o αντιαιµοπεταλιακή ΔΑΜΑ πέραν των 12 µηνών · Events between...
32
37 o Πανελλήνιο Καρδιολογικό Συνέδριο 2016 Διπλή αντιαιμοπεταλιακή αγωγή (ΔΑΜΑ) πέραν των 12 μηνών DAPT beyond 12 months Γεώργιος Χάχαλης, Αναπληρωτής Καθηγητής Καρδιολογίας Πανεπιστημίου Πατρών Διευθυντής Καρδιολογικής Κλινικής George Hahalis, Assoc. Professor, University of Patras, Director
Transcript of o αντιαιµοπεταλιακή ΔΑΜΑ πέραν των 12 µηνών · Events between...

37o Πανελλήνιο Καρδιολογικό Συνέδριο 2016
Διπλή αντιαιµοπεταλιακή αγωγή (ΔΑΜΑ) πέραν των
12 µηνών DAPT beyond 12 months
Γεώργιος Χάχαλης,
Αναπληρωτής Καθηγητής Καρδιολογίας Πανεπιστηµίου Πατρών
Διευθυντής Καρδιολογικής Κλινικής
George Hahalis, Assoc. Professor, University of Patras, Director

Σύγκρουση συµφερόντων του οµιλητή Γεωργίου Χάχαλη:
Αµοιβές για οµιλίες από τις εταιρίες Behringer Ingelheim, AstraZeneka, MSD, Pfizer, Servier
George Hahalis disclosures:
Speaker fees from Behringer Ingelheim, AstraZeneka, MSD, Pfizer, Servier
37o Πανελλήνιο Καρδιολογικό Συνέδριο 2016

2001 CURE-PCI: Clopidogrel in PCI after NSTACS
N=2658 patients; 1313 received clopidogrel and 1345 placebo. PCI performed during the initial hospital stay in 1730, and the remaining 928 after discharge. Patients were pretreated with aspirin and the study drug for a median of 6 days before PCI during the initial hospital admission, and a median of 10 days overall.
Mehta SR, et al. Lancet 2001; 358: 527–33
31% (Death,
MI)
PCI30
d.po
st
PCI
R
RR= 0·69 (0·54–0·87)
Interpretation. “In patients with ACS receiving aspirin, a strategy of clopidogrel pretreatment followed by long- term
therapy is beneficial in reducing MACEs,compared with placebo’

“Stent Thrombosis Late After Implantation of First-Generation Drug-Eluting Stents A Cause for Concern”
Edoardo Camenzind, MD; P. Gabriel Steg, MD; William Wijns, MD
TABLE 5. Calculated Death and All-Cause Mortality in the Cypher ( S ) Versus BMS ( C ) Trial Programs Up to Latest Available Follow-Up in Intention-to-Treat Patients According to Data on File at Cordis
S (N=878) C (N=870) Δ S-C Events, n Events, n Δ Events, n (% of Pts) (% of Pts) (Risk Difference, %)
Death–all 41 (4.67) 29 (3.33) 12 (1.34)
Death–calculated 81 (9.23) 74 (8.51) 7 (0.72)
Circulation 2007;115:1440-1455

ΜΙ
Stroke
Symptomatic
No MI
No Stroke
AsymptomaticPinteraction: 0.045(n=3284)
(n=12153)
2006 CHARISMA: ΔΑΜΑ εν. Ασπιρίνης στην ΚΑ πρόληψη Πρωτογενές Καταληκτικό σηµείο: ΚΑ θάνατος, ΕΜ, ΑΕΕ
Bhatt DL, et al. NEJM 2006;354:1706 - Berger PB, et al Circulation 2010;121:2575
“ Bhatt DL, et al JACC 2007;49:1982-8
CHARISMA: Patients with history of MI
CHARISMA : Clopidogrel vs. placebo All-cause mortality Major bleeding Asymptomatic 5.4% vs. 3.8%; P=0.04 2.0% vs. 1.2%; P=0.07
Symptomatic P=NS P=NS Excess bleeding did not explain the increase in mortality associated with clopidogrel in patients with risk factors alone”

Bhatt DL, et al JAMA. 2010;304(12):1350-1357
2010 REACH REGISTRY (Ν=45227) Τετραετής έκβαση (θάνατος, ΕΜ, ΑΕΕ) ασθενών µε
προηγούµενο ισχαιµικό επεισόδιο ή σταθερή νόσο ή ΠΚ
MACE at 4 years: symptomatic vs. with RF’s only

20 Degeration DES are safer- Bleeding is ominous => 2010-2016 Trials comparing Shorter vs. Longer DAPT post PCI

Μελέτη Έτος Αριθµός ασθενών
3-6 µ. >12 µ.
Διάρκεια ΔΑΜΑ 3-6 µήνες
Διάρκεια ΔΑΜΑ
>12 µήνες
ΟΣΣ (%)
2ης γενεάς DES (%)
ISAR-SAFE 2015 1997 2003 6 100% κλοπιδ
12 100% κλοπιδ
40 88 εν. 89
ITALIC
2014
926 924 6 99 % κλοπιδ
24 99% κλοπιδ
23 100 εν. 100
SECURITY 2014 682 717 6 98% κλοπιδ
12 99% κλοπιδ
38 100 εν. 100
OPTIMIZE 2013 1563 1556 3 κλοπιδ
12 κλοπιδ
32 100 εν. 100
RESET 2012 1058 1059 3 100% κλοπιδ
12 100% κλοπιδ
54 100 εν. 68
EXCELLENT 2012 722 721 6 100% κλοπιδ
12 100% κλοπιδ
52 75 εν . 75
Διάρκεια ΔΑΜΑ* µε DES 2ης Γενεάς 6 µελέτες, 12752 ασθενείς, µ.η. 64 ετών, 91.5% PCI µε DES - 39% λόγω ΟΣΣ
Wassef AWA, et al J Inv Cardiol 2016;28:Sept 15* ΔΑΜΑ: Διπλή Αντιαιµοπεταλιακή Αγωγή

Καρδιαγγειακή θνητότητα (CV mortality)
P=ΜΣ
Wassef AWA, et al J Inv Cardiol 2016;28:Sept 15* ΔΑΜΑ: Διπλή Αντιαιµοπεταλιακή Αγωγή
Διάρκεια ΔΑΜΑ* µε DES 2ης Γενεάς
Μείζονες αιµορραγίες (major bleeding)
-36% P=0.01

HR (95% CI) P
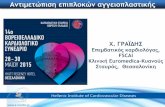
Cardiac death, MI, or ST 1.21 (0.77–1.89) 0.42
Cardiac death 1.25 (0.71–2.22) 0.43
All-cause death 1.14 (0.73–1.79) 0.58
MI 0.89 (0.47–1.67) 0.70
Stroke 0.74 (0.28–1.92) 0.54
Definite/probable ST 1.56 (0.44–5.56) 0.49
Major bleeding 0.30 (0.10–0.91) 0.03
Minor bleeding 0.73 (0.28–1.92) 0.53
All-cause death, MI, stroke, major bleed 0.91 (0.62–1.33) 0.63
Events between DAPT discontinuation and 1 yr (as treated)
Short- vs. Long-Term DAPT After DES PCI An Individual Patient Data Pairwise and Network Meta-Analysis; 4 trials, N=8180 patients included
Palmerini T, et al.JACC 2015;65:1092–102

2016 The NIPPON trial A prospective, multicenter, randomized trial to compare the net clinical benefits (NACCE*) between short DAPT (6 months) and prolonged DAPT (18 months) after
NOBORI stenting (DES with bioabsorbable polymer and abluminal coating)
*NACCE defined as the composite of all-cause death, MI, stroke, or major bleeding

• Open label: all studies
• Underpowered: all studies
• Premature termination of enrollment
• Wide non-inferiority margin
• Not all-comer studies (patients with high risk such as those
with MI < 72 hours, LM disease, or severe LV dysfunction
excluded)- EXCELLENT 2012
Shorter vs. Longer DAPT: Limitations of Previous RCT’s

2014 DAPT µετά DES-PCI (Ν=9961) “Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents”
Κλοπιδογρέλη (65%) ή Πρασουγρέλη (35%) έν. Placebo (µήνας 12 – µην. 30) (ACS=43% , NSTEMI =15.5%, STEMI=10.5%, ΕΕS=47%, PES=27%)
0
1,5
3
4,5
6
ΠΚΣ-1 (θρόµβωση stent) Θάνατος Μείζων αιµορραγία (BARC 3)
0,1
2,62,12
4,3
0,4
Θειενοπυριδίνη Placebo
-71% (P <0.001)
+36% (P =0.05)
-53% (P <0.001)
-29% (P <0.001)
(P <0.001)
(P = ΜΣ)
Mauri L, et al. NEJM 2014;371:2155-66

Yeh J, et al. JACC 2015;65:2211–21
DAPT: Pts With vs. Without Presenting MI: Outcome “Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents”
Πρασουγρέλη ή Κλοπιδογρέλη έναντι Placebo από µήνα 12 µέχρι µήνα 30 µετά DES (43% ΟΣΣ, 65% κλοπιδογρέλη, 47% ΕΕS, 27% PES, 14.5% BMS)
Inte
ract
ion
P=0.
15

Giustino N, et al. JACC 2015;65:1298–310
Short- vs. Long-Term DAPT After DES PCI Ten randomized controlled trials (N=32,135) included

Giustino N, et al. JACC 2015;65:1298–310
Short- vs. Long-Term DAPT After DES PCI Ten randomized controlled trials (N=32,135) included

2015 PEGASUS-ΤΙΜΙ 54 (Ν=21162) ΔΑΜΑ (Τικαγκρελόρη) έν. εικονικού φαρµάκου σε ασθενείς 1-3 χρόνια µετά από ΕΜ*
Διάµεση παρακολούθηση: 33 µήνες - Διάµεσος χρόνος µετά το ΟΕΜ: 1.7 έτη ΠΚΣ-αποτελεσµατικότητα: ΚΑ θάνατος, ΕΜ, ΑΕΕ
Bonaca MP, et al. NEJM, March, 14 DOI: 10.1056/NEJMoa1500857
*Ασθενείς > 50 ετών συν ένα από τα ακόλουθα: •> 65 ετών, •ΣΔ2 υπό αγωγή, •υποτροπή ΟΕΜ, •πολυαγγειακή ΣΝ, ή •ΧΝΑ (κάθαρση κρεατινίνης < 60 ml/min)
ΠΚΣ Θάνατος από ΣΝ ή ΟΕΜ ΟΕΜ Ολική θνητότητα
5,165,25
6,68
9,04
5,154,4
5,59
7,85
Ticagrelor 90Ticagrelor 60Placebo
-15% -16% Tik έναντι Placebo: P=0.008 P=0.04
-19% -16% Tik έναντι Placebo: P =0.004 P=0.01 -19% -16%
Tik έναντι Placebo: P =0.01 P=0.03

2015 PEGASUS-ΤΙΜΙ 54 (Ν=21162) ΔΑΜΑ (Τικαγκρελόρη) έν. εικονικού φαρµάκου - 1-3 χρόνια µετά από ΕΜ (54% STEMI)*
Διάµεση παρακολούθηση: 33 µήνες - Διάµεσος χρόνος µετά το ΟΕΜ: 1.7 έτη ΠΚΣ-ασφάλεια: µείζων αιµορραγία (ΤΙΜΙ) (safety)
Bonaca MP, et al. NEJM 2015, March, 14 DOI: 10.1056/NEJMoa1500857
0
0,75
1,5
2,25
3
Μείζων αιµορραγία Μετάγγιση Ενδοκράνια αιµορραγία
0,47
0,72
1,06
0,56
2,432,6
Ticagrelor 90 Ticagrelor 60 Placebo
+269% +232% Τικ έναντι Placebo: P <0.001 P<0.001
+375% +308% Τικ έναντι Placebo: P <0.004 P<0.01
Αποκλείστηκαν ασθενείς µε: πρόσφατη αιµορραγία, ιστορικό ΑΕΕ και θεραπεία µε αντιπηκτικά p.os.

2015 PEGASUS-ΤΙΜΙ 54 (Ν=21162) ΔΑΜΑ (Τικαγκρελόρη) έν. εικονικού φαρµάκου - 1-3 χρόνια µετά από ΕΜ (54% STEMI)*
Διάµεση παρακολούθηση: 33 µήνες - Διάµεσος χρόνος µετά το ΟΕΜ: 1.7 έτη ΠΚΣ-ασφάλεια: µείζων αιµορραγία (ΤΙΜΙ) (safety)
Bonaca MP, et al. NEJM 2015, March, 14 DOI: 10.1056/NEJMoa1500857
0
0,75
1,5
2,25
3
Μείζων αιµορραγία Μετάγγιση Ενδοκράνια αιµορραγία
0,47
0,72
1,06
0,56
2,432,6
Ticagrelor 90 Ticagrelor 60 Placebo-37% - 41% Placebo έναντι Τικ P <0.001 P<0.001
-27% -32% Placebo έναντι Τικ P <0.004 P<0.01
Αποκλείστηκαν ασθενείς µε: πρόσφατη αιµορραγία, ιστορικό ΑΕΕ και θεραπεία µε αντιπηκτικά p.os.

PEGASUS-ΤΙΜΙ 54 Diabetes (n=6806) vs. No Diabetes (n=14355))
Bhatt D, et al. JACC 2016;67:2732-40

Prevention of Stroke with Ticagrelor in Patients with Prior Myocardial Infarction: Insights from PEGASUS-TIMI 54
14112 patients; median F-U: 33 months
Bonaca MP, et al. Circulation 2016 Sep 20;134(12):861-71.
• Ticagrelor 60 mg over placebo reduced the risk of stroke (HR=0.75; 95% CI 0.57-0.98; P=0.034) due to ischemic stroke RR (HR=0.76; 95% CI, 0.56-1.02)
• Hemorrhagic stroke rates rare and similar
• A meta-analysis (4 placebo-controlled trials*, n=44 816): More intensive antiplatelet therapy in coronary disease patients markedly reduces ischemic stroke (HR=0.66; 95% CI, 0.54-0.81; P=0.0001)
* CHARISMA-MI, TRA2P=TIMI 50, DAPT, PEGASUS-TIMI 54

Bonaca MP, et al. JACC 2016;67:2719–28
PEGASUS-ΤΙΜΙ 54 Patients With vs. No Peripheral Artery Disease
Bonaca MP. Presented at ESC 2016
0 0.5 1.0 1.5 2.0 2.5 3. Έτη παρακολούθησης (years of follow-up)
Οξεία
ισχα
ιµία
κάτ
ω άκρ
ου /
/ περ
ιφ. επ
αναγ
γείω
ση για
ισχα
ιµία
(%)
0
0.
2
0.
4
0
.6
0.8
1
.0
Acute limb ischemia/limb revascularization
HR 0.65 95% CI (0.44-0.95) P=0.026
Placebo
Ticagrelor
Bonaca MP. Presented at ESC 2016

Bonaca MP, et al. EHJ 2016;37:1133–42
PEGASUS-ΤΙΜΙ 54 Timing of P2Y12 Inhibitor Withdrawal from Randomization
“The benefit of ticagrelor for long-term secondary prevention in patients with prior MI and > 1 additional risk factor appeared more marked in patients continuing on or re-starting after only a brief interruption of P2Y12 inhibition, when compared with patients who had proved themselves stable more than 2 years from their MI and off P2Y12 inhibitor therapy for more than a year”
CV death, MI, or stroke after P2Y12 inhibition withdrawal ≤30 days from randomization

2016 Udell JA, et al Meta-analysis of 6* RCTs (Ν=33435) “comparing > 1 year of DAPT with aspirin alone in
high-risk patients with a history of prior MI” *CHARISMA-MI, PRODIGY, ARCTIC-Interruption, DAPT, DES-LATE, PEGASUS-TIMI 54
0
2
4
6
8
KA θάνατος, EM, AEE ΟΕΜ ΑΕΕ
4,01
1,38
0,64
3,52
2,3
6,4
DAPT > 1 y. Aspirin alone
-15% P =0.03
-30% P =0.003
-50% P =0.02
-19% P =0.02
-8% P =0.13
Udell JA, et al. EHJ 2016;37:390-99

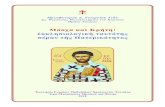
2016 Udell JA, et al Meta-analysis of 6 RCTs (Ν=33435) DAPT >1 year vs. Aspirin alone
0
2
4
6
8
KA θάνατος, EM, AEE ΟΕΜ ΑΕΕ
4,01
1,38
0,64
3,52
2,3
6,4
DAPT > 1 y. Aspirin alone -22% : P=0.001
-15% P =0.03
-50% P =0.02
-19% P =0.02
Udell JA, et al. EHJ 2016;37:390-99
Μείζων αιµορραγία (Major bleeding): +73%

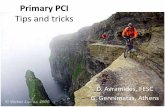
2013 TRILOGY-ACS (Ν=7243, ασθενείς <75 ετών) ΔΑΜΑ (Πρασουγρέλη έν. Κλοπιδογρέλης µετά από ΟΣΣ –
(2/3 ΝSTEMI, 1/3 ασταθής στηθάγχη) - Διάµεση παρακολούθηση: 17µήνες ΠΚΣ: ΚΑ θάνατος, ΕΜ, ΑΕΕ
HR for the time period of <12 vs. > 12 months comparing prasugrel with clopidogrel for the primary efficacy end point were: 0.99 (95% CI, 0.84 -1.16) vs. 0.72 (95% CI, 0.54 -0.97) (Pinteraction=0.07).
ΗR=1.31 (95% CI, 0.81-2.11; P=0.27
HR=0.9
HR=0.72

2012 TRA 2P–TIMI 50 Voraxapar vs. Placebo for 20 Prevention N=26449 pts with history of MI, Stroke or PAD; F-U 30 months
Morrow DA, et al. NEJM 2012_366_1404–1413

Risk comparing strategies of intensive vs. moderate antiplatelet therapy for 20 prevention of MACEs
among stabilized patients >1 y from a qualifying MI
Udell JA, et al. EHJ 2016;37:390-99

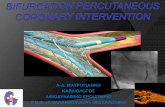
Trial Registration N Inclusion Criteria
Months until Randomization Event-Free and on DAPT
Intervention ControlFollow-up (months) Primary Endpoint Anticipated
CompletionAll with background aspirin unless otherwise stated
OPTIDUAL22 NCT00822536 1798
Patients treated with DES PCI
12Clopidogrel
- 36 additional months Aspirin alone 36 Death, MI, stroke, and major bleeding 09/2014
REDUCE23 NCT02118870 1500
ACS treated with COMBO dual-therapy PCI
0ADP antagonist
- 3 monthsADP antagonist
- 12 months 12 Death, MI, stroke, stent thrombosis, and bleeding 03/2015
ISR-DAPT24 NCT02402491 1000
Patients treated with PCI for in-stent restenosis
0ADP antagonist
- 24 monthsADP antagonist
- 12 months 24 Death, MI, stroke, and stent thrombosis 06/2015
GLOBAL-LEADERS25 NCT01813435 16000
Patients treated with PCI
0
Ticagrelor/aspirin x 1 m →
ticagrelor monotherapy - 24 months
Ticagrelor or clopidogrel - 12 months
24 Death or Q-wave MI 06/2016
SMART DATE26 NCT01701453 3000ACS treated with DES PCI
0Clopidogrel - 6 months
Clopidogrel - 12 months or
longer6-18
Death, spontaneous MI, cerebrovascular event, stent thrombosis and major bleeding
08/2016
NIPPON27 NCT01514227 4598
Patients treated with DES PCI
0Clopidogrel or ticlopidine
- 6 months
Clopidogrel or ticlopidine - 18 months
18 Death, MI, cerebrovascular event, and major bleeding 04/2017
DAPT-STEMI28 NCT01701453 1100
STEMI treated with primary PCI by DES
6 Aspirin alone
Prasugrel or ticagrelor
- 6 additional months
18 Death, MI, stroke, revascularization, and major bleeding 12/2017
SMART-CHOICE29 NCT02079194 5100
Patients treated with DES PCI
3 Clopidogrel aloneADP antagonist - 9 additional
months12 Death, MI, cerebrovascular event,
and major bleeding 02/2018
Ongoing or Unpublished Trials Testing Antiplatelet Strategies that are Enrolling Patients following an Acute Coronary Event
Udell JA, et al. EHJ 2016;37:390-99

ΔΑΜΑ (DAPT) > 12 µήνες (months): σε ποιόν; (for whom?)

Διαβητικοί, καπνιστές,
ιστορικό ΟΕΜ, ΧΝΑ,
πολυαγγειακής ΣΝ, πολυαγγειοπάθειας,
Χαµηλό ΚΕ
Κίνδυνος ενδοκράνιας αιµορραγίας,
Αναιµία, Θροµβοπενία, Πρόσφατη µείζων
αιµορραγία, Αιµορραγική προδιάθεση
Σε αντιπηκτική αγωγή
Ιστορικό θρόµβωσης stent
Πολλαπλά stents, PCI διχασµών
Σε µοναδικό εναποµείναν στεφανιαίο αγγείο
Για την µείωση (to reduce): •Νέων αυτόµατων ΕΜ (re-MI) •ΑΕΕ (strokes) •Κριτικής ισχαιµίας των κάτω άκρων (critical limb ischemia) •ΚΑ θνητότητας (CV mortality) •Χωρίς αύξηση των θανατηφόρων ή των ενδοκράνιων αιµορραγιών (without fatal or intracranial bleeding increase)
ΔΑΜΑ (DAPT) > 12 µήνες (months): σε ποιόν; (for whom?)

Ευχαριστώ για την προσοχή σας…
Thank you for your attention…