Pharmacokinetic-Pharmacodynamic Modeling of Apratastat: A Population-Based Approach
10
472 • J Clin Pharmacol 2011;51:472-481 T umor necrosis factor-alpha (TNF-α), a cytokine produced primarily by activated monocytes and macrophages, is an important mediator of immuno- inflammatory responses and inducer of other proin- flammatory cytokines. 1 TNF-α is produced as a 26 kDa membrane-bound pro-TNF-α that undergoes a specific proteolytic cleavage to generate the 17 kDa soluble form of TNF-α. 2 The enzyme that is respon- sible for this process is the factor-α converting enzyme (TACE), a zinc endopeptidase and a member of the a disintegrin and metalloproteinase (ADAM) family of enzymes (also designated as ADAM-17). TACE is closely related to the matrix metalloprotei- nases (MMPs) 3,4 that have also been implicated to play a critical role in rheumatoid arthritis (RA). 5 MMPs are a large family of Zn 2+ endopeptidases that are expressed in immuno-inflammatory conditions such as RA and are collectively capable of degrading most connective tissue macromolecules under both physiological and pathological conditions. 6,7 MMPs can degrade all components of the extracellular matrix. The collagenases, MMP-1 and MMP-13, have predominant roles in RA because they are rate limit- ing in the process of collagen degradation. In addi- tion to collagen, MMP-13 degrades the proteoglycan molecule, aggrecan, giving it a dual role in matrix destruction. 8 Expression of other MMPs, such as MMP-2, MMP-3, and MMP-9, is also elevated in arthritis and these enzymes degrade noncollagen matrix components of the joints. A significant effort has been expended in attempts to design effective inhibitors of MMP activity and/or synthesis with the goal of curbing connective tissues destruction within the joints. Several MMP proteins or activities have been demonstrated to be elevated in the synovium of RA patients. 9-11 Apratastat is an orally active, potent, and reversible dual inhibitor of tumor necrosis factor-α converting enzyme (TACE) and matrix metalloproteinases (MMPs). This study characterizes the pharmacodynamic (PD) effect of aprata- stat following oral administration on tumor necrosis factor- alpha (TNF-α) release. Data were obtained from 3 clinical studies carried out in healthy subjects. Apratastat was administered orally in these studies as single doses or multiple doses (twice daily). The inhibition of TNF-α release by apratastat was investigated in studies of in vitro, ex vivo, and in vivo. Inhibitory E max models were used to characterize the inhibition of TNF-α release in both in vitro and ex vivo studies. Apratastat inhibited TNF-α release with a population mean IC 50 of 144 ng/mL in vitro and of 81.7 ng/mL ex vivo, respectively. The relationship between TNF-α and apratastat plasma concentration in the endotoxin-challenged study in healthy subjects was well characterized by a mechanism-based PD population model with IC 50 of 126 ng/mL. Apratastat can potently inhibit the release of TNF-α in vitro, ex vivo, and in vivo. Even though the dosage provided adequate exposure to inhibit TNF-α release, apratastat was not efficacious in rheumatoid arthri- tis (RA). This inconsistency between TNF-α inhibition and the clinical response requires further investigation. Keywords: rheumatoid arthritis; TNF-α; apratastat; phar- macokinetics; pharmacodynamics; TACE/ MMP; population pharmacokinetic-pharma- codynamic modeling; endotoxin (LPS) Journal of Clinical Pharmacology, 2011;51:472-481 © 2011 The Author(s) From Pfizer (formerly Wyeth Research), Collegeville, Pennsylvania (Dr Shu, Dr Zhou, Dr Afsharvand, Dr Raible); Cephalon Inc, Frazer, Pennsylvania (Dr Shu); Centocor Research and Development, Malvern, Pennsylvania (Dr Zhou); QPS, LLC, Newark, Delaware (Dr Duan, Dr Zhang); MDS Pharma Services, Neptune, New Jersey (Dr Noveck); and Division of Clinical Pharmacology, Duke University School of Medicine, Durham, North Carolina (Dr Noveck). Submitted for publication January 27, 2010; revised version accepted March 12, 2010. Address for cor- respondence: Donald Raible, Pfizer, 500 Arcola Road, Collegeville, PA 19426; e-mail: [email protected]. DOI:10.1177/0091270010372389 Pharmacokinetic-Pharmacodynamic Modeling of Apratastat: A Population-Based Approach Cathye Shu, PhD, Honghui Zhou, PhD, FCP, Mehri Afsharvand, PharmD, Larry Duan, PhD, Hui Zhang, MB, Robert Noveck, MD, and Donald Raible, MD PHARMACOKINETICS AND PHARMACODYNAMICS
Transcript of Pharmacokinetic-Pharmacodynamic Modeling of Apratastat: A Population-Based Approach

472 • J Clin Pharmacol 2011;51:472-481
Tumor necrosis factor-alpha (TNF-α), a cytokine produced primarily by activated monocytes and
macrophages, is an important mediator of immuno-inflammatory responses and inducer of other proin-flammatory cytokines.1 TNF-α is produced as a 26 kDa membrane-bound pro-TNF-α that undergoes a specific proteolytic cleavage to generate the 17 kDa soluble form of TNF-α.2 The enzyme that is respon-sible for this process is the factor-α converting enzyme (TACE), a zinc endopeptidase and a member of the a disintegrin and metalloproteinase (ADAM) family of enzymes (also designated as ADAM-17).
TACE is closely related to the matrix metalloprotei-nases (MMPs)3,4 that have also been implicated to play a critical role in rheumatoid arthritis (RA).5 MMPs are a large family of Zn2+ endopeptidases that are expressed in immuno-inflammatory conditions such as RA and are collectively capable of degrading most connective tissue macromolecules under both physiological and pathological conditions.6,7 MMPs can degrade all components of the extracellular matrix. The collagenases, MMP-1 and MMP-13, have predominant roles in RA because they are rate limit-ing in the process of collagen degradation. In addi-tion to collagen, MMP-13 degrades the proteoglycan molecule, aggrecan, giving it a dual role in matrix destruction.8 Expression of other MMPs, such as MMP-2, MMP-3, and MMP-9, is also elevated in arthritis and these enzymes degrade noncollagen matrix components of the joints. A significant effort has been expended in attempts to design effective inhibitors of MMP activity and/or synthesis with the goal of curbing connective tissues destruction within the joints. Several MMP proteins or activities have been demonstrated to be elevated in the synovium of RA patients.9-11
Apratastat is an orally active, potent, and reversible dual inhibitor of tumor necrosis factor-α converting enzyme (TACE) and matrix metalloproteinases (MMPs). This study characterizes the pharmacodynamic (PD) effect of aprata-stat following oral administration on tumor necrosis factor-alpha (TNF-α) release. Data were obtained from 3 clinical studies carried out in healthy subjects. Apratastat was administered orally in these studies as single doses or multiple doses (twice daily). The inhibition of TNF-α release by apratastat was investigated in studies of in vitro, ex vivo, and in vivo. Inhibitory Emax models were used to characterize the inhibition of TNF-α release in both in vitro and ex vivo studies. Apratastat inhibited TNF-α release with a population mean IC50 of 144 ng/mL in vitro and of 81.7 ng/mL ex vivo, respectively. The relationship between TNF-α and apratastat plasma concentration in the
endotoxin-challenged study in healthy subjects was well characterized by a mechanism-based PD population model with IC50 of 126 ng/mL. Apratastat can potently inhibit the release of TNF-α in vitro, ex vivo, and in vivo. Even though the dosage provided adequate exposure to inhibit TNF-α release, apratastat was not efficacious in rheumatoid arthri-tis (RA). This inconsistency between TNF-α inhibition and the clinical response requires further investigation.
Keywords: rheumatoid arthritis; TNF-α; apratastat; phar-macokinetics; pharmacodynamics; TACE/MMP; population pharmacokinetic-pharma-codynamic modeling; endotoxin (LPS)
Journal of Clinical Pharmacology, 2011;51:472-481 © 2011 The Author(s)
From Pfizer (formerly Wyeth Research), Collegeville, Pennsylvania (Dr Shu, Dr Zhou, Dr Afsharvand, Dr Raible); Cephalon Inc, Frazer, Pennsylvania (Dr Shu); Centocor Research and Development, Malvern, Pennsylvania (Dr Zhou); QPS, LLC, Newark, Delaware (Dr Duan, Dr Zhang); MDS Pharma Services, Neptune, New Jersey (Dr Noveck); and Division of Clinical Pharmacology, Duke University School of Medicine, Durham, North Carolina (Dr Noveck). Submitted for publication January 27, 2010; revised version accepted March 12, 2010. Address for cor-respondence: Donald Raible, Pfizer, 500 Arcola Road, Collegeville, PA 19426; e-mail: [email protected]:10.1177/0091270010372389
Pharmacokinetic-Pharmacodynamic Modeling of Apratastat: A Population-Based Approach
Cathye Shu, PhD, Honghui Zhou, PhD, FCP, Mehri Afsharvand, PharmD, Larry Duan, PhD, Hui Zhang, MB, Robert Noveck, MD, and Donald Raible, MD
Pharmacokinetics and Pharmacodynamics

POPULATION PK-PD MODELING OF APRATASTAT
PhARMACOkINEtICS AND PhARMACODyNAMICS 473
RA is a chronic, inflammatory autoimmune dis-ease that results in progressive joint destruction and substantial morbidity. Despite a tremendous effort made to understand its etiology over more than 2 decades, the precise cause of RA remains unre-solved. In recent years, the proinflammatory cytokine TNF-α has been demonstrated to play a pivotal role in RA.12 Elevated concentrations of soluble TNF-α are found in the synovial fluid of RA patients.13,14 TNF-α also contributes to cartilage breakdown and bone erosion by stimulating the production of other proinflammatory cytokines, recruitment of inflam-matory cells into the synovium of joints, and induc-tion of degradative enzymes such as various MMPs.15 The recent clinical success of anti-TNF-α agents has further validated the pivotal role of TNF-α in various inflammatory autoimmune diseases.16 Three protein-based anti-TNF-α biologics, etanercept (Enbrel, Immunex-Wyeth, Thousand Oaks, CA), inf-liximab (Remicade, Centocor, Inc, Malvern, PA), and adalimumab (Humira, Abbott Laboratories, Chicago, IL) have all been approved for the treatment of rheu-matoid arthritis.17-19 However, all of these biologic agents need to be administered either intravenously (infliximab) or subcutaneously (etanercept, adalimu-mab). Thus, despite the success of these biological agents, small molecule inhibitors of TNF-α, which can be administered orally, present a highly desira-ble alternative for treating RA.
Apratastat is an orally bioavailable small-mole-cule dual TACE/MMP inhibitor. Apratastat blocks the shedding of membrane-bound TNF-α and is hypothesized to reduce the circulating systemic con-centration of the biologically active form of TNF-α. The human endotoxin (descending single-dose endotoxin [LPS]) challenge model has been used to characterize the anti-inflammatory profile of drugs such as etanercept,20,21 BIRB 796 BS p38 MAP kinase inhibitor,22 and GI5402 TACE/MMP inhibitor.23 These agents inhibit the in vivo production of TNF-α and other markers of inflammation (eg, IL-1ra, IL-6, IL-8, and E-selectin) following an LPS challenge, thus validating their mechanism of action. In this report, we described the in vitro, ex vivo inhibitory profiles of TNF-α by apratastat. We further explored the feasibility of using changes in LPS-induced TNF-α release as an indicator for in vivo TACE inhi-bition by apratastat. A population pharmacokinetic- pharmacodynamic (PK-PD) model was developed to link the inhibitory profiles of LPS-induced TNF-α release with the plasma concentration-time profiles of apratastat.
MeThods
study design
Data were compiled from 3 phase I studies: an ascending single-dose (SAD), an ascending multiple dose (MAD), and a LPS-challenge study, all of which were randomized, double-blind, single-center, and placebo-controlled studies. The primary objectives of the SAD and MAD studies were to assess the safety and tolerability of ascending oral doses of apratastat given as single or multiple doses, respectively. The secondary objectives of both the SAD and MAD stud-ies were to assess the PK and PD profiles of apratastat. The primary objective of the LPS-challenge study was to compare the effect of apratastat with that of pla-cebo on the in vivo production of TNF-α following an LPS challenge in healthy male subjects.
In the SAD study, 5 oral dose levels of apratastat (10, 40, 100, 200, and 350 mg) were administered to healthy subjects. In the MAD study, subjects received 10 to 300 mg of apratastat (10, 20, 40, 80, 150, and 300 mg) as oral administration every 12 hours for 14 consecutive days. In both SAD and MAD studies, there were 8 subjects in each dose cohort. Of the 8 subjects in each cohort, 6 received apratastat and 2 received a placebo.
Subjects in the LPS-challenge study received sequential, descending single doses of apratastat or placebo. After an overnight fast of at least 10 hours, each subject would receive a single 350-mg oral dose of apratastat or placebo 0.5 hours before receiving a bolus injection of 4 ng/kg of LPS. Lower dose groups (200, 100, 50, 20, and 10 mg) would be tested sequentially only if the mean production of LPS-stimulated TNF-α, as determined by the area under the concentration-time curve (AUC), decreased by more than 20% in the preceding higher dose group. Dose de-escalation would be stopped if the preced-ing dose failed to decrease TNF-α release by more than 20%. In addition, 1 dose cohort (100 mg) would be administered apratastat 3 hours prior to the administration of the LPS injection.
Subjects
Healthy men aged 18 to 45 years were recruited in all 3 studies. No clinically abnormal findings on medical history, physical examination, 12-lead elec-trocardiogram (ECG), or clinical laboratory evalua-tion were allowed. Subjects who had not taken any over-the-counter, investigational, or prescription drug 14 days before the study, or did not have any

474 • J Clin Pharmacol 2011;51:472-481
SHU ET AL
condition known to interfere with the absorption, distribution, metabolism, or excretion of drugs, were included in the study. Subjects who tested positive for human immunodeficiency virus (HIV) antibod-ies, hepatitis B surface antigen, and/or hepatitis C antibodies, or who had a history or presence of any allergic condition or any major organ or systemic disease, were excluded from the study.
All subjects gave written informed consent. The study was performed in accordance with the guide-lines for good clinical practice and the principles of the Helsinki Agreement and its amendments, and in accordance with local laws and guidelines. At each study center (Thomas Jefferson University Hospital, Philadelphia, PA, University of Miami School of Medicine, Miami, FL, and Clinical Research Center MDS Pharma Services, New Orleans, LA) an institu-tional review board reviewed and approved the rel-evant study protocols and consent forms.
Bioanalytical Methods
In all 3 studies, apratastat was assayed in plasma by a LC/MS/MS method with calibrators in the range of 1 to 1500 ng/mL. In brief, the method consisted of liquid-liquid extraction and gradient reverse phase chromatography on a Prodigy ODS column with MS/MS detection. The extraction efficiency was about 60% to 70%, and the lower limit of quantita-tion was 1 ng/mL.
LPS-Induced TNF-α Release from Human Whole Blood
In vitro. Predose blood from healthy subjects in the SAD, MAD, and LPS-challenge studies was col-lected in heparinized tubes (10 U/mL) by venipunc-ture. For the inhibitory effect of apratastat, blood was pre-incubated with apratastat 10 to 3000 ng/mL at room temperature for 1 hour in 24-well flat-bot-tom cell culture plates at 1 mL/well prior to the LPS incubation. Blood was then incubated in the pres-ence of 200 pg/mL LPS for 2 hours in a humidified 37°C incubator without CO2. Blood was centrifuged at 1000 g for 5 minutes at the end of incubation. The plasma was stored at −70°C for TNF-α analysis. The plasma TNF-α concentrations were analyzed using ELISA methods, which were validated at Quest Pharmaceutical Services, LLC.
Ex vivo. In SAD and MAD studies, blood samples (via venipuncture into heparinized vacutainers, 10 U/mL) were collected at the following time points: predose, 1, 2, 4, 8, 12, and 24 hours postdose administration. The heparinized whole blood was
incubated with LPS (200 pg/mL) or PBS control for 2 hours at 37°C. After incubation, the whole blood was mixed and centrifuged (1000 g for 5 min), and the plasma was used to determine levels of TNF-α by an ELISA method validated at Quest Pharmaceutical Services, LLC.
In vivo. In the LPS-challenge study, blood samples were collected from each subject at baseline, within 2 or 4 hours before test article administration, and 0 (2 minutes before LPS injection), 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 12, 16, and 24 hours after LPS administra-tion. Plasma concentrations of TNF-α were analyzed using an ELISA method validated at Quest Pharma-ceutical Services, LLC.
PK-Pd Modeling
All of the analyses were performed by using the population-based approaches with NONMEM ver-sion IV, level 1.2 (NONMEM Project Group, University of California, San Francisco, CA).24 Model selection was based on inspection of goodness-of-fit plots performed with the estimates of the parameters and their confidence intervals (CIs). The minimum value of the objective function (MOF) was used to assist the model selection.
In vitro and ex vivo. For in vitro and ex vivo data, when TNF-α concentrations (expressed as percent inhibition) were plotted against apratastat concen-tration in a time-ordered manner, no apparent hys-teresis loop was observed in any of the subjects. This suggested an immediate equilibration of apratastat with the biophase and, thus, a direct PK-PD correla-tion model was utilized.The relationships between the apratastat concentration and the PD effect (TNF-α expressed as percent baseline) were described by the following sigmoid Emax (Equation 1) and Emax models (Equation 2) for in vitro and ex vivo data, respectively:
where Eij is the jth PD measurement (TNF-α expressed as percent baseline) for the ith individual, E0i, Emaxi, and IC50i represent baseline, percentage of maximal decrease in TNF-α concentration, concentration of apratastat corresponding to 50% of the maximal
E EE C
IC Cij ii pij
i pijij= − −
×+
+100 050
max ‘γ
γ γ ε
E EE C
IC Cij ii pij
i pijij= − −
×+
+100 050
max ε
(1)
(2)

POPULATION PK-PD MODELING OF APRATASTAT
PhARMACOkINEtICS AND PhARMACODyNAMICS 475
(1)
(2)
effect, respectively, for the ith individual, εij is the residual (intraindividual) error, a random variable assumed to be normally distributed with a zero mean and variance σ. The γ is the shaping factor. For each parameter, the expression for the ith subject is:
where Ppop represents the typical parameter value in the population, and ηi is the random variable assumed to be normally distributed with a zero mean and variance ω.
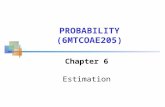
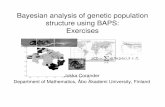
In Vivo. A mechanism-based PK-PD model is devel-oped to describe the relationship between the time course of LPS-induced TNF-α synthesis and elimina-tion and the inhibition of TACE enzyme by apratastat. The diagram for this PK-PD model is illustrated in Figure 1, and mathematically it can be described by 2 simultaneous differential equations as follows25:
It was assumed that LPS induced the TNF-α syn-thesis during a limited time interval (tsyn). The synthe-sis rate was described by a zero-order rate constant (k0) whereas the release rate constant (kin) of the syn-thesized amount of TNF-α as well as the disappear-ance rate constant from plasma (kout) were assumed to
follow first-order kinetics. The distinct time lag between LPS administration and TNF-α appearance in plasma was modeled by the parameter tlag; Z1 and Z2 were used as “dummy variables” so that Z1 was set to 1 if 0 ≤ t ≤ tsynt, else Z1 was set to 0. Similarly, Z2 was set to 1 if t ≥ tlag, else Z2 was set to 0. IC50 is the plasma apratastat concentration causing 50% of the maxi-mum inhibition of intracellular TNF-α synthesis.
ResulTs
lPs-Induced TNF-α Release
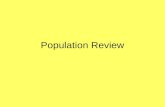
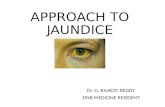
In vitro. In SAD, MAD, and LPS-challenge studies, the effect of apratastat on TNF-α release in LPS-stimulated predose whole blood in vitro was investi-gated. Preincubation with apratastat (concentration range, 10-3000 ng/mL) significantly reduced LPS-induced TNF-α release in a concentration-dependent manner in all subjects with, on average, greater than 95% inhibition achieved at 3000 ng/mL. The best fit for in vitro data was obtained with an inhibitory sig-moid Emax model in which no baseline (E0) was applied (Figure 2). The population parameters of Emax, IC50, and γ were 99.9%, 144 ng/mL, and 1.2, respec-tively. The interindividual variability in Emax and IC50 was calculated to be 3.4% and 32.4%, respec-tively, and the residual variability for TNF-α inhibi-tion was 4.8, as shown in Table I. The potential correlations between Bayesian estimated IC50 and age, body weight, or baseline TNF-α concentrations were evaluated visually. No significant relationship was
Apratastat(Cp-t)
IntracellularPrecursor
TNF-α
t1agIntracellularTNF-α (R1-t)
PlasmaTNF-α (R2-t)
K0 Kin Kout
(-) TACE during Tsynt
LPS (4 ng/kg)
Figure 1. A mechanism-based PK-PD model to characterize the induction of TNF-α synthesis following LPS injection and inhibition of TNF-α synthesis by apratastat in healthy subjects.
(3)(3)
(4)
(5)
P P ei popi= × η
dRdt
kI C
ICZ k R Zin
10
501 1 21= ⋅ −
⋅
⋅ − ⋅ ⋅maxγ
γ
dRdt
k R Z k Rin out2
1 2 2= ⋅ ⋅ − ⋅ .

476 • J Clin Pharmacol 2011;51:472-481
SHU ET AL
detected. A bootstrap approach was used to test the stability of the developed in vitro PK-PD model. All of the typical population parameters, interindividual variability, and residual variability fell within the 95% CI constructed based on 2000 bootstrap runs. The bootstrap results indicated the developed in vitro PK-PD model was stable.
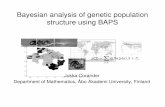
Ex vivo studies. The effect of oral administration of apratastat to healthy subjects on LPS-induced TNF-α release ex vivo significantly suppressed the
LPS-induced TNF-α release in whole blood, in a tran-sient time-dependent manner (Figure 3). The mean maximal inhibition was demonstrated at 1 hour after apratastat administration. The inhibition of TNF-α ex vivo is concentration-dependent. Figure 4 shows the relationship between percentage inhibitions of TNF-α versus ex vivo apratastat concentrations of all sub-jects as percentage inhibition from baseline for a single dose of apratastat. The best fit for ex vivo data was obtained with an inhibitory Emax model. The population parameter of IC50 was 81.7 ng/mL. The
Figure 2. Inhibition of TNF-α release in vitro by apratastat in healthy subjects.
Table I. Parameter Estimates in Population PK-PD Model for Apratastat In Vitroa
Parameter symbol estimate Rse (%) 2.5th Percentileb 50th Percentileb 97.5th Percentileb
PD parameters Emax θ2 99.9 0.33 99.3 99.9 101 IC50, ng/mL θ3 144 0.73 135 144 153 γ θ4 1.21 1.59 1.18 1.21 1.25IIV IIV (%) on Emax ωEmax 3.39 22.3 2.58 3.36 4.04 IIV (%) on IC50 ωIC50 32.4 18.1 27.0 32.4 37.3 IIV (%) on γ ωγ 14.0 21.4 10.8 14.0 16.5Residual variability Additive error variability (%)
σAdd 4.82 16.6 4.09 4.78 5.51
PK-PD, pharmacokinetic-pharmacodynamic; RSE, relative standard error; PD, pharmacodynamic; IIV, interindividual variability.a. Estimate: final parameter estimates for θ, ω, σ, etc. RSE %: 100 × (standard error/estimate). IIV (%): interindividual variability = 100 × sqrt (estimate for ω2). ω2: random effect parameter that represents residual variance. σ2: random effect parameter that represents residual variance. Emax: maximum PD response. IC50: aparatstat concentration needed to inhibit 50% of TNF-α release by LPS. γ: shaping factor.b. Based on 2000 bootstrapping runs.
Time (hr)
0 6 12 18 24
% o
f Bas
elin
e T
NF
-α C
once
ntra
tion
(%)
0
20
40
60
80
100
120Placebo 350 mg Apratastat
Figure 3. Inhibition of TNF-α by apratastat over time (in vitro or ex vivo).

POPULATION PK-PD MODELING OF APRATASTAT
PhARMACOkINEtICS AND PhARMACODyNAMICS 477
interindividual variability in IC50 was calculated to be 56.4%, and the residual variability for TNF-α inhibi-tion was 0.36, as illustrated in Table II. All the typical population parameters, interindividual variability, and residual variability fell within the 95% CI con-structed based on 2000 bootstrapping runs. The boot-strapping results indicated the developed ex vivo PK-PD model was stable.
lPs-Induced TNF-α Release in healthy subjects
The summary of the PK results following single oral administration of apratastat is shown in Table III. Apratastat was rapidly absorbed after oral
administration, with maximum plasma concentra-tions attained approximately 1 hour later. The mean half-life for each dose cohort ranged between 1.1 and 2.6 hours. The Cmax and AUC values increased in an approximately dose-proportional manner.
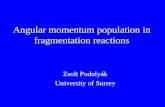
Following placebo, LPS elicited a monophasic increase in plasma TNF-α concentrations peaking after 1 hour (1469.7-969.4 pg/mL). Figure 5 depicts the mean plasma levels of TNF-α versus time follow-ing single doses of apratastat (10, 20, 50, 100, 200, and 350 mg). The median tmax of TNF-α was at 1.5 to 2.0 hours in all dose groups. Data indicated that coadministration of apratastat leads to profound suppression in the TNF-α exposure with respect to both maximal concentration and area under the plasma concentration curve of TNF-α. Maximum inhibition of TNF-α was achieved following single administration of 50 mg to 350 mg apratastat (Figure 5). Moderate inhibition was noted after the adminis-tration of 20 mg apratastat, while no apparent inhibi-tion was observed with 10 mg of apratastat. In contrast, no inhibition of LPS response was observed after administration of 10 mg or 100 mg of apratastat if administered 3 hours before LPS administration.
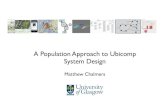
This integrated mechanism-based PK-PD model was successfully fitted to both plasma concentration-time data of apratastat and TNF-α. The model could satisfactorily describe TNF-α concentration-time course as illustrated by the good correlation between the model-predicted TNF-α concentrations and the observed TNF-α concentration (Figure 6). The population-predicted PK-PD parameters are shown in Table IV. The model indicated that TNF-α was
Table II. Parameter Estimates in Population PK-PD Model for Apratastat Ex Vivoa
Parameter symbol estimate Rse (%) 2.5th Percentileb 50th Percentileb 97.5th Percentileb
PD parameters E0 θ1 0 NE 0 0 0 Emax θ2 100 NE 100 100 100 IC50, ng/mL θ3 81.7 8.6 62.9 72.3 84.3 γ θ4 1 NE 1 1 1IIV IIV (%) on IC50 ωIC50 56.4 21.9 41.8 55.6 70.6Residual variability Proportional error variability (%)
σProp 35.6 40.0 25.6 32.4 42.4
PK-PD, pharmacokinetic-pharmacodynamic; RSE, relative standard error; PD, pharmacodynamic; IIV, interindividual variability.a. Estimate: final parameter estimates for θ, ω, σ, etc. RSE %: 100 × (standard error/estimate). IIV (%): interindividual variability = 100 × sqrt (estimate for ω2). ω2: random effect parameter that represents residual variance. σ2: random effect parameter that represents residual variance. E0: baseline PD response. Emax: maximum PD response. IC50: aparatstat concentration needed to inhibit 50% of TNF-α release by LPS. γ: shaping factor.b. Based on 2000 bootstrapping runs.
Figure 4. Inhibition of TNF-α release in vitro by apratastat in healthy subjects.

478 • J Clin Pharmacol 2011;51:472-481
SHU ET AL
synthesized during approximately 100 minutes. The IC50 of apratastat in this endotoxin model was esti-mated to be 126 ng/mL. The population median of the ratio of IC50 of apratastat in vivo versus respec-tive IC50 in vitro was 0.76. All of the typical popula-tion parameters, interindividual variability, and residual variability fell within the 95% CI con-structed based on 500 bootstrap runs. The bootstrap results indicated the developed in vivo mechanism-based PK-PD model was stable.
dIsCussIoN
The results of this study show that apratastat inhib-its LPS-induced TNF-α release in vitro and ex vivo, in a concentration-dependent manner, with IC50 val-ues of 144 and 81.7 ng/mL, respectively. The maxi-mal inhibition of LPS-stimulated TNF-α release of almost 100% in both human whole blood in vitro and ex vivo could be of importance in the treatment of rheumatic diseases. Although these in vitro and ex vivo systems have provided valuable informa-tion, they do not take into account the complexities that could occur in whole body such as protein binding, compartmentalization, and possible inter-action between different cell types.
Table III. PK Parameters of Apratastat Following Single Oral Dosing in LPS-Challenge Study
dose Group (mg) Cmax (ng/ml) tmaxa (h) half-life (h) AuClast (ng × h/ml) AuCinf (ng × h/ml) Cl/F (l) Vdss/F (l)
10 77.6 ± 41.2 1.0 1.1 ± 0.5 94.6 ± 38.5 103 ± 38 116 ± 64.6 165 ± 81.420 139 ± 68 0.9 1.6 ± 0.4 212 ± 60 212 ± 57 102 ± 36.5 234 ± 96.650 340 ±135 1.0 2.6 ± 1.7 602 ± 105 618 ± 98 82.5 ± 12.0 304 ± 197100 624 ± 220 0.9 2.5 ± 0.8 1144 ± 116 1155 ± 118 87.4 ± 9.2 318 ± 99.0200 922 ± 367 1.0 2.0 ± 0.8 2186 ± 327 2195 ± 324 93.0 ± 15.1 277 ± 175350 1416 ± 584 1.0 2.4 ± 0.7 4178 ± 1000 4205 ± 1009 87.6 ± 22.5 296 ± 101
LPS, endotoxin; Cmax, observed maximum (peak) concentrations; tmax, time to peak concentration; half-life, terminal-phase elimination half-life (0.693/λz); AUClast, area under the concentration-time curve to the last observable concentration; AUCinf, area under the concentration-time curve from time 0 extrapolated to infinite time; CL/F, apparent oral clearance; Vdss/F, apparent volume of distribution at steady state.a. Median value.
Figure 5. Mean TNF-α concentration-time profiles following the oral administration of single doses of apratastat (10, 20, 50, 100, 200, and 350 mg) or placebo. The profile following 350 mg dose was superimposed with that following 200 mg dose (not shown here).
Observed TNF-α Conc. (pg/mL)
0 500 1000 1500 2000 2500 3000
Pre
dict
ed T
NF
-α C
onc.
(pg
/mL)
0
500
1000
1500
2000
2500
3000
TNFα Concentrations, pg/mLLine of Unity
Figure 6. Posterior Bayesian predicated TNF-α concentrations versus observed TNF-α concentrations by the PK-PD model in healthy subjects.

POPULATION PK-PD MODELING OF APRATASTAT
PhARMACOkINEtICS AND PhARMACODyNAMICS 479
In the LPS-challenge study we have measured inhibition of LPS-induced TNF-α release in healthy subjects. Apratastat demonstrated potent inhibitory activity against LPS-induced systemic TNF-α release after oral administration (IC50 of 126 ng/mL). The concentrations of apratastat required to inhibit TNF-α production in vivo and in whole blood in vitro or ex vivo appeared to be similar. The minimum effec-tive dose to completely block the effect of LPS was determined to be 50 mg of apratastat when coadmin-istered with LPS. The peak plasma concentrations achieved in vivo following oral administration of 50 to 350 mg were greater than the IC50 values deter-mined in vitro and ex vivo for inhibition of TNF-α release. In contrast, the peak plasma concentrations following oral administration of 10 mg were lower than the IC50 values from in vitro and ex vivo analy-ses. No inhibition of endotoxin response was observed in vivo.
How much and how long must the concentration of apratastat persist in vivo for it to be an effective therapeutic agent in RA? It was shown that the lev-els of TNF-α inhibition achieved, as measured in the systemic LPS-challenge model, correlated well with clinical efficacy in the collagen-induced arthritis (CIA) model.26 In our LPS-challenge study, it was found that apratastat reduced TNF production in a dose-dependent manner with approximately 80% inhibition at the highest dose administered.
Assuming the concentration of apratastat ought to be above this level to achieve efficacy in vivo, this would suggest that a dosing regimen of more fre-quent than once daily be necessary based on our PK-PD model. The mean in vivo IC50 for inhibition of TNF-α generated from the LPS-challenge study was used as the threshold level to select the dose regi-men for a phase II dose-ranging study. The selected dose of 50, 100, and 150 mg 3 times daily (TID) were estimated to provide exposure above this threshold at 25%, 50%, and 75% of the time during a 24-hour period.
A phase II, double-blind, placebo-controlled, par-allel, randomized, multicenter, outpatient, compara-tive study in subjects with active RA and an inadequate response to stable dosages of methotrex-ate (MTX) (7.5 to 20 mg once weekly) was conducted with 50, 100, and 150 mg TID dose regimen.27 In the study, we failed to show that apratastat was effective in reducing signs and symptoms of RA in the clinic.28 What lessons can we learn from this PK-PD-guided approach for dose selection? We were using in vivo IC50 generated from a LPS-challenge study as a thresh-old level to select phase II dose regimens; however, TNF-α and apratastat levels in blood, as we measured in our LPS-challenge study, might not necessarily reflect those in the joints of patients with rheumatoid arthritis. In addition, differences in penetration of apratastat into inflamed and noninflamed tissues,
Table IV. Parameter Estimates in Mechanism-Based Population PK-PD Model for Apratastat In Vivoa
Parameter symbol estimate Rse (%) 2.5th Percentileb 50th Percentileb 97.5th Percentileb
PD parameters K0, ng/h θ1 1480 29.7 200 1500 8604 Kin-Kout, 1/h θ2 2.11 12.6 0.33 2.25 3.00 Kout, 1/h θ3 1.82 6.48 1.52 1.97 5.42 Tsynt, h θ4 1.72 3.60 0.53 1.68 2.69 Tlag, h θ5 0.94 0.73 0.35 0.94 1.44 IC50, in vivo/IC50, in vitro θ6 0.76 17.0 0.15 0.68 1.00IIV IIV (%) on θ1 ωθ1 142 78.7 76.7 172 260 IIV (%) on θ2 ωθ2 153 102 54.6 189 801 IIV (%) on θ3 ωθ3 197 85.8 0.95 293 15800Residual variability Additive error variability σAdd 35.5 2.72 5.33 34.1 106
PK-PD, pharmacokinetic-pharmacodynamic; RSE, relative standard error; PD, pharmacodynamic; IIV, interindividual variability.a. Estimate: final parameter estimates for θ, ω, σ, etc. RSE %: 100 × (standard error/estimate). IIV (%): interindividual variability = 100 × sqrt (estimate for ω2). ω2: random effect parameter that represents residual variance. σ2: random effect parameter that represents residual variance. IC50: apratastat concentration needed to inhibit 50% of TNF-α release by LPS.b. Based on 500 bootstrapping runs.

480 • J Clin Pharmacol 2011;51:472-481
SHU ET AL
and compartmentalization of TNF-α excretion at rel-evant tissue sites were not taken into account. It was possible that the concentration of apratastat in the joints following selected doses might be lower than that in the systemic circulation, which resulted in an insufficient inhibition of TNF-α in the joints.
Given that no inhibition of LPS-stimulated TNF-α release was observed after the administration of 100 mg of apratastat 3 hours before LPS administration, as opposed to a maximal suppression of LPS-stimulated TNF-α release being observed when apratastat was administered 0.5 hours before LPS injection, this would suggest that the sensitivity of LPS-stimulated TNF-α release to the suppressive effect of apratastat is transient. Our finding was similar to what is reported elsewhere in the litera-ture,29,30 which suggests that apratastat may be rap-idly inactivated while in systemic circulation. The rapid inactivation of apratastat does not result from fast elimination of apratastat, because the apratastat concentration 3 hours after a 100-mg dose is still greater than the Cmax after a 50-mg dose. The loss of activity with 100-mg apratastat administered 3 hours before LPS administration is possibly related to the protein binding of apratastat. A study with an endo-toxin antagonist drug has demonstrated that binding to liproproteins may result in a time-dependent loss of drug activity.31 The fact that the total concentra-tion of apratastat was used in the PK data analysis and not the unbound concentration may have influ-enced the results because the possible binding of apratastat to plasma protein was not taken into account. However, the plasma protein binding of apratastat was never analyzed in healthy subjects so we could not incorporate this parameter into the PK-PD model. Further investigation would be required to evaluate this hypothesis. In addition, we could not find any evidence in the literature demon-strating induction or different activation states of the TACE enzyme that would lead to tachyphylaxis to the effects of apratastat. Therefore tachyphylaxis is not one of the assumptions in the PK-PD model.
While the protein binding may affect apratastat’s activity in inhibiting LPS-stimulated TNF-α release, it would be reasonable to postulate that use of suf-ficiently high doses or extended administration of apratastat may counteract the protein binding effect. Furthermore, in a therapeutic setting, it is also pos-sible that disease state alterations in plasma protein levels may need to be considered in dosing calcula-tions. Because of rapid loss in PD activity following oral administration, an intravenous infusion might have been helpful to achieve desirable efficacy.
It should be noted that this PK-PD model was merely based on a relatively small number of healthy subjects with a limited number of measure-ments per subject. An investigation of the effect of apratastat on TNF-α release in patients with RA would have been more relevant, as it is likely that patients with RA respond to apratastat differently than healthy subjects. In patients with RA, there is evidence of an enhanced release of TNF-α after incubation of either whole blood32 or isolated monocyte preparations with LPS.33 The magnitude of LPS-induced release of TNF-α in whole blood is under genetic control,34 and there is evidence that certain polymorphisms of the TNF gene may be related to the severity of RA.35
Although apratastat inhibited the secretion of TNF-α induced by LPS, it had no effect on LPS-induced secretion of other soluble cytokines, such as IL-1β, IL-6, or IL-8 at the highest dose administered. It is unclear whether the lack of efficacy seen with apratastat was because of failure of inhibition of TACE, the inhibition of multiple MMPs, or the short duration of exposure. Apratastat is not the only experimental compound that has failed to show effi-cacy in RA subjects during clinical study, despite LPS-induced TNF-α levels being reduced in vitro and in vivo.36 The relevance of the LPS model to human RA and the relevance of the TNF-α inhibition in LPS-challenge studies to the progression of inflammatory arthritis are still unclear.
The authors wish to thank the patients and study personnel who made this study possible.
Financial disclosure: This study was funded by Wyeth Research.
ReFeReNCes
1. Vassali P. The pathophysiology of tumor necrosis factors. Annu Rev Immunol. 1992;10:411-452.2. Kriegler M, Perez C, DeFay K, Albert I, Lu SD. A novel form of TNF/cachectin is a cell surface cytotoxic transmembrane protein: ramifications for the complex physiology of TNF. Cell. 1988;53:45-53.3. Gearing AJH, Beckett P, Christodoulou M, et al. Processing of tumor necrosis factor-alpha precursor by metalloproteinases. Nature. 1994;370:555-557.4. McGeehan GM, Becherer JD, Bast RC, et al. Regulation of tumor necrosis factor-alpha processing by a metalloproteinase inhibitor. Nature 1994;370:558-561.5. Shaw T, Nixon JS, Bottomley KM. Metalloproteinase inhibitors: new opportunities for the treatment of rheumatoid arthritis and osteoarthritis. Expert Opin Investing Drugs. 2000;9:1469-1478.

POPULATION PK-PD MODELING OF APRATASTAT
PhARMACOkINEtICS AND PhARMACODyNAMICS 481
6. Buchan G, Barrett K, Turner M, Chantry D, Maini RN, Feldmann M. Interleukin-1 and tumor necrosis factor mRNA expression in rheumatoid arthritis: prolonged production of IL-1α. Clin Exp Immunol. 1988;73:449-455.7. Lewis EJ, Bishop J, Bottomley KMK, et al. Ro 32-3555, an orally active collagenase inhibitor, prevents cartilage breakdown in vitro and in vivo. Br J Pharmacol. 1997;121:540-546.8. Burrage PS, Mix KS, Brinckerhoff CE. Matrix metalloprotein-ases: role in arthritis. Front Biosci. 2006:11:529-543.9. Pap T, Shigeyama Y, Kuchen S, et al. Differential expression pattern of membrane-type matrix metalloproteinases in rheuma-toid arthritis. Arthritis Rheum. 2000;43:1226-1232.10. Katrib A, Tak PP, Bertouch JV, et al. Expression of chemokines and matrix metalloproteinases in early rheumatoid arthritis. Rheumatology (Oxford). 2001;40:988-994.11. Tomita T, Nakase T, Kaneko M, et al. Expression of extracel-lular matrix metalloproteinase inducer and enhancement of the production of matrix metalloproteinases in rheumatoid arthritis. Arthritis Rheum. 2002;46:373-378.12. Feldmann M, Charles P, Taylor P, Maini RN. Biological insights from clinical trials with anti-TNF therapy. Springer Semin Immunopathol. 1998;20:211-228.13. Feldmann M, Brennan FM, Elliott M, Katsikis P, Maini RN. TNF alpha as a therapeutic target in rheumatoid arthritis. Circ Shock. 1994;43:179-184.14. Feldmann M, Brennan FM, Foxwell BM, Maini RN. The role of TNF alpha and IL-1 in rheumatoid arthritis. Curr Dir Autoimmun. 2001;3:188-199.15. Choy EH, Panayi GS. Cytokine pathways and joint inflamma-tion in rheumatoid arthritis. N Engl J Med. 2001;344:907-916.16. Feldmann M, Charles P, Taylor P, Maini RN. Biological insights from clinical trials with anti-TNF-alpha therapies: the next generation. Nat Rev Drug Discov. 2003;2:736.17. Moreland LW, Baumgartner SW, Schiff MH, et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis fac-tor receptor (p75)-Fc fusion protein. N Engl J Med. 1997;337:141-147.18. Elliott MJ, Maini RN, Feldmann M, et al. Randomized double-blind comparison of chimeric monoclonal antibody to tumor necrosis factor alpha (cA2) versus placebo in rheumatoid arthri-tis. Lancet. 1994;344:1105-1110.19. Furst DE, Schiff MH, Fleischmann RM, et al. Adalimumab, a fully human anti tumor necrosis factor-alpha monoclonal anti-body, and concomitant standard antirheumatic therapy for the treatment of rheumatoid arthritis: results of STAR (Safety Trial of Adalimumab in Rheumatoid Arthritis). J Rheumatol. 2003;30:2563.20. Van der Poll T, Coyle SM, Levi M, et al. Effect of a recom-binant dimeric tumor necrosis factor receptor on inflammatory responses to intravenous endotoxin in normal humans. Blood. 1997;89:3727-3734.21. Suffredini AF, Reda D, Banks SM, Tropea M, Agosti JM, Miller R. Effects of recombinant dimeric TNF receptor on human inflam-matory responses following intravenous endotoxin administra-tion. J Immunol. 1995;155:5038-5045.22. Branger J, van den Blink B, Weijer S, et al. Anti-inflammatory effects of a p38 mitogen-activated protein kinase inhibitor during human endotoxemia. J Immunol. 2002;168:4070-4077.
23. Dekkers PE, Lauw FN, ten Hove T, et al. The effect of a metal-loproteinase inhibitor (GI5402) on tumor necrosis factor-alpha (TNF-alpha) and TNF-alpha receptors during human endotox-emia. Blood. 1999;94:2252-2258.
24. Sheiner LB, Beal SL, Boeckmann AJ. NONMEM Project Group. San Francisco, CA: University of California, San Francisco; 1992.
25. Gozzi P, Pahlman I, Palmer L, Grönberg A, Persson S. Pharmacokinetic-pharmacodynamic modeling of the immu-nomodulating agent susalimod and experimentally induced tumor necrosis factor-α levels in the mouse. JPET. 1999;291:199-203.
26. Newton RC, Solomon KA, Covington MB, Decicco CP, Haley PJ, Friedman SM. Biology of TACE inhibition. Ann Rheum Dis. 2001;60:iii25-32.
27. Fleischmann R, Kivitiz A, Franklin C. A Randomized, Double-Blind, Placebo-Controlled, Sequential-Dose Study of the Safety of Apratastat, A Novel Oral Dual Inhibitor of TNF-α Converting Enzyme/Metalloproteinase in Patients With Rheumatoid Arthritis on a Background of Methotrexate. Vienna: The Annual European Congress of Rheumatology (EULAR); 2005.
28. Fleischmann R, Genovese M, Keystone EC, et al. Lack of Efficacy With 3 Oral Dose Levels of Apratastat, in Subjects With Active Rheumatoid Arthritis on a Background of Methotrexate—A Phase 2 Double-Blind, Placebo-Controlled, Parallel, Randomized Study. Amsterdam: The Annual European Congress of Rheumatology (EULAR); 2006.
29. Lynn M, Rossignol DP, Wheeler JL, et al. Blocking of responses to endotoxin by E5564 in healthy volunteers with experimental endotoxemia. J Infect Dis. 2003;187:631-639.
30. Rossignol DP, Lynn M. Antagonism of in vivo and ex vivo response to endotoxin by E5564, a novel synthetic lipid A antago-nist. J Endotoxin Res. 2003;8:483-488.
31. Rose JR, Mullarkey MA, Christ WJ, et al. Consequences of interaction of a lipophilic endotoxin antagonist with plasma lipoproteins. Antimicrob Agents Chemother. 2000;44:504-510.
32. Zangerle PF, De Goote D, Lopez M, et al. Direct stimulation of cytokines (IL1, TNF, IL6 IFN-gamma and GM-CSF) in whole blood: application to rheumatoid arthritis and osteoarthritis. Cytokine. 1992;4:568-575.
33. Leirisalo-Repo M, Paimela L, Jaattela M, Koskimies S, Repo H. Prodiction of TNF by monocytes of patients with early rheumatoid arthritis is increased. Scand J Rheumatol. 1995;24:366-371.
34. Louis E, Franchimont D, Piron A, et al. Tumor necrosis factor gene polymorphism influences TNF production in lipopolysac-charide-stimulated whole blood cell culture in humans. Clin Exp Immunol. 1998;113:401-406.
35. Verwej C. Tumor necrosis factor gene polymorphisms as severity marker in rheumatoid arthritis. Ann Rheum Dis. 1999;58:120-126.
36. Palladino MA, Bahjat FR, Theodorakis EA, Moldawer LL. Anti-TNF-alpha therapies: the next generation. Nat Rev Drug Discov. 2003;2:736-746.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav.