Rationale for combined α–β–adrenoceptor blockade: haemodynamic considerations
6
87 Rationale for combined a-P-adrenoceptor blockade: haemodynamic considerations Giinter Koch Department of Clinical Physiology, Centrallasarettet, Karlskrona, Sweden, and Department of Physiology, Free University of Berlin, West-Berlin ABSTRACT. Increased peripheral vascular resist- ance is the cause of elevated blood pressure in most forms of systemic hypertension. Both structural changes in response to increased wall stress and functional alterations in vascular smooth muscle itself appear to contribute to the elevated resistance. As mediators of the vasoconstrictor responses, a- adrenoceptors apparently play an important if not predominant role in the initiation and/or mainten- ance of high resistance and pressure. In contrast to B-receptor blockade alone, com- bined a-&receptor blockade lowers blood pressure predominantly by a-receptor-mediated reduction of the systemic vascular resistance, both when induced acutely and, in particular, during long-term administration. Cardiac output is maintained at pre- treatment level, as is left ventricular tilling pressure. Since a well-balanced blockade of both a- and p- receptors counteracts the pathophysiological changes causing and/or maintaining hypertension and tends to restore cardiovascular dynamics towards normal, combined a-B-receptor blockade appears at present to be one of the most logical and rational therapeutic approaches to hypertension. Interpretation of the haemodynamic effects of agents that interfere with adrenoceptors in the heart and the vascular system is complicated by a number of difficulties. The most important one relates to the fundamental principle of maintenance of homeos- tasis which is characteristic of the intact organism: any interference with cardiovascular regulation has immediate reflex effects throughout the circulation, aimed at counteracting the primary changes. The haemodynamic alterations observed after such an intervention are thus the net effect of both primary changes and secondary adjustment. Hence, it is dif- ficult, if not impossible, to dissect the global haemodynamic response into its component sources. However, despite these limitations, an analysis of the overall haemodynamic response is extremely important since it enables us, at worst, to evaluate the usefulness of a given intervention in relation to a specific pathophysiological or disease state. SOME PATHOPHYSIOLOGICAL ASPECTS OF HYPERTENSION As a basis for proper analysis of the haemodynamic effects induced by combined a-D-receptor blockade and discussion of its usefulness, it appears mandat- ory to recall some essential physiological and pathophysiological features characteristic of the hypertensive process: 1. From the haemodynarnic point of view, the natural history of hypertension is characterised by a gradual change from the early normo- or hyperkine- tic pattern to the high-resistance hypokinetic pat- tern (6, 16, 17). However, even in the young hyper- tensive, peripheral resistance during heavy exercise does not fall to as low a level as in age-matched normotensives, and, under the same conditions, cardiac output is no longer high but rather subnor- mal. This strongly suggests that functional changes in the precapillary resistance vessels, resulting in increased flow resistance, are the earliest and pre- dominant haemodynamic alterations in hyperten- sion. 2. Many observations suggest that increased adrenergic activity plays an important role in the haemodynamic changes in hypertension, at least in its initial stage (15). Adrenergic hyperactivity, in terms of increased plasma catecholamine levels, has been repeatedly shown to prevail in most hyperten- sives under resting conditions (4, 15). In a study comparing young hypertensives with carefully age- matched normotensives (13) it was found that adreno-sympathetic activity, as measured by plasma noradrenaline, was distinctly higher in the hyper-
-
Upload
guenter-koch -
Category
Documents
-
view
216 -
download
2
Transcript of Rationale for combined α–β–adrenoceptor blockade: haemodynamic considerations

87
Rationale for combined a-P-adrenoceptor blockade: haemodynamic considerations
Giinter Koch
Department of Clinical Physiology, Centrallasarettet, Karlskrona, Sweden, and Department of Physiology, Free University of Berlin, West-Berlin
ABSTRACT. Increased peripheral vascular resist- ance is the cause of elevated blood pressure in most forms of systemic hypertension. Both structural changes in response to increased wall stress and functional alterations in vascular smooth muscle itself appear to contribute to the elevated resistance. As mediators of the vasoconstrictor responses, a- adrenoceptors apparently play an important if not predominant role in the initiation and/or mainten- ance of high resistance and pressure.
In contrast to B-receptor blockade alone, com- bined a-&receptor blockade lowers blood pressure predominantly by a-receptor-mediated reduction of the systemic vascular resistance, both when induced acutely and, in particular, during long-term administration. Cardiac output is maintained at pre- treatment level, as is left ventricular tilling pressure.
Since a well-balanced blockade of both a- and p- receptors counteracts the pathophysiological changes causing and/or maintaining hypertension and tends to restore cardiovascular dynamics towards normal, combined a-B-receptor blockade appears at present to be one of the most logical and rational therapeutic approaches to hypertension.
Interpretation of the haemodynamic effects of agents that interfere with adrenoceptors in the heart and the vascular system is complicated by a number of difficulties. The most important one relates to the fundamental principle of maintenance of homeos- tasis which is characteristic of the intact organism: any interference with cardiovascular regulation has immediate reflex effects throughout the circulation, aimed at counteracting the primary changes. The haemodynamic alterations observed after such an intervention are thus the net effect of both primary changes and secondary adjustment. Hence, it is dif- ficult, if not impossible, to dissect the global haemodynamic response into its component sources. However, despite these limitations, an analysis of the overall haemodynamic response is
extremely important since it enables us, at worst, to evaluate the usefulness of a given intervention in relation to a specific pathophysiological or disease state.
SOME PATHOPHYSIOLOGICAL ASPECTS OF HYPERTENSION
As a basis for proper analysis of the haemodynamic effects induced by combined a-D-receptor blockade and discussion of its usefulness, it appears mandat- ory to recall some essential physiological and pathophysiological features characteristic of the hypertensive process:
1. From the haemodynarnic point of view, the natural history of hypertension is characterised by a gradual change from the early normo- or hyperkine- tic pattern to the high-resistance hypokinetic pat- tern (6, 16, 17). However, even in the young hyper- tensive, peripheral resistance during heavy exercise does not fall to as low a level as in age-matched normotensives, and, under the same conditions, cardiac output is no longer high but rather subnor- mal. This strongly suggests that functional changes in the precapillary resistance vessels, resulting in increased flow resistance, are the earliest and pre- dominant haemodynamic alterations in hyperten- sion.
2 . Many observations suggest that increased adrenergic activity plays an important role in the haemodynamic changes in hypertension, at least in its initial stage (15). Adrenergic hyperactivity, in terms of increased plasma catecholamine levels, has been repeatedly shown to prevail in most hyperten- sives under resting conditions (4, 15). In a study comparing young hypertensives with carefully age- matched normotensives (13) it was found that adreno-sympathetic activity, as measured by plasma noradrenaline, was distinctly higher in the hyper-

88
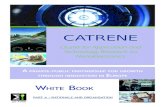
Fig. 1 . Means and standard deviations of plasma norad- renalinc in a group of n o r - motensivc young adults (n= 16) and a group of age- matched WlIO-st;ige 1 hypcrtcnsivcs (n=14) ;it rest supine (SUP) and upright (UPR) , and during stendy- state ergometer exercise. (sitting ) a t d i ffcrc n t work loads (W,: 50. w,: 100. w,: 150. w.,: 700 Watts) and after exercise again i n thc supine position Asterisks denote levels of statistical significance ol mean differ- cnccs bctwccn the two groups. ( * : p<O.OS, * * : p c o . 0 I , * * *p<o.oo I ).
tensives at rest in the supine and particularly in the upright position, and during submaximal exercise but not during high-intensity exercise (Fig. 1). Since the effects of noradrenaline are mediated via n- receptors, these findings suggcst that the u- adrenoceptors in the vascular smooth muscle play an important role in initiating and/or maintaining abnormally high vascular resistance and blood pressure.
3. Studies in animals and in man have shown that increased intravascular pressure not only promotes a-receptor-mediated precapillary vasoconstriction but leads above all t o structural changes in the pre- capillary resistance vessels. consisting of a reduction of the internal vessel diameter and an increase in the wall-lumen ratio ( 5 ) . The main effect of these changes is an alteration of the background upon which vasoconstrictor influences operate. Thus, they not only imply increased vascular resistance under basal vasomotor tone but also result in a hyperreactivity of these vesseles, with an exagger- ated constrictor response to a given smooth muscle activation. The consequent rise in average trans- mural pressure in turn intensifies the structural changes, creating some kind of positive feedback interaction. Another type of structural change which has been proposed to contribute to increased
vascular resistance in hypcrtcnsion is rarefaction of resistance vessels (9). 4. Recent evidence supports the concept that
changes in vascular smooth muscle cells themselves contribute to increased systemic vascular resistance (21). These changes are expressed functionally as increased sensitivity to vasomotor stimuli mil diminshed relaxation. Abnormalities in cyclic nuc- leotide metabolism, calcium metabolism. niein- brane permeability, membrane transport and elec- trogenesis have been proposed to be involved. Since altered membrane function has also been shown to occur in other cells in hypertension. it may be that ;I
general membrane disorder causes the increased vascular smooth muscle sensitivity responsible for increased resistance (cf. 21).
5. Adaptive hypertrophic wall changes, in response to the increased pressure load. occur not only in the precapillary resistance vessels but also in the conduit arteries and, in particular, i n the left heart. As a consequence, left ventricular diastolic compliance is reduced and a higher filling pressure is needed t o generate the same stroke volume as the normotensive heart (6, 8). Histologically, chronic pressure overload, a t least of the type seen in aortic stenosis, results in an increase in non-contractile tissue and a relative decrease in contractile tissue

89
(20), as well as in abnormalities in myocardial fibre arrangement as demonstrated by echocardiography in patients with essential hypertension (7) . The functional abnormalities of the hypertensive heart may be related to these structural changes, as has been demonstrated in patients with aortic stenosis (20).
RATIONALE FOR COMBINED
While it thus at present appears difficult, if not impossible, to define the prime mechanism that initiates the hypertensive process, the most impor- tant pathophysiological changes occurring during its course are well established. I t should thus be poss- ible to define the most rational and logical therapeutic approach: the one most likely to reverse the pathophysiological changes induced by the dis- ease process.
In order to counteract the pathophysiological consequences of hypertension, the most logical approach would evidently be to inhibit further rise or, preferably reverse the elevated vascular resist- ance towards normal and, with respect to left ven- tricular function, to decrease the load of the left ventricle. Since the noradrenaline effects and vaso- constrictor responses in the precapillary resistance vessels are mainly mediated thorugh a-adrenocep- tors, blockade of the a-receptors would appear, at least on theoretical grounds, to be the most logical and efficient way of lowering precapillary resistance and counteracting the vicious circle ensuring from the interaction of intravascular pressure rise, func- tional excitatory influences and structural changes.
The combination of an a-receptor antagonist with a ,!&receptor blocking agent appears rational for two main reasons: First, in contrast to P-receptor block- ade alone, blood pressure can be expected to be lowered predominantly by a reduction of systemic vascular resistance, while a possible baroreceptor- mediated reflex increase of cardiac output would be attenuated or prevented by the P-blocking compo- nent. Second, the activation of the renin-angioten- sin system generally seen after vasodilation and/or a-receptor blockade would be suppressed; the addi- tional reduction of blood pressure often achieved by adding a P-receptor antagonist to a vasodilator has actually been postulated to be dependent on a renin-suppressing action of the B-receptor antagon- ist in this situation (17).
a-B-RECEPTOR BLOCKADE
HAEMODYNAMIC EFFECTS OF COMBINED a-P-BLOCKADE WITH LABETAL.OL
The mode of action of combined a-e-adrenoceptor blockade on cardiovascular dynamics will be discus- sed on the basis of results obtained with labctalol
Labetalol constitutes a unique compound in this context since it combines in the same molecule an a- adrenoceptor blocking action, predominantly at the postsynaptic ( a l ) site, with P-adrenoceptor antagonistic properties ( 2 ) . The P-receptor antagon- ist component is non-selective but has membrane stabilizing properties. Based on observations of its effect on fetal lung maturation, labetalol has recently been claimed to possess intrinsic sympathe- tic activity, mainly with respect to Pz-adrenoceptors
While the preferential blocking action of labetalol on postjunctional al-receptors might theoretically be an advantage, the type of a-receptor that is antagonized by labetalol does not really appear cru- cial in relation to its haemodynamic effects: due to its P-receptor blocking properties, any baroreflex- mediated tachycardia and increase of cardiac out- put, as seen with prejunctional a-receptor antagon- ists such as phentolamine, would be attenuated or
(10, 11, 12).
( 1 9 .
Table I . Means, standard deviations ( S D ) und ranges of systemic arterial blood pressures before and their mean (D) and percentage ( D 96) changes after intravenous administration of labetalol, 50 m g , at rest in the supine ( S ) and the upright ( U ) position, and during exercise at two different work 1oad.s ( W , and W2). ***: p<0.001.
- - Mean S. D. Range D D %
Brachial ariery: Systolic pressure S 174 32 U 179 35 w, 202 34 Wz 241 34 Diastolic pressure S 97 15 U 108 19 w, 101 16 WZ 113 24 Mean pressure S 126 18 U 136 23 W, 143 20 Wz 163 28
144- 247 148- 247 157-261 177-294
87- 115 88- 123 87- 126 85- 144
112- 144 116- 162 106-165 131 -209
-33*** -19.0*** -6o* * * - 33 .s * * * - ( ) I * * * -30.2** * -MI** -35.3***
-14*** - IJ,J*** -35*** -32.4"' -24*** -23.8*** -36*** - 3 1 . Y * * *
-22*** - l7.5*** -42* * * - 30.9* * * - 40* * * - 2X. O* * * -52*** -31,9***

90
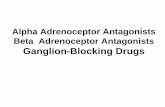
Fig. 2. Percentage changes from pretreatment values of some haemodynaniic vari- ables at rest and during exer- cise after intravenous administration of labetalol 50 mg (10). MSP: mean sys- tematic pressure, HR: heart rate, v#,2: oxygen uptake, AVO2: arterio-mixed venous oxygen difference, CO: cnr- diac output, SV: stroke vol- ume, TPR: total peripheral resistance. *:p<0.05, **p<0.01, * * * : p<O.O01.
inhibited. Moreover, the P-receptor blocking coni- ponent should decrease the plasma renin activity since renin secretion is at least partly mediated by renal P-receptors. In a series of haemodynamic studies (10, 11, 12) we were able to demonstrate that labetalol not only produces effects on car- diovascular dynamics and plasma renin activity, in accordance with what could be anticipated from its pharmacological profile, but that the balance bet- ween a- and P-receptor blocking activity is very appropriate in most cases.
Thirteen patients (12 men and 1 woman, mean age 52 years) participated in the acute investigation. Nine male patients agreed to be studied again after almost two years of treatment with oral labetalol in
an average dose of 900 mg daily. Throughout these investigations identical methods were used: blood pressures in the brachial artery and in the pulmo- nary circulation were recorded via catheters that had been introduced percutaneously ; cardiac output was measured according to the Fick principle. On each occasion, the patients were studied at rest in the supine and upright position and during steady- state bicycle ergometer exercise in the seated posi- tion with two different work loads, corresponding to approximately 60 and 120 Watts.
Acute administration of labetalol. 50 mg intravenously, induced a significant fall in systemic blood pressure under all conditions (Table 1. Fig. 2 ) . I t was due to a reduction of both systemic vascu-
Fig. 3. Percentagc changes from pretreatment values 0 1 some haemodynaniic vari- ables at rest and during exer- cise after 20 months d oral treatment with labetalol, average daily dose YO0 mg (11). Abbreviations and sym- bols as in Fig. 2.

91
1%
lo0
50
0
Heart rate
I
0 Supine
0 Upright
6 Exercise 1 2 l t 2 7 W
0 iv oral
( ml 1 5 0 .
100-
50
0
Stroke volume
0 iv oral
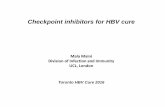
Fig. 4. Means and standard deviations of heart rate and stroke volume in the supine (0) and upright (0 ) resting positions and during exercise at 1212 27 W (A) before (0) and after acute intravenous and long-term oral treat- ment with labetalol.
lar resistance and cardiac output. The decrease of cardiac output was entirely due to reduction of heart rate. The arterio-mixed venous oxygen differ- ence changed inversely with the alterations of car- diac output. After a 20-month period of oral treat- ment, the reduction of blood pressure was largely maintained, but was now entirely due to a decrease in systemic vascular resistance, while cardiac output had reverted to pre-treatment levels (Fig. 3). The rise in cardiac output was due to an increase in stroke volume which entirely counterbalanced the fall in heart rate (Fig. 4). This effect was particularly marked in the upright position. After long-term oral treatment, the stroke volume in the upright position was actually of the same order as the supine stroke volume prior to treatment. This explains why post- ural hypotension, which frequently occurred after the acute administration of labetalol, had practically disappeared during the course of oral treatment.
It is evident that the haemodynamic pattern induced by labetalol is significantly different from that seen after /?-receptor blockade, in particular with respect to cardiac output and systemic vascular resistance. These particular haemodynamic effects can only be explained by a substantial a-receptor blocking effect in addition to the /?-receptor antagonistic action.
The tendency of labetalol to induce orthostatic hypotension in the acute experiment can also only be explained by additional a-receptor blockade and suggests that the a-blocking effect is not confined to
the precapillary resistance vessels but extends also to the postcapillary vessels. In the erect position, this would allow a shift of blood volume from the intrathoracic to the extrathoracic compartment of the capacitance system. Increased venous distensi- bility after acute intravenous administration of labetalol has actually been described (1). The attenuation of symptoms and signs of postural hypotension in the course of treatment suggests that the a-adrenoceptor blocking effect of labetalol on the capacitance vessels may be modulated by long- term oral treatment. It is well established that phar- macological intervention, including a- and B-recep- tor agonists and antagonists, may induce function- ally significant changes in the density and/or respon- siveness of both a- and /I-receptors (3).
In view of the early interference of the hyperten- sive process with left ventricular function, it is of special interest to analyse more closely the effects of combined a-B-receptor blockade by labetalol on left ventricular dynamics. From Fig. 5 it is evident that intrapulmonary pressures, including left ventricular filling pressures, and left ventricular performance characteristics in terms of the Starling relationship (stroke volume/filling pressure ratio) are not sig- nificantly altered (12). This clearly suggests that the negative inotropic effect of the b-receptor blocking component is counterbalanced by the concomitant a-receptor blockade. While this might not be essen- tial in the young and middle-aged hypertensive with largely intact circulatory function, this property should represent an important advantage to the patient exhibiting, or prone to, deterioration of car- diac function. It is well established that p-receptor blockers may have negative effects on left ventricu- lar dynamics in this type of patient, while beneficial effects on preload are generally observed when a suitable vasodilator is added (cf. 14).
Concerning left ventricular oxygen requirements as evaluated from the pressure-rate product. com- bined a-b-receptor blockade has at least the same beneficial effects as have been demonstrated for simple b-receptor blockers (12).
CONCLUSIONS Combined a-/?-adrenoceptor blockade lowers blood pressure predominantly by a-receptor-mediated reduction of the systemic vascular resistance, both when induced acutely and during long-term administration. Due to its ,!l-receptor blocking com-

92
150 - (ml)
100
sv
oral
8
"1 0 Supine 0 Upright A Exercise 121227W
0 0 5 10 15 (mmHg)
Fig. 5. Relationship between stroke volume (SV) and left ventricular filling pressure (LVFP) before (0) and after intravenous and long-term oral treatment with labetalol. Symbols as in Fig. 4.
ponent, any increase of cardiac output is inhibited: cardiac output is usually maintained at pre-treat- ment levels, as are left ventricular filling pressures.
Since a well-balanced blockade of both a- and p- receptors counteracts the pathophysiological changes responsible for, and maintaining, hyperten- sion, and tends to restore cardiovascular dynamics towards normal, combined a-p-receptor blockade appears at present to be one of the most logical and rational therapeutic approches to hypertension.
REFERENCES I . Bahlmann, J . , Brod, J . , Hubrich, W. , Cschovan, M.
& Pretschner, P.: Effect of an a- and/I-adrenoceptor- blocking agent (labetalol) on haemodynamics in hypertension. Br. J . Clin. Pharmac. (suppl) 8: 113. (1979).
2. Brogden, R. N. , Heel, R . C . , Speight, T. M B Avery, G. S.: Labetalol: A review of it5 pharmacol- ogy and therapeutic use in hypertension. Drugs 15: 251 (1978).
3. Brunner, H.: Modulation of sympathetic tone at the neuroeffector level. In: Modulation of sympathetic tonc in the treatmcnt of cardiovascular diseases. Ed. Gros., F. Hans Huber Publishers, Bern, 1978.
4. De Champlain. J . , Forley, L., Cousineau, D. B van Ameringen, M. R. : Circulating catecholamine lcvels in human and experimental hypertension. Circ. Res.
5 . Folkow, B.: Cardiovascular structural adaptation; its role in the inhibition and niaintcnancc of primary hypertension. Clin. Sci. Mol. Med. 55: 3 (1978).
6 . Freis, E. D . : Hemodynamics in hypcrtcnsion. Phys. Rev. 40: 27 (1960).
7. Gibson, D.: Personal Communication. 8. Hallback, M.: Interaction between central
neurogenic mechanisms and changes in cardiovascu- lar design in primary hypertension. Experimental studies in spontaneously hypertensive rats. Acta Physiol. Scand. (suppl) 424 (1975).
10. Koch, G.: Acute hemodynaniic effects of an u- and /j-receptor blocking agent ( A H 5158) on the systemic and pulmonary circulation at rest and during exercise in hypertensive patients. Am. Hcart J . 93: 5x5 (1977).
1 I . Koch, G.: Hernodynamic adaptation at rest and dur- ing exercise to long-term antihypertensive treatment with combined a-and b-adrenoreceptor blockade by labetalol. Br. Heart J . 41: 192 (1979 a) .
12. Koch, G . : Cardiovascular dynamics aftcr acutc and long-term u- and P-adrenoreceptor blockade at rest. supine and standing, and during exercise. Brit. J . Clin. Pharmac. (suppl) 8, 101 (1979 b).
13. Koch, G . : Exercise adreno-sympathetic activity in essential hypertension. Pfliigers Archiv (European J . of Physiology) 379: R 35 ( 1979 c ) .
14. Koch, G . : Hernodynamic changes after acute and long-term combined a-/]-adrenoreceptor blockade with lahetalol as compared with /I-receptor blockade. J . Cardiovasc. Pharmacol. 3 (suppl. 1): S 30 (1981).
15. Kuchel, 0.: Autonomic nervous system in hypertcn- sion: clinical aspects. In: Hypertension. Phy- siopathology and treatment. Ed . Genest. J . . Kolw, E . B Kuchel, 0. McGraw-Hill Book Company, New York 1977.
16. Lund-Johansen, P.: Hemodynamics in early essential hypertension. Acta Med. Scand. (Suppl) 428: I ( 1967).
17. Lund-Johansen, P . : Central hemodynarnics in essen- tial hypertension. Acta Med. Scand. (Suppl) 606: 35 (1977).
18. Pettinger, W.A. and Mitchell, M.C.: Renin release. saralasin and the vasodilator P-blocker drug intcrac- tion in man. New Eng. J . Med. 292: 1214 (1975).
19. Riley, A . J . : Clinical pharmacology of labctolol i n pregnancy. J . Cardiovasc. Pharmacol. 3 (suppl. I ) : S
20. Schaper, J . , Schwarz, F. & Hehrlein, F. : tiltrastruk- turelle Verinderungen im menschlichen Myokard bei Hypertrophie durch Aortenklappenfehler und deren Beziehung zur linksventrikularen Masse und Auswurfsfunktion. Herz 6: 217 (1981).
21. Webb, R. C. B Bohr, D . F.: Recent advances in the pathogenesis of hypertension: Consideration of structural, functional and metabolic vascular abnor- malities resulting in elevated arterial resistance. Am. Heart J . 102(2): 251 (1981).
SR: 109 (1976).
53 (1981).