Penicillins (ANTIBIOTICS)
18
Penicillins Dr. Arham Shabbir Pharm.D, M.Phil. Pharmacology, Ph.D. Pharmacology(U.H.S) Professor (Pharmacology) Lahore Pharmacy College of Lahore Medical & Dental College
-
Upload
muhammad-arsal -
Category
Health & Medicine
-
view
299 -
download
0
Transcript of Penicillins (ANTIBIOTICS)

PenicillinsDr. Arham ShabbirPharm.D, M.Phil. Pharmacology, Ph.D. Pharmacology(U.H.S)Professor (Pharmacology)Lahore Pharmacy College ofLahore Medical & Dental College

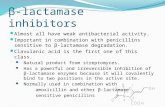
Structure A thiazolidine ring which is attached to β-lactam ring 6- aminopenicillanic acid nucleus is essential for activity If the β-lactam ring is enzymatically cleaved by bacterial β-
lactamases, the resulting product, penicilloic acid lacks antibacterial activity

Classification Natual penicillins Penicillin G (Benzyl penicillin) Penicillin V has a spectrum similar to that of penicillin G, but it is
not used for treatment of bacteremia because of its poor absorption, narrow spectrum and need for dosing four times.
Anti staphylococcal penicillins The semi synthetic penicillins Methicillin, nafcillin, oxacillin, and
dicloxacillin are penicillinase resistant penicillins. Because of its toxicity (interstitial nephritis), methicillin is not
used clinically except to identify resistant strains of S. aureus. Methicillin resistant Staphylococcus aureus (MRSA) is currently a source of serious community and nosocomial (hospital-acquired) infections and is resistant to all commercially available -lactam βantibiotics, including antistaphylococcal penicillins. This organism is usually susceptible to Vancomycin.

The penicillinase-resistant penicillins have no activity versus gram-negative infections.
However, for infections caused by methicillin susceptible strains of staphylococci these are considered the drugs of choice.
Extended spectrum penicillins Ampicillin and Amoxicillin have an antibacterial spectrum
similar to that of penicillin G but are more effective against gram-negative bacilli. Therefore, they are referred to as extended-spectrum penicillins
Resistance to these antibiotics is now a major clinical problem because of inactivation by plasmid mediated penicillinases.
Formulation with a -β lactamase inhibitor, such as clavulanic acid or sulbactam, protects amoxicillin or ampicillin, respectively, from enzymatic hydrolysis and extends their antimicrobial spectrum
Synergistic effect with aminoglycosides

Anti pseudomonal penicillins
Carbenicillin, ticarcillin, and piperacillin are called antipseudomonal penicillins because of their activity against P. aeruginosa
These drugs have activity against several gram-negative rods, including Pseudomonas, Enterobacter, and in some cases Klebsiella species.
susceptible to penicillinases and are often used in combination with penicillinase inhibitors (eg, tazobactam and clavulanic acid) to enhance their activity.
Synergism with aminoglycosides



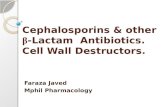
Mechanism of action The transpeptidation reaction in Staphylococcus aureus that is
inhibited by β-lactam antibiotics. The cell wall of gram-positive bacteria is made up of long peptidoglycan polymer chains consisting of the alternating N-acetylglucosamine (G) and N-acetylmuramic acid (M) with pentapeptide side chains linked (in S. aureus) by pentaglycine bridges. The exact composition of the side chains varies among species. The diagram illustrates small segments of two such polymer chains and their amino acid side chains. These linear polymers must be cross-linked by transpeptidation of the side chains at the points indicated by the asterisk to achieve the strength necessary for cell viability.
0 UDP-acetylmuramyl-L-Ala-D-Glu-L-Lys-D-Ala-D-Ala sequence is also called as “Park nucelotide”, formerly called as “Park peptide”

Penicillin binding proteins (PBPs) catalyze the transpeptidase reaction that removes the terminal alanine to form a cross link with a nearby peptide.
This gives cell wall its structural rigidity β- lactam antibiotics are structural analogs of the D-ala-D-
ala substrate. This substrate is bound by PBP at active site When a β- lactam is attached PBP, transpeptidation reaction
is blocked which leads to inhibition of peptidoglycan synthesis and the cell dies
Exact mechanism of bacterial cell death is unknown but involvement of autolysins activation and destabilization of bacterial membrane against high internal osmotic pressure is suggested.

Resistance1. Inactivation of antibiotic with β-lactamase2. Modification of target PBPs3. Impaired penetration of drug to target PBPs4. Presence of efflux pump β-lactamase production is the most common mechanism of
resistance Some β-lactamase hydrolyze penicillins but not
cephalosporins e.g. those produced by E. coli, S. aureus. Whereas, those produced by P. aeruginosa and enterobacter
hydrolyze both. Carbapenems are highly resistant to hydrolysis by
penicillinases and cephalosporinases but are hydrolyzed by metallo-β-lactamase.

Pharmacokinetics Absorption differs for different penicillins, depending upon
their acid stability and protein binding. Methicillin is acid labile Gastrointestinal absorption of nafcillin is erratic Both are not suitable for oral administration. Amoxicillin, ampicillin and dicloxacillin are acid stable and
relatively well absorbed Absorption of most oral penicillins are impaired by food
(except amoxicillin), therefore, should be administered 1-2 hrs before meal.
Absorption through IV route is preferred due to local irritation and pain produced by IM injection of large doses.

Penicillins are usually excreted by kidney through urine and small amounts are excreted by other routes
Those penicillins which are excreted through kidney, dose must be adjusted according to renal function e.g. normal half life of Penicillin G is usually 30 min and in renal failure it may increase upto 10 hours.
Nafcillin is primarily cleared by biliary excretion Oxacillin, dicloxacillin and cloxacillin are cleared by both
kidney and biliary excretion. No dose adjustments are required for these drugs in renal
failure.

Adverse reactions Penicillins are remarkably non toxic1- Hypersensitivity reactions Due to penicilloic acid (metabolite of penicillin) From skin rash to anaphylactic shock (includes fever,
nephritis, pruritis, urticaria, joint swelling etc.) Methicillin cause interstitial nephritis while nafcillin causes
neutropenia Incidence of allergic reaction in small children is negligible2-GIT disturbances Due to over growth of G+ organisms or by direct irritation Nausea, vomiting, diarrhea Pseudomembranous colitis (Inflammation of colon) Ampicillin (rare).

MOA: Penicillin causes normal flora to alter. When an antibiotic kills competing bacteria in the intestine, the remaining bacteria will have less competition for space and nutrition. The net effect is to permit more extensive growth than normal of certain bacteria. E.g. C. difficile.
Vaginal candidiasis can also occur.3- Seizures Penicillin G causes seizures if given intra-thecal in patients
especially with renal failure patients. They also can cause confusion and psychosis (neurotoxicity).
MOA: Most widely accepted theory involves binding to GABA receptors which are involved in inhibitory neurotransmission
Benzodiazepines and Barbiturates are used as treatment Cessation of seizure activity has been reported 12-72 hrs
after therapy is discontinued. The epilepticogenic activity may be due to β-lactam ring

Treatment / Anti-dot Allergy is treated by Anti-histamine Desensitization can be accomplished with gradually
increasing doses of penicillin Anaphylactic shock is treated by Adrenaline and
corticosteroids. MOA: Vasodilation (Fall in BP) and bronchoconstriction are
important symptoms of anaphylactic shock, whereas, adrenaline causes vasoconstriction and bronchodilation.
Corticosteroids have anti-inflammatory effects Penicillins and carbapenems are both neurotoxic. Dose
adjustment in renal failure is key strategy to avoid neurotoxicity.

Contraindications / drug interactions
Captopril (capotein) – Increase potassium level. Spironolactone (Aldactone) – K+ sparing diuretics K+ suppliments (KCl). Especially with those penicillins which are available in
potassium salts. Hyperkalemia can generate arrhythmia in cardiac patients. Sodium salts should be avoided in hypertensive patients. Ticarcillin and carbencillin have antiplatelet aggregation effect. Be careful when administering Streptokinase, warfarin,
heparin, clopidogrel etc to patients who are already taking these penicillins.

Penicillins inhibit the excretion of methotrexate (anti-cancer) due to which toxic effects of methotrexate occur, such as, bone marrow depression.
Probencid is a uricosuric agent. It increases the concentration of penicillin and inhibit its excretion.
Penicillins decrease the effectiveness of estrogens in contraceptive pills.
Dose of penicillins should be increased in immunocompromised patients.
Should not be taken with acidic juices and should be administered with full glass of water.

Patient history Allergy Hypertensive (having low salt diet) Impaired renal function GIT problems Tendency to bleed