The Canadian Review of - STA HealthCare … Canadian Review of Alzheimer’s Disease and Other...
32
The Review is online! You can find us at: www.stacommunications.com/ adreview.html The Canadian Review of Volume 11, Number 1 • January 2008 FOCUS ON IMAGING Potential Impact of Amyloid Imaging in Vivo on AD Treatment and Management 4 Nicolaas Paul L.G. Verhoeff, MD, PhD, FRCPC Imaging and Alzheimer’s Disease: A Review 13 Christian Bocti, MD, FRCPC Molecular Imaging of Alzheimer’s Disease Using PET 18 Pedro Rosa-Neto, MD, PhD; and Antoine Leuzy Advocating for Change: Making Dementia a National Health Priority 30 The Alzheimer Society of Canada Art by Sylvia Sinclaire
Transcript of The Canadian Review of - STA HealthCare … Canadian Review of Alzheimer’s Disease and Other...

The Review is online! You can find us at:
www.stacommunications.com/
adreview.html
The Canadian Review ofVolume 11, Number 1 • January 2008
FOCUS ON IMAGING
Potential Impact of AmyloidImaging in Vivo on AD Treatment andManagement 4Nicolaas Paul L.G. Verhoeff, MD, PhD, FRCPC
Imaging and Alzheimer’sDisease: A Review 13Christian Bocti, MD, FRCPC
Molecular Imaging ofAlzheimer’s Disease Using PET 18Pedro Rosa-Neto, MD, PhD; andAntoine Leuzy
Advocating for Change:Making Dementia a National Health Priority 30The Alzheimer Society of Canada
Art by Sylvia Sinclaire

CHAIRMANPeter N. McCracken, MD, FRCPCProfessor Emeritus of Medicine, Division of Geriatric MedicineUniversity of Alberta Edmonton, Alberta
Paul J. Coolican, MD, CCFP, FCFP Family Physician, St. Lawrence Medical ClinicMorrisburg, Ontario Active Staff, Winchester District Memorial HospitalWinchester, Ontario
Shannon Daly, RN, MNClinical Nurse Specialist in GeriatricsGrey Nuns Community Hospital & Health CentreEdmonton, Alberta
Howard Feldman, MD, FRCPCProfessor of Medicine,Division of Neurology,University of British Columbia (UBC)Director, UBC Alzheimer Clinical Trials UnitVancouver, British Columbia
Serge Gauthier, MD, CM, FRCPCProfessor of Neurology and Neurosurgery, Psychiatry and Medicine, McGill UniversityMcGill Centre for Studies in AgingMontreal, Quebec
Bernard Groulx, MD, CM, FRCPC Chief Psychiatrist, Ste-Anne-de-BellevueHospitalAssociate Professor, McGill UniversityMcGill Centre for Studies in AgingMontreal, Quebec
Nathan Herrmann, MD, FRCPCProfessor, University of TorontoHead of the Division of GeriatricPsychiatry, Sunnybrook Health Science CentreToronto, Ontario
Peter J. Lin, MD, CCFPPast Medical Director, University of TorontoHealth & Wellness Centre at ScarboroughDirector, Primary Care Initiatives,Canadian Heart Research CentreMedical Director, LinCorp Medical Inc.Toronto, Ontario
Kenneth Rockwood, MD, MPA, FRCPCProfessor of Medicine, Kathryn Allen Weldon Professor ofAlzheimer Research Dalhousie UniversityGeriatrician, Queen Elizabeth II HealthSciences CentreHalifax, Nova Scotia
Copyright 2008 STA HealthCare Communications Inc. All rights reserved. The Canadian Review of Alzheimer’s Disease and Other Dementias is published by STACommunications Inc. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the publisher. Physicians should take intoaccount the patient’s individual condition and consult officially approved product monographs before making any diagnosis or treatment, or following any procedurebased on suggestions made in this document. Publications Agreement Number 40063348.
Publishing Staff
Editorial Board
On the Cover…
This watercolor was produced by Sylvia Sinclaire, a remarkable 83-year-old, who wasdiagnosed with dementia right after her retirement from teaching art. Creativeexpression allows us glimpses into Sylvia’s mind, and this same artistic expressionoffers her an avenue to us, if only temporarily. Her humour and positive attitude, inspite of her awareness of her disease, reminds us that we should not let our ownpreconceptions about illness blind us to the potential of the human spirit. She completed this work during an art session with Dr. Dalia Gottlieb-Tanaka, whodeveloped the Creative Expression Activities Program, and has worked with andfilmed Sylvia for five years.
The editorial board has complete independence in reviewing the articles appearing in this publication and isresponsible for their accuracy. The advertisers exert no influence on the selection or the content of materialpublished.
Paul F. BrandExecutive Editor
Russell KrackovitchEditorial Director, Custom Division
Maeve BrooksManaging Editor
Mandi WatsonAssociate Editor
Dana WittenbergerEditor-proofreader, French
Donna GrahamProduction Manager
Dan OldfieldDesign Director
Jennifer BrennanFinancial Services
Sherri TobinAdministrative Assistant
Robert E. PassarettiPublisher
2 • The Canadian Review of Alzheimer’s Disease and Other Dementias
The Canadian Review of

E D I T O R I A L
Neuroimaging in Alzheimer’sDiseaseBy Peter Lin, MD, CCFP
The Canadian Review of Alzheimer’s Disease and Other Dementias • 3
This edition is devoted to the advances in neu-roimaging for Alzheimer’s disease (AD).
Broadly speaking, imaging can be put into threelarge categories:• structural imaging;• pathologic imaging; and• functional imaging.
Dr. Bocti reviews the importance of structuralimaging with computed tomography (CT) andmagnetic resonance imaging (MRI) scans. Thesescans can help to rule out diseases as well asdetect AD as they are able to detect atrophy instrategic locations which has become the hall-mark sign for AD. As well, the presence of silentcerebrovascular disease is also important as it sig-nificantly worsens the dementia presentation.Futuristic MRI scans can even detect healthy ver-sus unhealthy white-matter tracks which may allowfor earlier detection of the diseased neurons.
Dr. Verhoeff discusses the use of tracers thatcan attach to amyloid or tau. This would allow usto image the location and to quantify the patho-logic burden. This could be used to detect earlierstages of the disease, maybe even before signifi-cant neuronal death has occurred. This type of
pathologic imaging will also play a critical role inassessing the efficacy of the newer therapies thattarget the amyloid pathways and, in turn, couldaccelerate the drug-discovery program for thesedisease-modifying agents.
Finally in this issue, Dr. Rosa-Neto exploresthe area of molecular imaging whereby the func-tioning status of neurons can be measured.Fluorodeoxyglucose (FDG), a glucose analog,can be followed with positron emission tomogra-phy (PET) to see where the metabolically activecells are and where they are not. Neurons that aredying use less glucose. In the coming years, usingother molecular tags, we will be able to measureinflammation of the microglia and even neuro-transmission of acetylcholine cells using thissame technology.
In a sense, all of these imaging modalities aretrying to do the same thing: help us to understandthe disease process and to pick out patients at anearlier stage of the AD spectrum. Perhaps one dayall scans can be combined together to identifypatients of vulnerability, and targeted therapiescan be administered to these patients to avoid thedisease from ever materializing.

Potential Impact of Amyloid Imagingin Vivo on Alzheimer’s DiseaseTreatment and ManagementBeta-amyloid (Aß) modification therapies for Alzheimer’s disease (AD) are currently beingdeveloped that target Aß production, aggregation, and/or degradation. Some of thesemedications are already in Phase 3 studies. It will therefore be most relevant to be able toquantify the neurobiological target of such therapies directly in vivo in the brain. This couldpermit a reduction in the required sample size for future clinical trials and will allow a moreindividually tailored approach once such treatments become clinically available. This articlereviews the prevalence of AD amongst other dementias, the Aß cascade, various Aßpositron emission tomography (PET) tracers that are being developed, and the potentialapplication of these tracers for Aß-modification therapies.
By Nicolaas Paul L.G. Verhoeff, MD, PhD, FRCPC
Dementia is common in olderadults and approximately
doubles in frequency every fiveyears, from about 1% of peopleaged 60 years to 30% to 40% ofthose aged 85 years of age andolder.1,2 AD3 is the leading neu-rodegenerative disorder, account-ing for approximately one third totwo thirds of dementia cases.2,4
Improving early detection of ADand studying the effects of newtreatments for AD are of epidemicimportance. Studies indicate that,on average, acetylcholinesterase-inhibitor (AChEI) treatment
delays cognitive decline in ADpatients by nine to 12 months andthe need for institutionalization by18 months.5-9 Moreover, at oneyear, superior cognitive perform-ance was observed in patientswho started AChEI treatment atthe beginning than in those whostarted six months after the begin-ning in trials with rivastigmine,10
galantamine11 and donepezil.12
Therefore, it would be prudent toapply functional neuroimagingwithin six months of identifyingprogressive cognitive decline thatcould represent incipient AD.
Although the accuracy of theclinical evaluation for AD3 can befurther improved with [18F]fluo-rodeoxyglucose ([18F]FDG) glu-cose metabolism positron emissiontomography (PET)13,14 or perfu-sion single photon emission com-
puted tomography (SPECT),15 fur-ther improvements can be expectedfrom imaging in vivo of more spe-cific pathological processes forAD: extraneuronal Aß plaques,16-19
intraneuronal neurofibrillary tan-gles (NFT),16,20-22 and interneu-ronal synapse loss.23,24 To ourknowledge, no NFT-specific orsynapse-loss-specific tracers havebeen developed for imaging invivo. Therefore, this article focuseson Aß-specific tracers.
The ß-amyloid CascadeMechanism of Aß production.The Aß1-40 and Aß1-42 (peptidesof 40 to 42 amino acids) arederived from a transmembraneprotein named amyloid precursorprotein (APP).25 There are twoAPP cleavage pathways:18
• The non-amyloidogenic
4 • The Canadian Review of Alzheimer’s Disease and Other Dementias
Nicolaas Paul L.G. Verhoeff, MD,PhD, FRCPC, Clinician-Scientist,Kunin-Lunenfeld Applied ResearchUnit, and Staff Psychiatrist,Baycrest Memory DisordersClinic, Associate Professor ofPsychiatry, University of Toronto.

The Canadian Review of Alzheimer’s Disease and Other Dementias • 5
pathway: APP cleaved by α-secretase into fragments thatdo not contain intact Aß; thispathway does not result inamyloid deposition in thebrain; and,
• The amyloidogenic pathway:APP is cleaved by ß-secretase(or ß-amyloid cleavingenzyme, [BACE]), followedby γ-secretase cleavage.BACE cleavage liberates ß-APP that contains the Aßpeptide fragment, and γ-secretase cleavage liberatesthe Aß peptide from ß-APP.The Aß peptides aggregate tosenile plaques in the brainparenchyma and to cerebralamyloid angiopathy (CAA) inthe blood-vessel walls.26
Aggegation of Aß into senileplaques. Senile plaques are aform of Aß accumulation and areone of the earliest pathologicalchanges that appear before neu-ronal loss occurs in the aging andthe AD brain.17 Senile plaqueshave two histologically differentforms, which are thought toimpact on disease symptoms andprogression:17
• Diffuse plaques consist ofamorphous Aß, lack the ß-sheet structure and are notsurrounded by dystrophic neurites.27 They are associatedwith normal aging.
• Dense-core (or neuritic) plaquesconsist of fibrillar Aß and arefound mostly in patients withAD, but also in a small amountin the normal aging brain.28
Fibrillar Aß has the conforma-tion of a ß-sheet structure, whichis specifically detected by Congored or Thioflavin T staining.29
Most of the PET Aß radioligandsdiscussed below have beenderived from these two dyes andare thought to be mainly bindingto fibrillar Aß.
Amyloid PET and SPECTImaging Agents inDevelopment (Table 1)There has been considerable inter-est in measuring regional cerebralAß levels in vivo with magneticresonance imaging (MRI), PET orSPECT. MRI can provide high-res-olution images, but necessarilyrequires large amounts of contrastagents, such as Gd[N-4ab/Q-
4ab]Abeta-3030 or Gd-DTPA-K6Abeta1-30 in mannitol solution,to transiently open the blood-brainbarrier,31 or a very high magneticfield strength, e.g., 7 Tesla,32 togenerate reasonable signal:noiseratios. This review focuses on PETand SPECT, which can more sensi-tively measure much lower (i.e.,tracer) concentrations of small-molecule radioligands that can passthe blood brain barrier.33
The first successful in vivoattempt to image Aß plaques inthe AD brain used PET and the
malononitrile derivative [18F]2-(1-{6-[(2-fluoroethyl)methyl-amino]-2-naphthyl}ethylidend)malononitrile ([18F]FDDNP).34
The differences between nine ADpatients and seven controls weredemonstrated using the relativeresidence time (RRT) of the fore-brain regions versus the pons.However, since the RRT is proba-bly sensitive to peak and steady-state tracer levels, additionalanalyses have been used such asstandardized uptake values atequilibrium normalized to thecerebellum and Logan distribu-tion volume ratios with the cere-bellum as reference region,35 pro-viding similar results. The area ofhighest retention at equilibriumwas the hippocampus, amygdala
and entorhinal cortex region,where NFTs are mainly concen-trated post mortem.20 In contrast,autopsy studies16 have shown thatdense-core Aß plaques are moredensely concentrated in lateraltemporal and occipital lobes whilelimbic areas, including the hip-pocampus, amygdala and entorhi-nal cortex region, contain thefewest dense-core Aß plaques.Therefore, it has been hypothe-sized that [18F]FDDNP may be anin vivo marker for NFT as well asfor diffuse and dense-core Aß
Dementia is common in older adults and approximatelydoubles in frequency every five years, from about 1% of people aged 60 years to 30% to 40% of those aged
85 years of age and older.

6 • The Canadian Review of Alzheimer’s Disease and Other Dementias
plaques.36 This could increase theability of this tracer to detectpresymptomatic AD, but it alsosuggests that [18F]FDDNP is nota solely Aß-specific radiotracer,complicating its use in monitor-
ing the effectiveness of Aß-reducing medication. Moreover,[18F]FDDNP PET may also bepositive for tau aggregation infrontal-lobe dementia dementia37
and for prion pathology.38,39 The
use of [18F]FDDNP as an Aß PETtracer is further complicated bythe intriguing finding thatFDDNP competes with some butnot all non-steroidal anti-inflam-matory drugs (NSAIDs) for bind-ing to Aß fibrils in vitro and to Aßplaques ex vivo,40 and by the factthat the conventional parametersfor kinetic analysis of receptorbinding (such as affinity [1/Kd]and receptor density [Bmax]) maynot be sufficient to accuratelyquantify Aß binding.41
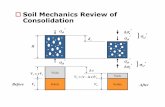
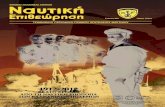
The second successful in vivoattempt to image Aß plaques inthe AD brain used the benzothia-zole aniline derivative [11C]2-(4’-(methylaminophenyl)-6-hydroxybenzothiazole ([11C]6-OH-BTA-1, also referred to as[11C]PIB), which has been report-ed to bind specifically to fibrillarAß at tracer concentrations invivo42 (Figure 1). Compared withnine healthy controls, 16 mild-ADpatients typically showed markedretention of [11C]PIB in areas ofassociation cortex known to con-tain large amounts of amyloiddeposits in AD, such as frontal,parietal, temporal, and occipitalcortices and the striatum.[11C]PIB retention was equivalentin AD patients and healthy con-trols in areas known to be relative-ly unaffected by amyloid deposi-tion, such as subcortical whitematter, pons, and cerebellum. Ofnote, significant and high correla-tions were observed between invivo [11C]PIB PET and post-mortem [3H]PIB and Aß Enzyme-
Table 1
Radioligands for Aß Imaging By PET or SPECT
Modality Radioligand Species
[18F]FDDNP Human34
[11C]PIB Human42
[11C]SB-13 Human121
[11C]ST1859 Human104
[11C]BF-227 Human55
[18F]3’-F-PIB Human59
[18F]FMS-IMPY Monkey105
[18F]FES-IMPY Monkey105
[18F]FBM Mouse106
[18F]6-methoxyphenyl-BTA Mouse107
[18F]6-methylphenyl-BTA Mouse107
[18F]FPEG-PIB Mouse108
[18F]FPEG-stilbenes Mouse109
[18F]FPEG-alkynes Mouse110
[18F]FP-PIB Mouse111
[18F]2-methylphenyl-BTA Mouse112
[18F]2-methylphenyl-BOX Mouse112
[18F]FP-curcumin Mouse113
[123I]IMPY Human57
[123I]IBOX Mouse114
[124I]clioquinol Mouse115
[125I]styrylchromones Mouse116
[125I]chalcones Mouse117
[125I]styrylpyridines Mouse118
[125I]bisphenyltriazoles Mouse119
[125I]alkynes Mouse120
PositronEmissionTomography(PET)
Single PhotonEmissionComputedTomography(SPECT)

The Canadian Review of Alzheimer’s Disease and Other Dementias • 7
Linked Immunosorbent Assay(ELISA) uptake in 14 brainregions examined, in one 63-year-old female severe-AD patient.43 Asignificant negative correlationbetween [18F]FDG and [11C]PIBretention was observed in the pari-etal cortex but not in the frontalcortex at initial and two-year fol-low-up evaluations.44,45 This isinteresting as in vitro studies havesuggested that the neurotoxicityof fibrillar Aß is related toimpaired glucose transport46 andis enhanced under conditions ofreduced glucose metabolism,47
while in vivo [18F]FDG PET andpostmortem neuropathology dataonly suggested correlations withNFT but not with Aß deposition.48
The relationship between glu-cose metabolism and Aß patholo-gy may be different in distinctbrain regions of AD patients, andAß plaque formation may not bedirectly responsible for neuronaldysfunction45 in all brain regions.Simplified quantification methodshave been validated for [11C]PIBagainst kinetic modeling usingarterial input data and graphicaland compartmental approach-es,49,50 and parameters derivedfrom 60 minutes may be similar tothose from 90 minutes acquisitiontime.51 Voxel-based analyses of[11C]PIB PET data have con-firmed the previously obtainedregion-of-interest data52,53 andhave shown that [11C]PIB PETwas superior to [18F]FDG PET indiscriminating mild-to-moderateAD patients from healthy con-
trols.45,53 Also, [11C]PIB providedbetter contrast between three ADpatients and three controls than[18F]FDDNP.54
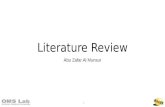
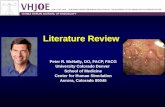
The third successful in vivoattempt to image Aß plaques inthe brain of AD patients comparedthe novel stilbene derivative[ 1 1C ] 4 - N - m e t h y l a m i n o - 4 ’ -hydroxystilbene ([11C]SB-13)
with [11C]PIB in five female ADpatients versus six matchedhealthy controls121 (Figure 2). Thetwo radiotracers demonstratedsimilar binding properties withrespect to regional distribution ofretention (increased retention inthe frontal and posterior temporal-inferior parietal association cor-tices in the AD patients, but not in
Figure 1
[11C]PIB Binding: Control vs. Mild AD
A. Parametric maps ofLogan’s invasive modelDistribution Volume (a measure for Aßbinding potential) fromdata 0-120 minutes afterIV injection of 10.4 mCi[11C]PIB in a 74-year-old female healthycontrol subject.121
B. Parametric maps ofLogan’s invasive modelDistribution Volume (ameasure for Aß bindingpotential) from data 0-120 minutes after IVinjection of 9.5 mCi [11C]PIB in a74-year-old femalemild-AD patient.121

the controls). The data indicatedthat [11C]SB-13 may be similar to[11C]PIB in discriminating ADpatients from healthy controls.
The fourth successful in vivoattempt to image Aß plaques inthe brain of AD patients used thebenzoxazole derivative [11C]2-[2-(2-dimethylaminothiazol-5-yl)ethenyl]-6-[2-(fluoro)ethoxy]benzoxazole ([11C]BF-227) andshowed retention in the frontal,temporal and parietal cortices in 10 AD patients, who could be distinctly differentiated from 11 healthy controls.55
The fifth successful in vivoattempt to image Aß plaques inthe brain of AD patients was madewith a SPECT radioligand:[123I]6-iodo-2-(4’dimethylamino)phenyl-imidazo[1,2-]pyridine([123I]IMPY).56,57 In one study, theaverage cortical:cerebellar equilib-rium distribution volume ratios
were 1.25 in eight AD patients ver-sus 1.06 in seven healthy con-trols,57 and 1.22 in four ADpatients versus 0.85 in three healthycontrols in another study.56
However, [123I]IMPY may not beselective for Aß only, as it has alsobeen reported to bind to priondeposits in scrapie-infected mice.58
Additional studies are in progress tomore fully validate [123I]IMPY as apotential tool for assessing ADonset and progression. Given thelonger radioactive half-life of 123I(13.2 hours), such tracers could besynthesized at one location andtransported to a nuclear-medicinefacility with a SPECT scanner atanother location, greatly increasingthe accessibility of this Aß imagingmethod to patients across the globe.
Successful attempts haverecently been made in vivo in ADpatients with 18F-labelled Aßradiotracers.59,60 Like 123I, 18F
has a much longer radioactive half-life (110 minutes) than 11C (20 min-utes), allowing Aß imaging at PETcentres without on-site cyclotrons.Given the fact that PET scannershave become much more prevalentat nuclear-medicine departments,this may also greatly increase theaccessibility of this Aß imagingmethod.
Aß Modification TherapiesAß modification therapies targetamyloid production, amyloidaggregation, and/or amyloid degra-dation. Some of them are being test-ed in on going clinical trials.61-64
Alpha-secretase activators includestatins and estrogen. It has beensuggested that some AChEIs maystimulate the non-amyloidogenicα-secretase cleavage of APP aswell.65 Beta-secretase inhibitorsinclude TAK-070.66 Gamma-secre-tase inhibitors include LY45 -0139,67 nonpeptidic isocoumarincompounds (JLK inhibitors),68
STI571 imatinib mesylate,69,70 andNSAIDs.70 Gamma-secretase mod-ulators include R-flurbiprofen(MPC-7869 or tarenflurbil).71,72
Especially, tarenflurbil has finishedits Phase 2 trials in Canada andEngland in 2005, and presentlyPhase 3 trials in AD patients are ongoing in the U.S. and Canada.Tarenflurbil has shown apparenteffect on activities of daily living,CDR score, and the Alzheimer’sDisease Assessment Scale-cognitiveitems (ADAS-cog) test.73
Amyloid-aggregation-targetingtherapies by antifibrillization
8 • The Canadian Review of Alzheimer’s Disease and Other Dementias
Figure 2
[11C]SB-13 Binding in Moderate AD
Parametric maps ofLogan’s invasive modelDistribution Volume (ameasure for ß-amyloidbinding potential) fromdata 0-60 minutes afterIV injection of9.5 mCi [11C]SB-13 in a 73-year-old femalemoderate-AD patient.121

include the glycosaminoglycanmimetic NC-531(tramiprostate),61,74
PBT-2, PPI-1019, and TTP-448.Tramiprostate was originallydeveloped by Neurochem inMontreal, Canada. The results ofa Phase 3 trial have been collectedbut—to our knowledge—not yetbeen reported.
The very latest drug is a cyclo-hexanehexol stereoisomer, whichblocks the accumulation of Aßoligomers and reduces AD-likebehavioral deficits, AD-like neu-ropathology, and accelerated mor-tality in a transgenic mouse modelof AD.75 Because this drug is ableto alter Aß pathology even afterthe symptoms appear, it seemsvery useful to be applied not onlyto preclinical-AD subjects butalso to AD patients.
Immunization is one Aß modifi-cation therapy option that has beenstudied in transgenic mice and ADpatients. Although immunizationimproves cognitive function in APPtransgenic mice76,77 and may slowcognitive decline in AD patients,78
and although it reduces Aß plaquesin APP transgenic mice79 and pos-sibly also in AD patients,80 thestudies in AD patients had to be ter-minated prematurely owing tobrain hemorrhage81 and/or menin-goencephalitis.80,82 Pathologicalevidence of the post-immunizationpatients showed that, althoughthere is no effect on the frequencyand severity of CAA per se, hemor-rhages could clearly be attributed toamyloid-laden blood vessels, andbleedings only occurred in brain
areas affected by CAA.81Antibodyresponders to active immunizationwith AN1792 had better cogntivefunction but more brain volumeloss.83 Passive immunization hasbeen tested in PDAPP transgenicmice,84-86 but to our knowledge, noclinical studies have been per-formed.
Potential Impact of AßImaging on AD ManagementAs cerebral fibrillar Aß depositionmay occur decades before themanifestation of the clinical ADsyndrome,19,87,88 imaging of thispathology in vivo may gain con-siderable amount of time for ther-apies that intend to prevent Aßaccumulation, (e.g., by inhibitingfibrillar Aß production or aggrega-tion). A syndrome of amnesticmild cognitive impairment (MCI)
has been identified for which sub-jects are at an increased risk of pro-gression to AD. MCI subjectshave—depending on the definitionand group from which the subjectshave been recruited—an annualincidence of about 12% progress-ing to AD in contrast to 1% to 2%for cognitively normal subjectsfrom the same community.89 TheseAß production or aggregation-inhibiting treatments may be the
most effective at earlier stages, (i.e.,as preventive rather than curativetherapies). There are several in vivoAß neuroimaging data that, whencombined, suggest that treatmentneeds to start as early as possible: 1. The [11C]PIB PET follow-up
study has shown a relatively stable [11C]PIB uptake over twoyears in mild-AD patients.44,90
2. Amnestic MCI subjects as agroup have an [18F]FDDNPuptake between that of cognitively normal subjectsand mild-AD patients.35
3. Some non-demented oramnestic MCI subjects alreadyhave an increased uptake comparable to mild-ADpatients of [11C]PIB.50,91-95 orof [11C]BF-227.96
4. These increases in [11C]PIBuptake in non-demented
subjects may be related to performance decline in cognitive tests that are highlysensitive to AD-like memorychanges.94,97-99
Of interest, the pattern of Aßdeposition in subjects with autoso-mal dominant PS1 mutations, pre-disposing to early-onset familialAD, is different from sporadic late-onset AD, with earlier and higher[11C]PIB retention in the stria-
The Canadian Review of Alzheimer’s Disease and Other Dementias • 9
The pattern of Aß deposition in subjects withautosomal dominant PS1 mutations, predisposing to
early onset familial AD, is different from sporadic lateonset AD, with earlier and higher [11C]PIB retention
in the striatum.

tum.100 Cerebral [11C]PIB bind-ing was inversely correlated withcerebrospinal fluid (CSF) Aß-42levels in a mixed group of sub-jects with Clinical DementiaRatings varying from zero (nodementia) to two (moderate demen-tia).90,101 Of note, three cognitivelynormal subjects showed high[11C]PIB uptake with low CSFAß-42, suggesting preclinicalAD.19,87,88 It may therefore bethat subjects at risk will have to beidentified even at a stage prior toamnestic MCI for these preven-tive therapies to be fully effective.
Since CAA is assumed to be acontraindication to Aß immuniza-tion (vide supra),81 screening forthis prior to immunization therapymight improve its results. The gra-dient-echo (GE) or T2-weightedMRI technique and Aß imagingcould be performed in ADpatients to assess for CAA and
cerebral ß-amyloidosis, respec-tively, prior to immunization ther-apy to prevent post-immunizationbrain hemorrhage.26,81 Moreover,[11C]PIB PET might also be ableto detect CAA in the absence ofcerebral ß-amyloidosis.102
Given the fact that thereappeared to be no change in Aßbinding measured with [11C]PIBPET over two years in mild-ADpatients,44 and that the test-retestreliability of [11C]PIB PET isabout 3% to 7%,44,50 it has beenestimated that anti-Aß therapyneeds to induce at least a 15%decrease in Aß load before itseffect can be detected.103
Incorporating in vivo Aß PETmay make clinical trials more effi-cient, as the target patient popula-tion group can be better definedand a relevant neurobiologicaloutcome measure can be assessedthat may be more sensitive than,
and predictive of, assessments ofclinical outcome.
ConclusionsAß PET can contribute to themanagement of AD by helping to:• establish whether there is a
cerebral ß-amyloidosis underlying the dementia syndrome, which can helpwith the differential diagnosisof the potential cause(s) of thedementia;
• identify patients at risk ofdeveloping AD, who would besuitable candidates for anti-Aßtherapies (particularly medications that target Aßproduction or aggregation);
• select patients for anti-Aßtherapies that could have serious adverse effects, suchas Aß immunization; and
• monitor the efficacy of anti-Aß therapies.
References1. Jorm AF. Cross-national comparisons of the occurrence
of Alzheimer’s and vascular dementias. Eur ArchPsychiatry Clin Neurosci 1991; 240:218-22.
2. Canadian Study of Health and Aging: Study methodsand prevalence of dementia. CMAJ 1994;150(6):899-913.
3. McKhann G, Drachman D, Folstein M, et al. Clinicaldiagnosis of Alzheimer's disease: Report of theNINCDS-ADRDA Work Group under the auspices ofDepartment of Health and Human Services TaskForce on Alzheimer's Disease. Neurology 1984;34(7):939-44.
4. Stevens T, Livingston G, Kitchen G, et al. Islingtonstudy of dementia subtypes in the community. Br JPsychiatry 2002; 180:270-6.
5. Rogers SL, Friedhoff LT. Long-term efficacy andsafety of donepezil in the treatment of Alzheimer'sdisease: An interim analysis of the results of a USmulticentre open label extension study. Eur
Neuropsychopharmacol 1998; 8(1):67-75.6. Imbimbo BP, Verdelli G, Martelli P, et al. Two-year
treatment of Alzheimer's disease with eptastigmine.The Eptastigmine Study Group. Dement GeriatrCogn Disord 1999; 10(2):139-47.
7. Coyle J, Kershaw P. Galantamine, a cholinesteraseinhibitor that allosterically modulates nicotinicreceptors: Effects on the course of Alzheimer'sdisease. Biol Psychiatry 2001; 49(3):289-99.
8. Fago JP. Dementia: Causes, evaluation, andmanagement. Hosp Pract 200; 36(1):59-69.
9. Geldmacher DS, Provenzano G, McRae T, et al.Donepezil is associated with delayed nursing homeplacement in patients with Alzheimer's disease. JAm Geriatr Soc 2003; 51(7):937-44.
10. Corey-Bloom J, Anand R, Veach J (the ENA 713B352 Study Group). A randomized trial evaluatingthe efficacy and safety of ENA 713 rivastigminetartrate, a new acetylcholinesterase inhibitor, inpatients with mild to moderately severe AD. Int J
Psychopharmacol 1998; 1:55-65. 11. Raskind MA, Peskind ER, Wessel T, et al.
Galantamine in AD: A 6-month randomized,placebo-controlled trial with a 6-month extension.The Galantamine USA-1 Study Group. Neurology2000; 54(12):2261-8.
12. Doody RS, Geldmacher DS, Gordon B, et al.Donepezil Study Group. Open-label, multicenter,phase 3 extension study of the safety and efficacyof donepezil in patients with Alzheimer disease. ArchNeurol 2001; 58(3):427-33.
13. Silverman DHS. Brain 18F-FDG PET in the diagnosisof neurodegenerative dementias: Comparison withperfusion SPECT and with clinical evaluationslacking nuclear imaging. J Nucl Med 2004;45(4):594-607.
14. Mosconi L. Brain glucose metabolism in the earlyand specific diagnosis of Alzheimer's disease. FDG-PET studies in MCI and AD. Eur J Nucl Med MolImaging 2005; 32(4):486-510.
10 • The Canadian Review of Alzheimer’s Disease and Other Dementias
Acknowledgements:This review article was supported by a New Investigator Research Grant from the Alzheimer’s Association; a Young Investigator Grant fromthe Alzheimer Society of Canada, the Institute of Aging (Canadian Institutes of Health Research) and the Alzheimer Society of Saskatchewan;a Major Research Grant from the Scottish Rite Charitable Foundation of Canada; and by a Dean’s Fund New Staff Grant from the Universityof Toronto.

The Canadian Review of Alzheimer’s Disease and Other Dementias • 11
15. Dougall NJ, Bruggink S, Ebmeier KP. Systematicreview of the diagnostic accuracy of 99mTc-HMPAO-SPECT in dementia. Am J Geriatr Psychiatry2004; 12(6):554-70.
16. Arnold SE, Hyman BT, Flory J, et al. Thetopographical and neuroanatomical distribution ofneurofibrillary tangles and neuritic plaques in thecerebral cortex of patients with Alzheimer's disease.Cereb Cortex 1991; 1:103-16.
17. Braak H, Braak E. Frequency of stages of Alzheimer-related lesions in different age categories.Neurobiology of Aging 1997; 18:351-7.
18. Hardy J, Selkoe DJ. The amyloid hypothesis ofAlzheimer's disease: progress and problems on theroad to therapeutics. Science; 297(5580):353-6.
19. Thal DR, Rub U, Orantes M, et al. Phases of A beta-deposition in the human brain and its relevance forthe development of AD. Neurology 2002;58(12):1791-1800.
20. Braak H, Braak E: Neuropathological stageing ofAlzheimer-related changes. Acta Neuropathol (Berl)1991; 82:239-59.
21. Delacourte A, David JP, Sergeant N, et al. Thebiochemical pathway of neurofibrillary degenerationin aging and Alzheimer's disease. Neurology 1999;52(6):1158-65.
22. Iqbal K, Alonso Adel C, Chen S, et al. Tau pathologyin Alzheimer disease and other tauopathies. BiochimBiophys Acta 2005; 1739(2-3):198-210.
23. Terry RD, Masliah E, Salmon DP, et al. Physicalbasis of cognitive alterations in Alzheimer's disease:synapse loss is the major correlate of cognitiveimpairment. Ann Neurol 199; 30(4):572-80.
24. Masliah E, Mallory M, Alford M, et al. Alteredexpression of synaptic proteins occurs early duringprogression of Alzheimer's disease. Neurology2001; 56(1):127-9.
25. Hardy J. Amyloid, the presenilins and Alzheimer’sdisease. Trends Neurosci 1997; 20:154-9.
26. Knudsen KA, Rosand J, Karluk D, et al. Clinicaldiagnosis of cerebral amyloid angiopathy: Validationof the Boston criteria. Neurology 2001; 56(4):537-9.
27. Huang TH, Yang DS, Fraser PE, et al. Alternateaggregation pathways of the Alzheimer beta-amyloidpeptide. An in vitro model of preamyloid. J BiolChem 2000; 275(46):36436-40.
28. Petersen RC, Parisi JE, Dickson DW, et al.Neuropathologic features of amnestic mild cognitiveimpairment. Arch Neurol 2006; 63(5):665-72.
29. Hartley DM, Walsh DM, Ye CP, et al. Protofibrillarintermediates of amyloid beta-protein induce acuteelectrophysiological changes and progressiveneurotoxicity in cortical neurons. J Neurosci 1999;19(20):8876-84.
30. Kandimalla KK, Wengenack TM, Curran GL, et al.Pharmacokinetics and amyloid plaque targetingability of a novel Peptide-based magnetic resonancecontrast agent in wild-type and Alzheimer's diseasetransgenic mice. J Pharmacol Exp Ther 2007;322(2):541-9.
31. Sigurdsson EM, Wadghiri YZ, Mosconi L, et al. Anon-toxic ligand for voxel-based MRI analysis ofplaques in AD transgenic mice. Neurobiol Aging2007; [Epub ahead of print].
32. Nakada T, Matsozawa H, Igarashi H, et al. Directvisualization of senile plaques of patients in vivo bymagnetic resonance microscopy on a 7T clinicalsystem. Presentation at the April 28-May 5, 2007,Annual Meeting of the American Academy ofNeurology, Boston, MA, USA. Neurology 2007; 68(Supp. 1):A98.
33. Verhoeff NPLG. Ligands for neuroreceptor imagingby positron or single-photon emission tomography. In: Ell PJ, Gambhir SS (eds). Nuclear Medicine inClinical Diagnosis and Treatment. 3rd Edition.
Churchill Livingstone, New York, 2004.pp. 1275-94.
34. Shoghi-Jadid K, Small GW, Agdeppa ED, et al.Localization of neurofibrillary tangles and beta-amyloid plaques in the brains of living patients withAlzheimer disease. Am J Geriatr Psychiatry 2002;10(1):24-35.
35. Small GW, Kepe V, Ercoli LM, et al. PET of brainamyloid and tau in mild cognitive impairment. NEngl J Med 2006; 355(25):2652-63.
36. Small GW, Agdeppa ED, Kepe V, Satyamurthy N,Huang SC, Barrio JR. In vivo brain imaging of tangleburden in humans. J Mol Neurosci. 2002Dec;19(3):323-327.
37. Small GW, Kepe V, Huang SC, Wu HM, Siddarth P,Ercoli L, Miler K, Lavretsky H, Wrught BC, Shoghi-Jadid K, Satyamurthy N, Phelps ME, Barrio JR. Invivo brain imaging of tau aggregation in frontaltemporal dementia using [F-18]FDDNP positronemission tomography. (Abstract) 9th InternationalConference on Alzheimer’s Disease and RelatedDisorders, 2004. Neurobiology of Aging 2004; 25(Supp. S2): S288-S289.
38. Boxer AL, Rabinovici GD, Kepe V, Goldman J, FurstAJ, Huang SC, Baker SL, O'neil JP, Chui H,Geschwind MD, Small GW, Barrio JR, Jagust W,Miller BL. Amyloid imaging in distinguishing atypicalprion disease from Alzheimer disease. Neurology.2007 Jul 17;69(3):283-290.
39. Kepe V, Ghetti B, Bresjanac M, Huang SC, Smid L,Farlow M, Satyamurthy N, Epperson F, Phelps M,Small G, Barrio J. [F-18]FDDNP PET imaging ofprion pathology in Gerstmann-Sträusller-Scheinkerdisease. J Nucl med 2007; 48 (Supp. 2): 172P.
40. Agdeppa ED, Kepe V, Petri A, Satyamurthy N, Liu J,Huang SC, Small GW, Cole GM, Barrio JR. In vitrodetection of (S)-naproxen and ibuprofen binding toplaques in the Alzheimer's brain using the positronemission tomography molecular imaging probe 2-(1-[6-[(2-[18F]fluoroethyl)(methyl) amino]-2-naphthyl]ethylidene) malononitrile. Neuroscience2003; 117(3):723-30.
41. Shoghi-Jadid K, Barrio JR, Kepe V, et al. Imagingbeta-amyloid fibrils in Alzheimer's disease: A criticalanalysis through simulation of amyloid fibrilpolymerization. Nucl Med Biol 2005; 32(4):337-51.
42. Klunk WE, Engler H, Nordberg A, et al. Imaging brainamyloid in Alzheimer's disease with PittsburghCompound-B. Ann Neurol 2004; 55(3):306-19.
43. DeKosky ST, Mathis CA, Price JC, et al. Correlationof in vivo PIB retention and postmortem A levels: Acase study. Presented at the 59th Annual Meetingof the American Academy of Neurology in Boston,MA, May 4, 2007.
44. Engler H, Forsberg A, Almkvist O, et al. Two-yearfollow-up of amyloid deposition in patients withAlzheimer's disease. Brain 2006; 129(Pt 11):2856-66.
45. Edison P, Archer HA, Hinz R, et al. Amyloid,hypometabolism, and cognition in Alzheimerdisease: An [11C]PIB and [18F]FDG PET study.Neurology 2007; 68(7):501-8.
46. Mark RJ, Pang Z, Geddes JW, et al. Amyloid beta-peptide impairs glucose transport in hippocampaland cortical neurons: involvement of membrane lipidperoxidation. J Neurosci 1997; 17(3):1046-54.
47. Copani A, Koh JY, Cotman CW. Beta-amyloidincreases neuronal susceptibility to injury by glucosedeprivation. Neuroreport 1991; 2(12):763-5.
48. DeCarli CS, Atack JR, Ball MJ et al. Post-mortemregional neurofibrillary tangle densities but notsenile plaque densities are related to regionalmetabolic rates for glucose during life in ADpatients. Neurodegeneration 1992; 1:113-21.
49. Lopresti BJ, Klunk WE, Mathis CA, et al. Simplifiedquantification of Pittsburgh Compound B amyloid
imaging PET studies: a comparative analysis. J NuclMed 2005; 46(12):1959-72.
50. Price JC, Klunk WE, Lopresti BJ, et al. Kineticmodeling of amyloid binding in humans using PETimaging and Pittsburgh Compound-B. J Cereb BloodFlow Metab 2005; 25(11):1528-47.
51. Zhou Y, Ye W, Brasic J, Alexander M, Resnick SM,Wong DF. Evaluation of data acquisition time on thequantification of [11C]PIB PET. Presented at the59th Annual Meeting of the American Academy ofNeurology in Boston, MA, May 4, 2007.
52. Kemppainen NM, Aalto S, Wilson IA, et al. Voxel-based analysis of PET amyloid ligand [11C]PIBuptake in Alzheimer disease. Neurology 2006;67(9):1575-80.
53. Ziolko SK, Weissfeld LA, Klunk WE, et al. Evaluationof voxel-based methods for the statistical analysis ofPIB PET amyloid imaging studies in Alzheimer'sdisease. Neuroimage 2006; 33(1):94-102.ƒ
54. Tolboom N, Yaqub M, Van der Flier W, et al. Imagingbeta-amyloid deposition in vivo: quantitativecomparison between [18F]FDDNP and [11C]PIB.Presented at the 59th Annual Meeting of theAmerican Academy of Neurology in Boston, MA,May 4, 2007.
55. Kudo Y, Okamura N, Furumoto S, et al. 2-(2-[2-Dimethylaminothiazol-5-yl] ethenyl)-6-(2-[fluoro]ethoxy) benzoxazole: A novel PET agent for invivo detection of dense amyloid plaques inAlzheimer's disease patients. J Nucl Med 2007;48(4):553-61.
56. Newberg A, Wintering N, Clark C, et al. Use of 123IIMPY SPECT to differentiate Alzheimer’s diseasefrom controls. J Nucl Med 2006; 47(Supp. 1):78P.
57. Marek K, Jennings D, Koren A, et al.[I-123]IMPY imaging to assess -amyloid burden inAlzheimer’s disease. Presented at the 59th AnnualMeeting of the American Academy of Neurology inBoston, MA, May 4, 2007.
58. Song P, Serge B, Sarradin P, et al. IMPY, a beta-amyloid imaging probe for prion detection. J Nuclmed 2006; 47(Supp. 1):134P.
59. Mathis C, Lopresti B, Mason N,et al. Comparison ofthe amyloid imaging agents [F-18]3’-F-PIB and [C-11]PIB in Alzheimer’s disease and control subjects.J Nucl Med 2007; 48 (Supp. 2):56P.
60. Rowe CC, Ng S, Mulligan R, et al. First results fromhuman studies of a novel F-18 PET ligand for brain-amyloid imaging. J Nucl Med 2007a;48 (Supp.2):57P.
61. Aisen PS. The development of anti-amyloid therapyfor Alzheimer's disease: From secretase modulatorsto polymerisation inhibitors. CNS Drugs 2005;19(12):989-996.
62. Klafki HW, Staufenbiel M, Kornhuber J, et al.Therapeutic approaches to Alzheimer's disease.Brain 2006; 129(Pt 11):2840-55.
63. Masters CL, Beyreuther K. Alzheimer's centenniallegacy: Prospects for rational therapeuticintervention targeting the Abeta amyloid pathway.Brain 2006; 129(Pt 11):2823-39.
64. Vardy ER, Hussain I, Hooper NM. Emergingtherapeutics for Alzheimer’s disease. Expert RevNeurother 2006; 6(5):695-704.
65. Verhoeff NPLG. Acetylcholinergic neurotransmissionand th beta-amyloid cascade: Implications forAlzheimer’s disease. Expert Rev Neurotherapeutics2005; 5(2):277-84.
66. Ghosh AK, Bilcer G, Hong L, et al. Memapsin 2(Beta-Secretase) Inhibitor Drug, between Fantasyand Reality. Curr Alzheimer Res 2007; 4(4):418-22.
67. Siemers ER, Quinn JF, Kaye J, et al. Effects of agamma-secretase inhibitor in a randomized study ofpatients with Alzheimer disease. Neurology 2006;28;66(4):602-4.

12 • The Canadian Review of Alzheimer’s Disease and Other Dementias
68. Checler F, Alves da Costa C, Ayral E, et al. JLKinhibitors: Isocoumarin compounds as putativeprobes to selectively target the gamma-secretasepathway. Curr Alzheimer Res 2005; 2(3):327-34.
69. Fraering PC, Ye W, LaVoie MJ, et al. Gamma-Secretase substrate selectivity can be modulateddirectly via interaction with a nucleotide-binding site.J Biol Chem 2005; 280(51):41987-96.
70. Evin G, Sernee MF, Masters CL Inhibition of gamma-secretase as a therapeutic intervention forAlzheimer's disease: Prospects, limitations andstrategies. CNS Drugs 2006; 20(5):351-72.
71. Eriksen JL, Sagi SA, Smith TE, et al. NSAIDs andenantiomers of flurbiprofen target gamma-secretaseand lower Abeta 42 in vivo. J Clin Invest 2003;112(3):440-9.
72. Lleo A, Berezovska O, Herl L, et al. Nonsteroidalanti-inflammatory drugs lower Abeta-42 and changepresenilin 1 conformation. Nat Med 2004;10(10):1065-6.
73. Mohs RC, Rosen WG, Davis KL. The Alzheimer'sdisease assessment scale: an instrument forassessing treatment efficacy. Psychopharmacol Bull1983; 19(3):448-550.
74. Geerts H. NC-531 (Neurochem). Curr Opin InvestigDrugs 2004; 5(1):95-100.
75. McLaurin J, Kierstead ME, Hawkes CA, et al.Cyclohexanehexol inhibitors of Abeta aggregationprevent and reverse Alzheimer phenotype in amouse model. Nat Med 2006; 12(7):801-8.
76. Janus C, Pearson J, McLaurin J,et al.A beta peptide immunization reduces behaviouralimpairment and plaques in a model of Alzheimer'sdisease. Nature 2000; 408(6815):979-82.
77. Morgan D, Diamond DM, Gottschall PE, et al. A betapeptide vaccination prevents memory loss in ananimal model of Alzheimer's disease. Nature 2000;408(6815):982-5.
78. Hock C, Konietzko U, Streffer JR, et al. Antibodiesagainst beta-amyloid slow cognitive decline inAlzheimer's disease. Neuron 2003; 38(4):547-54.
79. Schenk D, Barbour R, Dunn W, et al. Immunizationwith amyloid-beta attenuates Alzheimer-disease-likepathology in the PDAPP mouse. Nature 1999;400(6740):173-7.
80. Nicoll JA, Wilkinson D, Holmes C, et al.Neuropathology of human Alzheimer disease afterimmunization with amyloid-beta peptide: A casereport. Nat Med 2003; 9(4):448-52.
81. Pfeifer M, Boncristiano S, Bondolfi L, et al. Cerebralhemorrhage after passive anti-Abetaimmunotherapy. Science 2002; 298(5597):1379.
82. Orgogozo JM, Gilman S, Dartigues JF, et al.Subacute meningoencephalitis in a subset ofpatients with AD after Abeta42 immunization.Neurology 2003; 61(1):46-54.
83. Fox NC, Black RS, Gilman S, et al. AN1792(QS-21)-201 Study. Effects of Abeta immunization (AN1792)on MRI measures of cerebral volume in Alzheimerdisease. Neurology 2005; 64(9):1563-72.
84. DeMattos RB, Bales KR, Cummins DJ, et al. Brain toplasma amyloid-beta efflux: A measure of brainamyloid burden in a mouse model of Alzheimer'sdisease. Science 2002; 295(5563):2264-7.
85. Dodart JC, Bales KR, Gannon KS, et al.Immunization reverses memory deficits withoutreducing brain Abeta burden in Alzheimer's diseasemodel. Nat Neurosci 2002; 5(5):452-7.
86. Wilcock DM, Rojiani A, Rosenthal A, et al. Passiveamyloid immunotherapy clears amyloid andtransiently activates microglia in a transgenic mousemodel of amyloid deposition. J Neurosci 2004 Jul 7;24(27):6144-51.
87. Morris JC, Storandt M, McKeel DW Jr, et al.Cerebral amyloid deposition and diffuse plaques in
"normal" aging: Evidence for presymptomatic andvery mild Alzheimer's disease. Neurology 1996;46(3):707-19.
88. Hulette CM, Welsh-Bohmer KA, Murray MG, et al.Neuropathological and neuropsychological changesin "normal" aging: Evidence for preclinical Alzheimerdisease in cognitively normal individuals. JNeuropathol Exp Neurol 1998; 57(12):1168-74.
89. Petersen RC. Mild cognitive impairment as adiagnostic entity. J Intern Med 2004; 256(3):183-94.
90. Nordberg A, Forsberg A, Engler H, et al. Imaging ofamyloid pathology in prodromal Alzheimer’s disease.Presented at the 59th Annual Meeting of theAmerican Academy of Neurology in Boston, MA,May 4, 2007.
91. Mintun MA, Larossa GN, Sheline YI, et al. [11C]PIBin a nondemented population: Potential antecedentmarker of Alzheimer disease. Neurology 2006;67(3):446-52.
92. Aizenstein H, Nebes RD, Saxton JA, et al. Amyloidimaging with Pittsburgh Compound-B in non-demented elderly. Presented at the 59th AnnualMeeting of the American Academy of Neurology inBoston, MA, May 4, 2007.
93. Devanand DP, Parsey R, Pelton GH, et al. PETamyloid imaging with [11C]6-)H-BTA-1 (PIB) inAlzheimer’s disease, mild cognitive impairment, andhealthy controls. Presented at the 59th AnnualMeeting of the American Academy of Neurology inBoston, MA, May 4, 2007.
94. Rentz DM, Eng E, Moran EK, Becker JA, DeKoskyST, Klunk WE, Mathis CA, Sperling RA, Fischman AJ,Johnson KA. Mild memory impairments in normalsublects with high cognitive reserve are associatedwith amyloid deposition. Human Amyloid ImagingAbstract Book.
95. Rowe CC, Ng S, Ackermann U, et al. Imaging beta-amyloid burden in aging and dementia. Neurology2007b; 68(20):1718-25.
96. Arai H, Okamura N, Tashiro M, et al. In vivodetection of amyloid deposits in normals, mildcognitive impairment and Alzheimer’s diseasepatients using [11C]BF-227 and PET. Presented atthe 59th Annual Meeting of the American Academyof Neurology in Boston, MA, May 4, 2007.
97. Resnick SM, Zhou Y, An Y, et al. Longitudinalcognitive change is associated with amyloiddeposition measured by 11-C-PIB. Presented at the59th Annual Meeting of the American Academy ofNeurology in Boston, MA, May 4, 2007.
98. Sperling R, Laviolette P, White E, et al. Parietalamyloid deposition associated with impairedmemory-related functional activity. Presented at the59th Annual Meeting of the American Academy ofNeurology in Boston, MA, May 4, 2007.
99. Villemagne V, Pike K, Maruff P, et al. Amyloid burdenin ageing subjects with and without cognitivedecline. J Nucl Med 2007; 48(Supp. 2):57P.
100. Klunk WE, Price JC, Mathis CA, et al. Amyloiddeposition begins in the striatum of presenilin-1mutation carriers from two unrelated pedigrees. JNeurosci 2007; 27(23):6174-84.
101. Fagan AM, Mintun MA, Mach RH, et al. Inverserelation between in vivo amyloid imaging load andcerebrospinal fluid Abeta42 in humans. AnnNeurol 2006;5 9(3):512-9.
102. Johnson KA, Gregas M, Becker JA, et al. Imaging ofamyloid burden and distribution in cerebral amyloidangiopathy. Ann Neurol 2007; 62(3):229-34.
103. Klunk WE, Mathis CA, Price JC, et al. Two-yearfollow-up of amyloid deposition in patients withAlzheimer's disease. Brain 2006; 129(Pt11):2805-07.
104. Bauer M, Langer O, Dal-Bianco P, et al. A positron
emission tomography microdosing study with apotential antiamyloid drug in healthy volunteersand patients with Alzheimer's disease. ClinPharmacol Ther 2006; 80(3):216-27.
105. Cai L, Liow JS, Morse C, et al. [18F]FMS-IMPYand [18F]FES-IMPY as potential radioligands forimaging brain beta-amyloid. J Nucl Med 2007;48(Suppement 2):130P.
106. Wang C, Easwaramoorthy B, Pichika R, et al. 18F-FBM: A new PET radiotracer for imaging beta-amyloid plaques and neurofibrillary tangles. J NuclMed 2006; 47(Supp. 1):217P.
107. Serdons K, Terwinghe C, Vermaelen P, K et al. 6-Methoxy-2-(4’-[18F]fluorophenyl)-1, 3-benzothiazole and 6-methyl-2-(4’-[18F]fluorophenyl)-1,3-benzothiazole as potentialamyloidimaging agents. J Nucl Med 2006;47(Supp. 1):31P.
108. Chandra R, Stephenson K, Kung MP, Hou C, et al.2-Arylbenzothiazole derivatives for beta-amyloidplaque imaging. J Nucl med 2006; 47(Supp.1):217P.
109. Zhang W, Kung MP, Oya S,et al. F-18 labeled PEGstilbene derivatives as PET imaging agents forAlzheimer’s disease. J Nucl Med 2006; 47(Supp.1):218P.
110. Chandra R, Oya S, Kung MP, et al. 18F-Pegylatedalkynes as potential PET imaging agents forAlzheimer’s disease. J Nucl Med 2007; 48(Supp.2):301P.
111. Shoup T, Elmaleh D, Jin Y, et al.[N-2[18F]Fluoropropyl]2-4’(methylamino)phenyl)-6-hydroxybenzothiazole for potential A amyloidimaging. J Nucl Med 2007; 48(Supp. 2):299P.
112. Lee YS, Jeong J, Chang Y, et al. Syntheses andevaluation of 2-(4’-[18F] fluoromethylphenyl)benzothazole and benzoxazole derivatives as PETagents for -amyloid (A ) plaque imaging.J Nucl Med 2007; 48(Supp. 2):301P
113. Patel P, Collins D, Nistor M, et al. 18F-Fluoropropylcurcumin: A potential PET tracer for imaginginflammation and A -plaques. J Nucl Med 2007;48(Supp. 2):22P.
114. Shih-Ying L, Cheng-Xiang Y, Kang-Wei C, et al.Syntheses of 123I-IOBOX for binding beta-amyloidplaques in the Tg2576 transgenic mice. J NuclMed 2006; 47(Supp. 1):547P
115. Kulkarni P, Roney C, Arora V, et al. Imaging ADplaques in transgenic and animal model of ADwith radioiodinated clioquinol. J Nucl Med 2006;47(Supp. 1):218P.
116. Ono M, Maya Y, Haratake M, Nakayama M.Syntesis and characterization of styrylchomonederivatives as amyloid imaging agents. J Nucl Med2006; 47(Supp. 1):498P.
117. Ono M, Haratake M, Nakayama M. Novelchalcones as probes for in vivo detecting of -amyloid plaques in Alzheimer’s disease. J NuclMed 2007; 48(Supp. 2):300P.
118. Qu W, Kung MP, Hou C, et al. Novel iodinatedstyrylpyridines for SPECT imaging of -amyloidplaques. J Nucl Med 2007a; 48(Supp. 2):303P.
119. Qu W, Kung MP, Hou C, et al. Bisphenyltriazoles aspotential imaging agents for Alzheimer’s disease. JNucl Med 2007b; 48(Supp. 2):129P.
120. Qy W, Kung MP, Hou C, Kung H. Radioiodinatedalkynes as potential SPECT imaging agents forAlzheimer’s disease. J Nucl Med 2007c; 48(Supp.2):302P.
121. Verhoeff NPLG, Wilson AA, Takeshita S, Trop L,Hussey D, Singh K, Kung HF, Kung MP, Houle S. Invivo imaging of Alzheimer disease β-amyloid with[11C]SB-13 PET. Am J Geriatr Psychiatry 2004;12: 584-95.

The Canadian Review of Alzheimer’s Disease and Other Dementias • 13
Imaging and Alzheimer’s Disease: A ReviewNeuroimaging in Alzheimer’s disease (AD) has moved beyond the stage where it was usedpurely to exclude other disease processes. Structural brain magnetic resonance imaging (MRI)is useful to assess hippocampal atrophy on coronal slices; clinicians can use a simple visualrating scale, which can help to confirm the diagnosis of AD. Another useful indication forneuroimaging is to assess the contribution of cerebrovascular disease (CBVD) to the clinicalsyndrome of dementia. It has become clear in recent years that the most common situation inthe general population is the combination of AD and CBVD. A neuroimaging procedure (CT scan or, preferably, MRI) can detect silent CBVD, which would modify management ofmodifiable risk factors. The recent Canadian Consensus on Dementia recognized this indication.
Christian Bocti, MD, FRCPC
Neuroimaging has traditionnal-ly been recommended as a
way to exclude potentiallyreversible causes of dementia, eventhough the prevalence of treatablecauses of dementia in typical refer-ral clinics is very low.1 This tradi-tional view was largely held untilthe previous Canadian Consensusin 1999,2 where specific guidelineswere stated to restrict the indica-tions of neuroimaging in dementia.However, there has been muchdevelopment since those guidelineswere published. The most recentPractice Parameter from theAmerican Academy of Neurology
recommends that at least one neu-roimaging procedure should bedone in every patient with adementing disorder.3 This articlereviews structural and functionalimaging in the diagnosis ofAlzheimer’s disease (AD). Futuredevelopments of imaging hold greatpromise and are briefly overviewed.
BackgroundThe process that leads to ADprobably begins decades beforewe can detect it clinically.4 At onepoint, the functional connectivityand molecular changes that occurwithin cells result in neuronal lossand brain atrophy. This atrophyfollows a specific, systematicanatomical pattern for reasonsthat are still a matter of debate.One hypothesis holds that the ADprocess follows brain regions in
decreasing order of “neuroplastic-ity potential.”5 This view statesthat the hippocampus and its con-nections in the entorhinal cortex(the part of the medial temporallobe just adjacent to the hip-pocampus) remain the most activein terms of plasticity throughoutthe lifespan. Indeed, the formingof new memories occurs duringadult life, and is supported bystructural changes in the hip-pocampal-entorhinal complex:these structural changes are termedneuroplasticity.6 Neuroplasticityfailure would affect the medialtemporal lobe first, then its con-nections within the limbic andpara-limbic regions, then the mul-timodal associative cortex. It is thistopographical selectivity thatallows early detection of atrophy inthe medial temporal regions.7
Christian Bocti, MD, FRCPCDivision of Neurology,Maisonneuve-Rosemont Hospital,Clinical Associate Professor,University of Montreal, Montreal,Quebec.

14 • The Canadian Review of Alzheimer’s Disease and Other Dementias
Structural Neuroimaging:Brain AtrophySeveral studies using CT and MRIscans have shown significantly
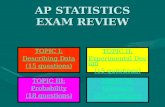
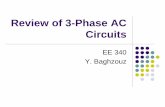
smaller hippocampi in subjectswith AD compared with normalcontrols, with accuracy of classifi-cation in the 85% range.1 There isa whole spectrum of tools withvarying degrees of technologicalintensity, ranging from the sim-plest visual rating scale8 to themost sophisticated 3D shape-deformation analysis of the hip-pocampus, which require advancedhardware, software and statisticalknowledge.9 Visual rating scales(Figure 1) can be performed by cli-nicians quickly (one to two min-utes), with minimal training, andhave been validated against volu-metric measures.10-12
For reasons of ease-of-use andavailability, this simple type ofimaging analysis is probably theone with the most potential use-fulness in clinical practice fornow. Recent developments havebrought automated measures clos-er to clinical practice, but even“simple” techniques require regis-tration to standardized 3D tem-plates, which is not likely to bewidely available.13,14
It should be kept in mind thathippocampal atrophy alone maynot be sufficient to diagnose ADin cohorts comparing differentdiagnostic groups: the addition ofa Mini Mental State Examination(MMSE) score to a visual ratingof medial-temporal-lobe atrophywas found to be necessary to dis-criminate between AD and non-AD in one study,11 and other tem-poral-lobe structures were assessedin another.15 There are several
reports where medial-temporal-lobe atrophy is found in non-ADdementias, such as fronto-temporaldementia.16-18 Nevertheless, agroup of experts recently recom-mended that research criteria forAD be revised, and that assessmentof medial-temporal atrophy shouldbe a part of the new criteria, whichalso include cognitive informationand other biomarkers.19
In conclusion, although medi-al-temporal atrophy does con-tribute to diagnostic specificity inexpert hands, it has yet to betranslated into widespread clini-cal and radiological practice.According to a recent stringentevidence-based review, there isinsufficient data on MRI in gener-al-practice settings to recommendits widespread use.20
Structural Neuroimaging:Cerebrovascular DiseaseIn recent years, CBVD has beenreconceptualized as a major factorin cognitive decline and dementia,including AD. Ischemic lesionssuch as lacunar infarcts greatlyinfluence the clinical syndrome ofdementia;21,22 this could be anadditive or a synergistic effect. Itappears that the most commonpathological substrate of dementiain population-based autopsyseries is combined CBVD and ADpathology; mixed dementia couldbe more frequent in the generalpopulation than “pure” AD.23,24 Itis also well known from large-scale, population-based imagingstudies that the prevalence of
Figure 1
Medial-temporal-lobeAtrophy (MTA) Scale12
The rating from 0 to 4 is displayed;higher scores indicate moreatrophy. When one score is given,left = right.
MTA = 0
MTA = 4
MTA = 3
MTA = 2 (right) and 4 (left)
MTA = 1

The Canadian Review of Alzheimer’s Disease and Other Dementias • 15
“silent” brain infarcts is quitehigh in the general populationand has an impact on cognitivedecline.25,26 In light of these data,it is quite surprising to find thatuntil recently, there were no offi-cial recommendations to includeneuroimaging as a means todetect CBVD in dementia assess-ment. Although neuroimagingevidence of what constitutes “sig-nificant” CBVD in dementia is stillnot agreed on, there is a generalagreement on the fact that detection
of silent CBVD should lead to amore pro-active management ofmodifiable vascular risk factors.27
These considerations have result-ed in a statement from the 3rdCanadian Consensus Conferenceon Diagnosis and Treatment ofDementia (CCCDTD):28 “There isfair evidence to support use ofstructural neuroimaging to rule inconcomitant CBVD that canaffect patient management.”
Ever since neuroimaging wasintegrated in clinical routine,29
there has been much controversyabout the white-matter changes (orleukoaraiosis) that appear ubiqui-tous in aging.30 Recent years ofresearch have finally crystallizedknowledge on this phenomenon,and there is an emerging consen-sus that confluent lesions (asopposed to punctate lesions) doprogress with time,31 and are asso-ciated with certain cognitivedeficits as well as motor and func-tional disability.32-34 Moderate-to-severe leukoaraiosis is thus farfrom benign, and can easily beassessed with simple rating scales(Figure 235).36,37
Advanced StructuralNeuroimaging TechniquesUntil now we have dealt with tra-ditional neuroimaging techniquesthat are in common clinical use.Recent developments in MRItechnology have revealed thatstructural damage can be detectedin areas outside of visibly abnor-mal regions on the standardimages: several techniques are
available, but will not be reviewedin detail here. One of the mostpromising techniques is diffusiontensor imaging (DTI), whereintegrity of the white-matter tractscan be assessed by analyzing themovement of free water mole-cules within the tracts.38 Moredegraded tracts will result inincreasingly random movements,which can be detected by DTI;such abnormalities can be corre-lated with cognitive functions.39
Studies have now shown that ADis associated with degradation ofwhite-matter tracts.40 It is still atechnical challenge to obtain suchdata and thus routine availabilityof DTI will not happen in theforeseeable future.
Functional NeuroimagingNuclear medicine has been usedin the study of dementia for manyyears, with single photon emis-sion computed tomography(SPECT) and positron emissiontomography (PET) scans tested asdiagnostic tools in AD and otherdementias. There are reports onPET imaging that show it is moresensitive and specific comparedwith clinical assessment in theearly diagnosis of dementia. Thevalue of PET in the differentialdiagnosis of frontotemporaldementia versus AD has recentlybeen demonstrated in a welldesigned study that looked atadded benefit over clinical infor-mation alone, notably with a sim-ple visual rating by the (experi-enced) clinician.41 SPECT is more
Figure 2
Assessment of LeukoaraiosisUsing Rating Scales35
A through F are examples of therating scores 1, 2, and 3 from CT andMRI scans. Each pair of images(CT/MRI) refers to the same patient.The lesions are chosen from matchingslices. Note that the slice angulationdiffers between CT and MRI (T2-weighted MRI images are shown). For a rating score of 1, a single lesionis clearly seen on CT (A) (see arrow);on MRI (B), and additional lesions arerated as 2; rating score 2 isexemplified in C and D (see arrows);rating score 3 is shown in E and F.

16 • The Canadian Review of Alzheimer’s Disease and Other Dementias
widely available, but is generallyless sensitive and specific thanPET.42,43 Nevertheless, it has somevalue in the diagnosis of AD44 anddifferential diagnosis of dementias,including frontal and anterior tem-poral hypoperfusion in fronto-tem-poral dementias, and occipitalhypoperfusion in dementia withLewy bodies45,46
Advanced Functional Neuroimaging TechniquesDirect imaging of neuropathologicalhallmarks of AD is becoming possi-ble with the development of specifictracers in PET imaging.47 This hassome potential to help in the earlydiagnosis of AD, but unfortunatelycorrelations between amyloid onneuropathology and cognition havebeen far from compelling.48 Also,there is a substantial proportion ofelderly without cognitive impair-ment who also have high amyloidburden on pathology. The specifici-
ty of an amyloid imaging techniqueremains to be proven in light ofthese known pathological correlates.Future development in tau imagingmight contribute more substantiallyto this field since tau and neurofib-rillary tangles are more robustlyassociated with cognition in AD49
ConclusionIn summary, the diagnosis ofdementia will likely remain clinicalfor most purposes in the next fewyears. However, there are potentialbenefits and diagnostic utility ofsome widely available imagingtechniques. In particular, systematicrating of medial-temporal atrophyon MRI has the potential of increas-ing diagnostic certainty for AD inspecialty clinics. Similarly, identifi-cation of lacunes and application ofa simple rating of leukoaraiosis onCT scans of the brain can provideprognostic information and altermanagement of patients.
The real challenge facing clini-cians will be increasing pressure todiagnose AD earlier and with moreaccuracy and diagnostic confi-dence. This pressure will becomemuch more important when effi-cient disease-modifying therapiesare available. Neuroimaging per-haps will have to be used in thatearly period of the disease, where itis likely to be more useful. Newresearch criteria have been pro-posed for that purpose, and right-fully include medial-temporal-lobeatrophy as a neuroimaging bio-marker.17 These criteria will cer-tainly give an impetus to the sys-tematic rating of medial-temporal-lobe atrophy by radiologists andclinicians in the next few years. Alarge-scale, open-access database iscurrently being developed in theU.S. and Canada and will likely bevery useful to further delineate thediagnostic value of neuroimagingin AD.50
References1. Scheltens P, Fox N, Barkhof F, De Carli
C. Structural magnetic resonanceimaging in the practical assessment ofdementia: beyond exclusion. LancetNeurol 2002; 1:13-21.
2. Patterson C, Gauthier S, Bergman H, etal. The recognition, assessment andmanagement of dementing disorders:conclusions from the CanadianConsensus Conference on Dementia.Can J Neurol Sci 2001; 28 Suppl 1:S3-S16.
3. Knopman DS, DeKosky ST, CummingsJL, et al. Practice parameter: diagnosisof dementia (an evidence-basedreview). Report of the QualityStandards Subcommittee of the
American Academy of Neurology.Neurology 2001; 56:1143-53.
4. Braak H, Braak E. Frequency of stagesof Alzheimer-related lesions in differentage categories. Neurobiol Aging 1997;18:351-57.
5. Mesulam MM. Neuroplasticity failurein Alzheimer's disease: bridging thegap between plaques and tangles.Neuron 1999; 24:521-29.
6. Squire LR, Stark CE, Clark RE. Themedial temporal lobe. Annu RevNeurosci 2004; 27:279-306.
7. Jack CR, Jr., Dickson DW, Parisi JE, etal. Antemortem MRI findings correlatewith hippocampal neuropathology intypical aging and dementia. Neurology2002; 58:750-57.
8. Scheltens P, Leys D, Barkhof F, et al.Atrophy of medial temporal lobes onMRI in "probable" Alzheimer's diseaseand normal ageing: diagnostic valueand neuropsychological correlates. JNeurol Neurosurg Psychiatry 1992;55:967-72.
9. Scher AI, Xu Y, Korf ES, et al.Hippocampal shape analysis inAlzheimer's disease: a population-based study. Neuroimage 2007; 36:8-18.
10. Frisoni GB, Scheltens P, Galluzzi S, etal. Neuroimaging tools to rateregional atrophy, subcorticalcerebrovascular disease, and regionalcerebral blood flow and metabolism:Consensus paper of the EADC. J

The Canadian Review of Alzheimer’s Disease and Other Dementias • 17
Neurol Neurosurg Psychiatry 2003;74:1371-81.
11. Wahlund LO, Julin P, Johansson SE, etal. Visual rating and volumetry of themedial temporal lobe on magneticresonance imaging in dementia: acomparative study. J Neurol NeurosurgPsychiatry 2000; 69:630-5.
12. Korf ES, Wahlund LO, Visser PJ, et al.Medial temporal lobe atrophy on MRIpredicts dementia in patients with mildcognitive impairment. Neurology 2004;63:94-100.
13. Ridha BH, Barnes J, van de Pol LA, etal. Application of automated medialtemporal lobe atrophy scale toAlzheimer disease. Arch Neurol 2007;64:849-54.
14. Gao FQ, Black SE, Leibovitch FS, et al.Linear width of the medial temporallobe can discriminate Alzheimer'sdisease from normal aging: theSunnybrook dementia study. NeurobiolAging 2004; 25:441-48.
15. O'Brien JT, Desmond P, Ames D, et al.Temporal lobe magnetic resonanceimaging can differentiate Alzheimer'sdisease from normal ageing,depression, vascular dementia andother causes of cognitive impairment.Psychol Med 1997; 27:1267-75.
16. Galton CJ, Gomez-Anson B, Antoun N,et al. Temporal lobe rating scale:application to Alzheimer's disease andfrontotemporal dementia. J NeurolNeurosurg Psychiatry 2001; 70:165-73.
17. van de Pol LA, Hensel A, van der FlierWM, et al. Hippocampal atrophy onMRI in frontotemporal lobardegeneration and Alzheimer's disease.J Neurol Neurosurg Psychiatry 2006;77:439-42.
18. Bocti C, Rockel C, Roy P, et al.Topographical patterns of lobar atrophyin frontotemporal dementia andAlzheimer's disease. Dement GeriatrCogn Disord 2006; 21:364-72.
19. Dubois B, Feldman HH, Jacova C, etal. Research criteria for the diagnosisof Alzheimer's disease: revising theNINCDS-ADRDA criteria. LancetNeurol 2007; 6:734-46.
20. Wahlund LO, Almkvist O, Blennow K,et al. Evidence-based evaluation ofmagnetic resonance imaging as adiagnostic tool in dementia workup.Top Magn Reson Imaging 2005;16:427-37.
21. Snowdon DA, Greiner LH, MortimerJA, et al. Brain infarction and theclinical expression of Alzheimerdisease. The Nun Study. JAMA 1997;277:813-7.
22. Esiri MM, Nagy Z, Smith MZ, et al.Cerebrovascular disease and thresholdfor dementia in the early stages ofAlzheimer's disease. Lancet 1999;354:919-20.
23. Lim A, Tsuang D, Kukull W, et al.Clinico-neuropathological correlationof Alzheimer's disease in a community-
based case series. J Am Geriatr Soc1999; 47:564-9.
24. MRC-CFAS. Pathological correlates oflate-onset dementia in a multicentre,community-based population inEngland and Wales. NeuropathologyGroup of the Medical ResearchCouncil Cognitive Function and AgeingStudy (MRC CFAS). Lancet 2001;357:169-75.
25. Vermeer SE, Prins ND, den Heijer T, etal. Silent brain infarcts and the risk ofdementia and cognitive decline. NEngl J Med 2003; 348:1215-22.
26. Vermeer SE, Koudstaal PJ, Oudkerk M,et al. Prevalence and risk factors ofsilent brain infarcts in the population-based Rotterdam Scan Study. Stroke2002; 33:21-5.
27. Bocti C, Black S, Frank C. Managementof dementia with a cerebrovascularcomponent. Alzheimer's & Dementia2007; 3:398-403.
28. Chow T. Structural Neuroimaging inthe Diagnosis of Dementia.Background article for the ThirdCanadian Consensus Conference onDiagnosis and Treatment of Dementia.Alzheimer's & Dementia 2007; inpress.
29. Hachinski VC, Potter P, Merskey H.Leuko-araiosis. Arch Neurol 1987;44:21-3.
30. Fernando MS, Ince PG. Vascularpathologies and cognition in apopulation-based cohort of elderlypeople. J Neurol Sci 2004; 226:13-7.
31. Schmidt R, Scheltens P, Erkinjuntti T, etal. White matter lesion progression: asurrogate endpoint for trials in cerebralsmall-vessel disease. Neurology 2004;63:139-44.
32. Prins ND, van Dijk EJ, den Heijer T, etal. Cerebral small-vessel disease anddecline in information processingspeed, executive function and memory.Brain 2005; 128:2034-41.
33. Pantoni L, Poggesi A, Basile AM, et al.Leukoaraiosis predicts hidden globalfunctioning impairment in nondisabledolder people: the LADIS (Leukoaraiosisand Disability in the Elderly) Study. JAm Geriatr Soc 2006; 54:1095-1101.
34. Bocti C, Swartz RH, Gao FQ, et al. Anew visual rating scale to assessstrategic white matter hyperintensitieswithin cholinergic pathways indementia. Stroke 2005; 36:2126-31.
35. Wahlund LO, Barkhof F, Fazekas F, etal. A new rating scale for age-relatedwhite matter changes applicable toMRI and CT. Stroke 2001; 32:1318-22.
36. Inzitari D, Simoni M, Pracucci G, et al.Risk of rapid global functional declinein elderly patients with severe cerebralage-related white matter changes: theLADIS study. Arch Intern Med 2007;167:81-8.
37. Gouw AA, Van der Flier WM, vanStraaten EC, et al. Simple versuscomplex assessment of white matter
hyperintensities in relation to physicalperformance and cognition: the LADISstudy. J Neurol 2006; 253:1189-96.
38. Catani M. Diffusion tensor magneticresonance imaging tractography incognitive disorders. Curr Opin Neurol2006; 19:599-606.
39. O'Sullivan M, Morris RG, Huckstep B,et al. Diffusion tensor MRI correlateswith executive dysfunction in patientswith ischaemic leukoaraiosis. J NeurolNeurosurg Psychiatry 2004; 75:441-7.
40. Stahl R, Dietrich O, Teipel SJ, et al.White matter damage in Alzheimerdisease and mild cognitive impairment:assessment with diffusion-tensor MRimaging and parallel imagingtechniques. Radiology 2007; 243:483-92.
41. Foster NL, Heidebrink JL, Clark CM, etal. FDG-PET improves accuracy indistinguishing frontotemporal dementiaand Alzheimer's disease. Brain 2007;130:2616-35.
42. Silverman DH, Alavi A. PET imaging inthe assessment of normal and impairedcognitive function. Radiol Clin NorthAm 2005; 43:67-77.
43. Nihashi T, Yatsuya H, Hayasaka K, etal. Direct comparison study betweenFDG-PET and IMP-SPECT fordiagnosing Alzheimer's disease using3D-SSP analysis in the same patients.Radiat Med 2007; 25:255-62.
44. Waragai M, Yamada T, Matsuda H.Evaluation of brain perfusion SPECTusing an easy Z-score imaging system(eZIS) as an adjunct to early-diagnosisof neurodegenerative diseases. J NeurolSci 2007; 260:57-64.
45. Mendez MF, Shapira JS, McMurtray A,et al. Accuracy of the clinicalevaluation for frontotemporaldementia. Arch Neurol 2007; 64:830-5.
46. Ishii K, Soma T, Kono AK, et al.Comparison of regional brain volumeand glucose metabolism betweenpatients with mild dementia with lewybodies and those with mildAlzheimer's disease. J Nucl Med 2007;48(5):704-1.
47. Klunk WE, Engler H, Nordberg A, et al.Imaging brain amyloid in Alzheimer'sdisease with Pittsburgh Compound-B.Ann Neurol 2004; 55:306-19.
48. Giannakopoulos P, Herrmann FR,Bussiere T, et al. Tangle and neuronnumbers, but not amyloid load, predictcognitive status in Alzheimer's disease.Neurology 2003; 60:1495-1500.
49. Small GW, Kepe V, Ercoli LM, et al.PET of brain amyloid and tau in mildcognitive impairment. N Engl J Med2006; 355:2652-63.
50. Mueller SG, Weiner MW, Thal LJ, et al.Ways toward an early diagnosis inAlzheimer's disease: The Alzheimer'sDisease Neuroimaging Initiative(ADNI). Alzheimers Dement 2005;1:55-66.

18 • The Canadian Review of Alzheimer’s Disease and Other Dementias
Molecular ImagingTechniquesMolecular imaging of the brainaims to quantify various biologi-cal processes via the modeling ofinteractions between a molecularprobe and a molecule of interestnaturally occurring in a livingorganism. Brain molecular-imag-ing techniques such as positronemission tomography (PET) andsingle photon emission tomogra-phy (SPECT) allow clinical inves-tigators to record and analyzesuch interactions in vivo. PET andSPECT associated with specificmolecular probes are sensitive to
detecting biological processes inthe order of pico-molar (10-12),however these techniques havelimited spatial resolution. In con-trast, magnetic resonance imaging(MRI) has a tremendous spatialresolution (sub-milliliter range)but lower sensitivity (micro-molar; 10-6) relative to PET andSPECT (Table 1). Together, thesetechniques reveal critical informa-tion with regards to the alterationsin the brain’s anatomy and physi-ology witnessed in dementia, aswell as canalizing diagnosticmethods and therapeutic interven-tions.
The Nature of PET Imaging The goal of a PET study indementia is to quantify importantbiological processes altered in thebrains of patients with dementia,such as glucose metabolism, cere-bral blood flow, the availability ofneuroreceptors and the detectionof disease-related molecules (i.e.,amyloid deposits, tangles, inflam-
mation).1 PET is a complex evalu-ation requiring expertise in manyfields such as nuclear medicine,radiochemistry, imaging, kineticsand neuroscience. A PET scanlikewise encompasses variousactivities such as:1. production of a radioisotope;2. synthesis of a
radiopharmaceutical;3. data acquisition;4. imaging reconstruction; and5. estimation of a biologically
relevant outcome by the analysis of the brain radioactivity distribution mapsrecorded during the course ofthe study (Figure 1).
The production of a radioisotope isgenerally obtained with a particleaccelerator known as a medicalcyclotron (Figure 1A) , which pro-duces a beam of high-energy pro-tons or deuterons directed against atarget consisting of the nuclei ofstable atoms. This process resultsin transmutation of the targetnucleus into a short-lived positron-
Research indicates that positron emission tomography (PET) aids in assisting specialists inthe early and differential diagnosis of Alzheimer’s disease (AD). In this article, Dr. Rosa-Neto and Mr. Leuzy discuss how PET reveals critical information on various aspects of thebrain physiology altered by dementia.
Pedro Rosa-Neto, MD, PhD; and Antoine Leuzy
Molecular Imaging of Alzheimer’sDisease Using PET
Pedro Rosa-Neto, MD, PhDAssistant Professor ofNeurology/Neurosurgery andPsychiatry, McGill University,affiliated to the Douglas ResearchCentre, Montreal, Quebec.
Antoine LeuzyResearch Associate at the BrainImaging Centre of the MontrealNeurological Institute, McGillUniversity, Montreal, Quebec.

The Canadian Review of Alzheimer’s Disease and Other Dementias • 19
emitting radioisotope (Figure 1B).Spontaneous decomposition of theproduced radioisotope occurs with-in a specific half-life ([15O], twominutes; [11C], 20.4 minutes and[18F], 109.8 minutes). The productof decomposition of these radioiso-topes is an anti-electron, known asa positron. Once produced at thecyclotron facility, positron-emittingradioisotopes are chemically incor-porated into radiopharmaceuticals(Figure 1C). Positrons emitted bythe radioisotope present in theradiopharmaceutical collide withsurrounding electrons. The result-ant collision between the emittedpositron and any electron locatedin its vicinity releases the rest-mass energy of the two particles(E = mc2) as two high-energy pho-tons (gamma rays) of 511 keVeach. The photons are released atan angle of 180 degrees. If thisannihilation event occurs within thePET field of view, a ring of detec-tors converts the coincident pho-tons into light, which is subse-quently amplified by photo-multi-pliers. Finally, the events computedby the scanner are analyzed byalgorithms, which reconstruct thedata as maps of the radioactivityconcentration in the brain as a func-tion of time (Figure 1F).
PET records the interactionsbetween radiopharmaceuticalsand molecules of interest. Inessence, PET is a technique thatcomputes patterns of spatial-tem-poral distributions of positron-emitting radioisotopes in the brainor any other part of the body
(Figure 1F). With few exceptions,positron-emitting radioisotopesadministered to dementia patientsare associated with molecularprobes called radiopharmaceuti-cals (Figure 1C), and thus, onemay assume that the distributionof radioactivity recorded by thePET camera refers to the distribu-tion of the radiopharmaceuticals inthe brain or any other organ. Theuse of mathematical modelsallows for the extraction of biolog-ically relevant information fromthe spatial-temporal distributionsof positron-emitting radioisotopesrecorded during the PET scan.However the mathematical models
provide accurate results if:1. the radiopharmaceuticals
specifically interact with onlyone molecule of interest in thebrain during the time frame ofthe PET scan; and
2. the radiopharmaceuticals are in“tracer concentration” (minutedoses incapable of causing anypharmacologic effect).
Typical biological outcomes ofinterest for clinical research indementia include the biodistribu-tion of pharmaceuticals, the identi-fication of disease-related mole-cules and the estimation of rates ofmolecular transport and energymetabolism.
Figure 1
Overview of the Procedures Involved in a PET Scan
Production of radioisotopes for PET scans requires short-lived positron-emitting radioiso-topes. Thus, a cyclotron (A) and radiochemistry unit must be located near the PET scannerto ensure the rapid delivery of short-lived positron-emitting radioisotopes (B) required tolabel radiopharmaceuticals (C). A radiochemistry unit is required for the synthesis of radio-pharmaceuticals and for quality control of PET radiopharmaceuticals. The PET scan requiresthe venous injection of a trace amount of the molecular probe (D). The PET (E) camerarecords the dynamic distribution of radioactivity (F) during the time-course of a study.Images of radiopharmaceutical concentrations in the brain are reconstructed using sophis-ticated methods. Further processing of PET images will eventually provide biologically rel-evant outcomes (G). The biologically relevant outcomes are frequently expressed usingcolour scales, which are numerical representations of a biological process for every singlevoxel of the brain.
(C) RadiochemistrySynthesis ofradiopharmaceutical
Molecular probeRadio isotope
Isotopes[18F][11C][124I][15 ]�
Half life109 min20 min4 days2.1 min
(E) Dataacquisition
(F) Datareconstruction
(G) Biologicaloutcome
(D) Injection
(A) CyclotronProduction of aradioisotope
(B) Position emittingradioisotopes
N
HN
N
O
O
F
S
�

20 • The Canadian Review of Alzheimer’s Disease and Other Dementias
PET Imaging Outcomes ofInterest for Alzheimer’sDisease (AD)Post-mortem studies indicate thatthe pathophysiologic processinvolved in AD begins long beforethe clinical symptoms develop.2,3
Thus, due to its high sensitivity andnoninvasive nature, PET can iden-tify the presence of the pathologi-cal molecules. Indeed, a number ofimaging studies using longitudinaldesigns have shown the potentialof PET to detect presymptomaticor prodromal AD in a population
with elevated genetic risk and insubjects with mild memory impair-ment.4-8 In general, PET studieson AD focus on the quantificationof abnormal metabolic changes,the detection of disease-specificabnormal proteins (tau and amy-loid deposits) as well as declines inneurotransmission.9,10 PET associ-ated with various molecular probeshas the potential to diagnose andmonitor disease progression andtreatment. Table 2 summarizes sev-eral PET radiopharmaceuticalsapplied to AD research.
Imaging abnormal cerebralblood flow and metabolism inAD. Pioneer studies of brainmetabolism performed by Ketyand Lassen3,10 in the mid 1950sshowed that a global decline ofbrain perfusion and metabolism ispresent in patients with dementia.The advent of tomographic imag-ing revealed that cerebral bloodflow and metabolic consequencesof dementia are not widely dif-fused through the brain; ratherthey are associated with a majordysfunction of certain brainregions (Figure 2 and 3).11,12
Brain regional glucose metabo-lism is typically estimated usingthe PET and the molecular probe2-fluoro-2-deoxy-D-glucose([18F]FDG), which is an analogueof glucose normally consumed bythe brain.13,14 In brief, the accumu-lation of [18F]FDG in a given brainregion is proportional to its glucosemetabolic rate (Figure 2).13,15 Intypical cases of AD, declines ofbrain glucose metabolism(hypometabolism) and cerebralblood flow initially occur in theposterior parieto-temporal cortexand posterior cingulate cortex(Figure 3).11,12,16 During the evolu-tion of AD, metabolic declines pro-gressively spread to other brainregions initially spared during theearly phase of the disease. Thehypometabolism revealed by PETin AD patients possibly reflectsseveral pathological processesunderlying AD pathology, such asloss of synaptic activity, gliosisand deposits of amyloid
Figure 2
Schematic Representation of [18F]FDG Uptake in the Brain inNormal Subjects and Patients with AD
Presynaptic Neuron
Postsynaptic Neuron
Blood Vessel
Glucose
CO2 + H2O CO2 + H2O
➔ ➔
Oxidativemetabolism
Synapse
[18F]FDG
GlucoseHexokinase 1
2
3 6 5
4
The glucose in the blood is transported from the vessel to the brain cells (1) where itundergoes anaerobic (2) and oxidative (3) metabolism resulting in energy, CO2 and H2O(4). Because energy and glucose consumption are linked with cell function, glucosemetabolism is accepted as an indicator of brain function. In a PET study, glucosemetabolism is measured after the venous injection of a tracer dose of [18F]FDG. Onceinjected, [18F]FDG is transported from the blood vessels to the brain cells (5). PETquantifies the amount of [18F]FDG-6P accumulated in the brain cells, as the hexokinase-mediated phosphorylation of [18F]FDG prevents any subsequent egress of [18F]FDG-6Pfrom these cells (6). [18F]FDG concentrations in the brain tissue and plasma are used tocalculate a biologically relevant outcome called the cerebral metabolic rate of glucose.The cerebral metabolic rate of glucose provides an estimate of the brains glucose-consumption rate. Low synaptic activity imposed by AD pathology (7) reduces glucosemetabolism and consequently reduces [18F]FDG accumulation in AD patients (right)compared to normal controls (left).
NORMAL AGING ALZHEIMER’S DISEASE
[18F]FDG-6P
Oxidativemetabolism
Glucose
Hexokinase[18F]FDG-6P
➔ ➔➔ ➔

The Canadian Review of Alzheimer’s Disease and Other Dementias • 21
plaques.17-19 Recent studies alsolink the hypometabolism in theposterior parieto-temporal cortexand posterior cingulate cortexwith various vulnerability factorsfor AD, such as the presence ofthe genetic polymorphism for theapolipoprotein E epsilon 4.12-14
Furthermore, several independentstudies strongly suggest that PET[18F]FDG is sensitive in detectingthe presence of hypometabolismin the brain several years beforethe onset of AD symptoms.15,16
Thus, the quantification of brainmetabolism in AD has potentialclinical relevance, since an earlydiagnosis of AD allows for earlyinterventions with disease-modi-fying therapies, which aim todelay the onset and progression ofAD.
Today, a PET [18F]FDG is typ-ically indicated by a specialist forpatients with a documented cogni-tive decline of at least six monthsand a recently established diagno-sis of dementia, meeting the diag-nostic criteria for AD. Althoughthe accuracy of a PET [18F]FDGas a diagnostic tool for AD maybe superior to a baseline clinicalevaluation,55 the diagnostic value
of a PET [18F]FDG is limitedsince regional hypometabolism isnot a specific finding of AD. PETassociated with radioligandsdesigned to target specific aspectsof AD neuropathology constitutesa research field with high transla-tional value.
Imaging brain pathology inAD. Advances in radiochemistrypermits the use of new radioli-gands specifically designed forthe quantification of pathologicalaspects of AD. Much attention hasbeen given to imaging of amyloiddeposition26,31 and neuroinflam-mation19,43,44 associated with AD.Imaging brain pathology usingPET may have important impacton disease-modifying therapies asthis therapeutic approach focuseson specific mechanisms such asthe formation of amyloid plaques,neuroprotection and neurorestora-tive approaches.
Imaging disease-related abnor-mal molecules. Progressive accu-mulation of abnormal proteinaggregates including amyloid ortau deposits are pathological hall-marks of AD. Abnormal amyloiddeposits in AD brains are found asneuritic plaques, amyloid
angiopathy and diffuse amyloiddeposits. The amyloid cascadehypothesis of AD predicts that theneurofibrillary tangles, cell loss,vascular damage, and dementiafollow as a direct result of pro-gressive abnormal amyloid depo-sition.22-24 Thus, quantifying theamyloid burden (amyloid accu-mulated) in the brain of ADpatients may aid in the diagnosisand monitoring of disease pro-gression.35,55 Another importantapplication for imaging disease-related abnormal proteins is toimprove the specificity and accu-racy of the diagnosis of AD andpredementia states.
Though several PET molecularagents for amyloid plaques havebeen tested, the [11C]PIB and the[18F]FDDNP have thus far provedto be the most effective radiophar-maceuticals in the demonstrationof AD pathology.26,27 While[11C]PIB seems to be more specif-ic to amyloid deposits, it has beensuggested that [18F]FDDNP hasan affinity for amyloid and tanglepathology. Preliminary studiesindicate that these lead com-pounds exhibit high binding inbrain areas affected by AD pathol-
Table 1
Summary of Molecular Imaging Modalities Utilized in the Investigation of Patients with AD
PET SPECT MRI
Sensitivity Pico-molar concentration Pico-molar concentration Micro-molar concentrationTypical anatomical 5 mm3 10 mm3 Less than 1mm3
resolutionQuantification Absolute Semiquantitative outcome Semiquantitative outcomeTypical radioisotopes [18F]FDG, [11C], [15O] [99mTc] Noneutilized [123I]

22 • The Canadian Review of Alzheimer’s Disease and Other Dementias
ogy, such as the frontal, temporaland parietal lobes. However, dep-osition in the brain is not uniqueto clinically apparent AD and hasbeen found in normal aging aswell as in patients in the presymp-tomatic stages of AD.28-31
The concept of amyloid imag-ing is currently being tested andhopefully PET imaging usingamyloid agents will be availablefor clinical purposes in the nearfuture.
Imaging neuroinflammationin AD. [11C]PK11195 is a radio-pharmaceutical that selectivelybinds to the peripheral benzodi-azepine receptor present in theactivated microglia, which is acell involved in brain inflammato-ry responses. In vivo studies car-ried out in various degenerativediseases, including AD, indicatethat the inflammation is an activeprocess underlying AD. The bind-ing of [11C]PK11195 is enhanced
in the entorhinal cortex, hip-pocampus and posterior cingulatecortex in patients with AD. In fact,neuroinflammation, as revealedby high [11C]PK11195 binding,was also present in AD patientswith a mild clinical presentationof the disease.19,43,44 The clinicalvalue of inflammation and amy-loid imaging techniques is stillunder evaluation.
Imaging abnormal neurotrans-mission in AD. Abnormalities invarious neurotransmission sys-tems such as those utilizing sero-tonin, glutamate and acetyl-choline, have been describedextensively in AD. In vivo quan-tification of such abnormalitiesmay help clinical researchers tounderstand the mechanismsunderlying AD and to proposenew therapeutic targets, theexploitation of which will hope-fully translate into improved qual-ity of life for AD patients.
Imaging cholinergic neuro-transmission. Declines in cholin-ergic neurotransmission have sig-nificant clinical relevance sincethe mechanisms of action of threeFDA-approved medications forthe treatment of AD aim toenhance brain acetylcholine neu-rotransmission through the inhibi-tion of acetylcholinesterase(AchE), the enzyme responsiblefor the breakdown of acetyl-choline. In fact, post-mortemstudies in AD patients indicateimportant declines in cholinergicinnervation as well as a globalreduction of acetylcholine synthe-sis capacity. These findings,together with the degeneration ofthe nucleus basalis of Meynert,strongly support that acetyl-choline neurotransmission isimpaired in AD. However, it hasbeen argued that in vivo quantifi-cation of presynaptic cholingergicneurotransmission in AD patients
Table 2
Summary of PET Molecular Agents Utilized in AD Research
Biological Process of Interest Molecular Agents Typical Findings in AD
Metabolism Glucose metabolism [18F]FDG HypometabolismOxygen metabolism [15O]O2 HypometabolismCerebral blood flow [15O]H2O Reduction of blood flow
Pathology Neuroinflammation [11C]PK11195 Inflammatory changesAmyloid plaques [11C]PIB High amyloid loadAmyloid plaques + tangles [18F]FDDNP High amyloid load
Serotonin 5-HT1A [18F]MPPF Low binding Serotonin 5-HT2A [18F]altanserin Unchanged
[18F]setoperone Low bindingDopamine D2 [11C]FLB Low bindingGABA [11C]flumazenil UnchangedAcetylcholinesterase (AchE) [11C]PMP, [11C]MP4A Reduction of AchE activity
Neurotransmission(Hippocampus/cortex)
(References: 12,16-18,48-52)
(References: 19,2117,18,25,26,29,30)
(References:2,35,36,41-44,53,54)

The Canadian Review of Alzheimer’s Disease and Other Dementias • 23
using PET is of limited value dueto peculiarities of the cholingergicneurotransmission.31 Therefore, itis expected that eventual progressin radiochemistry would allowadequate quantification of cholin-ergic neurotransmission in the liv-ing human brain. Studies using[11C]physostigmine, [11C]methyl-4-piperidyl-acetate ([11C]MP4A)and [11C]methylpiperidin-4-yl-propionate ([11C]PMP) confirmthe declines in cholinergic neuro-transmission reported by post-mortem studies; some of thesestudies found correlations betweencholinergic dysfunctions and cog-nitive deficits of AD patients.30-36
Cholinergic, muscarinic and nico-tinic receptors have been studied inpatients with AD, however theinterpretation of these studies islimited due the low specificity ofmost muscarinic and nicotinic neu-roreceptors. In brief, studies usingradiopharmaceuticals such as[11C]nicotine suggest a decline incholinergic nicotinic receptors inAD; studies with the muscarinicreceptor radiopharmaceuticals[11C]benztropine, [11C]-N-methyl-4-piperidyl benzilate and[18F]A85380 also indicate declinesin acetylcholine neurotransmissionin AD.38-40 So far no PET radio-pharmaceutical could properlyquantify the presynaptic aspects ofcholinergic neurotransmission.
Imaging serotonin anddopamine neurotransmission inAD. In contrast to cholinergic radio-pharmaceuticals, most of the currentserotonergic and dopaminergic PET
molecular agents allow for selective,reliable and accurate quantificationof various aspects of serotonin anddopamine neurotransmission. Serotonin 5-HT1A receptors areabundant in brain regions affectedby AD. Although there are con-flicting results regarding the 5-HT1A binding in the hippocam-pus of patients with predementia,it seems that AD patients havesubstantial declines in hippocam-pal 5-HT1A receptor binding.41,42
Declines in hippocampal dopa -mine D2 receptor binding are alsoreported in AD patients.51 In contrast, hippocampal and neo-cortical binding of gamma-aminobutyric acid (GABA) recep-tors remains unaltered in AD.52,53
Information regarding the avail-ability of serotonin 5-HT2A recep-tor is conflicting and remains tobe clarified.54-56 In the striatum,
while dopamine D2 receptors areunaffected by AD, dopamine D1
receptors are slightly decreased.57
Together these findings highlightthe role of hippocampal dopamineand serotonin neurotransmissionin the etiology of AD, howeverfurther research is necessary inorder to evaluate the clinical sig-nificance of these findings.
Future directions of PETimaging in ADCertainly, the main mission ofimaging in AD is the develop-ment of new techniques capableof accurately diagnosing prede-mentia states. Moreover, newradiopharmaceuticals for imag-ing cholinergic presynaptic ter-minals, imaging agents for glu-tamate synaptic function andefficient molecular probes fortau protein are amongst the
Figure 3
Typical Declines of Brain Glucose Metabolism in AD Patients
This is a composite plate showing an MRI (A,D), a PET [18F]FDG (B,E) and thecombination between PET and MRI images (C,F) obtained from a patient (female; 70years of age) with the diagnosis of probable AD. Note that in the fusion images (C,F), theMRI add spatial resolution to the PET. The indication (*) shows the posterior temporo-parietal junction (B,C) and the posterior cingulate gyrus (E,F), which are areas typicallyhypometabolic in AD.
A B C
D E F
* *
* *

24 • The Canadian Review of Alzheimer’s Disease and Other Dementias
important goals to be achievedby radiochemistry research.However, it is possible that sin-gle-mode imaging methods maynot provide sufficient diagnosticaccuracy for pre-AD dementia.Thus, multimodal imaging diag-nostic platforms with multiplemolecular probes may consti-tute an alternative for the currentsingle-mode imaging methods.
ConclusionsCurrent literature indicates thatonly PET [18F]FDG has clinicalrelevance in assisting specialists inthe early and differential diagnosisof AD.
Molecular imaging of ADpatients using PET associatedwith various radiopharmaceuti-cals provides valuable informa-tion regarding the numerous
aspects of the neurobiology ofdementia. Furthermore, PET haspotential research applicationssuch as early diagnosis, follow-ing the evolution of certain bio-markers during the course ofdementia, and in monitoringtreatment efficacy. Hopefullythese research applications willbe rapidly translated into benefitsfor patients living with AD.
References:1. Dubois B, Feldman HH, Jacova C et al.
Research criteria for the diagnosis ofAlzheimer's disease: Revising theNINCDS-ADRDA criteria. Lancetneurology 2007; 6:734-46.
2. Phelps ME. PET: The merging ofbiology and imaging into molecularimaging. J Nucl Med 2000; 41:661-81.
3. Lassen NA, Munck O, Tottey ER.Mental function and cerebral oxygenconsumption in organic dementia. AmMed Assoc 1957; 77:126-33.
4. Foster NL, Chase TN, Fedio P et al.Alzheimer's disease: Focal corticalchanges shown by positron emissiontomography. Neurology 1983; 33:961-5
5. Mosconi L, Tsui WH, Rusinek H et al.Quantitation, regional vulnerability,and kinetic modeling of brain glucosemetabolism in mild Alzheimer'sdisease. Eur J Nucl Med Mol Imaging2007; 34:1467-79.
6. Raichle ME, Mintun MA. Brain workand brain imaging. Annual review ofneuroscience 2006; 29:449-76.
7. Minoshima S, Frey KA, Koeppe RA etal. A diagnostic approach inAlzheimer's disease using three-dimensional stereotactic surfaceprojections of fluorine-18-FDG PET. JNucl Med 1995; 36:1238-48.
8. Mosconi L, Brys M, Glodzik-SobanskaL, et al. Early detection of Alzheimer'sdisease using neuroimaging. Experimentalgerontology 2007; 42:129-38.
9. McGeer PL, Kamo H, Harrop R et al.Comparison of PET, MRI, and CT withpathology in a proven case ofAlzheimer's disease. Neurology 1986;36:1569-74.
10. Mazziotta JC, Toga AW, FrackowiakRSJ (2000). Brain mapping: Thedisorders. San Diego: Academic Press,pp. 669.
11. Toga AW, Mazziotta JC. (2002). Brainmapping: The methods. 2nd ed. SanDiego: Academic Press, pp. 877.
12. Small GW, Mazziotta JC, Collins MT etal. Apolipoprotein E Type 4 allele andcerebral glucose metabolism inrelatives at risk for familial Alzheimerdisease. Jama 1995; 273:942-7
13. Reiman EM, Chen K, Alexander GE etal. Correlations betweenapolipoprotein E epsilon 4 gene doseand brain-imaging measurements ofregional hypometabolism. Proceedingsof the National Academy of Sciencesof the United States of America 2005;102:8299-302
14. Mosconi L, Perani D, Sorbi S et al. MCIconversion to dementia and the APOEgenotype: A prediction study with FDG-PET. Neurology 2004; 63:2332-40
15. Teipel SJ, Drzezga A, Bartenstein P, etal. Effects of donepezil on corticalmetabolic response to activation during(18)FDG-PET in Alzheimer's disease: Adouble-blind cross-over trial.Psychopharmacology 2006; 187:86-94
16. Mega MS, Cummings JL, O'Connor SM,et al. Cognitive and metabolic responsesto metrifonate therapy in Alzheimerdisease. Neuropsychiatry NeuropsycholBehav Neurol 2001; 14:63-8
17. Blennow K, Zetterberg H. Pinpointingplaques with PIB. Nature medicine2006; 12:753-4.
18. Nordberg A. PET imaging of amyloid inAlzheimer's disease. Lancet neurology2004; 3:519-27
19. Groom GN, Junck L, Foster NL et al.PET of peripheral benzodiazepinebinding sites in the microgliosis ofAlzheimer's disease. J Nucl Med 1995;36:2207-10
20. Diorio D, Welner SA, Butterworth RFet al. Peripheral benzodiazepinebinding sites in Alzheimer's diseasefrontal and temporal cortex.Neurobiology of aging 1991;12:255-58
21. Cagnin A, Brooks DJ, Kennedy AM etal. In-vivo measurement of activatedmicroglia in dementia. Lancet 2001;358:461-467
22. Van Broeck B, Van Broeckhoven C,Kumar-Singh S. Current insights intomolecular mechanisms of Alzheimerdisease and their implications fortherapeutic approaches. NeurodegenerDis 2007; 4:349-65
23. Hardy JA, Higgins GA. Alzheimer'sdisease: The amyloid cascadehypothesis. Science 1992; 256:184-5
24. Hardy J, Allsop D. Amyloid depositionas the central event in the aetiology ofTrends Pharmacol Sci 1991; 12:383-8
25. Engler H, Forsberg A, Almkvist O et al.Two-year follow-up of amyloiddeposition in patients with Alzheimer'sdisease. Brain 2006; 129:2856-66
26. Shoghi-Jadid K, Small GW, AgdeppaED et al. Localization of neurofibrillarytangles and beta-amyloid plaques inthe brains of living patients withAlzheimer disease. Am J GeriatrPsychiatry 2002; 10:24-35
27. Klunk WE, Engler H, Nordberg A et al. Imaging brain amyloid inAlzheimer's disease with PittsburghCompound-B. Annals of neurology.2004;55:306-19
To access this article’s full reference list please visit:www.stacommunications.com/adreview.html.

1-800-616-8816

Prescribing Summary
Patient Selection Criteria
THERAPEUTIC CLASSIFICATION: Cholinesterase inhibitor
INDICATIONS AND CLINICAL USEARICEPT (donepezil hydrochloride) is indicated for the symptomatic treatmentof patients with mild, moderate and severe dementia of the Alzheimer’s type.Efficacy of ARICEPT in patients with mild-to-moderate Alzheimer’s disease(AD) was established in two 24-week and one 54-week placebo-controlledtrials. Efficacy in patients with severe AD was established in two 24-week/6-month placebo-controlled trials.ARICEPT tablets should only be prescribed by (or following consultation with)clinicians who are experienced in the diagnosis and management of AD.
CONTRAINDICATIONSARICEPT (donepezil hydrochloride) is contraindicated in patients with knownhypersensitivity to donepezil hydrochloride or to piperidine derivatives.
SPECIAL POPULATIONSUse in pregnant or nursing womenThe safety of ARICEPT during pregnancy and lactation has not been establishedand therefore, it should not be used in women of childbearing potential or in nursingmothers unless, in the opinion of the physician, the potential benefits to the patientoutweigh the possible hazards to the fetus or the infant.Use in childrenThere are no adequate and well-controlled trials to document the safety andefficacy of ARICEPT in any illness occurring in children. Therefore, ARICEPTis not recommended for use in children.Use in elderly patients (≥65 years of age)In AD patients, nausea, diarrhea, vomiting, insomnia, fatigue and anorexiaincreased with dose and age, and the incidence appeared to be greater infemale patients. Since cholinesterase inhibitors as well as AD can beassociated with significant weight loss, caution is advised regarding the use ofARICEPT in low body weight elderly patients, especially in those ≥85 years old.Use in elderly patients with comorbid diseaseThere is limited safety information for ARICEPT in patients with mild-to-moderate or severe AD and significant comorbidity. The use of ARICEPT in ADpatients with chronic illnesses common among the geriatric population shouldbe considered only after careful risk/benefit assessment and include closemonitoring for adverse events (AEs). Caution is advised regarding the use ofARICEPT doses above 5 mg in this patient population.In severe AD, the possibility of comorbid vascular disease and risk factors forvascular AEs and mortality should be considered.Use in patients with vascular dementiaThree clinical trials, each of 6 months duration, were conducted to evaluate thesafety and efficacy of ARICEPT for the symptomatic treatment of individualsmeeting the NINDS-AIREN criteria for probable or possible vascular dementia(VaD).The NINDS-AIREN criteria are designed to identify patients with dementiathat appears to be due solely to vascular causes, and to exclude patients withAD. ARICEPT was not shown to be an effective treatment for patients withvascular dementia in two of these clinical trials.The safety profile from these controlled clinical trials in VaD patientsindicates that the rate of occurrence of treatment-emergent AEs overall washigher in VaD patients (86%) than in AD patients (75%). This was seen in bothARICEPT-treated subjects and placebo-treated subjects, and may relate to thegreater number of comorbid medical conditions in the VaD population.In two of the clinical trials, there was a higher rate of mortality among patients
treated with ARICEPT, during double-blind treatment; this result was statisticallysignificant for one of these two trials. For the three VaD studies combined, themortality rate in the ARICEPT group (1.7%, 25/1,475) was numerically higherthan in the placebo group (1.1%, 8/718), but this difference was not statisticallysignificant (see Supplemental Product Information below).There is no evidence of an increase risk of mortality when ARICEPT is used inpatients with mild-to-moderate AD.
Safety Information
WARNINGS AND PRECAUTIONSCardiovascularBecause of their pharmacological action, cholinesterase inhibitors may havevagotonic effects on heart rate (e.g., bradycardia). The potential for this actionmay be particularly important to patients with “sick sinus syndrome” or othersupraventricular cardiac conduction conditions.In clinical trials in AD, most patients with serious cardiovascular conditionswere excluded. Patients, such as those with controlled hypertension(DBP<95 mmHg), right bundle branch blockage, and pacemakers, wereincluded. Therefore, caution should be taken in treating patients with activecoronary artery disease and congestive heart failure. Syncopal episodes havebeen reported in association with the use of ARICEPT. It is recommendedthat ARICEPT should not be used in patients with cardiac conductionabnormalities (except for right bundle branch block) including “sick sinussyndrome” and those with unexplained syncopal episodes.GastrointestinalThrough their primary action, cholinesterase inhibitors may be expected toincrease gastric acid secretion due to increased cholinergic activity. Therefore,patients at increased risk for developing ulcers, e.g., those with a history ofulcer disease or those receiving concurrent nonsteroidal anti-inflammatorydrugs (NSAIDs) including high doses of acetylsalicylic acid (ASA), should bemonitored for symptoms of active or occult gastrointestinal bleeding. Clinicalstudies of ARICEPT have shown no increase, relative to placebo, in theincidence of either peptic ulcer disease or gastrointestinal bleeding (seeADVERSE REACTIONS section).ARICEPT, as a predictable consequence of its pharmacological properties, hasbeen shown to produce, in controlled clinical trials in patients with AD, diarrhea,nausea and vomiting. These effects, when they occur, appear more frequentlywith the 10 mg dose than with the 5 mg dose. In most cases, these effects haveusually been mild and transient, sometimes lasting 1 to 3 weeks and haveresolved during continued use of ARICEPT (see ADVERSE REACTIONS section).Treatment with the 5 mg/day dose for 4-6 weeks prior to increasing the dose to10 mg/day is associated with a lower incidence of gastrointestinal intolerance.GenitourinaryAlthough not observed in clinical trials of ARICEPT, cholinomimetics may causebladder outflow obstruction.HepaticThere is limited information regarding the pharmacokinetics of ARICEPT inhepatically-impaired AD patients.Close monitoring for AEs in patients with hepatic disease being treated withARICEPT is therefore recommended.NeurologicSeizures: Some cases of seizures have been reported with the use ofARICEPT in clinical trials and from spontaneous Adverse Reactionreporting. Cholinomimetics can cause a reduction of seizure threshold,increasing the risk of seizures. However, seizure activity may also be amanifestation of AD.The risk/benefit of ARICEPT treatment for patients with ahistory of seizure disorder must therefore be carefully evaluated.ARICEPT has not been studied in patients with Parkinsonian features. Theefficacy and safety of ARICEPT in these patients are unknown.Peri-operative considerationsAnesthesia: ARICEPT, as a cholinesterase inhibitor, is likely to exaggeratesuccinylcholine-type muscle relaxation during anesthesia.

RenalThere is limited information regarding the pharmacokinetics of ARICEPT inrenally impaired AD patients.Close monitoring for AEs in patients with renal disease being treated withARICEPT is therefore recommended.RespiratoryBecause of their cholinomimetic action, cholinesterase inhibitors should beprescribed with care to patients with a history of asthma or obstructive pulmonarydisease. ARICEPT has not been studied in patients under treatment for theseconditions and should therefore be used with particular caution in such patients.
ADVERSE REACTION SERIOUSNESS AND INCIDENCEMild-to-moderate Alzheimer’s diseaseA total of 747 patients with mild-to-moderate AD were treated in controlledclinical studies with ARICEPT (donepezil hydrochloride). Of these patients,613 (82%) completed the studies. The mean duration of treatment for allARICEPT groups was 132 days (range 1-356 days).The rates of discontinuation from controlled clinical trials of ARICEPT due toAEs for the ARICEPT 5 mg/day treatment groups were comparable to thoseof placebo-treatment groups at approximately 5%.The rate of discontinuationof patients who received the 10 mg/day dose after only a 1-week initialtreatment with 5 mg/day ARICEPT was higher at 13% (see Table 1).The most common AEs, defined as those occurring at a frequency of at least5% in patients receiving 10 mg/day and twice the placebo rate, are largelypredicted by ARICEPT’s cholinomimetic effects. These include nausea,diarrhea, insomnia, vomiting, muscle cramp, fatigue and anorexia.These AEs were often of mild intensity and transient, resolving during continuedARICEPT treatment without the need for dose modification.There is evidence to suggest that the frequency of these common AEs may beaffected by the duration of treatment with an initial 5 mg daily dose prior toincreasing the dose to 10 mg/day (see Table 2 and Supplemental ProductInformation below).Severe Alzheimer’s diseaseA total of 573 patients with severe AD were treated in controlled clinical studieswith ARICEPT. Of these patients, 441 (77%) completed the studies.The durationof double blind treatment in all studies was 24 weeks. The mean duration oftreatment for all ARICEPT groups was 148.4 days (range 1-231 days).The meandaily dose of ARICEPT was 7.5 mg/day.In clinical trials of patients with severe AD, most patients with significant comorbidconditions were excluded.The use of ARICEPT inAD patients with chronic illnessescommon among the geriatric population should be considered only after carefulrisk/benefit assessment and should include close monitoring for AEs.In controlled clinical trials in severe AD, the rate of discontinuation due to AEswas 11.3% in patients treated with ARICEPT, compared to 6.7% in the placebogroup.The most common AEs that led to discontinuation, more often in patientstreated with ARICEPT than placebo, were diarrhea, nausea, vomiting, urinarytract infection, decreased appetite, and aggression. Each of these AEs led todiscontinuation of less than 2% of patients treated with ARICEPT.The incidence profile for AEs for severe AD was similar to that of mild-to-moderate AD (see Table 4).The most common AEs, defined as those occurring at a frequency of at least5% in patients and twice the placebo rate, were vomiting, diarrhea, nausea,and aggression. Overall, the majority of AEs were judged by the investigatorsto be mild or moderate in intensity.Results from the controlled clinical trials indicate that the incidence of AEs,such as vomiting, urinary tract infection, urinary incontinence, pneumonia,falls, decreased appetite, aggression, restlessness, hallucination andconfusion, may be higher in ARICEPT- and placebo-treated patients withsevere AD than in patients with mild-to-moderate AD.Postmarket adverse drug reactionsVoluntary reports of AEs temporally associated with ARICEPT that have beenreceived since market introduction that are not listed above, and for whichthere is inadequate data to determine the causal relationship with the drug,include the following: abdominal pain, cholecystitis, convulsions, heart block (alltypes), hemolytic anemia, hepatitis, hyponatremia, pancreatitis, and rash.
DRUG INTERACTIONSConcomitant Use with Other DrugsUse with anticholinergics: Because of their mechanism of action,cholinesterase inhibitors have the potential to interfere with the activity ofanticholinergic medications.Use with cholinomimetics and other cholinesterase inhibitors: A synergisticeffect may be expected when cholinesterase inhibitors are given concurrentlywith succinylcholine, similar neuromuscular blocking agents or cholinergicagonists, such as bethanechol.Use with other psychoactive drugs: Few patients in controlled clinical trialsreceived neuroleptics, antidepressants or anticonvulsants. There is thus limitedinformation concerning the interaction of ARICEPT with these drugs.Drug-drug interactionsPharmacokinetic studies, limited to short-term, single-dose studies in youngsubjects, evaluated the potential of ARICEPT for interaction with theophylline,cimetidine, warfarin and digoxin administration. No significant effects on thepharmacokinetics of these drugs were observed. Similar studies in elderlypatients were not done (see Supplemental Product Information below).Health Canada may be notified by phone of serious or unexpected reaction to thisdrug at: 1-866-234-2345.
Administration
Dosing considerationsARICEPT (donepezil hydrochloride) or ARICEPT RDT should only be prescribedby (or following consultation with) clinicians who are experienced in the diagnosisand management of AD.Special populations: The use of ARICEPT in AD patients with chronic illnessescommon among the geriatric population, should be considered only aftercareful risk/benefit assessment and include close monitoring for AEs. It isrecommended that ARICEPT be used with caution in these patient populations.AEs are more common in individuals of low body weight, in patients ≥85 yearsold and in females.Recommended dose and dosage adjustmentAdults:The recommended initial dose of ARICEPT or ARICEPT RDT is 5 mg takenonce daily.Therapy with the 5 mg dose should be maintained for 4-6 weeks beforeconsidering a dose increase, in order to avoid or decrease the incidence of themost common adverse reactions to the drug (see ADVERSE REACTIONS section)and to allow plasma levels to reach steady state. Based on clinical judgement, the10 mg daily dose may be considered following 4-6 weeks of treatment at 5 mg/day.The maximum recommended dose is 10 mg taken once daily.Following initiation of therapy or any dosage increase, patients should be closelymonitored for AEs.Special populations: AEs are more common in individuals of low body weight,in patients ≥85 years old and in females. In elderly women of low body weight,the dose should not exceed 5 mg/day.In a population of cognitively-impaired individuals, safe use of this and all othermedications may require supervision.AdministrationARICEPT should be taken once daily in the morning or evening. It may betaken with or without food.ARICEPT tablets should be swallowed whole with water.ARICEPT RDT should be placed on the tongue and allowed to disintegratebefore swallowing with water.
Study References
1. Seltzer B et al. Efficacy of donepezil in early-stage Alzheimer disease.Arch Neurol 2004;61:1852-1856.
2. Rogers SL et al. A 24-week, double-blind, placebo-controlled trial ofdonepezil in patients with Alzheimer’s disease. Neurology 1998;50:136-145.

Supplemental Product InformationWARNINGS AND PRECAUTIONSUse in pregnant and nursing womenTeratology studies conducted in pregnant rats at doses of up to 16 mg/kg/day and in pregnant rabbits at doses of up to 10 mg/kg/daydid not disclose any evidence for a teratogenic potential of ARICEPT.
Use in elderly patients (≥65 years of age)In controlled clinical studies with 5 and 10 mg ARICEPT in patients with mild-to-moderate AD, there were 536 patients between theages of 65 to 84, and 37 patients aged ≥85 years treated with ARICEPT. In controlled clinical trials of patients with severe AD, therewere 158 patients who were ≤74 years of age, 276 patients between the ages of 75 and 84, and 139 patients aged ≥85 years treatedwith ARICEPT.
Use in patients with vascular dementiaMortality Rates in ARICEPT Vascular Dementia Clinical TrialsStudy Placebo ARICEPT 5 mg p-valuex ARICEPT 10 mg p-valuex
307 3.5% (7/199) 1.0% (2/198) 0.17 2.4% (5/206) 0.57308 0.5% (1/193) 1.9% (4/208) 0.37 1.4% (3/215) 0.62319 0% (0/326) 1.7% (11/648) 0.02 * NACombined 1.1% (8/718) 1.7% (25/1,475) 0.35* No 10 mg ARICEPT treatment arm in Study 319.x p-values are for 5 mg donepezil vs. placebo and 10 mg donepezil vs. placebo.The majority of deaths in patients taking either ARICEPT or placebo appear to have resulted from various vascular-related causes,which may be expected in this elderly, fragile, population with comorbid vascular disease. In the three combined VaD clinical trials,there were similar proportions of patients with serious AEs in both treatment groups (approximately 15%), and similar proportions ofpatients with serious cardiovascular or cerebrovascular AEs (non-fatal and fatal, approximately 8%). The proportion of patients whohad a fatal cardiovascular or cerebrovascular AE was numerically higher in the ARICEPT group than in the placebo group, but thisdifference was not statistically significant across the three trials.
ADVERSE REACTIONSMild-to-moderate Alzheimer’s diseaseThe most common AEs leading to discontinuation, defined as those occurring in at least 2% of patients and at twice the incidenceseen in placebo patients, are shown in Table 1.
Table 1. Most Frequent Adverse Events in Patients with Mild-to-Moderate Alzheimer’s Disease Leading to Withdrawalfrom Controlled Clinical Trials by Dose Group
Dose Group Placebo 5 mg/day ARICEPT 10 mg/day ARICEPTNumber of Patients Randomized 355 350 315Events/% DiscontinuingNausea 1% 1% 3%Diarrhea 0% <1% 3%Vomiting <1% <1% 2%An open-label study was conducted with 269 patients who received placebo in the 15- and 30-week studies.These patients receiveda 5 mg/day dose for 6 weeks prior to initiating treatment with 10 mg/day. The rates of common AEs were lower than those seen incontrolled clinical trial patients who received 10 mg/day after only a 1-week initial treatment period with a 5 mg daily dose, and werecomparable to the rates noted in patients treated only with 5 mg/day.See Table 2 for a comparison of the most common AEs following 1- and 6-week initial treatment periods with 5 mg/day ARICEPT.
Table 2. Comparison of Rates of Adverse Events in Patients with Mild-to-Moderate Alzheimer’s Disease Treated with10 mg/day after 1 and 6 Weeks of Initial Treatment with 5 mg/day
1-Week 6-WeekNo Initial Treatment Initial Treatment Initial Treatment
with 5 mg/day with 5 mg/dayAdverse Event Placebo 5 mg/day 10 mg/day 10 mg/day
(n=315) (n=311) (n=315) (n=269)Nausea 6% 5% 19% 6%Diarrhea 5% 8% 15% 9%Insomnia 6% 6% 14% 6%Fatigue 3% 4% 8% 3%Vomiting 3% 3% 8% 5%Muscle cramps 2% 6% 8% 3%Anorexia 2% 3% 7% 3%The events cited reflect experience gained under closely monitored conditions of clinical trials in a highly selected patient population.In actual clinical practice or in other clinical trials, these frequency estimates may not apply, as the conditions of use, reportingbehaviour, and the kinds of patients treated may differ.Table 3 lists treatment-emergent signs and symptoms (TESS) that were reported in at least 2% of patients from placebo-controlledclinical trials who received ARICEPT, and for which the rate of occurrence was greater for ARICEPT than placebo-assigned patients.In general, AEs occurred more frequently in female patients and with advancing age.
Table 3. Mild-to-Moderate Alzheimer’s Disease: Adverse Events Reported in Controlled Clinical Trials in at Least 2% ofPatients Receiving ARICEPT and at a Higher Frequency than Placebo-Treated Patients
Body System/Adverse Events Placebo n=355 ARICEPT n=747Percent of Patients with any Adverse Event 72 74Body as a Whole
Headache 9 10Pain, various locations 8 9Accident 6 7Fatigue 3 5
Cardiovascular SystemSyncope 1 2
Digestive SystemNausea 6 11Diarrhea 5 10Vomiting 3 5Anorexia 2 4
Hemic and Lymphatic SystemEcchymosis 3 4
Metabolic and NutritionalWeight decrease 1 3
Musculoskeletal SystemMuscle cramps 2 6Arthritis 1 2
Nervous SystemInsomnia 6 9Dizziness 6 8Depression <1 3Abnormal dreams 0 3Somnolence <1 2
UrogenitalFrequent urination 1 2
Other adverse events observed during clinical trials in mild-to-moderate Alzheimer’s diseaseDuring the premarketing phase, ARICEPT has been administered to over 1,700 individuals with mild-to-moderate AD for variouslengths of time during clinical trials worldwide. Approximately 1,200 patients have been treated for at least 3 months, and more than
1,000 patients have been treated for at least 6 months. Controlled and uncontrolled trials in the United States included approximately900 patients. In regards to the highest dose of 10 mg/day, this population includes 650 patients treated for 3 months, 475 patientstreated for 6 months and 115 patients treated for over 1 year. The range of patient exposure is from 1 to 1,214 days.Treatment-emergent signs and symptoms that occurred during 3 placebo-controlled clinical trials and 2 open-label trials of patientswith mild-to-moderate AD were recorded as AEs by the clinical investigators using terminology of their own choosing. To provide anoverall estimate of the proportion of individuals having similar types of events, the studies were integrated and the events weregrouped into a smaller number of standardized categories using a modified COSTART dictionary and event frequencies were calculatedacross all studies.These categories are used in the listing below.The frequencies represent the proportion of 900 patients from thesetrials experiencing that event while receiving ARICEPT. All AEs occurring at least twice are included. AEs already listed in Tables 2and 3 are not repeated here (i.e., events occurring at an incidence >2%). Also excluded are COSTART terms too general to beinformative, or events less likely to be drug-caused. Events are classified by body system and listed as occurring in ≥1% and <2%of patients (i.e., in 1/100 to 2/100 patients: frequent) or in <1% of patients (i.e., in 1/100 to 1/1,000 patients: infrequent). These AEsare not necessarily related to ARICEPT treatment, and in most cases were observed at a similar frequency in placebo-treated patientsin the controlled studies.Body as a Whole: (≥1% and <2%) influenza, chest pain, toothache; (<1%) fever, edema face, periorbital edema, hernia hiatal,abscess, cellulitis, chills, generalized coldness, head fullness, head pressure, listlessness.Cardiovascular System: (≥1% and <2%) hypertension, vasodilation, atrial fibrillation, hot flashes, hypotension; (<1%) angina pectoris,postural hypotension, myocardial infarction, premature ventricular contraction, arrhythmia, AV Block (first degree), congestive heartfailure, arteritis, bradycardia, peripheral vascular disease, supraventricular tachycardia, deep vein thromboses.Digestive System: (≥1% and <2%) fecal incontinence, gastrointestinal bleeding, bloating, epigastric pain; (<1%) eructation, gingivitis,increased appetite, flatulence, periodontal abscess, cholelithiasis, diverticulitis, drooling, dry mouth, fever sore, gastritis, irritable colon,tongue edema, epigastric distress, gastroenteritis, increased transaminases, hemorrhoids, ileus, increased thirst, jaundice, melena,polydipsia, duodenal ulcer, stomach ulcer.Endocrine System: (<1%) diabetes mellitus, goiter.Hemic & Lymphatic System: (<1%) anemia, thrombocythemia, thrombocytopenia, eosinophilia, erythrocytopenia.Nutritional Disorders: (≥1% and <2%) dehydration; (<1%) gout, hypokalemia, increased creatine kinase, hyperglycemia, weightincrease, increased lactate dehydrogenase.Musculoskeletal System: (≥1% and <2%) bone fracture; (<1%) muscle weakness, muscle fasciculation.Nervous System: (≥1% and <2%) delusions, tremor, irritability, paresthesia, aggression, vertigo, ataxia, libido increased, restlessness,abnormal crying, nervousness, aphasia; (<1%) cerebrovascular accident, intracranial hemorrhage, transient ischemic attack, emotionallability, neuralgia, coldness (localized), muscle spasm, dysphoria, gait abnormality, hypertonia, hypokinesia, neurodermatitis, numbness(localized), paranoia, dysarthria, dysphasia, hostility, decreased libido, melancholia, emotional withdrawal, nystagmus, pacing, seizures.Respiratory System: (≥1% and <2%) dyspnea, sore throat, bronchitis; (<1%) epistaxis, postnasal drip, pneumonia, hyperventilation,pulmonary congestion, wheezing, hypoxia, pharyngitis, pleurisy, pulmonary collapse, sleep apnea, snoring.Skin and Appendages: (≥1% and <2%) abrasion, pruritus, diaphoresis, urticaria; (<1%) dermatitis, erythema, skin discoloration,hyperkeratosis, alopecia, fungal dermatitis, herpes zoster, hirsutism, skin striae, night sweats, skin ulcer.Special Senses: (≥1% and <2%) cataract, eye irritation, blurred vision; (<1%) dry eyes, glaucoma, earache, tinnitus, blepharitis,decreased hearing, retinal hemorrhage, otitis externa, otitis media, bad taste, conjunctival hemorrhage, ear buzzing, motion sickness,spots before eyes.Urogenital System: (≥1% and <2%) urinary incontinence, nocturia; (< 1%) dysuria, hematuria, urinary urgency, metrorrhagia,cystitis, enuresis, prostate hypertrophy, pyelonephritis, inability to empty bladder, breast fibroadenosis, fibrocystic breast, mastitis,pyuria, renal failure, vaginitis.
Long-term safety for mild-to-moderate Alzheimer’s diseasePatients were exposed to ARICEPT in 2 open-label extension mild-to-moderate AD studies (n=885) of over 2 years. In 1 of thestudies, 763 patients who previously completed 1 of 2 placebo-controlled studies of 15 or 30 weeks duration continued to receiveARICEPT and were evaluated for safety and neuropsychological evaluations for up to 152 weeks; the safety profile of ARICEPT inthis extension study remained consistent with that observed in placebo-controlled trials. Following 1 and 2 years of treatment, 76%(n=580) and 49% (n=374) of these patients, respectively, were still receiving therapy (cumulative weeks 48 and 108).
Severe Alzheimer’s diseaseTable 4 lists treatment-emergent signs and symptoms (TESS) that were reported in at least 2% of patients from placebo-controlledclinical trials who received ARICEPT, and for which the rate of occurrence was greater for ARICEPT than placebo-assigned patients
Table 4. Severe Alzheimer’s Disease: Adverse Events Reported in Controlled Clinical Trials in at Least 2% of PatientsReceiving ARICEPT and at a Higher Frequency than Placebo-Treated Patients
Body system/Adverse events Placebo n=465 ARICEPT n=573Percent of Patients with Any Adverse Event 74 81Gastrointestinal
Diarrhea 4 10Vomiting 4 8Nausea 3 6Fecal incontinence 1 2
GeneralPyrexia 1 2Chest pain 0 2
Infections and InfestationsUrinary tract infection 7 8Nasopharyngitis 6 8Pneumonia 3 4
Injury, Poisoning, Procedural ComplicationsFall 9 10Contusion 2 4Skin laceration 1 2
InvestigationsBlood creatine phosphokinase increased 1 2
Metabolism and NutritionAnorexia 2 4Decreased appetite 1 3Dehydration 1 2
Musculoskeletal and Connective TissueBack pain 2 3Osteoarthritis 1 2
Nervous SystemHeadache 3 5Somnolence 0 2
PsychiatricAggression 2 5Insomnia 3 4Restlessness 2 3Hallucination 1 2Confusional state 1 2
Renal and UrinaryUrinary incontinence 2 3
RespiratoryCough 1 2
SkinEczema 1 2
VascularHypertension 1 2
A frequency of 0 has been used when frequencies were <0.5%Other AEs that occurred with an incidence of at least 2% in ARICEPT-treated patients, and at an equal or lower rate than in placebo-treated patients, included: abdominal pain, fatigue, gastroenteritis, excoriation, dizziness, anxiety and depression.

Long-term safety for severe Alzheimer’s diseaseIn Study 315, which was a 24-week, randomized, placebo-controlled study in severe AD patients, at the end of double-blind treatment,229 patients entered open-label ARICEPT treatment for up to an additional 12 weeks. Therefore, at the end of the open-label phase,111 patients had received up to 36 weeks of ARICEPT treatment and 118 patients had received up to 12 weeks of ARICEPTtreatment.The most commonly affected body systems, types and frequencies of AEs reported during 12 weeks of open-label ARICEPT treatmentwere similar to what was observed during 24 weeks of double-blind treatment.Gastrointestinal AEs (diarrhea, nausea, vomiting, anorexia) were reported at a higher frequency in patients who received up to 12 weeksof ARICEPT treatment. Other AEs reported at higher frequencies in patients treated with ARICEPT for up to 12 weeks includedinfection, insomnia, pneumonia, fever, dizziness, hypertension, asthenia, tremor, pharyngitis, hallucinations, convulsions and cysts.In patients treated with ARICEPT for up to 36 weeks, accidental injury, urinary incontinence and urinary tract infections were reportedat higher frequencies.
DRUG INTERACTIONSDrug-drug interactionsDrugs highly bound to plasma proteins: Drug displacement studies have been performed in vitro between donepezil, a highlybound drug (96%) and other drugs such as furosemide, digoxin, and warfarin. Donepezil at concentrations of 0.3-10 μg/mL did notaffect the binding of furosemide (5 μg/mL), digoxin (2 ng/mL) and warfarin (3 μg/mL) to human albumin. Similarly, the binding ofdonepezil to human albumin was not affected by furosemide, digoxin and warfarin.Effect of ARICEPT on the metabolism of other drugs: In vitro studies show a low rate of donepezil binding to CYP 3A4 andCYP 2D6 isoenzymes (mean Ki about 50-130 μM), which, given the therapeutic plasma concentrations of donepezil (164 nM),indicates little likelihood of interferences. In a pharmacokinetic study involving 18 healthy volunteers, the administration of ARICEPTat a dose of 5 mg/day for 7 days had no clinically significant effect on the pharmacokinetics of ketoconazole. No other clinical trialshave been conducted to investigate the effect of ARICEPT on the clearance of drugs metabolized by CYP 3A4 (e.g., cisapride,terfenadine) or by CYP 2D6 (e.g., imipramine).It is not known whether ARICEPT has any potential for enzyme induction.Effect of other drugs on the metabolism of ARICEPT: Ketoconazole and quinidine, inhibitors of CYP450, 3A4 and 2D6, respectively,inhibit donepezil metabolism in vitro. In a pharmacokinetic study, 18 healthy volunteers received 5 mg/day ARICEPT together with200 mg/day ketoconazole for 7 days. In these volunteers,mean donepezil plasma concentrations were increased by about 30%-36%.Inducers of CYP 2D6 and CYP 3A4 (e.g., phenytoin, carbamazepine, dexamethasone, rifampin and phenobarbital) could increase therate of elimination of ARICEPT.Pharmacokinetic studies demonstrated that the metabolism of ARICEPT is not significantly affected by concurrent administration ofdigoxin or cimetidine.
Drug-food interactionsFood does not have an influence on the rate and extent of donepezil hydrochloride absorption.
Drug-herb interactionsInteractions with herbal products have not been established.
Drug-laboratory interactionsInteractions with laboratory tests have not been established.
SYMPTOMS AND TREATMENT OF OVERDOSESymptoms: Overdosage with cholinesterase inhibitors can result in cholinergic crisis characterized by severe nausea, vomiting,salivation, sweating, bradycardia, hypotension, respiratory depression, collapse and convulsions. Increasing muscle weakness is apossibility and may result in death if respiratory muscles are involved.Treatment: The elimination half-life of ARICEPT (donepezil hydrochloride) at recommended doses is approximately 70 hours. Thus,in the case of overdose, it is anticipated that prolonged treatment and monitoring of adverse and toxic reactions will be necessary.As in any case of overdose, general supportive measures should be utilized.Tertiary anticholinergics, such as atropine, may be used as an antidote for ARICEPT overdosage. Intravenous atropine sulfate titratedto effect is recommended: an initial dose of 1.0 to 2.0 mg IV with subsequent doses based upon clinical response.Atypical responsesin blood pressure and heart rate have been reported with other cholinomimetics when co-administered with quaternary anticholinergicssuch as glycopyrrolate. It is not known whether ARICEPT and/or its metabolites can be removed by dialysis (hemodialysis, peritonealdialysis, or hemofiltration).Dose-related signs of toxicity observed in animals included: reduced spontaneous movement, prone position, staggering gait,lacrimation, clonic convulsions, depressed respiration, salivation, miosis, fasciculation, and lower body surface temperature.
Product Monograph available on request.
ARICEPT® Eisai Co. Ltd., owner/Pfizer Canada Inc., Licensee© 2007 Pfizer Canada Inc., Kirkland, Quebec H9J 2M5

Advocating for Change: MakingDementia a National Health Priority
News from the Alzheimer Society of Canada
As the national voice for people affected by demen-tia, the Alzheimer Society has an important role toplay in advocating for change within our provincialand federal governments.
With approximately half a million Canadiansaffected by dementia, or one in every 13 people olderthan 65 years, this is more than just an importanthealth concern. This disease has the potential to over-whelm the healthcare system if fundamental changesare not made in research funding and care delivery.
By working to influence the programs and initia-tives that directly affect people living withAlzheimer's or a related disease, the AlzheimerSociety is helping to improve the quality of life foreveryone touched by dementia.
“The Alzheimer Society believes that researchremains the key to finding a cure, and that a signif-icant investment in science is essential if we are toeradicate dementia,” says Scott Dudgeon, CEO ofthe Alzheimer Society of Canada. “We also believethat there must be better support, care and treat-ment for people living with Alzheimer’s or a relat-ed disease.”
With this in mind, the Alzheimer Society ofCanada is building on the success of previousfederal-government initiatives and advocating theGovernment of Canada to sponsor the developmentof a Canadian Dementia Management Strategy.
Canadian Dementia Management StrategyThe purpose of the strategy will be to guide policydevelopment and care delivery, and it will drawupon the collaborative efforts of policymakers,healthcare-system managers, clinicians, researchersand healthcare providers.
It will encompass those aspects that most direct-ly impact the lives of those touched by Alzheimer’s
or a related disease, including: research, prevention,diagnosis, improved treatment, improved care andcare for caregivers.
“We know that tremendous strides are beingmade in the development of biomarkers, and in theuse of neuroimaging to facilitate rapid reliable diag-nosis and early intervention,” says Dr. JackDiamond, scientific director for the AlzheimerSociety of Canada. “Part of this strategy would be toensure that policy is in place to expedite adoption ofthese emerging diagnostic technologies.”
Raise Your VoiceTime is of the essence. As the population demo-graphics shift in Canada, it becomes paramount thatpreventive measures are put into place to avoid theepidemic of dementia.
“Already, many Canadians have taken up thechallenge and become Alzheimer advocates. Peopleliving with Alzheimer's and related diseases, care-givers, healthcare professionals and researchers arejoining their voices together to become a powerfultool for change, working to create a future withoutAlzheimer’s disease,” adds Dudgeon. “You too canmake a difference. Let your voice be heard bybecoming an Alzheimer’s advocate today.”
The Alzheimer Society of Canada is a not-for-profithealth organization dedicated to helping people affect-ed by Alzheimer’s disease. The Society provides supportand educational programs for people with Alzheimer’sdisease and their caregivers. The Society also fundsresearch into finding a cure for the disease, and intoimproved methods of caregiving. For more information,or to become an Alzheimer Advocate, please contactyour local Alzheimer Society, or visit www.alzheimer.ca
30 • The Canadian Review of Alzheimer’s Disease and Other Dementias

Featured at the Third
International Conference
on Creative Expression,
Communication and
Dementia
Mindscapes 2008, an exhibition of art produced byseniors with dementia, will be featured from June 2 toJune 16, 2008 at Emily Carr Institute of Arts and Designon Granville Island in Vancouver. The exhibitionfollows the opening of the Third InternationalConference on Creative Expression, Communicationand Dementia which will take place on May 30 and 31,2008 at Emily Carr. The exhibition is open to thepublic; admission is by donation.
These events are hosted by the Society for the Arts inDementia Care and the Institute of Neurosciences,Mental Health and Addiction to bring attention to thecreative abilities of seniors with dementia and tospotlight the research that is underway to improve thequality of life for these seniors.
The program includes invited speakers who areinternational leaders in their fields. They come from theUnited States, Australia and universities on the east andwest coasts of Canada, and will discuss their researchand practical approaches to dementia care.
In addition, an elegant dinner is planned for conferenceparticipants at the Granville Island Hotel, followed by apiano concert featuring the celebrated artists, Tami andYuval Admony, which is open to the public (ticketsonline).
Visit the conference website at: www.cecd-society.orgfor more information. Professionals, practitioners andthe interested public are welcome to attend.
For more information, contact: Dr. Dalia Gottlieb-Tanaka at 604/986-6408or at [email protected]

See prescribing summary on page
ARICEPT is indicated forthe symptomatic treat-ment of patients withmild, moderate andsevere dementia ofthe Alzheimer’s type.
ARICEPT does not changethe underlying course of the disease.
In patients with mild-to-moderate AD, themost common adverse events with ARICEPT10 mg/d after proper dose escalation includenausea, diarrhea, insomnia, vomiting, musclecramp, fatigue and anorexia (occurring in at least5% of patients and at twice the placebo rate).These events are usually mild and transient,resolving with continued ARICEPT treatmentwithout the need for dose modification.
In patients with severe AD, the most commonadverse events were vomiting, diarrhea, nausea,and aggression (occurring in at least 5% ofpatients and at twice the placebo rate). Overall,the majority of adverse events were judgedby the investigators to be mild or moderatein intensity.† In a 24-week, randomized, double-blind, placebo-controlled study of
ARICEPT in 153 mild AD patients (MMSE 21-26). Patients received eitherARICEPT 5 mg/d for the first 6 weeks and 10 mg/d thereafter, (n=96),or placebo (n=57). 37% of ARICEPT-treated patients experienced a4 point ADAS-cog improvement and 10% experienced a 7 pointimprovement vs. 16% and 7% respectively with placebo.
‡ In a 24-week, multicentre, randomized, double-blind, placebo-controlledtrial, 473 patients (MMSE 10-26) were randomized to receive ARICEPT5 mg/d, ARICEPT 10 mg/d or placebo. Following the 24-week,double-blind phase, all patients underwent a 6-week, single-blindplacebo washout. Patients treated with either dose of ARICEPTdemonstrated significantly less decline on the CIBIC-plus vs. placebo(CIBIC-plus value at endpoint for ARICEPT 5 mg/d and 10 mg/d were 4.15and 4.07 respectively vs. 4.51 with placebo, p=0.0047 and p<0.0001).
Nowindicatedfor severe
AD
CHOOSE ARICEPT®
Helping hermakeconnections1,2†‡
ARICEPT® Eisai Co. Ltd., owner/Pfizer Canada Inc., Licensee© 2007 Pfizer Canada Inc., Kirkland, Quebec H9J 2M5
26