural (A) and synthetic (B) PPAR-γ agonists. (C) Synthetic PPAR-γ antagonists (appears here with the permission of the publisher and adapted from Zieleniak et al, Arch. Immunol. Ther. Exp., 56: 331–345, 2008 [72]).
A model of transactivation has been summarized by Feige et al, 2006 (Figure 8) [82]. It
proposes that in the absence of a ligand, PPAR-γ is coupled with its co-factor RXR-α and both are
bound to the PPRE in the target gene promoter. The heterodimer also interacts with several co-
repressors, histone deacetylases (HDACs) and nuclear co-repressor exchange factors (such as TBL1
and TBLR1), which results in a block of target gene transcription. Binding of an agonist to PPAR-γ at
the α-helix 12 (H12) within the carboxyl terminus (AF-2 domain) leads to conformational changes,
where H12 along with H3, 4 and 5 form a hydrophobic pocket which allows the recruitment of co-
activators. Furthermore, nuclear co-repressor exchange factors facilitate the degradation of co-
repressors and HDACs, while at the same time inducing a tighter binding of the heterodimer to the

16
PPRE and recruitment of co-activators and elements of the transcriptional machinery to initiate
transcription of downstream factors.
Figure 8: Transactivation model of PPAR-γ activity. In the absence of an agonist, PPAR-γ and RXR are bound to the PPRE, along with co-repressors, histone deacetylases (HDACs) and nuclear co-repressor exchange factors (TBL1 and TBLR1), blocking gene expression. Upon ligand binding, repressors dissociate and are replaced by co-activators; transcriptional machinery is recruited to induce transcription (appears here with the permission of the publisher and adapted from Feige et al, Progress in Lipid Research, 45: 120-159, 2006 [82]).
Another effect that agonist binding may have on gene expression is transrepression
(summarized in [82]). In this DNA-independent mechanism, activation of the PPAR-γ/RXR-α
heterodimer results in transrepression of target genes, thus, leading to a decrease in gene
expression. Transrepression can occur via three different pathways. First, agonist-binding to PPAR-
γ may lead to transcription factor tethering; under such circumstances, the PPAR-γ/RXR-α
heterodimer interacts with other transcription factors, preventing them from binding to their
response elements and inducing transcription of genes. In another mechanism, squelching, PPAR-γ
activation results in its competitive interaction (and sequestering) of co-activators shared between
both the transcription factor and PPAR-γ. Lastly, agonist binding might lead to a redirection of
common co-repressors to the other transcription factor in exchange for the factor’s co-activators;
this process is called inverse squelching. Irrespective of their mechanism, all three processes result
in repression of target gene expression without a direct interaction between PPAR-γ and the target
gene promoter (ie, independent of DNA binding).
Just as there are synthetic PPAR-γ agonists, several synthetic compounds have been
identified as PPAR-γ antagonists, among these, GW9662 (which also weakly antagonizes PPAR-α)
and T0070907 (Figure 7C) [83, 84]. T0070907 is an irreversible, non-competitive inhibitor of

17
PPAR-γ which binds covalently to the cysteine 313 residue of PPAR-γ2, located within helix 3 (H3).
This binding interferes with the proper alignment of helices 12, 3, 4, and 5, as well as induces the
recruitment of nuclear co-repressors (NCoRs) to the heterodimer [83, 84]. T0070907 can
outcompete the effects of rosiglitazone (an agonist) in biochemical assays and cell-based systems.
The overall effect that this antagonist binding has on receptor activity is an inhibition of PPAR-γ
activity and a decrease of target gene expression.
PPAR-γ can also undergo a series of post-translational modifications, including
phosphorylation, ubiquitination and sumoylation (Figure 9) (reviewed in [73, 85]). To date, one
phosphorylation site has been identified (located within the A/B domain), corresponding to serine
residue 84 in PPAR-γ1 or 112 in PPAR-γ2. Phosphorylation of this site with ERK1/2 kinases leads to
inhibition of PPAR-γ transcriptional activity as has been assessed in JEG-3 [86], 293K [87], and
fibroblast [88] cell models. This loss of transcriptional activity is accomplished either by the
recruitment of repressor proteins to the AF-1 domain, release of the activator or decrease in the
ligand binding efficiency, indicating that phosphorylation might impede transcription by
conformational changes within the LBD of PPAR-γ [86, 89]. Alternatively, phosphorylation of PPAR-
γ by complexes containing cdk7 or cdk9 kinases was shown to lead to activation of the
receptor [90, 91]. Although it appears that phosphorylation can either induce or inhibit PPAR-γ
activity, it remains as one of the most important ways of modulating receptor activity in a ligand-
independent manner.
Figure 9: Post-translational modifications of PPAR-γ. (A) Phosphorylation along with sumolyation within the activation function-1 (AF-1) domain results in reduced PPAR-γ activity. (B) Phosphorylation of PPAR-γ can also lead to higher receptor activity, for example, when phosphorylated by Cdk7 and Cdk9. (C) Ubiquitination is hypothesized to be related to phosphorylation of the PPAR-γ protein (although no direct ubiquitin-acceptor sites have been identified so far). Hypo-phosphorylated PPAR-γ was shown to have higher activity with respect to the adipogenic genes transcription and was associated with higher receptor degradation. (D) Lastly, sumoylation of PPAR-γ on K107 residue inhibits PPAR-γ activity in the context of inflammation (appears here with the permission of the publisher from van Beekum et al, Obesity, 17: 213-219, 2009 [85]).

18
1.6.5. PPAR-γ expression in healthy pregnancy and pregnancy complications
PPAR-γ expression patterns in human and mouse placentas have been studied extensively
[75, 92-94]. In the human placenta, PPAR-γ was found to localize in cytotrophoblast and
syncytiotrophoblast cells, as well as invading trophoblast columns [92-95]. In the mouse placenta,
PPAR-γ was detected as early as E8.5 and persisted throughout gestation. Its expression was
localized to the spongiotrophoblast and labyrinthine trophoblast, as well as secondary giant cells
[75].
Expression of PPAR-γ in placental insufficiency syndromes has not been well established.
Some reports have shown no differences in PPAR-γ mRNA and protein expression in sPE and IUGR
[92], while our preliminary results show an increase in mRNA expression and an upregulation of
PPAR-γ protein in pathologies when compared to controls (Figure 10) [patient population is the
same cohort as was used in Drewlo et al, Placenta, 33: 952-954, 2012 [96] (Appendix 1); Table 1,
appears here with permission of the publisher]. A study assessing expression of PPAR-γ during the
first trimester of pregnancy showed that its protein levels were highly upregulated in EVT cells
derived from placentas of spontaneous abortions (miscarriages) compared to those obtained from
terminations of pregnancy [95]. Furthermore, it was shown that activators of PPAR-γ are
significantly decreased in sera from PE pregnancies (implying lower PPAR-γ activity), and this
reduction is seen prior to onset of PE symptoms [97].

19
Figure 10: Placental expression of PPAR-γ in pathologies and controls. (A) PPAR-γ mRNA expression was assessed in different pathologies (PE and IUGR) and over gestation (early and late first trimester, second trimester and term). Patient characteristics are listed in Table 1. PPAR-γ protein expression in control (B) and PE (C) placentas was assessed using immunohistochemistry (400X magnification). Values represented as mean ± SEM; ***p≤0.001, *p≤0.05 (n=9-11). PTC, pre-term control; IUGR, intrauterine growth restriction; PE, pre-eclampsia.
Table 1: Patient characteristics
Severe intrauterine growth restriction (sIUGR): Birth weight ≤10th percentile, abnormal umbilical artery Doppler (absent end diastolic flow velocity (AEDFV) or reversed end diastolic flow velocity (REDFV)), normotensive women. Severe pre-eclampsia (sPE): Birth weight >10th percentile, BP >140/90, proteinuria >300 mg/day or ≥1+ on dipstick. Mixed IUGR (MIUGR) group contained patients with co-existing features of the two groups above. aPre-term control (PTC): Birth weight >20th percentile, no abnormal umbilical artery Doppler measurements, BP <140/90, no history of gestational diabetes, no histologic evidence of chorio-amnionitis. bHealthy term delivery by caesarian section. cHealthy term vaginal delivery, (>37+n weeks gestation).

20
Several animal studies have looked at how placental insufficiency affects PPAR-γ expression
in tissues other than the placenta, such as the adipose tissue and lungs. Interestingly, in the rat
utero-placental insufficiency model of IUGR, PPAR-γ expression in male and female neonatal lungs
was decreased [98] while it was increased in male visceral adipose tissue in the same model [99],
indicating that placental insufficiency plays a differential role on PPAR-γ expression in different
tissues. Additionally, in rats that were food-restricted during the second half of pregnancy (another
model of IUGR), an upregulation of PPAR-γ expression in adipose tissues of male pups was seen,
and these early programming events influenced rats’ development later in life, seen by adipocyte
hypertrophy and higher fat accumulation at 9 months of age [100]. Collectively, studies described
above support the role of PPAR-γ as an important modulator of pregnancy maintenance, as well as
its role in post-natal development.
1.6.6. Role of PPAR-γ in trophoblast physiology
Studies have shown that PPAR-γ plays a critical role in placentation, consistent with
findings by Barak et al in PPAR-γ null mice [75]. Linking the role of this nuclear receptor to
trophoblast layer physiology was a study done by Parast et al looking at the role of this nuclear
receptor in trophoblast differentiation [101]. Parast et al used PPAR-γ-null mouse trophoblast stem
(TS) cells to study the role of this transcription factor in normal trophoblast turnover. Of note is
their finding that PPAR-γ deficient TS cells showed decreased differentiation along the labyrinthine
trophoblast lineage and premature differentiation into giant cells (equivalent of human EVTs).
Equally as important was the finding that this transcription factor was able to directly regulate the
expression of Gcm-1, a differentiation marker described previously. Other studies have established
the regulation of Gcm-1 and syncytin-1 by PPAR-γ, supporting the role of these factors in normal
trophoblast differentiation and trophoblast turnover [102].
The role of PPAR-γ in cell proliferation and differentiation in terms of trophoblast
physiology has been explored using different models. As mentioned previously, lack of PPAR-γ in
murine trophoblast stem cells impairs their potential to differentiate [101]. Consistent with these
findings, addition of a specific PPAR-γ agonist to WT mouse TS cells induces their differentiation
along the labyrinthine pathway and upregulates expression of downstream markers such as Gcm-1
[101]. Further supporting their data, the group found that adenoviral re-introduction of PPAR-γ into
null TS cells decreased cell invasion (assessed using a Matrigel assay) and induced expression of
syncytiotrophoblast markers. A similar approach was taken when studying isolated human primary
trophoblast cells. It has been shown that in cultured primary cytotrophoblasts, synthetic ligand-

21
mediated stimulation of PPAR-γ induced their differentiation into syncytiotrophoblasts [93].
Additionally, in a follow-up study it was shown that cultured trophoblast cells treated with another
synthetic PPAR-γ agonist increased their lipid accumulation and free fatty acid uptake [103]. Lastly,
a study completed by Fournier and colleagues found that stimulation of PPAR-γ activity with either
natural or synthetic ligands decreased primary trophoblast invasion while having no effect on cell
proliferation [104]. Altogether, studies show that activation of PPAR-γ inhibits cytotrophoblast cell
invasion, which has important implications for sPE where EVT cell invasion is inadequate.
1.6.7. Modulation of PPAR-γ during pregnancy and models of PE
Several groups have studied how modulation of PPAR-γ activity during pregnancy impacts
placental development in rodents. Schaiff et al studied how the administration of rosiglitazone
throughout the last 8 days of pregnancy (E10.5-18.5 at 30mg/kg body weight) to WT mice mated
with WT or PPAR-γ+/- males affects placental morphology. They found that administration of PPAR-
γ agonist decreased fetoplacental weight, decreased spongiotrophoblast layer thickness and
reduced labyrinthine vasculature surface area in WT placentas, while it did not adversely impact
PPAR-γ+/- placentas [105]. The group, therefore, concluded that lower PPAR-γ expression was
protective against the effects of rosiglitazone during pregnancy. Furthermore, in a study conducted
by Nadra et al, rosiglitazone was administered to mice at a dose of 100mg/kg body weight for 12
days (E4.5-16.5) [106]. The group found that following rosiglitazone treatment, placental structure
exhibited overall disorganization, including features such as spongiotrophoblast thinning and
presence of glycogen cells within the labyrinth, as well as decreased expression of pro-agniogenic
genes. The study suggested that treatment of normal pregnancies with rosiglitazone negatively
influences placental development.
Contrary to the studies mentioned above which found that rosiglitazone has several
negative impacts on placental development, a study by McCarthy et al found a positive effect of
rosiglitazone treatment on PE-like pregnancies in rats [107]. Using the established reduced uterine
perfusion pressure (RUPP) rat model of PE [108], the group showed that administration of PPAR-γ
agonist during GD16-18 at a dose of 5mg/kg, ameliorated hypertension, endothelial dysfunction
and kidney function which were present in RUPP-treated animals receiving the vehicle, indicating a
beneficial effect of rosiglitazone on pregnancy complicated by placental insufficiency. Furthermore,
by blocking activity of PPAR-γ with a specific antagonist T0070907, the authors were able to induce
PE-like features, such as hypertension, higher plasma sFlt-1levels as well as lower levels of Vegf, in
healthy rats, indicating impaired endothelial function [109]. Additionally, blocking PPAR-γ activity

22
disrupted placental development assessed by lower rate of labyrinthine differentiation and higher
proliferation.
Studies described above indicate an important role of PPAR-γ in placental development and
pregnancy. Although results are contradictory, it should be mentioned that dosage (20mg/kg per
day dose in mice is the equivalent of the clinically relevant dose in humans), timing and duration of
drug administration differed in these studies. Thus, these factors should be strongly considered
when translating studies on rosiglitazone treatment to human pregnancies. Since it has been shown
that rosiglitazone is able to cross the placenta [110], the use of this drug as a therapeutic agent
should be carefully examined in the human placental explant model. Several case studies of women
being exposed to rosiglitazone (5mg/day) in first or second trimester at of pregnancy have not
shown any adverse pregnancy outcomes; however, these findings need to be confirmed in a large-
population study [111, 112].
1.6.8. PPAR-γ controls a cytoprotective enzyme, heme oxygenase-1 (HO-1)
Because of its role in placental development, and the ability of using pharmacological tools
to modulate its activity, PPAR-γ has been proposed as a potential therapeutic target for the
treatment of PE [107, 109, 113]. Interestingly, PPAR-γ is able to ameliorate disease characteristics
in the rat PE model by acting via its downstream target, heme oxygenase-1 (HO-1), an enzyme
responsible for heme breakdown within the cell [107]. Studies have shown that PPAR-γ is able to
directly regulate HO-1 expression in vascular smooth muscle cells and human umbilical vein
endothelial cells (HUVECs) [114]. Combined, these findings indicate that this enzyme, which
possesses multiple anti-inflammatory, cytoprotective and anti-oxidant functions, may play a role in
the pathogenesis of sPE.
1.7. Heme oxygenase-1 (HO-1)
Note: the following subsections have been published in Placenta journal by Levytska et al in 2013 (Appendix 2) [115].
Heme oxygenase (HO) family comprises three enzyme isoforms: HO-1, HO-2 and HO-3 [116,
117]. HO-1, the only inducible HO isoform, is highly expressed in tissues responsible for heme
metabolism, such as spleen and liver [118]. HO-2 is constitutively-expressed and mostly found in
the brain and testes [116]. The function of HO-3 is presently unknown, but the enzyme is believed
to be inactive. HO-1, a type I integral protein embedded in smooth ER membrane, was first isolated
from spleen and liver microsomal fractions and shown to catalyze the rate-limiting step of
intracellular heme breakdown [119]. Using oxygen, the enzyme metabolizes heme into three
components produced in equimolar amounts: carbon monoxide (CO), biliverdin and iron (Fe+2)

23
[120]. Under physiological conditions, biliverdin is immediately converted into bilirubin by
biliverdin reductase. The two metabolites of heme breakdown, CO and bilirubin, have important
cellular functions giving HO-1 its vasodilatory, anti-inflammatory, anti-apoptotic, anti-oxidant, and
cytoprotective properties (Figure 11) [121-128].
Figure 11: Schematic representation of heme breakdown by HO-1. HO-1 is responsible for heme metabolism within the cell. The process requires NADPH-cytochrome-P450 reductase and molecular oxygen (O2) which act as a co-enzyme and a substrate, respectively, for HO-1. HO-1 breaks down heme into three equimolar components: iron (Fe2+), biliverdin (immediately converted to bilirubin by biliverdin reductase), and CO. These metabolites are responsible for vasodilatory, anti-oxidant and other protective properties of HO-1 (appears here with the permission of the publisher from Levytska et al, Placenta, 34: 291-298, 2013 [115]).
1.7.1. HO-1 expression during pregnancy
Studies of HO-1 and HO-2 expression in mouse, rat and human placentas have been
numerous [129-133]. However, since the first report localizing HO to human placental tissue,
studies of HO-1 expression throughout human gestation and in pathology have been inconsistent.
McLean and colleagues were the first group to demonstrate HO-1 and HO-2 expression in human
placenta, showing that HO-2 protein was more abundant than HO-1 at term [134]. Yoshiki et al
reported that HO-1 and HO-2 proteins are localized in different cell types in the human placenta:
HO-1 immunohistochemistry revealed positive staining in the syncytiotrophoblast layer with traces

24
in the underlying cytotrophoblasts, while HO-2 was mostly expressed in endothelial and smooth
muscle cells [135]. This group also showed that HO-1 expression did not change throughout
gestation, while HO-2 expression increased towards term. Differential expression of HO-1 in the
invading cytotrophoblast cell columns has been noted; HO-1 was found to be high in distal, but
drastically decreased, in the proximal cell layers [133]. The first study looking at the expression of
HO-1 in pregnancy complications showed lower HO-1 protein expression in pre-eclamptic (PE)
placentas; this was in contrast to a positive association between placental HO-1 expression and
feto-placental vascularisation in normal pregnancy [122]. In support of pathologic sPE
observations, human in vivo studies demonstrate that while exhaled CO levels increase throughout
gestation in healthy women, end-tidal CO measurements are lower in hypertensive pregnant
women, especially those affected by sPE, supporting the role of CO as a physiologic vasodilator
implicated in gestational hemodynamic changes [136, 137]. Furthermore, Zenclussen et al. found
lower HO-2 protein levels in spontaneous abortion (SA) cases (vs normal pregnancy) and in PE (vs
age-matched controls), while HO-1 levels were low across all pathologies without significant
differences [138]. Lash et al found that infarcted villi in PE placentas had lower HO activity and
lower expression of HO-2 while HO-1 expression was unaffected [139]. In contrast to above studies,
Barber et al showed that HO-1 protein was undetectable in human placenta, and there was no
difference in HO-2 expression between PE and growth restricted pregnancies and preterm controls
[140]. These studies show that discrepancies regarding the expression of HO-1 and HO-2 in disease
states and throughout gestation exist and may be due to intra- and inter-tissue heterogeneity.
1.7.2. Role of HO-1 in placentation
The first description of an HO-1 knockout system was published by Poss and Tonegawa in
1997 [141, 142]. The authors found that HO-1 is required for proper iron reutilization, since adult
mice lacking HO-1 developed anemia and were susceptible to oxidative tissue damage and
inflammation [142]. Furthermore, the group showed that murine embryonic fibroblast cells lacking
HO-1 were sensitive to oxidative stress [141]. Kapturczak et al showed that mice lacking Hmox-1
had impaired immune responses and higher levels of pro-inflammatory Th1 factors [143]. Zhao and
colleagues were the first group to provide evidence for HO-1 as a critical player in proper placental
development [130, 144, 145]. The group demonstrated that in normal pregnancy, mice exhibit an
increase in utero-placental blood flow accompanied by a significant increase in maternal abdominal
aorta diameter (adaptations similar to those observed in humans). These changes were concurrent

25
with higher endogenous CO production and elevated plasma bilirubin levels, and placental HO-1
expression which peaked at E13.5 [130, 145]. In a follow-up study, Zhao et al characterized the
effect of HO-1 deficiency on placental development [144]. Crossing Hmox-1 heterozygous (+/-) mice
resulted in an altered Mendelian ratio of Hmox-1-/- pups (2.4% instead of the expected 25% ratio),
most of which aborted before E10.5. Hmox-1+/- placentas presented with a thinner
spongiotrophoblast (SP) layer due to increased apoptosis at the junction zone, supporting the role
of HO-1 as an anti-apoptotic player [144]. The implantation rate in heterozygous crossbreedings
was lower, and, at E12.5 and E15.5, the placentas were lighter and smaller (compared to wildtype
breedings). Furthermore, heterozygous mothers had higher plasma levels of sFlt-1, one of the key
players in vascular endothelial cell dysfunction, and elevated diastolic blood pressure, implying that
Hmox-1 is involved in the manifestation of sPE-like symptoms in mice, mimicking complications
seen in humans [146]. It was later shown that inadequate placentation of Hmox-1-/- placentas
resulted in IUGR and subsequent fetal death [147]. Exogenous application of CO, a product of heme
metabolism by HO-1, to Hmox-1-deficient mice during the implantation window decreased fetal
death in these pregnancies. It was also shown that Hmox-1+/+ blastocysts isolated from mice on E3.5
attached sooner than Hmox-1+/- blastocysts while blastocysts lacking Hmox-1 failed to attach
altogether [147]. This study also characterized the effect of Hmox-1 deficiency on placentation
showing that Hmox-1 is necessary for the differentiation of trophoblast stem cells to giant cells
which are critical for proper placental development. Early placental vascularisation is also affected
by Hmox-1 as seen from studies of crossbreeding Hmox-1 wildtype mice and Hmox-1 heterozygous
mice [146]. Breeding female mice partially deficient in Hmox-1 with males of the same genotype
resulted in feto-maternal interface malformations; namely, lower microvasculature blood vessel
volumes, less sinusoid spaces in the labyrinth and disorganized capillaries, when compared to
wildtype breedings. Interestingly, these alterations in placental morphology were independent of
the placental genotypes and occurred in both, Hmox-1+/+ and Hmox-1+/- placentas, as long as both
parents were Hmox-1 deficient. Since these impaired features of placental development are similar
to those observed in pregnancy complications such as sPE, the role of HO-1 in implantation and
placental development is further supported.

26
1.7.3. Studies of HO-1 in cell-based models
Cell models have also served as a useful tool to study HO-1 properties, which include
protection against cytotoxicity and cell death, induction of an angiogenic phenotype, and others.
HO-1 has been studied in cell models related to pregnancy and placental development, such as
HUVECs, HTR8 cells (a model for extravillous trophoblast cells, EVTs), and BeWo cells (a model for
syncytiotrophoblast formation). The activation of HO-1 by nuclear factor (erythroid-derived 2)-like
2 (Nrf-2), a prominent protector against oxidative stress, was described in the BeWo cell model,
where it protected cells against hydrogen peroxide- and Fe+2-induced stress [148]. Interestingly, a
cleaved isoform of HO-1 has been shown to have transcription factor-like activity by contributing to
the expression of cytoprotective genes in cultured fibroblast and Hepa cells [149]. Genetic profiling
of highly migratory EVTs and villous cytotrophoblast (CT) cells (with a low migratory potential)
isolated from cultured explants and first trimester human placentas, respectively, showed a lower
expression of HO-1 in EVTs vs CTs [150]. Confirming these findings, the group also showed that CT
cells had higher HO-1 RNA expression compared to EVT cells, as well as higher HO-1 protein
expression in proliferating CTs (vs EVTs) in first trimester placental explants, as seen by
immunohistochemistry. Furthermore, the study showed that retroviral induction of HO-1 in
naturally-migratory HTR-8 cells reduced their motility, while HO-1 silencing in non-migratory
BeWo cells increased their migration, suggesting that lower HO-1 expression is associated with a
lower cell motility and trophoblast invasion. Interestingly, the mechanism responsible for
increasing cell migration by HO-1 was via the regulation of PPAR-γ. These findings are in contrast
to a study by McCaig et al who showed that inhibition of global HO activity with zinc
protoporphyrin IX and antibody-mediated inhibition of HO-2 reduced invasion of primary CT cells
in vitro [151]. Discrepancies in studies of how HO affects cell invasion and motility may be due to
the use of different cell models; CT cells isolated from term placentas (when invasion is no longer
prominent) in the study by McCaig et al provide a different model compared to Bilban et al, who
used CT cells isolated from first trimester tissue (when invasion is high). Furthermore, cell models
used by Bilban et al are representative of the early placental development stages and, thus, might
reflect the actions of HO-1 in placental invasion more accurately. Although differential mechanisms
of HO-1 regulation in several cell types have been shown, collectively, studies suggest that HO-1
contributes to cell migration and invasion. These features are important in sPE since inadequate
invasion of the uterus by EVTs, together with defective formation of the outer syncytiotrophoblast,
imply dual defects in each type of the differentiated trophoblast [152].

27
1.7.4. Molecular manipulation of HO-1
The role of HO-1 in underlying mechanisms of placental insufficiency syndromes has been
studied extensively. Considering the prominent role of anti-angiogenic factors in the manifestation
of endothelial cell damage, it is natural to study the connection between the protective role of HO-1
and these disease markers. Implicating the role of HO-1 in sPE, it was shown that HO-1 induction or
CO administration in HUVECs inhibits their release of sFLT-1 and sEndoglin (sENG) [153, 154].
Both of these anti-angiogenic factors contribute to endothelial dysfunction in sPE; thus, reinforcing
the hypothesis that HO-1 and heme metabolites promote a pro-angiogenic phenotype [153]. This
same molecular pathway was studied in rats which have undergone the RUPP surgery; they had
elevated mean arterial pressure and exhibited lower fetal weight, suggesting that hypoxia
contributes to fetal growth restriction [155]. RUPP animals also have elevated plasma sFlt-1 and
higher superoxide production, both of which can be attenuated with an HO-1 activity inducer or by
the administration of bilirubin or CO. HO-1 placental expression is decreased in RUPP animals,
suggesting that in rat tissue, hypoxia negatively regulates HO-1 [156]. As mentioned previously,
HO-1 has the ability to decrease sFLT-1 release; interestingly, HO-1 is also able to offer protection
against sFlt-1 damage while bypassing this effect (ie, when plasma sFlt-1 levels are held constantly
high) [153, 157]. George et al showed that increasing HO-1 activity in rats with sFlt-1-induced
hypertension ameliorated elevated blood pressure despite the constantly elevated sFlt-1 levels
[157]. HO-1 induction improved endothelial function, decreased blood pressure and increased
VEGF levels. Supporting the anti-apoptotic role of HO-1, it was shown that HO-1 induction in the
RUPP-treated animals shifted the balance from pro-injury to pro-survival phenotype measured by
the restoration of intracellular ATP levels and increased phosphorylation of survival regulators
[158]. Collectively, studies described above support the hypothesis that pharmacologic
interventions aimed at increasing HO-1 expression and activity, particularly within the placenta,
may help restore maternal cardiovascular and endothelial functions which are defective in sPE.

28
1.8. Rationale of the project
sPE is a serious complication of pregnancy without a cure, other than delivery of the
placenta which often necessitates premature birth. Because of this observation, the placenta,
specifically the trophoblast layer, has been thought to be the key player in PE where altered
trophoblast turnover is observed. Several molecules localized to the trophoblast, such as GCM-1,
PPAR-γ and HO-1, have been shown to contribute to placental dysfunction. GCM-1, a trophoblast
differentiation marker, and HO-1, an enzyme with anti-oxidant and vasodilatory properties, are
both downregulated in PE placentas. It is speculated that decreased levels of these molecules lead
to shallow placental invasion, inadequate spiral artery remodeling, vasoconstriction and oxidative
damage.
In mice, the expression of both GCM-1 and HO-1 is regulated by another transcription factor,
PPAR-γ, the lack of which leads to loss of differentiation potential of trophoblast stem cells [101].
PPAR-γ is a ligand-activated nuclear receptor whose expression can be regulated with specific
natural and synthetic agonists and antagonists. Recently, we have shown that upregulating PPAR-γ
activity with rosiglitazone ameliorates disease features in a rat model of PE via its induction of HO-
1 [107]. Therefore, we decided to study the role of PPAR-γ in a human cell model. Our ability to
pharmacologically upregulate PPAR-γ activity poses a potential avenue for improving placental
trophoblast physiology (via upregulation of GCM-1 and differentiation) and lowering systemic
vascular resistance (via upregulation of HO-1 and vasodilatation).
1.9. Models used in this study
One of the objectives of our study was to test whether there is a connection between GCM-1
and HO-1 using two models. In the first model, we studied HO-1 expression in Gcm-1 heterozygous
mouse placentas. In the second model, we studied gene expression in GCM-1 silenced BeWo cells
originating from the human choriocarcinoma. Of the cell lines assessed, BeWo cells are the only cell
type which expresses all three genes of interest, namely, HO-1, GCM-1 and PPAR-γ. Furthermore,
while BeWo cells have an inherent ability to fuse spontaneously in culture, there is also a possibility
of inducing cell fusion pharmacologically. Because of these features, the BeWo cell model was used
to study key events associated with trophoblast function, namely, cell proliferation and
differentiation.

29
1.10. Hypotheses and specific aims
Our studies were based on the following hypotheses. First, we hypothesized that the
transcription factor GCM-1 controls the expression of HO-1 in the mouse placenta and in the human
choriocarcinoma-derived cell model. Second, we hypothesized that PPAR-γ-mediated expression of
GCM-1 and HO-1 regulates key events associated with trophoblast physiology, assessed in the
BeWo cell line.
Our hypotheses were tested in the following aims:
1. Analysis of gene expression in Gcm-1 heterozygous mice.
2. Analysis of gene expression in GCM-1-silenced BeWo cells.
3. Establishment of the role of PPAR-γ in trophoblast physiology using the BeWo cell model.
a. Establishing the effect of PPAR-γ agonist and antagonist on expression of HO-1.
b. Establishing the effect of PPAR-γ activity-modulating drugs on PPAR-γ mRNA and
protein expression and localization.
c. Establishing the effect of PPAR-γ agonist and antagonist on the differentiation axis,
including the effect on GCM-1 expression, cell proliferation, differentiation and
fusion.

30
MATERIALS AND METHODS
Chapter 2:

31
2.1. Mouse model
A mouse model was used to study the effects of Gcm-1 deletion on Hmox-1 expression.
Because the homozygous deletion of Gcm-1 is lethal in mice [53] and GCM-1 expression in human
PE placentas is hypomorphic [58], the heterozygous Gcm-1 mouse model was used (mouse
breeding and tissue collection, as well as mRNA isolation, was performed by members of Dr.
Adamson’s laboratory, University of Toronto, and kindly donated for our study [59]). Virgin 6-10
week old wildtype CD1 females (Gcm-1+/+) were mated with heterozygous males (Gcm-1+/-), which
resulted in an approximate 1:1 Mendelian ratio of Gcm-1 wildtype and heterozygous conceptuses.
2.1.1. Tissue collection
Once removed from the uterus on embryonic days 13.5 (E13.5) and E17.5, placentas were
dissected to remove decidual tissue; then they were further microdissected to enrich for the
labyrinth region. Samples were stored in RNAlater (Ambion, Life Technologies, Burlington, ON,
Canada) and frozen at -80oC for further RNA analysis by quantitative real time-polymerase chain
reaction (qRT-PCR). All conceptuses were genotyped at Transnetyx, Inc. (Cordova, Tennessee, USA).
2.1.2. RNA extraction, reverse transcription and qRT-PCR
RNA was isolated from mouse labyrinth-enriched placental samples using the TRIzol
method (Invitrogen, Burlington, ON, Canada) according to manufacturer’s instructions (n=6 per
genotype). Genomic DNA was removed using DNase treatment (RNase-free DNase Set, Qiagen,
Toronto, ON, Canada). RNA was further purified using the RNeasy Mini-elute Cleanup Kit (Qiagen,
Toronto, ON, Canada). RNA concentration was measured using NanoDrop 1000 (Thermo Scientific,
Ottawa, ON, Canada). One microgram (µg) of each sample was reverse transcribed to cDNA using
iScript™ Reverse Transcription Supermix (Bio-Rad, Mississauga, ON, Canada) according to the
following protocol: 5 minutes at 25OC, followed by 30 minutes at 42OC, and 5 minutes at 85OC. Gene
expression was measured using qRT-PCR and run on the CFX384 Real-Time PCR Detection System
(Bio-Rad, Mississauga, ON, Canada) with LuminoCt® SYBR® Green qPCR ReadyMix™ (Sigma-
Aldrich, Oakville, ON, Canada). qRT-PCR reactions were performed according to the following
protocol: initial activation at 95OC for 5 minutes, followed by 38 thermal cycles of denaturation at
95OC for 5 seconds and annealing/extension at 60OC for 20 seconds, followed by a melting curve
(from 65OC to 95OC in 0.5OC increments for 5 seconds). Primers were designed using the Primer-

32
BLAST tool (http://www.ncbi.nlm.nih.gov/tools/primer-blast/) for the following genes: murine
glial cell missing-1 (Gcm-1), heme oxygenase-1 (Hmox-1), heme oxygenase-2 (Hmox-2), peroxisome
proliferator-activated receptor-gamma (Ppar-γ). Primers were manufactured by Integrated DNA
Technologies, Inc (Skokie, IL, USA). Housekeeping genes [TATA box binding protein (Tbp), β-actin
(BAct), and glyceraldehyde-3-phosphate dehydrogenase (Gapdh)] were chosen according to
published literature [59]. Primer efficiency and specificity checks were performed on the CFX96
Real-Time PCR Detection System (Bio-Rad, Mississauga, ON, Canada) with LuminoCt® SYBR®
Green qPCR ReadyMix™ (Sigma-Aldrich, Oakville, ON, Canada). E15 placental cDNA was used as the
standard in 1:4 decreasing dilution series with the starting concentration of 50 x 10-9 ng/µL; qRT-
PCR reactions were performed as described above. Primer sequences and efficiencies are
summarized in Table 2. CFX ManagerTM Software, Version 2.1 (Bio-Rad, Mississauga, ON, Canada)
was used to analyze gene expression. Expression of genes of interest (ie, Gcm-1, Ppar-γ, Hmox-1 and
Hmox-2) was normalized to the geometric mean of three house-keeping genes (Tbp, BAct and
Gapdh). To compare gene expression between wildtype and heterozygous Gcm-1 placentas,
expression in heterozygous samples was expressed as fold change vs wildtype placentas (set as 1).
Table 2: Mouse primers
Gene Primer sequence (5’ → 3’) Number of bases Primer pair efficiency
Gcm-1 Forward TGA AGC TTA TTC CCT GCC GA 20 113.9% Reverse TGA TCA TGC TCG CCT TTG G 19
Ppar-γ Forward TCA CAA TGC CAT CAG GTT TGG 21 106.8% Reverse AAT GCT TTG CCA GGG CTC GCA 21
Hmox-1 Forward GGC TTT AAG CTG GTG ATG GCT TC 23 113.0% Reverse TTC GGT GCA GCT CCT CAG GGA A 22
Hmox-2 Forward ATG AGC CAA GGA CCA GAG TGA G 22 108.5% Reverse TCC GAG GTC TCC ACC TCT GAA GA 23
BAct Forward TCG TGC GTG ACA TCA AAG AGA 21 108.2% Reverse GAA CCG CTC GTT GCC AAT A 19
Gapdh Forward AGG AGT AAG AAA CCC TGG ACC 21 106.6% Reverse AGG CCC CTC CTG TTA TTA TGG 21
Tbp Forward CGG ACA ACT GCG TTG ATT TTC 21 108.6% Reverse AGC CCA ACT TCT GCA CAA CTC 21

33
2.2. In vitro model
2.2.1. Evaluation of cell models
Several pregnancy-related cell lines were evaluated to select a cell-based model that
expresses as many target genes as possible. Four cell models were evaluated: the human
choriocarcinoma cell lines JEG-3 and BeWo, human transformed extravillous trophoblast cell line
HTR8 cells and human umbilical vascular endothelial cells (HUCECs). JEG-3 and BeWo cells were
obtained from ATCC (Burlington, ON, Canada); HUVECs were purchased from Lonza (Allendale, NJ,
USA); and HTR8 cells were a kind gift from Dr. Graeme Smith (Queen’s University, Kingston, ON,
Canada). Based on gene expression analysis (Figure 12), the human choriocarcinoma cell line BeWo
was selected as the cell model of choice.
BeWo HTR8 JEG-3 HUVEC0.0
0.5
1.0
1.5
GCM-1
PPAR-
HO-1
sFLT-1
Cell line
Gene e
xpre
ssio
n
Figure 12: Gene expression in human pregnancy-related cell lines. GCM-1, HO-1, PPAR-γ and sFLT-1 expression was assessed in BeWo, HTR8, JEG-3 and HUVE cells. BeWo cells were chosen as the cell model of choice (n=1).
2.2.2. The BeWo cell line
Prior to performing any experiments, the BeWo cell line was fingerprinted at The Centre for
Applied Genomics (SickKids, Toronto, ON, Canada); markers were found to be identical to those in
the ATCC database. Gene expression of PPAR-γ, HMOX-1 and GCM-1 in BeWo cells across passages
was evaluated (Figure 13). Based on the results, only BeWo cells between passages 10-20 were
used in all experiments. Cells were maintained in F12K medium (Wisent Inc, St. Bruno, QC, Canada),
supplemented with 10% fetal bovine serum (FBS) (Canadian grade, heat-inactivated, Invitrogen,
Burlington, ON, Canada), 100 units/mL penicillin, 100 µg/mL streptomycin and 2nM L-glutamine
(Life Technologies, Burlington, ON, Canada), in atmospheric O2/5% CO2 at 37OC.

34
8 10 15 17 19 20 220.0
0.5
1.0
1.5
2.0
2.5
Passage
PP
AR
- m
RN
A e
xpre
ssio
n a
cro
ss p
assages
(norm
aliz
ed to H
KG
s)
8 10 15 17 19 20 220.0
0.5
1.0
1.5
2.0
2.5
Passage
HO
-1 m
RN
A e
xpre
ssio
n a
cro
ss p
assages
(norm
aliz
ed to H
KG
s)
8 10 15 17 19 20 220.0
0.1
0.2
0.3
0.4
Passage
GC
M-1
mR
NA
expre
ssio
n a
cro
ss p
assages
(norm
aliz
ed to H
KG
s)
Figure 13: Preliminary assessment of gene expression in BeWo cells across passages. mRNA expression of PPAR-γ (A), HO-1 (B), and GCM-1 (C) was assessed in BeWo cell passages 8, 10, 15, 17, 19, 20, and 22, and normalized to expression of housekeeping genes (HKGs). Cells between passages 10 and 20 were used in subsequent studies (n=1).
2.2.3. Drug treatments of BeWo cells
BeWo cells were seeded at 100,000 cells per well in 24-well culture plates and allowed to
attach for 24 hours. Cells were treated the following day with a variety of drugs (Table 3). First,
cells were pretreated with the inhibitor (T0070907) and/or vehicles for 30 minutes. Then, medium
containing treatments (ie, agonist, antagonist, and/or vehicles) was applied. Cell viability under all
treatments was assessed at 48 hours of culture using CytoTox-ONETM Homogeneous Membrane
Integrity Assay (Promega, Madison, WI, USA). No drug treatments resulted in significant cell
toxicity at 48 hours, except for T0070907 at 10µM (Figure 14). The chosen drug concentrations
were based on our preliminary results and/or published literature. Rosiglitazone and forskolin in
vitro administration is more common than that of T0070907, which has been mostly used in animal
models [159, 160]. The group which first described T0070907 as a PPAR-γ antagonist have
A B
C

35
identified its IC50 as 1nM and showed that 1µM is able to bind irreversibly and fully inhibit the
receptor activity; thus, we based our dose-response studies on this value [161].
Table 3: Drugs and concentrations
Chemical Mode of action Concentration(s) Vehicle Supplier
T0070907 specific antagonist of PPAR-γ; binds irreversibly to cysteine in helix 3, thus, changing conformation of helix 12 of the PPAR-γ LBD
0.1µM 1µM
10µM
DMSO Cayman Chemical Ann Arbor, MI, USA
Rosiglitazone selective synthetic PPAR-γ agonist; induces PPAR-γ translocation into the nucleus; increases transcriptional activity
10µM 100µM
DMSO Enzo Life Sciences Burlington, ON, Canada
Forskolin increases cellular concentration of cAMP; indirectly induces expression of GCM-1 and activity of PPAR-γ
20µM 25µM
Ethanol Sigma-Aldrich Oakville, ON, Canada
Vehicle Rosi (10M) Rosi (100M) T007 (1M) T007 (10M)
0.0
0.5
1.0
1.5
24 hours
48 hours
72 hours
a bbb
Treatment
Rela
tive c
ell
toxi
city
(com
pare
d to v
ehic
le)
Figure 14: Effects of drugs on cell viability over time. Cell viability was measured using the CytoTox-ONE Homogeneous Membrane Integrity Assay at 24, 48 and 72 hours post-treatment. No significant differences on cell viability were found at 24 and 48 hours of culture (with the exception of T0070907 at 10µM concentration). Data represented as mean ± SEM; a,b, p≤0.05 vs vehicle control, set as 1 (n=4-5). Rosi, rosiglitazone; T007, T0070907.
Cells were treated for 3, 6, 24 or 48 hours, then washed in ice-cold Dulbecco's phosphate-
buffered saline (D-PBS) (Wisent Inc, St. Bruno, QC, Canada), and collected according to different
downstream applications. For RNA analysis, cells were collected into RLT Plus buffer (Qiagen,
Toronto, ON, Canada) with 10% β-mercaptoethanol (Fisher Scientific, Ottawa, ON, Canada). For
protein analysis, cells were scraped and collected either in RIPA Buffer (Thermo Scientific, Ottawa,
ON, Canada) with phosphatase (Phosphatase Inhibitor Cocktail 2, Sigma-Aldrich, Oakville, ON,

36
Canada) and protease inhibitors (cOmplete Mini, EDTA-free Protease Inhibitor Cocktail Tablets,
Roche Applied Science, Laval, QC, Canada) diluted according to manufacturer’s instructions; or in
HO-1 Extraction Buffer (Enzo Life Sciences, Burlington, ON, Canada) with the same inhibitors
added. Conditioned medium was collected at 24 and 48 hour time points, centrifuged for 5 minutes
at 425g at room temperature (RT) to remove cellular debris. All collected samples were stored at -
80OC for further analysis.
2.2.4. Transfection of cells
Four different siRNA sequences targeting the human GCM-1 gene were assessed
(unpublished observations); two of them, siRNA 815 and 201, were found to have the strongest
effects on GCM-1 expression [57]. Furthermore, the combination of both oligonucleotide sequences
led to an even more pronounced gene downregulation; thus, the combination of siRNA 815 and 201
was used for our subsequent experiments in BeWo cells.
The cells were co-transfected with two double-stranded siRNA oligonucleotides (21mer),
named 815 and 201, against the human GCM-1 sequence (Qiagen, Toronto, ON, Canada). 815 siRNA
was designed to 5’-AACCTACAGTAGTGGAGACCT-3’ and 201 siRNA was designed to 5’-
AACTCCCGCATCCTCAAGAAG-3’ DNA targets (see Figure 15 for gene map). Non-silencing control
(sequence: 5’-TTCTCCGAACGTGTCACGT-3’) was used as a negative control. At 40-50% confluency,
BeWo cells were transfected with 20µM of a 1:1 cocktail of 815 and 201 GCM-1 siRNA or non-
silencing control siRNA with Lipofectamine Reagent (Invitrogen, Burlington, ON, Canada) overnight
for 24 hours, in accordance with the manufacturer’s instructions. The following day, media was
changed and cells were treated with 25µM forskolin or vehicle control for another 48 hours.
Experiments with fluorescent-labeled siRNA established 80-90% transfection efficiency (data not
shown). Toxicity of siRNA treatment was monitored with Human Interferon Alpha ELISA kit (PBL
Biomedical Laboratories, Brussels, Belgium).
Figure 15: Location of siRNA sequences in the human GCM-1 mRNA. Two sequences, 201 and 815, were designed against human GCM-1 mRNA transcript.

37
2.2.5. RNA analysis
2.2.5.1. Primer design
Human primers were designed using the online Primer-BLAST tool
(http://www.ncbi.nlm.nih.gov/tools/primer-blast/) for genes listed in Table 4. Primers were
produced by Integrated DNA Technologies, Inc (Skokie, IL, USA). Primer efficiency was tested using
RNA combined from samples from first and second trimester human placental tissue, placental
pathologies (PE, IUGR and mixed PE-IUGR) and age-matched controls. Placental tissue was crushed
with mortar and pestle in liquid nitrogen. RNA from these samples was isolated using the TRIzol
Reagent (Invitrogen, Burlington, ON, Canada) according to manufacturer’s instructions. Samples
were further purified using RNeasy Plus Mini Kit (Qiagen, Toronto, ON, Canada) according to
manufacturer’s specifications. RNA quality and amount was measured using the Experion RNA
StdSens Analysis Kit (Bio-Rad, Mississauga, ON, Canada); only samples with RQI>7.5 were used to
create a pooled cDNA sample. One microgram of pooled RNA sample was reverse transcribed using
iScript™ Reverse Transcription Supermix (Bio-Rad, Mississauga, ON, Canada) according to
manufacturer’s instructions. Primer efficiency and specificity checks were performed according to
the same protocol as summarized in section 2.1.2 (see Table 4 for human primer efficiencies).
Table 4: Human primers
Gene Primer sequence (5’ → 3’) Number of bases
Primer pair efficiency
GCM-1 Forward ATG GCA CCT CTA GCC CCT ACA 21 102.5% Reverse GCT CTT CTT GCC TCA GCT TCT AA 23
PPAR-γ Forward CTC AGT GGA GAC CGC CCA GG 20 109.2% Reverse GCT CCA GGG CTT GTA GCA GG 20
HMOX-1 Forward CGG CTT CAA GCT GGT GAT GGC 21 110.6% Reverse CCT GCT CCA GGG CAG CCT TG 20
GAPDH Forward AGA TCA TCA GCA ATG CCT CC 20 108.2% Reverse CAT GAG TCC TCC CAC GAT AC 20
YWHAZ Forward ACT TTT GGT ACA TTG TGG CTT CAA 24 95.3% Reverse CCG CCA GGA CAA ACC AGT AT 20
TBP Forward TGC ACA GGA GCC AAG AGT GAA 21 110.4% Reverse CAC ATC ACA GCT CCC CAC CA 20
SDHA Forward TGG GAA CAA GAG GGC ATC TG 20 101.7% Reverse CCA CCA CTG CAT CAA ATT CAT G 22
HPRT Forward TGA CAC TGG CAA AAC AAT GCA 21 95.7% Reverse GGT CCT TTT CAC CAG CAA GCT 21

38
2.2.5.2. Housekeeping gene stability check
Stability of five human housekeeping genes across different drug treatments was tested in
BeWo cells using the GeNorm method, which is part of BiogazelleTM software. The software
calculates relative housekeeping gene stability in relation to other housekeeping genes. The gene
stability value, M, indicates an average pairwise variation of the control housekeeping gene with
other housekeeping genes. Thus, higher M value indicates high variation in control gene expression
between treatments, and, conversely, lower M value indicates high gene stability (for a detailed
explanation, see [162]). Based on results obtained from the preliminary experiments, HPRT, YWHAZ
and TBP were chosen as housekeeping genes for subsequent gene analyses (Figure 16).
Figure 16: Stability of individual housekeeping genes in BeWo cells under different treatments. Lower GeNorm M value reflects a higher stability of the gene across different treatments. TBP, YWHAZ and HPRT were the most stable housekeeping genes and were used in subsequent qRT-PCR reactions.

39
2.2.5.3. RNA extraction
BeWo cell RNA was extracted using the RNeasy Plus Mini Kit (Qiagen, Toronto, ON, Canada)
according to manufacturer’s instructions. Briefly, cells in the 24-well plate were washed with ice-
cold D-PBS (Wisent Inc, St. Bruno, QC, Canada), and collected with 350µL of RLT Plus Buffer with
10% β-mercaptoethanol. After the removal of genomic DNA, RNA was precipitated using 70%
ethanol. Following several washes with RW1 and RPE buffers, total RNA was eluted with 30µL of
RNase-free water. RNA concentration was measured immediately using NanoDrop 1000 (Thermo
Scientific, Ottawa, ON, Canada).
2.2.5.4. Reverse transcription and quantitative real time-PCR (qRT-PCR)
Five hundred nanograms (ng) of each sample were reverse transcribed to cDNA using
iScript™ Reverse Transcription Supermix (Bio-Rad, Mississauga, ON, Canada) according to the
following protocol: 5 minutes at 25OC, 30 minutes at 42OC, and followed by 5 minutes at 85OC. Gene
expression was measured using quantitative real time-PCR and run on the CFX384 Real-Time PCR
Detection System (Bio-Rad, Mississauga, ON, Canada) with LuminoCt® SYBR® Green qPCR
ReadyMix™ (Sigma-Aldrich, Oakville, ON, Canada). qRT-PCR reactions were performed according to
the following protocol: initial activation at 95oC for 5 minutes, followed by 38 thermal cycles of
denaturation at 95oC for 5 seconds and annealing/extension at 60oC for 20 seconds. Gene
expression was normalized to the geometric mean of three housekeeping genes (HPRT, TBP and
YWHAZ). Gene of interest expression in each treatment was expressed as fold change relative to its
respective vehicle (set as 1).
2.2.6. Protein analysis
2.2.6.1. Protein isolation
Following treatment for 24 or 48 hours, BeWo cells were collected in 250µL of lysis buffer
with phosphatase and protease inhibitors added (as described above). Samples were homogenized
using the Bullet Blender Blue Homogenizer with Air Cooling (Ideal Scientific, Ancaster, ON, Canada)
for 3 minutes. Samples were then placed on a mutator for 1 hour at 4OC, after which they were spun
at top speed for 10 minutes at 4OC; the supernatant was transferred to a fresh tube. Protein
concentration was measured using Pierce BCA Protein Kit (Thermo Scientific, Ottawa, ON, Canada),
according to manufacturer’s instructions.

40
2.2.6.2. Western blotting
Twenty-five µg of total protein [diluted in RIPA Buffer with phosphatase and protease
inhibitors added (as described above), and 4X Loading Dye (Invitrogen, Burlington, ON, Canada)
with 10% β-mercaptoethanol (Fisher Scientific, Ottawa, ON, Canada)] were electrophoresed in 1x
TG-SDS Buffer (Wisent Inc., St. Bruno, QC, Canada) at 50-100V, on 4-20% Mini-PROTEAN TGXTM
pre-cast Gels, (Bio-Rad, Mississauga, ON, Canada). Following electrophoresis, proteins were
transferred onto 0.2µm PVDF membrane, Trans-Blot TurboTM Transfer Pack, Midi format (Bio-Rad,
Mississauga, ON, Canada) using the Trans-Blot Turbo Transfer System (Bio-Rad, Mississauga, ON,
Canada). Immediately following the transfer, membranes were blocked in 5% milk/TBS-T
(Blotting-Grade Blocker, Bio-Rad, Mississauga, ON, Canada; TWEEN®20, Sigma-Aldrich, Oakville,
ON, Canada) for 1 hour at room temperature. All primary antibodies were applied overnight at 4OC
(see Table 5 for dilutions) in 5% milk/TBS-T. The following day, membranes were washed with
0.001% TBST, 3x 20 minutes. Membranes were incubated for 1 hour at RT in respective secondary
antibodies (GE Healthcare UK Limited, UK) diluted 1:3,000 in 5% milk-TBST. Following three
washes in TBST (20 minutes each), membranes were developed using Western Lightning Plus-ECL
(Thermo Scientific, Ottawa, ON, Canada) on Premium Autoradiography Film (Denville Scientific,
South Plainfield, NJ, USA). Band intensities within linear range were quantified using Quantity One
software (Bio-Rad, Mississauga, ON, Canada). Protein of interest levels were normalized to a
housekeeping protein (α-tubulin or β-actin). Protein expression under each treatment was further
compared to its respective vehicle control (set as 1).
Table 5: Antibodies and dilutions
Antigen Origin Size (kDa) Dilution Supplier
HO-1 Rabbit 32 1:500 (western) Enzo Life Sciences Burlington, ON, Canada
PPAR-γ Rabbit 54-57 1:100 (western) 1:100 (F-IHC)
SantaCruz Biotechnology Dallas, TX, USA
Phospho-PPAR-γ Rabbit 57 1:500 (western) Sigma-Aldrich Oakville, ON, Canada
E-cadherin Mouse 110 1:1000 (western) 1:100 (F-IHC)
Abcam Toronto, ON, Canada
Lamin B Mouse 67 1:500 (western) SantaCruz Biotechnology Dallas, TX, USA
α-Tubulin Mouse 50 1:2000 (western) Sigma Oakville, ON, Canada
β-Actin Mouse 42 1:2000 (western) Abcam Toronto, ON, Canada

41
2.2.6.3. Enzyme-linked immunosorbent assay (ELISA)
Protein release from BeWo cells into the media was quantified using enzyme-linked
immunosorbent assays (ELISA). Conditioned media was collected into 96-well plates and was first
centrifuged at 425g for 5 minutes at RT after which the supernatant was transferred to a new plate.
Protein concentration in the media was measured using Pierce BCA Protein Kit (Thermo Scientific,
Ottawa, ON, Canada), according to manufacturer’s instructions. Samples were stored at -80OC until
further analyses.
2.2.6.3.1. Free β-hCG ELISA
Free β-hCG ELISA Kit (Phoenix Pharmaceuticals, Inc., Burlingame, CA, USA) was used to
measure β-hCG release in conditioned media following 48 hours of culture. The ELISA was
conducted according to manufacturer’s instructions. Briefly, 45µg of total protein (or 15µg of total
protein from forskolin-treated samples) was used per reaction, diluted in D-PBS (Wisent Inc, St.
Bruno, QC, Canada). Following incubation of samples and standards, the plate was washed with
deionized water (3X) and incubated with Enzyme Conjugate Reagent. The plate was developed
using the TMB Reagent; the reaction was stopped with the Stop Solution provided. Endpoint optical
density was measured at 450nm with a reference wavelength of 655nm. β-hCG protein was
quantified using the standard curve and protein levels were normalized to total released protein. β-
hCG release under different treatments was further normalized to respective vehicle(s) (set as 1).
2.2.6.3.2. HO-1 ELISA
Human ImmunoSet HO-1 ELISA development set was purchased from Enzo Life Sciences,
Burlington, ON, Canada; the final assay protocol was adapted from manufacturer’s instructions.
Briefly, black bottom, half-volume, 96-well plates were used to plate the HO-1 capture antibody
overnight. On the following day, plates were blocked for at least 1 hour at RT. Subsequent
incubations were performed on a shaker at RT. Standards and samples diluted in Assay Buffer were
incubated for 1 hour. After washing with Wash Buffer (4X), samples were incubated with detection
antibody for 45 minutes. Following another set of washes, the plate was incubated for 20 minutes
with SA-HRP conjugate. The plate was developed using QuantaBluTM Fluorogenic Peroxidase
Substrate Kit (Thermo Scientific, Ottawa, ON, Canada). After 30 minutes of incubation with
QuantaBlu working solution, stop solution was applied and excitation and emission maxima were
measured at 325nm and 420nm, respectively. Amount of HO-1 protein in ng/mL was calculated

42
using the standard curve. HO-1 protein levels were normalized to total released protein. HO-1
release under different treatments was further normalized to the corresponding vehicle (set as 1).
2.2.6.4. Fluorescent immunohistochemistry (F-IHC)
Immunofluorescence was used to visualize PPAR-γ protein localization and expression in
BeWo cells under different treatments and to study cell fusion using e-cadherin as a cell membrane
marker. The following protocol was used for the experiment. Coverslips were submerged into
100% ethanol and left to dry under UV light for 30 minutes. BeWo cells were plated on coverslips
placed into 6-well plates at a density of 150,000 cells per well. Cells were treated for 1, 3, 6, 24, and
48 hours the next day. Following treatment, cells were washed in ice-cold D-PBS (Wisent Inc, St.
Bruno, QC, Canada) and fixed in 1:1 methanol:acetone solution for 3 minutes on ice. Cells were
permeabilized in 0.2% TritonX-100 (Fisher Scientific, Ottawa, ON, Canada) for 5 minutes on ice,
washed, and blocked for 1 hour at RT in Protein Block Serum-Free, Ready-to-use (DAKO,
Carpinteria, CA, USA). Primary antibodies for PPAR-γ and e-cadherin (see Table 5 for dilutions)
were diluted in the same blocking solution and incubated overnight at 4OC. The following day,
PPAR-γ signal was amplified with anti-rabbit biotinylated antibody (diluted 1:300 in blocking
solution) for 1 hour at RT. Lastly, DAPI (1:1,000; Sigma-Aldrich, Oakville, ON, Canada), anti-mouse
Alexa546 antibody (1:200; Invitrogen, Burlington, ON, Canada) and SA-Alexa488 (1:1,000;
Invitrogen, Burlington, ON, Canada), all diluted in blocking solution, were incubated for 1 hour at
RT. Coverslips were mounted on slides using a Immu-Mount mounting medium (Thermo Scientific,
Ottawa, ON, Canada). Slides were left to dry in the dark and stored at 4OC until further analysis.
Fluorescent microscopy was performed using the Spinning Disc Confocal Microscope (DMI6000B,
Leica Microsystems, Concord, ON, Canada). Z stacks were taken using Volocity software, Version
5.3.0 (PerkinElmer, Woodbridge, ON, Canada) and deconvolved using Huygens Essential software,
Version 4.2.2 (Scientific Volume Imaging, Hilversum, The Netherlands). All images were taken on
the same day, under the same acquisition settings, normalized to the highest PPAR-γ expression
under T0070907 treatment, to minimize variability and allow parallel comparison in protein
expression across time points and treatments. For fusion visualization, images were taken at 200X
magnification; for PPAR-γ localization analysis, z stacks were taken at 630X magnification.

43
2.2.6.4.1. Validation of E-cadherin as a cell membrane marker
E-cadherin was chosen as a cell surface marker used to visualize cell fusion in BeWo cells.
Although its expression has been shown to decrease upon BeWo cell differentiation [163], we did
not see a difference in E-cadherin protein expression under rosiglitazone, T0070907 or forskolin
treatments (when normalized to α-tubulin as a housekeeping protein; Figure 17).
Vehicle Ro10M T1M For20M0.0
0.5
1.0
1.5
Treatment
Rela
tive e
-cadherin e
xpre
ssio
n
(com
pare
d to v
ehic
le)
Vehicle Ro10M T1M For20M0.0
0.5
1.0
1.5
TreatmentR
ela
tive e
-cadherin e
xpre
ssio
n
(com
pare
d to v
ehic
le)
Figure 17: E-cadherin expression in response to different drug treatments. E-cadherin protein expression was assessed at 24 (A) and 48 (B) hours of treatment. Protein expression was normalized to α-tubulin levels; expression under each drug treatment was compared to respective vehicle control (set as 1, red dashed line). No significant differences were observed. Values expressed as mean±SEM (n=3). Ro, rosiglitazone; T, T0070907; For, forskolin.
2.2.7. Luciferase assay
Two putative PPAR-γ binding consensus sequences were identified within 250bp upstream
region of the human GCM-1 promoter using the Gene2Promoter software (Version 6.3, Genomix,
Germany; see Figure 18 for gene map). Oligonucleotides of these sites were synthesised and linkers
added for cloning into the pGL4.10[luc2] cloning vector (binding sequences 1 and 2; Promega,
Madison, WI, USA). Sites were mutated to generate sequence-based controls (mutated sequences 1
and 2). Binding and mutated sequences are outlined in Figure 19. Oligonucleotides and vectors
were digested independently, purified and ligated. One-Shot TOP10 Chemically Competent E. coli
cells (Invitrogen, Burlington, ON, Canada) were transformed and plated on ampicillin-positive
plates. Antibiotic-resistant clones were selected and grown; plasmids (including the control renilla
gene-containing plasmid) were isolated using Plasmid Plus Midi Kit (Qiagen, Toronto, ON, Canada)
and sequenced to confirm sequence insertion. Quality and amount of plasmid DNA was confirmed
using the NanoDrop 1000 (Thermo Scientific, Ottawa, ON, Canada). All plasmids were brought to
similar concentrations in TE Buffer.

44
Figure 18: Gene map of the 1kb upstream region of the human GCM-1. The 1kb region upstream of the human GCM-1 gene was analyzed for PPAR-γ binding sites. Two putative PPREs were found within 250 base pairs from the transcription start site (sequence 1 and sequence 2). The gene map does not show the full GCM-1 DNA sequence; only exons 1 and 2 are displayed (map not to scale).
Figure 19: Plasmid design and oligonucleotide sequences in the luciferase reporter assay. (A) Plasmid map of the pGL4.10[luc2] vector (adapted from Promega Inc. protocol). (B) Duplex oligonucleotide sequences for binding sequence 1 (top) and mutated sequence 1 (bottom). (C) Duplex oligonucleotide sequences for binding sequence 2 (top) and mutated sequence 2 (bottom). Nucleotides conserved between the consensus PPRE (shown above for comparison) and our identified binding sites are bolded. Mutated nucleotides are shown in red. PPAR-γ binding site is highlighted in pink, RXR-α binding site shown in blue.
For transfection experiments, BeWo cells were seeded at 12,500 cells/well in clear-bottom
tissue culture-suitable 96-well plates (Greiner bio-one, Monroe, NC, USA) to obtain 30% confluency.
The following day, cells were transfected using ExGene 500 transfection reagent (Fermentas,
Pittsburgh, PA, USA) and transfection efficiency was confirmed using a GFP-expressing control

45
plasmid. Transfection optimization experiments established that 200-300ng of plasmid DNA was
optimal for 70-90% transfection efficiency using 0.7µL of transfection reagent. Transfection mixes
were generated for binding sequence 1, binding sequence 2, mutated sequence 1 and mutated
sequence 2. Each mix contained a 10:1 composition of experimental vector to a co-reporter vector
(renilla). Following transfection mix application to the cells, culture plates were centrifuged for 5
minutes at 300g to improve transfection efficiency, according to the manufacturer’s protocol. Eight
hours following transfection, media containing different chemicals was applied (rosiglitazone,
T0070907, both or vehicle). Cells were cultured for additional 24 hours, following which media was
removed, cells were lysed using Passive Lysis Buffer and the assay was performed according to
Dual-Luciferase Reporter Assay System protocol (Promega, Madison, WI, USA). Cell extracts were
kept on ice and luciferase activity was measured using an automated photometer. First, following
Luciferase Assay Reagent II application, firefly luciferase activity was measured. Then, well
contents were quenched with the Stop & Glo Reagent which also allowed the measurement of
renilla luciferase activity. Renilla luciferase activity was an internal calibrator used to correct for
differences in cell density and transfection efficiency between wells. Relative luciferase activity
under the treatment with each plasmid (binding sequences 1 and 2) and drug was normalized to its
corresponding vehicle control. Furthermore, to reduce random allosteric sequence-dependent
background signal, signal obtained with each binding sequence was normalized to the
corresponding mutated sequence.
2.2.8. Cell proliferation assay
Relative BeWo cell numbers were assessed using the CellTiter-FluorTM Cell Viability Assay
(Promega, Madison, WI, USA). In 96-well cell culture-suitable plates, cells were seeded at 10,000
cells per well, in 50µL of media. Cells were treated the following day with drugs diluted in 50µL of
media. Cell number was measured at 48 hours of culture. The manufacturer’s protocol was adapted
as follows. The GF-AFC Substrate was diluted 1:1,000 in Assay Buffer to make CellTiter-FluorTM
Reagent. Next, 15µL of D-PBS and 65µL of CellTiter-FluorTM Reagent were added to each well and
incubated for 45 minutes at 37OC, protected from light. The following controls were included in the
measurement: 1) maximum lysis control (to validate the absence of a false positive result), 2) no
cell, media only control (to use as a background fluorescence measurement), and 3) no cell, media
with vehicle control (to account for the effect of vehicle on fluorescence). The plate was read with
excitation and emission maxima set at 400nm and 505nm, respectively. Recorded optical density
(OD) values were blanked using the media only/no cell control to account for background

46
fluorescence; no differences were found between controls 2) and 3). Fluorescent measurements
obtained with this assay represent an indication of the relative BeWo cell number, such that cell
proliferation can be assessed between different drug treatments relative to their respective
controls (set as 1).
2.2.9. Cellular fractionation analysis
Cellular fractionation was performed using the Nuclear Extract Kit (Active Motif, Burlington,
ON, Canada). The protocol was adapted as follows. Cells in a 24-well plate were collected 1, 6, 24
hours post-treatment in 180µL PBS + Phosphatase inhibitor cocktail. Cells were centrifuged for 5
minutes at 500rpm at 4OC. After discarding the supernatant, the pellet was resuspended in 300µL
1X hypotonic buffer. Following a 15-min incubation on ice, 15µL of detergent were added and
mixture was vortexed. Then it was centrifuged for 30 seconds at 14,000g at 4OC and the
supernatant (ie, the cytoplasmic fraction) was collected. The remaining pellet was resuspended in
50µL of Complete Lysis Buffer, vortexed, and incubated for 30 minutes on a rocking platform at 4OC.
The suspension was centrifuged for 10 minutes at 14,000g at 4OC. The supernatant (ie, the nuclear
fraction) was collected. Protein concentration was measured using the Pierce BCA Protein Kit
(Thermo Scientific, Ottawa, ON, Canada). Protein amount was normalized and prepared for further
analysis using Western blotting [for phospho-PPAR-γ, PPAR-γ, α-tubulin (cytoplasmic protein) and
Lamin B (nuclear protein)].
2.2.10. Statistical analysis
Experiments were performed in technical duplicates of at least three biological replicates.
Data are represented as mean ± standard error of the mean. Student’s t-test was used to compare
drug treatments to corresponding vehicle controls. One-way ANOVA and Bonferroni's Multiple
Comparison Test were used to compare between treatment groups. Data in treatment groups were
normalized relative to corresponding vehicle controls. All statistical calculations were performed
using GraphPad Prism 5.2 software. P values <0.05 were considered significant.

47
RESULTS
Chapter 3:

48
3.1. Placental gene expression in Gcm-1 heterozygous mice
To study the effect of Gcm-1 downregulation on the expression levels of Ppar-γ and Hmox-1,
we utilized the Gcm-1 heterozygous CD1 mouse model. Labyrinth regions of wildtype and
heterozygous placentas were collected at days E13.5 and E17.5 corresponding to mid- and late
gestation, respectively. To dissect the connection between Ppar-γ, Hmox-1 and Gcm-1, mRNA levels
of Ppar-γ, Hmox-1, Hmox-2 and Gcm-1 were assessed using qRT-PCR; expression of these genes in
heterozygous placentas was normalized to wildtype placental expression (set as 1). Firstly, levels of
Gcm-1 were compared between heterozygous and wildtype placentas. Then, Hmox-1 expression
was studied to determine whether a decrease in Gcm-1 had an effect on Hmox-1 expression in the
placenta. Furthermore, levels of Hmox-2 were assessed to study possible compensatory effect in the
event of Hmox-1 expression being altered (as has been described previously [144]) (Figure 20). As
expected, Ppar-γ expression was not altered in heterozygous placentas at E13.5 and E17.5 despite a
50% downregulation of Gcm-1 expression in these placentas (p<0.0001, n=6). Contrary to our
expectations, levels of Hmox-1 and Hmox-2 also did not differ between wildtype and heterozygous
placentas at E13.5 and E17.5. Our findings suggest that, in the mouse placenta, Gcm-1 does not
regulate Hmox-1 or Ppar-γ levels.
Figure 20: Placental Hmox-1, Hmox-2 or Ppar-γ expression is unaltered in Gcm-1+/- mice. Placentas from Gcm-1 +/- mice were tested for their expression of Hmox-1, Hmox-2 and Ppar-γ. Relative mRNA levels of genes of interest were measured at E13.5 (A) and E17.5 (B) using qRT-PCR. All values are compared to corresponding wildtype (WT) pups from the same mother. Values represented as mean ± SEM; ****p<0.0001 (n=6).

49
3.2. GCM-1 silencing does not affect HO-1 and PPAR-γ expression in the BeWo
cell model
The human choriocarcinoma cell line BeWo was used as an in vitro system for studying how
GCM-1 downregulation influences expression of PPAR-γ and HO-1, based on the finding that BeWo
cells express all three genes (see Figure 12). mRNA expression was measured following 48 hours of
silencing and/or treatment (Figure 21). Using a combination of two siRNA sequences (815+201),
GCM-1 expression was downregulated by 62±0.1% compared to non-silencing (NS) control, set as 1
(p≤0.05, n=3) (Figure 21A). Treatment with forskolin induced GCM-1 expression 1.8±0.3-fold in NS-
transfected cells (p≤0.05, n=4); when the drug was combined with GCM-1-targeting siRNA, the
levels of GCM-1 did not differ compared to NS. Expression of HO-1 did not change with any of the
treatments (Figure 21B). PPAR-γ expression showed a mild (~22%) downregulation following
siRNA treatment, but this did not reach statistical significance. Addition of forskolin decreased
PPAR-γ levels by 46±10.0% (p≤0.05, n=3; Figure 21C). Confirming our findings from the Gcm-1
heterozygous mouse model, we did not see a GCM-1-dependent HO-1 expression mechanism in the
BeWo cell line.
NS siRNA NS+Forsk siRNA+Forsk0.0
0.5
1.0
1.5
2.0
2.5 ***
Treatment
GC
M-1
expre
ssio
n
(norm
aliz
ed to N
S c
ontr
ol)
*
*
NS siRNA NS+Forsk siRNA+Forsk0.0
0.5
1.0
1.5
Treatment
HO
-1 e
xpre
ssio
n
(norm
aliz
ed to N
S c
ontr
ol)
NS siRNA NS+Forsk siRNA+Forsk0.0
0.5
1.0
1.5
Treatment
PP
AR
- expre
ssio
n
(norm
aliz
ed to N
S c
ontr
ol)
*
Figure 21: Downregulation of GCM-1 in BeWo cells has no effect on HO-1 and PPAR-γ levels. BeWo cells were treated with siRNA against human GCM-1, non-silencing control, and forskolin for 48 hours. GCM-1 (A), HO-1 (B) and PPAR-γ (C) mRNA levels were measured and compared to NS control (set as 1, red line). Values represented as mean ± SEM, n=3-4; *p≤0.05 vs NS control; ***p≤0.001. NS, non-silencing; Forsk, forskolin.
A B
C

50
3.3. Time- and dose- responses to drug treatments in BeWo cells
The effects of rosiglitazone (PPAR-γ agonist), T0070907 (PPAR-γ antagonist) and forskolin
(cAMP inducer), either alone or in combinations, were tested for their efficacy and toxicity to BeWo
cells over time. Toxicity results are shown in Figure 14. Gene expression profiles for GCM-1, PPAR-γ
and HO-1 at 3, 6 and 24 hours of treatment are shown in Figures 22-24. Concentrations tested were
chosen either based on previously published work or our initial experiments. The following
concentrations were used: for rosiglitazone, 10µM and 100µM; for T0070907, 0.1µM, 1µM and
10µM; and for forskolin, 20µM [57]. Based on our findings, for subsequent experiments,
rosiglitazone and T0070907 were primarily used at 10µM and 1µM, respectively.
3.3.1. Expression of HO-1
HO-1 mRNA expression in response to PPAR-γ activity-modulating drugs was assessed at 3,
6 and 24 hours post-treatment and compared to vehicle control (set as 1; Figure 22 A-C). Lower
concentration of rosiglitazone induced HO-1 expression by 2.4±0.2, 2.6±0.1 and 2.7±0.1-fold at 3, 6
and 24 hours, respectively (p≤0.05, n=3-4). Analogous findings were obtained following treatment
with the higher dose, where HO-1 was induced more than 2-fold at all three time points studied
(p≤0.05, n=3-4). Activation of HO-1 expression with rosiglitazone was a robust and maintained
event, happening as early as 3 hours and persisting until 24 hours. All concentrations of T0070907
(0.1µM, 1µM, 10µM) significantly blocked HO-1 expression as early as 3 hours of culture (down to
59±2.8%, 66±9.3% and 65±4.4%, from lowest to highest dose) and decreased HO-1 expression by
68±3.9%, 67±2.7% and 34±6.9% (lowest to highest dose) by 24 hours (p≤0.05). By 24 hours, all
treatments of T0070907 were able to outcompete the activation of PPAR-γ induced by
rosiglitazone; however, 1µM concentration was the most effective dose decreasing HO-1 expression
by 62±0.6% (vs vehicle) at 24 hours (p≤0.05). Forskolin blocked the expression of HO-1 at 3 and 6
hours by 40±4.6% and 68±3.5%, respectively (p≤0.05), but this effect diminished by 24 hours of
treatment. Additive effects on HO-1 expression were seen at 24 hours when forskolin was combined
with T0070907 or rosiglitazone, where gene expression was further downregulated by 60±4.3% or
upregulated by 48±13.0%, respectively (p≤0.05).

51
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3
*
*
* * * * **
3hrs
Rela
tive
HO
1m
RN
A
expre
ssio
n le
vels
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3*
*
* **
**
6hrs
Rela
tive
HO
1m
RN
A
expre
ssio
n le
vels
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3*
*
* ** *
*
*
*
*
24hrs
Rela
tive
HO
1m
RN
A
expre
ssio
n le
vels
Figure 22: Dose-dependent expression of HO-1 in BeWo cells over time. Time- and concentration-course experiments were performed to study expression of HO-1 at 3 (A), 6 (B) and 24 (C) hours post-treatment. All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; *p≤0.05 vs vehicle control (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.
3.3.2. Expression of PPAR-γ
PPAR-γ expression in response to drug treatments was assessed at 3, 6 and 24 hours of
treatment and compared to vehicle control (Figure 23 A-C). Although changes at 3 hours of
treatment were less pronounced, by 6 and 24 hours, responses to agonist and antagonist
treatments were significantly different when compared to vehicle control. Following activation of
PPAR-γ with rosiglitazone (10µM), PPAR-γ expression decreased to 47±3.4% by 24 hours (p≤0.05,
n=4). Conversely, blocking PPAR-γ activity with T0070907 (1µM) resulted in a significant
upregulation of its expression by 24 hours (2.0±0.1-fold, p≤0.05, n=4). Forskolin alone did not have
a significant effect on PPAR-γ expression at 24 hours, while forskolin with T0070907 increased
gene expression 1.9±0.1-fold and addition of rosiglitazone significantly decreased expression by
60±4.1% (p≤0.05, n=4).
A B
C

52
Vehicle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0.0
0.5
1.0
1.5
2.0
2.5 3hrs
Rela
tive
PP
AR
- m
RN
A
expre
ssio
n le
vels
Vehicle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0.0
0.5
1.0
1.5
2.0
2.5 6hrs
* *
*
**
** *
*
Rela
tive
PP
AR
- m
RN
A
expre
ssio
n le
vels
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0.0
0.5
1.0
1.5
2.0
2.5
* *
* **
* **
*
24hrs
Rela
tive
PP
AR
- m
RN
A
expre
ssio
n le
vels
Figure 23: Dose-dependent expression of PPAR-γ in BeWo cells over time. Time- and concentration-course experiments were performed to study expression of PPAR-γ at 3 (A), 6 (B) and 24 (C) hours post-treatment. All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; *p≤0.05 vs vehicle control (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.
3.3.3. Expression of GCM-1
Lastly, the effect of PPAR-γ activity modulation on GCM-1 expression levels was tested at 3,
6 and 24 hours (Figure 24 A-C). It has been previously described that Ppar-γ regulates Gcm-1
expression in mouse trophoblast stem cells [101]. Therefore, we studied GCM-1 response to
rosiglitazone and T0070907 treatments at different time points. Activation of PPAR-γ with the
agonist (at 10µM concentration) led to a transient and weak induction of GCM-1 expression, evident
only at 3 hours of treatment (1.5±0.1-fold, p≤0.05, n=4). Blocking PPAR-γ activity with T0070907
(1µM) produced a more robust and prolonged reduction of GCM-1 mRNA expression which
persisted towards 24 hours and led to a 60±5.4% decrease (p≤0.05). Furthermore, when both
rosiglitazone and T0070907 were combined, there was a 34±8.2% reduction in GCM-1 mRNA
expression at 24 hours vs the vehicle (p≤0.05). As expected, forskolin alone significantly
A B
C

53
upregulated GCM-1 expression in BeWo cells as early as 3 hours of treatment (2.9±0.2-fold increase,
p≤0.05); this effect was also evident at 6 hours (2.3±0.1-fold rise, p≤0.05) and 24 hours (2.9±0.4-
fold change, p≤0.05).
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3
4
*
* *
**
*
3hrs
Rela
tive
GC
M-1
mR
NA
expre
ssio
n le
vels
Vehicle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3
4 6hrs
* * *
*
*
*
Rela
tive
GC
M-1
mR
NA
expre
ssio
n le
vels
Vehicle M
Ro1
0M
Ro1
00M
T0.1
MT1
M
T10M
M+T
0.1
Ro1
0
M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
M
M+T
1
For20
M
M+R
o100
For20
0
1
2
3
4
* * *
*
24hrs
**
Rela
tive
GC
M-1
mR
NA
expre
ssio
n le
vels
Figure 24: Dose-dependent expression of GCM-1 in BeWo cells over time. Time- and concentration-course experiments were performed to study expression of GCM-1at 3 (A), 6 (B) and 24 (C) hours post-treatment. All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; *p≤0.05 vs vehicle control (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.
3.4. Effect of PPAR-γ activity-modulating drugs on HO-1 expression in BeWo
cells
The effect of manipulating PPAR-γ activity on HO-1 expression was assessed. First, the
expression of HO-1 was tested following 3, 6 and 24 hours of treatment with the stimulators and
inhibitors at optimal concentrations. Second, HO-1 protein expression in BeWo cell lysates was
assessed using Western blotting under the same conditions. Lastly, HO-1 protein release from
BeWo cells was studied using ELISA.
A B
C

54
3.4.1. PPAR-γ activation induces a rapid rise in HO-1 RNA levels
Using rosiglitazone as a stimulator and T0070907 as an inhibitor of PPAR-γ activity, we
tested the response of HO-1 to PPAR-γ activity-modulating drugs at the mRNA level. HO-1 mRNA
responses to drugs at their optimal concentrations at 3, 6 and 24 hours are compiled in Figure 25
(results are described in detail in section 3.3.1). Briefly, PPAR-γ stimulation induced HO-1
expression in BeWo cells as has been described in other systems [114]. This response was robust
and prolonged, as it was maintained at 24 hours of treatment. T0070907 decreased gene
expression on its own, as well as outcompeted rosiglitazone when both drugs were co-administered
at 3, 6 and 24 hours (p≤0.001 vs rosiglitazone alone). Optimal drug concentrations, selected based
on mRNA studies, were used in subsequent protein analyses, namely, cellular HO-1 protein
expression and HO-1 release.
Rosi(10M) T007 (1M) Rosi+T007 Forskolin 0
1
2
3
3hrs
6hrs
24hrs
******
***
##
#
#
# # #
#
#
Re
lati
veH
O-1
mR
NA
exp
ressio
n l
eve
ls
Figure 25: HO-1 mRNA expression levels following modulation of PPAR-γ activity. Compiled HO-1 expression levels at optimal drug concentrations overtime are shown. All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; #p≤0.05 vs vehicle control; ***p≤0.001 (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.
3.4.2. Intracellular HO-1 protein expression increases following PPAR-γ activation
To validate our mRNA findings, we assessed intracellular HO-1 protein expression at 24 and
48 hours of treatment using Western blotting (Figure 26 A,B). Consistent with gene expression
results, HO-1 protein levels increased significantly following rosiglitazone treatment at 24 (Figure
26 A) and 48 (Figure 26 B) hours. At 24 hours, lower dose of rosiglitazone upregulated HO-1
expression by 54±14.8% (p≤0.05, n=4), while co-administration of T0070907 decreased HO-1

55
protein levels by 40±5.5% compared to baseline (p≤0.001 vs rosiglitazone alone). Higher agonist
dose also upregulated HO-1 expression by 69±20.7% (p≤0.05). Conversely, inhibition of PPAR-γ
activity (at 1µM dose of T0070907) led to a downregulation of HO-1 protein expression by
83±16.8% (p≤0.05). Forskolin treatment decreased HO-1 expression by 38±13.1%, however, this
did not reach significance (p=0.1011).
At 48 hours of treatment, analogous results were attained. Lower and higher rosiglitazone
concentrations increased HO-1 expression by 49±25.2% (p=0.1926) and 86±24.6% (p≤0.05, n=4),
respectively. T0070907 (1µM) decreased protein levels by 83±16.2% (p≤0.05); and the
combination of rosiglitazone and T0070907 was significantly different from antagonist treatment
alone (p≤0.01). Although HO-1 expression decreased following forskolin treatment at 24 hours, this
effect was diminished by 48 hours.
Veh
icle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0.0
0.5
1.0
1.5
2.0
2.5
***
Treatment
24 hours
Cellu
lar
HO
-1 e
xpre
ssio
n
(rela
tive to v
ehic
le) *
*
** *
Veh
icle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0.0
0.5
1.0
1.5
2.0
2.5
**
Treatment
48 hours
Cellu
lar
HO
-1 e
xpre
ssio
n
(rela
tive to v
ehic
le)
*
**
Figure 26: Expression of HO-1 protein in BeWo cells. BeWo cells were treated for 24 (A) and 48 (B) hours. HO-1 protein levels were assessed using Western blotting and normalized to α-tubulin; each treatment was expressed as fold-change relative to its vehicle control (set as 1, red dashed line). Representative Western blots for expression at 24 (C) and 48 (D) hours are shown. Values are represented as mean ± SEM; ***p≤0.001; **p≤0.01; *p≤0.05 vs vehicle control (n=4). Ro, rosiglitazone; T, T0070907; For, forskolin.
A B
C D

56
3.4.3. HO-1 release from BeWo cells increases with PPAR-γ activation
Based on previous work in our laboratory, HO-1 is released into the medium from placental
explants (unpublished observations). We tested whether this observation holds true in BeWo cells.
BeWo cell conditioned medium was collected following 24 and 48 hours of treatment with PPAR-γ
activity-modulating drugs and HO-1 protein content was measured by ELISA (Figure 27 A,B). By 48
hours of rosiglitazone exposure, HO-1 release from BeWo cells into the media was significantly
upregulated by 57±24.8% and 88±26.7% corresponding to lower and higher drug concentrations,
respectively (p≤0.05, n=4; Figure 27B). As expected, HO-1 release was decreased by 34±6.7%
following T0070907 treatment (1µM, p≤0.05). Furthermore, the presence of T0070907
significantly blocked the induction associated with rosiglitazone (p≤0.05 vs rosiglitazone alone) by
48 hours. Consistent with mRNA and cellular protein expression profiles, forskolin inhibited HO-1
release from BeWo cells at 48 hours (down by 39±7.4%, p≤0.05). This effect was exacerbated with
the addition of T0070907 to forskolin treatment (45±13.5% reduction, p≤0.05). Rosiglitazone, in
combination with forskolin, led to a significantly higher HO-1 release when compared to forskolin
alone (p≤0.01).
Vehicle M
Ro1
0M
Ro1
00M
T1M
M+T
1
Ro1
0
M
For20
M
For+T
1M
For+R
o100
0.0
0.5
1.0
1.5
2.0
2.5
24 hours
Treatment
HO
-1 r
ele
ase
(rela
tive to v
ehic
le)
#
##
Vehicle M
Ro1
0M
Ro1
00M
T1M
M+T
1
Ro1
0
M
For20
M
For+T
1M
For+R
o100
0.0
0.5
1.0
1.5
2.0
2.5 ***
48 hours
Treatment
HO
-1 r
ele
ase
(rela
tive to v
ehic
le)
#
#
# # # #
#
Figure 27: HO-1 release from BeWo cells. HO-1 release into culture media was assessed at 24 (A) and 48 (B) hours of treatment. HO-1 protein release was normalized to total protein content in conditioned media. Each drug treatment was compared to its respective vehicle control (set as 1, red dashed line). Values are represented as mean ± SEM; **p≤0.01; *p≤0.05; #p≤0.05 vs vehicle control (n=4). Ro, rosiglitazone; T, T0070907; For, forskolin.
A B

57
3.5. PPAR-γ participates in a negative auto-regulatory feedback mechanism
Based on our time- and dose-response experiments, we observed that PPAR-γ participates
in a negative auto-regulatory feedback, such that induction of its activity with rosiglitazone resulted
in decreased expression, and blocking receptor activity led to increased receptor levels. To study
this further, we assessed PPAR-γ mRNA expression and cellular PPAR-γ protein expression,
receptor phosphorylation and localization.
3.5.1. PPAR-γ expression is inversely related to PPAR-γ activity
The expression of PPAR-γ was studied at 3, 6 and 24 hours following drug treatment; levels
at optimized drug concentrations are shown in Figure 28. Results are also summarized in section
3.3.2. Briefly, induction of PPAR-γ activity resulted in a decrease of its expression, while treatment
with T0070907 had the opposite effect, with most pronounced changes observed 24 hours after
treatment. Co-administration of T0070907 with rosiglitazone significantly ameliorated
rosiglitazone-induced PPAR-γ downregulation at 6 (p≤0.01) and 24 (p≤0.001) hours of treatment
(vs rosiglitazone alone).
Rosi(10M) T007 (1M) Rosi+T007 Forskolin 0.0
0.5
1.0
1.5
2.0
2.5
3hrs
6hrs
24hrs
**
***
*
# #
#
#
#
#
Re
lati
veP
PA
R-
mR
NA
exp
ressio
n l
eve
ls
Figure 28: PPAR-γ mRNA expression levels following modulation of PPAR-γ activity. Compiled PPAR-γ expression levels at optimal drug concentrations are shown overtime (3, 6, 24 hours). All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; #p≤0.05 vs vehicle control; ***p≤0.001; **p≤0.01; *p≤0.05 (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.

58
3.5.2. PPAR-γ protein levels correlate with gene expression profiles
To confirm our gene expression findings, we examined the cellular PPAR-γ protein
expression at 24 and 48 hours following treatment (Figure 29 A,B). Total PPAR-γ protein levels
were decreased by 58±5.3% and 66±9.8% at 24 and 48 hours, respectively, by rosiglitazone (10µM)
treatment (p≤0.05, n=4). PPAR-γ expression was increased following treatment with T0070907
(1µM) 2.1±0.4-fold (p=0.0759) and 1.8±0.2-fold (p≤0.05) at 24 and 48 hours, respectively. Co-
administration of the inhibitor with rosiglitazone significantly induced PPAR-γ expression at 24
hours (p≤0.01 vs rosiglitazone alone). PPAR-γ expression decreased by 30±9.2% following a 24-
hour treatment with forskolin (p≤0.05). By 48 hours, effect of rosiglitazone was more pronounced
when combined with T0070907, resulting in decreased PPAR-γ expression (p≤0.001 vs T0070907
alone).
Vehicle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0
1
2
3
4
****
24 hours
Treatment
Ce
llu
lar
PP
AR
- e
xp
ressio
n(r
ela
tive to v
ehic
le)
* **
Vehicle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0
1
2
5
6
7
8 ***
48 hours
Treatment
Ce
llu
lar
PP
AR
- e
xp
ressio
n(r
ela
tive to v
ehic
le)
**
*
*
**
Figure 29: Expression of PPAR-γ protein in BeWo cells. PPAR-γ protein levels were assessed 24 (A) and 48 (B) hours using Western blotting and normalized to α-tubulin; each treatment was further normalized to its representative vehicle control (set as 1, red dashed line). Representative Western blots for expression at 24 (C) and 48 hours (D) are shown. Values are represented as mean ± SEM; ***p≤0.001; **p≤0.01; *p≤0.05 vs vehicle control (n=4). Ro, rosiglitazone; T, T0070907; For, forskolin.
A B
C D

59
3.5.3. Phosphorylation of PPAR-γ protein is increased following rosiglitazone treatment
To further study the inverse relationship between PPAR-γ expression and activity, we
looked at phosphorylation of the PPAR-γ protein (Figure 30 A,B). Levels of phosphorylated PPAR-γ
were compared to total cellular PPAR-γ protein levels at 24 and 48 hours; the effects were more
pronounced at the later time point (Figure 30B). By 48 hours of treatment, both lower and higher
doses of rosiglitazone led to a rise of PPAR-γ phosphorylation by 2.3±0.9-fold (p=0.2772) and
4.5±0.1-fold (p≤0.05), respectively (n=4). Inhibition of PPAR-γ activity with T0070907 (1µM)
resulted in a decrease of receptor phosphorylation at 48 hours by 17±1.5% (p≤0.05). By 48 hours
of treatment, forskolin also decreased PPAR-γ phosphorylation levels by 39±5.6% (p≤0.05).
Veh
icle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0
2
4
6
24 hours
*
*
Treatment
Ph
osp
ho
-PP
AR
- p
rote
in e
xp
ressio
n
(norm
aliz
ed to tota
l PP
AR
- e
xpre
ssio
n)
Veh
icle M
Ro1
0M
Ro1
00M
T1M
T10M
M+T
1
Ro1
0
M
M+T
10
Ro1
0
M
For20
0
2
4
6 **
48 hours
*
*
* * *
Treatment
Ph
os
ph
o-P
PA
R-
pro
tein
exp
ressio
n
(norm
aliz
ed to tota
l PP
AR
-
expre
ssio
n)
Figure 30: Expression of phosphorylated PPAR-γ protein in BeWo cells. Phospho-PPAR-γ (Ph-PPAR-γ) protein levels were assessed at 24 (A) and 48 (B) hours using Western blotting and normalized to total PPAR-γ protein levels. Each treatment was further represented as fold change relative to vehicle control (set as 1, red dashed line). Representative Western blots for expression at 24 (C) and 48 hours (D) are shown. Values are represented as mean ± SEM; ***p≤0.001; **p≤0.01; *p≤0.05 vs vehicle control (n=4). Ro, rosiglitazone; T, T0070907; For, forskolin.
A B
C D

60
3.5.4. Fluorescent immunohistochemistry analysis of PPAR-γ localization
PPAR-γ cellular localization and relative expression was assessed using fluorescent
immunohistochemistry at 3, 6 and 24 hours of treatment with rosiglitazone (10µM), T0070907
(1µM) or vehicle (Figure 31). Our studies showed that PPAR-γ localized to the nucleus, with some
expression seen in the cytoplasm. Concurrent with our PPAR-γ protein analysis using Western
blotting, we saw increased expression of PPAR-γ after T0070907 treatment and a decrease in
staining levels after rosiglitazone treatment. This trend persisted and became even more prominent
at 48 hours of treatment (data not shown).
Figure 31: Effect of PPAR-γ-modulating drugs on its localization in BeWo cells. PPAR-γ expression was visualized at 3 (top), 6 (middle) and 24 (bottom) hours following treatment with vehicle, rosiglitazone or T0070907. PPAR-γ shown in green, e-cadherin (cell surface marker) in red, DAPI (nuclear marker) in blue (630X magnification).

61
3.5.5. Nuclear and cytoplasmic (phospho-) PPAR-γ expression
Cellular fractionation analysis was used to study potential changes in PPAR-γ protein
localization at 1, 6 and 24 hours of treatment (Figure 32 A,B). Overall, expression of PPAR-γ was
stronger in the nucleus compared to the cytoplasm as was expected based on our fluorescent
studies. Within the nucleus, there was a trend towards a lower PPAR-γ protein expression with
rosiglitazone treatment: a 55±13.3% decrease at 6 hours post-treatment (p≤0.05, n=4) and a
30±18.1% decrease following 24 hours (p=0.1). By contrast, T0070907 treatment led to a
significant increase in nuclear PPAR-γ expression after 1 hour of treatment (2.3±0.6-fold, p≤0.05,
n=4); although the trend persisted, the results were not significant at 6 (2.6±0.9-fold increase,
p=0.1487) and 24 (1.8±0.5-fold induction, p=0.2309) hours. Combination of both chemicals did not
alter nuclear PPAR-γ localization at either time point.
Cytoplasmic PPAR-γ expression did not show pronounced changes (Figure 32B). Most of the
treatments did not show significant results at 1, 6 and 24 hours (possibly because of n=3). There
was a trend towards a lower PPAR-γ expression under rosiglitazone treatment at 6 hours (34±6.3%
decrease, p≤0.05, n=3) and 24 hours (28±35.2% downregulation, p=0.5166). T0070907 results
were not as pronounced in the cytoplasm as they were in the nucleus; there was no change in
PPAR-γ expression at 1, 6 and 24 hours.
1hr 6hrs 24hrs 0
1
2
3
4
#
*
#
Time
Rela
tive n
ucle
ar
PPA
R- e
xpre
ssio
n
(com
pare
d to v
ehic
le)
1hr 6hrs 24hrs 0
1
2
3
4
Vehicle
Rosi(10M)
T007 (1M)
Rosi+T007
##
Time
Rela
tive c
yto
pla
sm
ic P
PA
R-
expre
ssio
n
(com
pare
d to v
ehic
le)
Figure 32: Cellular fractionation analysis of PPAR-γ expression in BeWo cells. Nuclear (A) and cytoplasmic (B) PPAR-γ protein expression was assessed at 1, 6 and 24 hours of treatment using Western blotting; nuclear expression was normalized to lamin B; cytoplasmic expression normalized to α-tubulin. Each treatment was further normalized to DMSO (vehicle, set as 1, red dashed line). Representative Western blots for nuclear (C) and cytoplasmic (D) expressions are shown. Values are represented as mean ± SEM; *p≤0.05; #p≤0.05 vs vehicle control (n=4). Rosi, rosiglitazone; T007, T0070907.
A B
C D

62
Lastly, levels of nuclear phosphorylated PPAR-γ were assessed at 1 and 24 hours of
treatment (Figure 33). No significant changes were found in phosphorylated PPAR-γ protein
expression at either time point.
1hr 24hrs 0.0
0.5
1.0
1.5
Vehicle
Rosi(10M)
T007 (1M)
Rosi+T007
Time
Nucle
ar
Phospho-P
PA
R-
/PP
AR
- e
xpre
ssio
n
(com
pare
d to v
ehic
le)
Figure 33: Nuclear phosphorylated PPAR-γ expression in BeWo cells. Nuclear phosphorylated PPAR-γ (phospho-PPAR-γ) protein expression was assessed at 1 and 24 hours of treatment and normalized to total nuclear PPAR-γ expression using Western blotting. Each treatment was normalized to vehicle (set as 1, red dashed line). Values are represented as mean ± SEM (n=4). Rosi, rosiglitazone; T007, T0070907.

63
3.6. Role of PPAR-γ in proliferation/differentiation balance
The BeWo cell model was used to study the effect of pharmacological PPAR-γ activity
modulation on the proliferation/differentiation balance, an important physiologic process within
the trophoblast layer [57]. We assessed these events by studying markers of syncytial
differentiation (such as GCM-1 expression and free β-hCG release), visualizing cell fusion and
measuring BeWo cell proliferation.
3.6.1. PPAR-γ-mediated induction of GCM-1 expression is transient
GCM-1 mRNA expression levels were assessed at 3, 6 and 24 hours following treatment;
mRNA responses at optimal drug concentrations are summarized in Figure 34 and discussed in
detail in section 3.3.4. Briefly, forskolin was used as a positive control to show that GCM-1 induction
was possible in the BeWo cell model. Treatment with rosiglitazone did not have a pronounced
effect on GCM-1 expression except at 3 hours of culture. Conversely, blocking PPAR-γ activity with
T0070907 led to a downregulation of GCM-1 expression which persisted towards 24 hours of
treatment.
Rosi(10M) T007 (1M) Rosi+T007 Forskolin 0
1
2
3
4
3hrs
6hrs
24hrs
****
#
# ##
#
#
#
#
Rela
tive
GC
M-1
mR
NA
exp
ressio
n l
eve
ls
Figure 34: GCM-1 mRNA expression levels following modulation of PPAR-γ activity. Compiled GCM-1 expression levels at optimal drug concentrations are shown overtime (3, 6, 24 hours). All treatments are compared to their respective vehicle controls (set as 1, red dashed line). Values are represented as mean ± SEM; #p≤0.05 vs vehicle control; **p≤0.01; *p≤0.05 (n=3-4). Ro, rosiglitazone; T, T0070907; For, forskolin.

64
3.6.2. PPAR-γ activity in BeWo cells
In our mRNA expression experiments, we observed that although it was possible to block
the activity of PPAR-γ and, consequently, decrease the expression of downstream targets, it was
considerably more difficult to induce its activity and, thus, upregulate the expression of its target
genes, particularly GCM-1. Thus, because of our inability to induce GCM-1 expression over a
prolonged time in BeWo cells, we decided to study the transcriptional activity of PPAR-γ using the
luciferase reporter assay (Figure 32 A,B). We identified two PPREs in the human GCM-1 promoter;
these sequences were cloned into plasmids and transfected into BeWo cells (see Figure 17). PPAR-γ
activity was studied at 24 hours following treatment. Relative promoter activity upon binding to
sequence 1 and sequence 2 are shown in Figures 35A and 35B, respectively.
Luciferase activity following its transcription under the control of binding sequence 1 was
increased by 32±12.7% following treatment with rosiglitazone at 10µM, however, this failed to
reach statistical significance (p=0.1274, n=4; Figure 35A). Higher dose of rosiglitazone (100µM)
increased luciferase transcription levels by 46±11.8% (p≤0.05, n=4). Sequence 1 did not show a
response to T0070907 alone; however, in combination with rosiglitazone (100µM), T0070907
significantly blocked the effect of rosiglitazone (p≤0.01 vs rosiglitazone alone).
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
M
T0.5
M
M+T
0.5
Ro1
00
0.0
0.5
1.0
1.5
2.0
*
**
Binding sequence 1
Treatment
Re
lative
pro
mo
ter
activity
(no
rma
lize
d t
o v
eh
icle
)
Veh
icle M
Ro1
0M
Ro1
00M
T0.1
M
T0.5
M
M+T
0.5
Ro1
00
0.0
0.5
1.0
1.5
2.0
***
Binding sequence 2
Treatment
Re
lative
pro
mo
ter
activity
(no
rma
lize
d t
o v
eh
icle
)
*
Figure 35: PPAR-γ activity in BeWo cells. PPAR-γ activity in BeWo cells was assessed using the luciferase reporter assay. Two sequences identified as PPAR-γ binding sites in the GCM-1 promoter were used to test the activity of PPAR-γ in response following 24 hours post-treatment. PPAR-γ transcription of sequence 1 (A) and sequence 2 (B) following drug treatments are shown. Treatments are compared to vehicle (set as 1, red dashed line). Values are represented as mean ± SEM; ***p≤0.001; **p≤0.01; *p≤0.05 vs vehicle control (n=3-4). Ro, rosiglitazone; T, T0070907.
A B

65
Luciferase activity under the control of sequence 2 was quite different from that observed
under sequence 1 (Figure 35B). Here, rosiglitazone treatment did not have an effect on PPAR-γ
activity, but T0070907 treatment led to a 38±3.6% reduction in transcription of the reporter gene
(p≤0.05, n=4). Interestingly, a combination of rosiglitazone and T0070907 significantly increased
receptor activity when compared to T0070907 alone (p≤0.001) indicating that rosiglitazone was
still able to exert its effects on transcription.
3.6.3. Effect of PPAR-γ activity modulation on free β-hCG release
To further study the role of PPAR-γ on the maintenance of proliferation/differentiation
balance, we assessed differentiation of BeWo cells by using free β-hCG release as a marker (Figure
36). In our experiments, forskolin was used as a positive control for cell differentiation since it is
known to upregulate free β-hCG secretion. We saw a 20.9±2.8-fold induction in β-hCG release
following forskolin treatment at 48 hours (p≤0.05, n=7). Lower dose of rosiglitazone (10µM) did
not affect free β-hCG release, while higher concentration of the drug showed a trend toward an
increase in β-hCG release (34±20.4% increase, p=0.1914, n=4). On the contrary, blocking PPAR-γ
activity with T0070907 significantly downregulated β-hCG secretion by 41±7.3% (p≤0.05, n=7). Co-
administration of both the inhibitor and the activator resulted in no change of β-hCG protein
release.
Veh
icle M
Ro1
0M
Ro1
00M
T1M
M+T
1
Ro1
0
M
For20
0.0
0.5
1.0
1.5
2.0
15
20
25
#
*
#
Treatment
Fre
e-h
CG
secre
tion
(rela
tive t
o v
eh
icle
con
trol)
Figure 36: Effect of PPAR-γ manipulation on free β-hCG release in BeWo cells. β-hCG release was measured at 48 hours post-treatment. β-hCG levels were normalized to total protein content in the media. Each drug treatment was compared to its respective vehicle control (set as 1, red dashed line). Values are represented as mean ± SEM *p≤0.05; #p≤0.05 vs vehicle control (n=4-7). Ro, rosiglitazone; T, T0070907; For, forskolin.

66
3.6.4. Visualization of BeWo cell fusion using fluorescent immunohistochemistry
To visualize cell fusion in BeWo cells, we used E-cadherin as the cell surface marker (Figure
37). Loss of membrane integrity, seen as pigmented E-cadherin staining, and a rise in aggregation of
nuclei was observed following forskolin treatment (positive control) at 48 hours of treatment
(Figure 37B). Compared to vehicle (Figure 37A), rosiglitazone treatment did not appear to induce
cell fusion (Figure 37C). As expected, T0070907 did not increase cell fusion either (Figure 37D);
however, it appeared that BeWo cell numbers were altered under this treatment (seen as a high
incidence of condensed chromatin in diving cells).
Figure 37: Effect of PPAR-γ modulation on BeWo cell fusion. Cell fusion was assessed at 48 hours post-treatment. Cells were treated with forskolin (B) as a positive cell-fusion control, rosiglitazone (C), and T0070907 (D) and compared to vehicle control (A). E-cadherin (red) was used as a cell surface marker; DAPI (blue) was used as the nuclear stain (200X magnification).

67
3.6.5. Effect of PPAR-γ activity on BeWo cell proliferation
The role of PPAR-γ on BeWo cell number was assessed at 48 hours using the CellTiter-Fluo
Cell Viability Assay (Figure 38). Forskolin, because of its effect on cell differentiation, was expected
to decrease cell proliferation [57]. We found that following 48 hours of treatment, forskolin
decreased BeWo cell numbers by 16±1.4% (p≤0.05, n=4). Confirming our initial observations from
fluorescent immunohistochemistry studies (see section 3.6.4 above), treatment of BeWo cells with
T0070907 significantly induced cell proliferation by 39±12.8% when compared to vehicle control
(p≤0.05). Rosiglitazone did not have an effect on BeWo cell number.
Veh
icle M
Ro1
0M
Ro1
00M
T1M
M+T1
Ro1
0
M
For20
0.0
0.5
1.0
1.5
2.0
Treatment
Rela
tive
cell
pro
lifera
tion
(no
rma
lize
d t
o v
eh
icle
co
ntr
ol)
*
*
Figure 38: Effect of PPAR-γ activity modulation on BeWo cell proliferation. BeWo cell numbers were measured using CellTiter-Fluo Cell Viability Assay at 48 hours of treatment. Relative cell number was recorded in each treatment and compared to its respective vehicle control (set as 1, red dashed line). Values are represented as mean ± SEM; *p≤0.05 vs vehicle control (n=4). Ro, rosiglitazone; T, T0070907; For, forskolin.

68
DISCUSSION
Chapter 4:

69
Using the Gcm-1 heterozygous mouse model and the GCM-1-silenced BeWo cell model, we
showed that HO-1 expression is not GCM-1-dependent. Furthermore, we showed that there is no
feedback mechanism between GCM-1 and PPAR-γ. Additionally, we confirmed that PPAR-γ
positively regulates HO-1 expression in the BeWo cell line, as assessed on mRNA and protein
(cellular and conditioned media content) levels. When studying the effects of PPAR-γ activity-
modulating drugs on key events of trophoblast physiology (proliferation and differentiation), we
found that inducing PPAR-γ activity in BeWo cells with rosiglitazone did not alter cell proliferation
and did not have a profound effect on GCM-1 expression and cell differentiation as assessed by free
β-hCG release. Conversely, blocking PPAR-γ activity with T0070907 significantly upregulated cell
proliferation and led to lower GCM-1 levels and decreased β-hCG release. Collectively, we showed
that modulating PPAR-γ activity with an antagonist had a stronger effect on the cell
proliferation/differentiation balance. These findings have important implications for further
studies on the role of PPAR-γ in healthy pregnancy and placental insufficiency syndromes.
Transcription factor GCM-1 does not regulate HO-1 expression
Our initial work aimed to elucidate the relationship between the transcription factor and
differentiation marker GCM-1 and HO-1, an enzyme responsible for heme breakdown within the
cell. We undertook this task using two different models. First, we utilized an animal model where
heterozygous Gcm-1 mouse placentas were subjected to gene analysis. Second, we studied gene
expression following GCM-1 silencing in vitro using the BeWo cell line.
Gcm-1 heterozygous placentas were analyzed at two developmental stages: E13.5
(corresponding to mid gestation) and E17.5 (corresponding to late gestation). Maximum placental
Gcm-1 expression in the mouse is around E14-15 [164, 165], thus, we expected that if a regulatory
mechanism between GCM-1 and HO-1 was present, the differences would be most striking at this
stage. Contrary to our initial hypothesis, no differences in Hmox-1 mRNA expression levels were
seen at E13.5 or E17.5 in Gcm-1 heterozygous placentas when compared to wildtype. Furthermore,
when studying the expression of Hmox-2, another isoform of the heme oxygenase family, we did not
detect differences in gene expression between the two groups. Hmox-2 has been previously shown
to be higher in placentas with Hmox-1 downregulation, possibly as part of a compensatory
mechanism [144]. The fact that its expression is not altered in heterozygous placentas offers
additional evidence for lack of Gcm-1-controlled Hmox-1 regulation. Lastly, we did not see
differences in Ppar-γ mRNA levels, indicating that a decrease in Gcm-1 expression does not affect

70
the expression of its upstream regulator, Ppar-γ. Collectively, our studies show that, in mice, Gcm-1
does not regulate the expression of Ppar-γ, suggesting the lack of a potential regulatory feedback
mechanism between these two transcription factors in the mouse labyrinth.
Acknowledging the possibility that there is a potential differential gene regulation in mice
when compared to that of humans, we assessed the response of HO-1 to GCM-1 silencing in the
human choriocarcinoma cell line, BeWo. A significant downregulation of GCM-1 was accomplished
using a combination of siRNA sequences targeted to the human GCM-1 gene. GCM-1 levels were
downregulated by 62% after 48 hours of silencing; however, we found no differences in expression
levels of our genes of interest, namely, HO-1 and PPAR-γ. Therefore, as we had seen previously in
the mouse model, GCM-1 downregulation did not affect expression levels of HO-1 implying the lack
of transcriptional control of HO-1 by GCM-1. Furthermore, since levels of PPAR-γ remained
unchanged, we concluded that GCM-1 also does not control PPAR-γ. Collectively, our animal and the
BeWo cell models indicate that HO-1 and PPAR-γ are not under transcriptional control of GCM-1.
We acknowledge that based on our Gcm-1 heterozygous mouse model and GCM-1 silencing
experiments in BeWo cells, we cannot eliminate the possibility of GCM-1 controlling HO-1
expression. To definitively conclude that this connection is absent, subsequent studies, such as
chromatin immunoprecipitation (ChIP) or electrophoretic mobility shift assay (EMSA), are
necessary to show that GCM-1 does not bind to promoters of genes such as HO-1 and PPAR-γ.
However, our experiments do strongly support the lack of transcriptional control of HO-1 by GCM-1,
as well as the lack of any feedback mechanisms between GCM-1 and PPAR-γ.
Our subsequent studies focused on pharmacologic manipulation of PPAR-γ and the effect it
had on key features of the trophoblast turnover. We used the BeWo cell model to study how PPAR-γ
activity induction or inhibition influences gene and protein expression, protein localization, cell
proliferation and differentiation.

71
The PPAR-γ/HO-1 molecular axis is conserved and functional in the BeWo cell line
The relationship between HO-1 and PPAR-γ has been studied in several systems. Since the
initial proof that PPAR-γ directly binds to the HMOX-1 promoter in HUVECs and vascular smooth
muscle cells, studies have looked at how these molecules interact in other systems [114].
Considering that the connection between HO-1 and PPAR-γ was shown to be important in cell
migration, we decided to study how this molecular axis behaves in the BeWo cell line [150].
Our experiments indicated that stimulation of PPAR-γ with rosiglitazone significantly
increased HO-1 transcript expression, intra-cellular protein expression and protein release into the
culture medium. HO-1 mRNA induction was a rapid and persistent event where rosiglitazone
showed an effect as early as 3 hours post-treatment. Cellular protein expression was significantly
upregulated at 24 hours of treatment, while HO-1 protein content in the BeWo cell-conditioned
media was elevated at 48 hours of treatment. The time frames for these events support the efficacy
of our findings, such that changes at the mRNA level were followed by alternations of the
intracellular protein expression, which was further followed by changes in protein release.
Conversely, opposite effects on HO-1 expression were seen following T0070907 treatment.
In experiments where both drugs were combined, pre-treatment with T0070907 skewed
gene and protein expression profiles to resemble those consistent with antagonist treatment alone,
implicating that T0070907 is a more potent drug, even when the dose used is ten times lower.
Although both synthetic ligands (rosiglitazone and T0070907) are highly specific for PPAR-γ (and
especially the gamma isoform), the observed effect can be attributed to the ability of T0070907 to
bind irreversibly within the ligand-binding pocket of the receptor.
Surprisingly, when treating cells with forskolin, there was a decrease in HO-1 mRNA and
protein expression, despite the fact that forskolin is known to mildly increase the activity of PPAR-γ
[166], and has also been shown to increase HO-1 expression in smooth muscle cells [167]. These
changes in gene expression studies were performed at 3 and 6 hours of treatment; the effect
diminished by 24 hours of treatment. This explains the lack of HO-1 mRNA response in our GCM-1
silencing experiments on BeWo cells since they were assessed after 48 hours of treatment with
forskolin. Furthermore, this finding has implications for our study of whether and how GCM-1
controls HO-1 expression, considering that forskolin is the primary available inducer of GCM-1
expression. Thus, this observation must be taken into account when stimulating cells with this drug,
as it might override a possible connection between GCM-1 and HO-1.

72
PPAR-γ participates in a negative autoregulatory feedback mechanism
When studying the effect of PPAR-γ activity modulation on its expression, we observed that
this transcription factor is able to participate in a negative auto-regulation feedback mechanism.
We found that a rise in PPAR-γ activity (with treatment of an agonist) was accompanied by a
decrease in its expression, while the opposite was true with the treatment of cells with the
antagonist. Although forskolin slightly and transiently upregulated PPAR-γ mRNA expression, it led
to a modest downregulation of the receptor protein expression.
Since PPAR-γ is an important transcription factor with a wide range of actions, several
mechanisms have evolved to modulate its activity; one such mechanism is phosphorylation
(reviewed in [85]). We studied PPAR-γ phosphorylation at 24 and 48 hours of treatment.
Interestingly, when comparing phosphorylated PPAR-γ (phos-PPAR-γ) levels to total PPAR-γ
protein expression, we found that levels of phos-PPAR-γ are higher in rosiglitazone-treated cells,
while the opposite is seen when treating BeWo cells with the antagonist. These findings allow us to
speculate that this is another part of the feedback mechanism in which PPAR-γ participates.
Whether this happens directly or indirectly is yet to be elucidated, as is the identity of factors which
phosphorylate this protein. Until recently, most studies indicated that PPAR-γ phosphorylation
results in protein inactivation; however, there is a possibility that the opposite occurs, depending
on which kinases phosphorylate the receptor (ex. Cdk7 and 9 phosphorylation of PPAR-γ was
shown to increase receptor activity). Thus, although we cannot definitively state that
phosphorylation under our treatments leads to receptor inactivation, if it does, we can propose it to
be another part of the feedback mechanism aimed at stabilizing the activity of PPAR-γ when the
system is disrupted.
Several points should be addressed regarding our studies of PPAR-γ phosphorylation. First,
we measured phosphorylation of the receptor at 24 and 48 hours. Phosphorylation is a rapid event,
thus, measuring the levels of phosphorylated receptor at earlier time points (such as 1 and 3 hours)
in whole tissue lysates may produce different results. Second, the antibody used to detect
phosphorylated PPAR-γ protein is polyclonal; this might impair its ability to detect only the
phosphorylated isoform of the receptor. Therefore, we cannot conclusively state whether the
phosphorylated PPAR-γ isoform corresponds only to the top band (at 57 kDa) or to both bands
seen on the blot (corresponding to PPAR-γ1 and PPAR-γ2).

73
Our findings of PPAR-γ expression indicate that certain molecular mechanisms in BeWo
cells are in place (and possibly in other systems) to ensure fine-tuning of PPAR-γ activity which has
important implications in cell lipid metabolism, differentiation and immune response. The
induction of activity is compensated for by a decrease in transcription factor expression and a rise
in receptor phosphorylation (and possibly inactivation), while a decrease in its activity is
complimented with a rise in receptor levels and a decrease in protein phosphorylation.
To complete our study of PPAR-γ expression in BeWo cells, we analyzed its localization
using fluorescent IHC and cellular fractionation technique. Using fluorescent IHC, we showed that
PPAR-γ was predominantly localized in the nucleus with low levels found in the cytoplasm. This
finding was expected as PPAR-γ is a transcription factor and, thus, should localize to the nucleus;
since it is a protein, it should be present in the cytoplasm in trace amounts where it has to be
translated.
After performing a series of cellular fractionation analyses, we observed that changes in
PPAR-γ expression were mostly restricted to the nucleus; while cytoplasmic expression
fluctuations were much less prominent (although it should be acknowledged that n of 3 might
contribute to this result). Consistent with our findings from whole cell lysate experiments, PPAR-γ
expression decreased following rosiglitazone, and increased after T0070907, treatment in the
nuclear compartment; these effects were less striking in the cytoplasm. Interestingly, the levels of
nuclear phos-PPAR-γ when compared to total nuclear PPAR-γ expression remain unchanged
following different treatments.
Western blots illustrate that only one isoform of PPAR-γ is detected in the cell nucleus,
while both isoforms are present in the cytoplasm (as was the case in whole cell lysate analyses
described above). This suggests that expression and localization of one of the isoforms is affected
more than that of the other. Additionally, our data indicate that although synthesis of the PPAR-γ
protein may not be significantly affected (as seen by lack of prominent changes at the protein
synthesis site, the cytoplasm), changes in PPAR-γ protein expression are mediated at the level of
the nucleus. One way we can test this hypothesis is by blocking protein synthesis while treating
cells with chemicals to study whether the system will respond the same way to these
manipulations. It can be further speculated that changes in the nucleus, but not in the cytoplasm,
are due to altered protein stability (which may be affected by ubiquitination or unfolded protein
response) or shunting between the two cell compartments. Collectively, our findings suggest that
there are differential PPAR-γ protein regulation mechanisms in the nucleus and the cytoplasm.

74
Baseline activity of PPAR-γ on the GCM-1 promoter is high
In the next set of experiments, we aimed to study how molecular manipulation of PPAR-γ
affects the cascade of events associated with BeWo cellular dynamics, representing key features of
the trophoblast turnover, such as proliferation, differentiation and fusion. First, we studied how
PPAR-γ activation influences the expression of GCM-1. We found that rosiglitazone-mediated
increase in GCM-1 expression is transient and modest, where it is only seen at 3 hours of treatment.
In contrast, T0070907-mediated inhibition of PPAR-γ stably blocked the expression of GCM-1,
which persisted at 24 hours of treatment. Forskolin, a drug used to induce GCM-1 expression, was
used as a positive control to confirm that induction of GCM-1 was possible. These findings indicate
that induction of GCM-1 in BeWo cells is possible; however, it is not primarily mediated via the
transcription factor PPAR-γ.
Since it has been shown that PPAR-γ regulates GCM-1 expression in mouse trophoblast stem
cells [101], we found it surprising that our modulation of this axis could not be easily accomplished
in the BeWo cell model. To offer a possible explanation for this finding, we performed a series of
luciferase reporter assays where we studied PPAR-γ interaction with the GCM-1 promoter in vitro,
in the BeWo cell line. Upon treatment of cells with vehicle control, we observed a high baseline
activity of PPAR-γ; this activity was not greatly different from that observed following treatment of
cells with rosiglitazone. Furthermore, when treating cells with PPAR-γ antagonist, luciferase
expression was greatly downregulated. These finding suggest that baseline interaction of PPAR-γ
with the GCM-1 promoter in the BeWo cell line is strong, and rosiglitazone is not able to induce it
even further. The ability of inducing PPAR-γ activity is possible as seen by the rise of HO-1
transcription levels; however, data suggest that the PPAR-γ/GCM-1 axis does not have the potential
to be stimulated much further. Since it is easier to inhibit the activity of a highly active transcription
factor, we saw a robust decrease in luciferase gene expression with T0070907 treatment. These
reporter assay findings are useful in explaining the next set of experiments on cell proliferation and
differentiation.
Blocking PPAR-γ activity influences key features of the trophoblast physiology
To study the features of trophoblast turnover, we examined how manipulating PPAR-γ
activity affects cell proliferation and differentiation. In our experiments, we showed that cell
proliferation was unaffected by rosiglitazone stimulation at 48 hours; however, relative BeWo cell
numbers were significantly increased following T0070907 treatment. This further reinforced our

75
initial hypothesis that T0070907 is able to influence the PPAR-γ/GCM-1 axis more than
rosiglitazone. Forskolin, which is known to induce differentiation of BeWo cells, was used as a
positive control; its treatment resulted in a decrease in BeWo cell numbers.
To study differentiation, we used a well-characterized assay of free β-hCG release, where a
rise in free β-hCG secretion indicates cell differentiation in our model. Upon treatment of cells with
rosiglitazone, we did not see a significant increase in β-hCG release; this was also true after using a
higher dose of the drug. This finding was expected based on the transient and weak induction of
GCM-1 expression and our findings of weak luciferase reporter signals in BeWo cells following
rosiglitazone treatment. As a control, we showed that induction of differentiation was possible in
our system upon treatment with forskolin, which led to significantly higher levels of β-hCG in the
culture medium. As was predicted, PPAR-γ antagonist had a more prominent effect than the agonist
and significantly decreased β-hCG secretion. Our studies of BeWo cell differentiation were
confirmed with fusion studies (fluorescent IHC) using e-cadherin as a cell surface marker. Cell
fusion can be visualized as aggregation of nuclei and disintegration of the cell surface in forskolin-
treated cells. These characteristics were absent in rosiglitazone- and T0070907-treated cells.
Collectively, our studies indicate that baseline PPAR-γ activity in our BeWo cell model is relatively
high; inducing it even further is challenging, but blocking it with an antagonist has prominent
downstream effects on events such as GCM-1 expression, cell proliferation and differentiation.
Implications for treatment and/or management of sPE
PPAR-γ is a key regulator of many physiological processes, including trophoblast and
adipocyte differentiation, lipid metabolism, inflammation and others. Our studies have shown that
its expression and activity are inversely related, such that inducing its activity with an agonist leads
to a lower expression, while blocking its activity results in higher receptor levels. Importantly, we
observed a trend towards increased PPAR-γ mRNA and protein levels in sPE placentas; this might
reflect that the activity of this transcription factor and nuclear receptor is decreased in pathological
tissue. This also implies that the trophoblast differentiation axis, as controlled by PPAR-γ, is
disrupted in disease. Therefore, pharmacological upregulation of PPAR-γ activity has the potential
to restore placental physiology (via an upregulation of GCM-1) as well as ameliorate maternal
hypertension (via the induction of HO-1, and, subsequently, CO).
Although manipulation of PPAR-γ activity with rosiglitazone appears to be a promising tool
for the management and/or prevention of sPE, the possibility of treating women at risk of sPE with
this drug has to be approached with caution, considering that rosiglitazone exerts its effects on

76
multiple tissues in the human body. When implementing rosiglitazone into treatment plans for
women identified at risk of disease development, the dosage as well as start and duration of
treatment should be carefully determined. Lastly, and most importantly, since this
thiazolidinedione can cross the human placenta, the potential harmful effects of this drug on the
developing fetus deserve considerable attention and should undergo extensive research to warrant
its safe use in human pregnancy.
4.1 Conclusion
Our studies support the role of PPAR-γ in the regulation of several factors involved in
trophoblast layer function. We have shown that this transcription factor is able to regulate the
expression of two important molecules, HO-1 and GCM-1. Activation of PPAR-γ with an agonist
increased the levels of HO-1 on transcriptional and translational levels, without having a strong
effect on cellular GCM-1 levels, cell proliferation, differentiation and fusion. In comparison, blocking
the activity of PPAR-γ using T0070907 resulted in a prominent block of HO-1 and GCM-1
expression, decreased cell differentiation (as seen by a decrease in β-hCG release), and increased
cell proliferation. Our findings have important implications for further study of PPAR-γ in the
placenta and its role in sPE pathogenesis. Since both HO-1 and GCM-1 are downregulated in sPE
placentas [58, 122], our ability to induce their expression via an activation of an upstream factor,
PPAR-γ, is an invaluable tool for the development of possible prophylactic and/or treatment
options for women at risk of developing and suffering from sPE.

77
FUTURE DIRECTIONS
Chapter 5:

78
The current study aimed to (1) establish the relationship between GCM-1 and HO-1, and (2)
assess the effects of PPAR-γ activity modulation on trophoblast layer-related events. Our initial
findings open several avenues which can be explored in further research. To address our first aim
and conclusively state that GCM-1 does not directly regulate expression of HO-1 in BeWo cells, we
propose to perform EMSA or ChIP assays to prove that there is no interaction between the GCM-1
protein and the human HO-1 promoter.
The BeWo cell line is a useful model to study the molecular axes (PPAR-γ/HO-1 and PPAR-
γ/GCM-1) which are the focus of our study. Using this model, we will address several outstanding
questions from our second aim. We propose to study whether the effects of PPAR-γ activity
modulation on cell proliferation and differentiation are HO-1-dependent as well as determine the
role of this enzyme in trophoblast physiology. This can be approached using two different models.
Firstly, HO-1 gene expression can be downregulated using commercially available siRNA sequences.
Alternatively, HO-1 activity can be decreased using several antagonists, such as ZnPP-9 (zinc
protoporphyrin-9) or SnPP (tin protoporphyrin). These experiments will be done concurrently
with rosiglitazone treatment to assess the contribution of the enzyme’s activity to any of HO-1-
(in)dependent effects seen in vitro. Furthermore, to bypass PPAR-γ in the induction of HO-1
expression, drugs which directly stimulate HO-1 mRNA expression such as hemin or statins, as well
as those that stimulate HO-1 activity such as CoPP (cobalt protoporphyrin), can be used to study the
role of HO-1 in trophoblast physiology.
Alternatively, to prove that these effects are specific to PPAR-γ-associated activation, PPAR-
γ levels can be downregulated using siRNA or lentiviral vectors targeting human PPAR-γ
expression. Using either of these techniques will help us define the direct contribution of PPAR-γ to
events related to the trophoblast physiology when cells are treated with rosiglitazone or T0070907.
Although both drugs are specific to PPAR-γ, these experiments will also clarify whether the
chemicals have any secondary effects. A potential limitation of this technique must be
acknowledged: it appears that there are mechanisms in place which constantly attempt to
compensate for fluctuations in receptor activity. To account for this and monitor whether PPAR-γ
activity is decreased following gene downregulation, PPAR-γ trans-activation assay will be
performed.
Another avenue worth exploring is the role of PPAR-γ co-factor, RXR-α, in cell proliferation
and differentiation. This transcription factor can be activated with specific ligands, such as 9-cis-
retinoic acid, and a combination of RXR-α and PPAR-γ agonists might have additive positive effects
on trophoblast layer dynamics and integrity.

79
Although the BeWo cell model is a useful model to study trophoblast function in vitro, it has
limitations. The largest drawback is the lack of sFLT-1 expression in BeWo cells. As mentioned
previously, sFLT-1, an anti-angiogenic protein, is presently believed to be one of the key players in
maternal endothelial cell dysfunction in sPE. Because these cells do not express sFLT-1,
downstream effects of rosiglitazone on the placenta can only be speculated. Therefore, to study how
rosiglitazone affects the physiology of the organ itself, the established first trimester human floating
villous explant model will be used. Analogous experiments to those performed on BeWo cells in our
study, as well as experiments outlined above in this section, will be done using this explant model.
Firstly, we will study how GCM-1 and HO-1 mRNA and protein levels change in response to
rosiglitazone and T0070907 treatments. Secondly, we will assess the balance between
cytotrophoblast cell proliferation and differentiation using Ki67 and/or BrdU markers and β-hCG
release, respectively. Additionally, we will assess explant morphology in semi-thin sections and by
electron microscopy. Last, and most importantly, we will study levels of sFLT-1 in the conditioned
media following treatment with PPAR-γ agonists and antagonists. A decrease in the levels of sFLT-1
release following rosiglitazone treatment would validate the idea of using PPAR-γ as a potential
treatment option for women suffering from sPE. The ability to lower circulating serum sFLT-1
levels in the mother will help treat the systemic endothelial cell dysfunction and ameliorate disease
symptoms such as hypertension and proteinuria.
To conclude our studies on the role of PPAR-γ/HO-1 axis in placental physiology, we will
assess the activity of this enzyme in first trimester placental explants. HO-1 is an enzyme that
breaks down heme into three components, one of which is CO; assays are available to study the
concentration of CO in the gaseous phase above a homogenized sample. Furthermore, a new
technique is available to detect bilirubin levels using the UnaG protein which possesses a high
affinity for, and fluoresces upon the binding of, this metabolite. An interesting study will be to
assess whether drugs modulating PPAR-γ activity also influence HO-1 activity, as measured by CO
and/or bilirubin levels. A rise in their concentrations following rosiglitazone treatment would have
direct implications for the efficacy of the use of this drug for management of sPE. This finding would
suggest that rosiglitazone may help treat maternal hypertension and decrease systemic vascular
resistance by increasing the expression and activity of an enzyme responsible for secretion of a
potent vasodilator (CO) and an anti-oxidant (bilirubin).
The response of early- and late-onset sPE placentas to drugs of interest should be assessed.
Whether sPE placentas respond similarly and positively to treatment with rosiglitazone will
determine how useful this drug can be to treat the diseased organ. It must be mentioned that

80
whether or not rosiglitazone will exert its effects on the pathological tissue will depend on the
severity of placental pathology. It is possible that tissue response to rosiglitazone may not be
strongly pronounced, considering that at the time of delivery, sPE placentas are beyond the point of
when treatment can reverse or treat the pathology. If this will be the case, the study of the response
of first trimester explant tissue to rosiglitazone becomes even more urgent in order to deliver
rosiglitazone as a prophylactic treatment to women identified at risk of developing sPE.
Identifying the responses of healthy first trimester and sPE explants to drugs regulating
PPAR-γ activity will offer insights into the actions of this transcription factor during healthy
pregnancy progression and in placental insufficiency syndromes. In the event of a finding that
rosiglitazone treatment decreases secretion of sFLT-1 and induces the activity of HO-1 (seen as an
upregulation of CO levels), this drug will gain further support as a treatment option for women at
risk of or suffering from sPE.

81
REFERENCES
Chapter 6:

82
1. Metcalfe, J. and K. Ueland, Maternal cardiovascular adjustments to pregnancy. Prog Cardiovasc Dis, 1974. 16(4): p. 363-74.
2. Abbas, A.E., S.J. Lester, and H. Connolly, Pregnancy and the cardiovascular system. Int J Cardiol, 2005. 98(2): p. 179-89.
3. Roberts CL, F.J., Algert CS, et al, Population-based trends in pregnancy hypertension and pre-eclampsia: an international comparative study. BMJ Open 2011.
4. Hutcheon, J.A., S. Lisonkova, and K.S. Joseph, Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol, 2011. 25(4): p. 391-403.
5. Practice, A.C.o.O., ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet, 2002. 77(1): p. 67-75.
6. Parikh, S.M. and S.A. Karumanchi, Putting pressure on pre-eclampsia. Nat Med, 2008. 14(8): p. 810-2.
7. Franco, C., et al., Placental infarction and thrombophilia. Obstet Gynecol, 2011. 117(4): p. 929-34.
8. Witlin, A.G. and B.M. Sibai, Magnesium sulfate therapy in preeclampsia and eclampsia. Obstet Gynecol, 1998. 92(5): p. 883-9.
9. Hofmeyr, G.J., A.N. Atallah, and L. Duley, Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database Syst Rev, 2006(3): p. CD001059.
10. Zhou, S.J., et al., Fish-oil supplementation in pregnancy does not reduce the risk of gestational diabetes or preeclampsia. Am J Clin Nutr, 2012. 95(6): p. 1378-84.
11. Basaran, A., M. Basaran, and B. Topatan, Combined vitamin C and E supplementation for the prevention of preeclampsia: a systematic review and meta-analysis. Obstet Gynecol Surv, 2010. 65(10): p. 653-67.
12. Roberge, S., et al., Early administration of low-dose aspirin for the prevention of severe and mild preeclampsia: a systematic review and meta-analysis. Am J Perinatol, 2012. 29(7): p. 551-6.
13. Rey, E., et al., Dalteparin for the prevention of recurrence of placental-mediated complications of pregnancy in women without thrombophilia: a pilot randomized controlled trial. J Thromb Haemost, 2009. 7(1): p. 58-64.
14. Kingdom, J.C., et al., Unfractionated heparin for second trimester placental insufficiency: a pilot randomized trial. J Thromb Haemost, 2011. 9(8): p. 1483-92.
15. Drewlo, S., et al., Heparin promotes soluble VEGF receptor expression in human placental villi to impair endothelial VEGF signaling. J Thromb Haemost, 2011. 9(12): p. 2486-97.
16. Sobel, M.L., J. Kingdom, and S. Drewlo, Angiogenic response of placental villi to heparin. Obstet Gynecol, 2011. 117(6): p. 1375-83.
17. Sibley, C.P., et al., Mechanisms of maternofetal exchange across the human placenta. Biochem Soc Trans, 1998. 26(2): p. 86-91.
18. Gude, N.M., et al., Growth and function of the normal human placenta. Thromb Res, 2004. 114(5-6): p. 397-407.
19. Burton, G.J., J. Hempstock, and E. Jauniaux, Nutrition of the human fetus during the first trimester--a review. Placenta, 2001. 22 Suppl A: p. S70-7.
20. Benirschke K, K.P., Baergen R., Pathology of the human placenta. 2005, New York, NY: Springer.
21. Everett, T.R. and C.C. Lees, Beyond the placental bed: placental and systemic determinants of the uterine artery Doppler waveform. Placenta, 2012. 33(11): p. 893-901.
22. Pijnenborg, R., et al., Uteroplacental arterial changes related to interstitial trophoblast migration in early human pregnancy. Placenta, 1983. 4(4): p. 397-413.

83
23. Pijnenborg, R., et al., The pattern of interstitial trophoblastic invasion of the myometrium in early human pregnancy. Placenta, 1981. 2(4): p. 303-16.
24. Burton, G.J., E. Jauniaux, and A.L. Watson, Maternal arterial connections to the placental intervillous space during the first trimester of human pregnancy: the Boyd collection revisited. Am J Obstet Gynecol, 1999. 181(3): p. 718-24.
25. Bischof, P. and A. Campana, A model for implantation of the human blastocyst and early placentation. Hum Reprod Update, 1996. 2(3): p. 262-70.
26. Drewlo, S., et al., Glial cell missing-1 mediates over-expression of tissue inhibitor of metalloproteinase-4 in severe pre-eclamptic placental villi. Hum Reprod, 2011. 26(5): p. 1025-34.
27. Moffett-King, A., Natural killer cells and pregnancy. Nat Rev Immunol, 2002. 2(9): p. 656-63. 28. Morrish, D.W., J. Dakour, and H. Li, Functional regulation of human trophoblast
differentiation. J Reprod Immunol, 1998. 39(1-2): p. 179-95. 29. Mayhew, T.M., Villous trophoblast of human placenta: a coherent view of its turnover, repair
and contributions to villous development and maturation. Histol Histopathol, 2001. 16(4): p. 1213-24.
30. Huppertz, B., et al., Villous cytotrophoblast regulation of the syncytial apoptotic cascade in the human placenta. Histochem Cell Biol, 1998. 110(5): p. 495-508.
31. Lanoix, D., et al., Melatonin: the smart killer: the human trophoblast as a model. Mol Cell Endocrinol, 2012. 348(1): p. 1-11.
32. Kaufmann, P., S. Black, and B. Huppertz, Endovascular trophoblast invasion: implications for the pathogenesis of intrauterine growth retardation and preeclampsia. Biol Reprod, 2003. 69(1): p. 1-7.
33. Pijnenborg, R., et al., Placental bed spiral arteries in the hypertensive disorders of pregnancy. Br J Obstet Gynaecol, 1991. 98(7): p. 648-55.
34. Matsubara, K., et al., Role of nitric oxide and reactive oxygen species in the pathogenesis of preeclampsia. J Obstet Gynaecol Res, 2010. 36(2): p. 239-47.
35. Myatt, L., et al., Nitrotyrosine residues in placenta. Evidence of peroxynitrite formation and action. Hypertension, 1996. 28(3): p. 488-93.
36. Hung, T.H. and G.J. Burton, Hypoxia and reoxygenation: a possible mechanism for placental oxidative stress in preeclampsia. Taiwan J Obstet Gynecol, 2006. 45(3): p. 189-200.
37. Jonsson, Y., et al., Cytokine mapping of sera from women with preeclampsia and normal pregnancies. J Reprod Immunol, 2006. 70(1-2): p. 83-91.
38. Patel, J., et al., Regulation of hypoxia inducible factors (HIF) in hypoxia and normoxia during placental development. Placenta, 2010. 31(11): p. 951-7.
39. Araki-Taguchi, M., et al., Angiotensin II mimics the hypoxic effect on regulating trophoblast proliferation and differentiation in human placental explant cultures. Life Sci, 2008. 82(1-2): p. 59-67.
40. Nevo, O., et al., Increased expression of sFlt-1 in in vivo and in vitro models of human placental hypoxia is mediated by HIF-1. Am J Physiol Regul Integr Comp Physiol, 2006. 291(4): p. R1085-93.
41. Yinon, Y., et al., Severe intrauterine growth restriction pregnancies have increased placental endoglin levels: hypoxic regulation via transforming growth factor-beta 3. Am J Pathol, 2008. 172(1): p. 77-85.
42. Ahmad, S. and A. Ahmed, Elevated placental soluble vascular endothelial growth factor receptor-1 inhibits angiogenesis in preeclampsia. Circ Res, 2004. 95(9): p. 884-91.
43. Cudmore, M., et al., Negative regulation of soluble Flt-1 and soluble endoglin release by heme oxygenase-1. Circulation, 2007. 115(13): p. 1789-1797.

84
44. Rajakumar, A., et al., Transcriptionally active syncytial aggregates in the maternal circulation may contribute to circulating soluble fms-like tyrosine kinase 1 in preeclampsia. Hypertension, 2012. 59(2): p. 256-64.
45. Ellery, P.M., et al., Evidence for transcriptional activity in the syncytiotrophoblast of the human placenta. Placenta, 2009. 30(4): p. 329-34.
46. Fogarty, N.M., et al., A quantitative analysis of transcriptionally active syncytiotrophoblast nuclei across human gestation. J Anat, 2011. 219(5): p. 601-10.
47. Levine, R.J., et al., Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med, 2004. 350(7): p. 672-83.
48. Ferrara, N., H.P. Gerber, and J. LeCouter, The biology of VEGF and its receptors. Nat Med, 2003. 9(6): p. 669-76.
49. Hosoya, T., et al., glial cells missing: a binary switch between neuronal and glial determination in Drosophila. Cell, 1995. 82(6): p. 1025-36.
50. Schreiber, J., E. Sock, and M. Wegner, The regulator of early gliogenesis glial cells missing is a transcription factor with a novel type of DNA-binding domain. Proceedings of the National Academy of Sciences of the United States of America, 1997. 94(9): p. 4739-4744.
51. Schreiber, J., J. Enderich, and M. Wegner, Structural requirements for DNA binding of GCM proteins. Nucleic Acids Research, 1998. 26(10): p. 2337-2343.
52. Nait-Oumesmar, B., A.B. Copperman, and R.A. Lazzarini, Placental expression and chromosomal localization of the human Gcm 1 gene. J Histochem Cytochem, 2000. 48(7): p. 915-22.
53. Anson-Cartwright, L., et al., The glial cells missing-1 protein is essential for branching morphogenesis in the chorioallantoic placenta. Nat Genet, 2000. 25(3): p. 311-4.
54. Stecca, B., et al., Gcm1 expression defines three stages of chorio-allantoic interaction during placental development. Mech Dev, 2002. 115(1-2): p. 27-34.
55. Baczyk, D., et al., Complex patterns of GCM1 mRNA and protein in villous and extravillous trophoblast cells of the human placenta. Placenta, 2004. 25(6): p. 553-559.
56. Chang, C.-W., et al., Stimulation of GCMa transcriptional activity by cyclic AMP/protein kinase A signaling is attributed to CBP-mediated acetylation of GCMa. Molecular and cellular biology, 2005. 25(19): p. 8401-8414.
57. Baczyk, D., et al., Glial cell missing-1 transcription factor is required for the differentiation of the human trophoblast. Cell death and differentiation, 2009. 16(5): p. 719-727.
58. Chen, C.P., et al., Decreased placental GCM1 (glial cells missing) gene expression in pre-eclampsia. Placenta, 2004. 25(5): p. 413-421.
59. Bainbridge, S.A., et al., Effects of reduced Gcm1 expression on trophoblast morphology, fetoplacental vascularity, and pregnancy outcomes in mice. Hypertension, 2012. 59(3): p. 732-9.
60. Yu, C., et al., GCMa regulates the syncytin-mediated trophoblastic fusion. J Biol Chem, 2002. 277(51): p. 50062-8.
61. Lin, C., M. Lin, and H. Chen, Biochemical characterization of the human placental transcription factor GCMa/1. Biochem Cell Biol, 2005. 83(2): p. 188-95.
62. Mukherjee, R., et al., Identification, characterization, and tissue distribution of human peroxisome proliferator-activated receptor (PPAR) isoforms PPARgamma2 versus PPARgamma1 and activation with retinoid X receptor agonists and antagonists. J Biol Chem, 1997. 272(12): p. 8071-6.
63. Elbrecht, A., et al., Molecular cloning, expression and characterization of human peroxisome proliferator activated receptors gamma 1 and gamma 2. Biochem Biophys Res Commun, 1996. 224(2): p. 431-7.
64. Barbier, O., et al., Pleiotropic actions of peroxisome proliferator-activated receptors in lipid metabolism and atherosclerosis. Arterioscler Thromb Vasc Biol, 2002. 22(5): p. 717-26.

85
65. Abbott, B.D., Review of the expression of peroxisome proliferator-activated receptors alpha (PPAR alpha), beta (PPAR beta), and gamma (PPAR gamma) in rodent and human development. Reprod Toxicol, 2009. 27(3-4): p. 246-57.
66. Lehmann, J.M., et al., An antidiabetic thiazolidinedione is a high affinity ligand for peroxisome proliferator-activated receptor gamma (PPAR gamma). J Biol Chem, 1995. 270(22): p. 12953-6.
67. Lehrke, M. and M.A. Lazar, The many faces of PPARgamma. Cell, 2005. 123(6): p. 993-9. 68. Michalik, L. and W. Wahli, Peroxisome proliferator-activated receptors: three isotypes for a
multitude of functions. Curr Opin Biotechnol, 1999. 10(6): p. 564-70. 69. Marceau, G., Blanchon, L., Lobaccaro, J.-M., Sapin V. , Role of Nuclear Receptors Peroxisome
Proliferator-Activated Receptors (PPARs) and Liver X Receptors (LXRs) in the Human Placental Pathophysiology, in Recent Advances in Research on the Human Placenta, J. Zheng, Editor. 2012.
70. Chandra, V., et al., Structure of the intact PPAR-gamma-RXR- nuclear receptor complex on DNA. Nature, 2008. 456(7220): p. 350-6.
71. A, I.J., et al., Polarity and specific sequence requirements of peroxisome proliferator-activated receptor (PPAR)/retinoid X receptor heterodimer binding to DNA. A functional analysis of the malic enzyme gene PPAR response element. J Biol Chem, 1997. 272(32): p. 20108-17.
72. Zieleniak, A., M. Wojcik, and L.A. Wozniak, Structure and physiological functions of the human peroxisome proliferator-activated receptor gamma. Arch Immunol Ther Exp (Warsz), 2008. 56(5): p. 331-45.
73. Gelman, L., et al., Kinase signaling cascades that modulate peroxisome proliferator-activated receptors. Curr Opin Cell Biol, 2005. 17(2): p. 216-22.
74. Wang, H., et al., Stage-specific integration of maternal and embryonic peroxisome proliferator-activated receptor delta signaling is critical to pregnancy success. J Biol Chem, 2007. 282(52): p. 37770-82.
75. Barak, Y., et al., PPAR gamma is required for placental, cardiac, and adipose tissue development. Mol Cell, 1999. 4(4): p. 585-95.
76. Willson, T.M. and W. Wahli, Peroxisome proliferator-activated receptor agonists. Curr Opin Chem Biol, 1997. 1(2): p. 235-41.
77. Issemann, I. and S. Green, Activation of a member of the steroid hormone receptor superfamily by peroxisome proliferators. Nature, 1990. 347(6294): p. 645-50.
78. Forman, B.M., et al., 15-Deoxy-delta 12, 14-prostaglandin J2 is a ligand for the adipocyte determination factor PPAR gamma. Cell, 1995. 83(5): p. 803-12.
79. Kliewer, S.A., et al., A prostaglandin J2 metabolite binds peroxisome proliferator-activated receptor gamma and promotes adipocyte differentiation. Cell, 1995. 83(5): p. 813-9.
80. Yki-Jarvinen, H., Thiazolidinediones. N Engl J Med, 2004. 351(11): p. 1106-18. 81. Sakamoto, J., et al., Activation of human peroxisome proliferator-activated receptor (PPAR)
subtypes by pioglitazone. Biochem Biophys Res Commun, 2000. 278(3): p. 704-11. 82. Feige, J.N., et al., From molecular action to physiological outputs: peroxisome proliferator-
activated receptors are nuclear receptors at the crossroads of key cellular functions. Prog Lipid Res, 2006. 45(2): p. 120-59.
83. Leesnitzer, L.M., et al., Functional consequences of cysteine modification in the ligand binding sites of peroxisome proliferator activated receptors by GW9662. Biochemistry, 2002. 41(21): p. 6640-50.
84. Lee, G., et al., T0070907, a selective ligand for peroxisome proliferator-activated receptor gamma, functions as an antagonist of biochemical and cellular activities. J Biol Chem, 2002. 277(22): p. 19649-57.

86
85. van Beekum, O., V. Fleskens, and E. Kalkhoven, Posttranslational modifications of PPAR-gamma: fine-tuning the metabolic master regulator. Obesity (Silver Spring), 2009. 17(2): p. 213-9.
86. Adams, M., et al., Transcriptional activation by peroxisome proliferator-activated receptor gamma is inhibited by phosphorylation at a consensus mitogen-activated protein kinase site. J Biol Chem, 1997. 272(8): p. 5128-32.
87. Camp, H.S. and S.R. Tafuri, Regulation of peroxisome proliferator-activated receptor gamma activity by mitogen-activated protein kinase. J Biol Chem, 1997. 272(16): p. 10811-6.
88. Hu, E., et al., Inhibition of adipogenesis through MAP kinase-mediated phosphorylation of PPARgamma. Science, 1996. 274(5295): p. 2100-3.
89. Shao, D., et al., Interdomain communication regulating ligand binding by PPAR-gamma. Nature, 1998. 396(6709): p. 377-80.
90. Compe, E., et al., Dysregulation of the peroxisome proliferator-activated receptor target genes by XPD mutations. Mol Cell Biol, 2005. 25(14): p. 6065-76.
91. Iankova, I., et al., Peroxisome proliferator-activated receptor gamma recruits the positive transcription elongation factor b complex to activate transcription and promote adipogenesis. Mol Endocrinol, 2006. 20(7): p. 1494-505.
92. Rodie, V.A., et al., Human placental peroxisome proliferator-activated receptor delta and gamma expression in healthy pregnancy and in preeclampsia and intrauterine growth restriction. J Soc Gynecol Investig, 2005. 12(5): p. 320-9.
93. Schaiff, W.T., et al., Peroxisome proliferator-activated receptor-gamma modulates differentiation of human trophoblast in a ligand-specific manner. J Clin Endocrinol Metab, 2000. 85(10): p. 3874-81.
94. Waite, L.L., et al., Placental peroxisome proliferator-activated receptor-gamma is up-regulated by pregnancy serum. J Clin Endocrinol Metab, 2000. 85(10): p. 3808-14.
95. Toth, B., et al., Peroxisome proliferator-activated receptor-gamma in normal human pregnancy and miscarriage. Acta Histochem, 2009. 111(4): p. 372-8.
96. Drewlo, S., K. Levytska, and J. Kingdom, Revisiting the housekeeping genes of human placental development and insufficiency syndromes. Placenta, 2012. 33(11): p. 952-4.
97. Waite, L.L., R.E. Louie, and R.N. Taylor, Circulating activators of peroxisome proliferator-activated receptors are reduced in preeclamptic pregnancy. J Clin Endocrinol Metab, 2005. 90(2): p. 620-6.
98. Joss-Moore, L.A., et al., IUGR decreases PPARgamma and SETD8 Expression in neonatal rat lung and these effects are ameliorated by maternal DHA supplementation. Early Hum Dev, 2010. 86(12): p. 785-91.
99. Joss-Moore, L.A., et al., Uteroplacental insufficiency increases visceral adiposity and visceral adipose PPARgamma2 expression in male rat offspring prior to the onset of obesity. Early Hum Dev, 2010. 86(3): p. 179-85.
100. Desai, M., et al., Programmed upregulation of adipogenic transcription factors in intrauterine growth-restricted offspring. Reprod Sci, 2008. 15(8): p. 785-96.
101. Parast, M.M., et al., PPARgamma regulates trophoblast proliferation and promotes labyrinthine trilineage differentiation. PLoS One, 2009. 4(11): p. e8055.
102. Ruebner, M., et al., Regulation of the human endogenous retroviral Syncytin-1 and cell-cell fusion by the nuclear hormone receptors PPARgamma/RXRalpha in placentogenesis. J Cell Biochem, 2012. 113(7): p. 2383-96.
103. Schaiff, W.T., et al., Peroxisome proliferator-activated receptor-gamma and retinoid X receptor signaling regulate fatty acid uptake by primary human placental trophoblasts. J Clin Endocrinol Metab, 2005. 90(7): p. 4267-75.
104. Fournier, T., et al., Involvement of PPARgamma in human trophoblast invasion. Placenta, 2007. 28 Suppl A: p. S76-81.

87
105. Schaiff, W.T., et al., Ligand-activated peroxisome proliferator activated receptor gamma alters placental morphology and placental fatty acid uptake in mice. Endocrinology, 2007. 148(8): p. 3625-34.
106. Nadra, K., et al., PPARgamma in placental angiogenesis. Endocrinology, 2010. 151(10): p. 4969-81.
107. McCarthy, F.P., et al., Peroxisome proliferator-activated receptor-gamma as a potential therapeutic target in the treatment of preeclampsia. Hypertension, 2011. 58(2): p. 280-6.
108. Granger, J.P., et al., Reduced uterine perfusion pressure (RUPP) model for studying cardiovascular-renal dysfunction in response to placental ischemia. Methods Mol Med, 2006. 122: p. 383-92.
109. McCarthy, F.P., et al., Evidence implicating peroxisome proliferator-activated receptor-gamma in the pathogenesis of preeclampsia. Hypertension, 2011. 58(5): p. 882-7.
110. Chan, L.Y., J.H. Yeung, and T.K. Lau, Placental transfer of rosiglitazone in the first trimester of human pregnancy. Fertil Steril, 2005. 83(4): p. 955-8.
111. Yaris, F., et al., Normal pregnancy outcome following inadvertent exposure to rosiglitazone, gliclazide, and atorvastatin in a diabetic and hypertensive woman. Reprod Toxicol, 2004. 18(4): p. 619-21.
112. Kalyoncu, N.I., et al., A case of rosiglitazone exposure in the second trimester of pregnancy. Reprod Toxicol, 2005. 19(4): p. 563-4.
113. McCarthy, F.P., et al., PPAR-gamma -- a possible drug target for complicated pregnancies. Br J Pharmacol, 2013. 168(5): p. 1074-85.
114. Kronke, G., et al., Expression of heme oxygenase-1 in human vascular cells is regulated by peroxisome proliferator-activated receptors. Arterioscler Thromb Vasc Biol, 2007. 27(6): p. 1276-82.
115. Levytska, K., et al., Heme oxygenase-1 in placental development and pathology. Placenta, 2013. 34(4): p. 291-8.
116. Maines, M.D., G.M. Trakshel, and R.K. Kutty, Characterization of two constitutive forms of rat liver microsomal heme oxygenase. Only one molecular species of the enzyme is inducible. J Biol Chem, 1986. 261(1): p. 411-9.
117. Shibahara, S., et al., Functional analysis of cDNAs for two types of human heme oxygenase and evidence for their separate regulation. J Biochem, 1993. 113(2): p. 214-8.
118. Yoshida, T., et al., Human heme oxygenase cDNA and induction of its mRNA by hemin. Eur J Biochem, 1988. 171(3): p. 457-61.
119. Tenhunen, R., H.S. Marver, and R. Schmid, Microsomal heme oxygenase. Characterization of the enzyme. J Biol Chem, 1969. 244(23): p. 6388-94.
120. Montellano, P.R., The mechanism of heme oxygenase. Curr Opin Chem Biol, 2000. 4(2): p. 221-7.
121. Neuzil, J. and R. Stocker, Free and albumin-bound bilirubin are efficient co-antioxidants for alpha-tocopherol, inhibiting plasma and low density lipoprotein lipid peroxidation. J Biol Chem, 1994. 269(24): p. 16712-9.
122. Ahmed, A., et al., Induction of placental heme oxygenase-1 is protective against TNFalpha-induced cytotoxicity and promotes vessel relaxation. Mol Med, 2000. 6(5): p. 391-409.
123. Brouard, S., et al., Carbon monoxide generated by heme oxygenase 1 suppresses endothelial cell apoptosis. J Exp Med, 2000. 192(7): p. 1015-26.
124. Sarady, J.K., et al., Carbon monoxide modulates endotoxin-induced production of granulocyte macrophage colony-stimulating factor in macrophages. Am J Respir Cell Mol Biol, 2002. 27(6): p. 739-45.
125. Coceani, F., Carbon monoxide and dilation of blood vessels. Science, 1993. 260(5109): p. 739. 126. Morita, T., et al., Smooth muscle cell-derived carbon monoxide is a regulator of vascular cGMP.
Proc Natl Acad Sci U S A, 1995. 92(5): p. 1475-9.

88
127. Acevedo, C.H. and A. Ahmed, Hemeoxygenase-1 inhibits human myometrial contractility via carbon monoxide and is upregulated by progesterone during pregnancy. J Clin Invest, 1998. 101(5): p. 949-55.
128. Bainbridge, S.A., et al., Carbon monoxide decreases perfusion pressure in isolated human placenta. Placenta, 2002. 23(8-9): p. 563-9.
129. Kreiser, D., et al., Gestational pattern of heme oxygenase expression in the rat. Pediatr Res, 2003. 54(2): p. 172-8.
130. Zhao, H., et al., Regulation of maternal and fetal hemodynamics by heme oxygenase in mice. Biol Reprod, 2008. 78(4): p. 744-51.
131. Watanabe, S., et al., Marked developmental changes in heme oxygenase-1 (HO-1) expression in the mouse placenta: correlation between HO-1 expression and placental development. Placenta, 2004. 25(5): p. 387-95.
132. McLaughlin, B.E., et al., Heme oxygenase expression in selected regions of term human placenta. Exp Biol Med (Maywood), 2003. 228(5): p. 564-7.
133. Lyall, F., et al., Hemeoxygenase expression in human placenta and placental bed implies a role in regulation of trophoblast invasion and placental function. FASEB J, 2000. 14(1): p. 208-19.
134. McLean, M., et al., Expression of the heme oxygenase-carbon monoxide signalling system in human placenta. J Clin Endocrinol Metab, 2000. 85(6): p. 2345-9.
135. Yoshiki, N., T. Kubota, and T. Aso, Expression and localization of heme oxygenase in human placental villi. Biochem Biophys Res Commun, 2000. 276(3): p. 1136-42.
136. Baum, M., et al., End-tidal carbon monoxide measurements in women with pregnancy-induced hypertension and preeclampsia. Am J Obstet Gynecol, 2000. 183(4): p. 900-3.
137. Kreiser, D., et al., End tidal carbon monoxide levels are lower in women with gestational hypertension and pre-eclampsia. J Perinatol, 2004. 24(4): p. 213-7.
138. Zenclussen, A.C., et al., Heme oxygenases in pregnancy II: HO-2 is downregulated in human pathologic pregnancies. Am J Reprod Immunol, 2003. 50(1): p. 66-76.
139. Lash, G.E., et al., Relationship between tissue damage and heme oxygenase expression in chorionic villi of term human placenta. Am J Physiol Heart Circ Physiol, 2003. 284(1): p. H160-7.
140. Barber, A., et al., Heme oxygenase expression in human placenta and placental bed: reduced expression of placenta endothelial HO-2 in preeclampsia and fetal growth restriction. FASEB J, 2001. 15(7): p. 1158-68.
141. Poss, K.D. and S. Tonegawa, Reduced stress defense in heme oxygenase 1-deficient cells. Proc Natl Acad Sci U S A, 1997. 94(20): p. 10925-30.
142. Poss, K.D. and S. Tonegawa, Heme oxygenase 1 is required for mammalian iron reutilization. Proc Natl Acad Sci U S A, 1997. 94(20): p. 10919-24.
143. Kapturczak, M.H., et al., Heme oxygenase-1 modulates early inflammatory responses: evidence from the heme oxygenase-1-deficient mouse. Am J Pathol, 2004. 165(3): p. 1045-53.
144. Zhao, H., et al., Effect of heme oxygenase-1 deficiency on placental development. Placenta, 2009. 30(10): p. 861-8.
145. Wong, R.J., H. Zhao, and D.K. Stevenson, A deficiency in haem oxygenase-1 induces foetal growth restriction by placental vasculature defects. Acta Paediatr, 2012. 101(8): p. 827-34.
146. Zhao, H., et al., Maternal heme oxygenase 1 regulates placental vasculature development via angiogenic factors in mice. Biol Reprod, 2011. 85(5): p. 1005-12.
147. Zenclussen, M.L., et al., Haem oxygenase-1 dictates intrauterine fetal survival in mice via carbon monoxide. J Pathol, 2011. 225(2): p. 293-304.
148. Kweider, N., et al., Interplay between vascular endothelial growth factor (VEGF) and nuclear factor erythroid 2-related factor-2 (Nrf2): implications for preeclampsia. J Biol Chem, 2011. 286(50): p. 42863-72.

89
149. Lin, Q., et al., Heme oxygenase-1 protein localizes to the nucleus and activates transcription factors important in oxidative stress. J Biol Chem, 2007. 282(28): p. 20621-33.
150. Bilban, M., et al., Identification of novel trophoblast invasion-related genes: heme oxygenase-1 controls motility via peroxisome proliferator-activated receptor gamma. Endocrinology, 2009. 150(2): p. 1000-13.
151. McCaig, D. and F. Lyall, Heme oxygenase expression in human placental villous tissue in response to exposure to in vitro ischemia-reperfusion injury. Hypertens Pregnancy, 2009. 28(3): p. 256-72.
152. Fitzgerald, B., et al., Villous trophoblast abnormalities in extremely preterm deliveries with elevated second trimester maternal serum hCG or inhibin-A. Placenta, 2011. 32(4): p. 339-45.
153. Cudmore, M., et al., Negative regulation of soluble Flt-1 and soluble endoglin release by heme oxygenase-1. Circulation, 2007. 115(13): p. 1789-97.
154. Cudmore, M.J., et al., Resveratrol inhibits the release of soluble fms-like tyrosine kinase (sFlt-1) from human placenta. Am J Obstet Gynecol, 2012. 206(3): p. 253 e10-5.
155. Sedeek, M., et al., Role of reactive oxygen species in hypertension produced by reduced uterine perfusion in pregnant rats. Am J Hypertens, 2008. 21(10): p. 1152-6.
156. George, E.M., et al., Induction of heme oxygenase 1 attenuates placental ischemia-induced hypertension. Hypertension, 2011. 57(5): p. 941-8.
157. George, E.M., et al., Induction of heme oxygenase-1 attenuates sFlt-1-induced hypertension in pregnant rats. Am J Physiol Regul Integr Comp Physiol, 2011. 301(5): p. R1495-500.
158. George, E.M. and I. Arany, Induction of heme oxygenase-1 shifts the balance from proinjury to prosurvival in the placentas of pregnant rats with reduced uterine perfusion pressure. Am J Physiol Regul Integr Comp Physiol, 2012. 302(5): p. R620-6.
159. Schaefer, K.L., et al., PPARgamma inhibitors reduce tubulin protein levels by a PPARgamma, PPARdelta and proteasome-independent mechanism, resulting in cell cycle arrest, apoptosis and reduced metastasis of colorectal carcinoma cells. Int J Cancer, 2007. 120(3): p. 702-13.
160. McCarthy, F., et al., Evidence implicating peroxisome proliferator-activated receptor-γ in the pathogenesis of preeclampsia. Hypertension, 2011. 58(5): p. 882-887.
161. Lee, G., et al., T0070907, a selective ligand for peroxisome proliferator-activated receptor gamma, functions as an antagonist of biochemical and cellular activities. The Journal of biological chemistry, 2002. 277(22): p. 19649-19657.
162. Vandesompele, J., et al., Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol, 2002. 3(7): p. RESEARCH0034.
163. Coutifaris, C., et al., E-cadherin expression during the differentiation of human trophoblasts. Development, 1991. 113(3): p. 767-77.
164. Basyuk, E., et al., Murine Gcm1 gene is expressed in a subset of placental trophoblast cells. Dev Dyn, 1999. 214(4): p. 303-11.
165. Dawson, P.A., J. Rakoczy, and D.G. Simmons, Placental, renal, and ileal sulfate transporter gene expression in mouse gestation. Biol Reprod, 2012. 87(2): p. 43.
166. Watanabe, M., et al., Regulation of PPAR gamma transcriptional activity in 3T3-L1 adipocytes. Biochem Biophys Res Commun, 2003. 300(2): p. 429-36.
167. Durante, W., et al., cAMP induces heme oxygenase-1 gene expression and carbon monoxide production in vascular smooth muscle. The American journal of physiology, 1997. 273(1 Pt 2): p. 23.

90
APPENDIX
Chapter 7:

Technical note
Revisiting the housekeeping genes of human placental development andinsufficiency syndromes
S. Drewlo a,*, K. Levytska a, J. Kingdom a,b
aCentre for Research in Women’s and Infant’s health, Samuel Lunenfeld Research Institute, Mount Sinai Hospital, University of Toronto, 25 Orde Street #6-1020, Toronto,ON, Canada M5T 3H7bDepartment of Obstetrics & Gynaecology, Mount Sinai Hospital, University of Toronto, Canada
a r t i c l e i n f o
Article history:Accepted 11 September 2012
Keywords:House keeping genesPlacentaqRTPCR
a b s t r a c t
Gene expression analysis using semi-quantitative RT-PCR is a common tool in placental research.However the comparison of steady-state gene transcription between different clinical groups isdependent upon comparison of target mRNA data with mRNA obtained from so-called housekeeping(HK) genes whose steady-state transcription does not differ significantly between the groups. In thiscommunication, we evaluated the performance of candidate HK genes across nine clinical groupscommonly used in placental research. We used the GeNorm method to evaluate qRT-PCR data todetermine the performance of candidate HKs.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
The quantification of mRNA gene expression via qRT-PCR is oneof the most important tools used in placental research. It offers theopportunity to compare the expression levels of numerous genesusing small amounts of tissue generated from specific clinicalgroups of pathologies and control cases. As little as 5 pg of cDNA issufficient for a successful PCR reaction. Although qRT-PCR iswidely-used, many researchers do not follow established rules toensure the validity of their data. These rules may not be criticalwhen high-fold changes of a target gene are found in comparisonwith controls, but become critical at the lower end of relevant (2e4-fold) changes in gene expression (Supplemental Fig. 1 [1]).Inappropriate choice of housekeeping gene(s) could lead to wrongconclusions, evenwhen sample sizes createmean fold changes thatare statistically significant. In such circumstances, careful assess-ment of potential variation in selected HKG expression could eithercause, or obscure these smaller, but potentially relevant target genetranscription data.
The quality of housekeeping gene data is highly dependent onRNA purity and integrity, as well as the cDNA conversion rate andthe efficiency of the PCR reaction. To compare gene expression indifferent samples, it is important to use internal controls, describedas housekeeping (HK) genes. Ideally, these genes should be stablewith similar abundance as the target genes expressed in all
samples. In this way, the gene of interest can be normalized to theHK gene’s expression. Use of the geometric mean of multiplecontrols of at least two, and ideally three, HK genes is needed foroptimal precision [2]. Thus far a number of groups have addressedthis issue albeit with different results [3e5]. Different house-keeping genes have been proposed for use in human placentaltissue, but thus far, none of the current studies have evaluated HKgenes for potential changes across normal gestation or in the rangeof pregnancy complications attributed to placental dysfunction.
2. Material and methods
We isolated a total of 90 samples of RNA from 9 different clinical groups ofplacental material to search for ideal housekeeping genes applicable to all condi-tions. These groups are summarized in Table 1; healthy first trimester (early andlate), healthy second trimester, preterm controls, term controls (vaginal andcaesarian delivery), severe early onset intrauterine growth restriction (IUGR) andsevere pre-eclampsia (PET) as well as a mixed PET-IUGR group (MIUGR). Thesetissues specimens were obtained by the Research Centre for Women’s and Infants’Health (RCWIH) BioBank program of Mount Sinai Hospital, in accordance with thepolicies of the Mount Sinai Hospital Research Ethics Board (MSH,10-0128-E).Placentas from singleton pathologic pregnancies and age matched controls of liveborn infants delivered between 24 þ 0 and 34 þ 6 weeks of gestation. They wereclassified into different groups, with characteristics summarized in Table 1: Severeintrauterine growth restriction (IUGR): Birth weight �10%ile, abnormal umbilicalartery Doppler (absent end diastolic flow velocity (AEDFV) or reversed end diastolicflow velocity (REDFV)), normotensive women. Severe pre-eclampsia (PET): Birthweight >10%ile, BP > 140/90, proteinuria >300 mg/day or �1þ on dipstick. TheMixed IUGR (MIUGR) group contained patients with co-existing features of the twogroups above. Pre-term control (PTC): Birth weight >20th centile, no abnormalumbilical artery Doppler measurements, BP < 140/90, no history of gestationaldiabetes, no histologic evidence of chorio-amnionitis. First and early secondtrimester villous tissues from elective social terminations of pregnancy as well as
* Corresponding author. Tel.: þ1 416 586 4800x8322; fax: þ1 416 586 5116.E-mail address: [email protected] (S. Drewlo).
Contents lists available at SciVerse ScienceDirect
Placenta
journal homepage: www.elsevier .com/locate/placenta
0143-4004/$ e see front matter � 2012 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.placenta.2012.09.007
Placenta 33 (2012) 952e954
levytska
Text Box
Appendix 1

healthy term vaginal deliveries as well as group which underwent caesarian section(c/s), control placentas (>37 þ nweeks gestation) were also collected for gestationalage profile studies.
Immediately after delivery, placental weight was recorded and four 2e3 cm2
tissue cores through the full thickness of the placenta were obtained from a sitewithin each quadrant, avoiding areas with obvious evidence of thrombosis orother gross abnormalities. Chorionic plate tissue was removed. The resultantcores of villous tissue were rinsed briefly in chilled phosphate-buffered saline(PBS) to remove residual blood and further dissected to generate 0.5e1 cm3
pieces. Pooled samples, from individual placentas were generated containingone piece of tissue from each of the four cores then snap-frozen. RNA was iso-lated using the QiaZol� extraction kit (Qiagen), then quantified and quality-controlled using Nanodrop (Thermo Fisher) and Experion RNA chips (Bio-Rad).Respectively, 1 mg of total RNA from all samples was reverse-transcribed simul-taneously using the BIORAD i-Script Supermix (Bio-Rad). cDNA samples (10 ng)
were pipetted with a robot from Perkin Elmer (total volume 7 ml, with LuminoCTfrom Sigma Mastermix ¼ 3.5 ml per PCR reaction) and run on the CFX Bio-Rad384 PCR machine. All samples were run at the same time per gene to avoidinter-assay variations with the following PCR protocol: initial 95 �C for 5 minfollowed by 38 cycles of 95 �C for 15 s and 60 �C for 20 s. We evaluated 8commonly-used HG genes in placental research: TBP, HPRT, GAPDH, SDHA, TOP1,CYC, YWHAZ, and beta2M and designed or used previously published primerswith an efficiency of at least 95% (sequences are summarized in SupplementalTable 1). We isolated a total of 90 samples of RNA from 9 different clinicalgroups of placental material to search for ideal housekeeping genes applicable toall conditions. These groups are summarized in Table 1 and encompass healthyfirst trimester (early 6e8 weeks and late 9e12 weeks), healthy second trimester,preterm controls (before 34 weeks), term controls, severe early onset intra-uterine growth restriction (IUGR) and severe pre-eclampsia (PET) as well asa mixed PE-IUGR group (MIUGR).
Abbreviation
AEDFV absent end diastolic flow velocityREDFV reversed end diastolic flow velocityBeta2M beta-2-microglobulinCYC1 cytochrome c-1cDNA complimentary deoxyribonucleic acidGAPDH glyceraldehyde-3-phosphate dehydrogenaseHK housekeepingHPRT hypoxanthine phosphoribosyltransferasesIUGR Severe intrauterine growth restrictionMIUGR mixed pre-eclampsia and intrauterine growth
restrictionmRNA messenger ribonucleic acid
MSH Mount Sinai HospitalOD optical densityPBS phosphate-buffered salinesPE severe pre-eclampsiaPTC pre-term controlqRT-PCR quantitative real-time polymerase chain reactionRCWIH Research Centre for Women’s and Infants’ HealthTBP TATA box-binding proteinTC term controlTOP1 DNA topoisomerase 1SDHA succinate dehydrogenase complex, subunit A,
flavoprotein (Fp)YWHAZ tyrosine 3-monooxygenase/tryptophan 5-
monooxygenase activation protein, zeta polypeptide
Table 1Patient data summary.
Groupsa TCb vTermc MIUGR sIUGR sPE Early pregnancy group
PTC 5e7Weeks
8e12Weeks
13e18Weeks
N 10 11 11 9 10 9 10 10 10Maternal age(years)
28.6 � 6.4 36.6 � 3.4 32.4 � 9.8 32.3 � 7.9 31 � 4.1 33 � 4.2
Gravida 2 � 0.7 3 � 1.8 3 � 1.4 2.3 � 2.1 2 � 1.0 2 � 1.0Para 0.4 � 0.7 1 � 0.8 1 � 1.0 1 � 1.1 1 � 1 1 � 0.8Gestational age(weeks)
32 � 2.1 39 � 0.8 40 � 1 29 � 2.2 31 � 2.8 29.7 � 1.6 6 � 0.9 10 � 1.1 15 � 1.5
Ethnicity Black 2 2 1 0 2 5Caucasian 7 9 9 6 1 2Asian 0 1 1 2 5 1Other 0 0 0 0 2 1N/A 1 0 0 1 0 0
Systolic BP > 140mmHg No 8 4 11 0 10 0Yes 0 2 0 8 0 9N/A 1 5 0 1 0 0
Diastolic BP > 90 mmHg No 8 11 11 2 10 0Yes 0 0 0 5 0 9N/A 1 0 0 1 0 0
Abnormal umbilicalcord doppler(AEDV,REDFV)
0 0 0 9 10 0
Sex Male 7 3 8 3 6 4Female 2 6 3 6 4 5N/A 0 2 0 0 0 0Birth weight (g) 2057 � 505.7 3576 � 112.4 3482 � 115 804 � 259.0 933 � 278.8 1337 � 480
Placental weight (g) Wet 449 � 137.7 589 � 178.5 580 � 113 209 � 73.4 300 � 143.4 338 � 58
Severe intrauterine growth restriction (IUGR): Birth weight �10%ile, abnormal umbilical artery Doppler (absent end diastolic flow velocity (AEDFV) or reversed end diastolicflow velocity (REDFV)), normotensive women.. Severe pre-eclampsia (PET): Birth weight>10%ile, BP> 140/90, proteinuria>300 mg/day or�1þ on dipstick. The Mixed IUGR(MIUGR) group contained patients with co-existing features of the two groups above.
a Pre-term control (PTC): Birth weight >20th centile, no abnormal umbilical artery Doppler measurements, BP < 140/90, no history of gestational diabetes, no histologicevidence of chorio-amnionitis.
b Healthy term delivery by caesarian section.c Healthy term vaginal delivery, (>37 þ n weeks gestation).
S. Drewlo et al. / Placenta 33 (2012) 952e954 953

3. Results and discussion
We were able to show that freshly extracted RNA from patho-logical as well as normal tissues can be partially degraded underour standardized collection conditions, when analysed with theExperion RNA chip. Even if the OD values from the Nanodropprovided perfect results (OD¼ 2), up to 29% of all samples collectedshowed at least partial degradation (Experion QC values below<6.5 were excluded). These changes have previously been shown topotentially influence cDNA conversion and PCR performance [6].We highly suggest monitoring RNA integrity with a bioanalyzer orcomparable method, at least in a selected number of samples.
After the PCR run, we tested the expression stability of our HKgenes in all nine groups.We used the GeNormmethod published byVandesompele (2002)(2), which is part of the Biogazelle� softwarepackage. The software calculates the stability of each HK geneM fora reference gene as the average pairwise variation V for that genewith all other tested reference genes. Stepwise exclusion of thegene with the highest M value allows ranking of the tested genesaccording to their expression stability. This results in different Vscores. A V score �0.15 is desired as a cut-off and was determinedby the fact that the addition of another HK gene would not signif-icantly improve the sensitivity of the normalization [2]. We fol-lowed these rules to determine the best HK gene combinations forthe different groups and summarized these data in Table 2.
Wewere able to extend previously published data as follows. Aspredicted, specific HK genes were differentially regulated in thedifferent groups and, thus, did not meet HK gene criteria. The most
stable genes for analysing gestational changes were YWHAZ, TBPand CYC1. If PTC was included in this group, the following HK geneswere identified as appropriate controls: TOP1, TBP and CYC1. Whencomparing pathologies (sPE and sIUGR) with preterm and termcontrols, TOP1, TBP and CYC1 again gave the best results, which didnot change with the addition of the MIUGR group to the samplepool. We furthermore investigated if labour has an influence onhousekeeping gene stability by comparing vaginal deliveries versuscaesarian sections. We were able to show differential regulation ofTBP and HPRT in these groups (Supplemental Table 2). The moststable housekeeping genes were TOP1, CYC1 and YWAHZ.
Finally, if all nine groups are assessed our data indicates thatTOP1, CYC1 and YWHAZ are the most stable HK genes.
Our datawill assist researchers in choosing the appropriate HKGfor their experimental setup, although an initial validation of thehouse keeping genes in a specific sample population is highlyrecommended.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.placenta.2012.09.007.
References
[1] Drewlo S, Levytska K, Sobel M, Baczyk D, Lye SJ, Kingdom JCP. Heparin promotessoluble VEGF receptor expression in human placental villi to impair endothelialVEGF signaling. Journal of Thrombosis and Haemostasis: JTH 2011-Dec;9(12):2486e97.
[2] Vandesompele J, De Preter K, Pattyn F, Poppe B, Van Roy N, De Paepe A, et al.Accurate normalization of real-time quantitative RT-PCR data by geometricaveraging of multiple internal control genes [Research Support, Non-U.S. Gov’t].Genome Biology 2002 Jun 18;3(7). RESEARCH0034.
[3] Meller M, Vadachkoria S, Luthy DA, Williams MA. Evaluation of housekeepinggenes in placental comparative expression studies. Placenta 2005 SepeOct;26(8e9):601e7.
[4] Murthi P, Fitzpatrick E, Borg AJ, Donath S, Brennecke SP, Kalionis BGAPDH.18S rRNA and YWHAZ are suitable endogenous reference genes for relativegene expression studies in placental tissues from human idiopathic fetalgrowth restriction [Research Support, Non-U.S. Gov’t]. Placenta 2008 Sep;29(9):798e801.
[5] Patel P, Boyd CA, Johnston DG, Williamson C. Analysis of GAPDH as a standardfor gene expression quantification in human placenta [Letter Research Support,Non-U.S. Gov’t]. Placenta 2002 SepeOct;23(8e9):697e8.
[6] Fleige S, Pfaffl MW. RNA integrity and the effect on the real-time qRT-PCRperformance [Review]. Molecular Aspects of Medicine 2006 ApreJun;27(2e3):126e39.
Table 2Choice of housekeeping gene by clinical groupings.
Sample groups HKG. 3 HKG. 2 HKG. 1
First, second and term non-labour CS þvaginal delivery
TOP1 YWHZ CYC1
First, second and term non-labour CS YWHAZ TBP CYC1First, second, PTC and term non-labour CS TOP1 TBP CYC1sPE, sIUGR, PTC and term non-labour CS TOP1 TBP CYC1sPE, sIUGR, MIX, PTC, and term non-labour CS TOP1 TBP CYC1All groups combined TOP1 YWHAZ CYC1Vaginal delivery versus CS at term TOP1 CYC1 YWHAZ
HKG ¼ Housekeeping genes. HKG.1 most stable > HKG.2 > HKG.3; HKG1 and 2provide a variation index of <0.15 in each group.sPE ¼ severe pre-eclampsia, sIUGR ¼ severe intra uterine growth restriction,MIX ¼ mixed elements of sIUR and sPE, CS ¼ Cesarean section.
S. Drewlo et al. / Placenta 33 (2012) 952e954954

at SciVerse ScienceDirect
Placenta 34 (2013) 291e298
Contents lists available
Placenta
journal homepage: www.elsevier .com/locate/placenta
Current topic
Heme oxygenase-1 in placental development and pathology
K. Levytska a,b, J. Kingdoma,b,c,d, D. Baczyk a, S. Drewlo a,*
a Program in Development and Fetal Health, Samuel Lunenfeld Research Institute, Mount Sinai Hospital, CanadabDepartment of Laboratory Medicine and Pathobiology, University of Toronto, CanadacMaternal-Fetal Medicine Division, Department of Obstetrics and Gynecology, Mount Sinai Hospital, CanadadDepartment of Obstetrics and Gynecology, University of Toronto, Toronto, Canada
a r t i c l e i n f o
Article history:Accepted 12 January 2013
Keywords:Heme oxygenase-1Pre-eclampsiaPlacentasFLT-1
* Corresponding author. Samuel Lunenfeld Researcpital, 25 Orde St., Room 6-1020, Toronto, ON M5T 34800x8322.
E-mail addresses: [email protected], drewlo@ms
0143-4004/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.placenta.2013.01.004
a b s t r a c t
Pregnancy is accompanied by several adaptations in the mother, such as increased blood volume, highercardiac output and reduced peripheral vascular resistance. Inability to accomplish these changes placesboth her and her pregnancy at risk of major placental complications such severe pre-eclampsia (sPE) orsevere intra-uterine growth restriction (sIUGR). sPE is characterized by wide-spread maternal vasculardysfunction expressed as increased systemic vascular resistance; this state is accompanied by elevatedlevels of anti-angiogenic factors and lower production of vasodilatory gases. One of the key moleculesimplicated in sPE pathogenesis is heme oxygenase-1 (HO-1), a rate-limiting enzyme that breaks downheme into carbon monoxide (CO), biliverdin and free iron. CO and bilirubin (a downstream product ofbiliverdin processing) account for the angiogenic, vasodilatory and anti-oxidant properties of HO-1.These collective actions of the heme breakdown metabolites generated by HO-1 offer protectionagainst cytotoxicity, inflammation, hypoxia and other forms of cellular stress that are central to thepathogenesis of sPE. Placental HO-1 expression and exhaled CO levels are both lower in womenwith sPE,consistent with a pathogenic role of HO-1. In vitro experiments demonstrate that induction of HO-1downregulates secretion of the anti-angiogenic factor soluble fms-like tyrosine kinase-1 (sFLT-1) andincreases CO production. Advancing our understanding of regulatory pathways promoting placental HO-1 expression may offer new pharmacological tools to reduce maternal and perinatal morbidity in severeplacental insufficiency syndromes, especially in women at greatest risk of developing sPE.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Successful human pregnancy is accompanied by hemodynamicand immune changes in the mother to ensure proper embryo im-plantation and further fetal development. In normal pregnancy,both maternal cardiac output and blood volume increase by 30e45%; these changes support an exponential rise in utero-placentalblood flow that is needed to support the demands of the growingfetus [1,2]. These cardiovascular changes alone would predicta significant elevation in blood pressure were it not for the sub-stantial reduction in systemic vascular resistance that occurs in thesecond trimester. These maternal hemodynamic adaptations areoften defective in placental complications of pregnancy, especiallyin severe pre-eclampsia (sPE), where women exhibit unaltered, or
h Institute, Mount Sinai Hos-H7, Canada. Tel.: þ1 416 586
hri.on.ca (S. Drewlo).
All rights reserved.
decreased, cardiac output and a large increase in peripheral vascularresistance [3]. High peripheral vascular resistance implies systemicendothelial cell dysfunction in the mother and precedes thedevelopment of overt hypertension, one of the hallmarks of sPE.Systemic vasoconstriction and blood volume contraction, in tandemwith diseased utero-placental arteries, lead to unstable blood flowto the intervillous space [4]. The resultant ischemia-reperfusioninjury suppresses cytotrophoblast proliferation leading to syncy-tiotrophoblast damage and placental infarcts, eventually resultingin intrauterine growth restriction (IUGR) [5,6]. Ischemia-reperfusion injury may create a potent feed-forward loop for vas-cular dysfunction and severe hypertension in sPE that, at present,can only be reversed by delivery of the fetus and placenta.
The manifestation of maternal vascular dysfunction and hy-pertension stems from the imbalance between pro- and anti-angiogenic factors in maternal blood, and partially due toa decrease in production of vasodilatory gases (such as nitric oxide,carbon monoxide and hydrogen sulfide) [7e9]. The wide-spreadendothelial cell dysfunction resulting in maternal hypertension,proteinuria and generalized edema is, in part, attributed to the
levytska
Text Box
Appendix 2

K. Levytska et al. / Placenta 34 (2013) 291e298292
soluble fms-like tyrosine kinase-1 (sFLT-1) [10]. Excess levels ofsFLT-1, a decoy protein for the vascular endothelial growth factor(VEGF), shift the net angiogenic factor signaling response towardsan anti-angiogenic phenotype [11]. sFLT-1 levels are elevated inwomen destined to develop sPE, implicating a role for this mole-cule in disease pathogenesis [12]. Ameliorating the negative effectsof excess sFLT-1 via pharmacological and other means has been thefocus of several studies [13e15]. Recently, it has been shown thatthe induction of a cytoprotective enzyme heme oxygenase-1 (HO-1) may help ameliorate the wide-spread anti-angiogenic pheno-type by decreasing the levels of anti-angiogenic factors, such assFLT-1 and others, possibly via the actions of carbon monoxide(CO) [15,16]. Properties of HO-1, as discussed in this review, haveled researchers to suggest that HO-1 and its downstream factorsare potential therapeutic targets in sPE treatment and prevention[17e19].
Fig. 1. Schematic representation of heme breakdown by HO-1. HO-1 is responsible forheme metabolism within the cell. The process requires NADPH-cytochrome-P450reductase and molecular oxygen (O2) which act as a co-enzyme and a substrate,respectively, for HO-1. HO-1 breaks down heme into three equimolar components:iron (Fe2þ), biliverdin (immediately converted to bilirubin by biliverdin reductase), andCO. These metabolites are responsible for vasodilatory, anti-oxidant and other pro-tective properties of HO-1.
2. Heme oxygenases
Three isoforms of heme oxygenase have been described: HO-1,HO-2 and HO-3 [20,21]. HO-1, the only inducible HO isoform, ishighly expressed in tissues responsible for heme metabolism, suchas spleen and liver [22]. HO-2 is constitutively-expressed andmostly found in the brain and testes [20]. The function of HO-3 ispresently unknown, but the enzyme is believed to be inactive. HO-1, a type I integral protein embedded in smooth ER membrane, wasfirst isolated from spleen and liver microsomal fractions and shownto catalyze the rate-limiting step of intracellular heme breakdown[23]. Using oxygen, the enzyme metabolizes heme into threecomponents produced in equimolar amounts: carbon monoxide(CO), biliverdin and iron (Feþ2) [24]. Under physiological condi-tions, biliverdin is immediately converted into bilirubin by bili-verdin reductase. The twometabolites of heme breakdown, CO andbilirubin, have important cellular functions giving HO-1 its vaso-dilatory, anti-inflammatory, anti-apoptotic, anti-oxidant, andcytoprotective properties (Fig. 1) [25e32].
Analyses of HO-1 gene deficiency and promoter polymorphismshave emphasized the importance of this enzyme in growth andhomeostasis. The first case of HO-1 deficiency in humans wasreported in a 6-year old boy who had both alleles of the genemutated [33]. He presented with growth restriction, anemia, ele-vated iron deposition in renal and hepatic tissues, and susceptibilityto oxidative stress. These symptoms were accompanied by lowbilirubin plasma levels and profound endothelial cell damage,illustrating the cytoprotective qualities of HO-1. Subsequent geneticstudies of HMOX-1 (gene coding for HO-1) have identified an as-sociation between the number of nucleotide repeats [(GT)n repeats]in the promoter region and either cardiovascular diseases or preg-nancy complications [34e37]. Generally, longer (GT)n repeats in thepromoter correlate with lower HO-1 expression and activity andhave been shown to be associated with a higher risk of recurrentmiscarriage [34]. Conversely, short (�25 (GT)n) repeats in the pro-moter protect against oxidative stress and lower the risk of coronaryheart disease [37]. Some studies do not support this general hy-pothesis. For example, the presence of a medium or longer-sized(GT)n repeat variant in at least one of the alleles was shown tocorrelate with a lower risk of chronic hypertension and a lowersystolic blood pressure in the Chinese Han population [35]. Sur-prisingly, one study found that the AA genotype of T(-413)A locus(vs. TT and TA genotype), which is associated with an increasedexpression of HO-1, was more common in hypertensive women ofJapanese descent [36]. Although it appears that disrupted functionof the HMOX-1 gene may participate in the pathogenesis of car-diovascular and reproductive diseases, at present, no data exist
exploring a potential association between HMOX-1 promoterpolymorphisms and placental insufficiency syndromes.
3. Heme oxygenase expression in pregnancy
Studies of HO-1 and HO-2 expression in mouse, rat and humanplacentas have been numerous [38e42]. However, since the firstreport localizing HO to human placental tissue, studies of HO-1expression throughout human gestation and in pathology havebeen inconsistent. The expression patterns and activity of HO-1 inthe rodent and human placenta are summarized in Tables 1 and 2,respectively. McLean and colleagues were the first group to dem-onstrate HO-1 and HO-2 expression in the human placenta,showing that HO-2 protein was more abundant than HO-1 at term[43]. Yoshiki et al. reported that HO-1 and HO-2 proteins arelocalized in different cell types in the human placenta: HO-1immunohistochemistry revealed positive staining in the syncytio-trophoblast layer with traces in the underlying cytotrophoblasts,while HO-2 was mostly expressed in endothelial and smoothmuscle cells [44]. This group also showed that HO-1 expression didnot change throughout gestation, while HO-2 expression increasedtowards term. Differential expression of HO-1 in the invadingcytotrophoblast cell columns has been noted; HO-1was found to behigh in distal, but drastically decreased, in the proximal cell layers[41]. The first study looking at the expression of HO-1 in pregnancycomplications showed lower HO-1 protein expression in pre-eclamptic (PE) placentas; this was in contrast to a positive associ-ation between placental HO-1 expression and feto-placental vas-cularization in normal pregnancy [26]. In support of pathologic sPEobservations, human in vivo studies demonstrate that whileexhaled CO levels increase throughout gestation in healthy women,end-tidal CO measurements are lower in hypertensive pregnant

Table 1Summary of HO-1 and HO-2 expression and function in rodents.
Category Description References
Expression over gestation Placental HO-1 expression and HO activity peaks at E14.5 and decreases towardsterm (mouse)
Watanabe et al., 2004Zhao et al., 2008
Placental HO activity peaks on d21 of pregnancy; HO-1 and HO-2 expressionhighest on d19, HO-1 mRNA highest on d16 (rat)
Kreiser et al., 2003
Placental localization HO-1 protein localized to junction zone, predominantly to spongiotrophoblast cells(mouse)
Watanabe et al., 2004Zhao et al., 2009
HO-1 and HO-2 protein primarily expressed in the syncytiotrophoblast region (rat) Kreiser et al., 2003Expression in hypoxia or
hypoxia-reperfusion injuryHO-1 downregulated in placental tissue following 48 h of hypoxia (rat) George et al., 2012HO-1 downregulated in plasma of RUPP-treated rats George et al., 2011
McCarthy et al., 2011Expression in pregnancy
complicationsReduced placental HO-1 expression in model of spontaneous expression (mouse) Sollwedel et al., 2005
Zenclussen et al., 2005Zenclussen et al., 2006
Reduced HO-1 expression in IL-12-induced model of abortion (mouse) Zenclussen et al., 2002Genetic studies First HO-1 knock-out model (mouse) Poss & Tonegawa, 1997
Effect of HO-1 deficiency on placentation (mouse) Zhao et al., 2009Effect of maternal HO-1 deficiency on placental development (mouse) Zhao et al., 2011Effect of HO-1 deletion on inflammatory responses (mouse) Kapturczak et al., 2004
HO roles in placenta andrelated models
Inflammation, immunity Schumacher et al., 2012George et al., 2012Kapturczak et al., 2004
Cytoprotection George et al., 2012Brouard et al., 2000Tachibana et al., 2011Sollwedel et al., 2005
Muscle relaxation, vasodilatation Zhao et al., 2008Morita et al., 1995
K. Levytska et al. / Placenta 34 (2013) 291e298 293
women, especially those affected by sPE, supporting the role of COas a physiologic vasodilator implicated in gestational hemodynamicchanges [9,45]. Furthermore, Zenclussen et al. found lower HO-2protein levels in spontaneous abortion (SA) cases (vs. normalpregnancy) and in PE (vs. age-matched controls), while HO-1 levelswere low across all pathologies without significant differences [46].Lash et al. found that infarcted villi in PE placentas had lower HOactivity and lower expression of HO-2 while HO-1 expression wasunaffected [47]. In contrast to above studies, Barber et al. showedthat HO-1 protein was undetectable in human placenta, and therewas no difference in HO-2 expression between PE and growthrestricted pregnancies and preterm controls [48]. These studiesshow that discrepancies regarding the expression of HO-1 and HO-2 in disease states and throughout gestation exist and may be dueto intra- and inter-tissue heterogeneity.
4. HO-1 in hypoxic models of “utero-placental vascularinsufficiency”
Maternal vasoconstriction characteristic of sPE leads to inad-equate blood supply to the intervillous space, hypoxia-reperfusioninjury and tissue necrosis (infarcts) [5,49]. In attempts to recapit-ulate these conditions ex vivo, placental tissue hypoxia has been themodel of choice. It is well-established that HO-1 activity decreaseswith decreased oxygen availability since molecular oxygen is one ofthe substrates required for heme breakdown [50]. However,although HO-1 expression has been shown to increase in responseto hypoxia in several organ systems, placental HO response tohypoxia has not been established [51e53]. For example, Appletonet al. showed that HO-2 expression in term placental tissue is un-affected by different oxygen tensions and HO-1, which showeda very low expression overall, also was unaffected by manipulatingoxygen tension [54]. Furthermore, HO-1 and HO-2 expression inresponse to hypoxia-reperfusion injury was measured in termplacental explants and no differences in HO-1 or HO-2 levels werefound [55]. In contrast, in d19 rat placental tissue, HO-1 expressiondecreased following a 48-h exposure to hypoxic culture conditions
[56]. Hypoxia in the established placental ischemia (or reduceduterine perfusion pressure, RUPP) model in the rat has also resultedin a decrease of circulating plasma HO-1 levels [57]. Thus, studieson human placental explants challenge the central hypothesis thathypoxia and/or hypoxia-reperfusion injury alone is a good ex vivomodel for sPE, since while placental expression of HO-1 is reducedin sPE, this finding cannot be recapitulated in hypoxic tissue cultureexperiments. Possible explanations include explant gestational ageand tissue heterogeneity, relevance of a simple hypoxic protocol vs.the more likely ischemia-reperfusion injury model (that may bemore potent at reducing syncytiotrophoblast protein translation),and others [6]. Hypoxia is the postulated feature of sPE and oxygenis an important factor in human and murine placental develop-ment. Prolonged hypoxia in disease states leads to reactive oxygenspecies accumulation and oxidative damage and contributes toplacental insufficiency. Although hypoxic stress is not the onlycause of placental syndromes, it is one of the factors in the etiologyof disease; thus, hypoxia remains as one of the best models avail-able to researchers in their attempts to understand the physiologyof the placenta and the underlying mechanisms of disease.
5. Role of HO-1 in models of spontaneous abortion
Pregnancy is a state of balance between immune tolerance andimmune suppression in the mother to allow her to tolerate thepresence of the “foreign” material, that is, the fetus (reviewed inRef. [58]). Several immune responses occur during pregnancy,including the shift in balance of pro- and anti-inflammatory cyto-kines towards the latter [59,60]. The balance between anti-inflammatory helper T type 2 (Th2) cytokines (such as IL-4, IL-10,TGF-b) and pro-inflammatory helper T type 1 (Th1) cytokines (suchas IL-2, IFN-g, TNF-a) has been studied in pregnancy complicationsand models; while normal pregnancy has been labeled as a Th2phenomenon, this observation does not hold true in pregnancycomplications [60e64]. Consequently, it has been shown that fol-lowing exposure to trophoblast cell-conditioned media, the secre-ted ratio of Th1/Th2 cytokines from T lymphocytes decreases,

Table 2Summary of HO-1 and HO-2 expression and function in humans and human cell-based models.
Category Description References
Expression over gestation First localizations of HO-1 and HO-2 proteins in placental tissue McLean et al., 2000No differences in HO-1 RNA or protein expression between firsttrimester and term placentas; HO-2 RNA and protein increasedtowards term
Yoshiki et al., 2000
HO-1 protein expression increases towards term Ahmed et al., 2000HO-2 protein expression higher in endothelial cells at term Lyall et al., 2000
Placental localization HO-1 found in syncytiotrophoblast with traces in cytotrophoblast;HO-2 expressed in endothelial and smooth muscle cells
Yoshiki et al., 2000
HO-2 expressed in syncytiotrophoblast, endothelial cells,cytotrophoblast cells in cell columns and shell; HO-1 stronglyexpressed in distal, but not proximal, layers of invadingcytrotrophoblast cell columns
Lyall et al., 2000
HO-2 protein expressed in vascular endothelium, smooth musclecells and syncytiotrophoblast; HO-1 expression in syncytiotrophoblastand vascular endothelium, less abundant than HO-2
McLean et al., 2000
Expression in hypoxia orhypoxia-reperfusion injury
Lower HO-1 expression than HO-2; neither is affected by hypoxiain term explants
Appleton et al., 2003
HO-1 and HO-2 expression unaffected by fluctuating O2
concentrations in term explantsMcCaig & Lyall, 2009
Expression in pregnancycomplications
Decreased HO-1 protein expression in PE Ahmed et al., 2000Lower HO activity in infacted regions of PE placentas; HO-2 levelsdecreased in infracted PE regions, while HO-1 protein expressiondid not change
Lash et al., 2008
Reduced HO-2 expression in SA vs. normal pregnancy, andPE vs. age-matched controls; low HO-1 protein expression acrosspathologies and not different from age-matched controls
Zenchlussen et al., 2003
HO activity did not differ between mild PE and normotensivepregnancies; higher HO-1 protein expression in chorionic villi;no differences in HO-2 expression
McLaughlin et al., 2003
No differences in placental bed expression of HO-1 and HO-2 inPE and fetal growth restricted (FGR) cases; HO-2 lower inendothelial cells in PE and FGR
Barber et al., 2001
Genetic studies Human HO-1 gene mutation Yachi et al., 1999HMOX-1 promoter polymorphisms Denschlag et al., 2004
Lin et al., 2011Ono et al., 2003Chen et al., 2012
HO roles in placenta andrelated models
Inflammation, immunity Neuzil et al., 1994Ahmed et al., 2000Kweider et al., 2011
Cell migration and fusion, angiogenesis Cudmore et al., 2007Cudmore et al., 2011Bilban et al., 2009McCaig et al., 2009
Muscle relaxation, vasodilatation Bainbridge et al., 2002Acevedo & Ahmed, 1998Coceani et al., 1993Kreiser et al., 2004Baum et al., 2000
K. Levytska et al. / Placenta 34 (2013) 291e298294
suggesting that the presence of trophoblast cells promotes an anti-inflammatory environment [63]. Several studies have looked at thebalance between Th1 and Th2 cytokines during pregnancy andshowed, for example, that administration of IL-10, a Th2 cytokine,to pregnant rats suffering from endothelial cell dysfunction andhypertension improved pregnancy outcomes [65]. Connection hasbeen shown between Th2 cytokines and HO-1, for example, whereIL-10 increased the expression of HO-1 in murine macrophages andexerted its anti-inflammatory effects via the production of CO [66].Furthermore, pregnancy is characterized by an expansion of anti-inflammatory regulatory T (Treg) cell population, which is knownto contribute to implantation and early pregnancy maintenance;implicating their role in pregnancy complications is the finding thatTreg cell numbers are lower in human and murine abortion-pronepregnancies [67e69]. Collectively, the placenta and maternalhelper T cells contribute to the creation of a favorable, tolerantmaternal environment which will support the developing fetus.These and other adaptations in the maternal immune responsecontribute to proper embryo implantation, establishment anddevelopment.
Aberrant immune response is one of the key features in murinemodels of spontaneous abortion (SA); conversely, the introductionof pro-inflammatory cytokines can be used to induce abortion inmice [70]. The role of HO-1 in human and murine models ofabortion as well as its role in the maternal immune response hasbeen explored recently. Women with pregnancies ending inspontaneous abortions have a specific HMOX-1 promoter poly-morphism leading to a lower expression of HO-1 [34]. Studies havealso shown reduced levels of placental and decidual HO-1 expres-sion in a murine SA model [62,71,72]. Furthermore, it has beenshown that adenoviral delivery of HO-1 to SA mice is able toameliorate the abortion rates by increasing the IL-4/IFN-g ratio inspleen lymphocytes, as well as decreasing apoptosis at the fetoematernal interface [73]. Additionally, it was shown that the trans-fer of pregnancy-induced Treg cells (which are particularlyimportant for early stages of pregnancy) from healthy pregnantmice into abortion-prone mice decreased fetal rejection rates andincreased the levels of HO-1 and TGF-b at the fetoematernalinterface, without affecting the Th1/Th2 ratio, however [71]. Inanother study, inducing HO-1 activity pharmacologically led to

K. Levytska et al. / Placenta 34 (2013) 291e298 295
a rise in the expression of an anti-apoptotic factor Bag-1 at thefetoematernal interface and increased the activation of Treg cells,collectively resulting in a lower SA rate [62]. Further supporting therole of HO-1 in pregnancy maintenance was a study showing thatblocking the activity of HO-1 with zinc protoporphyrin IX (ZnPPIX)increased abortion rates in normal as well as in abortion-pronepregnancies and abrogated the protective effects of Treg celltransfer into abortion-prone mice [74]. Furthermore, induction ofabortion in mice with IL-12, a cytokine which upregulates thesecretion of Th1 cytokines, decreased HO-1 and HO-2 expression,led to placental necrosis and hemorrhage and, subsequently, fetalrejection [70]. Collectively, studies suggest that HO-1 contributes toproper placental development and pregnancy maintenance in micevia its anti-apoptotic properties and plays a role in the induction ofa tolerant, favorable environment throughout gestation.
6. Physiology of HO-1 in placentation and cell-based models
The first description of an HO-1 knockout systemwas publishedby Poss and Tonegawa in 1997 [75,76]. The authors found that HO-1is required for proper iron reutilization, since adult mice lackingHO-1 developed anemia and were susceptible to oxidative tissuedamage and inflammation [76]. Furthermore, the group showedthat murine embryonic fibroblast cells lacking HO-1 were sensitiveto oxidative stress [75]. Kapturczak et al. showed that mice lackingHO-1 had impaired immune responses and higher levels of pro-inflammatory Th1 factors [77]. Zhao and colleagues were the firstgroup to provide evidence for HO-1 as a critical player in properplacental development [40,78,79]. The group demonstrated that innormal pregnancy, mice exhibit an increase in utero-placentalblood flow accompanied by a significant increase in maternalabdominal aorta diameter (adaptations similar to those observed inhumans). These changes were concurrent with higher endogenousCO production, elevated plasma bilirubin levels, and placental HO-1expression which peaked at E13.5 [40,79]. In a follow-up study,Zhao et al. characterized the effect of HO-1 deficiency on placentaldevelopment [78]. Crossing Hmox-1 heterozygous (þ/�) miceresulted in an altered Mendelian ratio of Hmox-1�/� pups (2.4%instead of the expected 25% ratio), most of which aborted beforeE10.5. Hmox-1þ/� placentas presented with a thinner spongio-trophoblast (SP) layer due to increased apoptosis at the junctionzone, supporting the role of HO-1 as an anti-apoptotic player [78].The implantation rate in heterozygous crossbreedings was lower,and, at E12.5 and E15.5, the placentas were lighter and smaller(compared to wildtype breedings). Furthermore, heterozygousmothers had higher plasma levels of sFlt-1, one of the key players invascular endothelial cell dysfunction, and elevated diastolic bloodpressure, implying that Hmox-1 is involved in the manifestation ofsPE-like symptoms in mice, mimicking complications seen inhumans [80]. It was later shown that inadequate placentation ofHmox-1�/� placentas resulted in IUGR and subsequent fetal death[18]. Exogenous application of CO, a product of heme metabolismby HO-1, to Hmox-1-deficient mice during the implantation win-dow decreased fetal death in these pregnancies. It was also shownthat Hmox-1þ/þ blastocysts isolated from mice on E3.5 attachedsooner thanHmox-1þ/� blastocysts while blastocysts lacking Hmox-1 failed to attach altogether [18]. This study also characterized theeffect of Hmox-1 deficiency on placentation showing that Hmox-1is necessary for the differentiation of trophoblast stem cells togiant cells which are critical for proper placental development.Early placental vascularization is also affected by Hmox-1 as seenfrom studies of crossbreeding Hmox-1 wildtype mice and Hmox-1heterozygous mice [80]. Breeding female mice partially deficientin Hmox-1 with males of the same genotype resulted infetoematernal interface malformations; namely, lower
microvasculature blood vessel volumes, less sinusoid spaces in thelabyrinth and disorganized capillaries, when compared to wildtypebreedings. Interestingly, these alterations in placental morphologywere independent of the placental genotypes and occurred in both,Hmox-1þ/þ and Hmox-1þ/� placentas, as long as both parents wereHmox-1 deficient. Since these impaired features of placentaldevelopment are similar to those observed in pregnancy compli-cations such as sPE, the role of HO-1 in implantation and placentaldevelopment is further supported.
Cell models have also served as a useful tool to study HO-1properties which include protection against cytotoxicity and celldeath induction of an angiogenic phenotype, and others. HO-1 hasbeen studied in cell models related to pregnancy and placentaldevelopment, such as human umbilical vein endothelial cells(HUVECs), HTR8 cells (a model for extravillous trophoblast cells,EVTs), and BeWo cells (a model for syncytiotrophoblast formation).The activation of HO-1 by nuclear factor (erythroid-derived 2)-like2 (Nrf-2), a prominent protector against oxidative stress, wasdescribed in the BeWo cell model, where it protected cells againsthydrogen peroxide- and Feþ2-induced stress [81]. Interestingly,a cleaved isoform of HO-1 has been shown to have transcriptionfactor-like activity by contributing to the expression of cytopro-tective genes in cultured fibroblast and Hepa cells [82]. Geneticprofiling of highly migratory EVTs and villous cytotrophoblast (CT)cells (with a low migratory potential) isolated from cultured ex-plants and first trimester human placentas, respectively, showeda lower expression of HO-1 in EVTs vs. CTs [83]. Confirming thesefindings, the group also showed that CT cells had higher HO-1 RNAexpression compared to EVT cells, as well as higher HO-1 proteinexpression in proliferating CTs (vs. EVTs) in first trimester placentalexplants, as seen by immunohistochemistry. Furthermore, thestudy showed that retroviral induction of HO-1 in naturally-migratory HTR-8 cells reduced their motility, while HO-1 silenc-ing in non-migratory BeWo cells increased their migration, sug-gesting that lower HO-1 expression is associated with a lower cellmotility and trophoblast invasion. Interestingly, the mechanismresponsible for increasing cell migration by HO-1 was via the reg-ulation of another factor, a nuclear receptor peroxisomeproliferator-activated receptor-gamma (PPAR-g) which, as will bediscussed shortly, has been shown to affect cell migration and in-vasion [83]. These findings are in contrast to the study by McCaiget al. who showed that inhibition of global HO activity with zincprotoporphyrin IX and antibody-mediated inhibition of HO-2reduced invasion of primary CT cells in vitro [55]. Discrepancies instudies of how HO affects cell invasion and motility may be due tothe use of different cell models; CT cells isolated from term pla-centas (when invasion is no longer prominent) in the study byMcCaig et al. provide a different model compared to Bilban et al.,who used CT cells isolated from first trimester tissue (when inva-sion is high). Furthermore, cell models used by Bilban et al. arerepresentative of the early placental development stages and, thus,might reflect the actions of HO-1 in placental invasion moreaccurately. Although differential mechanisms of HO-1 regulation inseveral cell types have been shown, collectively, studies suggestthat HO-1 contributes to cell migration and invasion. These featuresare important in sPE since inadequate invasion of the uterus byEVTs, together with defective formation of the outer syncytio-trophoblast, imply dual defects in each type of the differentiatedtrophoblast [84].
7. Molecular manipulations of HO-1
The role of HO-1 in underlying mechanisms of placental insuf-ficiency syndromes has been studied extensively. Considering theprominent role of anti-angiogenic factors in the manifestation of

K. Levytska et al. / Placenta 34 (2013) 291e298296
endothelial cell damage, it is natural to study the connection be-tween the protective role of HO-1 and these disease markers.Implicating the role of HO-1 in sPE, it was shown that HO-1 in-duction or CO administration in HUVECs inhibits their release ofsFLT-1 and sEndoglin (sEng) [15,16]. Both of these anti-angiogenicfactors contribute to endothelial dysfunction in sPE; thus, rein-forcing the hypothesis that HO-1 and heme metabolites promotea pro-angiogenic phenotype [15]. This same molecular pathwaywas studied in a model of placental hypoxia in rats, or the RUPPmodel [85]. Animals which have undergone the RUPP surgery haveelevated mean arterial pressure and exhibit lower fetal weight,suggesting that hypoxia contributes to fetal growth restriction [86].RUPP animals also have elevated plasma sFlt-1 and higher super-oxide production, both of which can be attenuated with an HO-1activity inducer or by the administration of bilirubin or CO. HO-1placental expression is decreased in RUPP animals, suggestingthat in rat tissue, hypoxia negatively regulates HO-1 [57]. Asmentioned previously, HO-1 has the ability to decrease sFLT-1release; interestingly, HO-1 is also able to offer protection againstsFlt-1 damage while bypassing this effect (i.e., when plasma sFlt-1levels are held constantly high) [14,15]. George et al. showed thatincreasing HO-1 activity in rats with sFlt-1-induced hypertensionameliorated elevated blood pressure despite the constantly highsFlt-1 levels [14]. HO-1 induction improved endothelial function,decreased blood pressure and increased VEGF levels. Supportingthe anti-apoptotic role of HO-1, it was shown that HO-1 inductionin the RUPP-treated animals shifted the balance from pro-injury topro-survival phenotype measured by the restoration of intra-cellular ATP levels and increased phosphorylation of survival reg-ulators [87].
Studies of molecular regulation of HO-1 in several models haveidentified a prominent transcriptional factor and nuclear receptorPPAR-g as one of the regulators of HO-1 [88e90]. Upon ligandbinding, PPAR-g translocates into the nucleus, binds to the PPAR-gresponse element (PPRE), and induces transcription of genesinvolved in fat metabolism and lipid peroxidation. The role of PPAR-g in trophoblast layer dynamics has been explored; some groupshave shown that activation of PPAR-g activity controlled theexpression of genes critical for trophoblast formation, such as glialcell missing-1 and syncytin-1, while others demonstrated itsinvolvement in cell invasion and migration, under the influence ofHO-1 induction [83,91e94]. More importantly, in linewith the rolesof HO-1 and PPAR-g in sPE pathogenesis, PPAR-g has been sug-gested to be one of the key targets for the treatment of sPE based onthe rat RUPP model [19,90]. Induction of PPAR-g activity increasedcirculating HO-1 levels and was able to ameliorate PE-like symp-toms (i.e., high blood pressure, endothelial cell dysfunction andhigh microalbumin:creatine ratio) in RUPP-treated animals [19].Further supporting the role of PPAR-g in sPE pathogenesis was thefinding that blocking PPAR-g activity increased circulating sFlt-1levels, an analogous feature to the one found in mice withdecreased Hmox-1 expression [78,90]. These studies support thehypothesis that pharmacologic interventions aimed at increasingHO-1 expression and activity in the placenta may help restorematernal cardiovascular function which is defective in sPE.
8. Conclusions and future directions
sPE pathology originates as a disorder of placental, specificallytrophoblast, function leading to the clinical manifestations of“placental insufficiency.” Developmentally-abnormal sPE placentais characterized by defective trophoblast layer turnover and syn-cytiotrophoblast formation as well as abnormal shedding of anti-angiogenic proteins. Their excess release into maternal serumleads to endothelial cell damage, systemic vascular peripheral
resistance and vasoconstriction, all of which are the hallmark fea-tures of sPE. In normal pregnancy, the physiologic placentalexpression of HO-1 may effectively ameliorate the symptoms of sPEand prevent systemic vasculopathy by lowering the release of anti-angiogenic proteins. The rescue of placental function via themanipulation of HO-1 may restore the physiology of the tropho-blast layer by inhibiting the rise in plasma sFLT-1 levels seen in sPEas well as inducing the production of CO, a potent vasodilator.Caution should be taken when interpreting these data, however,since the contribution of placental HO-1 to the disease is unknown.Novel interventions exploiting the properties of HO-1 may giveclinicians the capacity to significantly improve perinatal outcomes,should they prove capable of safely advancing pregnancies com-plicated by sPE for even 2e3weeks. Furthermore, advancing in vitropharmacologic tools to the clinical area may provide an opportu-nity to move beyond the removal of the placenta as the onlydefinitive treatment for established sPE. Indeed, manipulation ofHO-1 using statins as potential treatment of sPE is already beingexplored in a clinical trial [95].
Acknowledgments
The authors thank Drs. Sarah Keating, Theodore Brown, S. LeeAdamson (University of Toronto) and Asif Ahmed (University ofEdinburgh) for their helpful discussions and supervision of Ms.Levytska in herMSc studies. Dr. Kingdom’s research is supported byCIHR (No. 64302) and the Rose Torno Chair at Mount Sinai Hospital,Toronto, ON, Canada.
References
[1] Metcalfe J, Ueland K. Maternal cardiovascular adjustments to pregnancy. ProgCardiovasc Dis 1974;16(4):363e74.
[2] Abbas AE, Lester SJ, Connolly H. Pregnancy and the cardiovascular system. Int JCardiol 2005;98(2):179e89.
[3] Melchiorre K, Sutherland GR, Liberati M, Thilaganathan B. Maternal car-diovascular impairment in pregnancies complicated by severe fetal growthrestriction. Hypertension 2012;60(2):437e43.
[4] Burton GJ, Woods AW, Jauniaux E, Kingdom JC. Rheological and physiologicalconsequences of conversion of the maternal spiral arteries for uteroplacentalblood flow during human pregnancy. Placenta 2009;30(6):473e82.
[5] Franco C, Walker M, Robertson J, Fitzgerald B, Keating S, McLeod A, et al.Placental infarction and thrombophilia. Obstet Gynecol 2011;117(4):929e34.
[6] Yung HW, Calabrese S, Hynx D, Hemmings BA, Cetin I, Charnock-Jones DS,et al. Evidence of placental translation inhibition and endoplasmic reticulumstress in the etiology of human intrauterine growth restriction. Am J Pathol2008;173(2):451e62.
[7] Holwerda KM, Bos EM, Rajakumar A, Ris-Stalpers C, van Pampus MG,Timmer A, et al. Hydrogen sulfide producing enzymes in pregnancy andpreeclampsia. Placenta 2012;33(6):518e21.
[8] Kulandavelu S, Whiteley KJ, Qu D, Mu J, Bainbridge SA, Adamson SL. Endo-thelial nitric oxide synthase deficiency reduces uterine blood flow, spiral ar-tery elongation, and placental oxygenation in pregnant mice. Hypertension2012;60(1):231e8.
[9] Baum M, Schiff E, Kreiser D, Dennery PA, Stevenson DK, Rosenthal T, et al.End-tidal carbon monoxide measurements in women with pregnancy-induced hypertension and preeclampsia. Am J Obstet Gynecol 2000;183(4):900e3.
[10] Diagnosis and management of preeclampsia and eclampsia. Number 33 ACOGpractice bulletin. American college of obstetricians and gynecologists. Int JGynaecol Obstet January 2002;77(1):67e75.
[11] Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, et al. Excess placentalsoluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dys-function, hypertension, and proteinuria in preeclampsia. J Clin Invest 2003;111(5):649e58.
[12] Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, et al. Circulatingangiogenic factors and the risk of preeclampsia. N Engl J Med 2004;350(7):672e83.
[13] Thadhani R, Kisner T, Hagmann H, Bossung V, Noack S, Schaarschmidt W, et al.Pilot study of extracorporeal removal of soluble fms-like tyrosine kinase 1 inpreeclampsia. Circulation 2011;124(8):940e50.
[14] George EM, Arany M, Cockrell K, Storm MV, Stec DE, Granger JP. Induction ofheme oxygenase-1 attenuates sFlt-1-induced hypertension in pregnant rats.Am J Physiol Regul Integr Comp Physiol 2011;301(5):R1495e500.

K. Levytska et al. / Placenta 34 (2013) 291e298 297
[15] Cudmore M, Ahmad S, Al-Ani B, Fujisawa T, Coxall H, Chudasama K, et al.Negative regulation of soluble Flt-1 and soluble endoglin release by hemeoxygenase-1. Circulation 2007;115(13):1789e97.
[16] Cudmore MJ, Ramma W, Cai M, Fujisawa T, Ahmad S, Al-Ani B, et al.Resveratrol inhibits the release of soluble fms-like tyrosine kinase (sFlt-1)from human placenta. Am J Obstet Gynecol 2012;206(3). 253 e10-5.
[17] El-Mousleh T, Casalis PA, Wollenberg I, Zenclussen ML, Volk HD, Langwisch S,et al. Exploring the potential of low doses carbon monoxide as therapy inpregnancy complications. Med Gas Res 2012;2(1):4.
[18] Zenclussen ML, Casalis PA, El-Mousleh T, Rebelo S, Langwisch S, Linzke N,et al. Haem oxygenase-1 dictates intrauterine fetal survival in mice via carbonmonoxide. J Pathol 2011;225(2):293e304.
[19] McCarthy FP, Drewlo S, Kingdom J, Johns EJ, Walsh SK, Kenny LC. Peroxisomeproliferator-activated receptor-gamma as a potential therapeutic target in thetreatment of preeclampsia. Hypertension 2011;58(2):280e6.
[20] Maines MD, Trakshel GM, Kutty RK. Characterization of two constitutiveforms of rat liver microsomal heme oxygenase. Only one molecular species ofthe enzyme is inducible. J Biol Chem 1986;261(1):411e9.
[21] Shibahara S, Yoshizawa M, Suzuki H, Takeda K, Meguro K, Endo K. Functionalanalysis of cDNAs for two types of human heme oxygenase and evidence fortheir separate regulation. J Biochem 1993;113(2):214e8.
[22] Yoshida T, Biro P, Cohen T, Müller RM, Shibahara S. Human heme oxy-genase cDNA and induction of its mRNA by hemin. Eur J Biochem 1988;171(3):457e61.
[23] Tenhunen R, Marver HS, Schmid R. Microsomal heme oxygenase. Character-ization of the enzyme. J Biol Chem 1969;244(23):6388e94.
[24] Montellano PR. The mechanism of heme oxygenase. Curr Opin Chem Biol2000;4(2):221e7.
[25] Neuzil J, Stocker R. Free and albumin-bound bilirubin are efficient co-antioxidants for alpha-tocopherol, inhibiting plasma and low density lip-oprotein lipid peroxidation. J Biol Chem 1994;269(24):16712e9.
[26] Ahmed A, Rahman M, Zhang X, Acevedo CH, Nijjar S, Rushton I, et al. In-duction of placental heme oxygenase-1 is protective against TNFalpha-induced cytotoxicity and promotes vessel relaxation. Mol Med 2000;6(5):391e409.
[27] Brouard S, Otterbein LE, Anrather J, Tobiasch E, Bach FH, Choi AM, Soares MP.Carbon monoxide generated by heme oxygenase 1 suppresses endothelial cellapoptosis. J Exp Med 2000;192(7):1015e26.
[28] Sarady JK, Otterbein SL, Liu F, Otterbein LE, Choi AM. Carbon monoxidemodulates endotoxin-induced production of granulocyte macrophagecolony-stimulating factor in macrophages. Am J Respir Cell Mol Biol 2002;27(6):739e45.
[29] Coceani F. Carbon monoxide and dilation of blood vessels. Science 1993;260(5109):739.
[30] Morita T, Perrella MA, Lee ME, Kourembanas S. Smooth muscle cell-derivedcarbon monoxide is a regulator of vascular cGMP. Proc Natl Acad Sci U S A1995;92(5):1475e9.
[31] Acevedo CH, Ahmed A. Hemeoxygenase-1 inhibits human myometrial con-tractility via carbon monoxide and is upregulated by progesterone duringpregnancy. J Clin Invest 1998;101(5):949e55.
[32] Bainbridge SA, Farley AE, McLaughlin BE, Graham CH, Marks GS, Nakatsu K,et al. Carbon monoxide decreases perfusion pressure in isolated human pla-centa. Placenta 2002;23(8e9):563e9.
[33] Yachie A, Niida Y, Wada T, Igarashi N, Kaneda H, Toma T, et al. Oxidative stresscauses enhanced endothelial cell injury in human heme oxygenase-1 defi-ciency. J Clin Invest 1999;103(1):129e35.
[34] Denschlag D, Marculescu R, Unfried G, Hefler LA, Exner M, Hashemi A, et al.The size of a microsatellite polymorphism of the haem oxygenase 1 gene isassociated with idiopathic recurrent miscarriage. Mol Hum Reprod 2004;10(3):211e4.
[35] Lin R, Fu W, Zhou W, Wang Y, Wang X, Huang W, et al. Association of hemeoxygenase-1 gene polymorphisms with essential hypertension and bloodpressure in the Chinese Han population. Genet Test Mol Biomarkers 2011;15(1e2):23e8.
[36] Ono K, Mannami T, Iwai N. Association of a promoter variant of the haemeoxygenase-1 gene with hypertension in women. J Hypertens 2003;21(8):1497e503.
[37] Chen M, Zhou L, Ding H, Huang S, He M, Zhang X, et al. Short (GT) ( n ) repeatsin heme oxygenase-1 gene promoter are associated with lower risk of coro-nary heart disease in subjects with high levels of oxidative stress. Cell StressChaperones 2012;17(3):329e38.
[38] Kreiser D, Kelly DK, Seidman DS, Stevenson DK, Baum M, Dennery PA. Ges-tational pattern of heme oxygenase expression in the rat. Pediatr Res 2003;54(2):172e8.
[39] Watanabe S, Akagi R, Mori M, Tsuchiya T, Sassa S. Marked developmentalchanges in heme oxygenase-1 (HO-1) expression in the mouse placenta:correlation between HO-1 expression and placental development. Placenta2004;25(5):387e95.
[40] Zhao H, Wong RJ, Doyle TC, Nayak N, Vreman HJ, Contag CH, et al. Regulationof maternal and fetal hemodynamics by heme oxygenase in mice. Biol Reprod2008;78(4):744e51.
[41] Lyall F, Barber A, Myatt L, Bulmer JN, Robson SC. Hemeoxygenaseexpression in human placenta and placental bed implies a role in regu-lation of trophoblast invasion and placental function. FASEB J 2000;14(1):208e19.
[42] McLaughlin BE, Lash GE, Smith GN, Marks GS, Nakatsu K, Graham CH, et al.Heme oxygenase expression in selected regions of term human placenta. ExpBiol Med (Maywood) 2003;228(5):564e7.
[43] McLean M, Bowman M, Clifton V, Smith R, Grossman AB. Expression of theheme oxygenase-carbon monoxide signalling system in human placenta.J Clin Endocrinol Metab 2000;85(6):2345e9.
[44] Yoshiki N, Kubota T, Aso T. Expression and localization of heme oxygenase inhuman placental villi. Biochem Biophys Res Commun 2000;276(3):1136e42.
[45] Kreiser D, Baum M, Seidman DS, Fanaroff A, Shah D, Hendler I, et al. End tidalcarbon monoxide levels are lower in women with gestational hypertensionand pre-eclampsia. J Perinatol 2004;24(4):213e7.
[46] Zenclussen AC, Lim E, Knoeller S, Knackstedt M, Hertwig K, Hagen E, et al.Heme oxygenases in pregnancy II: HO-2 is downregulated in human patho-logic pregnancies. Am J Reprod Immunol 2003;50(1):66e76.
[47] Lash GE, McLaughlin BE, MacDonald-Goodfellow SK, Smith GN, Brien JF,Marks GS, et al. Relationship between tissue damage and heme oxygenaseexpression in chorionic villi of term human placenta. Am J Physiol Heart CircPhysiol 2003;284(1):H160e7.
[48] Barber A, Robson SC, Myatt L, Bulmer JN, Lyall F. Heme oxygenase expressionin human placenta and placental bed: reduced expression of placenta endo-thelial HO-2 in preeclampsia and fetal growth restriction. FASEB J 2001;15(7):1158e68.
[49] Hung TH, Skepper JN, Charnock-Jones DS, Burton GJ. Hypoxia-reoxygenation:a potent inducer of apoptotic changes in the human placenta and possibleetiological factor in preeclampsia. Circ Res 2002;90(12):1274e81.
[50] Appleton SD, Marks GS, Nakatsu K, Brien JF, Smith GN, Graham CH. Hemeoxygenase activity in placenta: direct dependence on oxygen availability.Am J Physiol Heart Circ Physiol 2002;282(6):H2055e9.
[51] Panchenko MV, Farber HW, Korn JH. Induction of heme oxygenase-1 byhypoxia and free radicals in human dermal fibroblasts. Am J Physiol CellPhysiol 2000;278(1):C92e101.
[52] Motterlini R, Foresti R, Bassi R, Calabrese V, Clark JE, Green CJ. Endothelialheme oxygenase-1 induction by hypoxia. Modulation by inducible nitric-oxide synthase and S-nitrosothiols. J Biol Chem 2000;275(18):13613e20.
[53] Carraway MS, Ghio AJ, Carter JD, Piantadosi CA. Expression of hemeoxygenase-1 in the lung in chronic hypoxia. Am J Physiol Lung Cell MolPhysiol 2000;278(4):L806e12.
[54] Appleton SD, Marks GS, Nakatsu K, Brien JF, Smith GN, Graham CH, et al. Ef-fects of hypoxia on heme oxygenase expression in human chorionic villi ex-plants and immortalized trophoblast cells. Am J Physiol Heart Circ Physiol2003;284(3):H853e8.
[55] McCaig D, Lyall F. Heme oxygenase expression in human placental villoustissue in response to exposure to in vitro ischemia-reperfusion injury.Hypertens Pregnancy 2009;28(3):256e72.
[56] George EM, Colson D, Dixon J, Palei AC, Granger JP. Heme oxygenase-1 at-tenuates hypoxia-induced sFlt-1 and oxidative stress in placental villi throughits metabolic products CO and bilirubin. Int J Hypertens 2012;2012:486053.
[57] George EM, Cockrell K, Aranay M, Csongradi E, Stec DE, Granger JP. Inductionof heme oxygenase 1 attenuates placental ischemia-induced hypertension.Hypertension 2011;57(5):941e8.
[58] Leber A, Zenclussen ML, Teles A, Brachwitz N, Casalis P, El-Mousleh T, et al.Pregnancy: tolerance and suppression of immune responses. Methods MolBiol 2011;677:397e417.
[59] Gonzalez IT, Barrientos G, Freitag N, Otto T, Thijssen VL, Moschansky P, et al.Uterine NK cells are critical in shaping DC immunogenic functions compatiblewith pregnancy progression. PLoS One 2012;7(10):e46755.
[60] Wegmann TG, Lin H, Guilbert L, Mosmann TR. Bidirectional cytokine in-teractions in the maternal-fetal relationship: is successful pregnancy a TH2phenomenon? Immunol Today 1993;14(7):353e6.
[61] Tachibana M, Hashino M, Nishida T, Shimizu T, Watarai M. Protective role ofheme oxygenase-1 in Listeria monocytogenes-induced abortion. PLoS One2011;6(9):e25046.
[62] Sollwedel A, Bertoja AZ, Zenclussen ML, Gerlof K, Lisewski U, Wafula P, et al.Protection from abortion by heme oxygenase-1 up-regulation is associatedwith increased levels of Bag-1 and neuropilin-1 at the fetal-maternal inter-face. J Immunol 2005;175(8):4875e85.
[63] Liu F, Guo J, Tian T, Wang H, Dong F, Huang H, et al. Placental trophoblastsshifted Th1/Th2 balance toward Th2 and inhibited Th17 immunity at feto-maternal interface. APMIS 2011;119(9):597e604.
[64] Dong M, He J, Wang Z, Xie X, Wang H. Placental imbalance of Th1- and Th2-type cytokines in preeclampsia. Acta Obstet Gynecol Scand 2005;84(8):788e93.
[65] Tinsley JH, South S, Chiasson VL, Mitchell BM. Interleukin-10 reducesinflammation, endothelial dysfunction, and blood pressure in hypertensivepregnant rats. Am J Physiol Regul Integr Comp Physiol 2010;298(3):R713e9.
[66] Lee TS, Chau LY. Heme oxygenase-1 mediates the anti-inflammatory effect ofinterleukin-10 in mice. Nat Med 2002;8(3):240e6.
[67] Somerset DA, Zheng Y, Kilby MD, Sansom DM, Drayson MT. Normal humanpregnancy is associated with an elevation in the immune suppressive CD25þCD4þ regulatory T-cell subset. Immunology 2004;112(1):38e43.
[68] Sasaki Y, Sakai M, Miyazaki S, Higuma S, Shiozaki A, Saito S. Decidual andperipheral blood CD4þCD25þ regulatory T cells in early pregnancy subjectsand spontaneous abortion cases. Mol Hum Reprod 2004;10(5):347e53.
[69] Zenclussen AC, Gerlof K, Zenclussen ML, Sollwedel A, Bertoja AZ, Ritter T, et al.Abnormal T-cell reactivity against paternal antigens in spontaneous abortion:

K. Levytska et al. / Placenta 34 (2013) 291e298298
adoptive transfer of pregnancy-induced CD4þCD25þ T regulatory cells pre-vents fetal rejection in a murine abortion model. Am J Pathol 2005;166(3):811e22.
[70] Zenclussen AC, Joachim R, Hagen E, Peiser C, Klapp BF, Arck PC. Heme oxy-genase is downregulated in stress-triggered and interleukin-12-mediatedmurine abortion. Scand J Immunol 2002;55(6):560e9.
[71] Zenclussen AC, Gerlof K, Zenclussen ML, Ritschel S, Zambon Bertoja A, Fest S,et al. Regulatory T cells induce a privileged tolerant microenvironment at thefetal-maternal interface. Eur J Immunol 2006;36(1):82e94.
[72] Zenclussen AC, Sollwedel A, Bertoja AZ, Gerlof K, Zenclussen ML,Woiciechowsky C, et al. Heme oxygenase as a therapeutic target inimmunological pregnancy complications. Int Immunopharmacol 2005;5(1):41e51.
[73] Zenclussen ML, Anegon I, Bertoja AZ, Chauveau C, Vogt K, Gerlof K, et al. Over-expression of heme oxygenase-1 by adenoviral gene transfer improvespregnancy outcome in a murine model of abortion. J Reprod Immunol 2006;69(1):35e52.
[74] Schumacher A, Wafula PO, Teles A, El-Mousleh T, Linzke N, Zenclussen ML,et al. Blockage of heme oxygenase-1 abrogates the protective effect of regu-latory T cells on murine pregnancy and promotes the maturation of dendriticcells. PLoS One 2012;7(8):e42301.
[75] Poss KD, Tonegawa S. Reduced stress defense in heme oxygenase 1-deficientcells. Proc Natl Acad Sci U S A 1997;94(20):10925e30.
[76] Poss KD, Tonegawa S. Heme oxygenase 1 is required for mammalian ironreutilization. Proc Natl Acad Sci U S A 1997;94(20):10919e24.
[77] Kapturczak MH, Wasserfall C, Brusko T, Campbell-Thompson M, Ellis TM,Atkinson MA, et al. Heme oxygenase-1 modulates early inflammatory re-sponses: evidence from the heme oxygenase-1-deficient mouse. Am J Pathol2004;165(3):1045e53.
[78] Zhao H, Wong RJ, Kalish FS, Nayak NR, Stevenson DK. Effect of hemeoxygenase-1 deficiency on placental development. Placenta 2009;30(10):861e8.
[79] Wong RJ, Zhao H, Stevenson DK. A deficiency in haem oxygenase-1 inducesfoetal growth restriction by placental vasculature defects. Acta Paediatr 2012;101(8):827e34.
[80] Zhao H, Azuma J, Kalish F, Wong RJ, Stevenson DK. Maternal heme oxy-genase 1 regulates placental vasculature development via angiogenic fac-tors in mice. Biol Reprod 2011;85(5):1005e12.
[81] Kweider N, Fragoulis A, Rosen C, Pecks U, Rath W, Pufe T, et al. Interplaybetween vascular endothelial growth factor (VEGF) and nuclear factorerythroid 2-related factor-2 (Nrf2): implications for preeclampsia. J Biol Chem2011;286(50):42863e72.
[82] Lin Q, Weis S, Yang G, Weng YH, Helston R, Rish K, et al. Heme oxygenase-1protein localizes to the nucleus and activates transcription factors impor-tant in oxidative stress. J Biol Chem 2007;282(28):20621e33.
[83] Bilban M, Haslinger P, Prast J, Klinglmüller F, Woelfel T, Haider S, et al.Identification of novel trophoblast invasion-related genes: heme oxygenase-1controls motility via peroxisome proliferator-activated receptor gamma.Endocrinology 2009;150(2):1000e13.
[84] Fitzgerald B, Levytska K, Kingdom J, Walker M, Baczyk D, Keating S. Villoustrophoblast abnormalities in extremely preterm deliveries with elevatedsecond trimester maternal serum hCG or inhibin-A. Placenta 2011;32(4):339e45.
[85] Granger JP, LaMarca BB, Cockrell K, Sedeek M, Balzi C, Chandler D, et al.Reduced uterine perfusion pressure (RUPP) model for studyingcardiovascular-renal dysfunction in response to placental ischemia. MethodsMol Med 2006;122:383e92.
[86] SedeekM, Gilbert JS, LaMarca BB, Sholook M, Chandler DL, Wang Y, et al. Role ofreactive oxygen species in hypertension produced by reduced uterine perfusionin pregnant rats. Am J Hypertens 2008;21(10):1152e6.
[87] George EM, Arany I. Induction of heme oxygenase-1 shifts the balance fromproinjury to prosurvival in the placentas of pregnant rats with reduceduterine perfusion pressure. Am J Physiol Regul Integr Comp Physiol 2012;302(5):R620e6.
[88] Kronke G, Kadl A, Ikonomu E, Blüml S, Fürnkranz A, Sarembock IJ, et al.Expression of heme oxygenase-1 in human vascular cells is regulated byperoxisome proliferator-activated receptors. Arterioscler Thromb Vasc Biol2007;27(6):1276e82.
[89] Cheng CF, Lian WS, Chen SH, Lai PF, Li HF, Lan YF, et al. Protective effects ofadiponectin against renal ischemia-reperfusion injury via prostacyclin-PPARalpha-heme oxygenase-1 signaling pathway. J Cell Physiol 2011;227(1):239e49.
[90] McCarthy FP, Drewlo S, English FA, Kingdom J, Johns EJ, Kenny LC, et al. Ev-idence implicating peroxisome proliferator-activated receptor-gamma in thepathogenesis of preeclampsia. Hypertension 2011;58(5):882e7.
[91] Fournier T, Handschuh K, Tsatsaris V, Evain-Brion D. Involvement of PPAR-gamma in human trophoblast invasion. Placenta 2007;28(Suppl. A):S76e81.
[92] Fournier T, Guibourdenche J, Handschuh K, Tsatsaris V, Rauwel B, Davrinche C,et al. PPARgamma and human trophoblast differentiation. J Reprod Immunol2011;90(1):41e9.
[93] Parast MM, Yu H, Ciric A, Salata MW, Davis V, Milstone DS. PPARgammaregulates trophoblast proliferation and promotes labyrinthine trilineage dif-ferentiation. PLoS One 2009;4(11):e8055.
[94] Ruebner M, Langbein M, Strissel PL, Henke C, Schmidt D, Goecke TW, et al.Regulation of the human endogenous retroviral Syncytin-1 and cell-cellfusion by the nuclear hormone receptors PPARgamma/RXRalpha in pla-centogenesis. J Cell Biochem 2012;113(7):2383e96.
[95] Ahmed A. New insights into the etiology of preeclampsia: identification of keyelusive factors for the vascular complications. Thromb Res 2011;127(Suppl.3):S72e5.





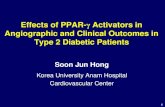



![Isoflavonoids from Crotalaria albida Inhibit Adipocyte ...€¦ · germacranolidecompounds[18]thatpresent PPAR-γantagonismeffectshavebeenshownto inhibit adipocytedifferentiationandlipidaccumulationin](https://static.fdocument.org/doc/165x107/5f4dcbe6465a9b47ae7bbf0a/isoflavonoids-from-crotalaria-albida-inhibit-adipocyte-germacranolidecompounds18thatpresent.jpg)