Pre-op and Post-op Beta Blockers
50
Pre-op and Post-op Beta Blockers Alla Kotlyanskaya, Pharm.D. Clinical Pharmacist – Critical Care Woodhull Medical Center, Brooklyn, New York Adjunct Professor of Pharmacology College of Nursing Graduate Programs SUNY Downstate College of Nursing And Adjunct Professor of Pharmacotherapy Physician Assistant Program
-
Upload
keegan-avila -
Category
Documents
-
view
47 -
download
0
description
Pre-op and Post-op Beta Blockers. Alla Kotlyanskaya, Pharm.D. Clinical Pharmacist – Critical Care Woodhull Medical Center, Brooklyn, New York Adjunct Professor of Pharmacology College of Nursing Graduate Programs SUNY Downstate College of Nursing And Adjunct Professor of Pharmacotherapy - PowerPoint PPT Presentation
Transcript of Pre-op and Post-op Beta Blockers
Pre-op and Post-op Beta Blockers
Alla Kotlyanskaya, Pharm.D. Clinical Pharmacist – Critical Care
Woodhull Medical Center, Brooklyn, New YorkAdjunct Professor of Pharmacology
College of Nursing Graduate ProgramsSUNY Downstate College of Nursing
AndAdjunct Professor of Pharmacotherapy
Physician Assistant Program
Objectives Discuss the protective effects of β-blockers in
setting of perioperative beta blockade Present standards of care for use of peri-
operative β-blocker therapy Describe the benefits & limitations of β-blockers
in surgical population Deliver final recommendations on when to use
and why to avoid β-blockers in select patients
Magnitude of Risks of Non-Cardiac Surgery
NON-cardiac surgery risk of CARDIAC mortality
Adverse outcomes of post-op myocardial infarction (MI) LOS & healthcare costs Results in 15 - 25% of all in-hospital mortality Cardiac death or non-fatal MI in next 6 months
Why is Non-Cardiac Surgery Associated with Cardiac Complications 100 million have non-cardiac surgery each year
Huge at-risk population 1 million suffer perioperative cardiac event
huge burden of disease Frequently silent Few interventions proven to lower risk
Barriers Surrounding a Silent Myocardial Infarction Frequency of silent MI
Chest pain (14%) Single symptom or sign (50%)
Numerous explanations for under-diagnosis Opioids administration for surgical pain Residual effect of anesthesia Other reasons for BP, HR, SOB, N&V Different pathophysiology of perioperative MI?
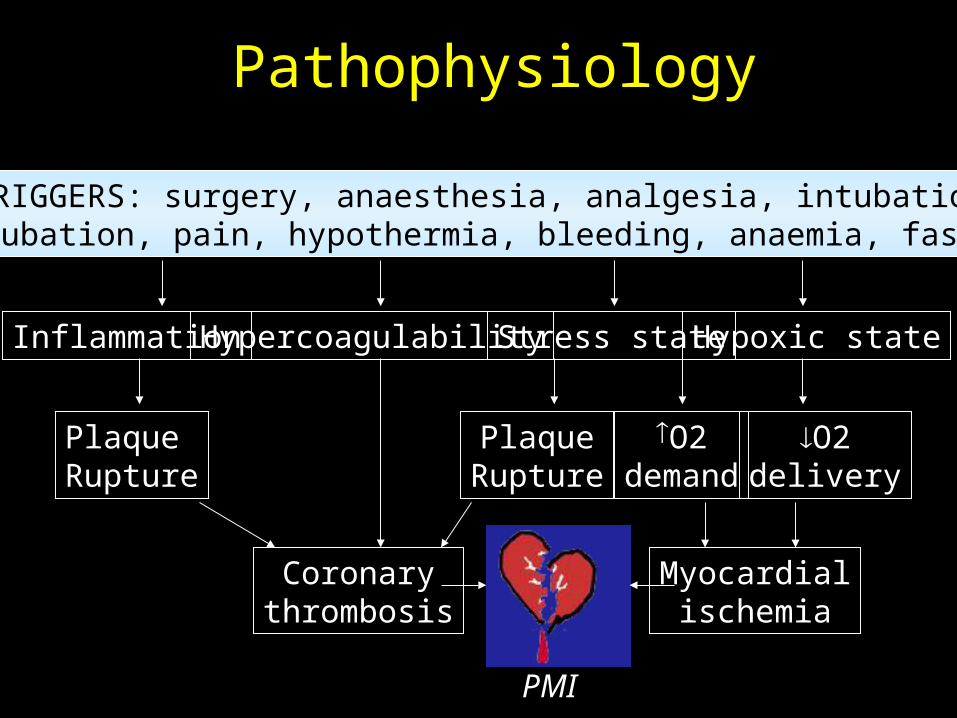
Pathophysiology
PMI
TRIGGERS: surgery, anaesthesia, analgesia, intubation,extubation, pain, hypothermia, bleeding, anaemia, fasting
Inflammation Hypercoagulability Stress state Hypoxic state
PlaqueRupture
PlaqueRupture
Coronarythrombosis
O2demand
O2delivery
Myocardialischemia

Initial Risk Assessment In 1977 Goldman et al
developed a preoperative cardiac risk index
9 Individual risk factors and their scores
Risk Index: Class I = 0-5 points (low) Class II = 6-12 points
(intermediate) Class III = 13-25 pts (high) Class IV 25 pts (very high)
Risk Factor Score
3rd Heart sound (S3) 11
Elevated JV pressure 11
MI in past 6 months 10
ECG: premature atrial contractions or any rhythm other than sinus
7
ECG shows >5 premature ventricular contractions per minute
7
Age >70 years 5
Emergency Procedure 4
Intra-thoracic, intra-abdominal or aortic surgery
3
Poor general status, metabolic or bedridden
3
N Engl J Med 1977;297:845-850
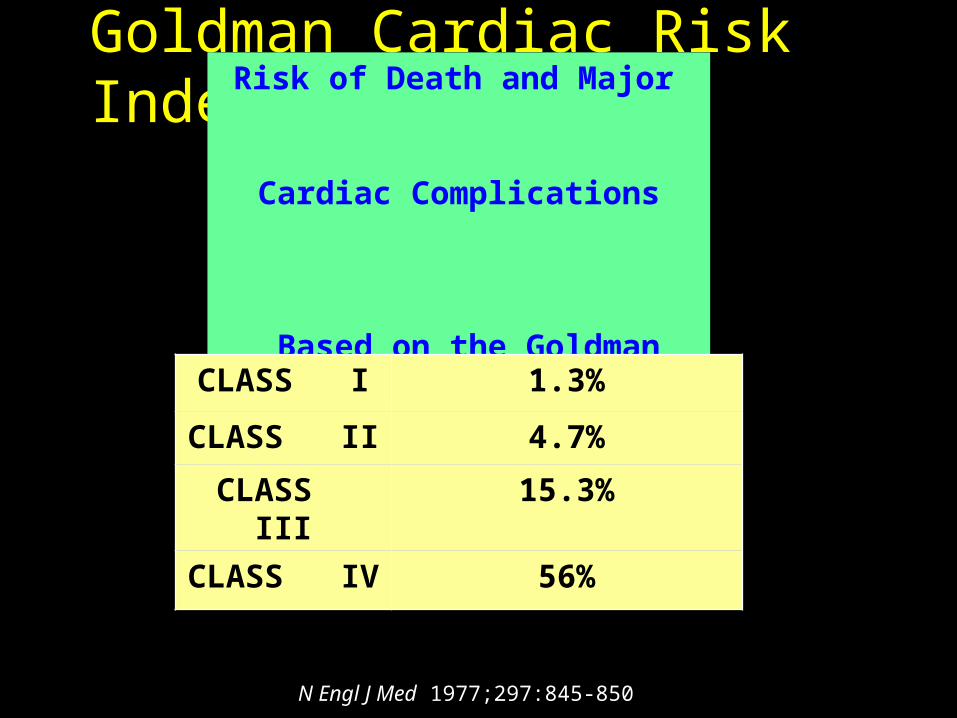
Goldman Cardiac Risk Index Risk of Death and Major
Cardiac Complications Based on the
Goldman Index Class
CLASS I 1.3%
CLASS II 4.7%
CLASS III 15.3%
CLASS IV 56%
N Engl J Med 1977;297:845-850
Cardiac Risk Stratification Proposals
Goldman: 1977
Detsky: 1986
Eagle: 1989
Lee:1999
ACC/AHA Guidelines
Am Coll Cardiol. 2007 Oct 23;50(17):e159-241.
Risk stratification according to major, intermediate or minor clinical predictors
Surgery
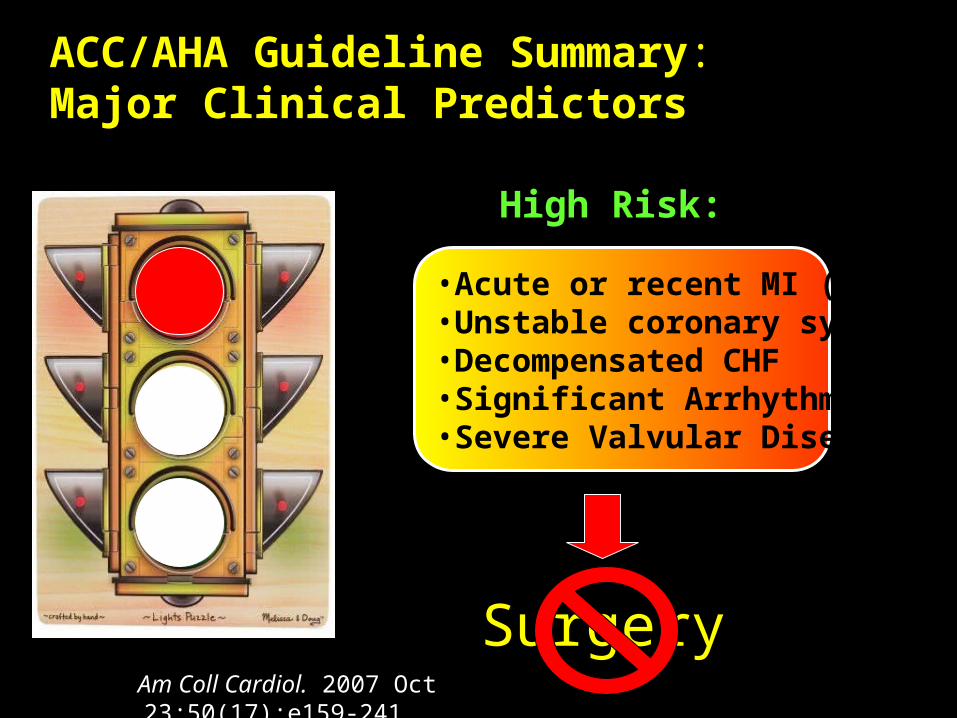
ACC/AHA Guideline Summary: Major Clinical Predictors
•Acute or recent MI (7-30 d)•Unstable coronary syndrome•Decompensated CHF•Significant Arrhythmias•Severe Valvular Disease
High Risk:
Am Coll Cardiol. 2007 Oct 23;50(17):e159-241.
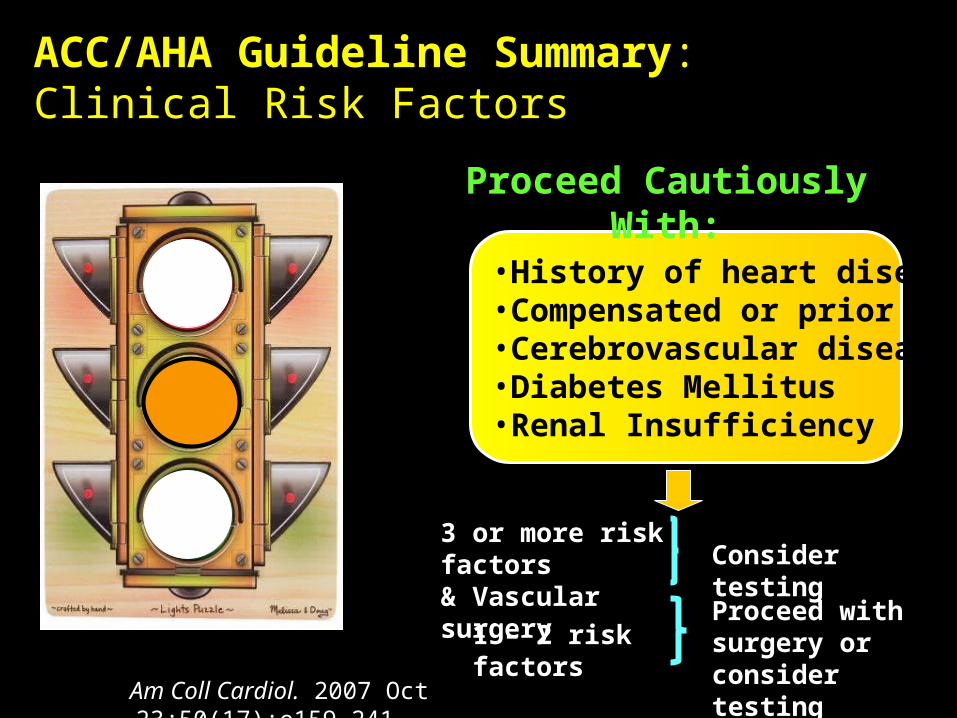
ACC/AHA Guideline Summary: Clinical Risk Factors
3 or more risk factors& Vascular surgery
•History of heart disease•Compensated or prior CHF•Cerebrovascular disease•Diabetes Mellitus•Renal Insufficiency
Proceed Cautiously With:
Consider testing
1 – 2 risk factorsProceed with surgery or consider testing
Am Coll Cardiol. 2007 Oct 23;50(17):e159-241.
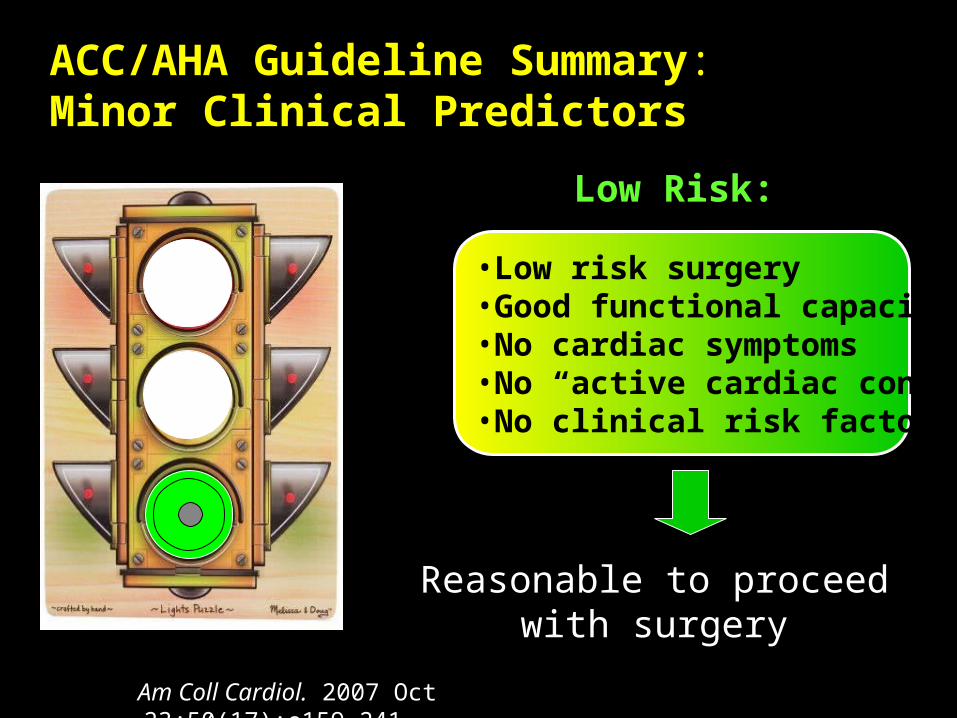
ACC/AHA Guideline Summary: Minor Clinical Predictors
Reasonable to proceed with surgery
•Low risk surgery•Good functional capacity•No cardiac symptoms•No “active cardiac conditions”•No clinical risk factors
Low Risk:
Am Coll Cardiol. 2007 Oct 23;50(17):e159-241.

Functional Capacity
Determined by how much physical activity a patient can tolerate without severe exertion
Provides valuable prognostic information
Patients with good functional status have a lower risk of complications
How to stratify it How to modify it
ß Blocker Other New Agents
Perioperative MI
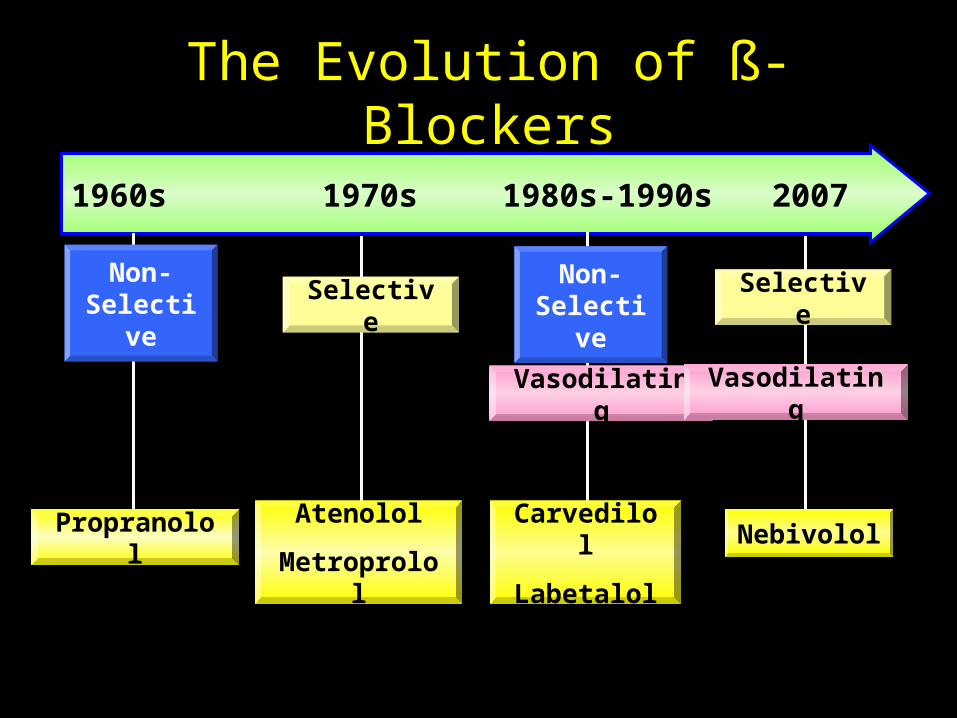
The Evolution of ß-Blockers
1960s 1970s 1980s-1990s 2007
Non-Non-SelectiveSelective
Non-Non-SelectiveSelective
VasodilatingVasodilatingVasodilating Vasodilating
Non-Selective
Non-Selective
Selective Selective
Propranolol Atenolol
Metroprolol
Carvedilol
Labetalol
Nebivolol
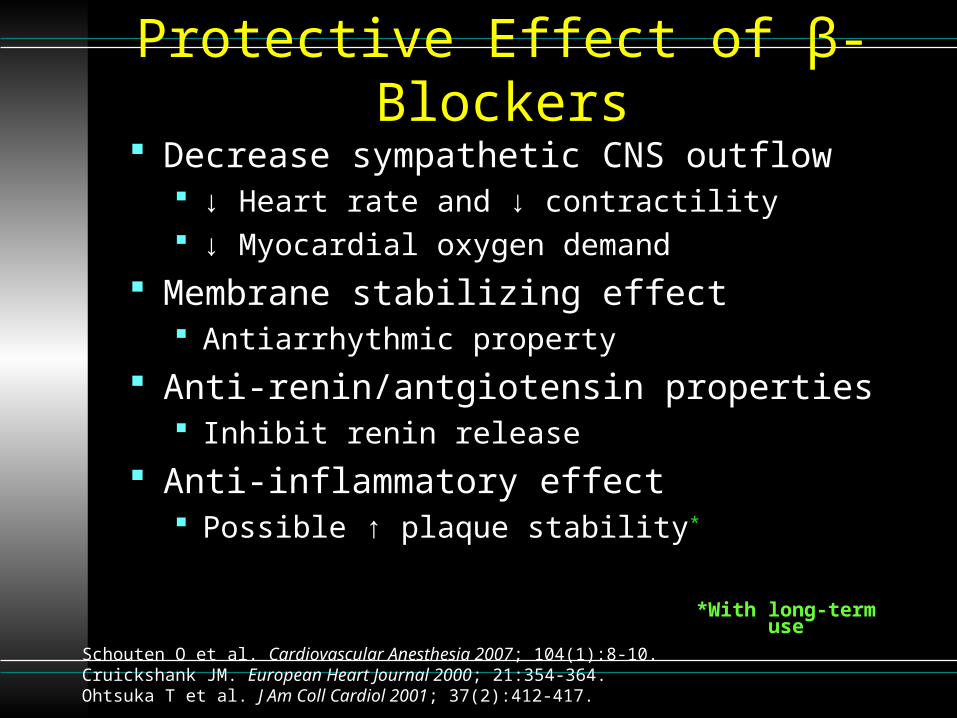
Protective Effect of β-Blockers Decrease sympathetic CNS outflow
↓ Heart rate and ↓ contractility ↓ Myocardial oxygen demand
Membrane stabilizing effect Antiarrhythmic property
Anti-renin/antgiotensin properties Inhibit renin release
Anti-inflammatory effect Possible ↑ plaque stability*
Schouten O et al. Cardiovascular Anesthesia 2007; 104(1):8-10.Cruickshank JM. European Heart Journal 2000; 21:354-364.Ohtsuka T et al. J Am Coll Cardiol 2001; 37(2):412-417.
*With long-term use
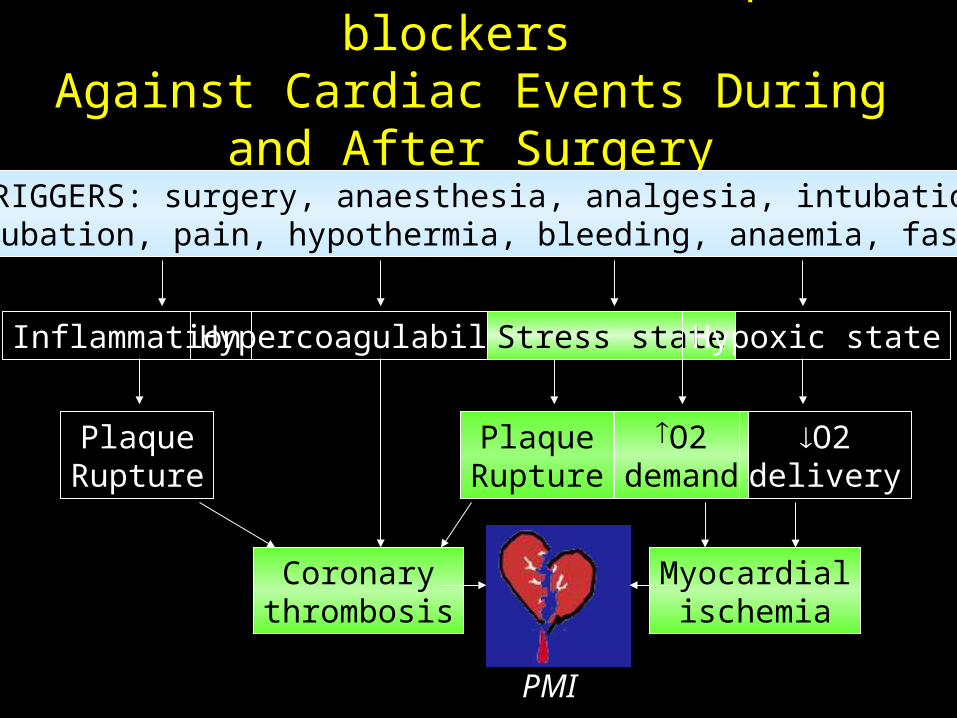
Protective Effect of -blockers Against Cardiac Events During and After Surgery
TRIGGERS: surgery, anaesthesia, analgesia, intubation,extubation, pain, hypothermia, bleeding, anaemia, fasting
Inflammation Hypercoagulability Stress state Hypoxic state
PlaqueRupture
PlaqueRupture
Coronarythrombosis
O2demand
O2delivery
Myocardialischemia
PMI
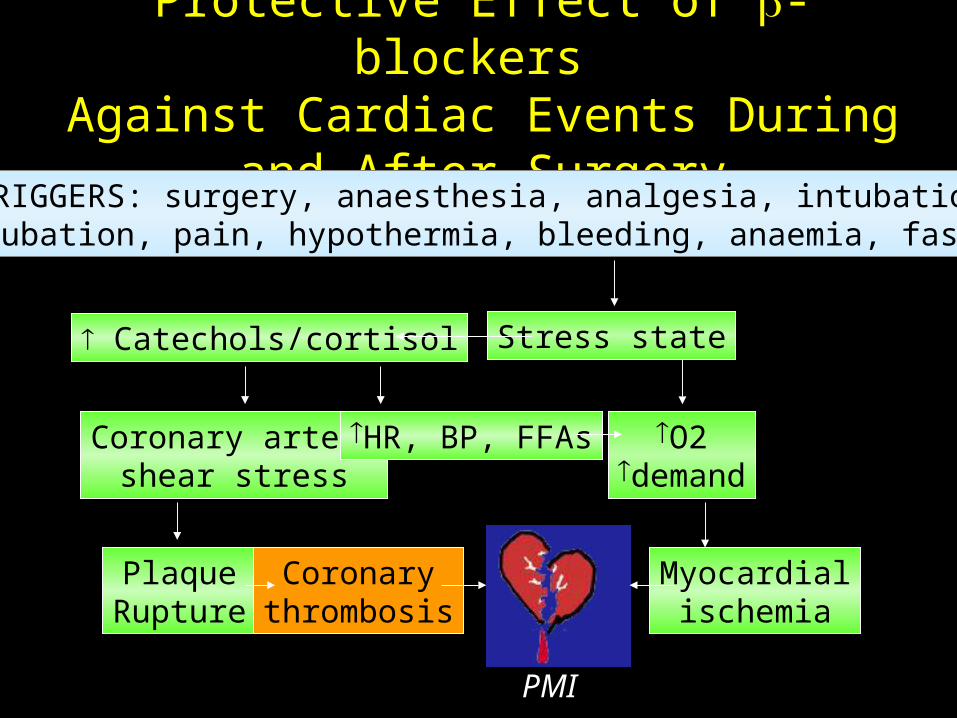
Protective Effect of -blockers Against Cardiac Events During and After Surgery
TRIGGERS: surgery, anaesthesia, analgesia, intubation,extubation, pain, hypothermia, bleeding, anaemia, fasting
Stress state
PlaqueRupture
Coronarythrombosis
O2demand
Myocardialischemia
PMI
Catechols/cortisol
Coronary arteryshear stress
HR, BP, FFAs
Reducing Myocardial Ischemia
Avoid tachycardia & hypertension Avoid hypotension Avoid pain Avoid hypercoagulation Avoid vasospasm Avoid tissue injury
Does Perioperative Beta Blockade Work?
Perioperative β-Blockers 1995 to 2005 Mangano et al. at 19961
Atenolol study Poldermans et al. at 19992
DECREASE trialPerioperative β -blockers 2005–2008 Yang et al. at 20064
MaVS study Juul et al. at 20065
DiPoM trial
Effect of Atenolol on Mortality andCardiovascular Morbidity After
Noncardiac Surgery
Mangano DT, Layug EL, Wallace A, et al. N Engl J Med. 1996; 335: 1713-1720
Mangano Trial: Overview Randomized, double-blind, placebo-controlled trial 200 patients included VA (Veterans’ Admin) patients with >= 2
risk factors for CAD Age >65 y/o Total cholesterol >240 mg/dL Hypertension Diabetes mellitus Current smoking
Surgeries were: Major vascular (~40%) “Intraabdominal” (~20%) Neurosurgery, general, plastic surgery and head and neck surgery
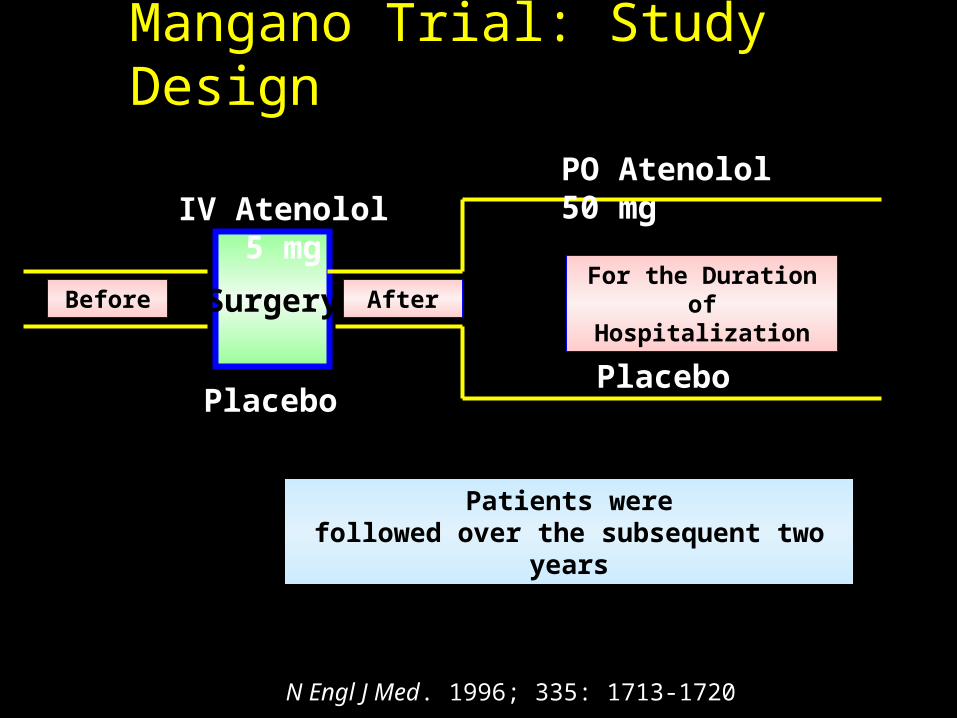
Mangano Trial: Study Design
Surgery
PO Atenolol 50 mg
Patients werefollowed over the subsequent two years
IV Atenolol 5 mg
Placebo
Before After
Placebo
For the Duration of Hospitalization
N Engl J Med. 1996; 335: 1713-1720
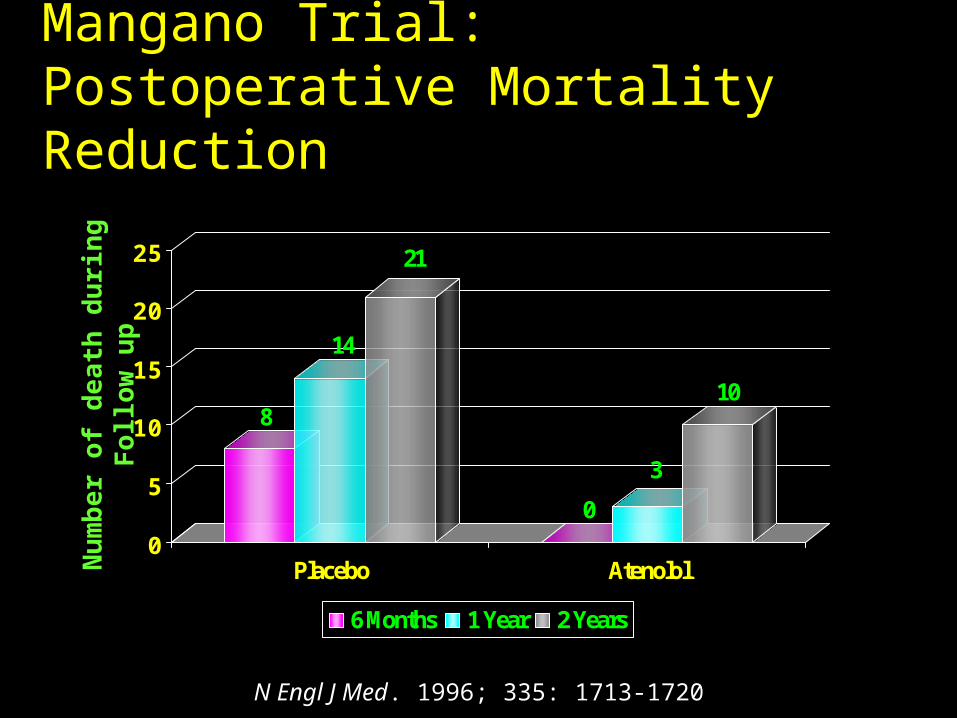
Mangano Trial: Postoperative Mortality Reduction
8
14
21
0
3
10
0
5
10
15
20
25
Placebo Atenolol
6 Months 1 Year 2 Years
Num
ber o
f dea
th d
urin
g Fo
llow
up
N Engl J Med. 1996; 335: 1713-1720
The Effect of Bisoprolol on PerioperativeMortality and Myocardial Infarction in High-risk
Patients Undergoing Vascular SurgeryDutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group
Poldermans D, Boersma E, Bax JJ, et al. N Engl J Med 1999; 341:1789–1794
The DECREASE Trial : Overview
European, multicentered, unblinded RCT 112 high risk patients undergoing major vascular
surgery were randomized to Bisoprolol 5mg orally (min. of 7 days before surgery)
(n = 59) Standard care (n = 53)
The study was stopped early
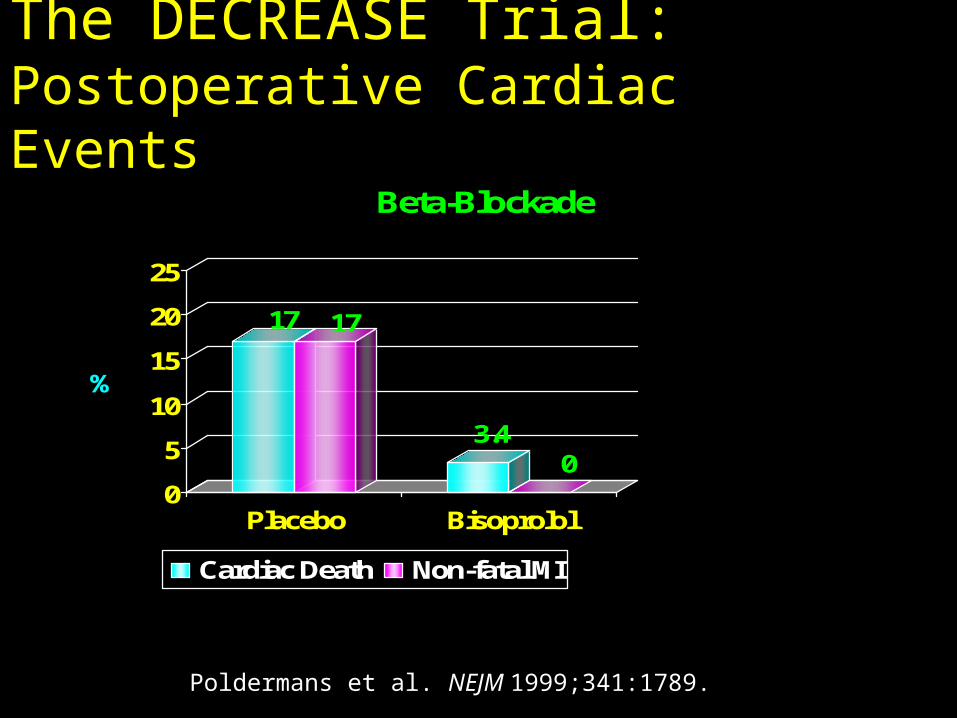
The DECREASE Trial:Postoperative Cardiac Events
17 17
3.40
0
5
10
15
20
25
%
Placebo Bisoprolol
Beta-Blockade
Cardiac Death Non-fatal MI
Poldermans et al. NEJM 1999;341:1789.
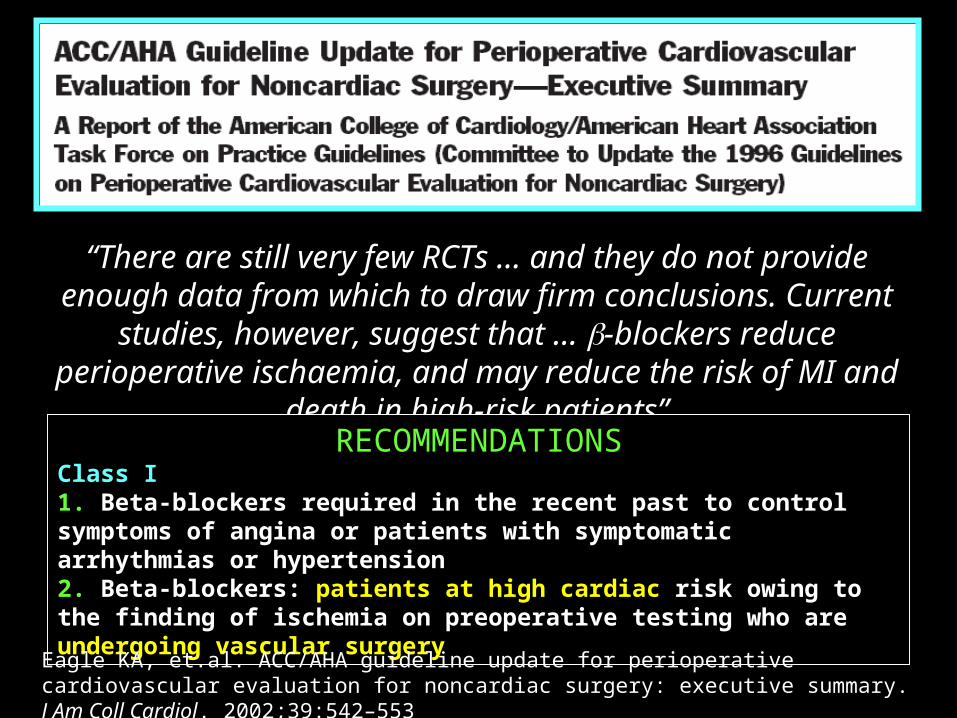
““There are still very few RCTs … and they do not provide enough data from which to draw firm
conclusions. Current studies, however, suggest that … -blockers reduce perioperative ischaemia, and may reduce the risk of MI and death in high-risk
patients”RECOMMENDATIONSClass I1. Beta-blockers required in the recent past to control symptoms of angina or patients with symptomatic arrhythmias or hypertension2. Beta-blockers: patients at high cardiac risk owing to the finding of ischemia on preoperative testing who are undergoing vascular surgery
Eagle KA, et.al. ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery: executive summary. J Am Coll Cardiol. 2002;39:542–553
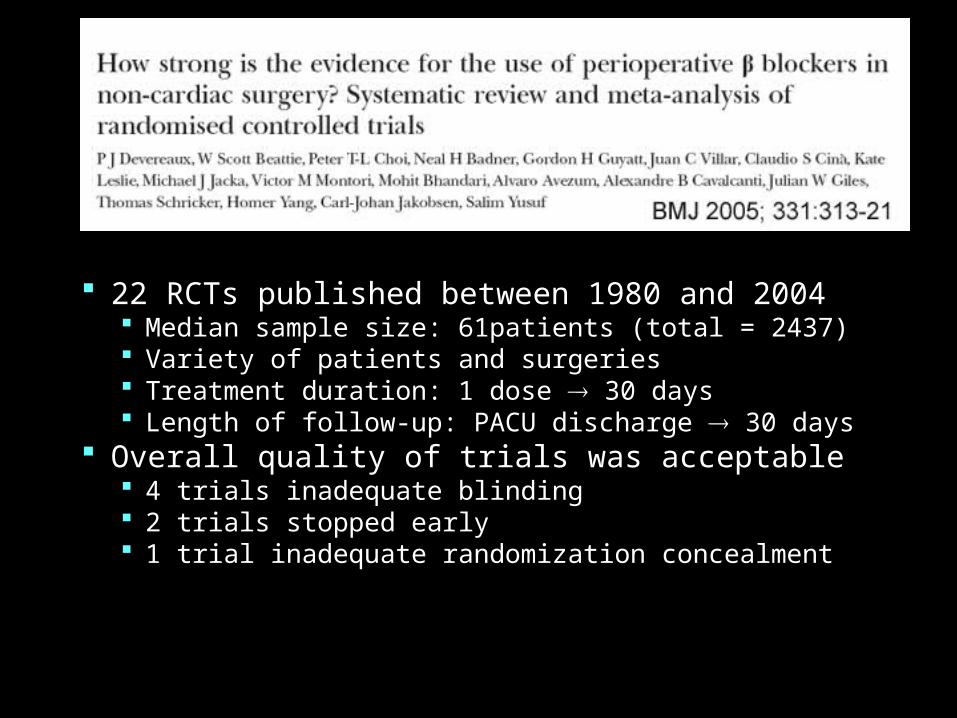
22 RCTs published between 1980 and 2004 Median sample size: 61patients (total = 2437) Variety of patients and surgeries Treatment duration: 1 dose 30 days Length of follow-up: PACU discharge 30 days
Overall quality of trials was acceptable 4 trials inadequate blinding 2 trials stopped early 1 trial inadequate randomization concealment
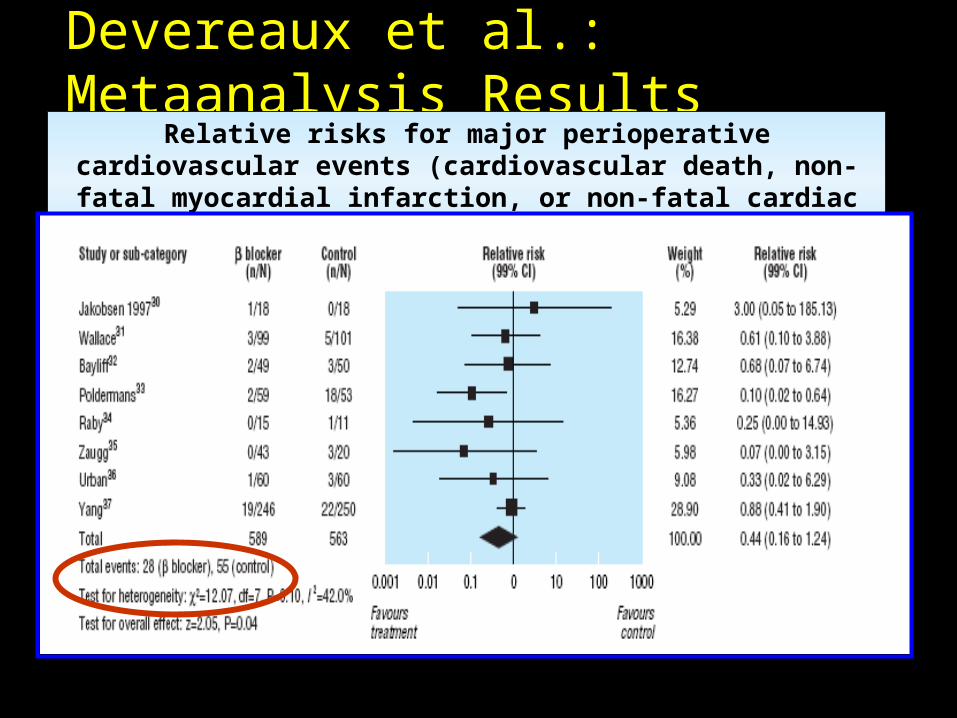
Devereaux et al.: Metaanalysis ResultsRelative risks for major perioperative cardiovascular events (cardiovascular
death, non-fatal myocardial infarction, or non-fatal cardiac arrest)
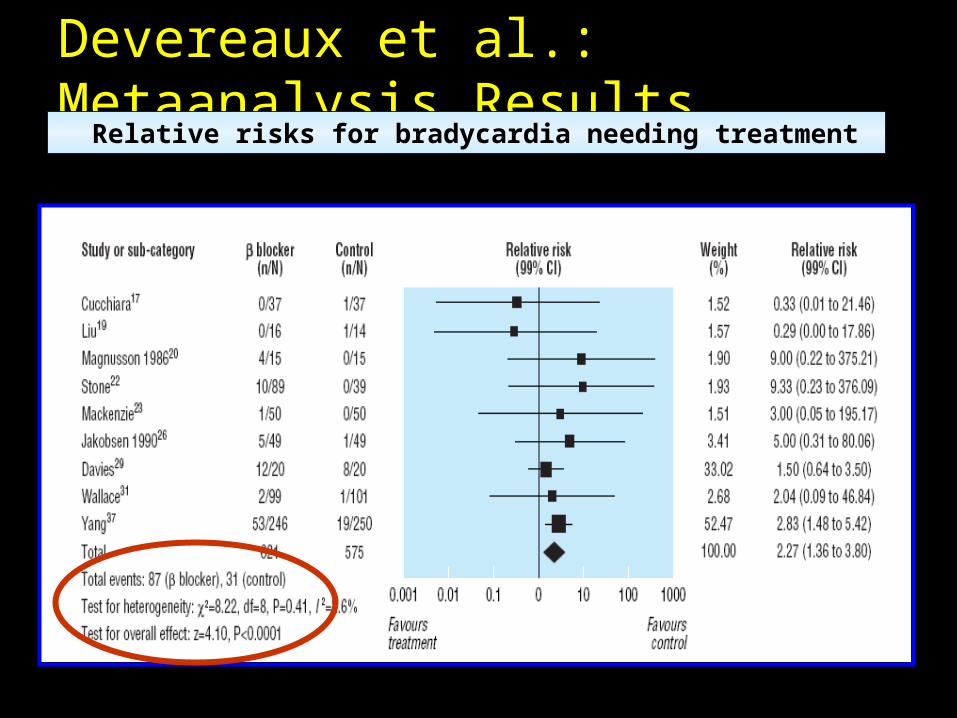
Devereaux et al.: Metaanalysis Results Relative risks for bradycardia needing treatment
Devereaux et al.: Metaanalysis Conclusion Growing evidence suggests BB may reduce the
risk of major perioperative cardiovascular events However, increases the risk of bradycardia and
hypotension requiring treatment Evidence indicates that more further studies are
needed
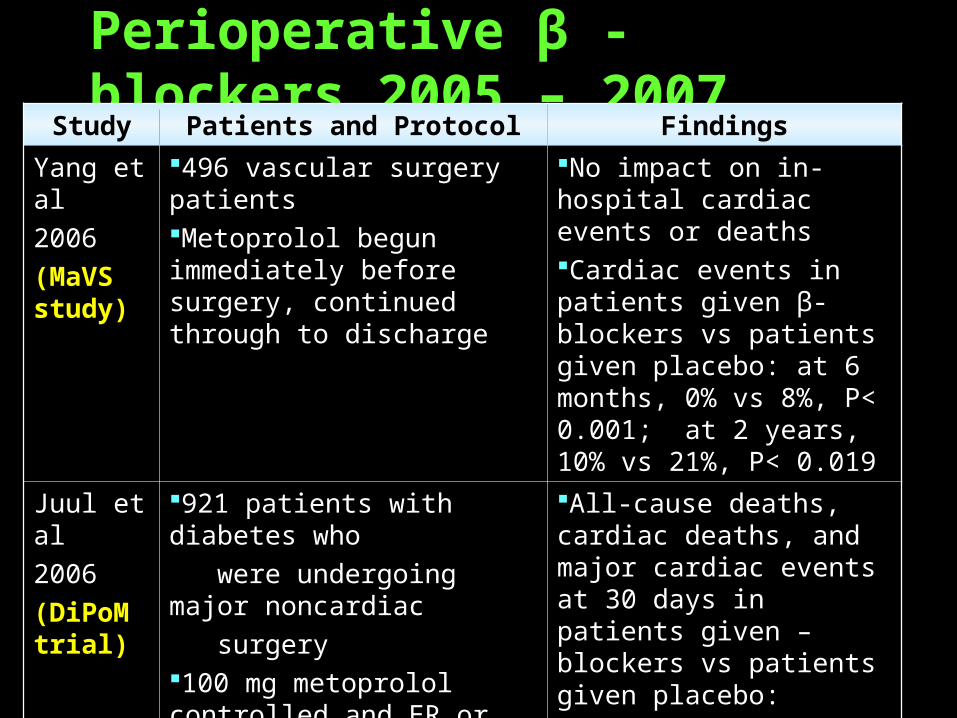
Perioperative β -blockers 2005 – 2007Study Patients and Protocol Findings
Yang et al2006(MaVS study)
496 vascular surgery patientsMetoprolol begun immediately before surgery, continued through to discharge
No impact on in-hospital cardiac events or deathsCardiac events in patients given β-blockers vs patients given placebo: at 6 months, 0% vs 8%, P< 0.001; at 2 years, 10% vs 21%, P< 0.019
Juul et al2006(DiPoM trial)
921 patients with diabetes who were undergoing major noncardiac surgery100 mg metoprolol controlled and ER or placebo administered from the day before surgery to a maximum of 8 perioperative days
All-cause deaths, cardiac deaths, and major cardiac events at 30 days in patients given –blockers vs patients given placebo:
21% vs 20%, P = NS
Does Perioperative Beta Blockade Increase Risk ?
Perioperative -blockade (POBBLE) for patients
undergoing infrarenal vascular surgery: Results of
a randomized double-blind controlled trial.
POBBLE Trial Investigators, London, United Kingdom
Brady AR, et.al. J Vasc Surg 2005; 41:602–609
Double-blind randomized placebo-controlled trial Included low risk patients
Treatment Metoprolol 50 mg PO BID or placebo ( from
admission until 7 days after surgery) Primary endpoint
30 day cumulative risk of cardiac death, non-fatal MI, unstable angina, VT or stroke
Patient group (n = 103 [stopped early])
POBBLE Trial Overview
Brady AR, et.al. J Vasc Surg 2005; 41:602–609
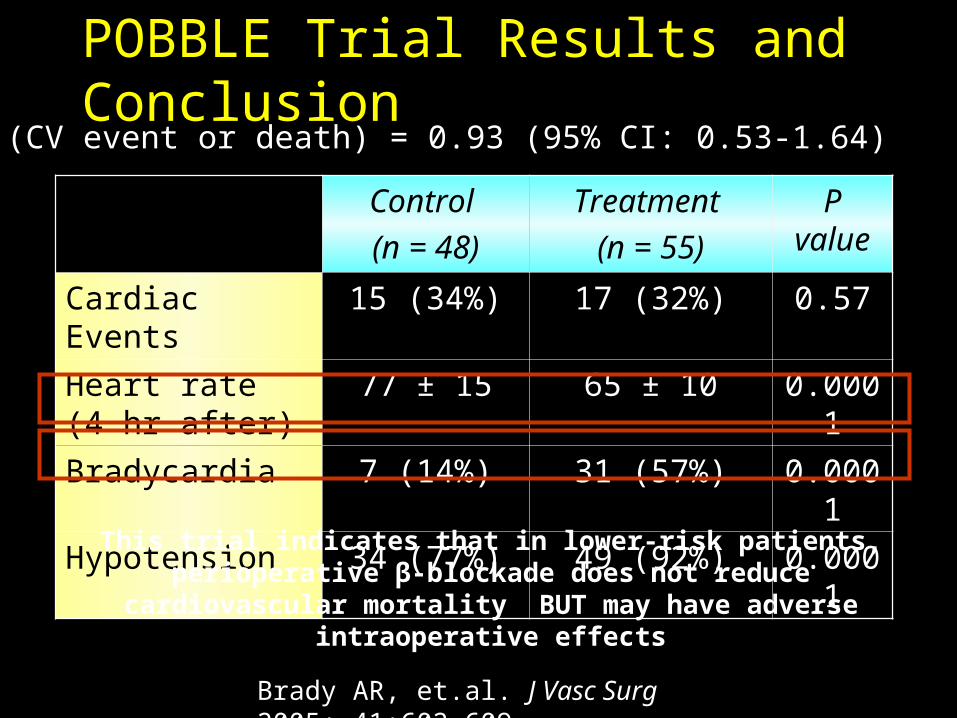
Control
(n = 48)
Treatment
(n = 55)
P value
Cardiac Events 15 (34%) 17 (32%) 0.57
Heart rate (4 hr after) 77 ± 15 65 ± 10 0.0001
Bradycardia 7 (14%) 31 (57%) 0.0001
Hypotension 34 (77%) 49 (92%) 0.0001
POBBLE Trial Results and ConclusionOR (CV event or death) = 0.93 (95% CI: 0.53-1.64)
This trial indicates that in lower-risk patients, perioperative β-blockade does not reduce cardiovascular mortality BUT may have adverse intraoperative effects
Brady AR, et.al. J Vasc Surg 2005; 41:602–609
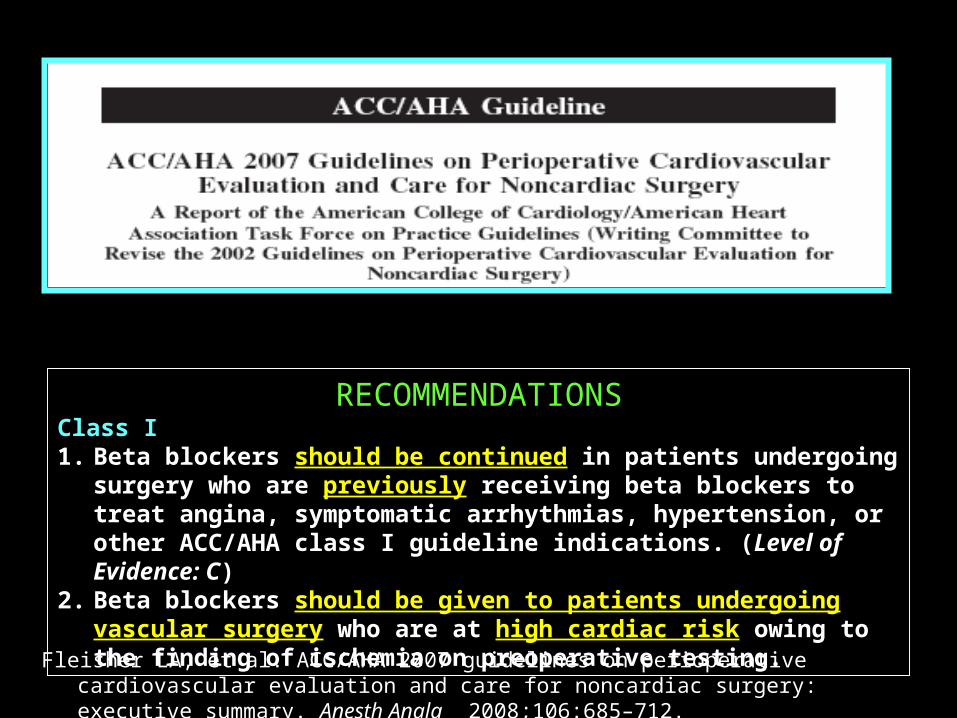
RECOMMENDATIONSClass I1. Beta blockers should be continued in patients undergoing surgery who are previously
receiving beta blockers to treat angina, symptomatic arrhythmias, hypertension, or other ACC/AHA class I guideline indications. (Level of Evidence: C)
2. Beta blockers should be given to patients undergoing vascular surgery who are at high cardiac risk owing to the finding of ischemia on preoperative testing.
Fleisher LA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary. Anesth Analg 2008;106:685–712.
Perioperative Beta Blockade After
Another heated debate about the pros and cons of using beta blockers perioperatively in noncardiac surgery
RCT of metoprolol versus placebo (30 d) Non-cardiac surgery With or at risk of IHD
Sample size 10,000 patients
Primary outcome 30 day cumulative risk of cardiac death, nonfatal MI and
non-fatal cardiac arrest
Devereaux PJ,et al. Am J Heart 2006; 152: 223-30
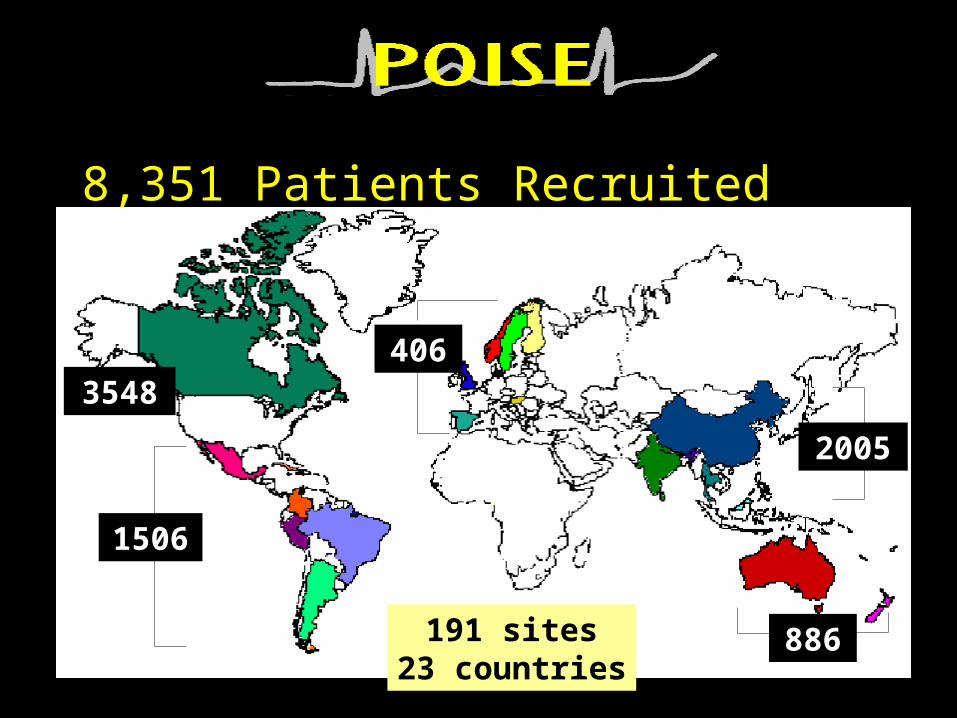
8,351 Patients Recruited
3548
1506
406
886191 sites23 countries
2005
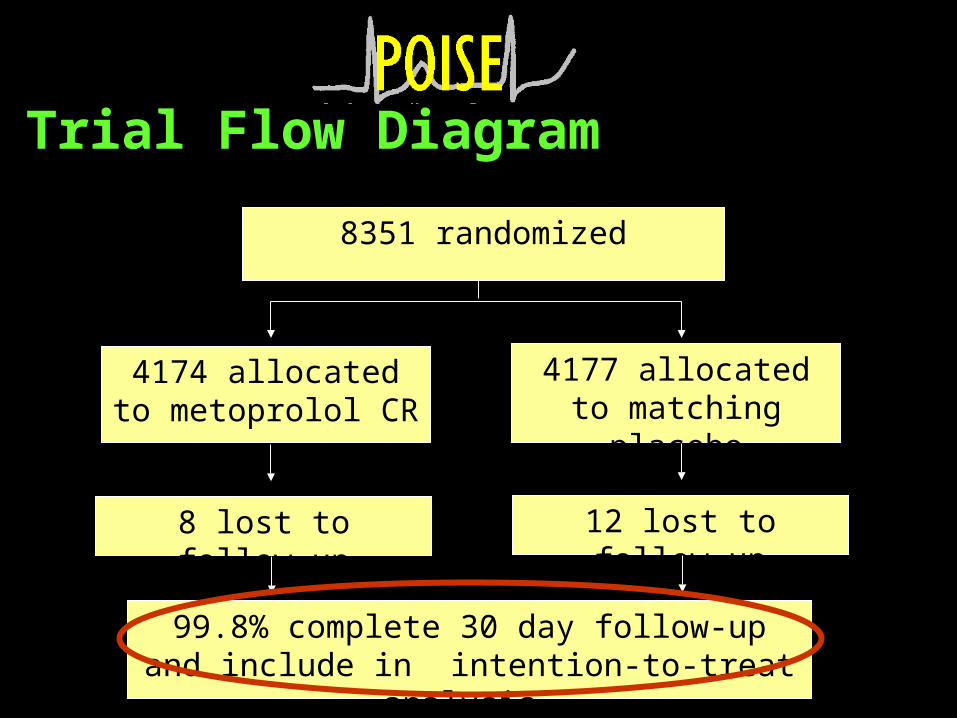
Trial Flow Diagram
8351 randomized
4174 allocated to metoprolol CR
8 lost to follow-up
4177 allocated to matching placebo
12 lost to follow-up
99.8% complete 30 day follow-up and include in intention-to-treat analysis
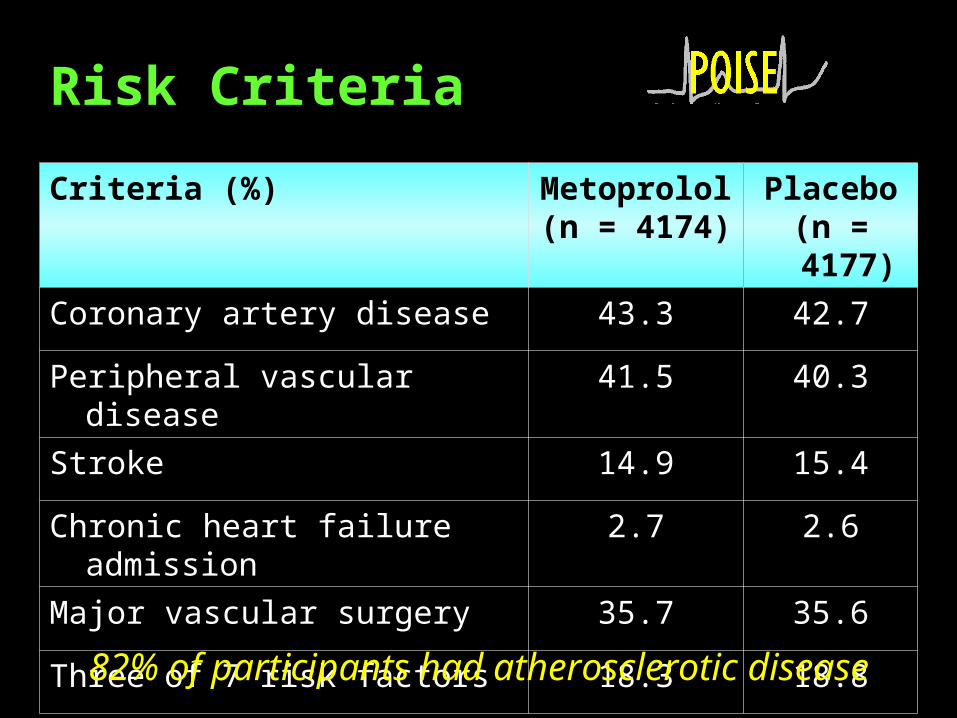
Criteria (%) Metoprolol (n = 4174)
Placebo(n = 4177)
Coronary artery disease 43.3 42.7
Peripheral vascular disease 41.5 40.3
Stroke 14.9 15.4
Chronic heart failure admission 2.7 2.6
Major vascular surgery 35.7 35.6
Three of 7 risk factors 18.3 18.8
82% of participants had atherosclerotic disease
Risk Criteria
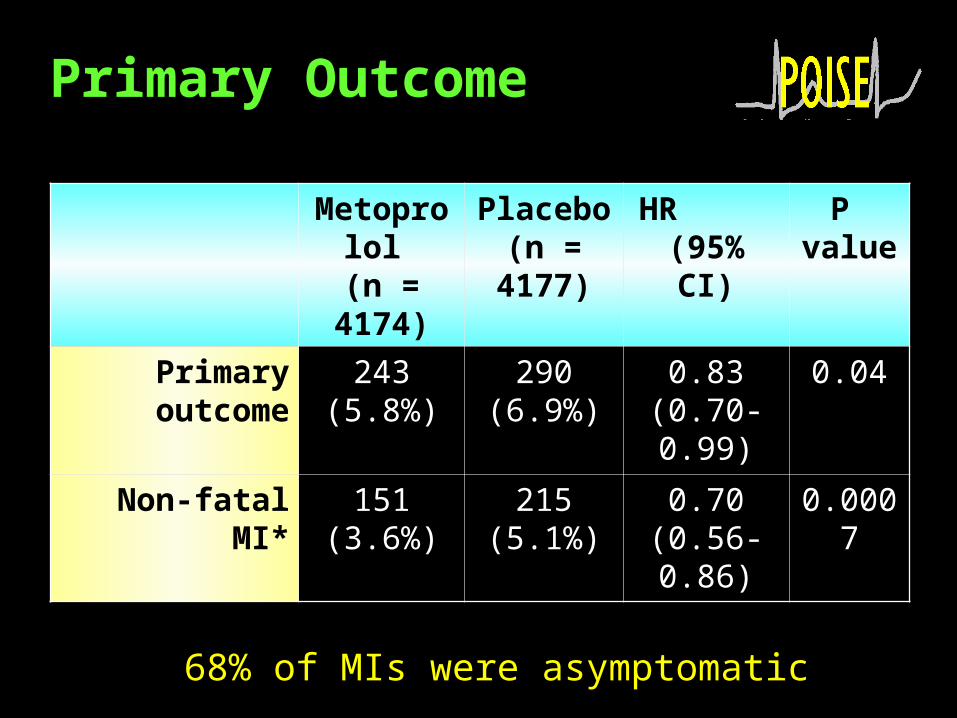
Primary Outcome
Metoprolol (n = 4174)
Placebo(n = 4177)
HR (95% CI)
P value
Primary outcome 243(5.8%)
290(6.9%)
0.83(0.70-0.99)
0.04
Non-fatal MI* 151(3.6%)
215(5.1%)
0.70(0.56-0.86)
0.0007
68% of MIs were asymptomatic
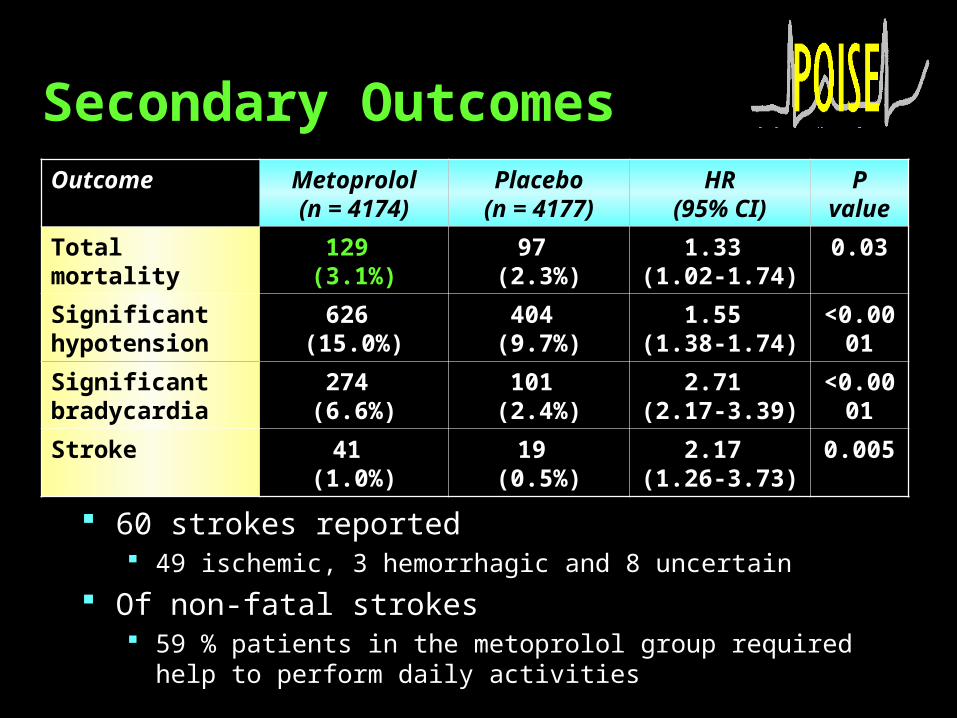
Secondary Outcomes
60 strokes reported 49 ischemic, 3 hemorrhagic and 8 uncertain
Of non-fatal strokes 59 % patients in the metoprolol group required help to perform daily
activities
Outcome Metoprolol(n = 4174)
Placebo(n = 4177)
HR(95% CI)
Pvalue
Total mortality 129 (3.1%)
97 (2.3%)
1.33 (1.02-1.74)
0.03
Significanthypotension
626 (15.0%)
404 (9.7%)
1.55 (1.38-1.74)
<0.0001
Significant bradycardia
274 (6.6%)
101 (2.4%)
2.71 (2.17-3.39)
<0.0001
Stroke 41 (1.0%)
19 (0.5%)
2.17 (1.26-3.73)
0.005
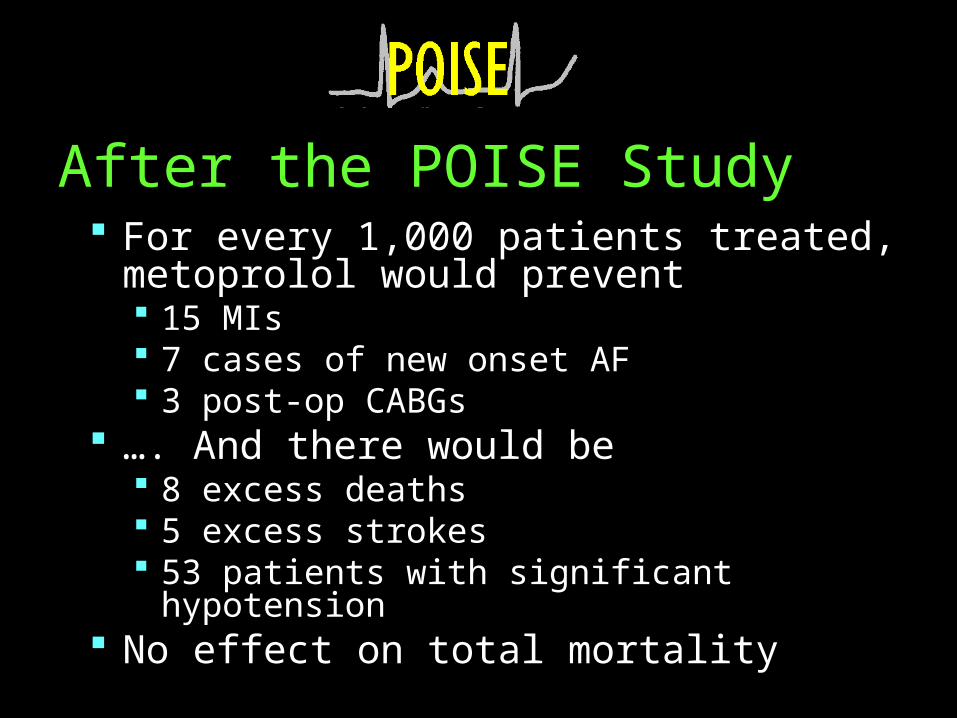
After the POISE Study For every 1,000 patients treated, metoprolol would
prevent 15 MIs 7 cases of new onset AF 3 post-op CABGs
…. And there would be 8 excess deaths 5 excess strokes 53 patients with significant hypotension
No effect on total mortality
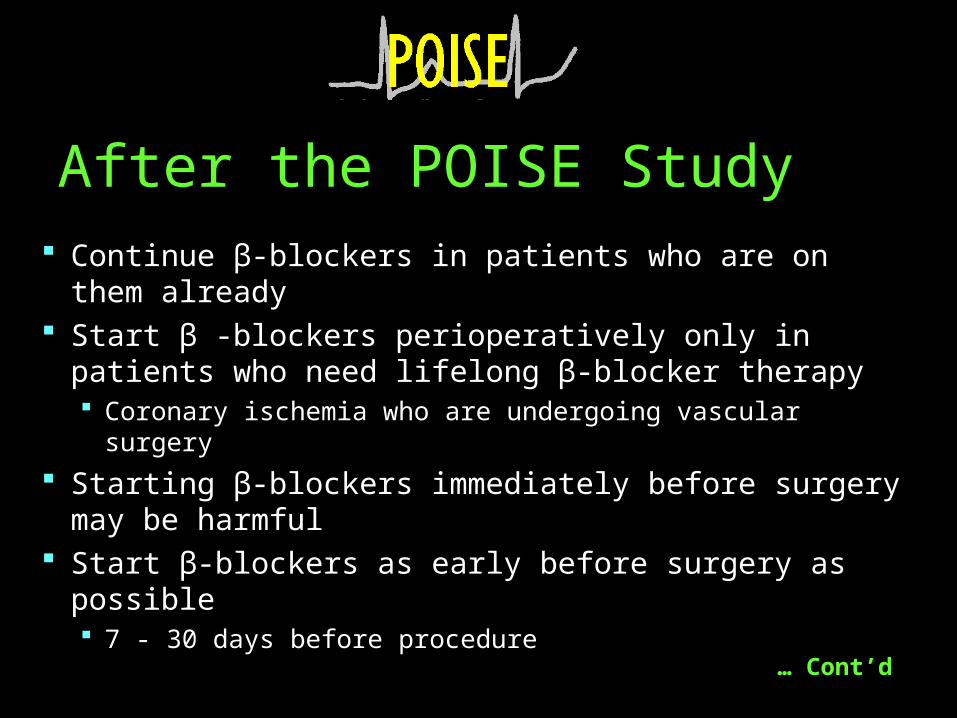
Continue β-blockers in patients who are on them already Start β -blockers perioperatively only in patients who need
lifelong β-blocker therapy Coronary ischemia who are undergoing vascular surgery
Starting β-blockers immediately before surgery may be harmful
Start β-blockers as early before surgery as possible 7 - 30 days before procedure
After the POISE Study
… Cont’d
After surgery focus shifts to continuing β-blockers appropriately Assess for infection, pain, hypovolemia, or bleeding
If discontinuing β-blockers Titrate Restart as soon as unstable issues are resolved
After the POISE Study
… Cont’d
Conclusion
The data suggests that Beta Blockers are beneficial in patients with major cardiac risk
Beta Blockers associated with severe bradycardia and hypotension leading to stroke and death
Patients with low cardiac risk may exhibit a higher risk/benefit ratio
Intermediate risk patient need to undergo for further work up