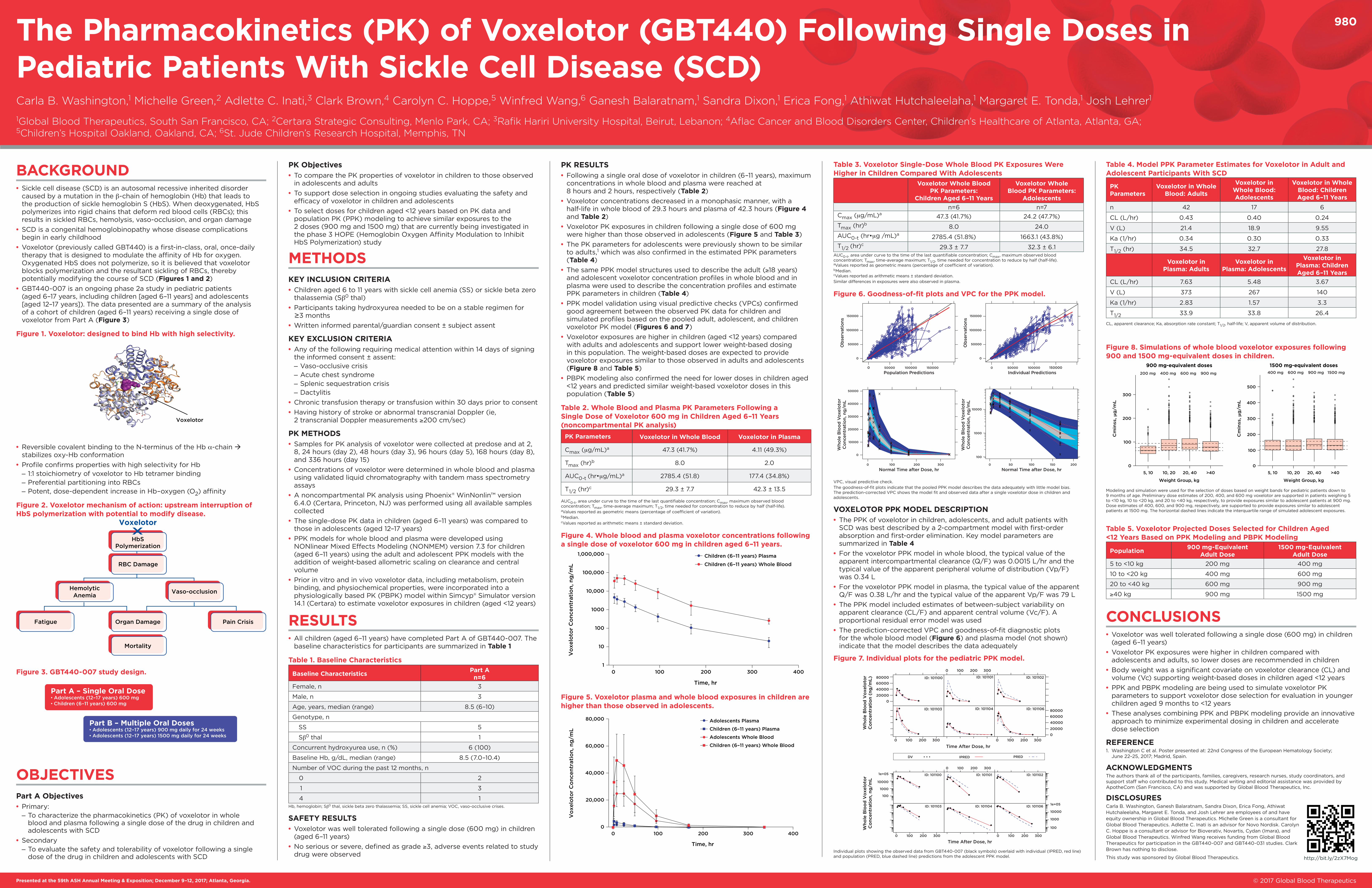
The Pharmacokinetics (PK) of Voxelotor (GBT440) …...The goodness-of-fit plots indicate that the...
1
BACKGROUND • Sickle cell disease (SCD) is an autosomal recessive inherited disorder caused by a mutation in the β-chain of hemoglobin (Hb) that leads to the production of sickle hemoglobin S (HbS). When deoxygenated, HbS polymerizes into rigid chains that deform red blood cells (RBCs); this results in sickled RBCs, hemolysis, vaso-occlusion, and organ damage • SCD is a congenital hemoglobinopathy whose disease complications begin in early childhood • Voxelotor (previously called GBT440) is a first-in-class, oral, once-daily therapy that is designed to modulate the affinity of Hb for oxygen. Oxygenated HbS does not polymerize, so it is believed that voxelotor blocks polymerization and the resultant sickling of RBCs, thereby potentially modifying the course of SCD (Figures 1 and 2 ) • GBT440-007 is an ongoing phase 2a study in pediatric patients (aged 6–17 years, including children [aged 6–11 years] and adolescents [aged 12–17 years]). The data presented are a summary of the analysis of a cohort of children (aged 6–11 years) receiving a single dose of voxelotor from Part A (Figure 3) Figure 1. Voxelotor: designed to bind Hb with high selectivity. Voxelotor • Reversible covalent binding to the N-terminus of the Hb α-chain stabilizes oxy-Hb conformation • Profile confirms properties with high selectivity for Hb – 1:1 stoichiometry of voxelotor to Hb tetramer binding – Preferential partitioning into RBCs – Potent, dose-dependent increase in Hb–oxygen (O 2 ) affinity Figure 2. Voxelotor mechanism of action: upstream interruption of HbS polymerization with potential to modify disease. HbS Polymerization Voxelotor RBC Damage Hemolytic Anemia Fatigue Organ Damage Pain Crisis Mortality Vaso-occlusion Figure 3. GBT440-007 study design. Part A – Single Oral Dose • Adolescents (12–17 years) 600 mg • Children (6–11 years) 600 mg Part B – Multiple Oral Doses • Adolescents (12–17 years) 900 mg daily for 24 weeks • Adolescents (12–17 years) 1500 mg daily for 24 weeks OBJECTIVES Part A Objectives • Primary: – To characterize the pharmacokinetics (PK) of voxelotor in whole blood and plasma following a single dose of the drug in children and adolescents with SCD • Secondary – To evaluate the safety and tolerability of voxelotor following a single dose of the drug in children and adolescents with SCD The Pharmacokinetics (PK) of Voxelotor (GBT440) Following Single Doses in Pediatric Patients With Sickle Cell Disease (SCD) Carla B. Washington, 1 Michelle Green, 2 Adlette C. Inati, 3 Clark Brown, 4 Carolyn C. Hoppe, 5 Winfred Wang, 6 Ganesh Balaratnam, 1 Sandra Dixon, 1 Erica Fong, 1 Athiwat Hutchaleelaha, 1 Margaret E. Tonda, 1 Josh Lehrer 1 1 Global Blood Therapeutics, South San Francisco, CA; 2 Certara Strategic Consulting, Menlo Park, CA; 3 Rafik Hariri University Hospital, Beirut, Lebanon; 4 Aflac Cancer and Blood Disorders Center, Children’s Healthcare of Atlanta, Atlanta, GA; 5 Children’s Hospital Oakland, Oakland, CA; 6 St. Jude Children’s Research Hospital, Memphis, TN 980 PK Objectives • To compare the PK properties of voxelotor in children to those observed in adolescents and adults • To support dose selection in ongoing studies evaluating the safety and efficacy of voxelotor in children and adolescents • To select doses for children aged <12 years based on PK data and population PK (PPK) modeling to achieve similar exposures to the 2 doses (900 mg and 1500 mg) that are currently being investigated in the phase 3 HOPE (Hemoglobin Oxygen Affinity Modulation to Inhibit HbS Polymerization) study METHODS KEY INCLUSION CRITERIA • Children aged 6 to 11 years with sickle cell anemia (SS) or sickle beta zero thalassemia (Sβ 0 thal) • Participants taking hydroxyurea needed to be on a stable regimen for ≥ 3 months • Written informed parental/guardian consent ± subject assent KEY EXCLUSION CRITERIA • Any of the following requiring medical attention within 14 days of signing the informed consent ± assent: – Vaso-occlusive crisis – Acute chest syndrome – Splenic sequestration crisis – Dactylitis • Chronic transfusion therapy or transfusion within 30 days prior to consent • Having history of stroke or abnormal transcranial Doppler (ie, 2 transcranial Doppler measurements ≥200 cm/sec) PK METHODS • Samples for PK analysis of voxelotor were collected at predose and at 2, 8, 24 hours (day 2), 48 hours (day 3), 96 hours (day 5), 168 hours (day 8), and 336 hours (day 15) • Concentrations of voxelotor were determined in whole blood and plasma using validated liquid chromatography with tandem mass spectrometry assays • A noncompartmental PK analysis using Phoenix® WinNonlin™ version 6.4.0 (Certara, Princeton, NJ) was performed using all available samples collected • The single-dose PK data in children (aged 6–11 years) was compared to those in adolescents (aged 12–17 years) • PPK models for whole blood and plasma were developed using NONlinear Mixed Effects Modeling (NONMEM) version 7.3 for children (aged 6–11 years) using the adult and adolescent PPK models with the addition of weight-based allometric scaling on clearance and central volume • Prior in vitro and in vivo voxelotor data, including metabolism, protein binding, and physiochemical properties, were incorporated into a physiologically based PK (PBPK) model within Simcyp® Simulator version 14.1 (Certara) to estimate voxelotor exposures in children (aged <12 years) RESULTS • All children (aged 6–11 years) have completed Part A of GBT440-007. The baseline characteristics for participants are summarized in Table 1 Table 1. Baseline Characteristics Baseline Characteristics Part A n=6 Female, n 3 Male, n 3 Age, years, median (range) 8.5 (6–10) Genotype, n SS 5 Sβ 0 thal 1 Concurrent hydroxyurea use, n (%) 6 (100) Baseline Hb, g/dL, median (range) 8.5 (7.0–10.4) Number of VOC during the past 12 months, n 0 2 1 3 4 1 Hb, hemoglobin; Sβ 0 thal, sickle beta zero thalassemia; SS, sickle cell anemia; VOC, vaso-occlusive crises. SAFETY RESULTS • Voxelotor was well tolerated following a single dose (600 mg) in children (aged 6–11 years) • No serious or severe, defined as grade ≥3, adverse events related to study drug were observed PK RESULTS • Following a single oral dose of voxelotor in children (6–11 years), maximum concentrations in whole blood and plasma were reached at 8 hours and 2 hours, respectively (Table 2 ) • Voxelotor concentrations decreased in a monophasic manner, with a half-life in whole blood of 29.3 hours and plasma of 42.3 hours (Figure 4 and Table 2 ) • Voxelotor PK exposures in children following a single dose of 600 mg were higher than those observed in adolescents (Figure 5 and Table 3) • The PK parameters for adolescents were previously shown to be similar to adults, 1 which was also confirmed in the estimated PPK parameters (Table 4 ) • The same PPK model structures used to describe the adult ( ≥ 18 years) and adolescent voxelotor concentration profiles in whole blood and in plasma were used to describe the concentration profiles and estimate PPK parameters in children (Table 4 ) • PPK model validation using visual predictive checks (VPCs) confirmed good agreement between the observed PK data for children and simulated profiles based on the pooled adult, adolescent, and children voxelotor PK model (Figures 6 and 7) • Voxelotor exposures are higher in children (aged <12 years) compared with adults and adolescents and support lower weight-based dosing in this population. The weight-based doses are expected to provide voxelotor exposures similar to those observed in adults and adolescents (Figure 8 and Table 5) • PBPK modeling also confirmed the need for lower doses in children aged <12 years and predicted similar weight-based voxelotor doses in this population (Table 5) Table 2. Whole Blood and Plasma PK Parameters Following a Single Dose of Voxelotor 600 mg in Children Aged 6–11 Years (noncompartmental PK analysis) PK Parameters Voxelotor in Whole Blood Voxelotor in Plasma C max (µg/mL) a 47.3 (41.7%) 4.11 (49.3%) T max (hr) b 8.0 2.0 AUC 0-t (hr•µg/mL) a 2785.4 (51.8) 177.4 (34.8%) T 1/2 (hr) c 29.3 ± 7.7 42.3 ± 13.5 AUC 0-t , area under curve to the time of the last quantifiable concentration; C max , maximum observed blood concentration; T max , time-average maximum; T 1/2 , time needed for concentration to reduce by half (half-life). a Values reported as geometric means (percentage of coefficient of variation). b Median. c Values reported as arithmetic means ± standard deviation. Figure 4. Whole blood and plasma voxelotor concentrations following a single dose of voxelotor 600 mg in children aged 6–11 years. 1 10 100 1000 10,000 100,000 1,000,000 Voxelotor Concentration, ng/mL Time, hr 0 100 Children (6–11 years) Plasma Children (6–11 years) Whole Blood 200 300 400 Figure 5. Voxelotor plasma and whole blood exposures in children are higher than those observed in adolescents. 0 20,000 40,000 60,000 80,000 Voxelotor Concentration, ng/mL Time, hr 0 100 Adolescents Plasma Children (6–11 years) Plasma Adolescents Whole Blood Children (6–11 years) Whole Blood 200 300 400 Table 3. Voxelotor Single-Dose Whole Blood PK Exposures Were Higher in Children Compared With Adolescents Voxelotor Whole Blood PK Parameters: Children Aged 6–11 Years Voxelotor Whole Blood PK Parameters: Adolescents n=6 n=7 C max (µg/mL) a 47.3 (41.7%) 24.2 (47.7%) T max (hr) b 8.0 24.0 AUC 0-t (hr•µg /mL) a 2785.4 (51.8%) 1663.1 (43.8%) T 1/2 (hr) c 29.3 ± 7.7 32.3 ± 6.1 AUC 0-t , area under curve to the time of the last quantifiable concentration; C max , maximum observed blood concentration; T max , time-average maximum; T 1/2 , time needed for concentration to reduce by half (half-life). a Values reported as geometric means (percentage of coefficient of variation). b Median. c Values reported as arithmetic means ± standard deviation. Similar differences in exposures were also observed in plasma. Figure 6. Goodness-of-fit plots and VPC for the PPK model. Whole Blood Voxelotor Concentration, ng/mL Normal Time after Dose, hr Normal Time after Dose, hr 10000 1000 100 50000 40000 30000 20000 10000 0 Whole Blood Voxelotor Concentration, ng/mL 0 0 50 100 150 200 100 200 300 Observations Population Predictions 150000 100000 50000 0 0 50000 100000 150000 Observations Individual Predictions 150000 100000 50000 0 0 50000 100000 150000 VPC, visual predictive check. The goodness-of-fit plots indicate that the pooled PPK model describes the data adequately with little model bias. The prediction-corrected VPC shows the model fit and observed data after a single voxelotor dose in children and adolescents. VOXELOTOR PPK MODEL DESCRIPTION • The PPK of voxelotor in children, adolescents, and adult patients with SCD was best described by a 2-compartment model with first-order absorption and first-order elimination. Key model parameters are summarized in Table 4 • For the voxelotor PPK model in whole blood, the typical value of the apparent intercompartmental clearance (Q/F) was 0.0015 L/hr and the typical value of the apparent peripheral volume of distribution (Vp/F) was 0.34 L • For the voxelotor PPK model in plasma, the typical value of the apparent Q/F was 0.38 L/hr and the typical value of the apparent Vp/F was 79 L • The PPK model included estimates of between-subject variability on apparent clearance (CL/F) and apparent central volume (Vc/F). A proportional residual error model was used • The prediction-corrected VPC and goodness-of-fit diagnostic plots for the whole blood model (Figure 6) and plasma model (not shown) indicate that the model describes the data adequately Figure 7. Individual plots for the pediatric PPK model. ID: 101104 ID: 101106 ID: 101103 ID: 101101 ID: 101102 ID: 101100 Whole Blood Voxelotor Concentration, ng/mL 1e+05 10000 1000 100 0 100 200 300 Time After Dose, hr 0 100 200 300 0 100 200 300 1e+05 10000 1000 100 Whole Blood Voxelotor Concentration (ng/mL) 80000 ID: 101104 ID: 101106 ID: 101103 ID: 101101 ID: 101102 Time After Dose, hr ID: 101100 IPRED DV • • • PRED 60000 40000 20000 0 80000 60000 40000 20000 0 0 100 200 300 0 100 200 300 0 100 200 300 Individual plots showing the observed data from GBT440-007 (black symbols) overlaid with individual (IPRED, red line) and population (PRED, blue dashed line) predictions from the adolescent PPK model. Table 4. Model PPK Parameter Estimates for Voxelotor in Adult and Adolescent Participants With SCD PK Parameters Voxelotor in Whole Blood: Adults Voxelotor in Whole Blood: Adolescents Voxelotor in Whole Blood: Children Aged 6–11 Years n 42 17 6 CL (L/hr) 0.43 0.40 0.24 V (L) 21.4 18.9 9.55 Ka (1/hr) 0.34 0.30 0.33 T 1/2 (hr) 34.5 32.7 27.8 Voxelotor in Plasma: Adults Voxelotor in Plasma: Adolescents Voxelotor in Plasma: Children Aged 6–11 Years CL (L/hr) 7.63 5.48 3.67 V (L) 373 267 140 Ka (1/hr) 2.83 1.57 3.3 T 1/2 33.9 33.8 26.4 CL, apparent clearance; Ka, absorption rate constant; T 1/2 , half-life; V, apparent volume of distribution. Figure 8. Simulations of whole blood voxelotor exposures following 900 and 1500 mg-equivalent doses in children. 0 100 200 300 Cminss, μ g/mL Weight Group, kg 900 mg-equivalent doses 5, 10 10, 20 20, 40 >40 0 100 300 500 Cminss, μ g/mL Weight Group, kg 1500 mg-equivalent doses 200 400 5, 10 10, 20 20, 40 >40 200 mg 400 mg 600 mg 900 mg 400 mg 600 mg 900 mg 1500 mg Modeling and simulation were used for the selection of doses based on weight bands for pediatric patients down to 9 months of age. Preliminary dose estimates of 200, 400, and 600 mg voxelotor are supported in patients weighing 5 to <10 kg, 10 to <20 kg, and 20 to <40 kg, respectively, to provide exposures similar to adolescent patients at 900 mg. Dose estimates of 400, 600, and 900 mg, respectively, are supported to provide exposures similar to adolescent patients at 1500 mg. The horizontal dashed lines indicate the interquartile range of simulated adolescent exposures. Table 5. Voxelotor Projected Doses Selected for Children Aged <12 Years Based on PPK Modeling and PBPK Modeling Population 900 mg-Equivalent Adult Dose 1500 mg-Equivalent Adult Dose 5 to <10 kg 200 mg 400 mg 10 to <20 kg 400 mg 600 mg 20 to <40 kg 600 mg 900 mg ≥40 kg 900 mg 1500 mg CONCLUSIONS • Voxelotor was well tolerated following a single dose (600 mg) in children (aged 6–11 years) • Voxelotor PK exposures were higher in children compared with adolescents and adults, so lower doses are recommended in children • Body weight was a significant covariate on voxelotor clearance (CL) and volume (Vc) supporting weight-based doses in children aged <12 years • PPK and PBPK modeling are being used to simulate voxelotor PK parameters to support voxelotor dose selection for evaluation in younger children aged 9 months to <12 years • These analyses combining PPK and PBPK modeling provide an innovative approach to minimize experimental dosing in children and accelerate dose selection REFERENCE 1. Washington C et al. Poster presented at: 22nd Congress of the European Hematology Society; June 22–25, 2017; Madrid, Spain. ACKNOWLEDGMENTS The authors thank all of the participants, families, caregivers, research nurses, study coordinators, and support staff who contributed to this study. Medical writing and editorial assistance was provided by ApotheCom (San Francisco, CA) and was supported by Global Blood Therapeutics, Inc. DISCLOSURES Carla B. Washington, Ganesh Balaratnam, Sandra Dixon, Erica Fong, Athiwat Hutchaleelaha, Margaret E. Tonda, and Josh Lehrer are employees of and have equity ownership in Global Blood Therapeutics. Michelle Green is a consultant for Global Blood Therapeutics. Adlette C. Inati is an advisor for Novo Nordisk. Carolyn C. Hoppe is a consultant or advisor for Bioverativ, Novartis, Cydan (Imara), and Global Blood Therapeutics. Winfred Wang receives funding from Global Blood Therapeutics for participation in the GBT440-007 and GBT440-031 studies. Clark Brown has nothing to disclose. This study was sponsored by Global Blood Therapeutics. http://bit.ly/2zX7Mog © 2017 Global Blood Therapeutics Presented at the 59th ASH Annual Meeting & Exposition; December 9–12, 2017; Atlanta, Georgia.
Transcript of The Pharmacokinetics (PK) of Voxelotor (GBT440) …...The goodness-of-fit plots indicate that the...
BACKGROUND • Sickle cell disease (SCD) is an autosomal recessive inherited disorder caused by a mutation in the β-chain of hemoglobin (Hb) that leads to the production of sickle hemoglobin S (HbS). When deoxygenated, HbS polymerizes into rigid chains that deform red blood cells (RBCs); this results in sickled RBCs, hemolysis, vaso-occlusion, and organ damage
• SCD is a congenital hemoglobinopathy whose disease complications begin in early childhood
• Voxelotor (previously called GBT440) is a first-in-class, oral, once-daily therapy that is designed to modulate the affinity of Hb for oxygen. Oxygenated HbS does not polymerize, so it is believed that voxelotor blocks polymerization and the resultant sickling of RBCs, thereby potentially modifying the course of SCD (Figures 1 and 2)
• GBT440-007 is an ongoing phase 2a study in pediatric patients (aged 6–17 years, including children [aged 6–11 years] and adolescents [aged 12–17 years]). The data presented are a summary of the analysis of a cohort of children (aged 6–11 years) receiving a single dose of voxelotor from Part A (Figure 3)
Figure 1. Voxelotor: designed to bind Hb with high selectivity.
Voxelotor
• Reversible covalent binding to the N-terminus of the Hb α-chain stabilizes oxy-Hb conformation
• Profile confirms properties with high selectivity for Hb – 1:1 stoichiometry of voxelotor to Hb tetramer binding – Preferential partitioning into RBCs – Potent, dose-dependent increase in Hb–oxygen (O2) affinity
Figure 2. Voxelotor mechanism of action: upstream interruption of HbS polymerization with potential to modify disease.
HbSPolymerization
Voxelotor
RBC Damage
HemolyticAnemia
Fatigue Organ Damage Pain Crisis
Mortality
Vaso-occlusion
Figure 3. GBT440-007 study design.
Part A – Single Oral Dose • Adolescents (12–17 years) 600 mg• Children (6–11 years) 600 mg
Part B – Multiple Oral Doses • Adolescents (12–17 years) 900 mg daily for 24 weeks• Adolescents (12–17 years) 1500 mg daily for 24 weeks
OBJECTIVESPart A Objectives • Primary:
– To characterize the pharmacokinetics (PK) of voxelotor in whole blood and plasma following a single dose of the drug in children and adolescents with SCD
• Secondary – To evaluate the safety and tolerability of voxelotor following a single dose of the drug in children and adolescents with SCD
The Pharmacokinetics (PK) of Voxelotor (GBT440) Following Single Doses in Pediatric Patients With Sickle Cell Disease (SCD)Carla B. Washington,1 Michelle Green,2 Adlette C. Inati,3 Clark Brown,4 Carolyn C. Hoppe,5 Winfred Wang,6 Ganesh Balaratnam,1 Sandra Dixon,1 Erica Fong,1 Athiwat Hutchaleelaha,1 Margaret E. Tonda,1 Josh Lehrer1
1Global Blood Therapeutics, South San Francisco, CA; 2Certara Strategic Consulting, Menlo Park, CA; 3Rafik Hariri University Hospital, Beirut, Lebanon; 4Aflac Cancer and Blood Disorders Center, Children’s Healthcare of Atlanta, Atlanta, GA; 5Children’s Hospital Oakland, Oakland, CA; 6St. Jude Children’s Research Hospital, Memphis, TN
980
PK Objectives • To compare the PK properties of voxelotor in children to those observed in adolescents and adults
• To support dose selection in ongoing studies evaluating the safety and efficacy of voxelotor in children and adolescents
• To select doses for children aged <12 years based on PK data and population PK (PPK) modeling to achieve similar exposures to the 2 doses (900 mg and 1500 mg) that are currently being investigated in the phase 3 HOPE (Hemoglobin Oxygen Affinity Modulation to Inhibit HbS Polymerization) study
METHODSKEY INCLUSION CRITERIA • Children aged 6 to 11 years with sickle cell anemia (SS) or sickle beta zero thalassemia (Sβ0 thal)
• Participants taking hydroxyurea needed to be on a stable regimen for ≥3 months
• Written informed parental/guardian consent ± subject assent
KEY EXCLUSION CRITERIA • Any of the following requiring medical attention within 14 days of signing the informed consent ± assent: – Vaso-occlusive crisis – Acute chest syndrome – Splenic sequestration crisis – Dactylitis
• Chronic transfusion therapy or transfusion within 30 days prior to consent • Having history of stroke or abnormal transcranial Doppler (ie, 2 transcranial Doppler measurements ≥200 cm/sec)
PK METHODS • Samples for PK analysis of voxelotor were collected at predose and at 2, 8, 24 hours (day 2), 48 hours (day 3), 96 hours (day 5), 168 hours (day 8), and 336 hours (day 15)
• Concentrations of voxelotor were determined in whole blood and plasma using validated liquid chromatography with tandem mass spectrometry assays
• A noncompartmental PK analysis using Phoenix® WinNonlin™ version 6.4.0 (Certara, Princeton, NJ) was performed using all available samples collected
• The single-dose PK data in children (aged 6–11 years) was compared to those in adolescents (aged 12–17 years)
• PPK models for whole blood and plasma were developed using NONlinear Mixed Effects Modeling (NONMEM) version 7.3 for children (aged 6–11 years) using the adult and adolescent PPK models with the addition of weight-based allometric scaling on clearance and central volume
• Prior in vitro and in vivo voxelotor data, including metabolism, protein binding, and physiochemical properties, were incorporated into a physiologically based PK (PBPK) model within Simcyp® Simulator version 14.1 (Certara) to estimate voxelotor exposures in children (aged <12 years)
RESULTS • All children (aged 6–11 years) have completed Part A of GBT440-007. The baseline characteristics for participants are summarized in Table 1
Table 1. Baseline Characteristics
Baseline Characteristics Part A n=6
Female, n 3
Male, n 3
Age, years, median (range) 8.5 (6–10)
Genotype, n
SS 5
Sβ0 thal 1
Concurrent hydroxyurea use, n (%) 6 (100)
Baseline Hb, g/dL, median (range) 8.5 (7.0–10.4)
Number of VOC during the past 12 months, n
0 2
1 3
4 1Hb, hemoglobin; Sβ0 thal, sickle beta zero thalassemia; SS, sickle cell anemia; VOC, vaso-occlusive crises.
SAFETY RESULTS • Voxelotor was well tolerated following a single dose (600 mg) in children (aged 6–11 years)
• No serious or severe, defined as grade ≥3, adverse events related to study drug were observed
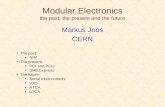
PK RESULTS • Following a single oral dose of voxelotor in children (6–11 years), maximum concentrations in whole blood and plasma were reached at 8 hours and 2 hours, respectively (Table 2)
• Voxelotor concentrations decreased in a monophasic manner, with a half-life in whole blood of 29.3 hours and plasma of 42.3 hours (Figure 4 and Table 2)
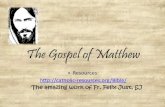
• Voxelotor PK exposures in children following a single dose of 600 mg were higher than those observed in adolescents (Figure 5 and Table 3)
• The PK parameters for adolescents were previously shown to be similar to adults,1 which was also confirmed in the estimated PPK parameters (Table 4)
• The same PPK model structures used to describe the adult (≥18 years) and adolescent voxelotor concentration profiles in whole blood and in plasma were used to describe the concentration profiles and estimate PPK parameters in children (Table 4)
• PPK model validation using visual predictive checks (VPCs) confirmed good agreement between the observed PK data for children and simulated profiles based on the pooled adult, adolescent, and children voxelotor PK model (Figures 6 and 7)
• Voxelotor exposures are higher in children (aged <12 years) compared with adults and adolescents and support lower weight-based dosing in this population. The weight-based doses are expected to provide voxelotor exposures similar to those observed in adults and adolescents (Figure 8 and Table 5)
• PBPK modeling also confirmed the need for lower doses in children aged <12 years and predicted similar weight-based voxelotor doses in this population (Table 5)
Table 2. Whole Blood and Plasma PK Parameters Following a Single Dose of Voxelotor 600 mg in Children Aged 6–11 Years (noncompartmental PK analysis)
PK Parameters Voxelotor in Whole Blood Voxelotor in Plasma
Cmax (µg/mL)a 47.3 (41.7%) 4.11 (49.3%)
Tmax (hr)b 8.0 2.0
AUC0-t (hr•µg/mL)a 2785.4 (51.8) 177.4 (34.8%)
T1/2 (hr)c 29.3 ± 7.7 42.3 ± 13.5
AUC0-t, area under curve to the time of the last quantifiable concentration; Cmax, maximum observed blood concentration; Tmax, time-average maximum; T1/2, time needed for concentration to reduce by half (half-life).aValues reported as geometric means (percentage of coefficient of variation).bMedian.cValues reported as arithmetic means ± standard deviation.
Figure 4. Whole blood and plasma voxelotor concentrations following a single dose of voxelotor 600 mg in children aged 6–11 years.
1
10
100
1000
10,000
100,000
1,000,000
Vo
xelo
tor
Co
ncen
trat
ion,
ng
/mL
Time, hr
0 100
Children (6–11 years) Plasma
Children (6–11 years) Whole Blood
200 300 400
Figure 5. Voxelotor plasma and whole blood exposures in children are higher than those observed in adolescents.
0
20,000
40,000
60,000
80,000
Vo
xelo
tor
Co
ncen
trat
ion,
ng
/mL
Time, hr
0 100
Adolescents Plasma
Children (6–11 years) Plasma
Adolescents Whole Blood
Children (6–11 years) Whole Blood
200 300 400
Table 3. Voxelotor Single-Dose Whole Blood PK Exposures Were Higher in Children Compared With Adolescents
Voxelotor Whole Blood PK Parameters:
Children Aged 6–11 Years
Voxelotor Whole Blood PK Parameters:
Adolescentsn=6 n=7
Cmax (µg/mL)a 47.3 (41.7%) 24.2 (47.7%)Tmax (hr)b 8.0 24.0AUC0-t (hr•µg /mL)a 2785.4 (51.8%) 1663.1 (43.8%)T1/2 (hr)c 29.3 ± 7.7 32.3 ± 6.1
AUC0-t, area under curve to the time of the last quantifiable concentration; Cmax, maximum observed blood concentration; Tmax, time-average maximum; T1/2, time needed for concentration to reduce by half (half-life). aValues reported as geometric means (percentage of coefficient of variation).bMedian. c Values reported as arithmetic means ± standard deviation.Similar differences in exposures were also observed in plasma.
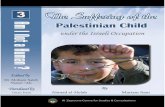
Figure 6. Goodness-of-fit plots and VPC for the PPK model.
Who
le B
loo
d V
oxel
oto
rC
onc
entr
atio
n, n
g/m
L
Normal Time after Dose, hr Normal Time after Dose, hr
10000
1000
100
50000
40000
30000
20000
10000
0
Who
le B
loo
d V
oxel
oto
rC
onc
entr
atio
n, n
g/m
L
0 0 50 100 150 200100 200 300
Ob
serv
atio
ns
Population Predictions
150000
100000
50000
0
0 50000 100000 150000
Ob
serv
atio
ns
Individual Predictions
150000
100000
50000
0
0 50000 100000 150000
VPC, visual predictive check.The goodness-of-fit plots indicate that the pooled PPK model describes the data adequately with little model bias. The prediction-corrected VPC shows the model fit and observed data after a single voxelotor dose in children and adolescents.
VOXELOTOR PPK MODEL DESCRIPTION • The PPK of voxelotor in children, adolescents, and adult patients with SCD was best described by a 2-compartment model with first-order absorption and first-order elimination. Key model parameters are summarized in Table 4
• For the voxelotor PPK model in whole blood, the typical value of the apparent intercompartmental clearance (Q/F) was 0.0015 L/hr and the typical value of the apparent peripheral volume of distribution (Vp/F) was 0.34 L
• For the voxelotor PPK model in plasma, the typical value of the apparent Q/F was 0.38 L/hr and the typical value of the apparent Vp/F was 79 L
• The PPK model included estimates of between-subject variability on apparent clearance (CL/F) and apparent central volume (Vc/F). A proportional residual error model was used
• The prediction-corrected VPC and goodness-of-fit diagnostic plots for the whole blood model (Figure 6) and plasma model (not shown) indicate that the model describes the data adequately
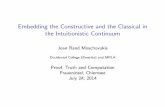
Figure 7. Individual plots for the pediatric PPK model.
ID: 101104 ID: 101106ID: 101103
ID: 101101 ID: 101102ID: 101100
Who
le B
loo
d V
oxe
loto
rC
onc
entr
atio
n, n
g/m
L
1e+05
10000
1000
100
0 100 200 300
Time After Dose, hr0 100 200 300 0 100 200 300
1e+05
10000
1000
100
Who
le B
loo
d V
oxe
loto
rC
onc
entr
atio
n (n
g/m
L) 80000
ID: 101104 ID: 101106ID: 101103
ID: 101101 ID: 101102
Time After Dose, hr
ID: 101100
IPREDDV • • • PRED
60000
40000
20000
0
80000
60000
40000
20000
0
0 100 200 300
0 100 200 300 0 100 200 300
Individual plots showing the observed data from GBT440-007 (black symbols) overlaid with individual (IPRED, red line) and population (PRED, blue dashed line) predictions from the adolescent PPK model.
Table 4. Model PPK Parameter Estimates for Voxelotor in Adult and Adolescent Participants With SCD
PK Parameters
Voxelotor in Whole Blood: Adults
Voxelotor in Whole Blood: Adolescents
Voxelotor in Whole Blood: Children Aged 6–11 Years
n 42 17 6
CL (L/hr) 0.43 0.40 0.24
V (L) 21.4 18.9 9.55
Ka (1/hr) 0.34 0.30 0.33
T1/2 (hr) 34.5 32.7 27.8
Voxelotor in Plasma: Adults
Voxelotor in Plasma: Adolescents
Voxelotor in Plasma: Children Aged 6–11 Years
CL (L/hr) 7.63 5.48 3.67
V (L) 373 267 140
Ka (1/hr) 2.83 1.57 3.3
T1/2 33.9 33.8 26.4
CL, apparent clearance; Ka, absorption rate constant; T1/2, half-life; V, apparent volume of distribution.
Figure 8. Simulations of whole blood voxelotor exposures following 900 and 1500 mg-equivalent doses in children.
0
100
200
300
Cm
inss
, μg
/m
L
Weight Group, kg
900 mg-equivalent doses
5, 10 10, 20 20, 40 >40
0
100
300
500
Cm
inss
, μg
/m
L
Weight Group, kg
1500 mg-equivalent doses
200
400
5, 10 10, 20 20, 40 >40
200 mg 400 mg 600 mg 900 mg 400 mg 600 mg 900 mg 1500 mg
Modeling and simulation were used for the selection of doses based on weight bands for pediatric patients down to 9 months of age. Preliminary dose estimates of 200, 400, and 600 mg voxelotor are supported in patients weighing 5 to <10 kg, 10 to <20 kg, and 20 to <40 kg, respectively, to provide exposures similar to adolescent patients at 900 mg. Dose estimates of 400, 600, and 900 mg, respectively, are supported to provide exposures similar to adolescent patients at 1500 mg. The horizontal dashed lines indicate the interquartile range of simulated adolescent exposures.
Table 5. Voxelotor Projected Doses Selected for Children Aged <12 Years Based on PPK Modeling and PBPK Modeling
Population 900 mg-Equivalent Adult Dose
1500 mg-Equivalent Adult Dose
5 to <10 kg 200 mg 400 mg
10 to <20 kg 400 mg 600 mg
20 to <40 kg 600 mg 900 mg
≥40 kg 900 mg 1500 mg
CONCLUSIONS • Voxelotor was well tolerated following a single dose (600 mg) in children (aged 6–11 years)
• Voxelotor PK exposures were higher in children compared with adolescents and adults, so lower doses are recommended in children
• Body weight was a significant covariate on voxelotor clearance (CL) and volume (Vc) supporting weight-based doses in children aged <12 years
• PPK and PBPK modeling are being used to simulate voxelotor PK parameters to support voxelotor dose selection for evaluation in younger children aged 9 months to <12 years
• These analyses combining PPK and PBPK modeling provide an innovative approach to minimize experimental dosing in children and accelerate dose selection
REFERENCE1. Washington C et al. Poster presented at: 22nd Congress of the European Hematology Society;
June 22–25, 2017; Madrid, Spain.
ACKNOWLEDGMENTSThe authors thank all of the participants, families, caregivers, research nurses, study coordinators, and support staff who contributed to this study. Medical writing and editorial assistance was provided by ApotheCom (San Francisco, CA) and was supported by Global Blood Therapeutics, Inc.
DISCLOSURESCarla B. Washington, Ganesh Balaratnam, Sandra Dixon, Erica Fong, Athiwat Hutchaleelaha, Margaret E. Tonda, and Josh Lehrer are employees of and have equity ownership in Global Blood Therapeutics. Michelle Green is a consultant for Global Blood Therapeutics. Adlette C. Inati is an advisor for Novo Nordisk. Carolyn C. Hoppe is a consultant or advisor for Bioverativ, Novartis, Cydan (Imara), and Global Blood Therapeutics. Winfred Wang receives funding from Global Blood Therapeutics for participation in the GBT440-007 and GBT440-031 studies. Clark Brown has nothing to disclose.
This study was sponsored by Global Blood Therapeutics. http://bit.ly/2zX7Mog
© 2017 Global Blood TherapeuticsPresented at the 59th ASH Annual Meeting & Exposition; December 9–12, 2017; Atlanta, Georgia.