Pathobiology of Lymphoid and Myeloid Blast Crisis and Management...
7
Click here to load reader
Transcript of Pathobiology of Lymphoid and Myeloid Blast Crisis and Management...

188 American Society of Hematology
Pathobiology of Lymphoid and Myeloid BlastCrisis and Management Issues
Robert L. Ilaria, Jr.
Despite recent improvements in the treatment ofearly-stage disease, the blastic phase of chronicmyeloid leukemia (CML) remains a therapeuticchallenge. For imatinib-naïve patients, imatinibprovided encouraging hematologic and cytogeneticbenefits; however, the vast majority of CML blastcrisis cases today arise in patients already on imat-inib-based therapy. Clonal evolution and duplication ofthe Philadelphia chromosome continue to be associ-ated with blastic phase transformation, but recentstudies have identified BCR/ABL kinase domain
mutations in 30%-40% of blast crisis patients. Thisimplies that BCR-ABL–targeted therapy might haveinfluenced the molecular road map to blastic transfor-mation. In this review, we will examine the effect ofimatinib on primitive CML progenitors and how thismight influence the pathophysiology of blast crisis. Arational framework for deciding how best to integratestem cell transplantation, traditional chemotherapy,imatinib, and other BCR-ABL kinase inhibitors in thecare of blast crisis patients will also be discussed.
Statement of the Problem:What Is CML Blast Crisis?Chronic myeloid leukemia (CML) in blastic phase is thetransition of CML in chronic or accelerated phase to anacute leukemia, characterized by ≥ 30% blasts in the bonemarrow or peripheral blood, or the development of ex-tramedullary disease outside of the spleen. In light of re-cent changes in the World Health Organization definitionof acute leukemia, the percentage of blasts required forCML in blastic phase may someday be reduced to 20%.Consistent with the early stem cell nature of CML,1 blastictransformation may be myeloid, lymphoid, or undifferenti-ated/mixed, with myeloid blast crisis being about two timesmore common than lymphoid. Although the definition ofCML in blastic phase has not changed from the pre- topost-imatinib era, the treatment history of our current CMLpatient population has: an ever-increasing proportion ofpatients with CML will have been managed exclusivelywith imatinib or other ABL kinase inhibitor therapy. Sucha significant change in therapeutic approach will almostcertainly affect the kinetics and molecular phenotype ofCML blast crisis.
Pathophysiology of CML Blast Crisis—Why Does It Occur?The pathophysiology of CML blast crisis is incompletelyunderstood. However, recent advances in our understand-ing of cancer and leukemia stem cell biology and emerg-
ing data about imatinib-resistant CML and BCR-ABL-re-lated genomic instability have led to the formulation of ageneral framework. This working mechanistic model ofCML blast crisis is based on a few assumptions. The first isthat BCR-ABL is directly or indirectly responsible for pro-gressive genomic instability or epigenetic changes, whichoccur at the CML stem cell level and/or in later CML pro-genitor cells. The second is that the degree of genomicinstability is proportional to the level of BCR-ABL kinaseactivity. The third is that CML stem cells are the least vul-nerable to ABL-targeted therapy and may serve as reser-voirs for occult CML progression. Together, these phenom-ena conspire to bring about an acquired loss of hematopoi-etic cell differentiation, resulting in a highly aggressive,acute leukemia.
Numerous studies have implicated BCR-ABL in pro-viding a milieu favorable for the generation and mainte-nance of secondary DNA alterations.2-9 The findings of theseand other studies are consistent with clinical studies link-ing clonal evolution to CML progression, including thedevelopment of blast crisis. The most common gross cyto-genetic abnormalities associated with CML blast crisis in-clude duplication of the Ph chromosome, trisomy 8, andisochromosome 17; however, these abnormalities may alsobe observed in patients with earlier stages of CML10,11 Al-though more prevalent in blastic phase than other CMLstages, alterations in p53 have been found in only a minor-ity (24%) of cases.12 Loss of p16INK4A/ARF has been reportedin up to half of patients with CML in lymphoid blast crisisbut is rare in the myeloid form.13 Thus, it is reasonable tohypothesize that clonal evolution plays a role in blasticprogression,10 likely facilitated by the dysregulation ofnormal apoptotic pathways by BCR-ABL.14-17 Althoughclonal evolution implies some degree of BCR-ABL inde-pendence, some common cytogenetic changes observed in
University of Texas Southwestern Medical Center
Correspondence: Robert Ilaria, Jr., MD, Medical Advisor, LillyResearch Laboratories, Lilly Corporate Center DC 2133,Indianapolis, IN 46285; Phone (317)433-4759, Fax (317)276-9666, [email protected]

Hematology 2005 189
advanced CML may be surrogate markers of genomic in-stability rather than direct clues to which genes are pivotalto CML progression. Recent studies have implicated acti-vation of the LYN, AKT, and STAT5 signaling pathways inthe development of BCR-ABL-independent leukemogen-esis,18,19 but additional studies will be required to deter-mine if specific blockade of these pathways will have thera-peutic benefit in CML.
How might the degree of residual BCR-ABL kinaseactivity present in CML progenitors, which appear to sur-vive imatinib treatment,20 influence CML progression toblast crisis? The essential role of BCR-ABL tyrosine ki-nase activity in cellular transformation is well established21
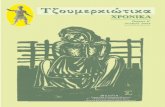
and played a central role in the decision to pursue ABL-targeted therapy for CML. Thus, it is reasonable to con-clude that CML progenitors surviving imatinib therapywould still be vulnerable to BCR-ABL–dependent influ-ences underlying CML progression. Prior to imatinib, pro-gression to CML blast crisis was virtually inevitable in theabsence of a suitable allogeneic bone marrow transplantdonor (Figure 1; dark circles). Although the length of fol-low up is still relatively short, it appears that imatinib willincrease the latency of blastic transformation compared tointerferon-α–based therapy;22 however, what proportion ofpatients with CML will avoid blastic transformation is un-known. If the amount of residual BCR-ABL kinase activityin CML progenitors were reduced to negligible levels, thenimatinib would achieve durable CML control, perhaps pre-venting the secondary changes requisite for blastic phase(Figure 1; open circles). Alternatively, imatinib-mediatedBCR-ABL inhibition might only delay the inevitable pro-gression of CML from chronic to blastic phase (Figure 1;light gray circles). Whether any level of BCR-ABL tyrosinekinase activity is safe, that is, will not carry a risk for leuke-mic progression, is unknown. Studies using high-dose imat-inib23 or more potent ABL kinase inhibitors24,25 at diagno-
sis will provide important opportunities to determine ifmore potent BCR-ABL suppression will lessen the chancesof blastic transformation.
What about CML progenitors that harbor BCR/ABLkinase domain mutations? If the risk for acquiring second-ary events correlates with the degree of BCR-ABL kinaseactivity, then CML progenitors with imatinib-resistantforms of BCR-ABL would be predicted to foster CML pro-gression.26 Presumably, in these cells BCR-ABL tyrosinekinase activity is only modestly suppressed by imatinib,and this might shorten the interval between chronic andblastic phase (Figure 1; dark gray circles). Indeed, inimatinib-naïve CML patients screened by allele specificoligonucleotide PCR, the presence of BCR/ABL kinasedomain mutations correlated with clonal evolution andadvanced stage, but interestingly not with response toimatinib or survival.27 These findings suggest that clini-cally meaningful BCR/ABL mutations must occur in the“appropriate” hematopoietic progenitor and survive com-petition with wild-type BCR-ABL progenitors and normalhematopoietic elements. Further, since almost two-dozendifferent BCR-ABL mutants have been reported, it is un-likely that all will have equal biological potency.28 BCR/ABL kinase domain mutations appear to be rare at CMLchronic phase diagnosis,29 but detection of rare mutantclones can be technically challenging. So, while it appearsthat most BCR/ABL kinase domain mutations may arisedue to wild-type BCR-ABL-induced genomic instability,further research will be required to more precisely definecause versus effect. Perhaps a retrospective analysis of CMLcohorts treated entirely in the pre-imatinib era will helpanswer these questions.
Imatinib and the CML Stem CellThe limited ability of conventional chemotherapeutic drugsto eradicate leukemia stem cells has recently been indictedas the cause of most cases of leukemic relapse.30,31 So, theactivity of imatinib or other ABL-targeted therapies againstCML stem cells has critical implications for long-term dis-ease control and even cure.32 The mechanisms responsiblefor the persistence of BCR/ABL-positive progenitors in mostimatinib-treated CML patients have not been fully eluci-dated. Cell-extrinsic factors, such as the levels of the plasmaprotein α-1-acid glycoprotein which could enhance imat-inib catabolism, have been implicated in imatinib-resis-tance,33,34 but most studies suggest cell-intrinsic factors mayplay a greater role in protecting CML progenitors fromimatinib-induced cytotoxicity. Imatinib interacts with themultidrug resistance (MDR) ATP-binding cassette (ABC)proteins MDR1 (P-glycoprotein) and ABCG2, suggestingthese drug efflux pumps may play a role in protecting CMLprogenitors from therapeutic concentrations of imatinib.35-40
ABCG2 is downregulated during hematopoietic cell differ-entiation,41 perhaps explaining why imatinib achieves rapidhematological responses, while elimination of the earliesthematopoietic progenitors proves more challenging. Be-
Figure 1. A working model depicting a link between BCR-ABL tyrosine kinase activity and the accumulation ofsecondary genetic and epigenetic changes in CMLprogenitors over time. Once a threshold (at top) of secondarymolecular events is reached, hematopoietic differentiation islost, resulting in blastic transformation. Drugs with no effect onBCR-ABL tyrosine kinase activity would be associated with aninevitable progression to blast crisis (black circles). Completesuppression of BCR-ABL (white circles) in CML stem cellsmight prevent blastic progression indefinitely, while incompletesuppression (gray shaded circles) due to ineffective drugdelivery or BCR/ABL kinase domain mutations would only delaythe accumulation of secondary events.

190 American Society of Hematology
sides mechanisms involving imatinib efflux from cells, arecent study reported that imatinib is a substrate for or-ganic cation transporter (OCT)1, a protein involved in cel-lular drug uptake, suggesting another possible variable inmaintaining effective imatinib concentrations in CML pro-genitors.42
Studies in primary CML patient samples have shownthat BCR-ABL–positive progenitors are resistant to a vari-ety of apoptotic stimuli, particularly the infrequently di-viding, or quiescent subset.43,44 In CML progenitors fromchronic phase CML, imatinib had marked activity againstthe proliferative fraction but tended to spare non-dividingcells.44 Consistent with these findings, BCR/ABL-positivecells have been detected in CD34+ cells from imatinib-treated patients with chronic phase CML in complete cyto-genetic response.20 This phenomenon is not unique toimatinib, as BCR-ABL–positive hematopoietic colonieswere also obtained from interferon-α–treated CML patientsin long-term complete cytogenetic remission.45 Does thismean imatinib and interferon-α have the same biologiclimitations in the CML stem cell compartment? Longerfollow-up studies will be required to compare the clinicalfate of CML progenitors rendered dormant by imatinib- orinterferon-α–based therapy.
Irrespective of issues of drug delivery to CML-recon-stituting cells, does imatinib achieve effective kinase inhi-bition within this early progenitor compartment? In a re-cent study of purified CML CD34+ cells, imatinib was ef-fective in suppressing the constitutive phosphorylation ofCrk-L, a commonly used surrogate marker of BCR-ABLkinase activity.46,47 However, the effect of imatinib on sig-naling within the CML-reconstituting or quiescent cell frac-tion, which comprises only a small proportion of total CMLCD34+ cells, is unknown.32,48 Further, it is conceivable thatCML stem cells are less dependent on BCR-ABL kinaseactivity than later progenitors and may be able to persistdespite effective kinase inhibition.49 In P210BCR/ABL-trans-duced human CD34+ cells, imatinib blocked proliferationbut did not completely restore altered adhesion and cellmotility.50 Whether this phenomenon indicates a tyrosinekinase independent function of BCR-ABL or is a conse-quence of imatinib-mediated inhibition of other signalingpathways such as c-KIT will require further study.51 It willalso be informative to study the effect of other ABL kinaseinhibitors on CML progenitor populations, since thesecompounds will likely have distinct patterns of tyrosinekinase inhibition.24,25,52 Although CML stem cells are un-likely to be BCR-ABL independent in early stage disease,disruption of constitutive tyrosine kinase activity in thesecells may rely more on winning a war of attrition ratherthan a quick victory, and may even warrant considerationof an intermittent and/or combination approach to BCR-ABL–targeted therapy. Carefully designed clinical studieswill be required to determine the most effective strategy topharmacologically eradicate all CML progenitors.
The Kinetics of CML Blast Crisis in thePre- and Post-imatinib EraIdeally CML blastic phase can be prevented with BCR-ABL inhibition, stem cell transplantation or other means.For those patients who progress despite such maneuvers,the establishment of an early warning system for CML pro-gression could allow initiation of more aggressive or alter-native therapies at a stage where interventions have theoptimal chance of being clinically meaningful. Because ofthe well-established cure rate of allogeneic transplantationin CML, patients in the appropriate age range should beHLA typed at diagnosis so that the options for related orunrelated stem cell transplantation are known early on. Theprincipal fear of most CML caregivers is that patients willprogress to blast crisis too rapidly to allow sufficient timefor stem cell transplantation or other investigative strate-gies to be implemented. To determine the frequency of rapidprogression to CML blast crisis, investigators at MD Ander-son retrospectively analyzed 1093 CML patients who hadreceived a variety of non-transplant treatments (only about10% had received imatinib) and found that 17% had de-veloped blast crisis during the course of study.53 Of pa-tients with blast crisis, one-quarter had experienced sud-den onset, defined as the development of CML in blasticphase within 3 months of a documented complete hemato-logic response. Interestingly, the survival of patients withsudden-onset blast crisis was slightly better than thosewhose blastic phase was more gradual in onset, perhapsbecause lymphoid blast crisis (which carried a more favor-able prognosis) was three times more common in patientswith sudden-onset blastic phase. Fifty-seven percent ofsudden-onset patients were able to proceed to transplanta-tion, but only one quarter of the transplanted patientsachieved durable disease-free survival. With the availabil-ity of more sensitive molecular monitoring techniques, itis likely our definition of rapid-onset blast crisis maychange, but thus far the prognosis of blast crisis appearsominous independent of its rate of onset, at least in the pre-imatinib era.
Because most de novo imatinib-treated CML patientsachieve a complete cytogenetic response,22 quantitativeassessment of BCR-ABL transcript levels has become a sen-sitive and clinically useful tool in CML management. Al-though patients may abruptly lose their response toimatinib,54,55 there is no evidence that imatinib-treated pa-tients progress to blastic phase more rapidly than thosetreated with other modalities, including bone marrow trans-plantation,56 but formal comparative studies are lacking.Nonetheless, regular monitoring of imatinib-treated CMLpatients will maximize the opportunity for implementingchanges in therapy. A recent study found that a greater thantwofold rise in BCR-ABL transcript levels identified pa-tients at high risk for harboring imatinib-resistant BCR/ABL mutations.57 In another study of 103 CML patientswho had achieved a complete cytogenetic response withimatinib (two-thirds had previously received interferon-

Hematology 2005 191
α), 26 suffered cytogenetic relapse at 48 months that waspresaged by increasing BCR-ABL transcript levels.58 Fourof the 26 patients progressed to accelerated or blast crisisduring the study period. In contrast, patients who achieveundetectable BCR-ABL transcript levels or major molecu-lar responses with imatinib appear at quite low risk for pro-gression to blastic phase.59
Therapeutic Options for Patients Developing/Evolving into CML Blast CrisisHistorically, therapy for patients with CML in blastic phasehas been disappointing because response rates have beenfar lower than those achieved with standard induction regi-mens for de novo acute myelogenous leukemia (AML) oracute lymphoblastic leukemia (ALL). The introduction ofimatinib led to improved hematologic response rates inblastic phase CML (52%-70%), including some completehematologic and major cytogenetic responses, leading to a
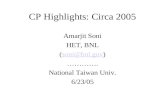
median survival of 7-10 months.60,61 The relatively favor-able results of imatinib in blast crisis CML represented asignificant breakthrough. Imatinib allowed more durabledisease control with less toxicity than traditional chemo-therapeutic regimens and provided some patients a bridgeto stem cell transplantation. However, management of blastcrisis CML in the present and near future may not be muchmore favorable than in the pre-imatinib era because almostall patients will have progressed to this stage despiteimatinib. Thus, the establishment of treatment algorithmsfor patients with CML blast crisis is truly a work in progress(Figure 2).
In patients progressing to blastic phase while onimatinib, it is reasonable to discontinue imatinib while al-ternative treatment plans are being formulated. In somecases, improvements in molecular markers or clinical sta-tus have been observed after cessation of imatinib.62,63 Incontrast, CML blast crisis associated with specific BCR/ABL mutations might temporarily respond to imatinib doseescalation, providing time to pursue additional therapeu-tic options.63 The initial choice of therapy for CML in blas-tic phase may depend in part on the kinetics of onset andthe clinical status of the patient. Although it is highly de-sirable to enroll such patients on clinical trials, some mayrequire traditional chemotherapy to allow time to assesstrial eligibility. The recent availability of the novel ABLtyrosine kinase inhibitors AMN107 and dasatinib (BMS-354825) for clinical study broadens the options for pa-tients developing blastic transformation on imatinib.24,25,64
It is anticipated that these agents will be most effective inpatients whose blast crisis is driven by imatinib-resistantBCR-ABL mutants or increased levels of BCR-ABL, whichmay comprise 30%-40% of cases.65 However, dasatinib alsohas activity against SRC family members, which have re-cently been implicated in imatinib-resistant CML.18
Whether these novel ABL tyrosine kinase inhibitors willachieve durable remissions in blastic phase patients is un-known, but updated results of ongoing trials will be avail-able soon. Ideally, choice of therapy for CML blast crisispatients should be based on screening for imatinib-resis-tant BCR/ABL mutations, since dasatinib and AMN107 areactive against most imatinib-resistant BCR/ABL mutants,except for T315I.64 As BCR/ABL mutation screening is notyet widely available, other factors, such as patient stabil-ity, the presence of clonal evolution, and other clinicalfeatures must be considered when developing treatmentplans.
Regarding more traditional chemotherapeutic agents,high-dose Ara-C–based regimens have often been used forthe treatment of myeloid/mixed/undifferentiated blast cri-sis, which in the pre-imatinib era had a worse prognosisthan the lymphoid form.11 Complete remission rates haveranged from 20% to 30%.66 Thus far, no high-intensity che-motherapy regimen has shown clear superiority, and dura-bility has been poor, with median survivals of only a fewmonths. Single agents are generally ineffective, although
Figure 2. A general treatment algorithm for CML blastcrisis occurring during imatinib therapy. Options includeclinical trials studying alternate ABL tyrosine kinase inhibitors(TKI) or other novel agents, more traditional chemotherapeuticregimens tailored to the lineage of acute leukemictransformation, and/or allogeneic stem cell transplantation.Some potential chemotherapeutic regimens include HIDAC(high-dose Ara-C); FLAG-Ida (fludarabine, Ara-C, G-CSF,idarubicin) with or without gemtuzumab ozogamicin (GO); APO(adriamycin, prednisone, vincristine)-like regimens; or Hyper-CVAD (hyperfractionated cytoxan, vincristine, adriamycin,decadron). Because of the limited penetration of imatinib into thecentral nervous system, the risk of concomitant leukemicmeningitis should be strongly considered, particularly inlymphoid blast crisis. (As discussed in the text, some patientswith BCR-ABL mutations might respond temporarily to imatinibdose escalation.)

192 American Society of Hematology
in one study high- to intermediate-dose decitabine hadactivity similar to more intensive regimens.67 Recently, theFLAG-Ida regimen (fludarabine, Ara-C, granulocyte colony-stimulating factor [G-CSF], idarubicin), with or withoutgemtuzumab ozogamicin,68 has shown encouraging activ-ity in CML in myeloid blast crisis.55 Although active inearly-stage disease, interferon-α–mediated responses aretoo gradual to be effective alone in blastic phase disease.For CML in lymphoid blastic phase, ALL-like inductionregimens have been most commonly used, including thehyper-CVAD regimen.69 Because the response rate and du-rability of most traditional salvage chemotherapy regimenshave been disappointing, a variety of new agents are beinginvestigated for activity in CML blast crisis. They includeinhibitors of the mammalian target of rapamycin (MTOR)pathway; anti-vascular endothelial growth factor (VEGF)–based agents; histone deacetylase inhibitors; and othernovel small molecule inhibitors.66 The proportion of CMLpatients progressing to blastic phase is still relatively small,so further studies will be required to determine which agentsshow the most activity. Given the molecular heterogeneityof blastic phase CML, it is likely that combinations of noveltargeted agents, or targeted agents plus traditional chemo-therapeutic agents, will be required for maximum effect.Because imatinib penetrates poorly into the cerebrospinalfluid,70-72 evaluation or prophylactic treatment of the cen-tral nervous system (CNS) should be strongly consideredwhile treatment plans are being formulated, particularly inlymphoid or mixed lineage blast crisis.
Because it is the only established curative modality,allogeneic bone marrow transplantation remains the ulti-mate salvage therapy for patients with imatinib-resistantCML. Long-term disease-free survival/cure rates range from50% to 70% in patients in early chronic phase, but out-comes decline with advancing disease stage, nadiring atabout 10% for patients transplanted while still in blast cri-sis.73,74 Outcome is somewhat better for CML blast crisispatients transplanted after achieving a second chronic phasewith salvage therapy. With the availability of imatinib, fewerCML patients are being transplanted in the early stages oftheir disease, suggesting future challenges for stem celltransplantation. Perhaps further advances in targeted anti-CML drugs and non-myeloablative transplantation willcounterbalance the risks inherent in transplanting olderCML patients with more advanced disease. Unfortunately,only about one-third of CML patients have a suitable HLA-compatible donor and are within an appropriate age range,making allogeneic transplantation unavailable to most blastcrisis patients. For these patients, autologous stem cell trans-plant might be considered, but advances in purging CMLprogenitors from both patient and autograft will be re-quired. Effective autologous stem cell transplant strategiesmay also benefit from the availability of cryopreservedautologous product obtained during maximal molecularresponse, but this procedure is not in routine practice andmay not be covered by third-party payers.
In summary, the last 5 years have seen important ad-vances for the treatment of early-stage CML, but improve-ment in the care of blastic phase CML has been more mod-est. New ABL tyrosine kinase inhibitors will broaden theoptions for patients with CML in blast crisis, particularlythose with leukemia still highly dependent on BCR-ABL.However, the molecular heterogeneity of blastic phase CMLmay limit the durability of treatment regimens based solelyon ABL-targeted therapy. Allogeneic stem cell transplan-tation remains an important option for some patients butwill be most successful when carefully integrated into asensitive and rigorous monitoring plan based on validatedmolecular markers of CML progression. The limited num-ber of patients with CML eligible for allogeneic transplan-tation underscores the importance of further research toimprove allogeneic and autologous transplant technolo-gies and to identify the mechanisms by which CML stemcells evade imatinib-mediated cytotoxicity.
References1. Martin PJ, Najfeld V, Hansen JA, Penfold GK, Jacobson RJ,
Fialkow PJ. Involvement of the B-lymphoid system inchronic myelogenous leukaemia. Nature. 1980;287:49-50.
2. Salloukh HF, Laneuville P. Increase in mutant frequencies inmice expressing the BCR-ABL activated tyrosine kinase.Leukemia. 2000;14:1401-1404.
3. Canitrot Y, Lautier D, Laurent G, et al. Mutator phenotype ofBCR-ABL transfected Ba/F3 cell lines and its associationwith enhanced expression of DNA polymerase beta.Oncogene. 1999;18:2676-2680.
4. Brummendorf TH, Holyoake TL, Rufer N, et al. Prognosticimplications of differences in telomere length betweennormal and malignant cells from patients with chronicmyeloid leukemia measured by flow cytometry. Blood.2000;95:1883-1890.
5. Sattler M, Verma S, Shrikhande G, et al. The BCR/ABLtyrosine kinase induces production of reactive oxygenspecies in hematopoietic cells. J Biol Chem.2000;275:24273-24278.
6. Canitrot Y, Falinski R, Louat T, et al. p210 BCR/ABL kinaseregulates nucleotide excision repair (NER) and resistance toUV radiation. Blood. 2003;102:2632-2637.
7. Deutsch E, Jarrousse S, Buet D, et al. Down-regulation ofBRCA1 in BCR-ABL-expressing hematopoietic cells. Blood.2003;101:4583-4588.
8. Deutsch E, Dugray A, AbdulKarim B, et al. BCR-ABL down-regulates the DNA repair protein DNA-PKcs. Blood.2001;97:2084-2090.
9. Dierov J, Dierova R, Carroll M. BCR/ABL translocates to thenucleus and disrupts an ATR-dependent intra-S phasecheckpoint. Cancer Cell. 2004;5:275-285.
10. Marktel S, Marin D, Foot N, et al. Chronic myeloid leukemiain chronic phase responding to imatinib: the occurrence ofadditional cytogenetic abnormalities predicts diseaseprogression. Haematologica. 2003;88:260-267.
11. Kantarjian HM, Keating MJ, Talpaz M, et al. Chronicmyelogenous leukemia in blast crisis. Analysis of 242patients. Am J Med. 1987;83:445-454.
12. Ahuja H, Bar-Eli M, Advani SH, Benchimol S, Cline MJ.Alterations in the p53 gene and the clonal evolution of theblast crisis of chronic myelocytic leukemia. Proc Natl AcadSci U S A. 1989;86:6783-6787.
13. Sill H, Goldman JM, Cross NC. Homozygous deletions ofthe p16 tumor-suppressor gene are associated with

Hematology 2005 193
lymphoid transformation of chronic myeloid leukemia. Blood.1995;85:2013-2016.
14. Sattler M, Griffin JD. Molecular mechanisms of transformationby the BCR-ABL oncogene. Semin Hematol. 2003;40:4-10.
15. Melo JV, Deininger MW. Biology of chronic myelogenousleukemia—signaling pathways of initiation and transforma-tion. Hematol Oncol Clin North Am. 2004;18:545-568, vii-viii.
16. Van Etten RA. Mechanisms of transformation by the BCR-ABL oncogene: new perspectives in the post-imatinib era.Leuk Res. 2004;28 Suppl 1:21-28.
17. Calabretta B, Perrotti D. The biology of CML blast crisis.Blood. 2004;103:4010-4022.
18. Donato NJ, Wu JY, Stapley J, et al. BCR-ABL independenceand LYN kinase overexpression in chronic myelogenousleukemia cells selected for resistance to STI571. Blood.2003;101:690-698.
19. Klucher KM, Lopez DV, Daley GQ. Secondary mutationmaintains the transformed state in BaF3 cells with inducibleBCR/ABL expression. Blood. 1998;91:3927-3934.
20. Bhatia R, Holtz M, Niu N, et al. Persistence of malignanthematopoietic progenitors in chronic myelogenous leukemiapatients in complete cytogenetic remission following imatinibmesylate treatment. Blood. 2003;101:4701-4707.
21. Lugo TG, Pendergast A, Muller AJ, Witte ON. Tyrosinekinase activity and transformation potency of bcr-abloncogene products. Science. 1990;247:1079-1082.
22. O’Brien SG, Guilhot F, Larson RA, et al. Imatinib comparedwith interferon and low-dose cytarabine for newly diagnosedchronic-phase chronic myeloid leukemia. N Engl J Med.2003;348:994-1004.
23. Kantarjian H, Talpaz M, O’Brien S, et al. High-dose imatinibmesylate therapy in newly diagnosed Philadelphia chromo-some-positive chronic phase chronic myeloid leukemia.Blood. 2004;103:2873-2878.
24. Shah NP, Tran C, Lee FY, Chen P, Norris D, Sawyers CL.Overriding imatinib resistance with a novel ABL kinaseinhibitor. Science. 2004;305:399-401.
25. Weisberg E, Manley PW, Breitenstein W, et al. Characteriza-tion of AMN107, a selective inhibitor of native and mutantBcr-Abl. Cancer Cell. 2005;7:129-141.
26. Soverini S, Martinelli G, Rosti G, et al. ABL mutations in latechronic phase chronic myeloid leukemia patients with up-front cytogenetic resistance to imatinib are associated with agreater likelihood of progression to blast crisis and shortersurvival: a study by the GIMEMA Working Party on ChronicMyeloid Leukemia. J Clin Oncol. 2005;23:4100-4109
27. Willis S, Lange T, Demehri S, et al. High sensitivity detectionof BCR-ABL kinase domain mutations in imatinib-naivepatients: correlation with clonal cytogenetic evolution but noresponse to therapy. Blood. 2005;106:2128-2137
28. Branford S, Rudzki Z, Walsh S, et al. Detection of BCR-ABLmutations in patients with CML treated with imatinib isvirtually always accompanied by clinical resistance, andmutations in the ATP phosphate-binding loop (P-loop) areassociated with a poor prognosis. Blood. 2003;102:276-283.
29. Roche-Lestienne C, Lai JL, Darre S, Facon T, PreudhommeC. A mutation conferring resistance to imatinib at the time ofdiagnosis of chronic myelogenous leukemia. N Engl J Med.2003;348:2265-2266.
30. Pardal R, Clarke MF, Morrison SJ. Applying the principles ofstem-cell biology to cancer. Nat Rev Cancer. 2003;3:895-902.
31. Huntly BJ, Gilliland DG. Leukaemia stem cells and theevolution of cancer-stem-cell research. Nat Rev Cancer.2005;5:311-321.
32. Elrick LJ, Jorgensen HG, Mountford JC, Holyoake TL.Punish the parent not the progeny. Blood. 2005;105:1862-1866.
33. Gambacorti-Passerini C, Barni R, le Coutre P, et al. Role ofalpha1 acid glycoprotein in the in vivo resistance of humanBCR- ABL(+) leukemic cells to the abl inhibitor STI571. J
Natl Cancer Inst. 2000;92:1641-1650.34. Gambacorti-Passerini C, Zucchetti M, Russo D, et al. Alpha1
acid glycoprotein binds to imatinib (STI571) and substantiallyalters its pharmacokinetics in chronic myeloid leukemiapatients. Clin Cancer Res. 2003;9:625-632.
35. Widmer N, Colombo S, Buclin T, Decosterd LA. Functionalconsequence of MDR1 expression on imatinib intracellularconcentrations. Blood. 2003;102:1142.
36. Hegedus T, Orfi L, Seprodi A, Varadi A, Sarkadi B, Keri G.Interaction of tyrosine kinase inhibitors with the humanmultidrug transporter proteins, MDR1 and MRP1. BiochimBiophys Acta. 2002;1587:318-325.
37. Dai H, Marbach P, Lemaire M, Hayes M, Elmquist WF.Distribution of STI-571 to the brain is limited by P-glycopro-tein-mediated efflux. J Pharmacol Exp Ther. 2003;304:1085-1092.
38. Mahon FX, Belloc F, Lagarde V, et al. MDR1 geneoverexpression confers resistance to imatinib mesylate inleukemia cell line models. Blood. 2003;101:2368-2373.
39. Ozvegy-Laczka C, Hegedus T, Varady G, et al. High-affinityinteraction of tyrosine kinase inhibitors with the ABCG2multidrug transporter. Mol Pharmacol. 2004;65:1485-1495.
40. Burger H, van Tol H, Boersma AW, et al. Imatinib mesylate(STI571) is a substrate for the breast cancer resistanceprotein (BCRP)/ABCG2 drug pump. Blood. 2004;104:2940-2942.
41. Scharenberg CW, Harkey MA, Torok-Storb B. The ABCG2transporter is an efficient Hoechst 33342 efflux pump and ispreferentially expressed by immature human hematopoieticprogenitors. Blood. 2002;99:507-512.
42. Thomas J, Wang L, Clark RE, Pirmohamed M. Activetransport of imatinib into and out of cells: implications fordrug resistance. Blood. 2004;104:3739-3745.
43. Holtz MS, Slovak ML, Zhang F, Sawyers CL, Forman SJ,Bhatia R. Imatinib mesylate (STI571) inhibits growth ofprimitive malignant progenitors in chronic myelogenousleukemia through reversal of abnormally increasedproliferation. Blood. 2002;99:3792-3800.
44. Graham SM, Jorgensen HG, Allan E, et al. Primitive,quiescent, Philadelphia-positive stem cells from patients withchronic myeloid leukemia are insensitive to STI571 in vitro.Blood. 2002;99:319-325.
45. Talpaz M, Estrov Z, Kantarjian H, Ku S, Foteh A, KurzrockR. Persistence of dormant leukemic progenitors duringinterferon-induced remission in chronic myelogenousleukemia. Analysis by polymerase chain reaction ofindividual colonies. J Clin Invest. 1994;94:1383-1389.
46. Chu S, Holtz M, Gupta M, Bhatia R. BCR/ABL kinaseinhibition by imatinib mesylate enhances MAP kinase activityin chronic myelogenous leukemia CD34+ cells. Blood.2004;103:3167-3174.
47. Oda T, Heaney C, Hagopian JR, Okuda K, Griffin JD,Druker BJ. Crkl is the major tyrosine-phosphorylated proteinin neutrophils from patients with chronic myelogenousleukemia. J Biol Chem. 1994;269:22925-22928.
48. Holyoake T, Jiang X, Eaves C, Eaves A. Isolation of a highlyquiescent subpopulation of primitive leukemic cells inchronic myeloid leukemia. Blood. 1999;94:2056-2064.
49. Bueno-da-Silva AE, Brumatti G, Russo FO, Green DR,Amarante-Mendes GP. Bcr-Abl-mediated resistance toapoptosis is independent of constant tyrosine-kinaseactivity. Cell Death Differ. 2003;10:592-598.
50. Ramaraj P, Singh H, Niu N, et al. Effect of mutationalinactivation of tyrosine kinase activity on BCR/ABL-inducedabnormalities in cell growth and adhesion in humanhematopoietic progenitors. Cancer Res. 2004;64:5322-5331.
51. Heinrich MC, Griffith DJ, Druker BJ, Wait CL, Ott KA, ZiglerAJ. Inhibition of c-kit receptor tyrosine kinase activity by STI571, a selective tyrosine kinase inhibitor. Blood.2000;96:925-932.

194 American Society of Hematology
52. Wolff NC, Veach DR, Tong WP, Bornmann WG, Clarkson B,Ilaria RL, Jr. PD166326, a novel tyrosine kinase inhibitor, hasgreater antileukemic activity than imatinib mesylate in amurine model of chronic myeloid leukemia. Blood.2005;105:3995-4003.
53. Kantarjian H, O’Brien S, Cortes J, et al. Sudden onset of theblastic phase of chronic myelogenous leukemia: patternsand implications. Cancer. 2003;98:81-85.
54. Avery S, Nadal E, Marin D, et al. Lymphoid transformation ina CML patient in complete cytogenetic remission followingtreatment with imatinib. Leuk Res. 2004;28 Suppl 1:S75-77.
55. Alimena G, Breccia M, Mancini M, et al. Biclonal blast crisiswith a mutated ABL catalytic domain in a Ph, del (9q)-positive CML patient responsive to imatinib: drug resistanceshould be monitored in all patients irrespective of responsestatus. Leukemia. 2005;19:287-289.
56. Cullis JO, Marks DI, Schwarer AP, et al. Relapse into blastcrisis following bone marrow transplantation for chronicphase chronic myeloid leukaemia: a report of five cases. BrJ Haematol. 1992;81:378-382.
57. Branford S, Rudzki Z, Parkinson I, et al. Real-time quantita-tive PCR analysis can be used as a primary screen toidentify patients with CML treated with imatinib who haveBCR-ABL kinase domain mutations. Blood. 2004;104:2926-2932.
58. Marin D, Kaeda J, Szydlo R, et al. Monitoring patients incomplete cytogenetic remission after treatment of CML inchronic phase with imatinib: patterns of residual leukaemiaand prognostic factors for cytogenetic relapse. Leukemia.2005;19:507-512.
59. Hughes TP, Kaeda J, Branford S, et al. Frequency of majormolecular responses to imatinib or interferon alfa pluscytarabine in newly diagnosed chronic myeloid leukemia. NEngl J Med. 2003;349:1423-1432.
60. Sawyers CL, Hochhaus A, Feldman E, et al. Imatinibinduces hematologic and cytogenetic responses in patientswith chronic myelogenous leukemia in myeloid blast crisis:results of a phase II study. Blood. 2002;99:3530-3539.
61. Kantarjian HM, Cortes J, O’Brien S, et al. Imatinib mesylate(STI571) therapy for Philadelphia chromosome-positivechronic myelogenous leukemia in blast phase. Blood.2002;99:3547-3553.
62. Gorre ME, Mohammed M, Ellwood K, et al. Clinical resis-tance to STI-571 cancer therapy caused by BCR-ABL genemutation or amplification. Science. 2001;293:876-880.
63. Liu NS, O’Brien S. Spontaneous reversion from blast tochronic phase after withdrawal of imatinib mesylate in apatient with chronic myelogenous leukemia. Leuk Lym-phoma. 2002;43:2413-2415.
64. O’Hare T, Walters DK, Stoffregen EP, et al. In vitro activity ofBcr-Abl inhibitors AMN107 and BMS-354825 againstclinically relevant imatinib-resistant Abl kinase domainmutants. Cancer Res. 2005;65:4500-4505.
65. Hochhaus A. Cytogenetic and molecular mechanisms ofresistance to imatinib. Semin Hematol. 2003;40:69-79.
66. Giles FJ, Cortes JE, Kantarjian HM, O’Brien SM. Acceler-ated and blastic phases of chronic myelogenous leukemia.Hematol Oncol Clin North Am. 2004;18:753-774, xii.
67. Sacchi S, Kantarjian HM, O’Brien S, et al. Chronic myelog-enous leukemia in nonlymphoid blastic phase: analysis ofthe results of first salvage therapy with three differenttreatment approaches for 162 patients. Cancer.1999;86:2632-2641.
68. Kell WJ, Burnett AK, Chopra R, et al. A feasibility study ofsimultaneous administration of gemtuzumab ozogamicin withintensive chemotherapy in induction and consolidation inyounger patients with acute myeloid leukemia. Blood.2003;102:4277-4283.
69. Kantarjian HM, O’Brien S, Smith TL, et al. Results oftreatment with hyper-CVAD, a dose-intensive regimen, inadult acute lymphocytic leukemia. J Clin Oncol.2000;18:547-561.
70. Takayama N, Sato N, O’Brien SG, Ikeda Y, Okamoto S.Imatinib mesylate has limited activity against the centralnervous system involvement of Philadelphia chromosome-positive acute lymphoblastic leukaemia due to poorpenetration into cerebrospinal fluid. Br J Haematol.2002;119:106-108.
71. Wolff NC, Richardson JA, Egorin M, Ilaria RL, Jr. The CNS isa sanctuary for leukemic cells in mice receiving imatinibmesylate for Bcr/Abl-induced leukemia. Blood.2003;101:5010-5013.
72. Leis JF, Stepan DE, Curtin PT, et al. Central nervous systemfailure in patients with chronic myelogenous leukemialymphoid blast crisis and Philadelphia chromosome positiveacute lymphoblastic leukemia treated with imatinib (STI-571).Leuk Lymphoma. 2004;45:695-698.
73. Hansen JA, Gooley TA, Martin PJ, et al. Bone marrowtransplants from unrelated donors for patients with chronicmyeloid leukemia. N Engl J Med. 1998;338:962-968.
74. Weisdorf DJ, Anasetti C, Antin JH, et al. Allogeneic bonemarrow transplantation for chronic myelogenous leukemia:comparative analysis of unrelated versus matched siblingdonor transplantation. Blood. 2002;99:1971-1977.