Prediction of efficacy to pegylated interferon-α-2b plus ribavirin in patients with genotype 2...
8
Click here to load reader
Transcript of Prediction of efficacy to pegylated interferon-α-2b plus ribavirin in patients with genotype 2...

Original Article
Prediction of efficacy to pegylated interferon-a-2b plusribavirin in patients with genotype 2 hepatitis C virus usingviral response within 2 weeks
Yuki Wada,1 Hideyuki Tamai,1 Akiko Uno,2 Akira Kawashima,2 Naoki Shingaki,1
Yoshiyuki Mori,1 Kosaku Moribata,1 Kaori Miyata,2 Katsuhiko Higashi,3 Hisanobu Deguchi,1
Kazuki Ueda,1 Izumi Inoue,1 Takao Maekita,1 Mikitaka Iguchi,1 Jun Kato1 andMasao Ichinose1
1Second Department of Internal Medicine, Wakayama Medical University, 2Department of Internal Medicine,Naga Municipal Hospital, and 3First Department of Internal Medicine, Hidaka General Hospital, Wakayama,Japan
Aim: Rapid virological response (RVR), defined as serumhepatitis C virus (HCV) RNA negativity at 4 weeks, is the mostuseful predictor of sustained virological response (SVR) tostandard pegylated interferon (PEG IFN) plus ribavirin therapyfor patients infected with genotype 2 HCV. The aim of thepresent study was to predict SVR using viral response within2 weeks of therapy initiation.
Methods: Of 64 HCV genotype 2 patients with a high viralload treated with standard PEG IFN-a-2b plus weight-basedribavirin for 24 weeks, 58 patients whose adherence wasmore than 67% were analyzed. RNA and core antigen levelswere measured at four time points: the day of therapy initia-tion, the following day, and at 1 and 2 weeks.
Results: SVR was achieved in 73% (47/64) of patients.Univariate analysis of SVR contributing factors showed signifi-cant differences with age, bodyweight, white blood cell
count, platelet count, fibrosis marker levels, baseline coreantigen level and viral response. The area under the receiver–operator curve (AUC) of the core antigen level at 1 week (AUC,0.940) was the highest among the significant SVR predictingfactors. Setting 100 fmol/L as the cut-off value for coreantigen level at 1 week, the sensitivity, specificity, positivepredictive value, negative predictive value and accuracy forpredicting SVR were 100%, 86%, 96%, 100% and 97%, respec-tively, and for predicting RVR were 66%, 93%, 97%, 46% and72%, respectively.
Conclusion: The HCV core antigen level at 1 week aftertherapy initiation is the most useful predictor for SVR.
Key words: hepatitis C core antigen, pegylatedinterferon-a-2b, prediction, ribavirin, sustained virologicalresponse
INTRODUCTION
HEPATITIS C VIRUS (HCV) infection is one of themajor causes of liver cirrhosis and hepatocellular
carcinoma. The primary goal of therapy for patientsinfected with HCV is achievement of a sustained viralresponse (SVR). Viral elimination can reduce the risk ofcarcinogenesis and resolve histological fibrosis.1 The
current standard therapy for HCV patients is pegylatedinterferon (PEG IFN) plus ribavirin. The response toIFN-based therapy differs according to HCV genotypeand baseline HCV RNA levels. Patients with genotype 2HCV have a better response compared to those withgenotype 1 HCV. Following current guidelines for treat-ment of HCV infection,2–5 SVR is expected in approxi-mately 80% of patients with HCV genotype 2 aftertreatment with PEG IFN plus ribavirin for 24 weeks;however, approximately 20% of patients will notachieve SVR.
When considering treatment strategies, prediction ofSVR is important before starting antiviral therapy;however, accurate prediction of treatment outcome inpatients with HCV genotype 2 has not been established.
Correspondence: Dr Hideyuki Tamai, Second Department of InternalMedicine, Wakayama Medical University, 811-1 Kimiidera,Wakayama, Wakayama 641-0012, Japan. Email:[email protected] 12 September 2012; revision 28 December 2012; accepted18 February 2013.
bs_bs_banner
Hepatology Research 2014; 44: 179–186 doi: 10.1111/hepr.12101
© 2013 The Japan Society of Hepatology 179

Rapid virological response (RVR), defined as serumHCV RNA negativity at 4 weeks, is known to be the mostuseful predictor of SVR to PEG IFN plus ribavirintherapy.6 If an earlier virological response can predictoutcome more effectively than RVR, a trial administra-tion of PEG IFN plus ribavirin for 1 or 2 weeks could bea sensitive test for predicting outcome and for guidingtreatment strategy. The aim of the present study wasto evaluate whether the therapeutic efficacy of PEGIFN plus ribavirin therapy for patients with a high viralload of HCV genotype 2 can be predicted on the basisof virological response within 2 weeks of therapyinitiation.
METHODS
Patients
THIS WAS A prospective multicenter cohort study ofPEG IFN-a-2b plus ribavirin therapy for patients
with a genotype 2 HCV high viral load (>5.0 logIU/mL).A total of 64 chronic hepatitis C patients with a geno-type 2 high viral load were enrolled from March 2008 toSeptember 2011 in the Wakayama Medical UniversityHospital, Naga Municipal Hospital, and Hidaka GeneralHospital. Exclusion criteria were: (i) pregnant women,women who may have been pregnant, lactating women,men whose partners were pregnant or men whose part-ners hoped to become pregnant; (ii) patients who usedshosaikoto (a Kampo medicine); (iii) intractable heartdisease; (iv) renal failure or renal dysfunction with crea-tinine clearance of less than 50 mL/min; (v) patientswith uncontrollable psychoneurotic disorders; (vi)hemoglobin (Hb) levels of less than 12 g/dL; (vii) plate-let count of less than 70 000/mm3; (viii) white bloodcell count of less than 1500/mm3 (or granulocyte count<1000/mm3); and (ix) hepatic failure or cancer.
In the present study, the potential benefits and riskswere explained to all patients before obtaining writteninformed consent. All study protocols were approved bythe ethics committee of the participating hospitals.
Treatment regimensPegylated IFN-a-2B (PEG-INTRON; MSD, Tokyo,Japan) and ribavirin (Rebetol; MSD) were used;1.5 mg/kg PEG IFN-a-2b was administrated s.c. once aweek, and ribavirin was administrated p.o. for 24 weeks(1000 mg/day for patients weighing >80 kg, 800 mg/day for patients weighing between 60 and 80 kg, and600 mg/day for patients weighing <60 kg).
The PEG IFN-a-2b and ribavirin doses were reducedor discontinued based on the following criteria: (i) if the
Hb fell below 10 g/dL, the ribavirin dose was reduced(to 400 mg/day from 600 mg/day, to 600 mg/day from800 mg/day, or to 800 mg/day from 1000 mg/day), andif the Hb fell below 8.5 g/dL, the ribavirin was discon-tinued; (ii) if the granulocyte count fell below 750/mm3
or the platelet count fell below 70 000/mm3, the PEGIFN dose was reduced to half of the initial dose; (iii) ifthe granulocyte count fell below 500/mm3 or the plate-let count fell below 30 000/mm3, the PEG IFN wasdiscontinued; and (iv) PEG IFN and ribavirin were dis-continued if deemed necessary by the attending physi-cian because of adverse events. The dose of PEG IFN orribavirin was increased back to the starting dose if thecytopenia improved. If there was no improvement inhematological parameters within 4 weeks, this therapywas discontinued. Although the granulocyte colony-stimulating factor could be used as supplementarytreatment for granulocytopenia less than 500/mm3,erythropoietin was not allowed for treatment of anemiabecause the Ministry of Health in Japan had notapproved its use.
Laboratory tests and ultrasoundsIn all patients, laboratory tests and ultrasounds wereperformed before therapy began. Fatty liver was definedas positive hepatorenal contrast on ultrasound B modeimaging. The amount of HCV RNA was measured usingquantitative reverse transcription polymerase chainreaction (RT–PCR) (COBAS TaqMan PCR assay; RocheDiagnostics, Branchburg, NJ, USA). A high viral loadwas defined as more than 5.0 logIU/mL using quantita-tive RT–PCR. Determination of HCV genotype was per-formed by Simmonds et al.7: the amount of HCV RNAand HCV core antigen levels (Ortho Clinical Diagnos-tics, Tokyo, Japan) were measured simultaneously atfour time points (day of therapy initiation, the follow-ing day, and at weeks 1 and 2). Serum ribavirin concen-tration was measured at week 2. During therapy,quantitative HCV RNA and biochemical analyses(including blood counts, serum alanine aminotrans-ferase [ALT], and aspartate aminotransferase [AST]),were performed every 4 weeks up to 24 weeks after theend of therapy. After treatment, single nucleotide poly-morphism (SNP) of interleukin (IL)-28B host genotypes(rs8099917), which was reported as a pretreatment pre-dictor for the efficacy of PEG IFN plus ribavirin therapyin Japanese patients,8 were also evaluated after writteninformed consent for genome analysis was obtainedfrom each patient. Homozygosity for the major allele(T/T) was defined as the IL-28B major type, and het-
180 Y. Wada et al. Hepatology Research 2014; 44: 179–186
© 2013 The Japan Society of Hepatology

erozygosity (T/G) or homozygosity for the minor allele(G/G) was defined as the IL-28B minor type.
Liver histologyIn all patients, core needle biopsy of the liver was per-formed under ultrasound guidance using a 16-G corebiopsy needle (Bard Monopty, Covington, GA, USA)within 3 months before the start of therapy. Histologicalfindings were classified using the METAVIR scoringsystem9 based on activity (grades A0, A1, A2 and A3)and fibrosis (stages F0, F1, F2, F3 and F4).
Assessment of effectivenessDuring IFN therapy, RVR was defined as undetectableusing quantitative RT–PCR (COBAS TaqMan PCR assay;Roche Diagnostics) results at week 4 after therapy ini-tiation. SVR was defined as follows: HCV RNA measuredusing the TaqMan PCR assay was negative at the end oftherapy and remained negative for 24 weeks after theend of therapy. No response was defined as detectableHCV RNA at week 24 from treatment initiation or at theend of treatment. Relapse was defined as negative at theend of therapy but positive 24 weeks after the end oftherapy. The virological response within 2 weeks aftertherapy initiation was assessed by viral level at eachtime point, viral depletion from baseline viral load andrebound index (RI). RI was defined as the coefficientderived by dividing the viral load of week 1 by that ofday 1.10
Statistical analysisTherapeutic effectiveness was evaluated using anintention-to-treat analysis. Predictive factors for SVRwere analyzed using a per protocol analysis thatexcluded patients who had discontinued therapy due toadverse events, or whose adherence was under 67%. TheMann–Whitney U-test was used to analyze continuousvariables. Fisher’s exact test or the c2-test was used toanalyze categorical variables. Each optimal cut-off valuefor continuous variables of SVR predicting factors wasdecided by the Youden index method on the basis of thereceiver–operator curve (ROC). The SVR predictabilityof significant SVR contributing factors was evaluated bymeasuring the area under the ROC (AUC). The sensitiv-ity, specificity, positive predictive value (PPV), negativepredictive value (NPV) and accuracy for SVR were cal-culated on day 1, week 1, week 2 and RVR. Values ofP < 0.05 were considered statistically significant. SPSSstatistical software ver. 20.0J for Windows (SPSS, Tokyo,Japan) was used for data analyses.
RESULTS
Patients’ baseline characteristics
PATIENTS’ BASELINE CHARACTERISTICS are sum-marized in Table 1. There were 31 male and 33
female patients. Their mean age was 56 years, ranging21–76 years: 34 patients (53%) were less than 60 yearsold, and 30 (47%) were 60 years or older. Twenty-twopatients (34%) had advanced fibrosis (F3–F4). Eightpatients (13%) had undergone prior IFN therapy. Fourof those eight patients had undergone IFN plus ribavirintherapy.
Treatment response and drug adherenceRapid virological response was achieved in 78% (50/64)of patients. SVR was achieved in 73% (47/64), relapseoccurred in 17% (11/64) and no response in 9% (6/64)patients. Of the 64 patients in the present study, nopatients discontinued the therapy due to adverse effects.The mean adherences to both PEG IFN-a-2b and ribavi-rin therapy among the 64 patients who were enrolledin the present study were 97 1 8% and 88 1 16%,
Table 1 Patients’ baseline characteristics
Age (years, mean 1 SD) (range) 56 1 13 (21–76)Sex (male/female) 31/33Bodyweight (kg, mean 1 SD) 60 1 10Body mass index (kg/m2, mean 1 SD) 23.0 1 3.6Prior interferon therapy (%) 8 (13)Genotype (2a/2b) 47/17HCV RNA (logIU/mL, mean 1 SD) 5.7 1 0.8White blood cell count (/mm3,
mean 1 SD)4808 1 1735
Hemoglobin (g/dL, mean 1 SD) 13.6 1 1.6Platelets (¥104/mm3, mean 1 SD) 16.3 1 5.5ALT (IU/L, mean 1 SD) 78 1 69g-GT (IU/L, mean 1 SD) 60 1 57AFP (ng/mL, mean 1 SD) 14.1 1 27.2Ferritin (ng/mL, mean 1 SD) 159 1 113Type IV collagen 7S (ng/mL,
mean 1 SD)5.0 1 2.3
Hyaluronic acid (ng/mL, mean 1 SD) 109.1 1 150.4HOMA-IR 2.7 1 2.8Fatty liver (%) 17 (27)Activity grade (A0/A1/A2/A3) 4/27/28/5Fibrosis stage (F0/F1/F2/F3/F4) 3/16/23/10/12
AFP, a-fetoprotein; ALT, alanine aminotransferase; HCV,hepatitis C virus; HOMA-IR, Homeostasis Model of Assessment –Insulin Resistance; SD, standard deviation; g-GT, g-glutamyltransferase.
Hepatology Research 2014; 44: 179–186 SVR prediction within 2 weeks in genotype 2 181
© 2013 The Japan Society of Hepatology

respectively. Nine of the 64 patients (14%) requireddose reduction or interruption of PEG IFN-a-2b becauseof adverse effects including neutropenia and thromb-ocytopenia. Twenty-seven of the 64 patients (42%)required dose reduction or interruption of ribavirinbecause of anemia.
Eighteen of the 30 older patients (360 years) and nineof the 34 younger patients (<60 years) required a drugdose reduction. The drug dose reduction rate in olderpatients was significantly higher than that in youngerpatients (60% vs 26%, P = 0.007). Twenty-two of 33female patients and nine of 31 male patients required adrug dose reduction. The drug dose reduction rate infemale patients was significantly higher than in malepatients (67% vs 29%, P = 0.003). Fifteen of 18 olderfemale patients and five of 12 older male patientsrequired a drug dose reduction. The drug dose reductionrate in older female patients was significantly higherthan that in older male patients (83% vs 42%,P = 0.018). The SVR rate in older female patients wasonly 39% (7/18).
Contributing factors for SVR and predictionof SVR
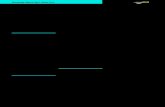
Of all 64 patients, 58 patients whose adherence wasmore than 67% were analyzed for SVR contributingfactors: 44 SVR patients and 14 non-SVR patients. Onunivariate analysis of factors contributing to SVR,significant differences were noted in age, bodyweight,white cell count, platelet count, serum fibrosis markers(type IV collagen 7S and hyaluronic acid), baseline HCVcore antigen level, and RI between the SVR group andthe non-SVR group. However, there were no significantdifferences in IL-28B host genotypes, HCV genotypesand serum ribavirin level at week 2 between the SVRgroup and non-SVR group at week 2 (Table 2). Thekinetics of the HCV core antigen and the HCV RNAlevels during the therapy within 2 weeks after therapyinitiation are shown in Figure 1. Significant differencesin the mean HCV core antigen and HCV RNA levelsduring the 2 weeks after therapy initiation were seenbetween the SVR group and the non-SVR group.
Table 2 Comparison of factors between patients with and without SVR
Factors SVR (n = 44) Non-SVR (n = 14) P-value
Age (years, mean 1 SD) 52 1 13 67 1 6 <0.001Sex (male/female) 27/17 4/10 0.063Prior interferon therapy 7 1 0.665Bodyweight (kg, mean 1 SD) 63 1 10 55 1 9 0.012Body mass index (kg/m2, mean 1 SD) 23.0 1 2.5 23.3 1 6.2 0.223White blood cell count (/mm3, mean 1 SD) 5211 1 1806 4123 1 1355 0.047Hemoglobin (g/dL, mean 1 SD) 13.9 1 1.5 13.1 1 1.4 0.059Platelets (¥104/mm3, mean 1 SD) 17.2 1 5.3 13.6 1 5.8 0.017ALT (IU/L, mean 1 SD) 86 1 77 55 1 39 0.139g-GT (IU/L, mean 1 SD) 63 1 62 54 1 49 0.669AFP (ng/mL, mean 1 SD) 13.0 1 28.0 20.6 1 29.9 0.440Ferritin (ng/mL, mean 1 SD) 148.4 1 92.9 176.0 1 159.3 0.875Type IV collagen 7S (ng/mL, mean 1 SD) 4.5 1 1.3 7.1 1 3.7 0.049Hyaluronic acid (ng/mL, mean 1 SD) 68.8 1 75.8 257.5 1 252.0 <0.001HOMA-IR 2.9 1 3.1 2.3 1 1.6 0.603Fatty liver (-/+) 30/14 11/3 0.523Activity grade (A0–1/A2–3) 25/19 6/8 0.362Fibrosis stage (F0–2/F3–4) 30/14 8/6 0.449IL-28B (TT/TG/GG) 34/10/0 11/3/0 1.000HCV genotype (2a/2b) 34/10 9/5 0.334HCV RNA (logIU/mL, mean 1 SD) 5.6 1 0.8 6.1 1 0.7 0.054HCV core Ag (fmol/L, mean 1 SD) 3664 1 4263 6514 1 4903 0.037Rebound index of HCV RNA (mean 1 SD) 0.7 1 0.4 0.9 1 0.1 0.006Rebound index of HCV core Ag (mean 1 SD) 0.1 1 0.1 0.8 1 0.8 <0.001Ribavirin at week 2 (ng/mL, mean 1 SD) 1975.7 1 655.2 2078.1 1 612.6 0.716
AFP, a-fetoprotein; Ag, antigen; ALT, alanine aminotransferase; HCV, hepatitis C virus; HOMA-IR, Homeostasis Model of Assessment –Insulin Resistance; IL-28B, interleukin-28B; SD, standard deviations; SVR, sustained virological response; g-GT, g-glutamyl transferase.
182 Y. Wada et al. Hepatology Research 2014; 44: 179–186
© 2013 The Japan Society of Hepatology

The AUC according to significant SVR predictingfactors are summarized in Table 3. For all significantfactors, the highest AUC for HCV RNA level was at week2 and the highest AUC for HCV core antigen level was atweek 1. Among SVR predicting factors, the AUC fordepletion of HCV core antigen level at week 2 was notsignificant. The AUC for HCV core antigen level at week1 was the highest out of all of the significant SVR con-tributing factors.
The sensitivity, specificity, PPV, NPV and accuracyfor SVR according to significant predictive virologicalfactors within 4 weeks of therapy initiation are summa-rized in Table 4. The accuracy for SVR by HCV coreantigen level at week 1 was the highest.
DISCUSSION
ADHERENCE TO THERAPY is one of the most impor-tant factors associated with treatment success in
HCV. However, in PEG IFN-a plus ribavirin therapy,side-effects such as cytopenia can reduce adherence totherapy. For analysis of the predictive factors for SVR thatare not influenced by drug adherence, patients with lowadherence should be avoided. With respect to optimalPEG IFN dose, Manns et al.11 reported that there was nosignificant difference in the SVR rate between low dose(1.0 mg/kg) and standard dose (1.5 mg/kg) PEG IFN-a-2b to PEG IFN-a-2b plus ribavirin therapy for patientswith genotype 2 HCV. As above, a one-third dose reduc-tion of the recommended PEG IFN-a-2b dose does notaffect the SVR rate. With respect to ribavirin dose, Ferenciet al.12 reported that in patients with genotype 2 HCV,reducing the daily ribavirin dose to 400 mg resulted insignificantly lower SVR rates compared to standard rib-avirin 800 mg regimen (55.6% vs 77.8%, respectively).However, Inoue et al.13 reported that reducing both PEGIFN and ribavirin dose had no impact on RVR and SVR toPEG IFN-a-2b plus ribavirin therapy in patients withgenotype 2 HCV. Furthermore, they showed that therewas no significant difference in SVR rate betweenpatients who received average ribavirin doses up to8 mg/kg per day and patients who received more than12 mg/kg per day. From the details mentioned above,even though a one-half reduction of ribavirin dose mayreduce SVR rate, a one-third reduction will not affect theSVR rate. Therefore, in the present study, contributingfactors for SVR and prediction of SVR to PEG IFN-a-2bplus ribavirin therapy were analyzed using a per protocolanalysis that excluded patients who discontinued due toadverse events or whose adherence was under 67%.
Several baseline host factors in genotype 2 HCV infec-tions have already been identified to be associated withSVR. Factors associated with SVR included younger age(<40 years),14–16 lower bodyweight,15,17 body mass indexless than 30,18 low g-glutamyl transferase level,19 highALT level,15,20 platelet count of 140 000 or more,18 lowerviral load17,19,20 and absence of severe fibrosis.14,15,17,19 Inthis study, significant host factors associated with SVRwere younger age, higher bodyweight, higher white cellcount, higher hemoglobin level, higher platelet count,lower HCV core antigen level and lower serum fibrosismarker (type IV collagen 7S and hyaluronic acid) levels.Aside from bodyweight, other significant host factorsassociated with SVR were consistent with the previousreports. In considering possible explanations for thisdiscrepancy, Japanese female patients had a relativelylower bodyweight and lower hemoglobin level thanthose of male patients, and their adherence to ribavirintherapy was lower. Drug adherence may more stronglyaffect SVR in older female patients.
00
1000
2000
3000
4000
5000
6000
7000
1 2 3
HC
V c
ore
antig
en le
vel (
fmol
/L)
4 5 6 7
1244 ± 1497
165 ± 184677 ± 704
260 ± 4120 ± 314 ± 26
3664 ± 4263
6514 ± 4903
8 9 10 11 13 14 (days)12
00
1
2
3
4
5
6
7
1
(a)
(b)
2 3
HC
V-R
NA
leve
l (lo
gIU
/mL)
4 5 6 7
6.1 ± 0.75.6 ± 0.8
5.0 ± 0.8
3.7 ± 1.2
4.8 ± 0.8
2.9 ± 1.5
4.2 ± 1.2
1.6 ± 1.3
8 9 10 11 13 14 (days)12
Figure 1 Kinetics of hepatitis C virus (HCV) RNA (a) and HCVcore antigen (b) levels are shown by line graphs according tothe effect of therapy. Significant differences were observed invirological response of both HCV RNA and HCV core antigenlevels at all time points within 2 weeks of therapy initiationbetween the sustained virological response (SVR) and the non-SVR groups (P < 0.001). , SVR; , non-SVR.
Hepatology Research 2014; 44: 179–186 SVR prediction within 2 weeks in genotype 2 183
© 2013 The Japan Society of Hepatology

Recently, as other predictive host factors, some studieshave reported that different SNP of the IL-28B gene havebeen associated with response to PEG IFN plus ribavirintherapy for patients with genotype 2 HCV.21–24 However,
these reports could not accurately predict treatmentresponse. In the present study, IL-28B SNP was not asignificant factor for predicting SVR. At the moment,although pretreatment predictors of response may be
Table 3 AUC according to significant contributing factors for SVR
Factors AUC P-value 95% CI
Age 0.877 <0.001 0.787–0.966Bodyweight 0.726 0.012 0.572–0.880White blood cell count 0.675 0.050 0.523–0.828Platelets 0.708 0.020 0.538–0.877Type IV collagen 7S 0.674 0.058 0.460–0.889Hyaluronic acid 0.818 0.001 0.688–0.949HCV RNA at day 1 0.827 <0.001 0.690–0.965HCV RNA at week 1 0.919 <0.001 0.827–1.000HCV RNA at week 2 0.938 <0.001 0.849–1.000HCV core Ag at day 0 0.691 0.039 0.517–0.864HCV core Ag at day 1 0.810 0.001 0.651–0.969HCV core Ag at week 1 0.940 <0.001 0.842–1.000HCV core Ag at week 2 0.725 0.015 0.539–0.910Depletion of HCV RNA at day 1 0.751 0.005 0.586–0.916Depletion of HCV RNA at week 1 0.909 <0.001 0.827–0.992Depletion of HCV RNA at week 2 0.910 <0.001 0.835–0.985Depletion of HCV core Ag (log) at day 1 0.762 0.003 0.616–0.909Depletion of HCV core Ag (log) at week 1 0.935 <0.001 0.869–1.000Depletion of HCV core Ag (log) at week 2 0.645 0.107 0.436–0.853Rebound index of HCV RNA 0.737 0.010 0.605–0.869Rebound index of HCV core Ag 0.915 <0.001 0.813–1.000RVR (HCV RNA undetectable at week 4) 0.794 0.001 0.671–0.917
Ag, antigen; AUC, area under the receiver–operator curve; CI, confidence interval; HCV, hepatitis C virus; SVR, sustained virologicalresponse; RVR, rapid virological response.
Table 4 SVR according to significant factors related to virological response within 4 weeks of therapy initiation
Significant predictive viral factors Sensitivity Specificity PPV NPV Accuracy
HCV RNA at day 1 <4.7 logIU/mL 81% (35/43) 71% (10/14) 90% (35/39) 56% (10/18) 79% (45/57)HCV RNA at week 1 <4.3 logIU/mL 84% (37/44) 86% (12/14) 95% (37/39) 63% (12/19) 85% (49/58)HCV RNA at week 2 <3.2 logIU/mL 84% (37/44) 93% (13/14) 97% (37/38) 65% (13/20) 86% (50/58)HCV core Ag at day 1 <760 fmol/mL 100% (43/43) 50% (7/14) 86% (43/50) 100% (7/7) 88% (50/57)HCV core Ag at week 1 <100 fmol/mL 100% (44/44) 86% (12/14) 96% (44/46) 100% (12/12) 97% (56/58)HCV core Ag at week 2 <160 fmol/mL 100% (44/44) 43% (6/14) 85% (44/52) 100% (6/6) 86% (50/58)Depletion of HCV RNA at day 1 >1.1 log 84% (36/43) 57% (8/14) 86% (36/42) 53% (8/15) 77% (44/57)Depletion of HCV RNA at week 1 >2.0 log 75% (33/44) 93% (13/14) 97% (33/34) 54% (13/24) 79% (46/58)Depletion of HCV RNA at week 2 >3.5 log 68% (30/44) 100% (14/14) 100% (30/30) 50% (14/28) 76% (44/58)Depletion of HCV core Ag at day 1 >0.9 log 88% (38/43) 57% (8/14) 86% (38/44) 62% (8/13) 81% (46/57)Depletion of HCV core Ag at week 1 >2.2 log 75% (33/44) 100% (14/14) 100% (33/33) 56% (14/25) 81% (47/58)Rebound index of HCV RNA <0.8 51% (22/43) 93% (13/14) 96% (22/23) 38% (13/34) 79% (45/57)Rebound index of HCV core Ag <0.2 91% (39/43) 86% (12/14) 95% (39/41) 75% (12/16) 90% (51/57)RVR (HCV RNA undetectable at week 4) 66% (29/44) 93% (13/14) 97% (29/30) 46% (13/28) 72% (42/58)
Ag, antigen; HCV, hepatitis C virus; NPV, negative predictive value; PPV, positive predictive value; SVR, sustained virological response;RVR, rapid virological response.
184 Y. Wada et al. Hepatology Research 2014; 44: 179–186
© 2013 The Japan Society of Hepatology

useful for advising patients with genotype 2 HCV ontheir likelihood of achieving an SVR, absence of favor-able predictive factors should not deny therapy.3
To date, the most reliable predictive factor for SVR isRVR.6 On the basis of RVR, response-guided treatmentprofiles are decided.5 However, a negative predictionrule for patients with genotype 2 HCV that could accu-rately predict who will not achieve an SVR has not beenwell established. In the present study, although PPV forSVR by RVR was high (97%), NPV for SVR by RVR wasvery low (46%) because the HCV RNA levels by theTaqMan method were positive at week 4 in more than ahalf of the SVR patients. Whereas a HCV core antigenlevel less than 100 fmol/mL at week 1, which was set asa best cut-off level based on the ROC curve, was moreaccurate than RVR in prediction of SVR, and was supe-rior to RVR in terms of sensitivity and NPV for SVR. Thereason for this may be that the detectability for HCVRNA by the TaqMan method was higher than that by thequalitative Amplicor method. A negativity of HCV RNAlevel at week 4 by the TaqMan method would not be thebest cut-off level for predicting non-SVR.
In patients with genotype 2 HCV, only a smallnumber of studies concerning prediction of SVR to PEGIFN plus ribavirin using early viral kinetics have beenpublished. Lagging et al.16 demonstrated that with stan-dard PEG IFN plus ribavirin therapy for patients withgenotype 2 or 3, sensitivity, specificity, PPV and NPV forthe likelihood of achieving SVR by HCV RNA of lessthan 1000 IU/mL on day 7 was 36%, 95%, 98% and20%, respectively. Although the specificity and PPV weresuperior, sensitivity and NPV were lower. In addition, inthe same study, according to HCV core antigen level onday 3, PPV by HCV core antigen level of less than0.2 pg/mL was very high (95%), but NPV was very low(26%).25 However, Nomura et al.10 showed that an RI ofless than 1.0 was the only significant independent pre-dictive factor for SVR. Their sensitivity, specificity, PPVand NPV for SVR by RI was 98%, 100%, 100% and 89%,respectively. However, in the present study, RI was a lessaccurate predictive factor for SVR than other viral kinet-ics factors. The reason for this discrepancy may be thatthey measured the viral load by employing a less sensi-tive quantitative RT–PCR assay (COBAS Amplicor HCVmonitor ver. 2.0), which has a threshold of 3.70 logIU/mL. On the other hand, Neumann et al.26 showed that afirst-phase decline of 1.25 logIU/mL or a day-3 viralload of less than 4 2 logIU/mL were accurate predictorsfor SVR response to albinterferon-a-2b therapy withoutribavirin in patients with genotype 2/3 HCV. Especially,they were better than RVR for specificity and NPV for
SVR. In the present study, however, the levels of HCVRNA and the HCV core antigen were more accuratepredictors for SVR than the decline of those levels ateach time point. Furthermore, the most accurate timepoints for prediction of SVR by the HCV RNA level andthe HCV core antigen level was at weeks 2 and 1, respec-tively. The accuracy for predicting SVR by HCV coreantigen level at week 1 was superior to that at week 2,and the cut-off level of HCV core antigen at week 1 waslower than that at week 2. The reason for this may bethat the detectability of the HCV core antigen was lowerthan that of HCV RNA.
As HCV core antigen is better than the HCV RNA assayin terms of lower cost, convenience and rapid results,treatment response within 1 week after therapy initia-tion should be monitored by measuring HCV coreantigen rather than by measuring HCV RNA load. Thepresent study indicated that as a substitute for RVR, thevirological response of HCV core antigen level (cut-offvalue, <100 fmol/mL) at week 1 may be able to used asa sensitive test for predicting outcome and treatmentstrategy decisions. These findings will be especiallyuseful for elderly and/or cirrhotic patients who have ahigh risk of severe adverse effects and should be treatedwith a reduced dose regimen.
One limitation of the present study is the smallnumber of patients. Although HCV core antigen level atweek 1 after therapy initiation was the best predictorof SVR among all significant predictive factors in thepresent study, the P-values of HCV core antigen level atweek 1 was almost similar to other various factors. Inorder to validate the present results, further large scaleprospective studies are necessary.
In conclusion, from the analysis of viral dynamicswithin 2 weeks of therapy initiation, it was demon-strated that the HCV core antigen level at 1 week is themost useful predictor for SVR to standard PEG IFN-a-2bplus ribavirin therapy in patients infected with genotype2 HCV. The virological response within 2 weeks may beable to substitute for RVR in predicting SVR and treat-ment strategy decisions.
REFERENCES
1 Veldt BJ, Heathcote EJ, Wedemeyer H et al. Sustained viro-logic response and clinical outcomes in patients withchronic hepatitis C and advanced fibrosis. Ann Intern Med2007; 147: 677–84.
2 Asian Pacific Association for the Study of the Liver Hepa-titis CWP, McCaughan GW, Omata M, Amarapurkar Det al. Asian Pacific Association for the Study of the Liver
Hepatology Research 2014; 44: 179–186 SVR prediction within 2 weeks in genotype 2 185
© 2013 The Japan Society of Hepatology

consensus statements on the diagnosis, management andtreatment of hepatitis C virus infection. J GastroenterolHepatol 2007; 22: 615–33.
3 Ghany MG, Strader DB, Thomas DL, Seeff LB, AmericanAssociation for the Study of Liver D. Diagnosis, manage-ment, and treatment of hepatitis C: an update. Hepatology2009; 49: 1335–74.
4 Kumada H, Okanoue T, Onji M et al. Guidelines for thetreatment of chronic hepatitis and cirrhosis due to hepati-tis C virus infection for the fiscal year 2008 in Japan.Hepatol Res 2010; 40: 8–13.
5 European Association for the Study of the L. EASL ClinicalPractice Guidelines: management of hepatitis C virus infec-tion. J Hepatol 2011; 55: 245–64.
6 Fried MW, Hadziyannis SJ, Shiffman ML, Messinger D,Zeuzem S. Rapid virological response is the most impor-tant predictor of sustained virological response acrossgenotypes in patients with chronic hepatitis C virus infec-tion. J Hepatol 2011; 55: 69–75.
7 Simmonds P, Holmes EC, Cha TA et al. Classification ofhepatitis C virus into six major genotypes and a series ofsubtypes by phylogenetic analysis of the NS-5 region. J GenVirol 1993; 74: 2391–9.
8 Tanaka Y, Nishida N, Sugiyama M et al. Genome-wideassociation of IL28B with response to pegylated interferon-alpha and ribavirin therapy for chronic hepatitis C. NatGenet 2009; 41: 1105–9.
9 Bedossa P, Poynard T. An algorithm for the grading ofactivity in chronic hepatitis C. The METAVIR CooperativeStudy Group. Hepatology 1996; 24: 289–93.
10 Nomura H, Miyagi Y, Tanimoto H, Ishibashi H. Impact ofearly viral kinetics on pegylated interferon alpha 2b plusribavirin therapy in Japanese patients with genotype 2chronic hepatitis C. J Viral Hepat 2009; 16: 346–51.
11 Manns M, Zeuzem S, Sood A et al. Reduced dose and dura-tion of peginterferon alfa-2b and weight-based ribavirinin patients with genotype 2 and 3 chronic hepatitis C.J Hepatol 2011; 55: 554–63.
12 Ferenci P, Brunner H, Laferl H et al. A randomized, pro-spective trial of ribavirin 400 mg/day versus 800 mg/day incombination with peginterferon alfa-2a in hepatitis C virusgenotypes 2 and 3. Hepatology 2008; 47: 1816–23.
13 Inoue Y, Hiramatsu N, Oze T et al. Factors affecting efficacyin patients with genotype 2 chronic hepatitis C treated bypegylated interferon alpha-2b and ribavirin: reducing drugdoses has no impact on rapid and sustained virologicalresponses. J Viral Hepat 2010; 17: 336–44.
14 Dalgard O, Bjoro K, Hellum KB et al. Treatment with pegy-lated interferon and ribavarin in HCV infection with geno-type 2 or 3 for 14 weeks: a pilot study. Hepatology 2004; 40:1260–5.
15 Shiffman ML, Suter F, Bacon BR et al. Peginterferon alfa-2aand ribavirin for 16 or 24 weeks in HCV genotype 2 or 3.N Engl J Med 2007; 357: 124–34.
16 Lagging M, Langeland N, Pedersen C et al. Randomizedcomparison of 12 or 24 weeks of peginterferon alpha-2aand ribavirin in chronic hepatitis C virus genotype 2/3infection. Hepatology 2008; 47: 1837–45.
17 Diago M, Shiffman ML, Bronowicki JP et al. Identifyinghepatitis C virus genotype 2/3 patients who can receivea 16-week abbreviated course of peginterferon alfa-2a(40KD) plus ribavirin. Hepatology 2010; 51: 1897–903.
18 Mangia A, Minerva N, Bacca D et al. Determinants ofrelapse after a short (12 weeks) course of antiviral therapyand re-treatment efficacy of a prolonged course in patientswith chronic hepatitis C virus genotype 2 or 3 infection.Hepatology 2009; 49: 358–63.
19 von Wagner M, Huber M, Berg T et al. Peginterferon-alpha-2a (40KD) and ribavirin for 16 or 24 weeks inpatients with genotype 2 or 3 chronic hepatitis C. Gastro-enterology 2005; 129: 522–7.
20 Mecenate F, Pellicelli AM, Barbaro G et al. Short versusstandard treatment with pegylated interferon alfa-2A plusribavirin in patients with hepatitis C virus genotype 2 or 3:the cleo trial. BMC Gastroenterol 2010; 10: 21.
21 Sakamoto N, Nakagawa M, Tanaka Y et al. Association ofIL28B variants with response to pegylated-interferon alphaplus ribavirin combination therapy reveals intersubgeno-typic differences between genotypes 2a and 2b. J Med Virol2011; 83: 871–8.
22 Sarrazin C, Susser S, Doehring A et al. Importance of IL28Bgene polymorphisms in hepatitis C virus genotype 2 and 3infected patients. J Hepatol 2011; 54: 415–21.
23 Yu ML, Huang CF, Huang JF et al. Role of interleukin-28Bpolymorphisms in the treatment of hepatitis C virus geno-type 2 infection in Asian patients. Hepatology 2011; 53:7–13.
24 Kawaoka T, Hayes CN, Ohishi W et al. Predictive value ofthe IL28B polymorphism on the effect of interferontherapy in chronic hepatitis C patients with genotypes 2aand 2b. J Hepatol 2011; 54: 408–14.
25 Alsio A, Jannesson A, Langeland N et al. Early quantifica-tion of HCV core antigen may help to determine the dura-tion of therapy for chronic genotype 2 or 3 HCV infection.Eur J Clin Microbiol Infect Dis 2011; 31: 1631–5.
26 Neumann AU, Pianko S, Zeuzem S et al. Positive and nega-tive prediction of sustained virologic response at weeks 2and 4 of treatment with albinterferon alfa-2b or peginter-feron alfa-2a in treatment-naive patients with genotype 1,chronic hepatitis C. J Hepatol 2009; 51: 21–8.
186 Y. Wada et al. Hepatology Research 2014; 44: 179–186
© 2013 The Japan Society of Hepatology