«STEMI- Τρέχουσα θέση της...
89
Aθανάσιος Ν. Καρτάλης Επιμελητής Α΄ Καρδιολογική Κλινική Γ.Ν. Χίου Αμφιθέατρο Ελληνικής Καρδιολογικής Εταιρείας Παρασκευή 21 Ιουνίου 2013, Αθήνα «STEMI - Τρέχουσα θέση της Θρομβόλυσης»
Transcript of «STEMI- Τρέχουσα θέση της...
Aθανάσιος Ν. Καρτάλης
Επιμελητής Α΄
Καρδιολογική Κλινική Γ.Ν.
Χίου
Αμφιθέατρο
Ελληνικής Καρδιολογικής Εταιρείας
Παρασκευή 21 Ιουνίου 2013, Αθήνα
«STEMI - Τρέχουσα θέση της
Θρομβόλυσης»
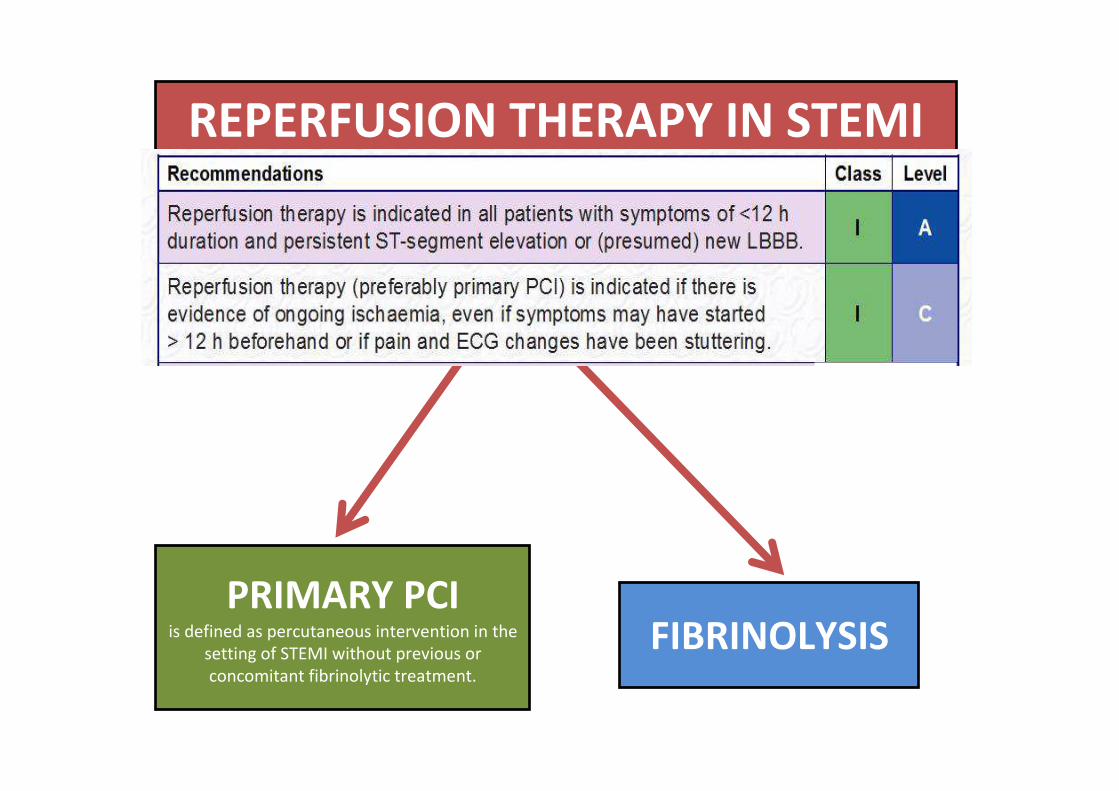
REPERFUSION THERAPY IN STEMI
PRIMARY PCI is defined as percutaneous intervention in the
setting of STEMI without previous or
concomitant fibrinolytic treatment.
FIBRINOLYSIS
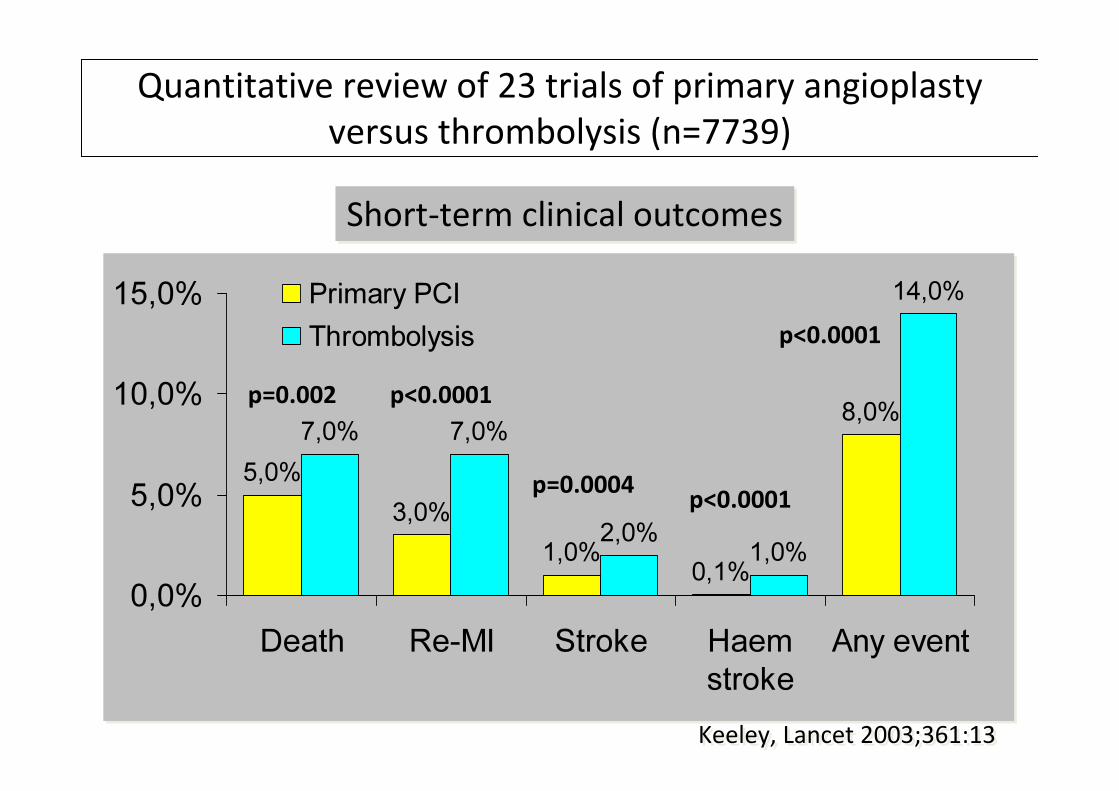
Quantitative review of 23 trials of primary angioplasty
versus thrombolysis (n=7739)
5,0%
3,0%
1,0%0,1%
8,0%7,0% 7,0%
2,0%1,0%
14,0%
0,0%
5,0%
10,0%
15,0%
Death Re-MI Stroke Haem
stroke
Any event
Primary PCI
Thrombolysis
Keeley, Lancet 2003;361:13Keeley, Lancet 2003;361:13
Short-term clinical outcomesShort-term clinical outcomes
p=0.002 p<0.0001
p=0.0004
p<0.0001
p<0.0001
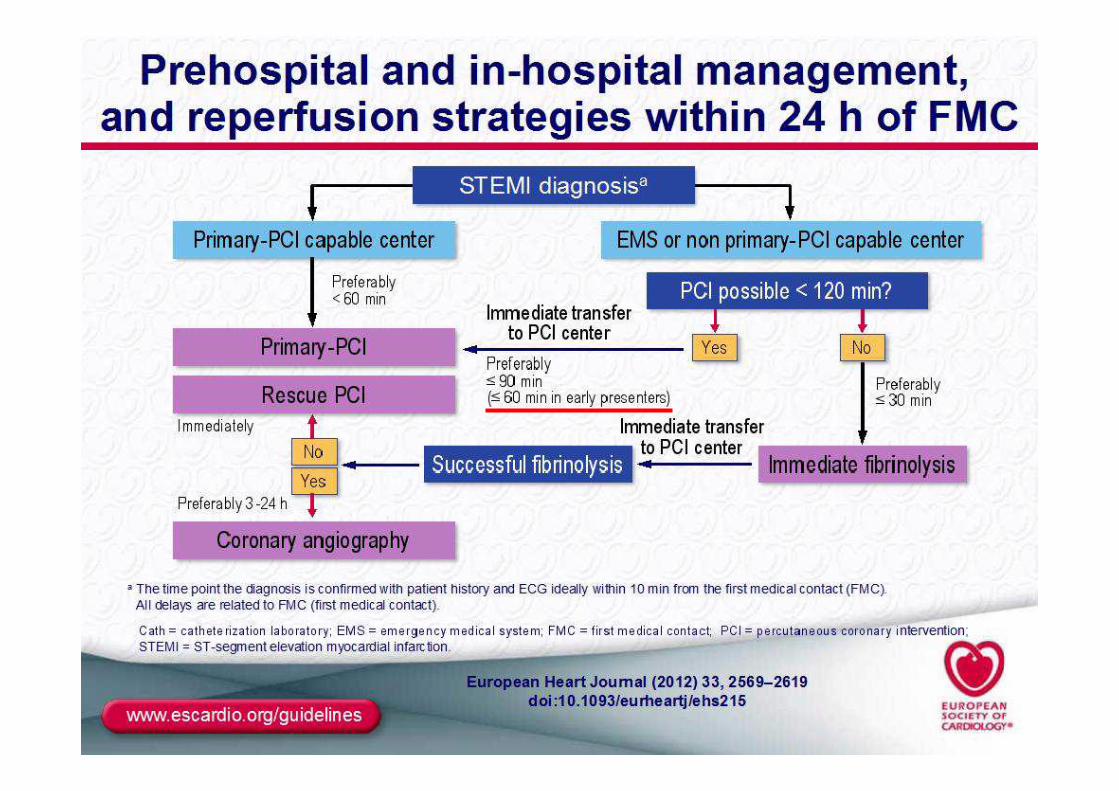
Reperfusion Therapy for Patients with STEMI
*Patients with cardiogenic shock or severe heart failure initially seen at a non–PCI-capable hospital should be transferred for cardiac catheterization and
revascularization as soon as possible, irrespective of time delay from MI onset (Class I, LOE: B). †Angiography and revascularization should not be performed
within the first 2 to 3 hours after administration of fibrinolytic therapy.
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
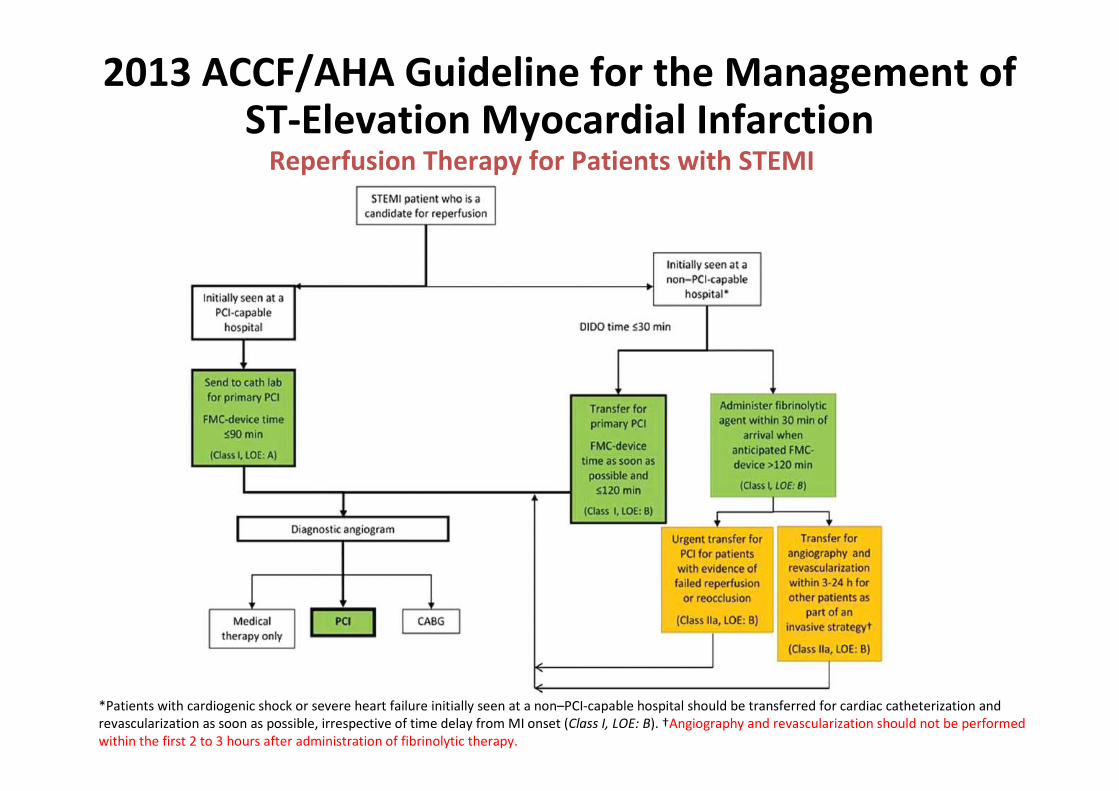
Time is Muscle
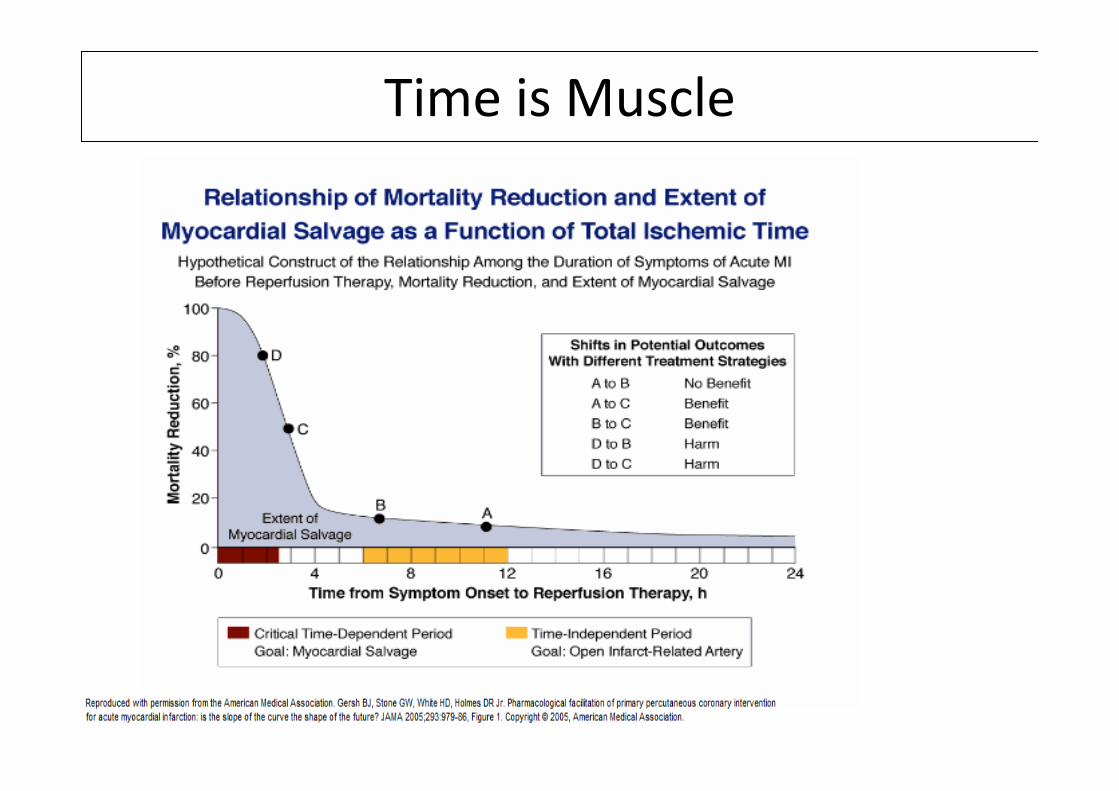
18% reduction
in mortality at 21 days
p=0.0002
GISSI trial
1986
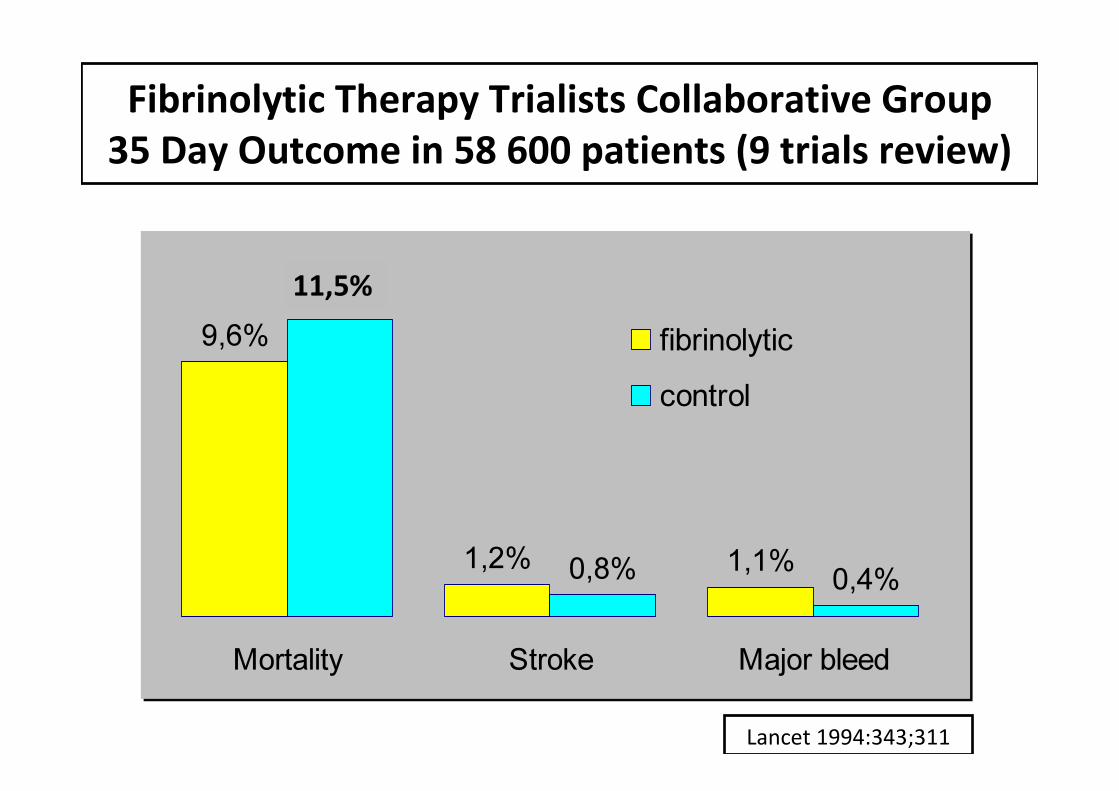
Fibrinolytic Therapy Trialists Collaborative Group
35 Day Outcome in 58 600 patients (9 trials review)
9,6%
1,2% 1,1%
11,2%
0,8% 0,4%
Mortality Stroke Major bleed
fibrinolytic
control
Lancet 1994:343;311
11,5%
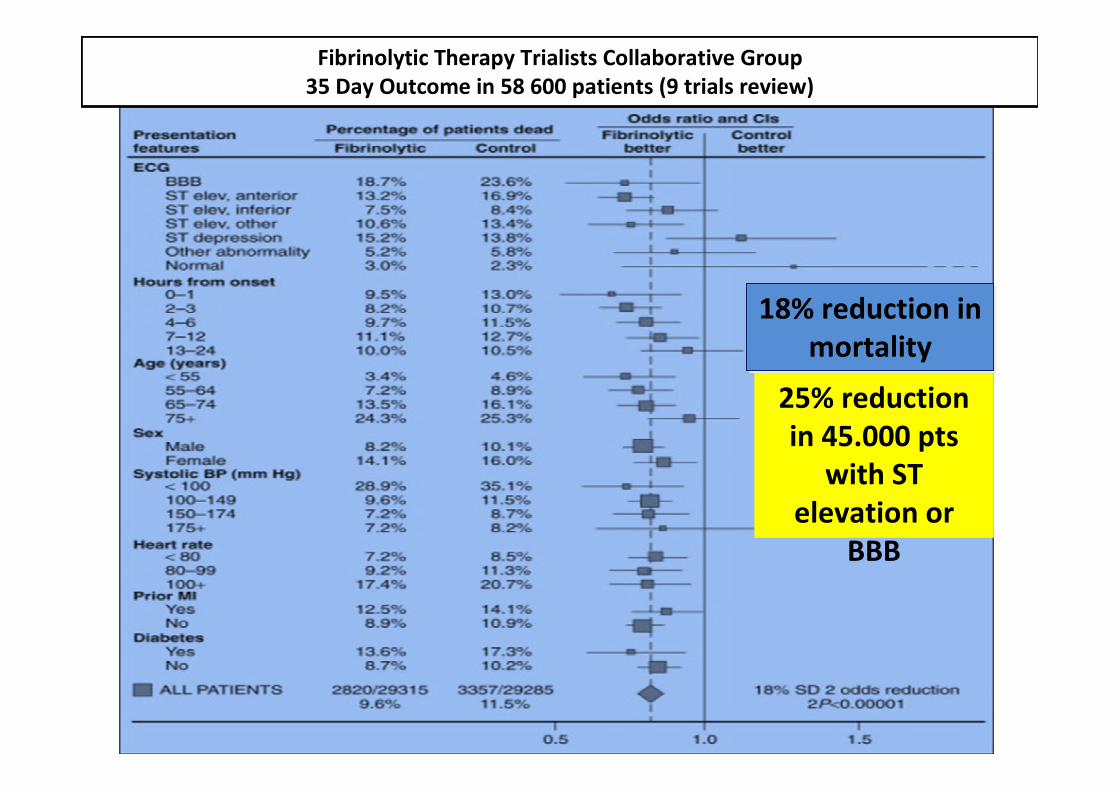
Fibrinolytic Therapy Trialists Collaborative Group
35 Day Outcome in 58 600 patients (9 trials review)
18% reduction in
mortality
18% reduction in
mortality
25% reduction
in 45.000 pts
with ST
elevation or
BBB
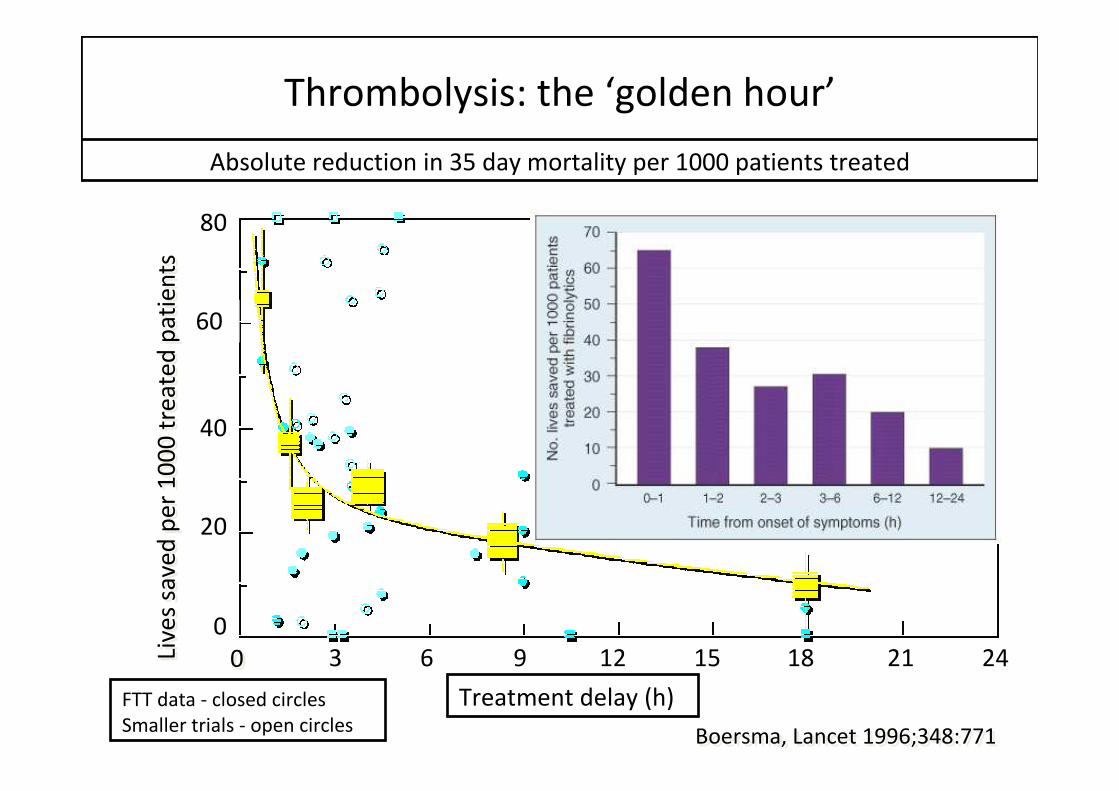
Thrombolysis: the ‘golden hour’
20
40
60
80
0
3 6 9 12 15 18 21 24
Treatment delay (h)
Absolute reduction in 35 day mortality per 1000 patients treated
FTT data - closed circles
Smaller trials - open circles
00
Boersma, Lancet 1996;348:771Boersma, Lancet 1996;348:771
Live
s sa
ve
d p
er
10
00
tre
ate
d p
ati
en
tsLi
ve
s sa
ve
d p
er
10
00
tre
ate
d p
ati
en
ts
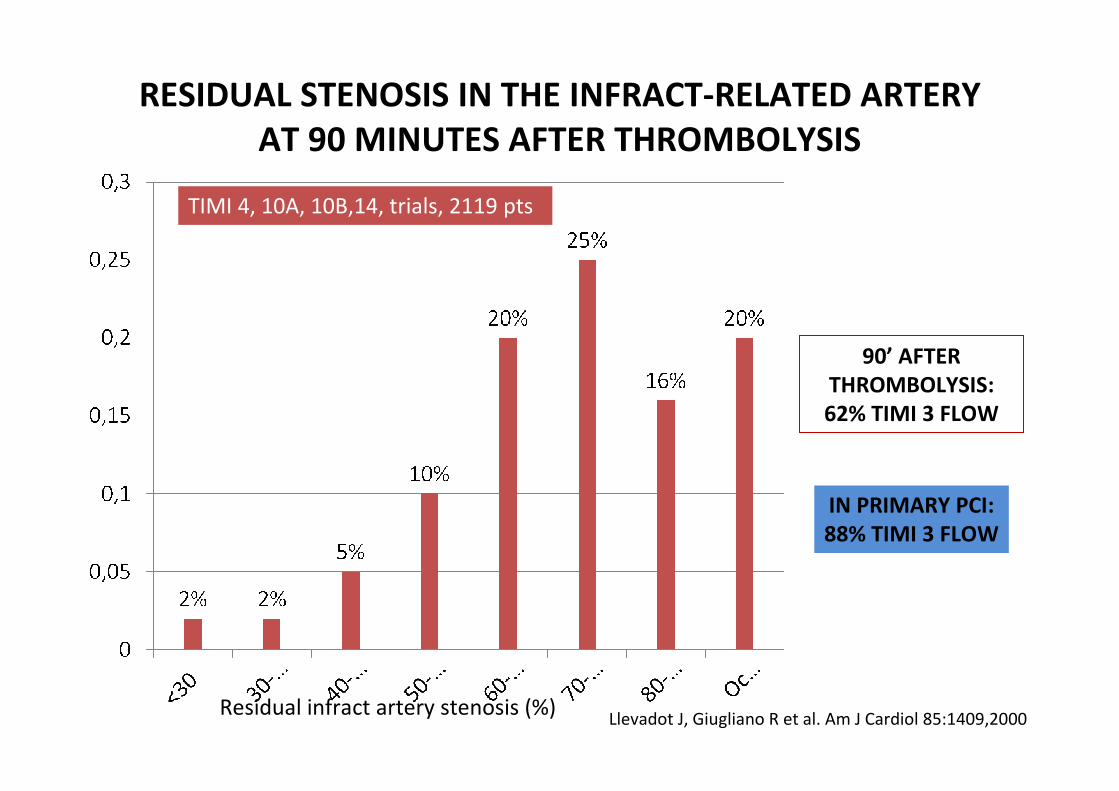
Residual infract artery stenosis (%)
TIMI 4, 10A, 10B,14, trials, 2119 pts
Llevadot J, Giugliano R et al. Am J Cardiol 85:1409,2000
RESIDUAL STENOSIS IN THE INFRACT-RELATED ARTERY
AT 90 MINUTES AFTER THROMBOLYSIS
90’ AFTER
THROMBOLYSIS:
62% TIMI 3 FLOW
IN PRIMARY PCI:
88% TIMI 3 FLOW
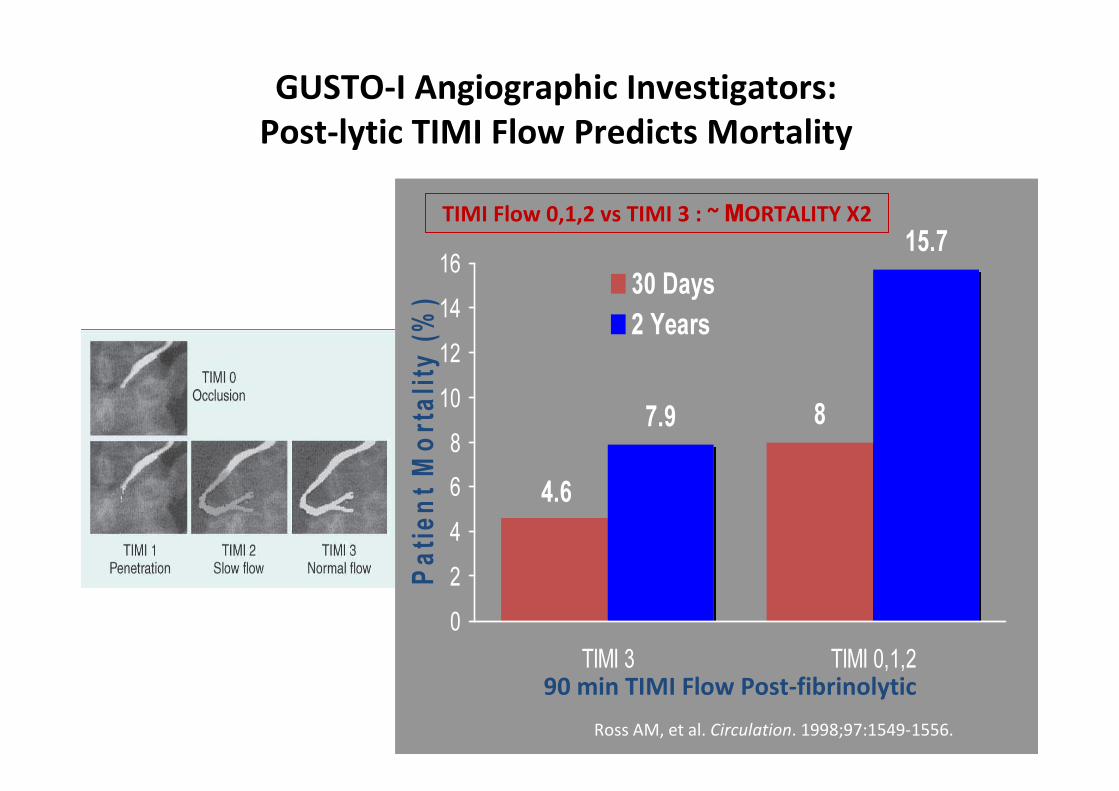
4.6
87.9
15.7
0
2
4
6
8
10
12
14
16
TIMI 3 TIMI 0,1,2
Pa
tie
nt
Mo
rta
lity
(%
) 30 Days
2 Years
Ross AM, et al. Circulation. 1998;97:1549-1556.
90 min TIMI Flow Post-fibrinolytic
GUSTO-I Angiographic Investigators:
Post-lytic TIMI Flow Predicts Mortality
TIMI Flow 0,1,2 vs TIMI 3 : ~ ΜORTALITY X2
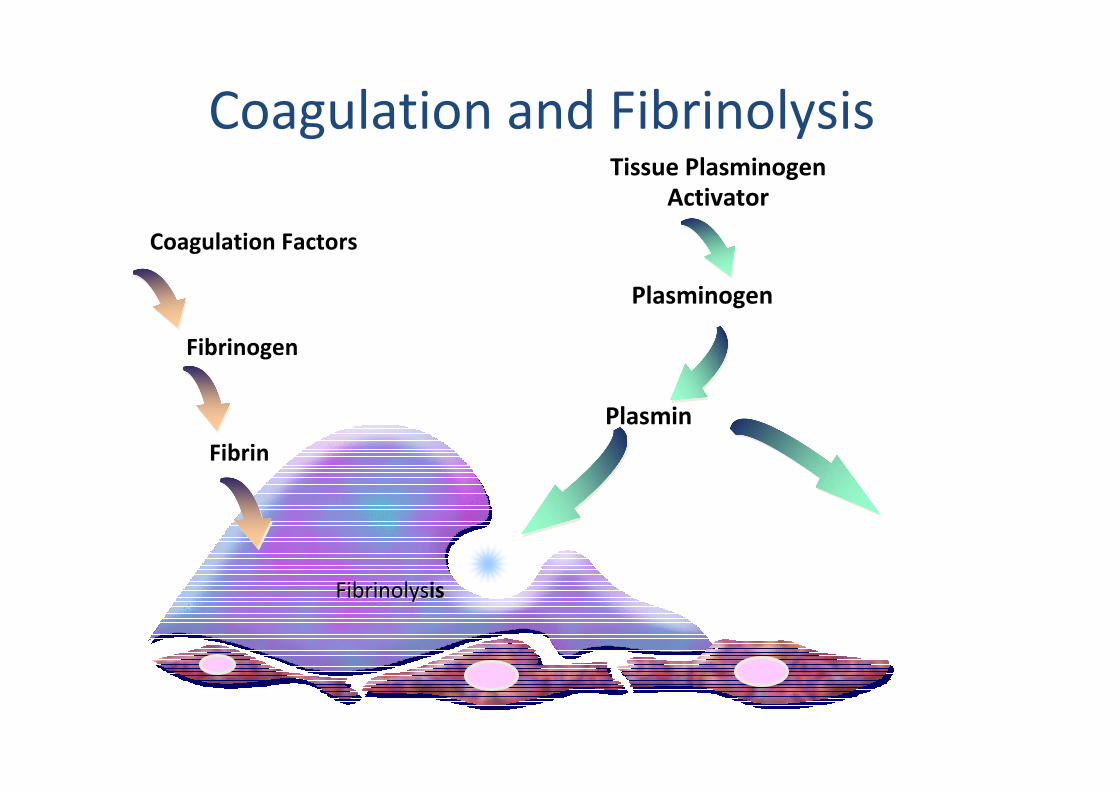
Coagulation and Fibrinolysis
FibrinolysFibrinolysisis
Fibrin
Coagulation Factors
Fibrinogen
Plasmin
Plasminogen
Tissue Plasminogen
Activator
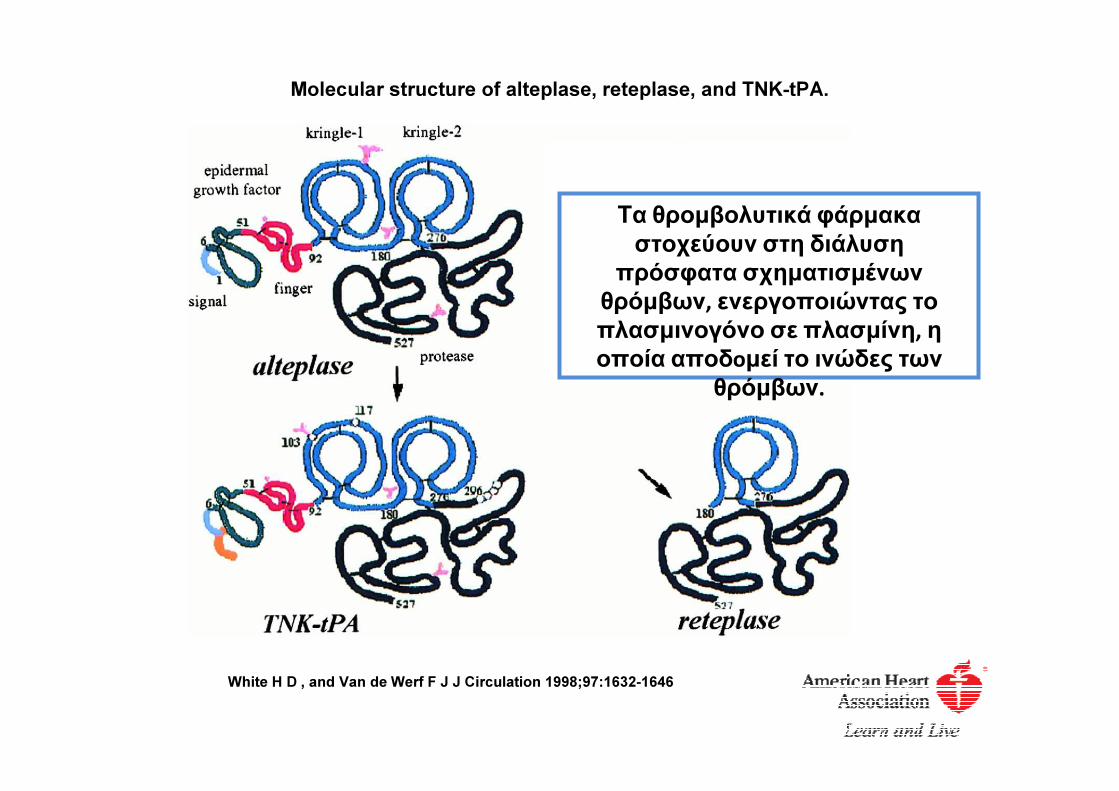
Molecular structure of alteplase, reteplase, and TNK-tPA.
White H D , and Van de Werf F J J Circulation 1998;97:1632-1646
Τα θρομβολυτικά φάρμακα
στοχεύουν στη διάλυση
πρόσφατα σχηματισμένων
θρόμβων, ενεργοποιώντας το
πλασμινογόνο σε πλασμίνη, η
οποία αποδoμεί το ινώδες των
θρόμβων.
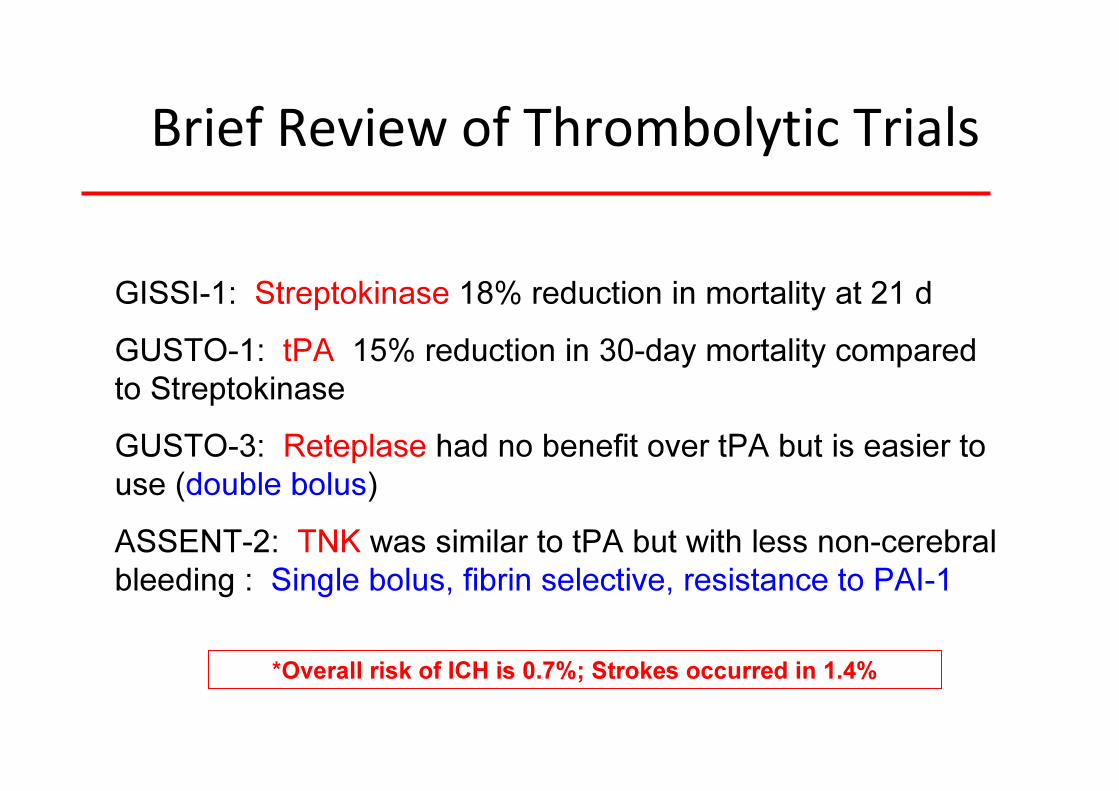
Brief Review of Thrombolytic Trials
GISSI-1: Streptokinase 18% reduction in mortality at 21 d
GUSTO-1: tPA 15% reduction in 30-day mortality compared
to Streptokinase
GUSTO-3: Reteplase had no benefit over tPA but is easier to
use (double bolus)
ASSENT-2: TNK was similar to tPA but with less non-cerebral
bleeding : Single bolus, fibrin selective, resistance to PAI-1
*Overall risk of ICH is 0.7%; Strokes occurred in 1.4%
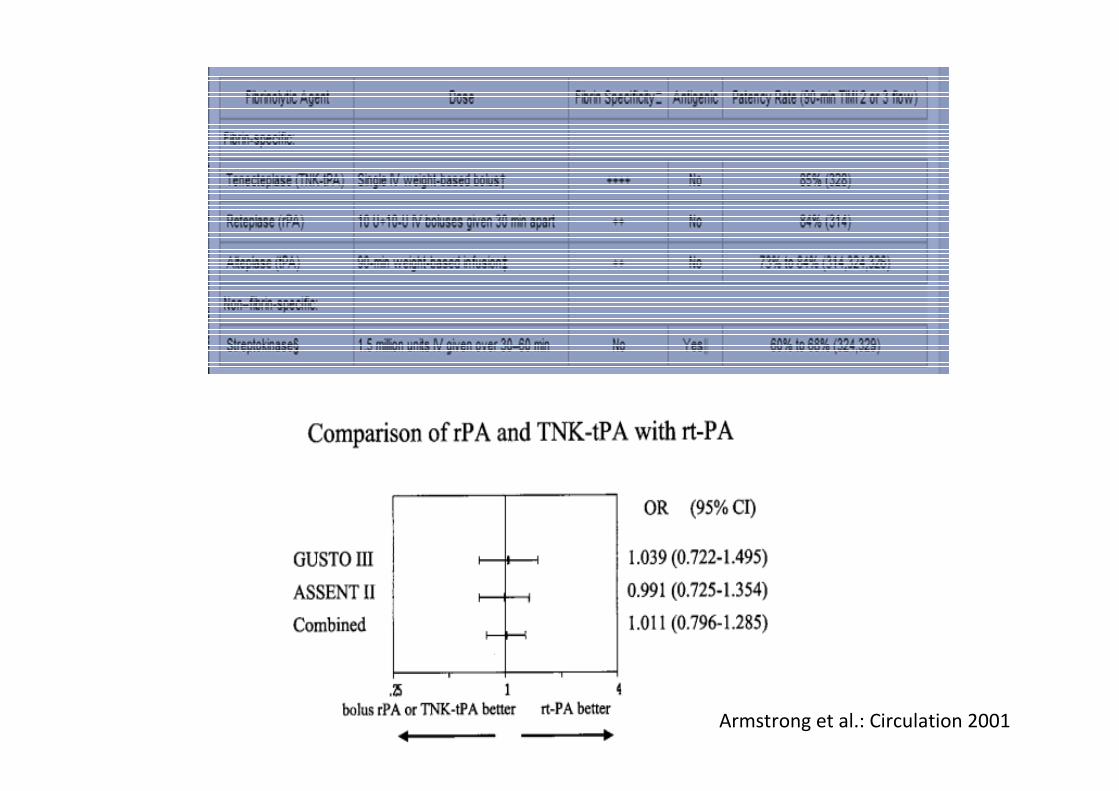
Armstrong et al.: Circulation 2001
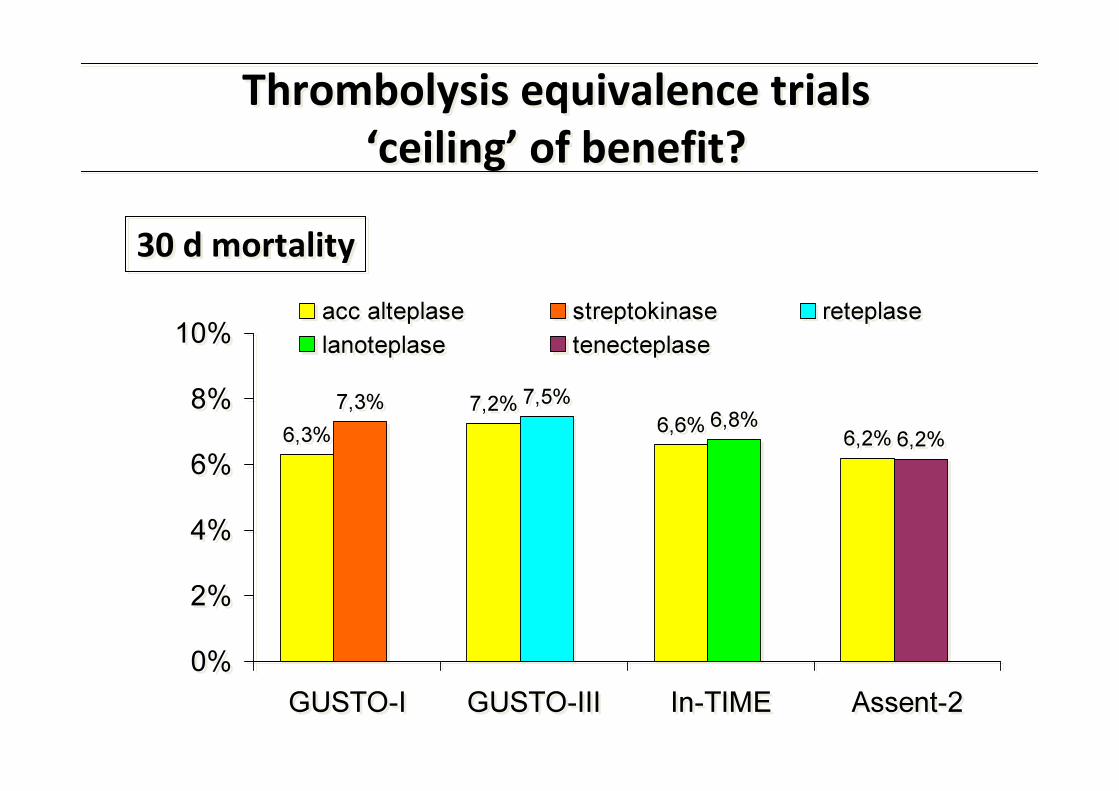
Thrombolysis equivalence trials
‘ceiling’ of benefit?
Thrombolysis equivalence trials
‘ceiling’ of benefit?
6,3%
7,2%6,6%
6,2%
7,3% 7,5%6,8%
6,2%
0%
2%
4%
6%
8%
10%
GUSTO-I GUSTO-III In-TIME Assent-2
acc alteplase streptokinase reteplase
lanoteplase tenecteplase
6,3%
7,2%6,6%
6,2%
7,3% 7,5%6,8%
6,2%
0%
2%
4%
6%
8%
10%
GUSTO-I GUSTO-III In-TIME Assent-2
acc alteplase streptokinase reteplase
lanoteplase tenecteplase
30 d mortality30 d mortality
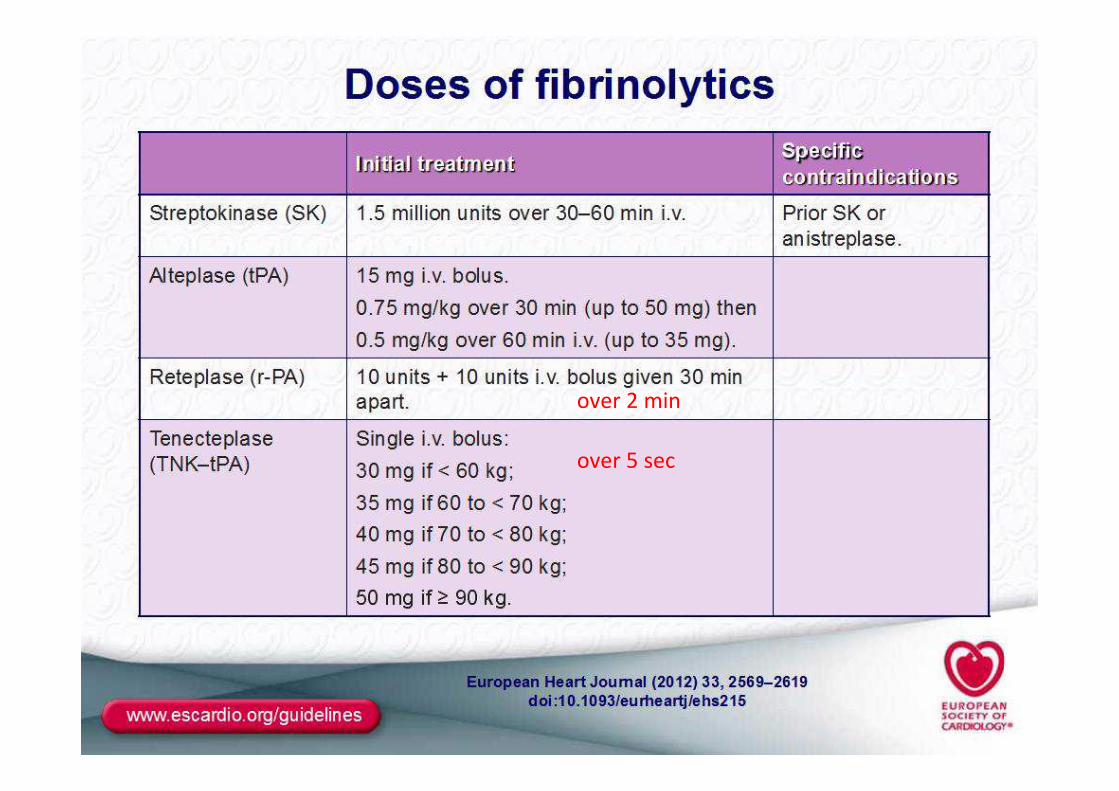
over 5 sec
over 2 min
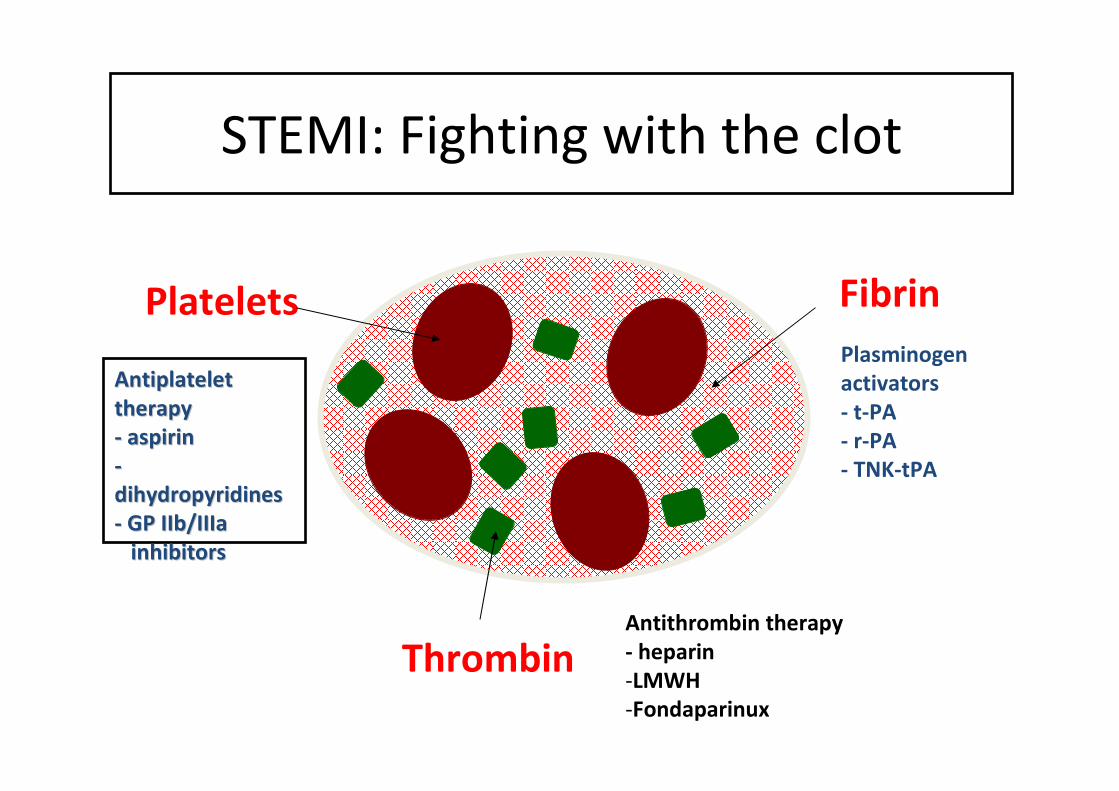
Platelets
Antiplatelet Antiplatelet
therapytherapy
-- aspirinaspirin
--
dihydropyridinesdihydropyridines
-- GP IIb/IIIaGP IIb/IIIa
inhibitorsinhibitors
Fibrin
Plasminogen
activators
- t-PA
- r-PA
- TNK-tPA
ThrombinAntithrombin therapy
- heparin
-LMWH
-Fondaparinux
STEMI: Fighting with the clot
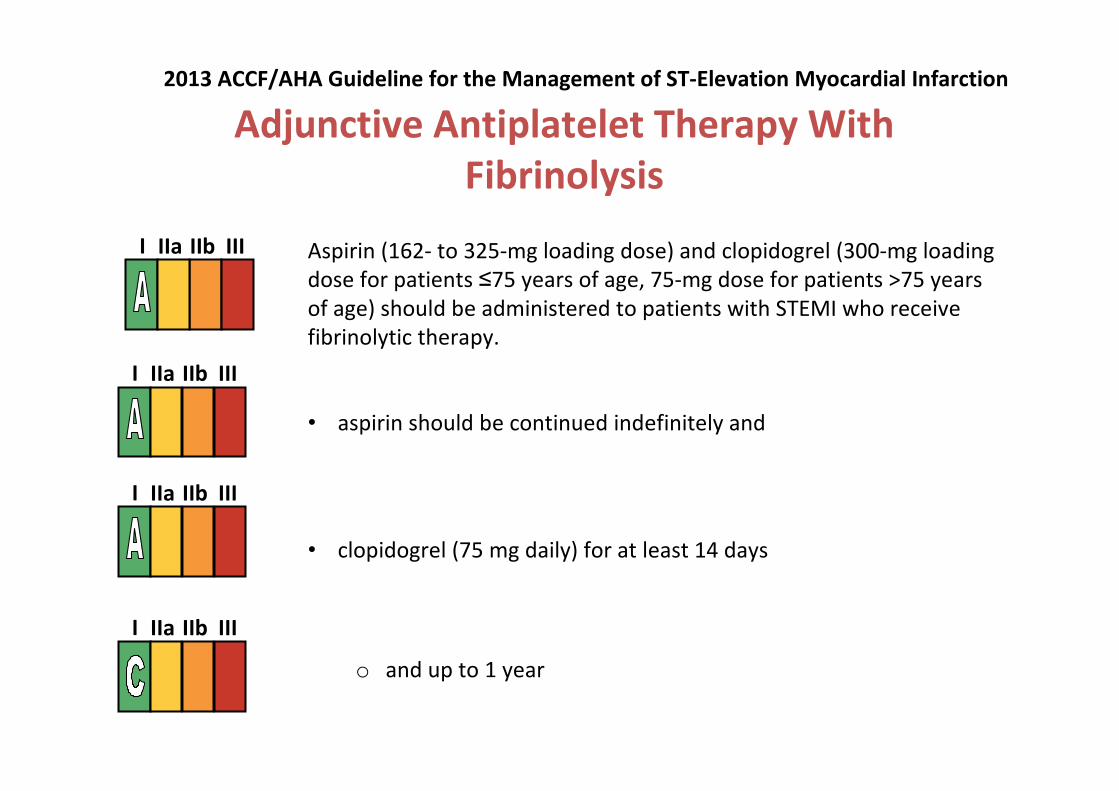
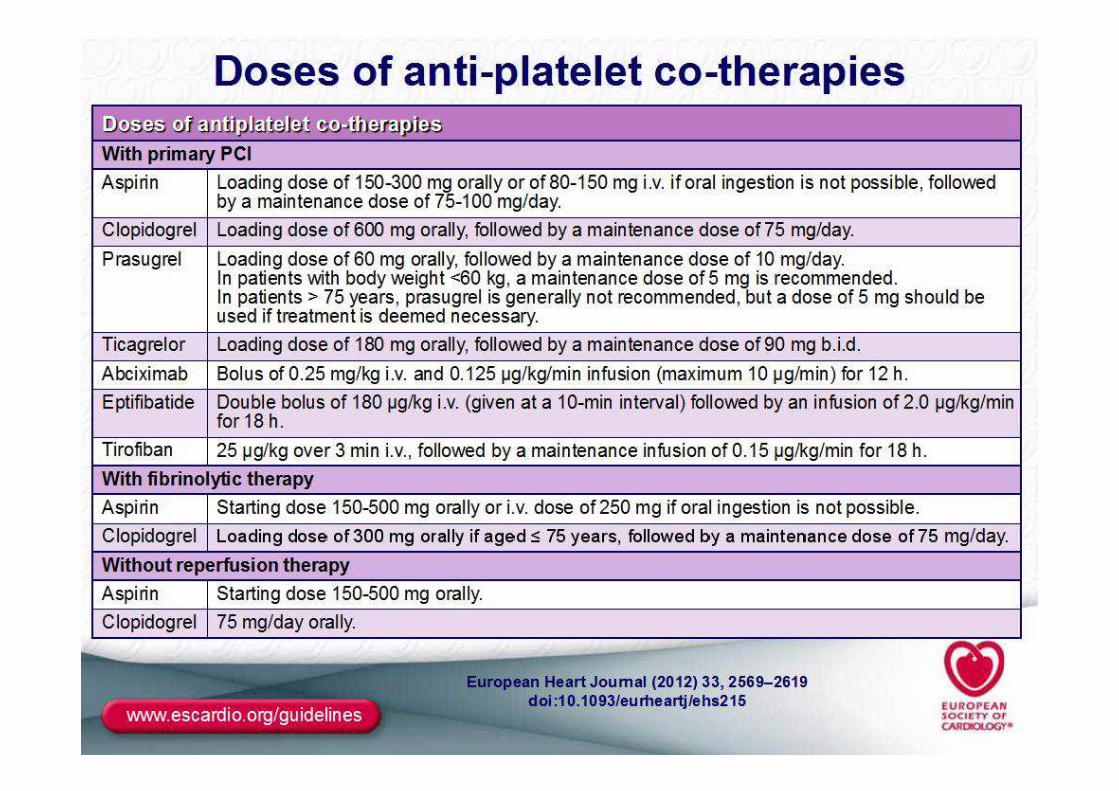
Adjunctive Antiplatelet Therapy With
Fibrinolysis
Aspirin (162- to 325-mg loading dose) and clopidogrel (300-mg loading
dose for patients ≤75 years of age, 75-mg dose for patients >75 years
of age) should be administered to patients with STEMI who receive
fibrinolytic therapy.
I IIa IIb III
• aspirin should be continued indefinitely and
I IIa IIb III
• clopidogrel (75 mg daily) for at least 14 days
o and up to 1 year
I IIa IIb III
I IIa IIb III
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
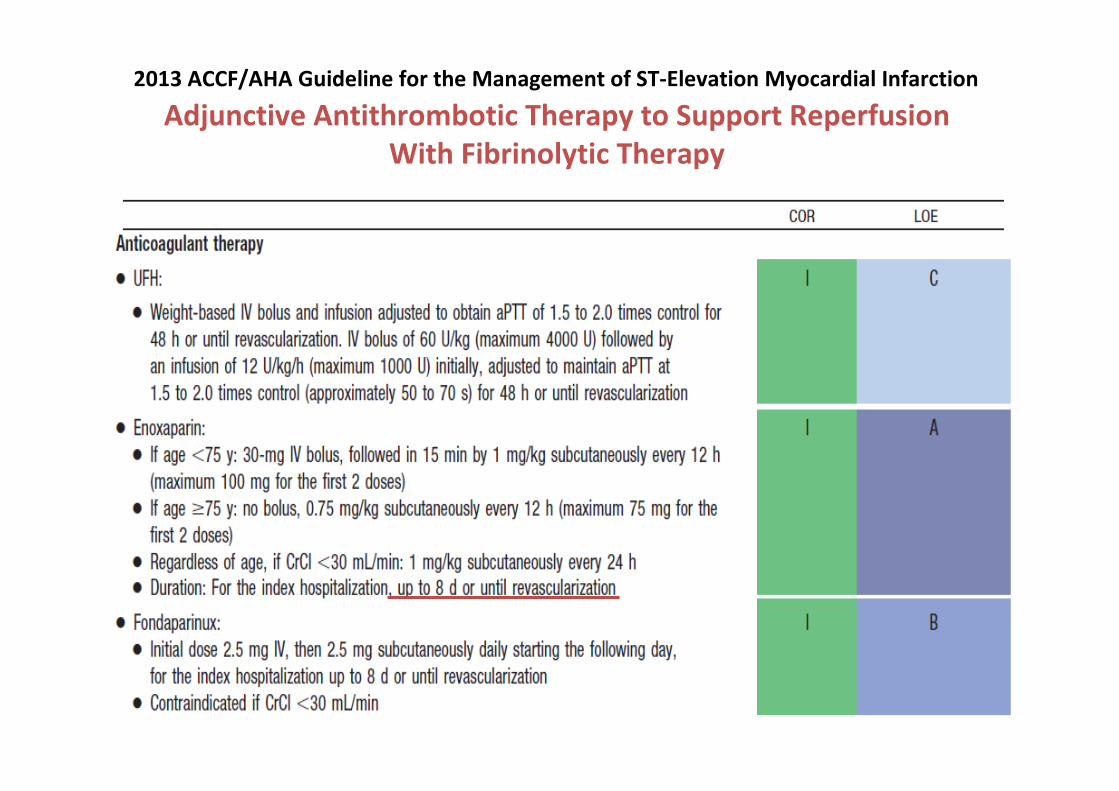
Adjunctive Antithrombotic Therapy to Support Reperfusion
With Fibrinolytic Therapy
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
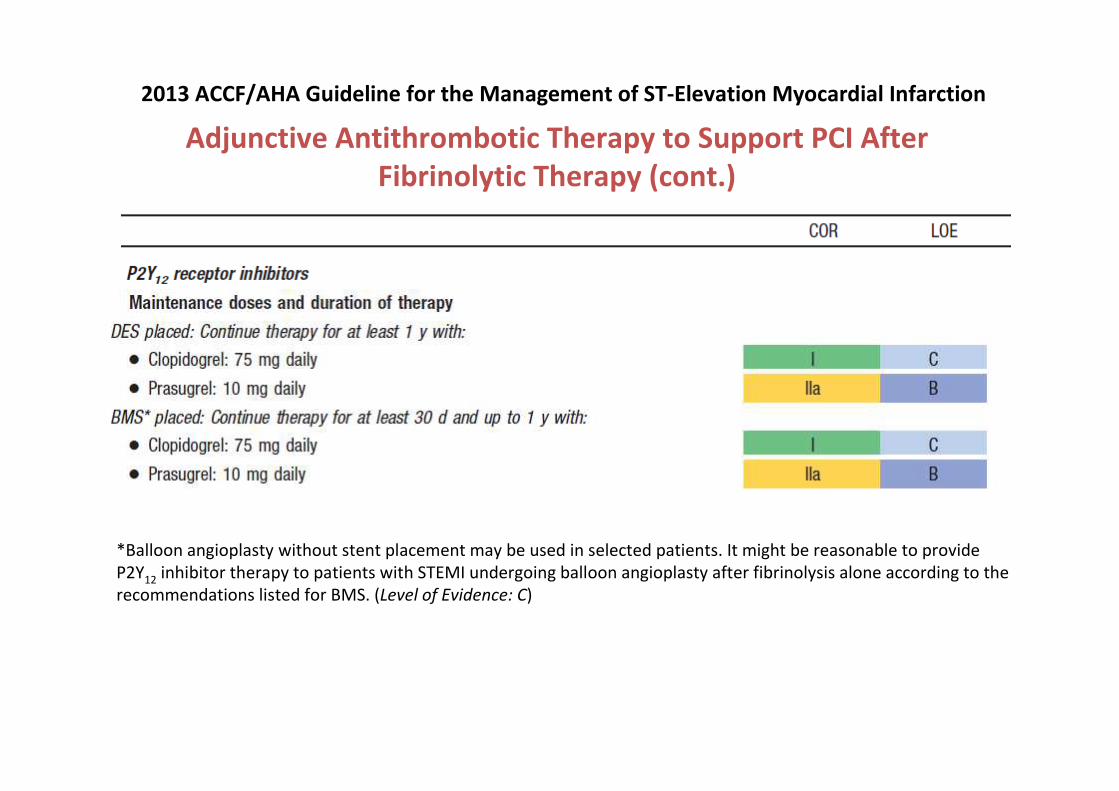
Adjunctive Antithrombotic Therapy to Support PCI After
Fibrinolytic Therapy (cont.)
*Balloon angioplasty without stent placement may be used in selected patients. It might be reasonable to provide
P2Y12
inhibitor therapy to patients with STEMI undergoing balloon angioplasty after fibrinolysis alone according to the
recommendations listed for BMS. (Level of Evidence: C)
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
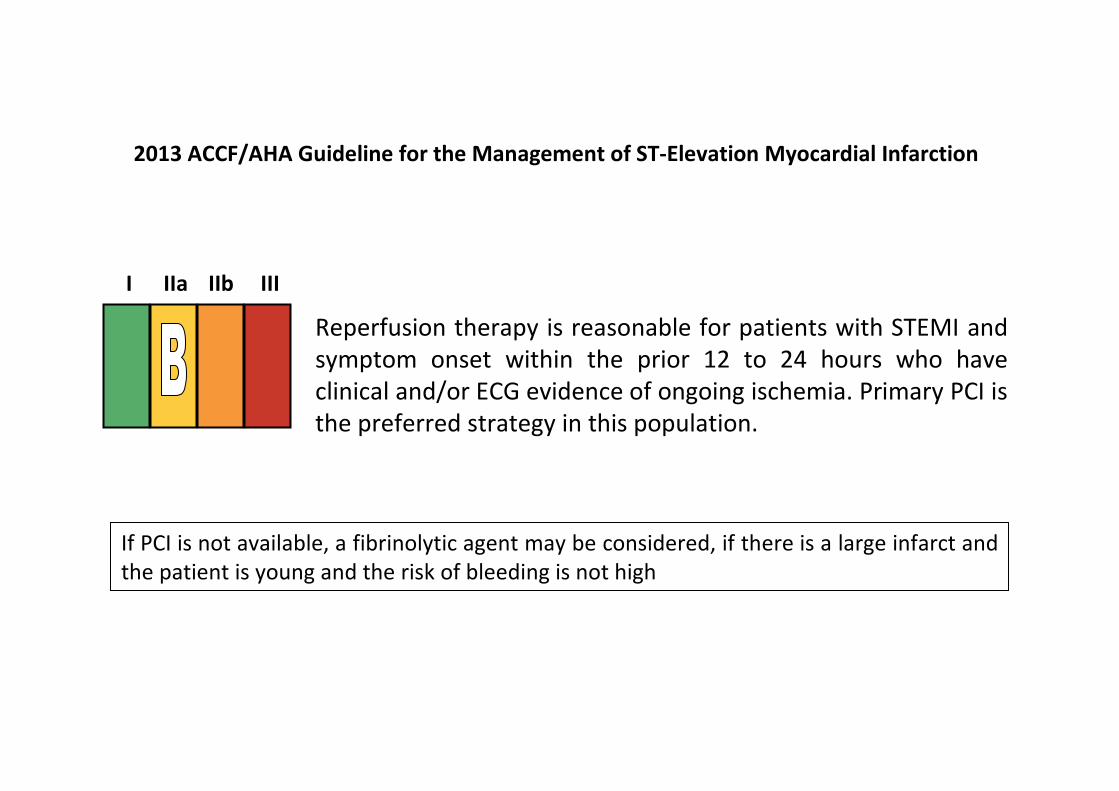
Reperfusion therapy is reasonable for patients with STEMI and
symptom onset within the prior 12 to 24 hours who have
clinical and/or ECG evidence of ongoing ischemia. Primary PCI is
the preferred strategy in this population.
I IIa IIb III
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
If PCI is not available, a fibrinolytic agent may be considered, if there is a large infarct and
the patient is young and the risk of bleeding is not high
10,711,8
4,3
14,615,7
6,5
2,7
7,8
0
5
10
15
20
Mortality ReMI Major Bleed Minor Bleed
Repeat fibrinolysis Conservative treatment
10,711,8
4,3
14,615,7
6,5
2,7
7,8
0
5
10
15
20
Mortality ReMI Major Bleed Minor Bleed
Repeat fibrinolysis Conservative treatment
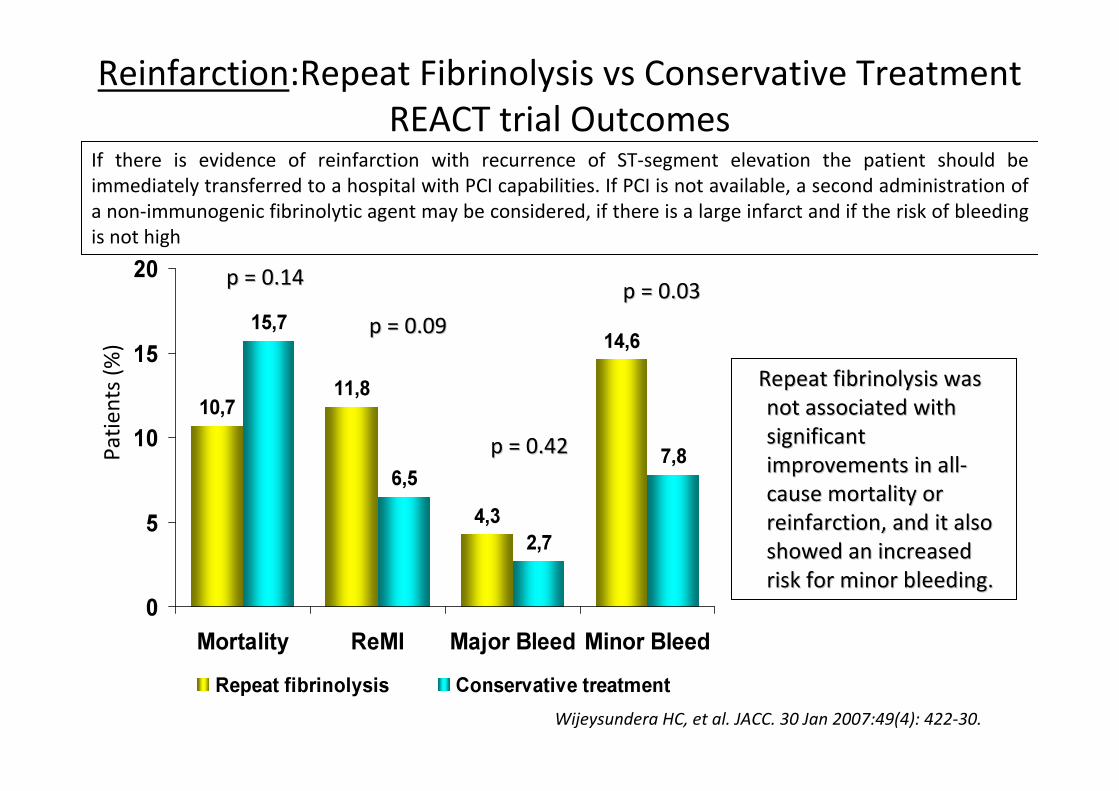
p = 0.14p = 0.14
p = 0.09p = 0.09
p = 0.03p = 0.03
Repeat fibrinolysis was Repeat fibrinolysis was
not associated with not associated with
significant significant
improvements in allimprovements in all--
cause mortality or cause mortality or
reinfarction, and it also reinfarction, and it also
showed an increased showed an increased
risk for minor bleeding.risk for minor bleeding.
Reinfarction:Repeat Fibrinolysis vs Conservative Treatment
REACT trial Outcomes
Wijeysundera HC, et al. JACC. 30 Jan 2007:49(4): 422-30.Wijeysundera HC, et al. JACC. 30 Jan 2007:49(4): 422-30.
Pa
tie
nts
(%
)
p = 0.42p = 0.42
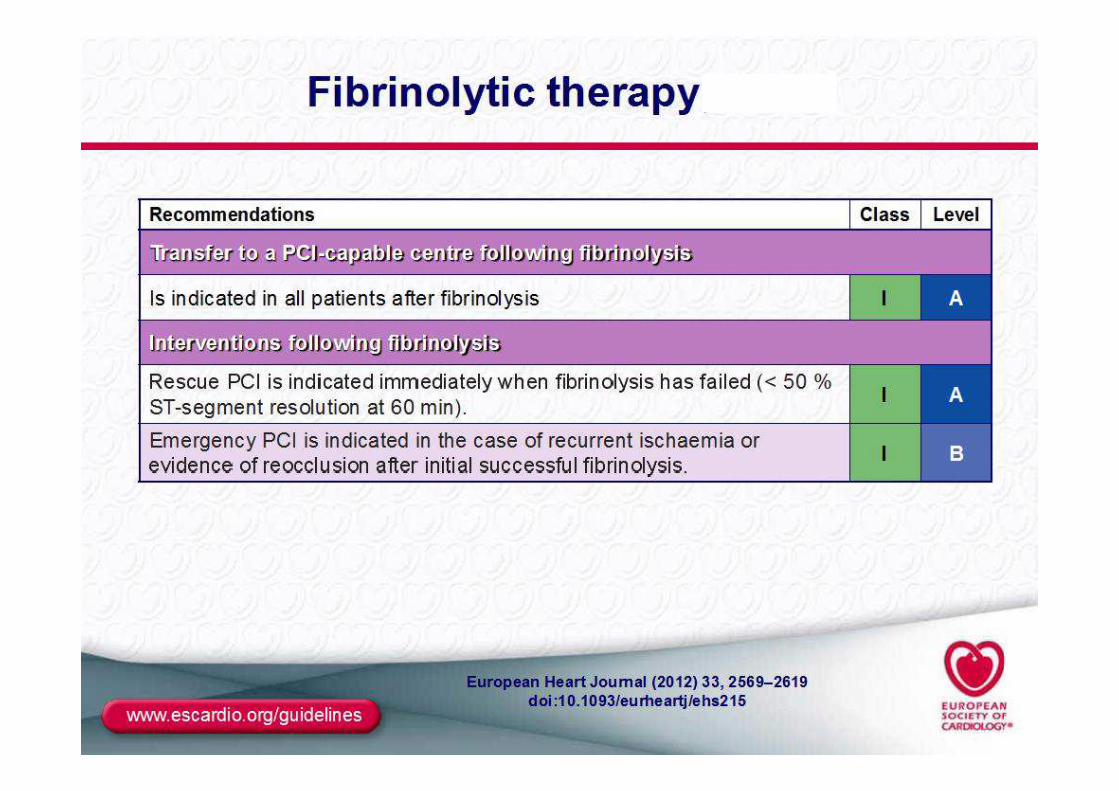
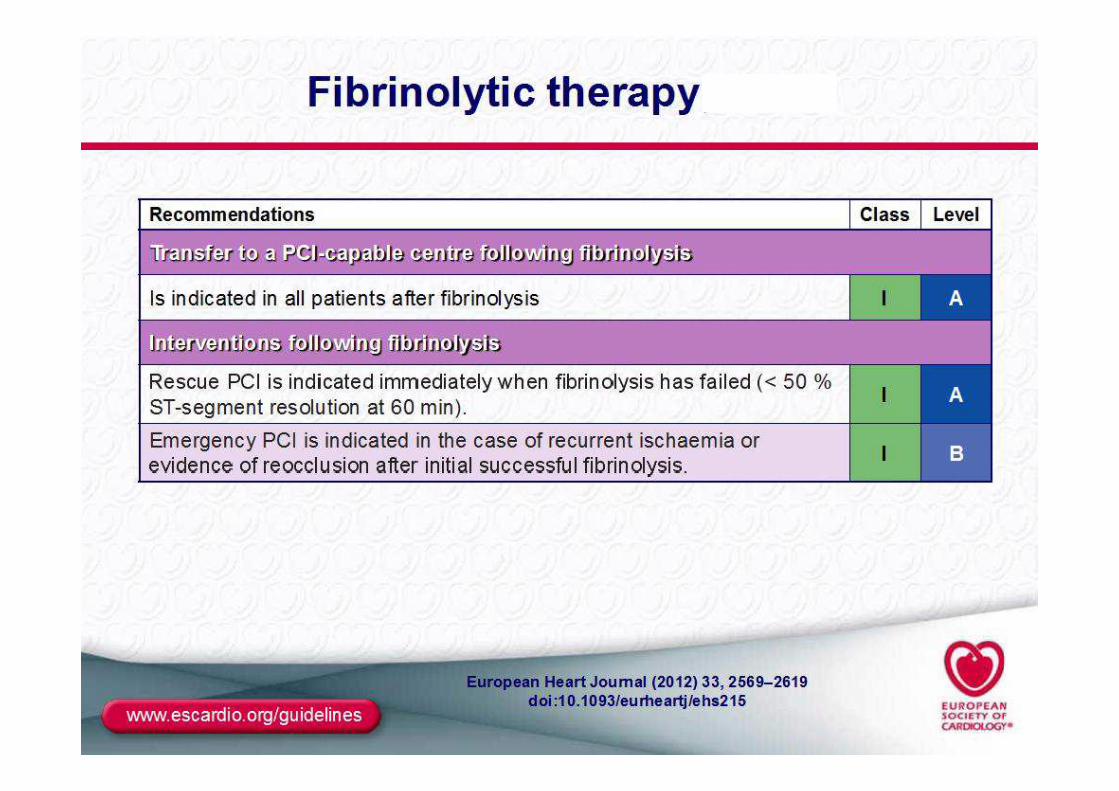
If there is evidence of reinfarction with recurrence of ST-segment elevation the patient should be
immediately transferred to a hospital with PCI capabilities. If PCI is not available, a second administration of
a non-immunogenic fibrinolytic agent may be considered, if there is a large infarct and if the risk of bleeding
is not high
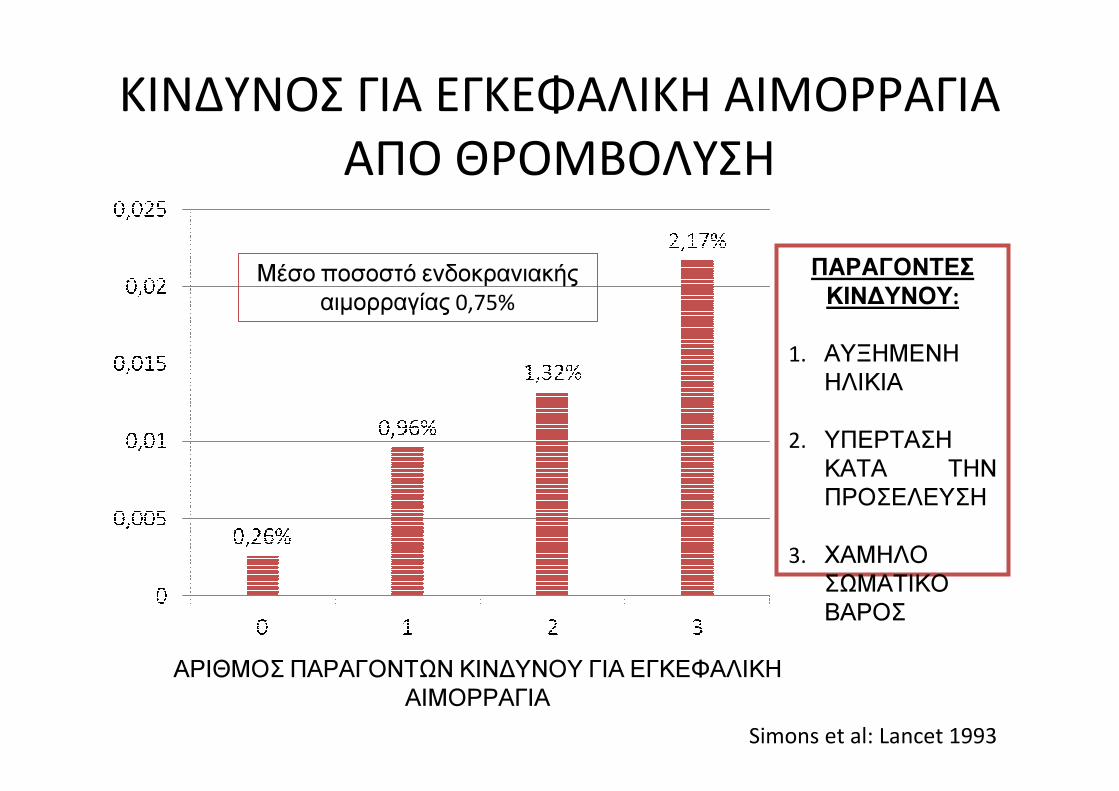
ΚΙΝΔΥΝΟΣ ΓΙΑ ΕΓΚΕΦΑΛΙΚΗ ΑΙΜΟΡΡΑΓΙΑ
ΑΠΟ ΘΡΟΜΒΟΛΥΣΗ
ΑΡΙΘΜΟΣ ΠΑΡΑΓΟΝΤΩΝ ΚΙΝΔΥΝΟΥ ΓΙΑ ΕΓΚΕΦΑΛΙΚΗ
ΑΙΜΟΡΡΑΓΙΑ
Simons et al: Lancet 1993
ΠΑΡΑΓΟΝΤΕΣ
ΚΙΝΔΥΝΟΥ:
1. ΑΥΞΗΜΕΝΗ
ΗΛΙΚΙΑ
2. ΥΠΕΡΤΑΣΗ
ΚΑΤΑ ΤΗΝ
ΠΡΟΣΕΛΕΥΣΗ
3. ΧΑΜΗΛΟ
ΣΩΜΑΤΙΚΟ
ΒΑΡΟΣ
Μέσο ποσοστό ενδοκρανιακής
αιμορραγίας 0,75%
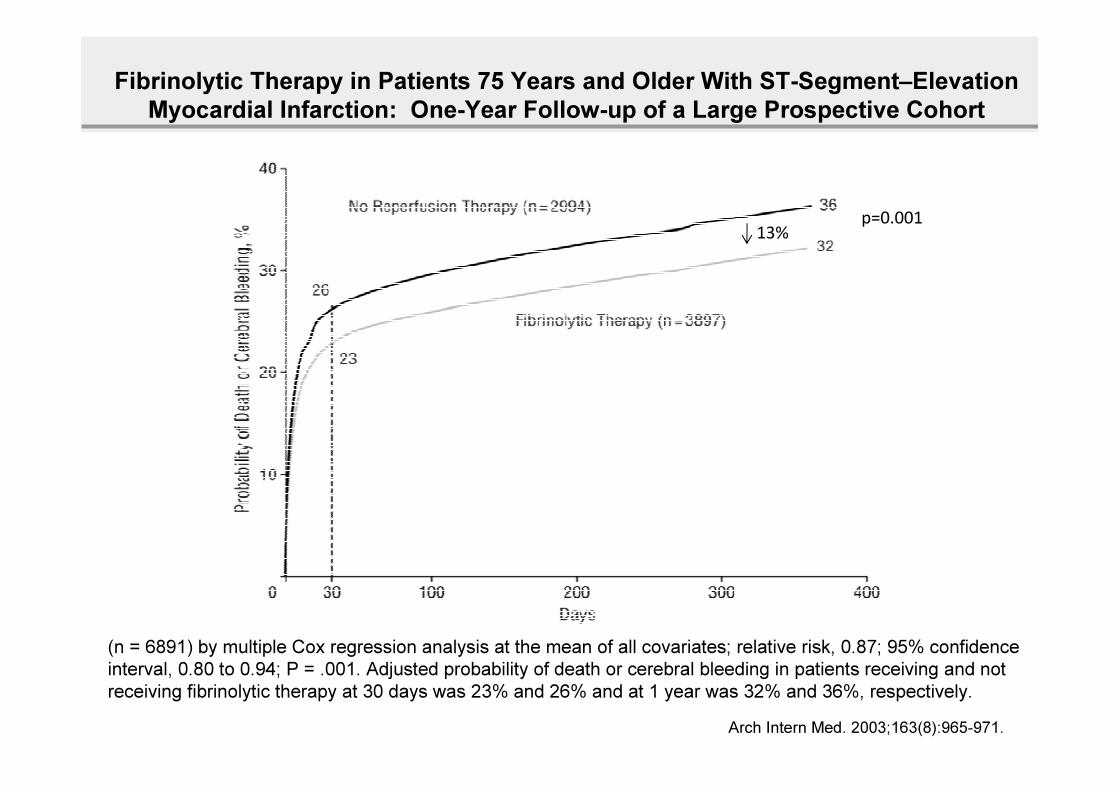
Fibrinolytic Therapy in Patients 75 Years and Older With ST-Segment–Elevation
Myocardial Infarction: One-Year Follow-up of a Large Prospective Cohort
Arch Intern Med. 2003;163(8):965-971.
(n = 6891) by multiple Cox regression analysis at the mean of all covariates; relative risk, 0.87; 95% confidence
interval, 0.80 to 0.94; P = .001. Adjusted probability of death or cerebral bleeding in patients receiving and not
receiving fibrinolytic therapy at 30 days was 23% and 26% and at 1 year was 32% and 36%, respectively.
p=0.00113%
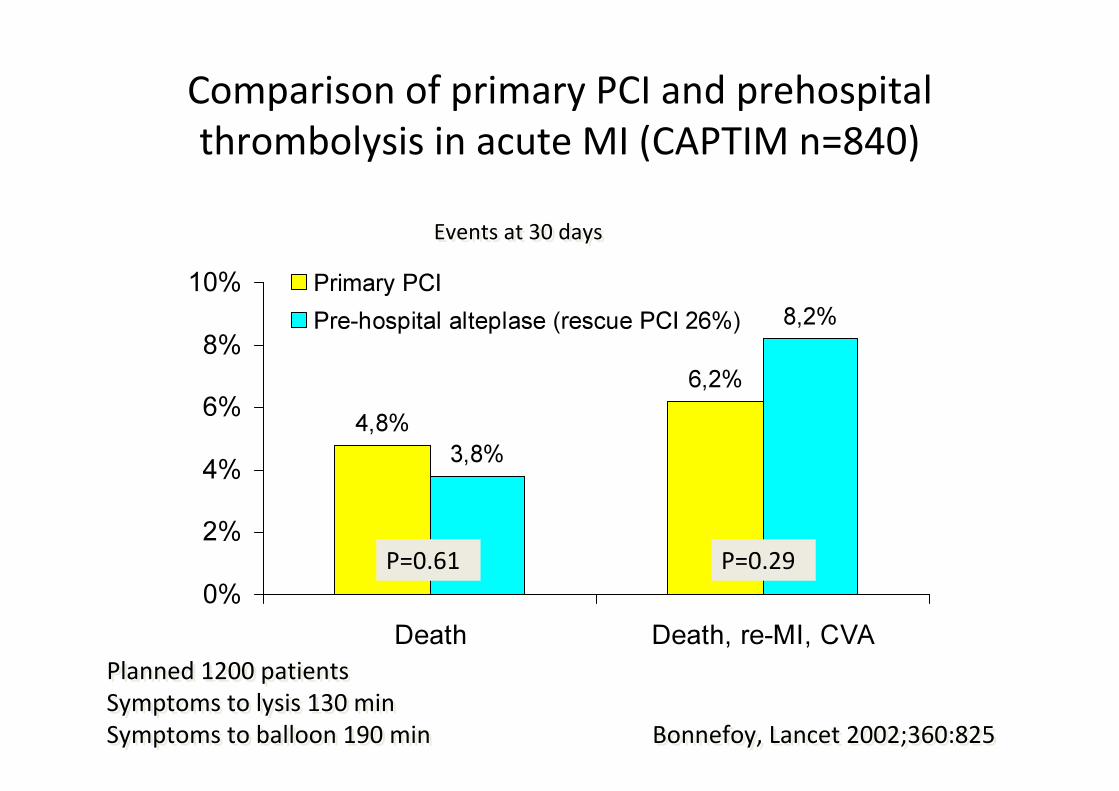
Comparison of primary PCI and prehospital
thrombolysis in acute MI (CAPTIM n=840)
4,8%
6,2%
3,8%
8,2%
0%
2%
4%
6%
8%
10%
Death Death, re-MI, CVA
Primary PCI
Pre-hospital alteplase (rescue PCI 26%)
Bonnefoy, Lancet 2002;360:825Bonnefoy, Lancet 2002;360:825
Events at 30 daysEvents at 30 days
Planned 1200 patients
Symptoms to lysis 130 min
Symptoms to balloon 190 min
Planned 1200 patients
Symptoms to lysis 130 min
Symptoms to balloon 190 min
P=0.61 P=0.29
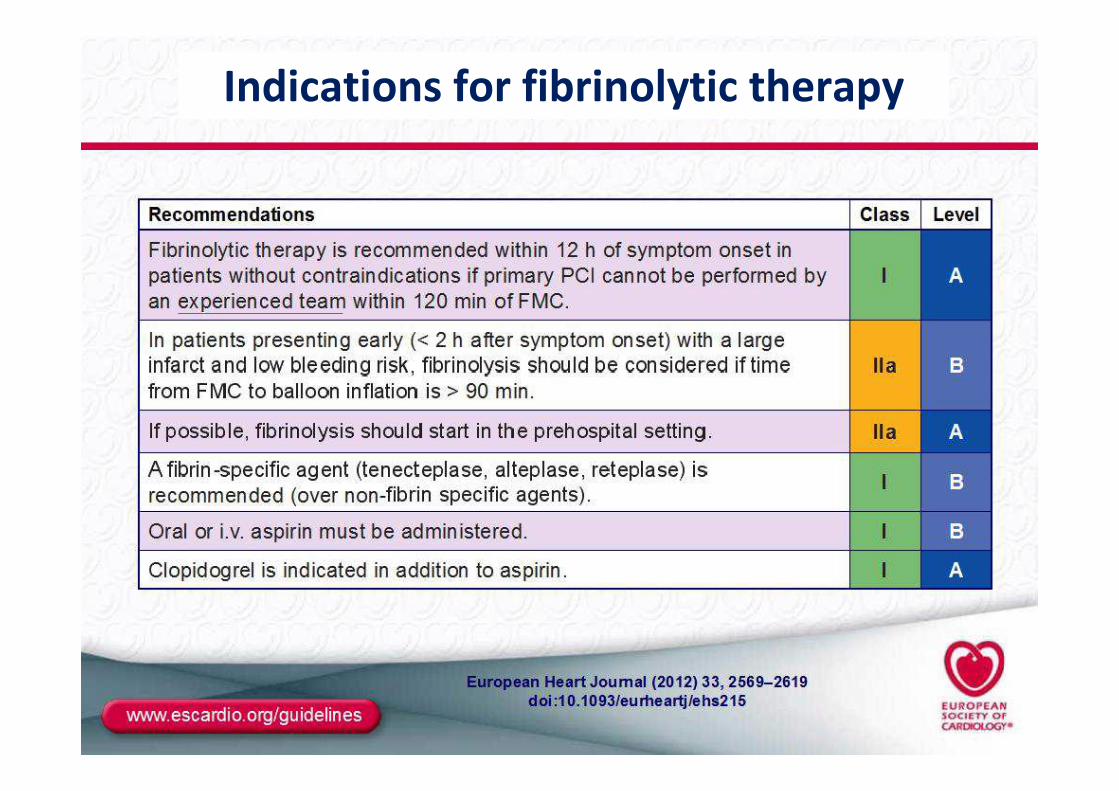
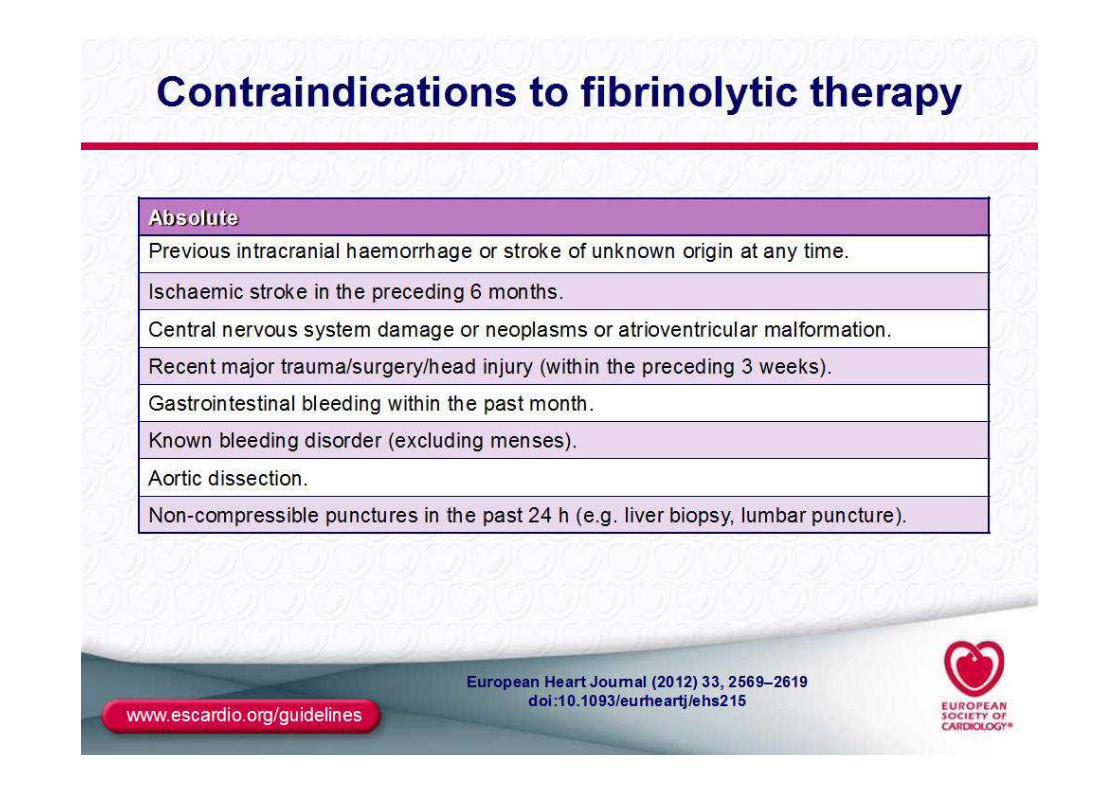
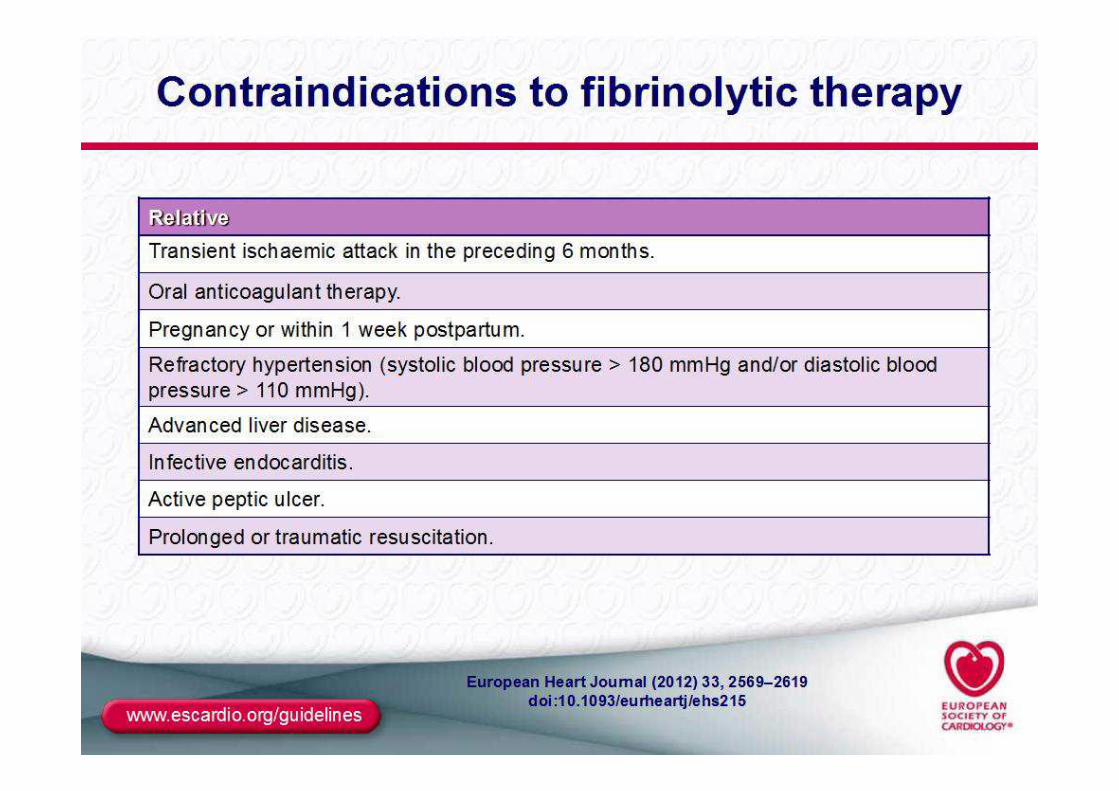
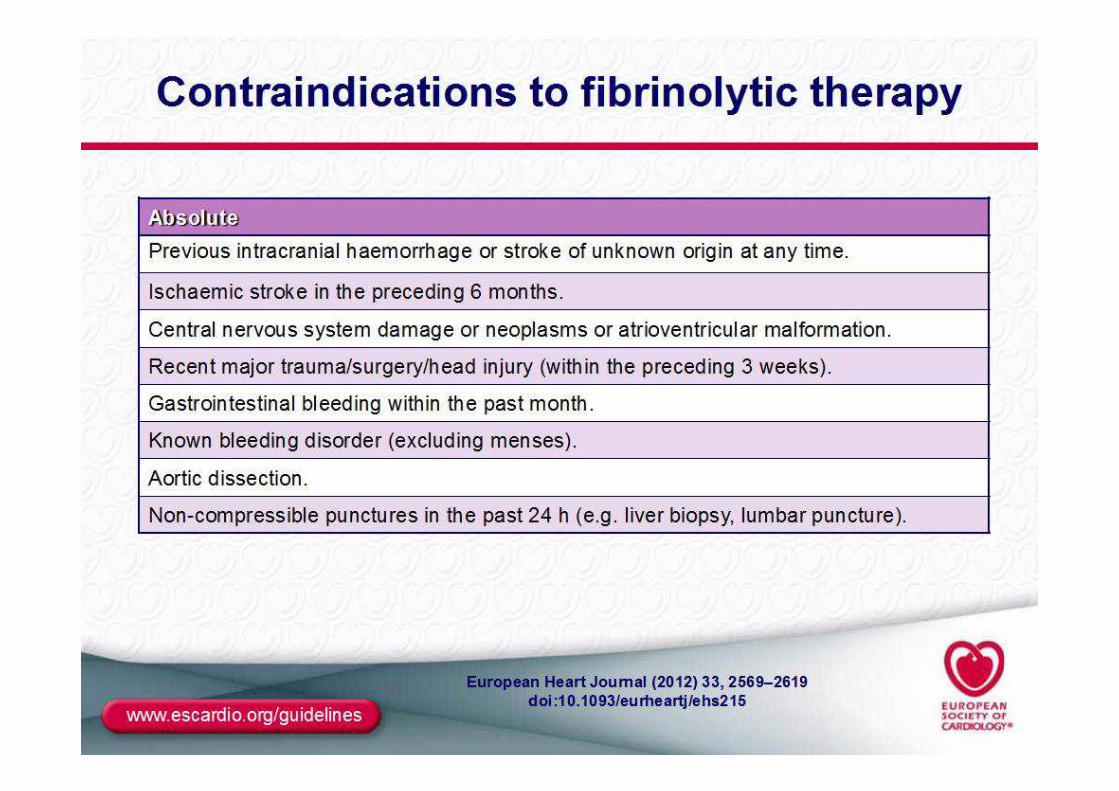
Indications for fibrinolytic therapy
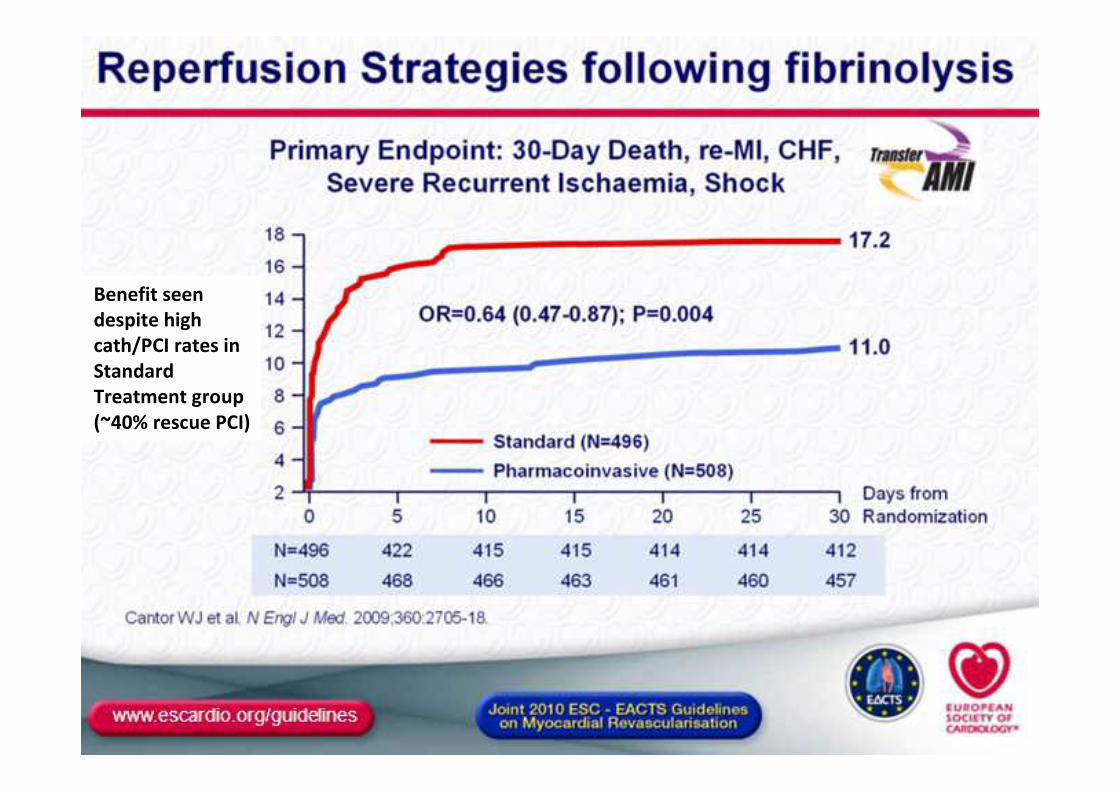
Benefit seen
despite high
cath/PCI rates in
Standard
Treatment group
(~40% rescue PCI)
ACC, 2013
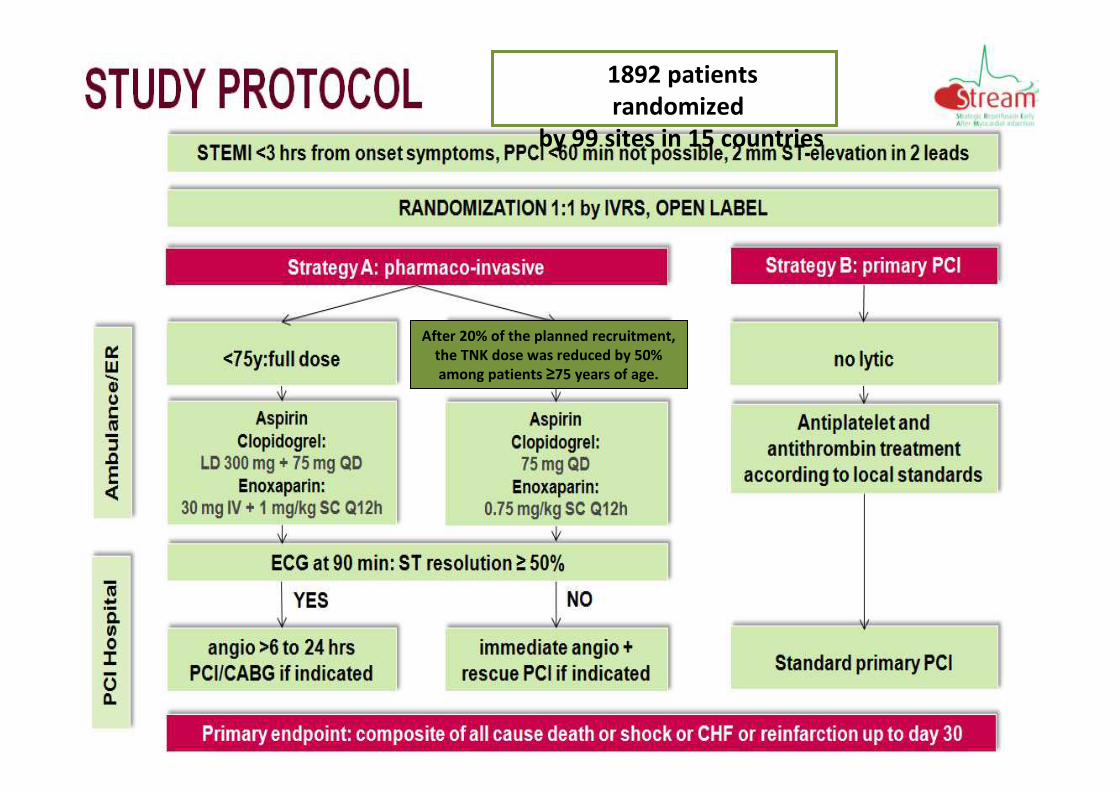
After 20% of the planned recruitment,
the TNK dose was reduced by 50%
among patients ≥75 years of age.
1892 patients
randomized
by 99 sites in 15 countries
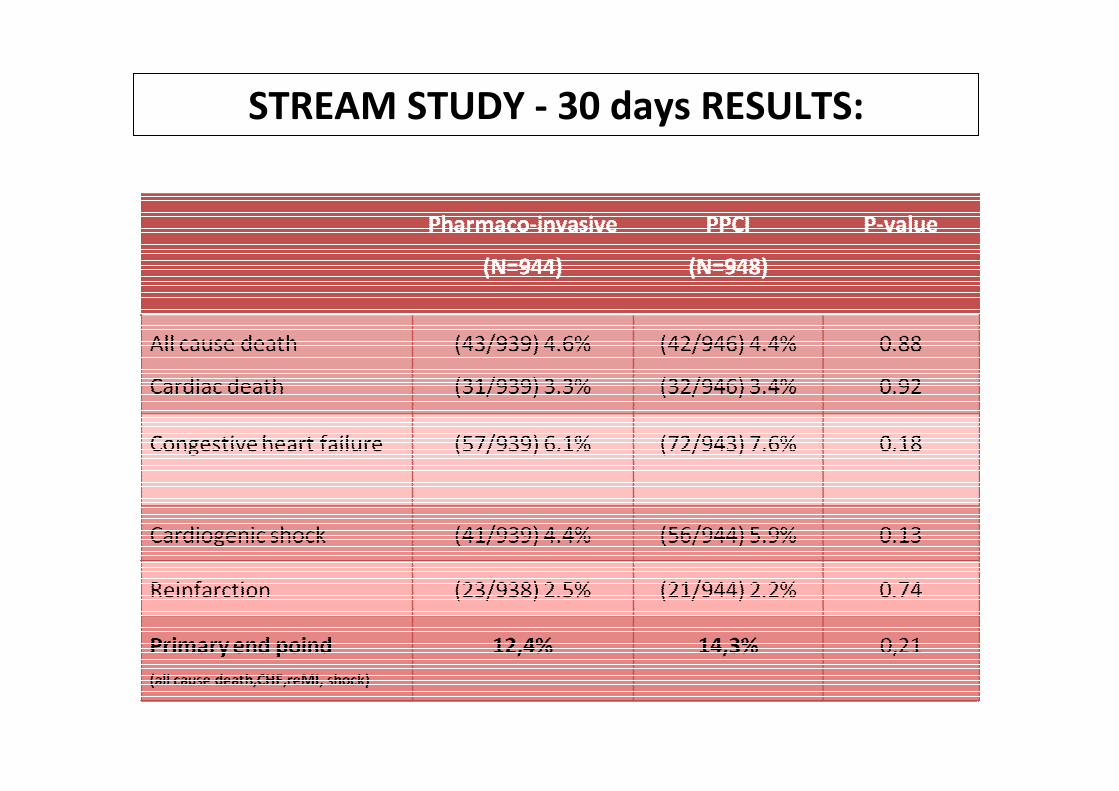
STREAM STUDY - 30 days RESULTS:
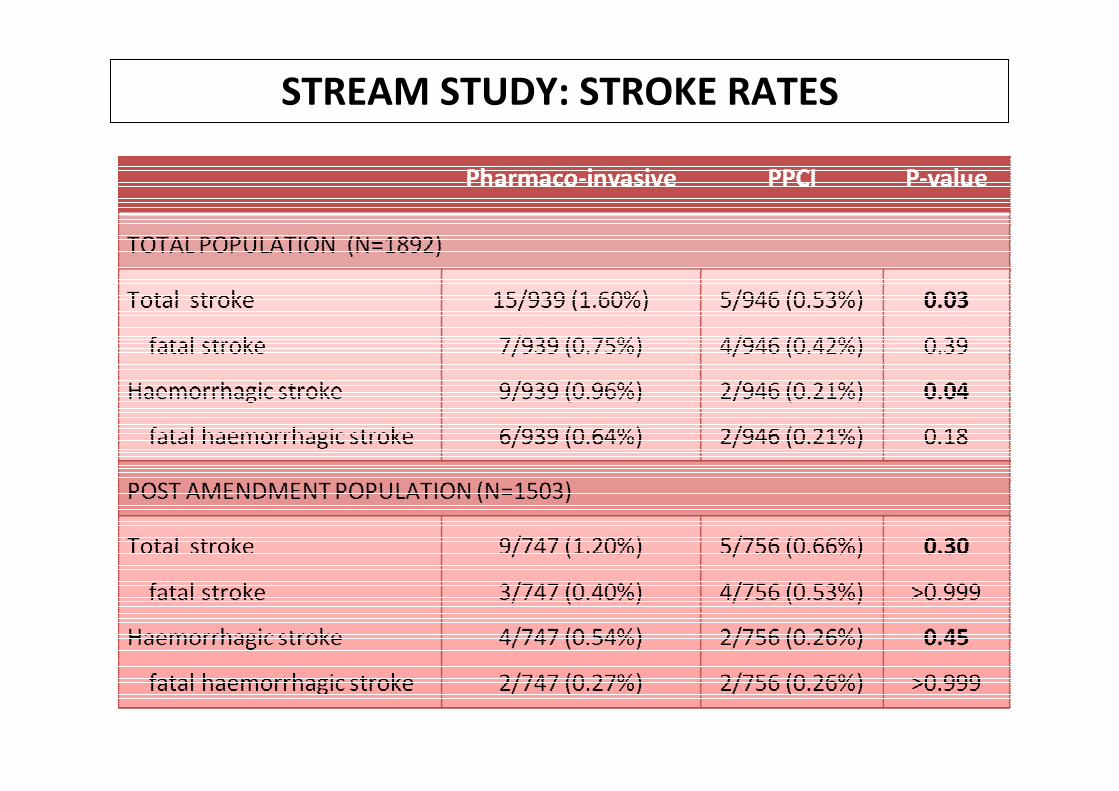
STREAM STUDY: STROKE RATES
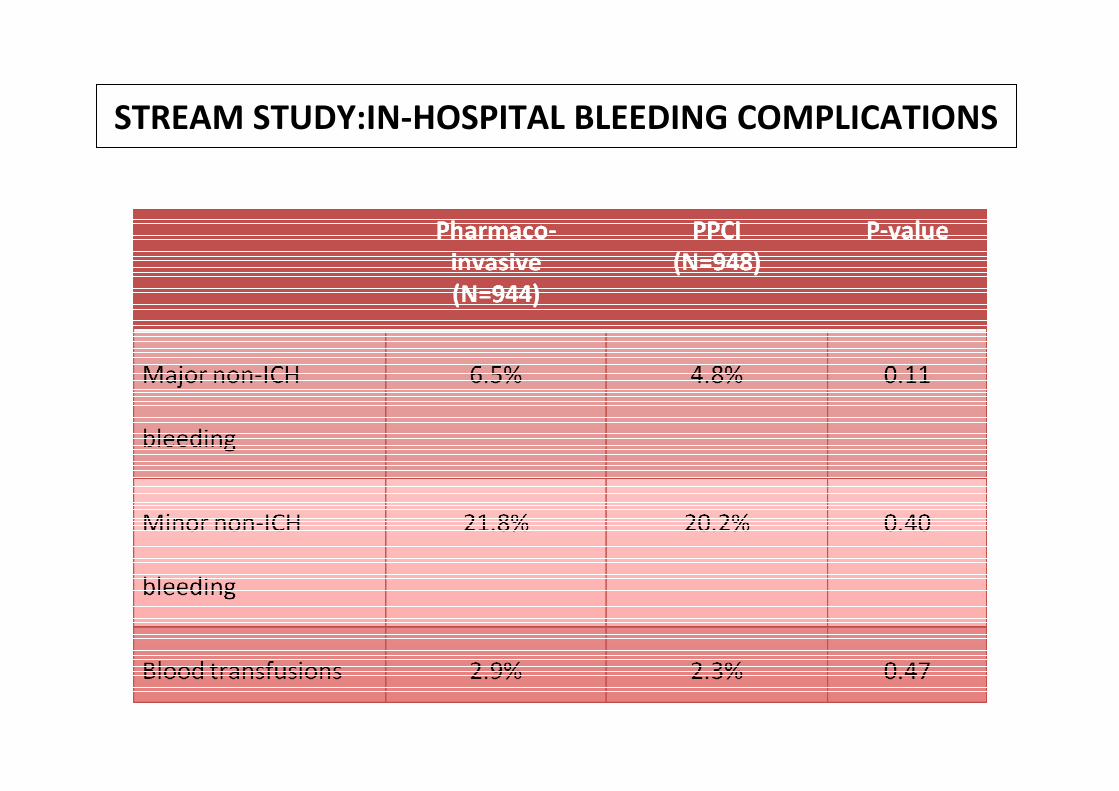
STREAM STUDY:IN-HOSPITAL BLEEDING COMPLICATIONS
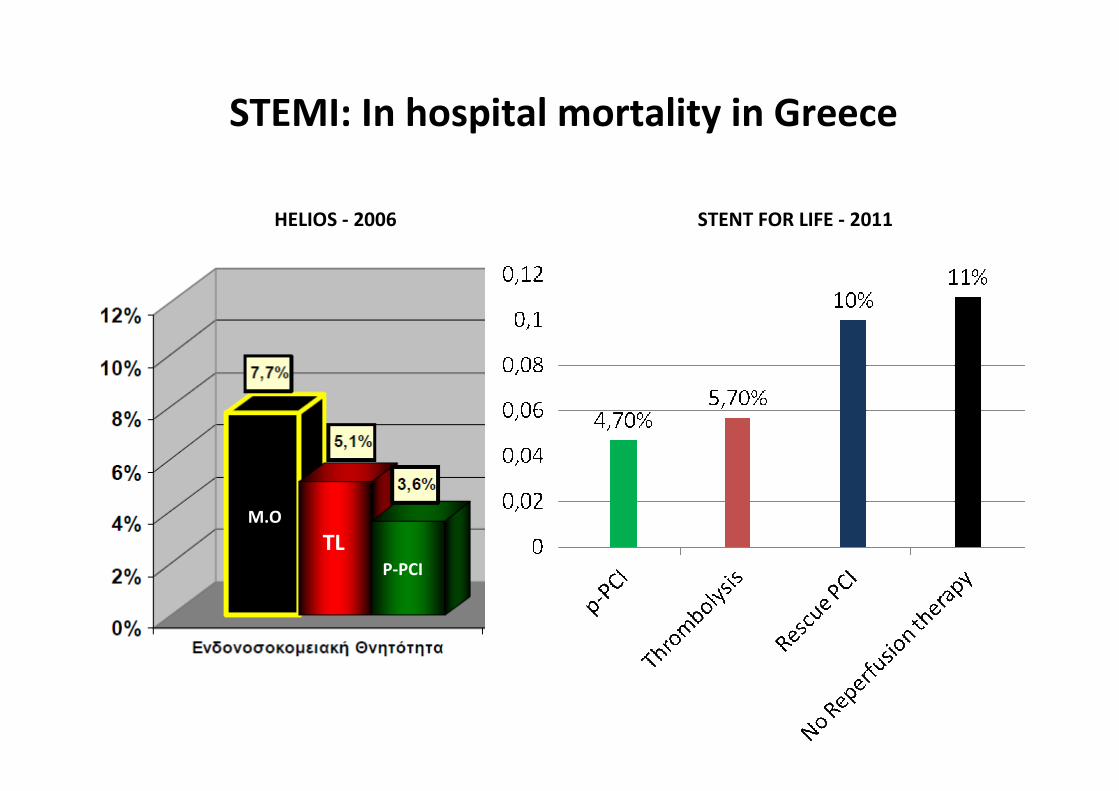
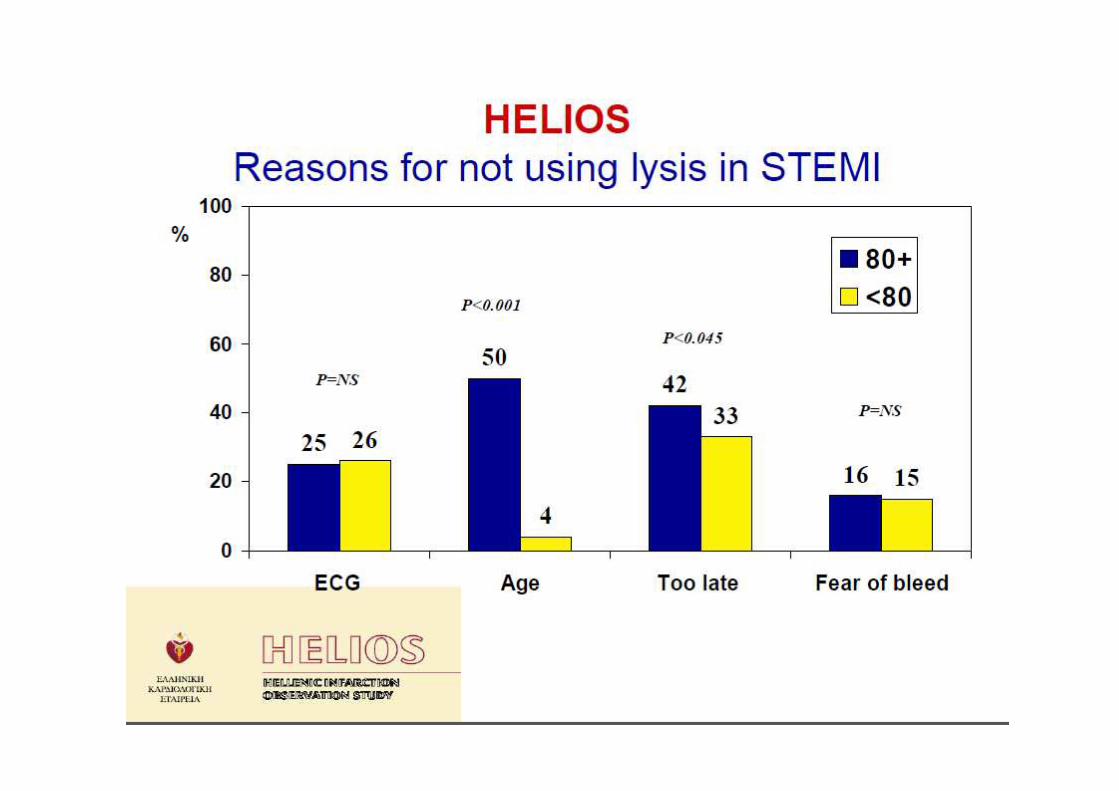
STEMI: In hospital mortality in Greece
HELIOS - 2006 STENT FOR LIFE - 2011
M.O
TLP-PCI

REPERFUSION THERAPIES IN GREECE
Thrombolysis pts:
Rescue PCI: 7,4%
Pharmacoinvasive: 6,4%
THROMBOLYSIS
P-PCI
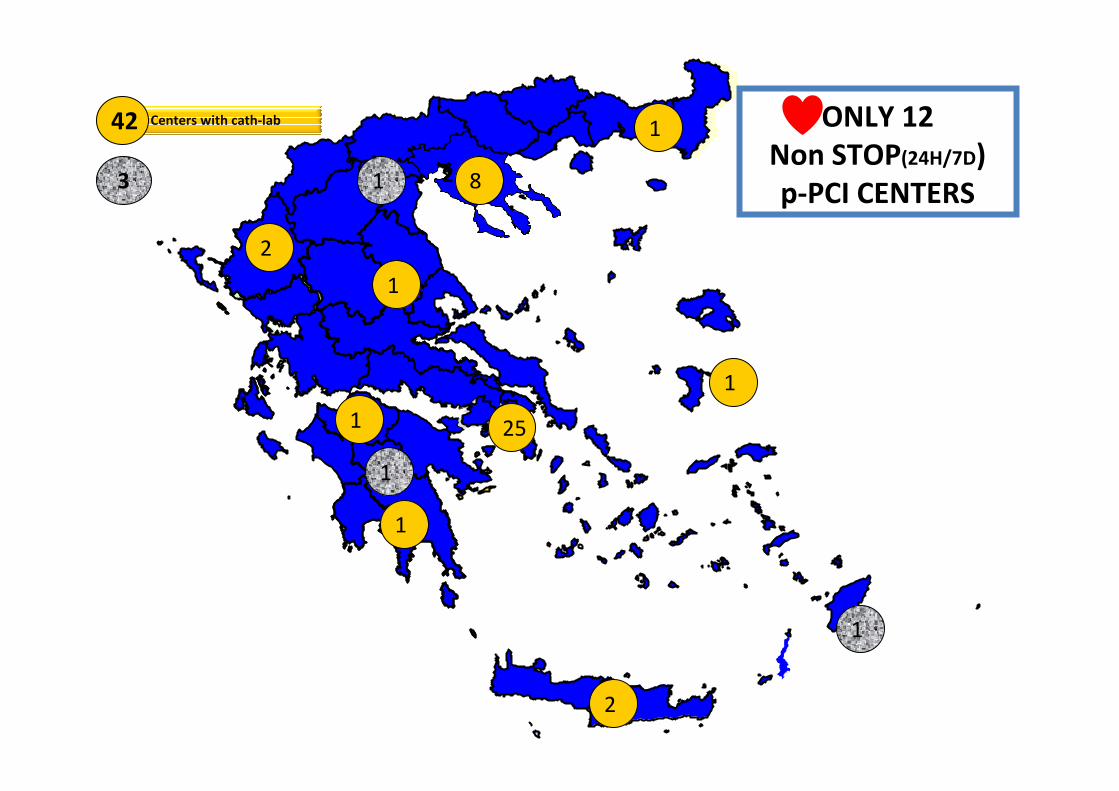
25
2
1
1
1
2
Centers with cath-lab ONLY 12
Non STOP(24H/7D)
p-PCI CENTERS
2
8
1
1
42
1
1
13
• However, in many areas of the world, like Greece primary PCI cannot be performed within the recommended time limits(<90-120 min).
• In these remote areas, thrombolysis is still the treatment of choice.
• Primary PCI is the preferred
treatment of ST-elevation
myocardial infarction.
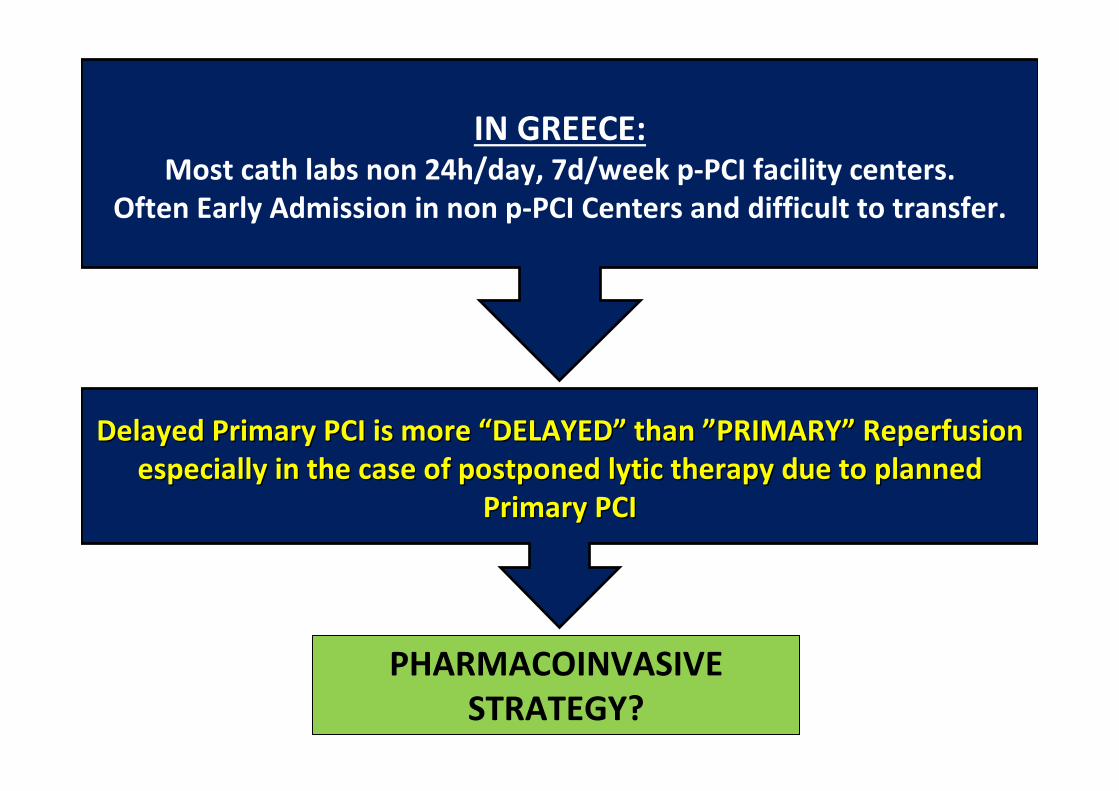
IN GREECE:Most cath labs non 24h/day, 7d/week p-PCI facility centers.
Often Early Admission in non p-PCI Centers and difficult to transfer.
PHARMACOINVASIVE
STRATEGY?
Delayed Primary PCI is more Delayed Primary PCI is more ““DELAYEDDELAYED”” than than ””PRIMARYPRIMARY”” Reperfusion Reperfusion
especially in the case of postponed lytic therapy due to plannedespecially in the case of postponed lytic therapy due to planned
Primary PCIPrimary PCI
Α. Διαχωριστικό ανεύρυσμα αορτής
Β. Γαστρορραγία τον τελευταίο μήνα
Γ. Ανθεκτική υπέρταση
(συστολική> 180mmHg και διαστολική> 110mmHg)
Δ. Ισχαιμικό εγκεφαλικό τους τελευταίους 6 μήνες
Ε. Προηγούμενο αιμορραγικό εγκεφαλικό επεισόδιο 2 χρόνια πριν
1. ΠΟΙΟ ΑΠΟ ΤΑ ΠΑΡΑΚΑΤΩ ΔΕΝ ΕΙΝΑΙ ΑΠΟΛΥΤΗ
ΑΝΤΕΝΔΕΙΞΗ ΘΡΟΜΒΟΛΥΣΗΣ ;
Α. Να περιμένει και να αξιολογήσει εκ νέου το ΗΚΓ σε 30 λεπτά
Β. Να χορηγήσει αναστολείς αιμοπεταλίων IIb – IIIa
Γ. Να διακομίσει άμεσα τον ασθενή για αγγειοπλαστική
Δ. Να χορηγήσει ξανά θρομβόλυση
2. Ασθενής με πρόσθιο STEMI προσήλθε 1ώρα από την έναρξη των
ενοχλημάτων σε non-PCI Νοσοκομείο, που βρίσκεται σε απόσταση 130
λεπτών από PCI Νοσοκομείο. Τρεις ώρες μετά από την αρχικά επιτυχημένη
θρομβόλυση ο ασθενής παρουσιάζει επανέμφραγμα. Ποια είναι η επόμενη
ενέργεια του εφημερεύοντα με βάση τις τελευταίες κατευθυντήριες οδηγίες;
Α. Να περιμένει και να αξιολογήσει εκ νέου το ΗΚΓ στα 90 λεπτά
Β. Να διακομίσει άμεσα τον ασθενή για αγγειοπλαστική
διάσωσης
Γ. Να χορηγήσει αναστολείς αιμοπεταλίων IIb – IIIa
Δ. Να διακομίσει τον ασθενή για αγγειοπλαστική 3 ώρες
μετά τη χορήγηση της θρομβόλυσης
3. Ασθενής με πλάγιο STEMI θρομβολύθηκε σε non-PCI Νοσοκομείο. Στα 60 λεπτά
μετά τη χορήγηση θρομβολυτικής θεραπείας οι αρχικές ανασπάσεις έχουν
ελαττωθεί 30%. Ποια είναι η επόμενη ενέργεια του εφημερεύοντα με βάση τις
τελευταίες κατευθυντήριες οδηγίες, με δεδομένο ότι το πλησιέστερο PCI-
Νοσοκομείο βρίσκεται σε απόσταση 130 λεπτών;

Back up slides
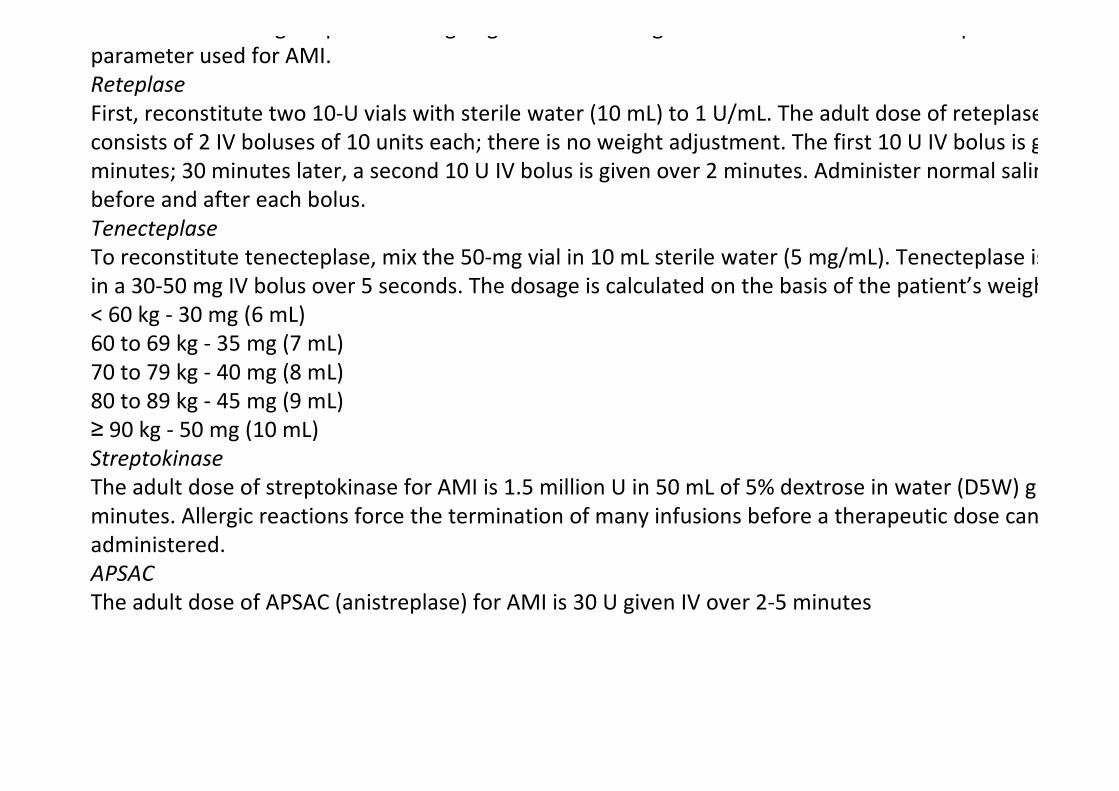
total dose is 100 mg for patients weighing more than 67 kg. This is the most common alteplase infusion
parameter used for AMI.
Reteplase
First, reconstitute two 10-U vials with sterile water (10 mL) to 1 U/mL. The adult dose of reteplase for AMI
consists of 2 IV boluses of 10 units each; there is no weight adjustment. The first 10 U IV bolus is given over 2
minutes; 30 minutes later, a second 10 U IV bolus is given over 2 minutes. Administer normal saline (NS) flush
before and after each bolus.
Tenecteplase
To reconstitute tenecteplase, mix the 50-mg vial in 10 mL sterile water (5 mg/mL). Tenecteplase is admini
in a 30-50 mg IV bolus over 5 seconds. The dosage is calculated on the basis of the patient’s weight, as follows:
< 60 kg - 30 mg (6 mL)
60 to 69 kg - 35 mg (7 mL)
70 to 79 kg - 40 mg (8 mL)
80 to 89 kg - 45 mg (9 mL)
≥ 90 kg - 50 mg (10 mL)
Streptokinase
The adult dose of streptokinase for AMI is 1.5 million U in 50 mL of 5% dextrose in water (D5W) given IV over 60
minutes. Allergic reactions force the termination of many infusions before a therapeutic dose can be
administered.
APSAC
The adult dose of APSAC (anistreplase) for AMI is 30 U given IV over 2-5 minutes
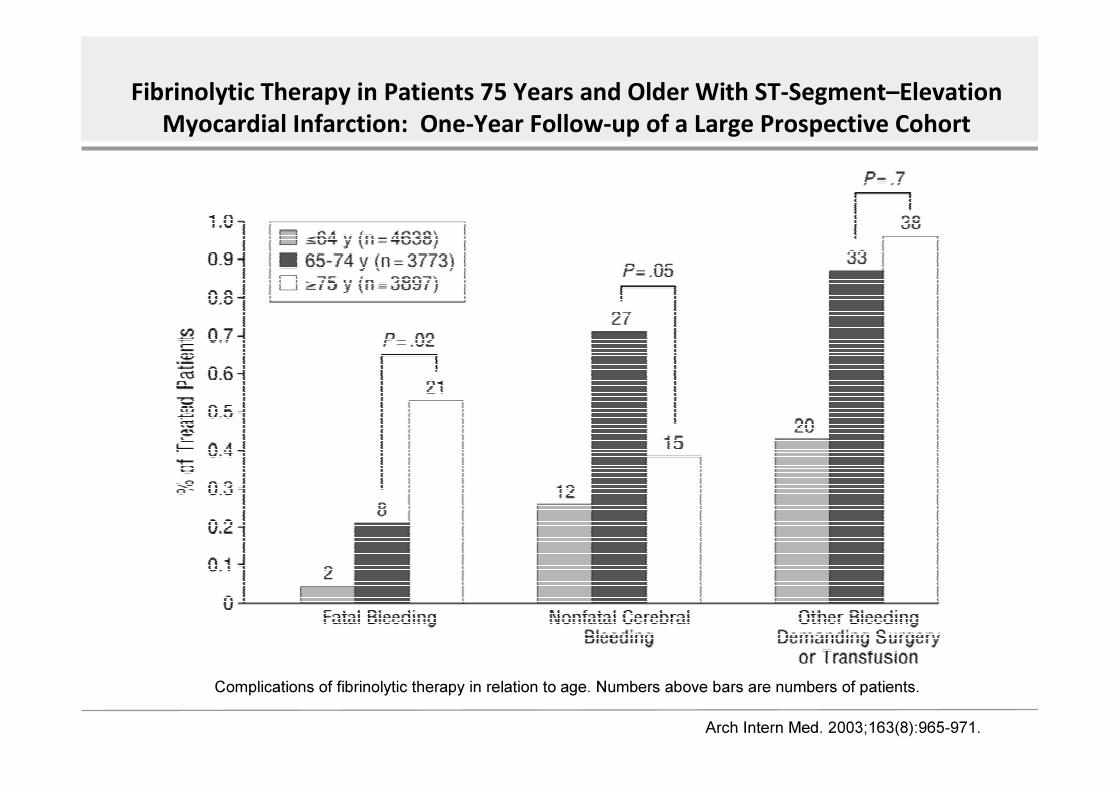
Fibrinolytic Therapy in Patients 75 Years and Older With ST-Segment–Elevation
Myocardial Infarction: One-Year Follow-up of a Large Prospective Cohort
Complications of fibrinolytic therapy in relation to age. Number s above bars are numbers of patients.
Arch Intern Med. 2003;163(8):965-971.
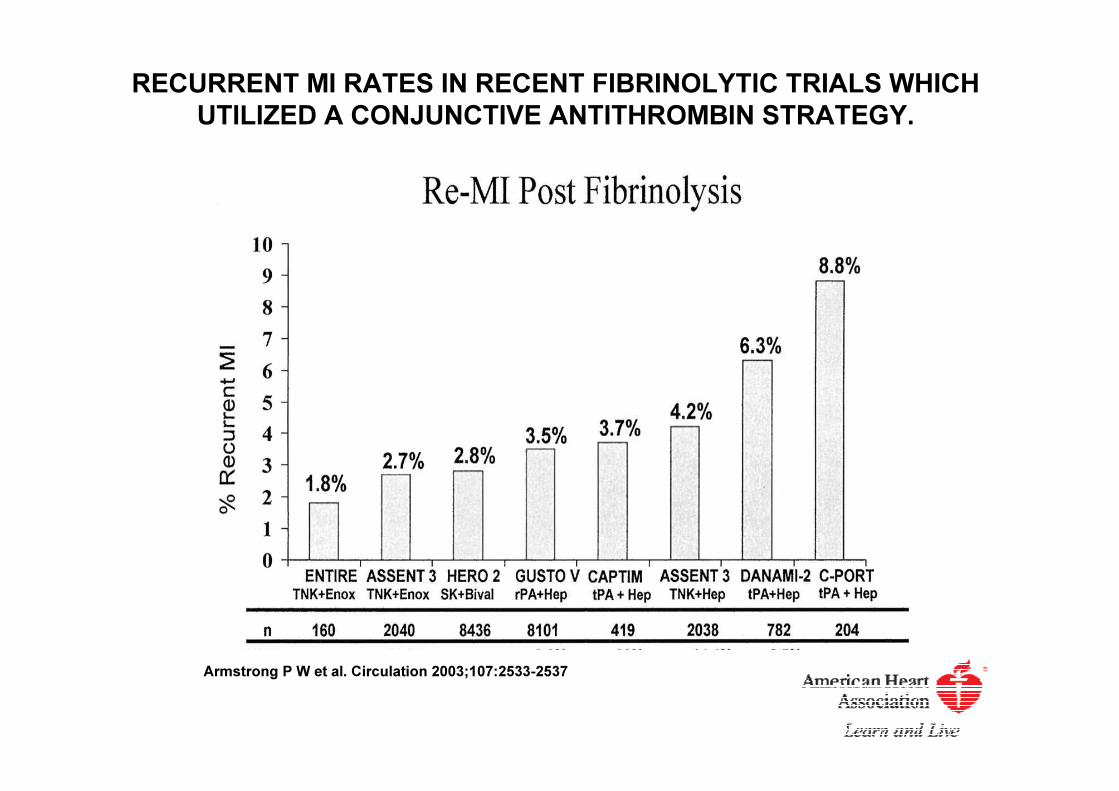
RECURRENT MI RATES IN RECENT FIBRINOLYTIC TRIALS WHICH
UTILIZED A CONJUNCTIVE ANTITHROMBIN STRATEGY.
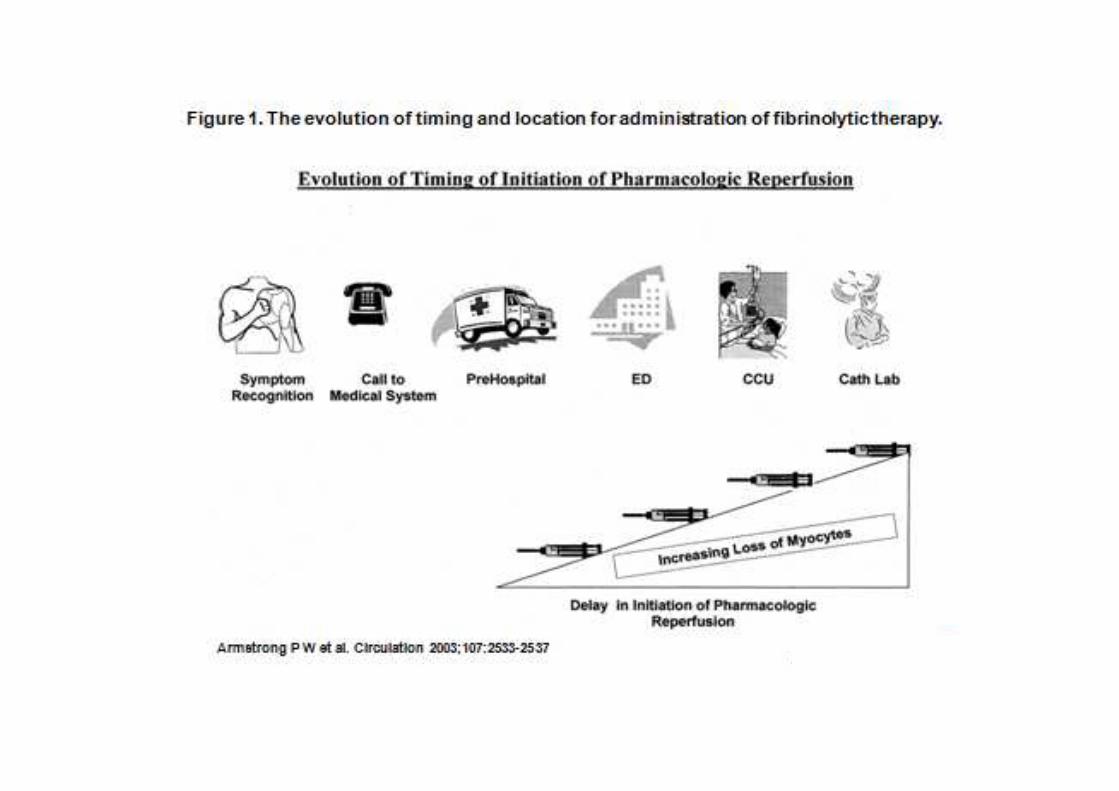
Armstrong P W et al. Circulation 2003;107:2533-2537
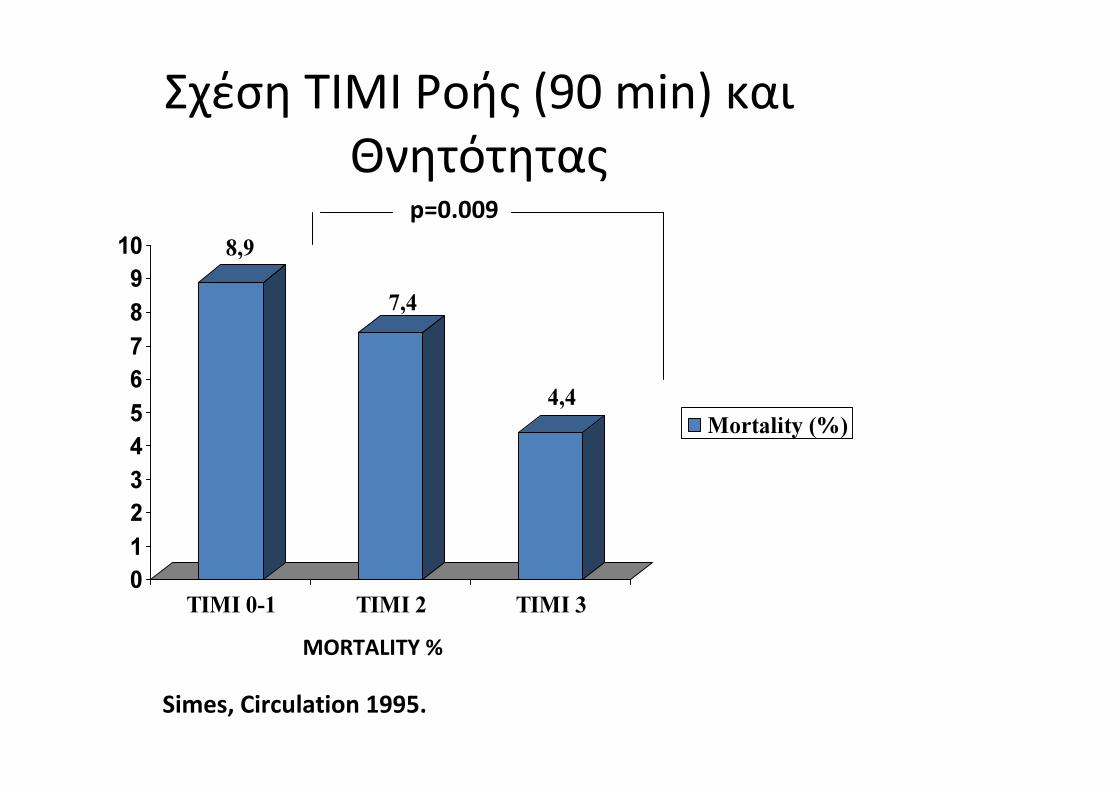
Σχέση TIMI Ροής (90 min) και
Θνητότητας
8,9
7,4
4,4
0
1
2
3
4
5
6
7
8
9
10
TIMI 0-1 TIMI 2 TIMI 3
Mortality (%)
Simes, Circulation 1995.
p=0.009
MORTALITY %
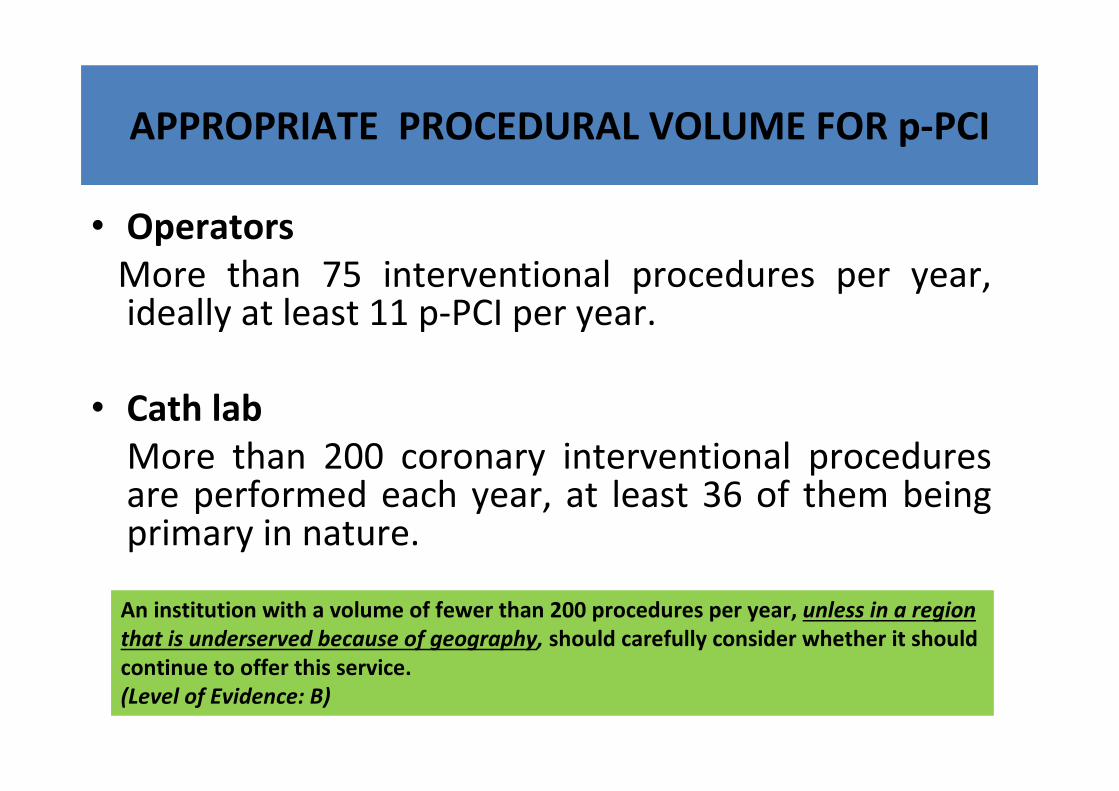
APPROPRIATE PROCEDURAL VOLUME FOR p-PCI
• Operators
More than 75 interventional procedures per year, ideally at least 11 p-PCI per year.
• Cath lab
More than 200 coronary interventional procedures are performed each year, at least 36 of them being primary in nature.
An institution with a volume of fewer than 200 procedures per year, unless in a region
that is underserved because of geography, should carefully consider whether it should
continue to offer this service.
(Level of Evidence: B)
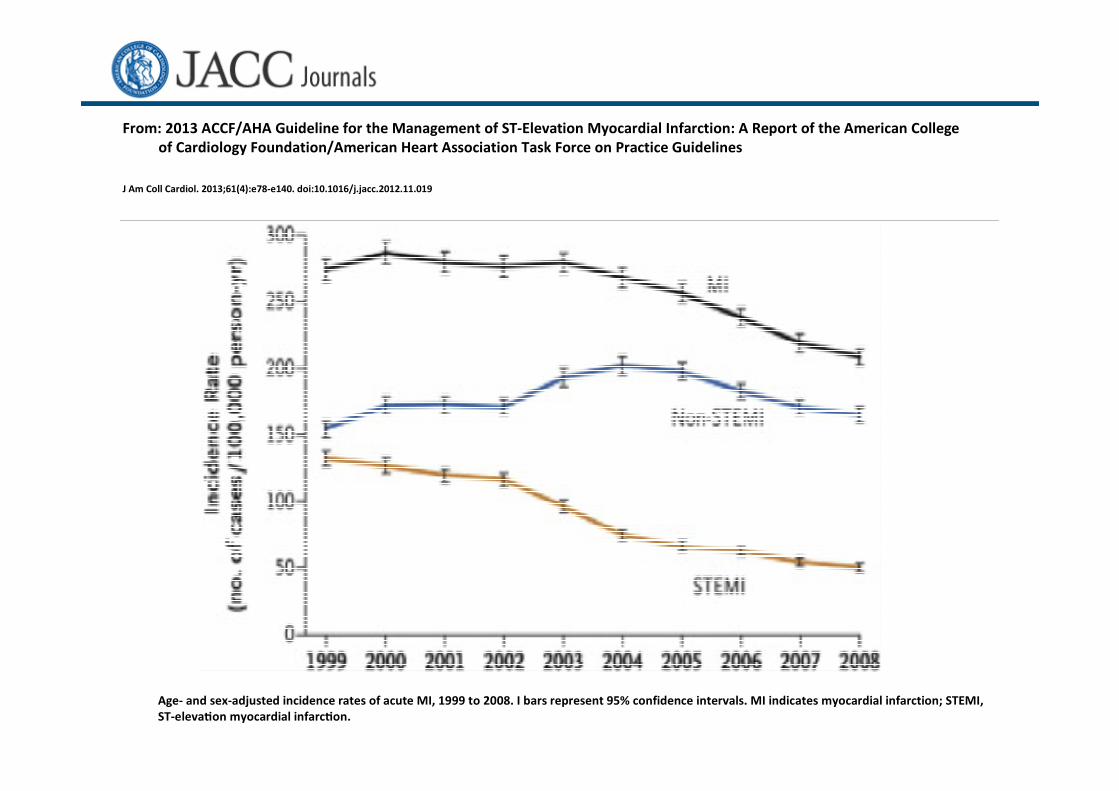
From: 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College
of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
J Am Coll Cardiol. 2013;61(4):e78-e140. doi:10.1016/j.jacc.2012.11.019
Age- and sex-adjusted incidence rates of acute MI, 1999 to 2008. I bars represent 95% confidence intervals. MI indicates myocardial infarction; STEMI,
ST- eleva�on myocardial infarc�on.
1/3
1/2
1/4
Convincing evidence of the effectiveness of aspirin was demonstrated by the ISIS-2
trial,79 in which the benefits of aspirin and streptokinase were additive. The first dose of
150–325 mg should be chewed (no enteric-coated aspirin because of slow onset of
action) and a lower dose (75–100 mg) given orally daily thereafter. If oral ingestion is not
possible, aspirin can be given i.v. (250–500 mg). In the CLARITY trial, patients ≤75 years
were treated with a standard fibrinolytic regimen and randomized to 300 mg clopidogrel
loading dose followed by 75 mg per day or placebo on top of aspirin up to and including
the day of angiography with a maximum of 8 days (mean duration 3 days). By 30 days,
clopidogrel therapy reduced the odds of the composite end-point of death from
cardiovascular causes, recurrent myocardial infarction, or recurrent ischaemia, leading to
a reduction of the need for urgent revascularization of 20%. The rates of major bleeding
and intracranial haemorrhage were similar in the two groups.52 In the COMMIT
study,80 45 852 Chinese patients of any age (but <1000 patients >75 years) with
suspected myocardial infarction (93% with STEMI) were randomized to clopidogrel 75 mg
(no loading dose) or placebo in addition to aspirin. Clopidogrel significantly reduced the
odds of the composite of death, myocardial infarction, or stroke, corresponding to nine
fewer events per 1000 patients treated for ∼2 weeks. Accordingly, there is a good case
for the routine use of clopidogrel in the acute phase
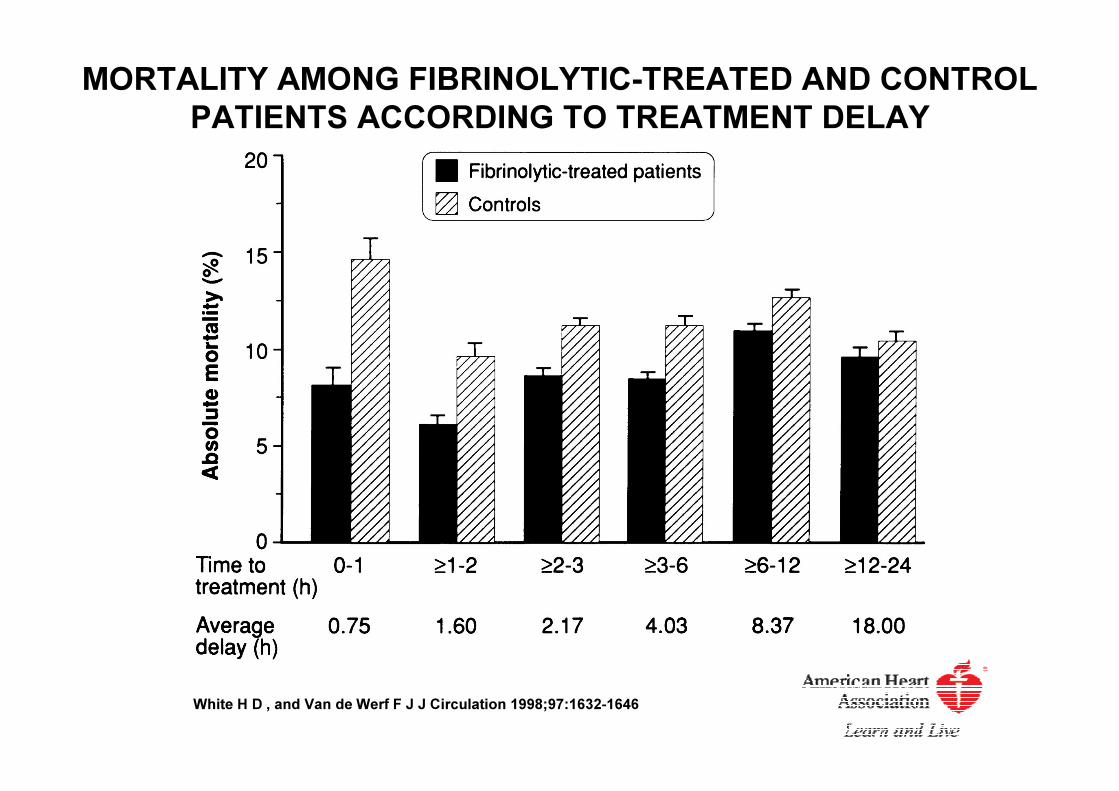
MORTALITY AMONG FIBRINOLYTIC-TREATED AND CONTROL
PATIENTS ACCORDING TO TREATMENT DELAY
White H D , and Van de Werf F J J Circulation 1998;97:1632-1646
STREAM STUDY - CONCLUSIONS
A strategy of fibrinolysis with bolus tenecteplase and
contemporary antithrombotic therapy given before
transport to a PCI-capable hospital coupled with timely
coronary angiography :
�circumvents the need for an urgent procedure in about
two thirds of fibrinolytic treated STEMI patients.
�is associated with a small increased risk of intracranial
bleeding.
�is as effective as primary PCI in STEMI patients presenting
within 3 hours of symptom onset who cannot undergo
primary PCI within one hour of first medical contact.
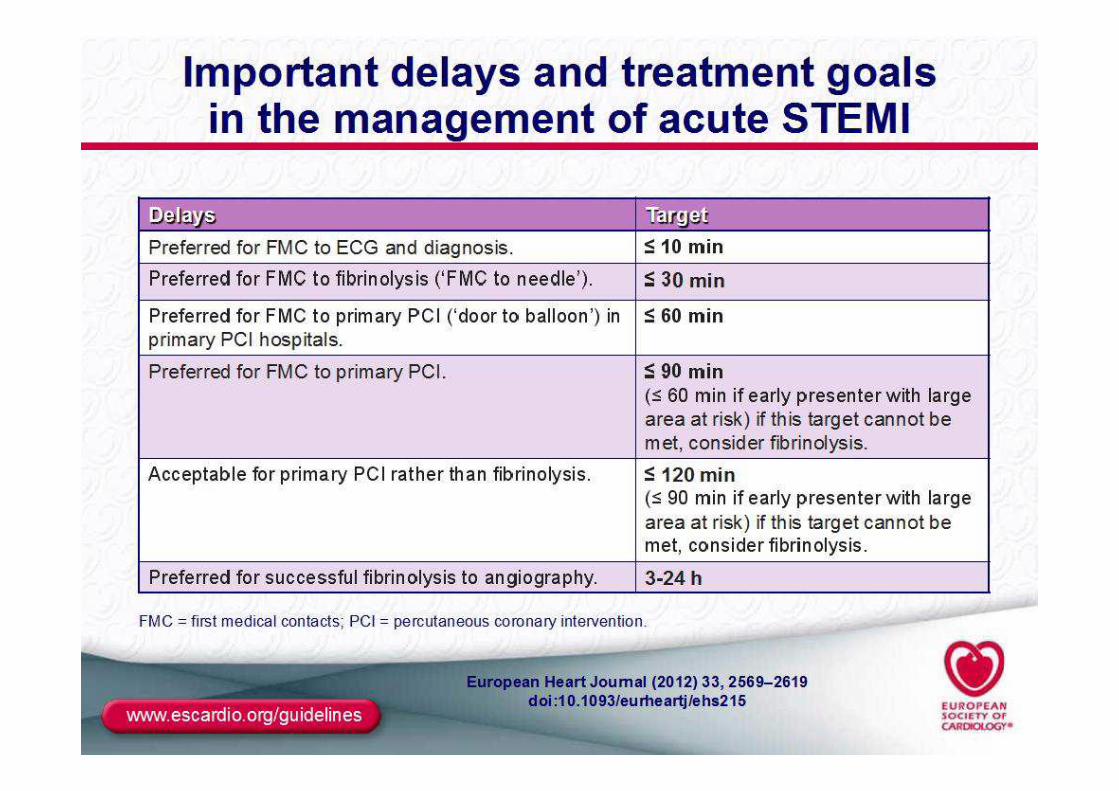
Fibrinolytic Therapy When There Is an Anticipated Delay Fibrinolytic Therapy When There Is an Anticipated Delay Fibrinolytic Therapy When There Is an Anticipated Delay Fibrinolytic Therapy When There Is an Anticipated Delay
to Performing Primary PCI Within 120 Min of FMC to Performing Primary PCI Within 120 Min of FMC to Performing Primary PCI Within 120 Min of FMC to Performing Primary PCI Within 120 Min of FMC
Reperfusion at a Non–PCI-Capable Hospital
When fibrinolytic therapy is indicated or chosen as the primary
reperfusion strategy, it should be administered within 30 minutes of
hospital arrival.*
I IIa IIb III
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
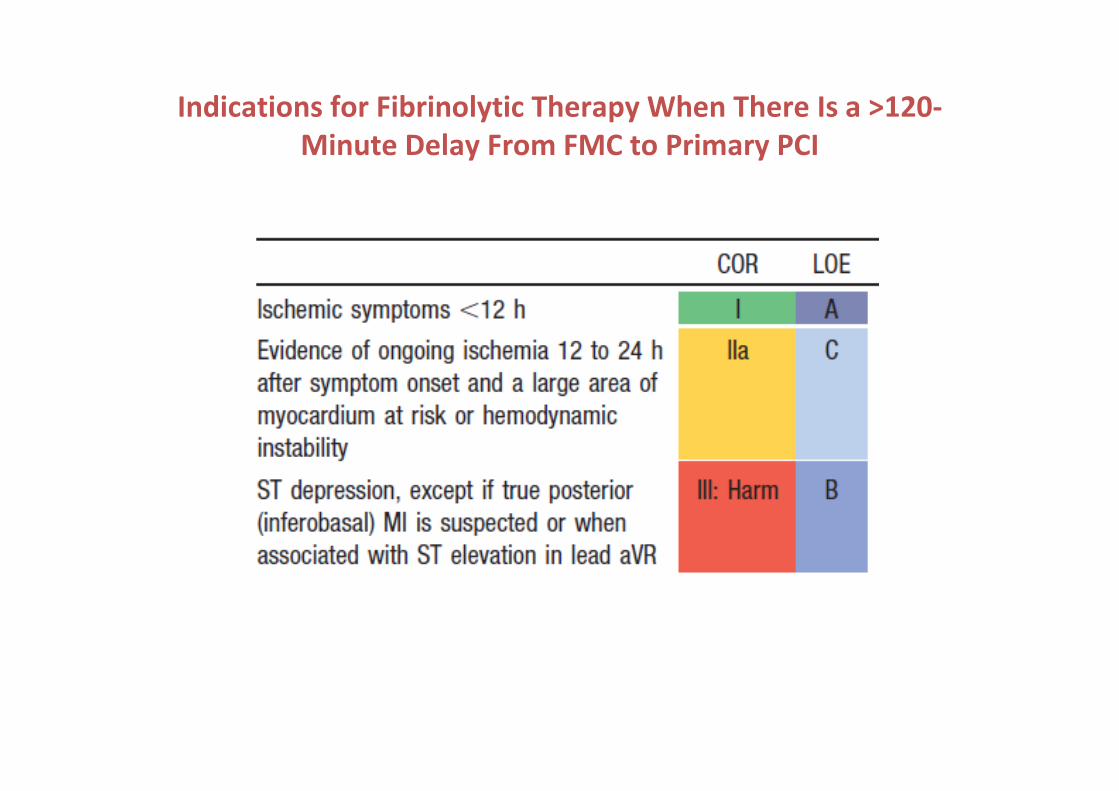
Indications for Fibrinolytic Therapy When There Is a >120-
Minute Delay From FMC to Primary PCI
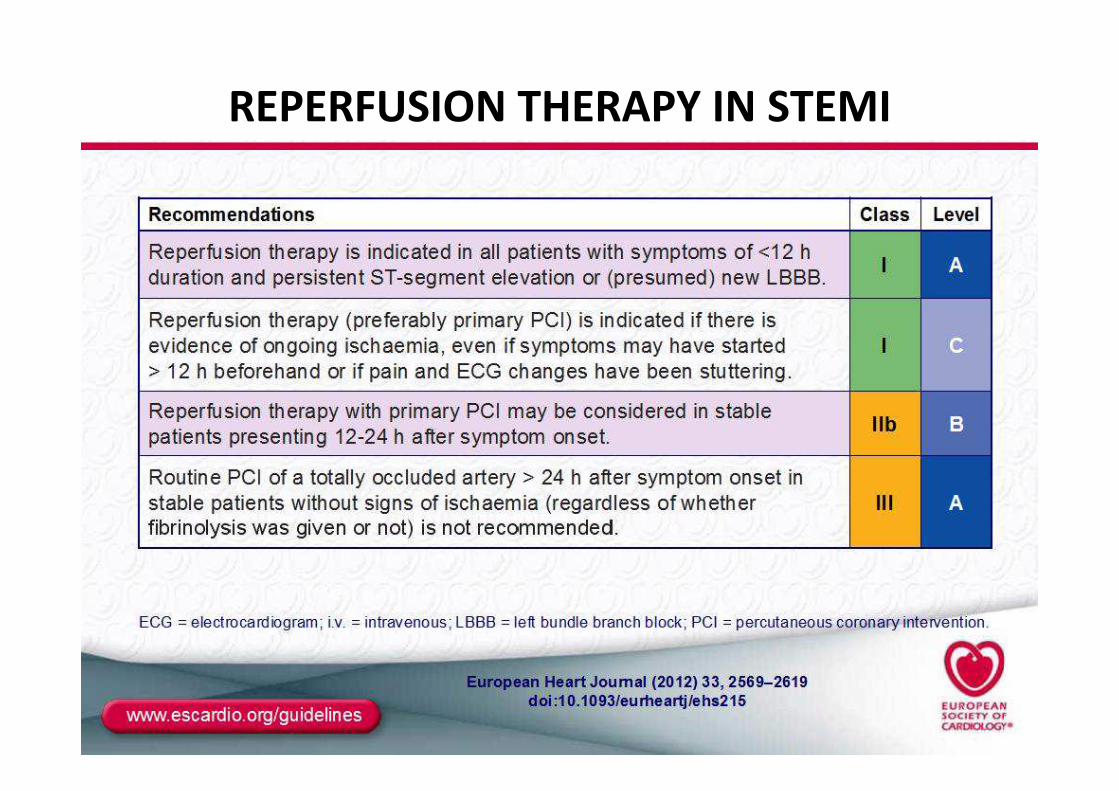
REPERFUSION THERAPY IN STEMI
In this trial, 1572 STEMI patients were randomized within 12 hours of symptom onset to a fibrinolytic versus
a primary percutaneous coronary intervention (PCI) strategy in both community (n=1129) and primary PCI
(n=443) hospitals.19 This study integrated an inter-institutional transfer policy for those randomized to
primary PCI if it could be achieved within 3 hours. The Data and Safety Monitoring Board prematurely
terminated DANAMI 2 because of the perception of “clear benefit” of primary PCI. Although DANAMI 2 did
show a substantial reduction in the composite 30-day endpoint of death, re-MI, and disabling stroke (13.7%
versus 8.0%; P=0.003) in favor of the primary PCI strategy, this outcome was overwhelmingly influenced by
the reduction in reinfarction (from 6.3% to 1.6%; P<0.0001). Importantly, this reduction in reinfarction
occurred in a clinical environment where transfer from a community hospital was considered
“investigational” if a mechanical intervention after fibrinolysis was needed. Hence, urgent PCI occurred in
only 2.5% of patients, even though 28% of the patients were randomized in interventional institutions. An
additional study, interpreted by some as impetus to move to an overall primary PCI strategy, was conducted
by the Cardiovascular Patients Outcomes Research Team (C-PORT) investigators who randomized 451 STEMI
patients within 12 hours of symptom onset to primary PCI versus tPA.20 Although there was no difference in
mortality, there was a substantial reduction in the composite endpoints of death, re-MI, and stroke with
primary PCI (17.7% versus 10.7% with tPA; P=0.03); this was again largely accounted for by a reduction in an
unusually high reinfarction rate amongst fibrinolytic-treated versus PCI-treated patients (8.8% versus
4%; P=0.04). Hence, in both the aforementioned studies, which used unfractionated heparin as the
antithrombin fibrinolytic partner, the recurrent infarction rate was by far the most important element in the
composite endpoint and seemed unusually high relative to other trials. This is well demonstrated in Figure 2,
where we compare the incidence of recurrent infarction in a number of recent STEMI studies that evaluated
fibrinolysis and antithrombin therapy; it is useful to evaluate them in the context of the frequency with
which mechanical cointervention with PCI was used.
J Am Coll Cardiol 2010;55:102–10
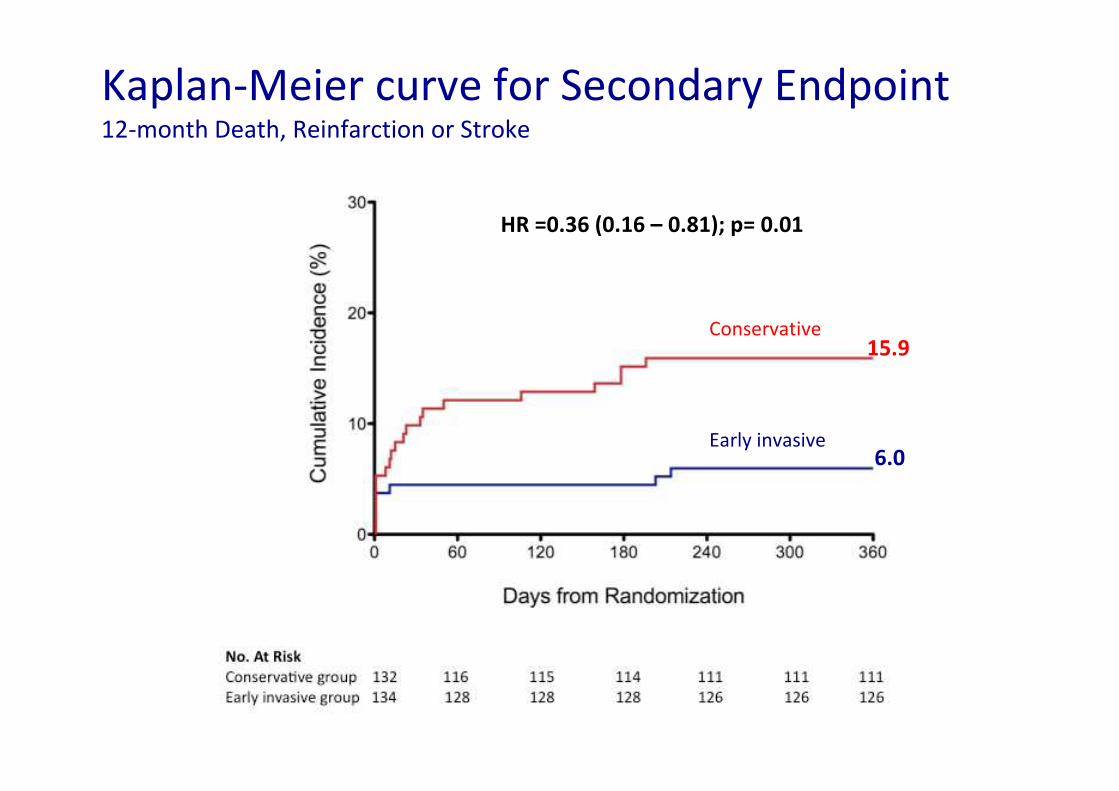
Kaplan-Meier curve for Secondary Endpoint12-month Death, Reinfarction or Stroke
Conservative
Early invasive
15.9
6.0
HR =0.36 (0.16 – 0.81); p= 0.01
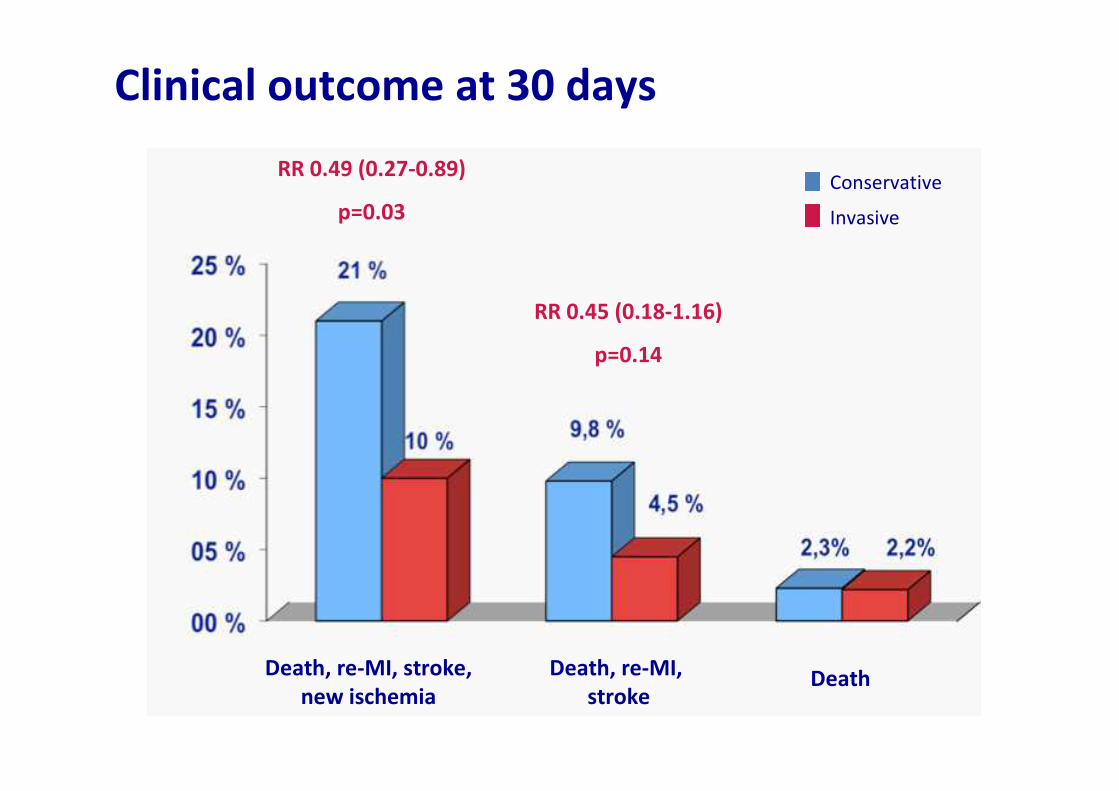
Clinical outcome at 30 days
Death, re-MI, stroke,
new ischemia
Death, re-MI,
strokeDeath
RR 0.49 (0.27-0.89)
p=0.03
RR 0.45 (0.18-1.16)
p=0.14
Invasive
Conservative
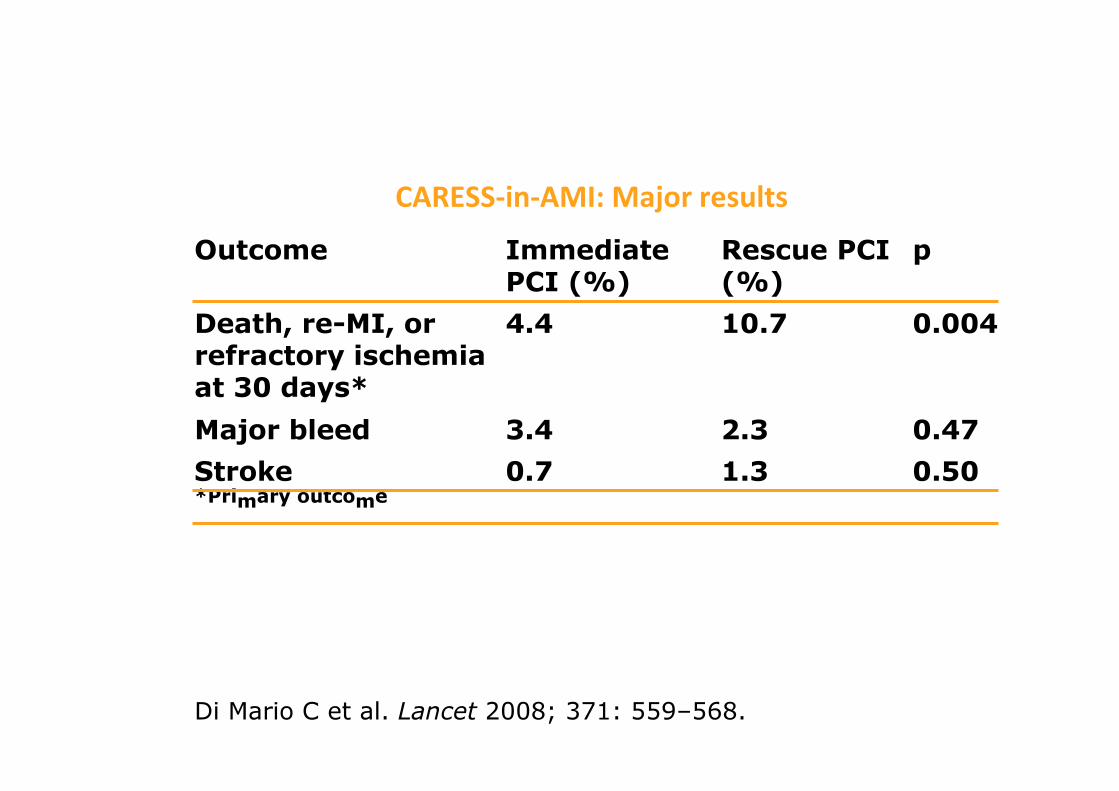
Di Mario C et al. Lancet 2008; 371: 559–568.
CARESS-in-AMI: Major results
Outcome Immediate PCI (%)
Rescue PCI (%)
p
Death, re-MI, or refractory ischemia at 30 days*
4.4 10.7 0.004
Major bleed 3.4 2.3 0.47
Stroke 0.7 1.3 0.50*Primary outcome
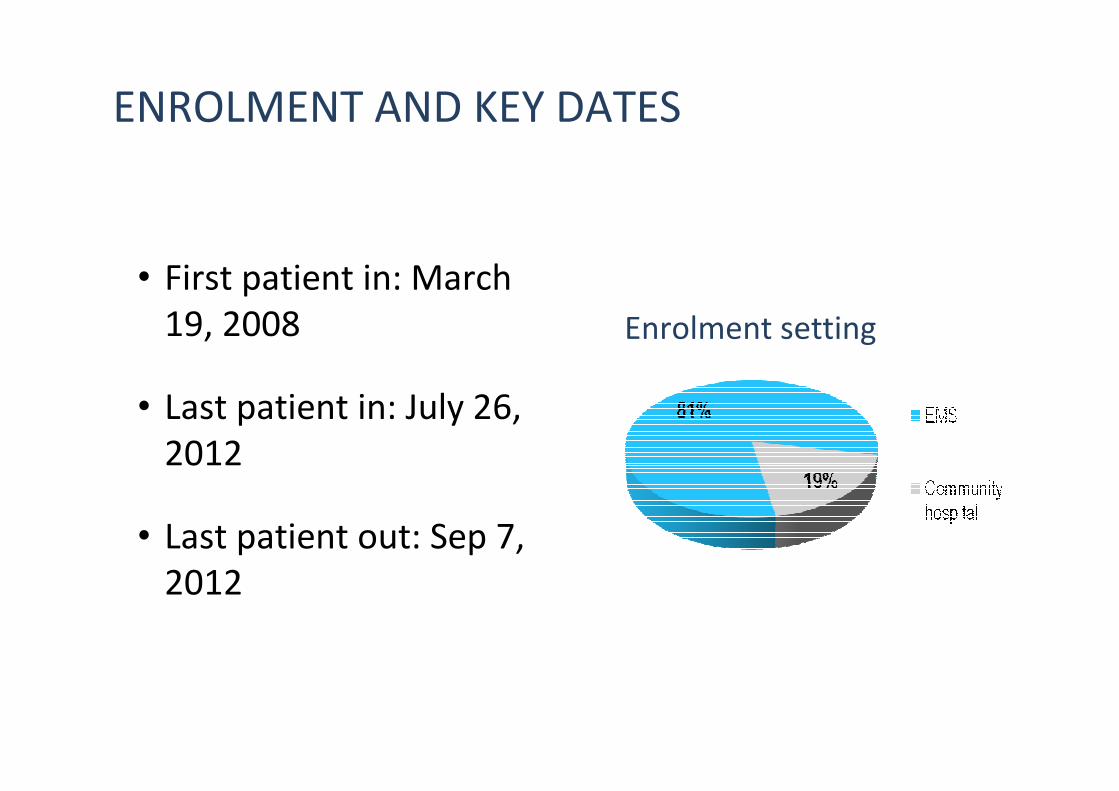
ENROLMENT AND KEY DATES
• First patient in: March
19, 2008
• Last patient in: July 26,
2012
• Last patient out: Sep 7,
2012
Enrolment setting
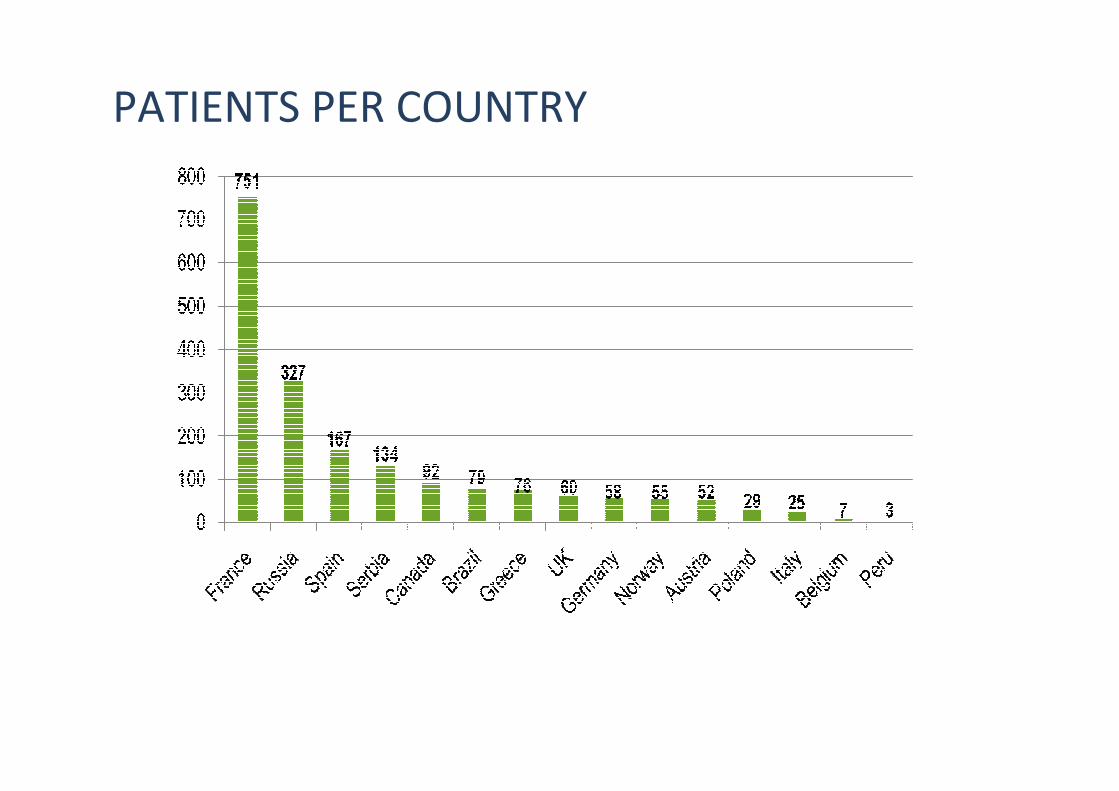
PATIENTS PER COUNTRY
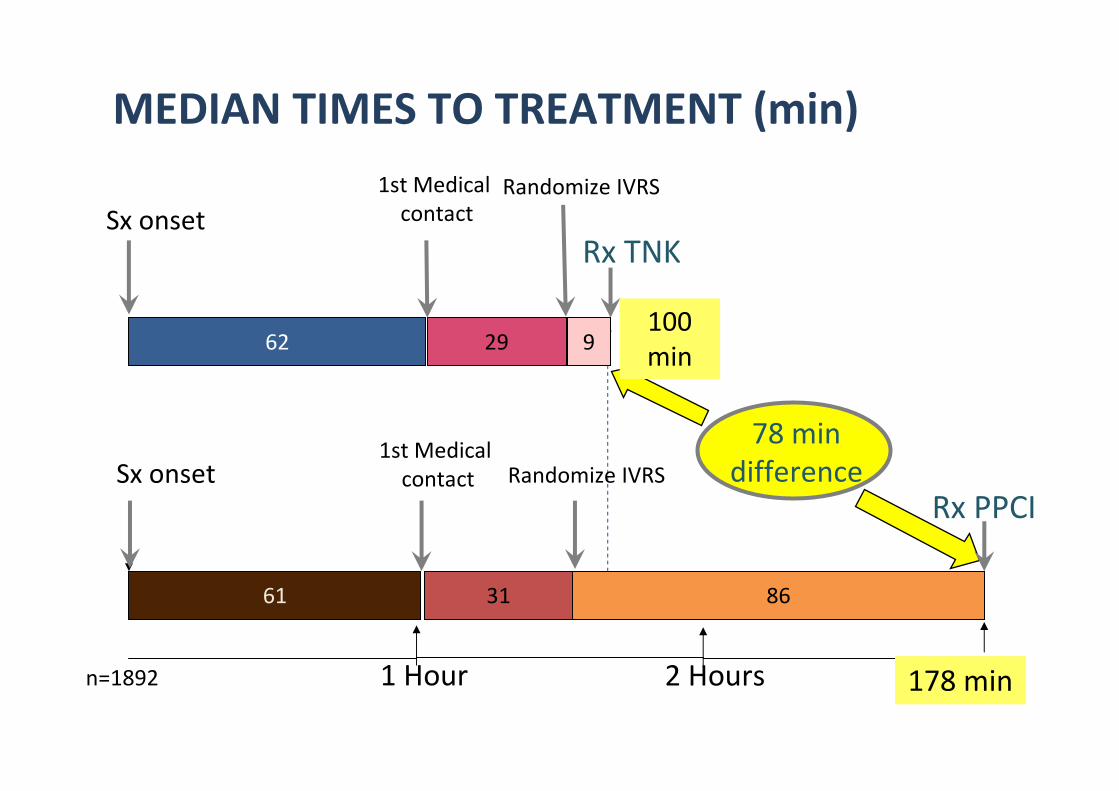
62
Sx onset
1st Medical
contact
61
1 Hour 2 Hoursn=1892
29
Randomize IVRS
9
Rx TNK
31 86
Sx onset
Rx PPCI
100
min
178 min
MEDIAN TIMES TO TREATMENT (min)
1st Medical
contact
78 min
differenceRandomize IVRS
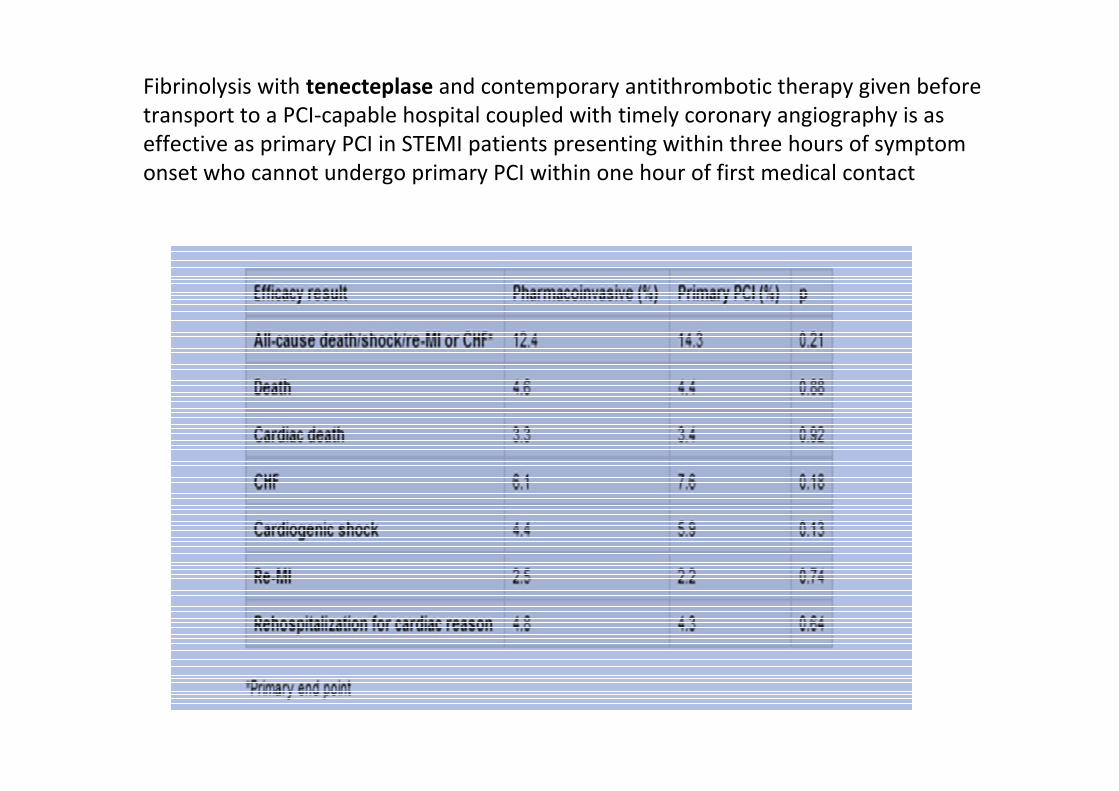
Fibrinolysis with tenecteplase and contemporary antithrombotic therapy given before
transport to a PCI-capable hospital coupled with timely coronary angiography is as
effective as primary PCI in STEMI patients presenting within three hours of symptom
onset who cannot undergo primary PCI within one hour of first medical contact
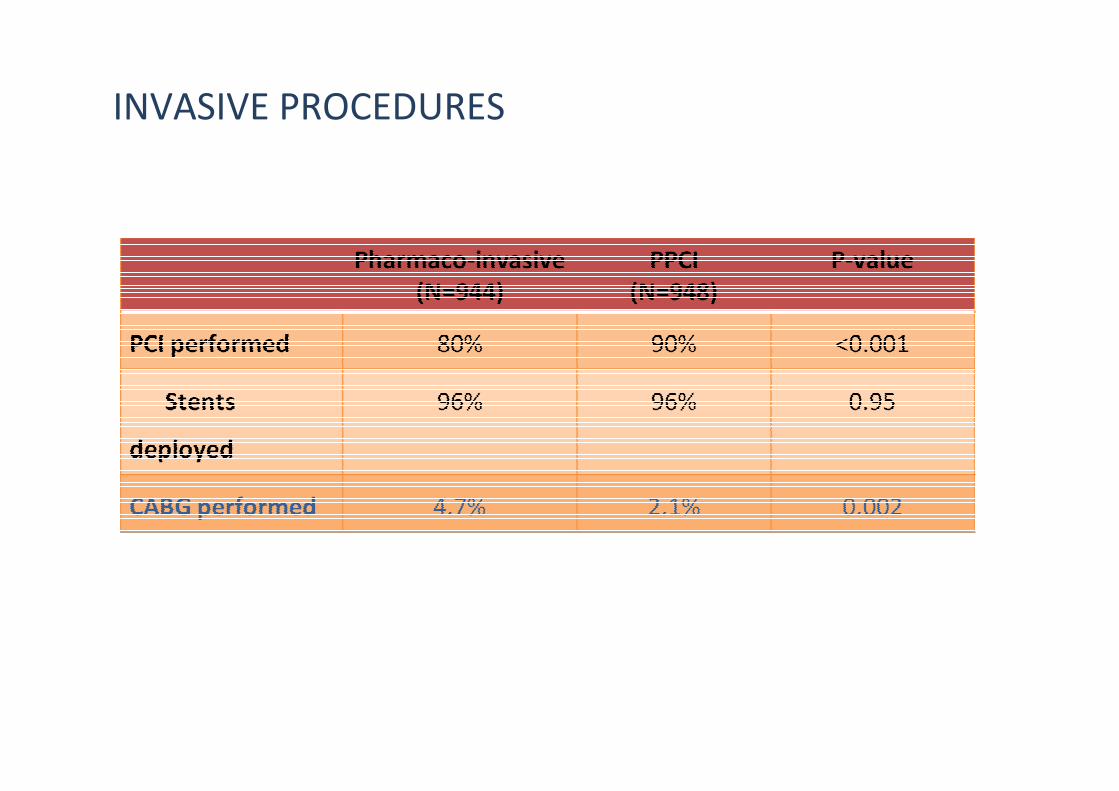
INVASIVE PROCEDURES
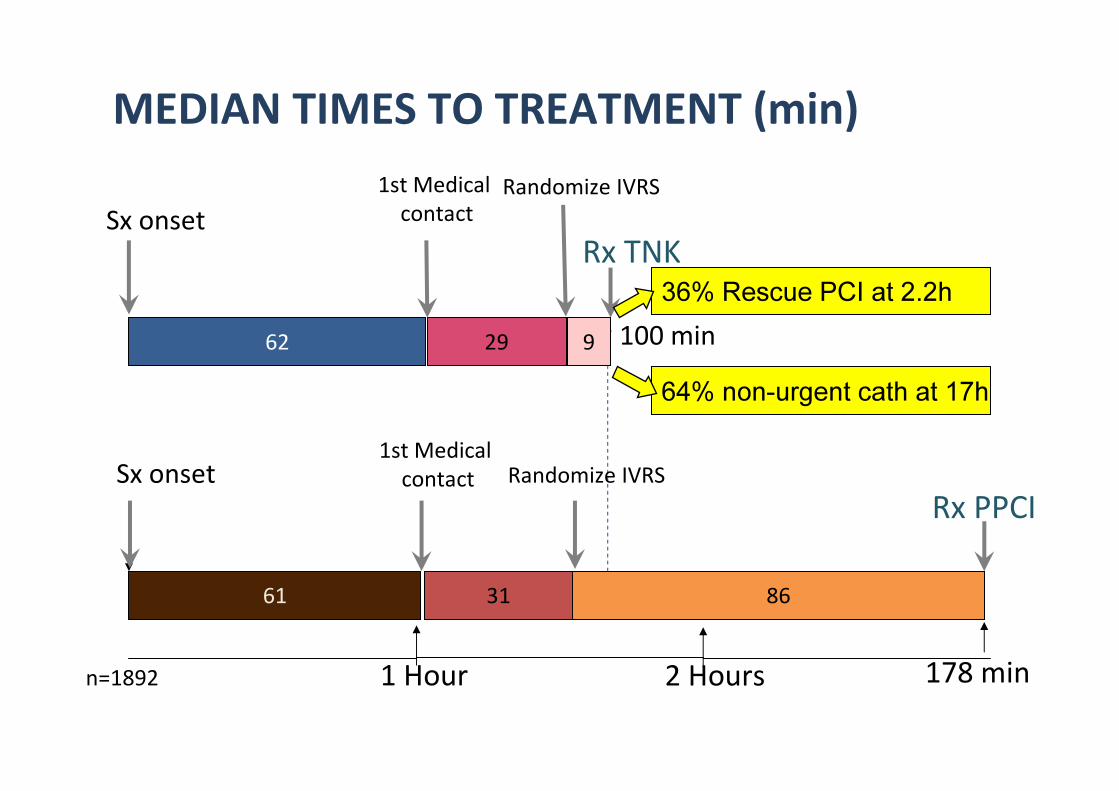
62
Sx onset
61
1 Hour 2 Hours
29 9
Rx TNK
31 86
Sx onset
Rx PPCI
100 min
178 min
MEDIAN TIMES TO TREATMENT (min)
36% Rescue PCI at 2.2h
n=1892
64% non-urgent cath at 17h
1st Medical
contactRandomize IVRS
1st Medical
contact Randomize IVRS
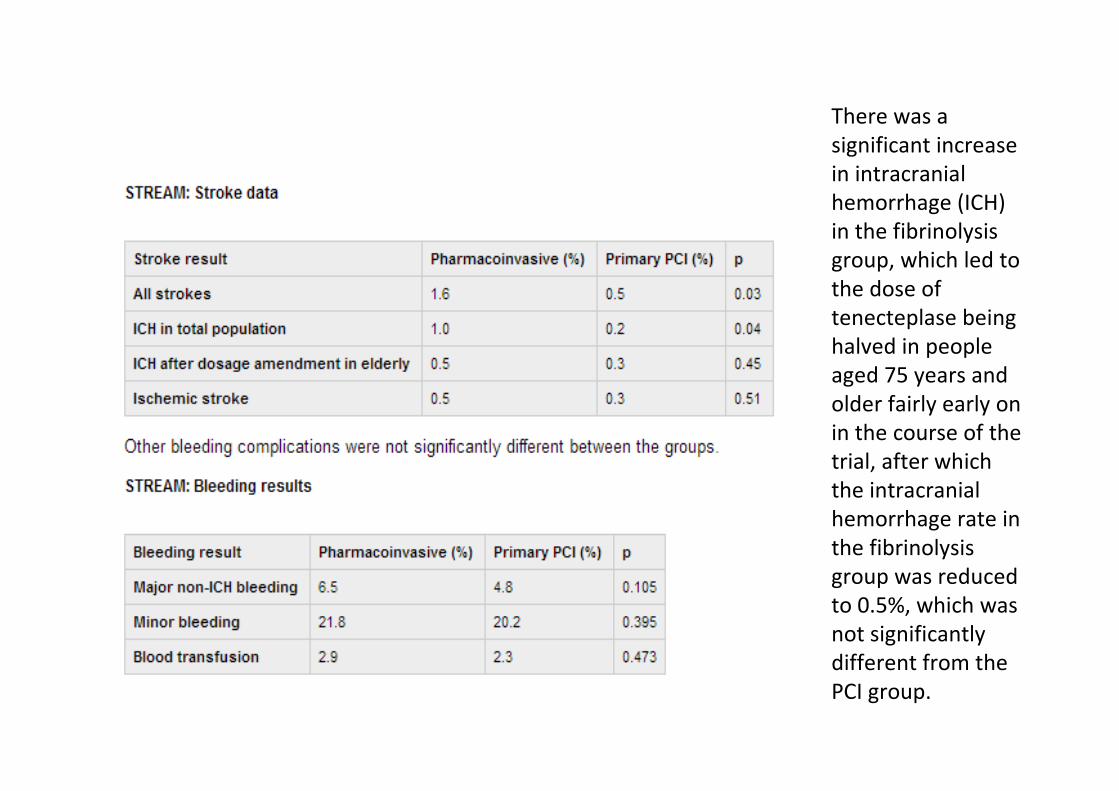
There was a
significant increase
in intracranial
hemorrhage (ICH)
in the fibrinolysis
group, which led to
the dose of
tenecteplase being
halved in people
aged 75 years and
older fairly early on
in the course of the
trial, after which
the intracranial
hemorrhage rate in
the fibrinolysis
group was reduced
to 0.5%, which was
not significantly
different from the
PCI group.
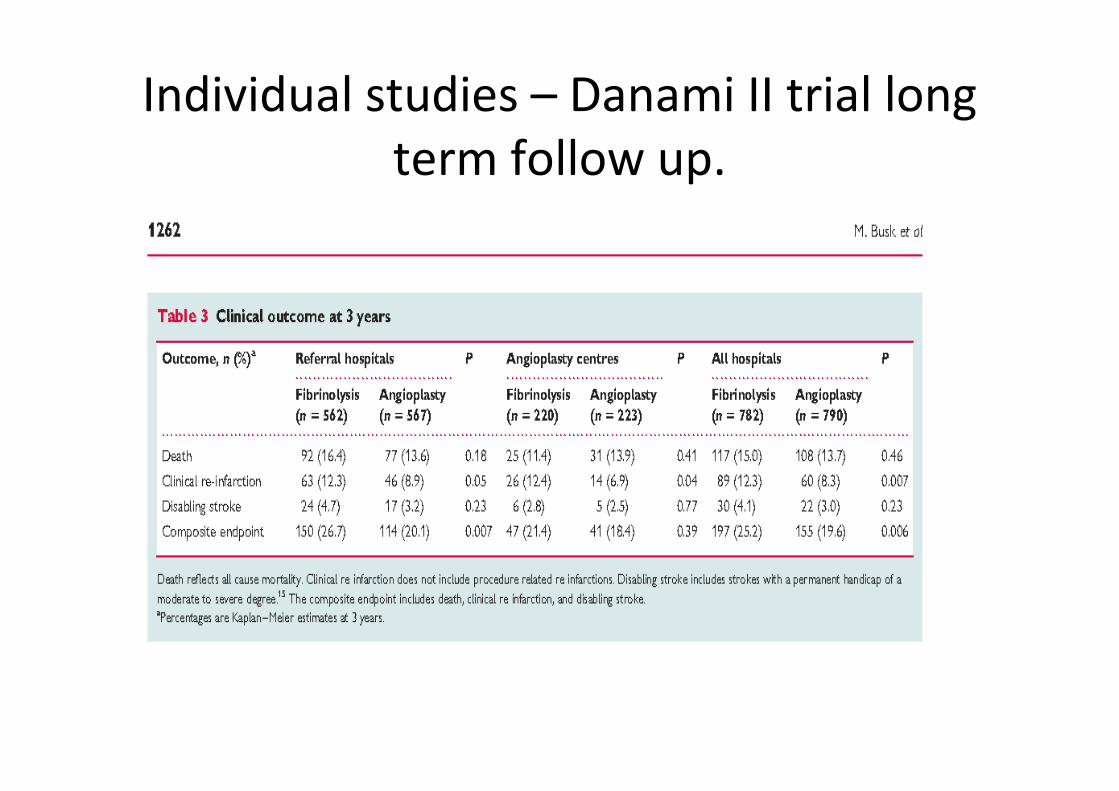
Individual studies – Danami II trial long
term follow up.
Long term follow up CAPTIM trial
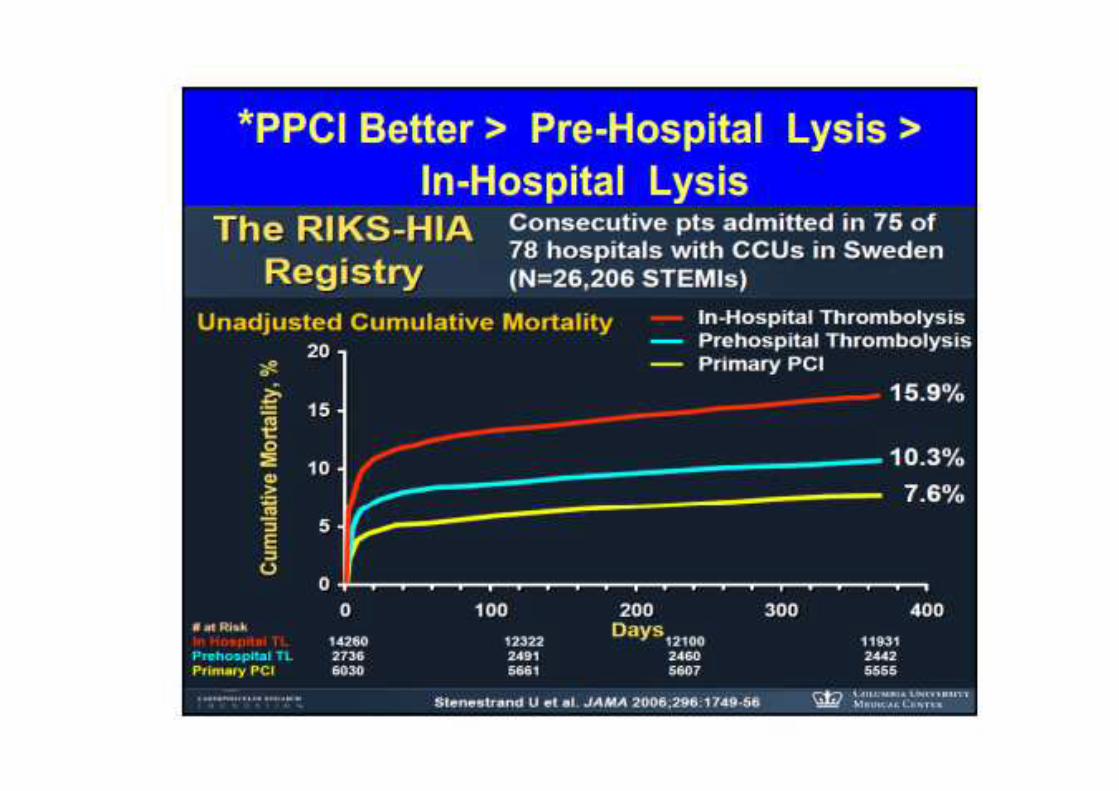
Prospective registries RIKS - HIA
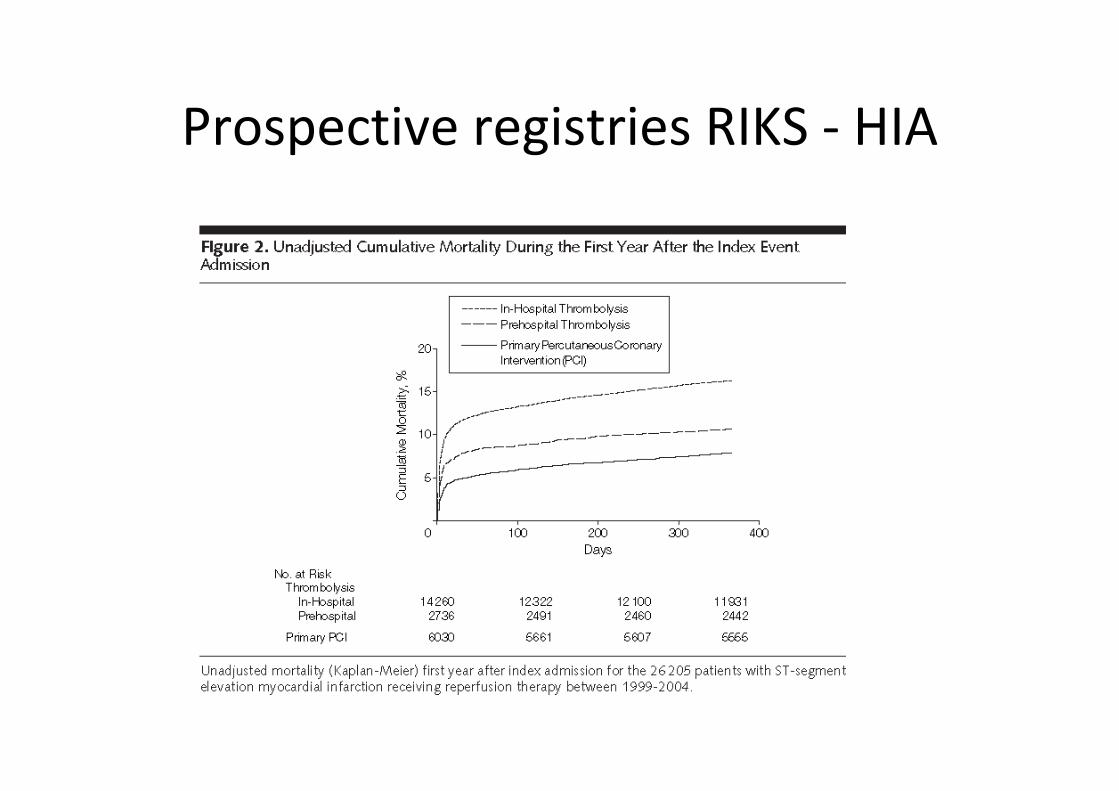
Prospective registries RIKS - HIA
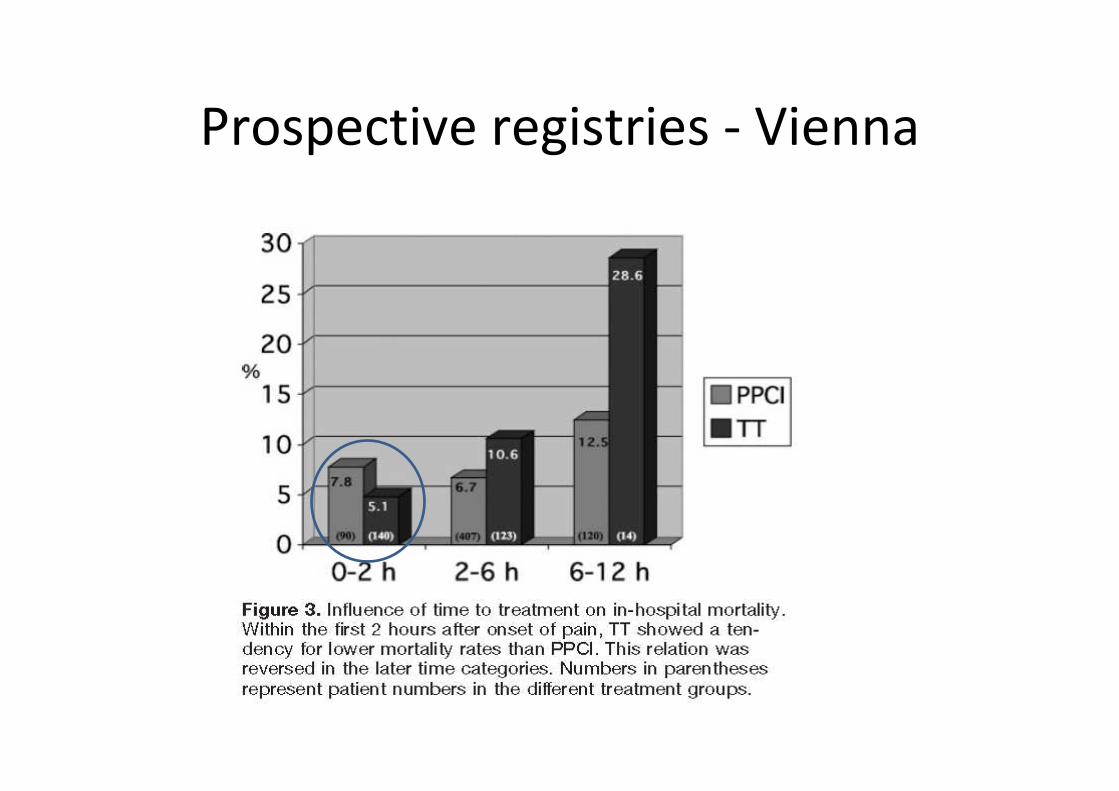
Prospective registries - Vienna
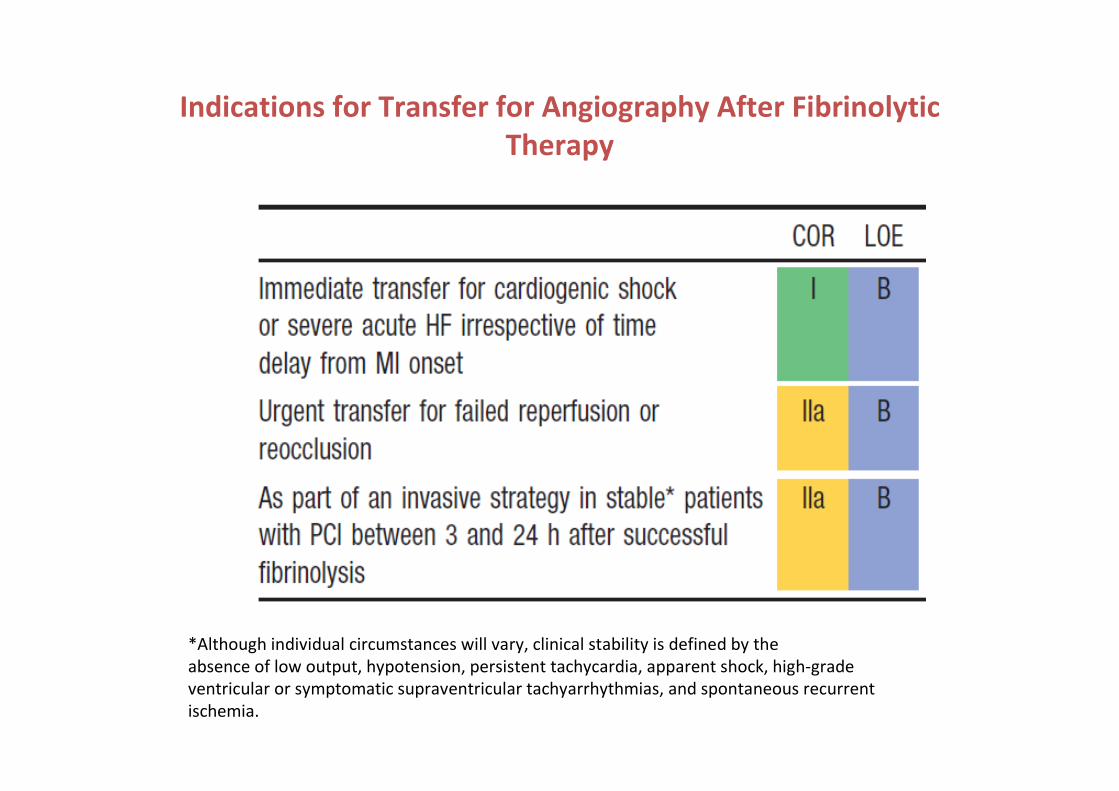
Indications for Transfer for Angiography After Fibrinolytic
Therapy
*Although individual circumstances will vary, clinical stability is defined by the
absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade
ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent
ischemia.
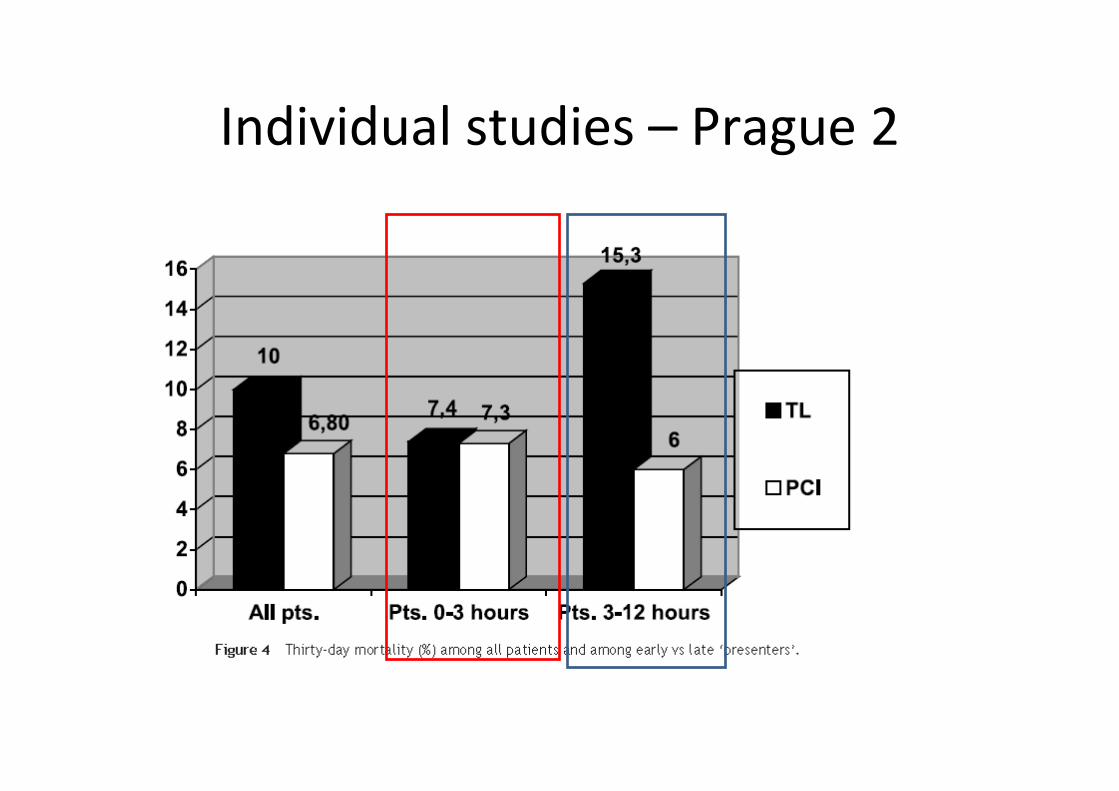
Individual studies – Prague 2








![PCI 10.6 1x1 BNC NoWindow 102 · Ø =4mm ~36 ~36 ~36 ~66 ~102 FOV [°], Ø =6mm ~36 ~36 ~36 ~88 ~124 TO39 detector package Bottom view Pin number Function 1(+), 2(-) signal 3 chassis](https://static.fdocument.org/doc/165x107/6101de4255b28b39da300aa1/pci-106-1x1-bnc-nowindow-4mm-36-36-36-66-102-fov-6mm-36-36.jpg)