Phase 2 study of bintrafusp alfa, a bifunctional fusion protein ......Abstract No. 1416. Presented...
1
Abstract No. 1416. Presented at the ESMO Virtual Congress 2020, September 19–21, 2020 Phase 2 study of bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in platinum-experienced advanced cervical cancer M. J. Birrer 1 , L. R. Mileshkin 2 , K. Fujiwara 3 , I. Ray-Coquard 4,5 , J. Alexandre 4,6 , A. Okamoto 7 , M. R. Mirza 8 , J. L. Gulley 9 , G. Jehl 10 , S. C. Ramage 11 , L. S. Ojalvo 11 , S. M. Campos 12 1 Winthrop P. Rockefeller Cancer Institute, University of Arkansas Medical School, Little Rock, AR, USA; 2 Peter MacCallum Cancer Centre, Melbourne, VIC, Australia; 3 Saitama Medical University International Medical Center, Saitama, Japan; 4 GINECO Group, Paris, France; 5 Department of Medical Oncology, Centre Leon Berard, University Claude Bernard Lyon, Lyon, France; 6 Department of Medical Oncology, Université de Paris, Hôpital Cochin, Paris, France; 7 The Jikei University School of Medicine, Tokyo, Japan; 8 Nordic Society of Gynaecological Oncology, Clinical Trial Unit and Copenhagen University Hospital, Copenhagen, Denmark; 9 Genitourinary Malignancies Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA; 10 Merck KGaA, Darmstadt, Germany; 11 EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany; 12 Division of Medical Oncology, Dana Farber Cancer Institute, Harvard Medical School, Boston, MA, USA Poster No. 879TiP BACKGROUND Cervical cancer • Cervical cancer is one of the most common and lethal cancers among females worldwide, with virtually all cases associated with persistent human papillomavirus (HPV) infection 1-3 • Platinum-containing chemotherapy (CT), with or without bevacizumab, are the most common first-line (1L) treatments for recurrent/metastatic cervical cancer with median overall survival (OS) between 9.7 months (without bevacizumab) to 25.0 months (with bevacizumab) 4-9 • There is currently no globally accepted standard-of-care treatment for patients with recurrent/metastatic cervical cancer that progressed during or after platinum-containing CT, and there remains an urgent, unmet need for these patients 4 – Therapeutic options after 1L therapy are limited due to low response rates (3–10%) that are short-lived and associated with variable toxicities 10,11 • In the United States, pembrolizumab has received accelerated approval for the treatment of PD-L1–positive (combined positive score ≥1) cervical cancer that progressed on/after CT 12 – The overall response rate (ORR) of patients with PD-L1– positive tumors was 14.3% (11/77) – Responses were limited in patients with adenocarcinoma histology and those who previously received bevacizumab; there were no responses in patients with PD-L1–negative tumors Transforming growth factor β (TGF-β) • TGF-β has a multifunctional role in the development and progression of cervical cancer, and is upregulated in cervical cancer cells and in the tumor microenvironment (TME) by HPV 13-16 – TGF-β signaling can induce epithelial-to-mesenchymal transition (EMT), a hallmark of tumor progression and a key driver of metastasis, which plays an important role in cervical cancer 14 – TGF-β can promote immune escape and may play a role in mediating resistance to anti–PD-(L)1 therapies 13-14 – TGF-β signaling promotes angiogenesis in cervical cancer, which is commonly associated with increased invasiveness and worse survival 13-16 • Therefore, inhibition of the TGF-β pathway in the TME while simultaneously blocking an additional immunosuppressive cellular mechanism, such as the PD-L1 pathway, may provide a novel treatment approach for cervical cancer Bintrafusp alfa • Bintrafusp alfa is a first-in-class bifunctional fusion protein composed of the extracellular domain of the TGF-βRII receptor to function as a TGF-β “trap” fused to a human IgG1 antibody blocking PD-L1 (Figure 1) 17 – The bifunctional nature of bintrafusp alfa might allow for colocalized, simultaneous inhibition of two nonredundant immunosuppressive pathways (TGF-β and PD-L1) within the TME, which might enhance the anticancer effect observed with independent blockade of both pathways 17,18 • In cohorts of a global, phase 1 trial (NCT02517398), bintrafusp alfa treatment demonstrated encouraging clinical activity and a manageable safety profile in 25 patients with heavily pretreated recurrent/metastatic cervical cancer who had disease progression during or after platinum-containing CT 19 – The investigator-assessed ORR per RECIST 1.1 was 24.0%; an additional patient developed a sustained response after initial progressive disease (total clinical response, 28.0%) – Responses were irrespective of tumor cell PD-L1 expression, histology, and prior treatments, including bevacizumab – Responses were long-lasting (range, 4.2–30.4 months), and the median OS was 11.6 months • INTR@PID CERVICAL 017 (NCT04246489) will evaluate the clinical benefit of bintrafusp alfa in patients with advanced unresectable/metastatic cervical cancer who progressed during or after platinum-containing CT Figure 1. Proposed mechanism of action of bintrafusp alfa Fibroblast CAF Fibrosis and impaired drug access EMT (leading to metastasis and resistance to therapy [including checkpoint inhibition]) Tumor angiogenesis Tumor cells PD-L1 Bintrafusp alfa PD-1 T cell Suppression of immune response NK cell TAM Dendritic cell Cytotoxic T cell Tumor cells Mesenchymal-like tumor cell TGF-β “trap” moiety sequesters TGF-β to block downstream signaling Anti–PD-L1 mAb moiety blocks PD-L1 interactions with PD-1 TGF-β* CAF, cancer-associated fibroblast; NK, natural killer; TAM, tumor-associated macrophage. *Tumor cells are also a major source of TGF-β in the microenvironment. TRIAL DESIGN • This is a global, single-arm, phase 2 trial to evaluate the safety and efficacy of bintrafusp alfa monotherapy in patients with advanced unresectable/metastatic cervical cancer who had disease progression with or were intolerant of platinum- containing CT (NCT04246489) (Figure 2) • Planned enrollment is 135 patients • As a monotherapy treatment in cervical cancer, a 1200 mg every 2 weeks (Q2W) flat dose of bintrafusp alfa by intravenous (IV) infusion has been selected as the recommended phase 2 dose 20 – Eligible patients will receive study treatment until confirmed disease progression, death, unacceptable toxicity, or study withdrawal; treatment past progression is allowed for patients with stable clinical status • Key inclusion and exclusion criteria are described in Table 1 Figure 2. INTR@PID CERVICAL 017 (NCT04246489) Bintrafusp alfa 1200 mg IV Q2W Key endpoints: ORR, DOR, DRR, safety, PFS, OS, pharmacokinetics, clinical efficacy according to PD-L1 expression Advanced unresectable/metastatic cervical cancer N=135 DOR, duration of response; DRR, durable response rate. Table 1. Key eligibility criteria Selected inclusion criteria Selected exclusion criteria • Age ≥18 years • Histologically documented advanced unresectable and/or metastatic cervical cancer • Disease progression during or after prior platinum-containing CT* • Availability of archival tumor tissue sample or newly obtained (preferred) biopsy of tumor lesion • ECOG performance status of 0 or 1 • Adequate organ and coagulation function • Life expectancy ≥12 weeks • Prior cancer immunotherapy or treatment targeting T-cell costimulation, checkpoint pathways, or immune- suppressive pathways (such as TGF-β) • Active central nervous system metastases causing clinical symptoms or requiring therapeutic intervention ECOG, Eastern Cooperative Oncology Group. *Prior platinum-containing CT may be a systemic treatment for metastatic disease or in the adjuvant or neoadjuvant setting. Participants who were intolerant to or ineligible for platinum-containing CT are eligible for this trial. • Primary and secondary endpoints are described in Table 2 • Key exploratory objectives include: – Evaluation of the clinical efficacy of bintrafusp alfa based on immune-related ORR and immune-related PFS – Evaluation of biological response or predictive markers in blood, tumor, and TME, and their relationship to drug exposure, clinical response, or other biological markers of response – Clinical efficacy according to demographic and clinical variables corresponding to cervical cancer prognosis – Patient-reported quality of life and symptoms Table 2. Trial endpoints Primary endpoints • ORR according to RECIST 1.1 as assessed by IRC Secondary endpoints • DOR, DRR,* and PFS according to RECIST 1.1 as assessed by IRC • Safety (TEAEs, TRAEs, SAEs) according to NCI-CTCAE v5.0 • ORR, DOR, DRR,* and PFS according to RECIST 1.1 as assessed by investigator • OS • Pharmacokinetics of bintrafusp alfa • Clinical efficacy of bintrafusp alfa according to PD-L1 expression IRC, independent review committee; SAE, serious adverse event; TEAE, treatment-emergent adverse event; TRAE, treatment-related adverse event. *Durable response of ≥6 months. • Enrollment in the INTR@PID CERVICAL 017 trial began in March 2020 and is ongoing • This trial is being conducted at 85 sites in North and South America, Europe, and the Asia-Pacific region (Figure 3) • Refer to ClinicalTrials.gov (NCT04246489) for additional information Figure 3. Participating countries Argentina Australia Belgium Brazil China France Hungary Japan Republic of Korea Russia Spain United States REFERENCES 1. Saraiya M, et al. J Natl Cancer Inst. 2015;107:jv086. 2. Walboomers JM, et al. J Pathol. 1999;189:12-9. 3. Bray F, et al. CA Cancer J Clin. 2018;68:394-424. 4. Marth C, et al. Ann Oncol. 2017;28(Suppl 4):iv72-iv83. 5. Moore DH, et al. J Clin Oncol. 2004;22:3113-9. 6. Monk BJ C, et al. J Clin Oncol. 2009;27:4649-55. 7. Kitagawa R, et al. J Clin Oncol. 2015;33:2129-35. 8. Tewari KS, et al. Lancet. 2017;390:1654-63. 9. Redondo A, et al. Gynecol Oncol. 2020 Aug 4. [Epub ahead of print]. 10. McLachlan J, et al. Clin Oncol (R Coll Radiol). 2017;29:153-60. 11. Monk BJ, et al. J Clin Oncol. 2009;27:1069-74. 12. Chung HC, et al. J Clin Oncol. 2019;37:1470-8. 13. Torres-Poveda K, et al. World J Clin Oncol. 2014;5:753-63. 14. Lee MY and Shen MR. Am J Transl Res. 2012;4:1-13. 15. Holmgaard RB, et al. J Immunother Cancer. 2018;6:47. 16. Zijlmans JH, et al. Br J Cancer. 2009;100: 1617-26. 17. Lan Y, et al. Sci Transl Med. 2018;10:eaan5488. 18. Knudson KM. Oncoimmunol. 2018;7:e1426519. 19. Allan S, et al. Int J Gynecol Cancer. 2019;29(Suppl 4):Poster P37. 20. Vugmeyster Y, et al. Clin Pharmacol Ther. 2020 Jan 18. [Epub ahead of print]. ACKNOWLEDGEMENTS This trial is sponsored by Merck KGaA, Darmstadt, Germany, and is part of an alliance between Merck KGaA and GlaxoSmithKline. The authors thank the patients and their families, investigators, co-investigators, and study teams at each of the participating centers and at Merck KGaA and EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA. Medical writing support was provided by Yao Bian, PhD, MedicalExpressions Inc, Chicago, IL, USA, which was also funded by Merck KGaA and GlaxoSmithKline, in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3). Correspondence: Michael J. Birrer, [email protected] DISCLOSURES MJB has received honoraria (self) from Clovis, AstraZeneca, and Roche/Genentech. LRM has nothing to disclose. KF has received honoraria (self) from Chugai-Roche, AstraZeneca, Nipponkayaku, Kyowa-Kirin, and Zeria; had advisory/ consultancy roles with Eisai, MSD, Genmab, and Nanocarrier; received research grants/funding from AstraZeneca, Chugai-Roche, Eisai, Genmab, Regeneron, and Zeria; received travel/accommodation/expenses from Merck KGaA, Darmstadt, Germany. IR-C has received honoraria (self) from AbbVie, Agenus, Advaxis, Bristol Myers Squibb, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche, GlaxoSmithKline, Deciphera, Mersena, Merck Serono, Novartis, Amgen, Tesaro, Clovis, and Merck KGaA, Darmstadt, Germany; received honoraria (institution) from GlaxoSmithKline, Roche, Bristol Myers Squibb, and Merck KGaA; had advisory/consultancy roles with AbbVie, Agenus, Advaxis, Bristol Myers Squibb, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche/Genentech, GlaxoSmithKline, Deciphera, Mersena, Merck Serono, Novartis, Amgen, Tesaro, Clovis, and Merck KGaA; received research grant/funding (self) from Merck KGaA, Roche, and Bristol Myers Squibb; received research grant/funding (institution) from Merck KGaA, Roche, Bristol Myers Squibb, Novartis, AstraZeneca, and Merck Serono; received travel/accommodation/expenses from Roche, AstraZeneca, and GlaxoSmithKline; participated in non-remunerated activities for GINECO, ENGOT, GCIG, European Community, ESMO, ASCO, ESGO, IGSC, Inca, and Swiss, Italian, Belgium and German health authorities. JA has received honoraria (self) from AstraZeneca, GlaxoSmithKline, Roche, PharmaMar, Novartis, and Merck KGaA, Darmstadt, Germany; had advisory/ consultancy roles with Merck KGaA, AstraZeneca, GlaxoSmithKline, Roche, PharmaMar, and Novartis; received grant/ funding (institution) from Merck KGaA and Janssen; received travel/accommodation/expenses from Janssen, Roche, and Novartis. AO has had speaking/expert testimony roles for AstraZeneca and received research grants/funding from Kissei Pharmaceuticals, Kaken Pharmaceutical, Meiji Holdings, Nippon Shinyaku, Chugai, Taiho, Daiichi Sankyo, Tsumura & Co., and ASKA Pharmaceutical. MRM has personal financial interests in AstraZeneca, Biocad, Clovis, Geneos, Genmab, Karyopharm Therapeutics, Merck Serono, Oncology Venture, Pfizer, Roche, Seattle Genetics, Sera Prognostics, Sotio, Tesaro/GlaxoSmithKline, ZaiLab, and Merck KGaA, Darmstadt, Germany; had leadership roles with Karyopharm Therapeutics and Sera Prognostics; received research grant/funding (institution) from AstraZeneca, Boehringer Ingelheim, Clovis Oncology, Pfizer, and Tesaro/GlaxoSmithKline; participated in other activities with DGCG, GCIG, ESGO, and ENGOT. JLG has received research grant/funding (institution) from Merck KGaA, Darmstadt, Germany. GJ is an employee of Merck KGaA, Darmstadt, Germany. SR and LSO are employees of and may hold shares in EMD Serono Research & Development Institute, Inc; a business of Merck KGaA, Darmstadt, Germany. SMC has received honoraria (self and institution) from Tesaro and Eisai; had advisory/consultancy roles with Tesaro and Eisai. Copies of this e-poster obtained through QR (Quick Response) and/or text key codes are for personal use only and may not be reproduced without written permission of the authors. GET POSTER PDF
Transcript of Phase 2 study of bintrafusp alfa, a bifunctional fusion protein ......Abstract No. 1416. Presented...
Abstract No. 1416. Presented at the ESMO Virtual Congress 2020, September 19–21, 2020
Phase 2 study of bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in platinum-experienced advanced cervical cancer
M. J. Birrer1, L. R. Mileshkin2, K. Fujiwara3, I. Ray-Coquard4,5, J. Alexandre4,6, A. Okamoto7, M. R. Mirza8, J. L. Gulley9, G. Jehl10, S. C. Ramage11, L. S. Ojalvo11, S. M. Campos12
1Winthrop P. Rockefeller Cancer Institute, University of Arkansas Medical School, Little Rock, AR, USA; 2Peter MacCallum Cancer Centre, Melbourne, VIC, Australia; 3Saitama Medical University International Medical Center, Saitama, Japan; 4GINECO Group, Paris, France; 5Department of Medical Oncology, Centre Leon Berard, University Claude Bernard Lyon, Lyon, France; 6Department of Medical Oncology, Université de Paris, Hôpital Cochin, Paris, France; 7The Jikei University School of Medicine, Tokyo, Japan; 8Nordic Society of Gynaecological Oncology, Clinical Trial Unit and Copenhagen University Hospital, Copenhagen, Denmark; 9Genitourinary Malignancies Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA; 10Merck KGaA, Darmstadt, Germany; 11EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA, Darmstadt, Germany; 12Division of Medical Oncology, Dana Farber Cancer Institute, Harvard Medical School, Boston, MA, USA
Poster No. 879TiP
BACKGROUND
Cervical cancer• Cervical cancer is one of the most common and lethal cancers
among females worldwide, with virtually all cases associated with persistent human papillomavirus (HPV) infection1-3
• Platinum-containing chemotherapy (CT), with or without bevacizumab, are the most common first-line (1L) treatments for recurrent/metastatic cervical cancer with median overall survival (OS) between 9.7 months (without bevacizumab) to 25.0 months (with bevacizumab)4-9
• There is currently no globally accepted standard-of-care treatment for patients with recurrent/metastatic cervical cancer that progressed during or after platinum-containing CT, and there remains an urgent, unmet need for these patients4
– Therapeutic options after 1L therapy are limited due to low response rates (3–10%) that are short-lived and associated with variable toxicities10,11
• In the United States, pembrolizumab has received accelerated approval for the treatment of PD-L1–positive (combined positive score ≥1) cervical cancer that progressed on/after CT12
– The overall response rate (ORR) of patients with PD-L1–positive tumors was 14.3% (11/77)
– Responses were limited in patients with adenocarcinoma histology and those who previously received bevacizumab; there were no responses in patients with PD-L1–negative tumors
Transforming growth factor β (TGF-β)• TGF-β has a multifunctional role in the development and
progression of cervical cancer, and is upregulated in cervical cancer cells and in the tumor microenvironment (TME) by HPV13-16
– TGF-β signaling can induce epithelial-to-mesenchymal transition (EMT), a hallmark of tumor progression and a key driver of metastasis, which plays an important role in cervical cancer14
– TGF-β can promote immune escape and may play a role in mediating resistance to anti–PD-(L)1 therapies13-14
– TGF-β signaling promotes angiogenesis in cervical cancer, which is commonly associated with increased invasiveness and worse survival13-16
• Therefore, inhibition of the TGF-β pathway in the TME while simultaneously blocking an additional immunosuppressive cellular mechanism, such as the PD-L1 pathway, may provide a novel treatment approach for cervical cancer
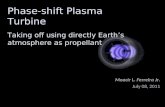
Bintrafusp alfa• Bintrafusp alfa is a first-in-class bifunctional fusion protein
composed of the extracellular domain of the TGF-βRII receptor to function as a TGF-β “trap” fused to a human IgG1 antibody blocking PD-L1 (Figure 1)17
– The bifunctional nature of bintrafusp alfa might allow for colocalized, simultaneous inhibition of two nonredundant immunosuppressive pathways (TGF-β and PD-L1) within the TME, which might enhance the anticancer effect observed with independent blockade of both pathways17,18
• In cohorts of a global, phase 1 trial (NCT02517398), bintrafusp alfa treatment demonstrated encouraging clinical activity and a manageable safety profile in 25 patients with heavily pretreated recurrent/metastatic cervical cancer who had disease progression during or after platinum-containing CT19
– The investigator-assessed ORR per RECIST 1.1 was 24.0%; an additional patient developed a sustained response after initial progressive disease (total clinical response, 28.0%)
– Responses were irrespective of tumor cell PD-L1 expression, histology, and prior treatments, including bevacizumab
– Responses were long-lasting (range, 4.2–30.4 months), and the median OS was 11.6 months
• INTR@PID CERVICAL 017 (NCT04246489) will evaluate the clinical benefit of bintrafusp alfa in patients with advanced unresectable/metastatic cervical cancer who progressed during or after platinum-containing CT
Figure 1. Proposed mechanism of action of bintrafusp alfa
Fibroblast
CAF
Fibrosis and impaireddrug access
EMT (leading to metastasis and resistanceto therapy [including checkpoint inhibition])
Tumor angiogenesis
Tumor cells
PD-L1
Bintrafuspalfa
PD-1
T cell
Suppression of immune response
NK cell
TAMDendritic
cell
CytotoxicT cell
Tumor cellsMesenchymal-like
tumor cell
TGF-β “trap” moiety sequesters TGF-β to block downstream signaling
Anti–PD-L1 mAb moietyblocks PD-L1 interactions with PD-1
TGF-β*
CAF, cancer-associated fibroblast; NK, natural killer; TAM, tumor-associated macrophage.
*Tumor cells are also a major source of TGF-β in the microenvironment.
TRIAL DESIGN• This is a global, single-arm, phase 2 trial to evaluate the
safety and efficacy of bintrafusp alfa monotherapy in patients with advanced unresectable/metastatic cervical cancer who had disease progression with or were intolerant of platinum-containing CT (NCT04246489) (Figure 2)
• Planned enrollment is 135 patients
• As a monotherapy treatment in cervical cancer, a 1200 mg every 2 weeks (Q2W) flat dose of bintrafusp alfa by intravenous (IV) infusion has been selected as the recommended phase 2 dose20
– Eligible patients will receive study treatment until confirmed disease progression, death, unacceptable toxicity, or study withdrawal; treatment past progression is allowed for patients with stable clinical status
• Key inclusion and exclusion criteria are described in Table 1
Figure 2. INTR@PID CERVICAL 017 (NCT04246489)
Bintrafusp alfa1200 mg IV Q2W
Key endpoints:
ORR, DOR, DRR, safety,PFS, OS, pharmacokinetics,clinical ef�cacy according to
PD-L1 expression
Advanced unresectable/metastatic
cervical cancerN=135
DOR, duration of response; DRR, durable response rate.
Table 1. Key eligibility criteriaSelected inclusion criteria Selected exclusion criteria
• Age ≥18 years
• Histologically documented advanced unresectable and/or metastatic cervical cancer
• Disease progression during or after prior platinum-containing CT*
• Availability of archival tumor tissue sample or newly obtained (preferred) biopsy of tumor lesion
• ECOG performance status of 0 or 1
• Adequate organ and coagulation function
• Life expectancy ≥12 weeks
• Prior cancer immunotherapy or treatment targeting T-cell costimulation, checkpoint pathways, or immune-suppressive pathways (such as TGF-β)
• Active central nervous system metastases causing clinical symptoms or requiring therapeutic intervention
ECOG, Eastern Cooperative Oncology Group.*Prior platinum-containing CT may be a systemic treatment for metastatic disease or in the adjuvant or neoadjuvant setting. Participants who were intolerant to or ineligible for platinum-containing CT are eligible for this trial.
• Primary and secondary endpoints are described in Table 2
• Key exploratory objectives include:
– Evaluation of the clinical efficacy of bintrafusp alfa based on immune-related ORR and immune-related PFS
– Evaluation of biological response or predictive markers in blood, tumor, and TME, and their relationship to drug exposure, clinical response, or other biological markers of response
– Clinical efficacy according to demographic and clinical variables corresponding to cervical cancer prognosis
– Patient-reported quality of life and symptoms
Table 2. Trial endpointsPrimary endpoints
• ORR according to RECIST 1.1 as assessed by IRC
Secondary endpoints
• DOR, DRR,* and PFS according to RECIST 1.1 as assessed by IRC
• Safety (TEAEs, TRAEs, SAEs) according to NCI-CTCAE v5.0
• ORR, DOR, DRR,* and PFS according to RECIST 1.1 as assessed by investigator
• OS
• Pharmacokinetics of bintrafusp alfa
• Clinical efficacy of bintrafusp alfa according to PD-L1 expression
IRC, independent review committee; SAE, serious adverse event; TEAE, treatment-emergent adverse event; TRAE, treatment-related adverse event.*Durable response of ≥6 months.
• Enrollment in the INTR@PID CERVICAL 017 trial began in March 2020 and is ongoing
• This trial is being conducted at 85 sites in North and South America, Europe, and the Asia-Pacific region (Figure 3)
• Refer to ClinicalTrials.gov (NCT04246489) for additional information
Figure 3. Participating countries
ArgentinaAustraliaBelgium
BrazilChinaFrance
HungaryJapan
Republic of Korea
RussiaSpain
United States
REFERENCES1. Saraiya M, et al. J Natl Cancer Inst. 2015;107:jv086.2. Walboomers JM, et al. J Pathol. 1999;189:12-9.3. Bray F, et al. CA Cancer J Clin. 2018;68:394-424.4. Marth C, et al. Ann Oncol. 2017;28(Suppl 4):iv72-iv83.5. Moore DH, et al. J Clin Oncol. 2004;22:3113-9.6. Monk BJ C, et al. J Clin Oncol. 2009;27:4649-55.7. Kitagawa R, et al. J Clin Oncol. 2015;33:2129-35.8. Tewari KS, et al. Lancet. 2017;390:1654-63. 9. Redondo A, et al. Gynecol Oncol. 2020 Aug 4. [Epub ahead
of print].10. McLachlan J, et al. Clin Oncol (R Coll Radiol). 2017;29:153-60.
11. Monk BJ, et al. J Clin Oncol. 2009;27:1069-74.12. Chung HC, et al. J Clin Oncol. 2019;37:1470-8.13. Torres-Poveda K, et al. World J Clin Oncol. 2014;5:753-63. 14. Lee MY and Shen MR. Am J Transl Res. 2012;4:1-13. 15. Holmgaard RB, et al. J Immunother Cancer. 2018;6:47.16. Zijlmans JH, et al. Br J Cancer. 2009;100: 1617-26.17. Lan Y, et al. Sci Transl Med. 2018;10:eaan5488.18. Knudson KM. Oncoimmunol. 2018;7:e1426519.19. Allan S, et al. Int J Gynecol Cancer. 2019;29(Suppl 4):Poster P37.20. Vugmeyster Y, et al. Clin Pharmacol Ther. 2020 Jan 18. [Epub
ahead of print].
ACKNOWLEDGEMENTSThis trial is sponsored by Merck KGaA, Darmstadt, Germany, and is part of an alliance between Merck KGaA and GlaxoSmithKline. The authors thank the patients and their families, investigators, co-investigators, and study teams at each of the participating centers and at Merck KGaA and EMD Serono Research & Development Institute, Inc., Billerica, MA, USA; a business of Merck KGaA.
Medical writing support was provided by Yao Bian, PhD, MedicalExpressions Inc, Chicago, IL, USA, which was also funded by Merck KGaA and GlaxoSmithKline, in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
Correspondence: Michael J. Birrer, [email protected]
DISCLOSURESMJB has received honoraria (self) from Clovis, AstraZeneca, and Roche/Genentech. LRM has nothing to disclose. KF has received honoraria (self) from Chugai-Roche, AstraZeneca, Nipponkayaku, Kyowa-Kirin, and Zeria; had advisory/consultancy roles with Eisai, MSD, Genmab, and Nanocarrier; received research grants/funding from AstraZeneca, Chugai-Roche, Eisai, Genmab, Regeneron, and Zeria; received travel/accommodation/expenses from Merck KGaA, Darmstadt, Germany. IR-C has received honoraria (self) from AbbVie, Agenus, Advaxis, Bristol Myers Squibb, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche, GlaxoSmithKline, Deciphera, Mersena, Merck Serono, Novartis, Amgen, Tesaro, Clovis, and Merck KGaA, Darmstadt, Germany; received honoraria (institution) from GlaxoSmithKline, Roche, Bristol Myers Squibb, and Merck KGaA; had advisory/consultancy roles with AbbVie, Agenus, Advaxis, Bristol Myers Squibb, PharmaMar, Genmab, Pfizer, AstraZeneca, Roche/Genentech, GlaxoSmithKline, Deciphera, Mersena, Merck Serono, Novartis, Amgen, Tesaro, Clovis, and Merck KGaA; received research grant/funding (self) from Merck KGaA, Roche, and Bristol Myers Squibb; received research grant/funding (institution) from Merck KGaA, Roche, Bristol Myers Squibb, Novartis, AstraZeneca, and Merck Serono; received travel/accommodation/expenses from Roche, AstraZeneca, and GlaxoSmithKline; participated in non-remunerated activities for GINECO, ENGOT, GCIG, European Community, ESMO, ASCO, ESGO, IGSC, Inca, and Swiss, Italian, Belgium and German health authorities. JA has received honoraria (self) from AstraZeneca, GlaxoSmithKline, Roche, PharmaMar, Novartis, and Merck KGaA, Darmstadt, Germany; had advisory/consultancy roles with Merck KGaA, AstraZeneca, GlaxoSmithKline, Roche, PharmaMar, and Novartis; received grant/funding (institution) from Merck KGaA and Janssen; received travel/accommodation/expenses from Janssen, Roche, and Novartis. AO has had speaking/expert testimony roles for AstraZeneca and received research grants/funding from Kissei Pharmaceuticals, Kaken Pharmaceutical, Meiji Holdings, Nippon Shinyaku, Chugai, Taiho, Daiichi Sankyo, Tsumura & Co., and ASKA Pharmaceutical. MRM has personal financial interests in AstraZeneca, Biocad, Clovis, Geneos, Genmab, Karyopharm Therapeutics, Merck Serono, Oncology Venture, Pfizer, Roche, Seattle Genetics, Sera Prognostics, Sotio, Tesaro/GlaxoSmithKline, ZaiLab, and Merck KGaA, Darmstadt, Germany; had leadership roles with Karyopharm Therapeutics and Sera Prognostics; received research grant/funding (institution) from AstraZeneca, Boehringer Ingelheim, Clovis Oncology, Pfizer, and Tesaro/GlaxoSmithKline; participated in other activities with DGCG, GCIG, ESGO, and ENGOT. JLG has received research grant/funding (institution) from Merck KGaA, Darmstadt, Germany. GJ is an employee of Merck KGaA, Darmstadt, Germany. SR and LSO are employees of and may hold shares in EMD Serono Research & Development Institute, Inc; a business of Merck KGaA, Darmstadt, Germany. SMC has received honoraria (self and institution) from Tesaro and Eisai; had advisory/consultancy roles with Tesaro and Eisai.
Copies of this e-poster obtained through QR (Quick Response) and/or text key codes are for personal use only and may not be reproduced without written permission of the authors.
GET POSTER PDF