Pharmacology of Dexmed
17
Dexmed : α 2 – Agonists Adrenergic Receptors Initially, α-adrenergic receptors were distinguished from β-adrenergic receptors by their greater response to epinephrine and norepinephrine than to isoproterenol. The development of α and β antagonists further supported the existence of separate α receptors. Traditionally, adrenergic receptors have been classified as α or β and more recently as α 1 , α 2 , β 1 , or β 2 based on responses to specific drugs 3 . Physiology of the Αlpha 2 Receptor α 2 adrenergic receptors are primarily located on the presynaptic membrane and modulate release of norepinephrine, whereas postsynaptic α 1 adrenergic receptors mediate smooth muscle vasoconstriction . α 2 receptors are found in the peripheral nervous system, in the CNS, and in a variety of organs, including platelets, liver, pancreas, kidney, and eyes,
-
Upload
anne-shirley -
Category
Documents
-
view
87 -
download
2
Transcript of Pharmacology of Dexmed

Dexmed : α2 – Agonists
Adrenergic Receptors
Initially, α-adrenergic receptors were distinguished from β-adrenergic receptors by their
greater response to epinephrine and norepinephrine than to isoproterenol. The
development of α and β antagonists further supported the existence of separate α
receptors. Traditionally, adrenergic receptors have been classified as α or β and more
recently as α1, α2, β1, or β2 based on responses to specific drugs3.
Physiology of the Αlpha2 Receptor
α2 adrenergic receptors are primarily located on the presynaptic membrane and modulate release
of norepinephrine, whereas postsynaptic α1 adrenergic receptors mediate smooth muscle
vasoconstriction . α2 receptors are found in the peripheral nervous system, in the CNS, and in a
variety of organs, including platelets, liver, pancreas, kidney, and eyes, where specific physiologic
functions have been identified. Of late, the predominant α 2 receptor of the human spinal cord
was also identified and was named as the α2a subtype3.
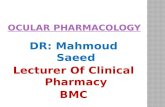
Responses mediated by α2-adrenergic receptors
Activation of the receptors in the brain and spinal cord inhibits neuronal firing, causing
hypotension, bradycardia, sedation, and analgesia. The responses to activation of the
receptors in other areas include decreased salivation, decreased secretion, and decreased
bowel motility in the gastrointestinal tract; contraction of vascular and other smooth

muscle; inhibition of renin release, increased glomerular filtration, and increased secretion
of sodium and water in the kidney; decreased intraocular pressure; and decreased insulin
release from the pancreas 2,21.
.
Responses mediated by α2-adrenergic receptors2

Pharmacology of Dexmedetomidine
Dexmedetomidine is the d-enantiomer of medetomidine, a substance that has been used
for sedation and analgesia in veterinary medicine for many years. It belongs to the
imidazole subclass of α2 receptor agonists, similar to clonidine. It is freely soluble in
water.
Chemical structure
Mechanism of action
Presynaptic α2 receptors regulate the release of norepinephrine and adenosine triphosphate
through a negative feedback mechanism. In general, presynaptic activation of the α2
adrenoceptor inhibits the release of norepinephrine, terminating the propagation of pain
signals while postsynaptic activation of α2 adrenoceptors in the central nervous system
(CNS) inhibits sympathetic activity and thus can decrease blood pressure and heart rate.

Combined, these effects can produce analgesia, sedation, and anxiolysis thus avoiding
some of the side effects of multiagent therapies21.
Mechanism of
action21.
The mechanism of the analgesic effects
A number of sites, both supraspinal and spinal, modulate the transmission of nociceptive
signals in the CNS. In addition to dexmedetomidine's action in the locus coeruleus of
the brain stem, it has been shown to stimulate α2 receptors directly in the spinal cord,
thus inhibiting the firing of nociceptive neurons. Even peripheral α2 adrenoceptors may
mediate antinociception16.
The mechanism of the hypnotic and sedative effects

One of the highest densities of α2 receptors has been detected in the locus coeruleus, the
predominant noradrenergic nucleus in the brain and an important modulator of vigilance.
The hypnotic and sedative effects of dexmedetomidine have been attributed to the
endogenous sleep-promoting pathways16.

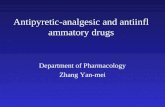
Mechanisms of the analgesic effects of alpha 2 agonists
and other commonly used analgesics.
Pharmacological actions
Cardiovascular System
A biphasic cardiovascular response has been described after the application of
dexmedetomidine. The administration of a bolus of 1 μg/kg dexmedetomidine initially
results in a transient increase of the blood pressure and a reflex decrease in heart rate,
especially in younger, healthy patients. The initial increase in blood pressure is probably
due to the vasoconstrictive effects of dexmedetomidine when stimulating peripheral α2
receptors. The initial response lasts for 5 to 10 minutes and is followed by a decrease
in blood pressure of approximately 10% to 20% below baseline and a stabilization of the
heart rate, also below baseline values; both of these effects are caused by the inhibition
of the central sympathetic outflow overriding the direct stimulating effects21.
Central Nervous System
1. Sedation
The quality of sedation produced by dexmedetomidine is different from that produced by
other sedatives acting through the GABA systems. They act through the endogenous sleep
promoting pathways. Patients have been described as being very easy to wake up and

having the ability to follow commands and cooperate while being tracheally intubated 9.
Despite sound levels of sedation, there is limited respiratory depression, providing wide
safety margins22.
2. Analgesia
The primary site of analgesic action is thought to be the spinal cord. It is also shown to
have an analgesic effect when injected via the intrathecal or epidural route.
Dexmedetomidine also inhibits the release of substance P from the dorsal horn of the
spinal cord, leading to primary analgesic effects23.
3. Central Nervous System Protection and Other Central Nervous System Effects
Dexmedetomidine in animal models of incomplete cerebral ischemia and reperfusion
reduces cerebral necrosis and improves neurologic outcome. It is shown to reduce the
intracerebral catecholamine outflow during injury resulting in less neural tissue damage
with better neurologic outcome24.
Respiratory System
Although dexmedetomidine produces sedative, analgesic and anxiolytic affects, unlike
other sedatives, it provides respiratory stability and does not cause ventilatory depression.
The changes in ventilation appear similar to those observed during natural sleep. It
exhibits a hypercarbic arousal phenomenon similar to that in normal sleep. Intravenous or
inhaled dexmedetomidine has been implicated in blocking histamine induced
bronchoconstriction in dogs16,25.
Renal System

It is shown to result in diuresis and natriuresis, possibly through an ability to reduce
efferent sympathetic outflow of the renal nerve. It decreases the secretion of vasopressin
and increases the release of atrial natriuretic peptide7,16.
Endocrine System
Action of dexmedetomidine on endocrine system is mainly related to its action on
sympathetic outflow and the decrease of catecholamines. This attenuates the responses to
stress by inhibiting the secretion of adrenocorticotropic hormone (ACTH) and cortisol. In
addition, stimulation of α2 adrenoceptor agonists located on cells of the Islet of
langerhans can temporally cause direct inhibition of insulin release with concomitant
detectable clinical hyperglycemia16.
Preparation and dosage
Available
in 1 or 2 ml vials as dexmedetomidine hydrochloride ; 1ml equivalent to 100 mcg of
dexmedetomidine.

Dexmedetomidine must be diluted in 0.9% normal saline prior to injection. To prepare
the solution, dilute 2 ml in 48 ml or 1 ml in 24 ml of normal saline solution to a total
of 50 ml to make a concentration of 4 µg/ ml.
Dexmedetomidine should be administered through a controlled infusion device.
Dosing should be individualised and titrated to the desired clinical effect.
It is not indicated for infusions lasting more than 24 hrs.
Dexmedetomidine is generally initiated with a loading infusion of 1 μg/kg over 10 min
followed by a maintainence infusion of 0.2 - 0.7 μg/hour. The rate should be adjusted to
maintain the desired level of response.
Pharmacokinetics
Dexmedetomidine is rapidly distributed and extensively metabolized in the liver and
excreted in urine and feces. It undergoes conjugation (41%), n-methylation (21%), or
hydroxylation followed by conjugation. Dexmedetomidine is 94% protein bound, and its
concentration ratio between whole blood and plasma is 0.66. Dexmedetomidine has
profound effects on cardiovascular variables and may alter its own pharmacokinetics.
With large doses, there is marked vasoconstriction, which probably reduces the drug's
volume of distribution. In essence, dexmedetomidine displays nonlinear
pharmacokinetics16,26.
The elimination half-life of dexmedetomidine is 2 to 3 hours, with a context-sensitive
half-time ranging from 4 minutes after a 10-minute infusion to 250 minutes after an 8-

hour infusion. Postoperative patients sedated with dexmedetomidine display similar
pharmacokinetics to the pharmacokinetics seen in healthy volunteers27 .
The steady-state volume of distribution is 118 L, and the distribution phase is rapid,
with a half-life of distribution of approximately 6 minutes28 .
Therapeutic uses
1. Intensive Care Unit
i. For sedation in mechanically ventilated patients in loading doses of 0.5 to 1
µg/kg and infusion rates of 0.2 to 0.7 µg/kg/hr.
ii. For weaning patients from the ventilator: the unique characteristics of
dexmedetomidine in providing adequate sedation with minimal respiratory
depression allows for easy weaning29.
iii. To facilitate daily “wake up” tests in mechanically ventilated patients30 .
iv. For treatment of alcohol and drug withdrawal: Dexmedetomidine has been
successfully used in the treatment of withdrawal of narcotics, benzodiazepines,
alcohol, and recreational drugs. It is shown to control withdrawal behaviour and
allows for successful detoxification16 .
2. Anesthesia
i. As a premedicant : to attenuate sympathetic activation during induction of
anesthesia and to provide a more stable hemodynamic profile16,19,24 . Apart from
the intravenous route, it can be given as intramuscular injection in doses of 2.5
µg/kg.26 Administration of intranasal dexmedetomidine at 0.5 or 1 mcg/kg has also
been proved to produce adequate sedation31 .

ii. Sedation for monitored anesthesia care: It has been successfully used in patients
receiving local anesthesia or regional block. Dexmedetomidine has also been
reported to provide successful sedation in paediatric patients undergoing MRI
scans32,33 .
iii. Maintenance of anesthesia: It promotes hemodynamic stability and decreases the
doses of anesthetics and analgesics23 .
iv. Awake fiberoptic intubation: The use of dexmedetomidine when securing the
airway with a fiberoptic intubation is shown to be well tolerated with no
hemodynamic compromise or respiratory depression16.
v. As anesthetic adjunct or sedative agent in patients susceptible to narcotic induced
respiratory depression or sleep apnea. It has been successfully used in patients
undergoing transesophageal echocardiography examination16 .
Drug interactions
A reduction in dosage of all an.esthetics, sedatives, hypnotics and opioids is seen. Care
should be taken when used in concurrence with drugs causing bradycardia like beta
blockers, vecuronium, fentanyl and neostigmine.
Side effects
i. Hypotension, hypertension, nausea, bradycardia, atrial fibrillation, and hypoxia
ii. Overdose may cause first-degree or second-degree atrioventricular block.

Most of the adverse events associated with dexmedetomidine use occur during or briefly
after loading of the drug. By omitting or reducing the loading dose, adverse effects can
be reduced.
Atipamezole, a selective α2 antagonist, at 50 µg/kg was effective in reversing the
sedation of dexmedetomidine (2 µg/kg intramuscularly), when used to provide sedation
for brief operative procedures. This reversal of effects results in more rapid recovery
than occurred after equisedative doses of midazolam34.