Spontaneous closure of a stage III idiopathic macular hole
2
Click here to load reader
Transcript of Spontaneous closure of a stage III idiopathic macular hole

Spontaneous closure of a stage III idiopathic macular holeKelly D. Schweitzer,* BSc; Raúl García,† MD
ABSTRACT • RÉSUMÉ
Case report: We report spontaneous closure of an idiopathic 200 μm stage III macular hole, confirmed byoptical coherence tomography, in a 76-year-old woman.
Comments: Spontaneous closure is rare and not well understood. Possible mechanisms are discussed. Delayof surgery is not recommended.
Observation : Nous signalons la fermeture spontanée d’un trou maculaire idiopathique de 200 μm au stadeIII confirmé par la tomographie en cohérence optique chez une femme de 76 ans.
Commentaires : La fermeture spontanée est rare et on ne la comprend pas bien. Nous en examinons lesmécanismes possibles, mais ne recommandons pas de retarder la chirurgie.
This report outlines the progression of a spontaneousclosure of a full-thickness, stage III, macular hole.
The closure of traumatic macular holes has beenreported in the literature and various mechanisms havebeen suggested.1 The spontaneous closure of idiopathicmacular holes is less prevalent and less well understood.A literature search of EMBASE and MEDLINE pro-duced 13 articles addressing case reports of spontaneousclosure of idiopathic macular holes at various stages.One study that looked at the progression of idiopathicmacular holes reported that 3 of 35 patients (8.6%) witha follow-up of at least 6 years had spontaneous resolu-tion of their macular holes.2
CASE REPORT
A 76-year-old woman presented with a 2-week historyof decreased vision and metamorphopsia with her lefteye. Her ophthalmic history included a right retinaldetachment complicated with proliferative vitreo-retinopathy (PVR), resulting in complete loss of vision.Her past medical history included hypertension andpartial thyroidectomy. Her medications included lisino-pril and hydrochlorothiazide (Zestoretic) and alen-dronate (Fosamax).
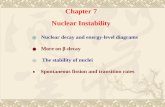
The ocular examination showed no light perceptionin the right eye and 20/60+ with near vision of J5 in herleft eye. Anterior segment examination showed a densecataract in the right and cortical opacities in the left eye.The intraocular pressure (IOP) was normal.Examination of the left posterior segment showed a 200μm stage III macular hole with a pseudo-operculum.Optical coherence tomography (OCT) images con-firmed the presence of a full-thickness macular hole(Fig. 1).
OCT classification of macular holes defines stage IIholes as continued attachment of the posterior vitreouscortex and the partially detached operculum. With stageIII holes, the posterior hyaloid has detached from themacular area.3 The absence of subretinal or intraretinalfluid on OCT suggested lack of traction by the vitreouson the parafovea, thus the patient was diagnosed with astage III hole.
The risks and benefits of surgery were discussed. Thepatient was hesitant to proceed with surgery because ofher monocular status. Four months after presentation,she was able to read again.
One month later, vision had improved to 20/30 withnear vision of J2. Clinically, the macular hole had
From *the College of Medicine, University of Saskatchewan, Regina, and†the Pasqua Hospital Eye Centre, Regina, Sask.
Originally received Nov. 4, 2005. Revised May 23, 2006Accepted for publication May 30, 2006
Correspondence to: Raúl García, MD, 1-4101 Dewdney Ave., Regina SKS4T 1A5; [email protected]
This article has been peer-reviewed. Cet article a été évalué par les pairs.
Can J Ophthalmol 2007;42:127–8doi:10.3129/can j ophthalmol.06-107
Spontaneous macular hole closure—Schweitzer & García 127
Fig. 1—Stage III idiopathic macular hole.

resolved spontaneously, and the OCT confirmed thatthe macular hole was closed (Fig. 2). A posterior vitre-ous detachment (PVD) was visible. Nine months afterinitial presentation, the vision was 20/25 with a nearvision of J1.
COMMENTS
In our patient, the posterior hyaloid appeareddetached from the macular area with OCT; thus, thepatient was diagnosed with a stage III idiopathicmacular hole. Four mechanisms have been suggested forthe spontaneous closure of these holes, including releaseof traction placed on the fovea by the detachment of theposterior hyaloid in the perifoveal area.3–7 Also consid-ered, cell proliferation to fill in the hole, bridging overof retinal tissue, and the formation of a contractileepiretinal membrane to close the hole.4,5,7 In our case, itis possible that a partial PVD over the macula waspresent with continued attachment of the vitreous to thedisc, explaining the lack of subretinal and intraretinalfluid in the original OCT image.
Since the posterior hyaloid had already fully detachedfrom the macular area when the hole was confirmed byOCT, release of vitreous traction does not explain thespontaneous resolution of this hole. Considering thesmall size of the macular hole and having excludedrelease of anteroposterior traction, we propose thatbridging of the gap by glial cell proliferation was the
mechanism of closure for this stage III macular hole.Despite the resolution of the idiopathic macular hole
in this patient’s case, delaying surgery is not recom-mended. Spontaneous closure is rare, and the longer anidiopathic macular hole remains open, the smaller theimprovement in vision that can be expected after treat-ment.8
The authors would like to thank Medical Media Services ofthe Pasqua Hospital in Regina, Saskatchewan, for their help inpreparation of the images.
Supported by the University of Saskatchewan, College ofMedicine. The authors have no financial interest in any aspectof this study.
REFERENCES
1. Menchini U, Virgili G, Giacomelli G, Cappelli S, GiansantiF. Mechanism of spontaneous closure of traumatic macularhole: OCT study of one case. Retina 2003;23:104–6.
2. Chew EY, Sperduto RD, Hiller R, et al. Clinical course ofmacular holes: the Eye Disease Case-Control Study. ArchOphthalmol 1999;117:242–6.
3. Tadayoni R, Massin P, Haouchine B, Cohen D, Erginay A,Gaudric A. Spontaneous resolution of small stage 3 and 4 full-thickness macular holes viewed by optical coherence tomog-raphy. Retina 2001;21:186–9.
4. Guyer DR, de Bustros S, Diener-West M, Fine SL.Observations on patients with idiopathic macular holes andcysts. Arch Ophthalmol 1992;110:1264–8.
5. Freund KB, Ciardella AP, Shah V, Yannuzzi LA, Fisher YA.Optical coherence tomography documentation of sponta-neous macular hole closure without posterior vitreous detach-ment. Retina 2002;22:506–9.
6. Hikichi T, Yoshida A, Akiba J, Trempe CL. Natural outcomeof idiopathic macular hole. Nippon Ganka Gakkai Zasshi1995;99:445–9.
7. Lewis H, Cowan GM, Straatsma BR. Apparent disappear-ance of a macular hole associated with development of anepiretinal membrane. Am J Ophthalmology 1986;102:172–5.
8. Ishida M, Takeuchi S, Okisaka S. Optical coherence tomog-raphy images of idiopathic macular holes with spontaneousclosure. Retina 2004;24:625–8.
Key words: optical coherence tomography, idiopathic macularhole, spontaneous closure, posterior vitreous detachment
Spontaneous macular hole closure—Schweitzer & García
128 CAN J OPHTHALMOL—VOL. 42, NO. 1, 2007
Fig. 2—Optical coherence tomography imagedisplaying complete resolution of macular hole,9 months after initial presentation.



![elasticity and locality of -closure - arXiv · elasticity tensors. In contrast to these, our approach is completely variational, resembling the classical-convergence method [5, 9],](https://static.fdocument.org/doc/165x107/5fdd8789834b4e5f8e71bc9e/elasticity-and-locality-of-closure-arxiv-elasticity-tensors-in-contrast-to-these.jpg)





![Local function vs. local closure function · Local function vs. local closure function ... Let ˝be a topology on X. Then Cl (A) ... [Kuratowski 1933]. Local closure function](https://static.fdocument.org/doc/165x107/5afec8997f8b9a256b8d8ccd/local-function-vs-local-closure-function-vs-local-closure-function-let-be.jpg)