![TheOngoingChallengeofHematopoieticStemCell-Based ...downloads.hindawi.com/journals/sci/2011/987980.pdf · Thalassemias are caused by more than 200 mutations ... [27], while in primates](https://static.fdocument.org/doc/165x107/602afc26aeb6bc151050ebdc/theongoingchallengeofhematopoieticstemcell-based-thalassemias-are-caused-by.jpg)
Non-Carbapenem Therapy for Bacteremia Caused by...
16
Non-Carbapenem Therapy for Bacteremia Caused by Extended- Spectrum β-Lactamase-Producing Enterobacteriaceae: When Can We Afford to Bench the Big Three? Manuel Escobar, Pharm.D. PGY2 Infectious Diseases Pharmacy Resident South Texas Veterans Health Care System Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center University of Texas Health Science Center at San Antonio October 4, 2013 Learning Objectives: 1. Understand the epidemiologic importance of limiting carbapenem use 2. Understand the mechanisms and clinical implications of extended-spectrum β-lactamase (ESBL) production in Enterobacteriaceae 3. Describe the in-vitro and human primary literature available for therapy of bacteremia due to ESBL-producing organisms 4. Describe the situations where non-carbapenem agents are an acceptable option for treatment of ESBL bacteremia IMI ERTA MERO Escobar Page 1
-
Upload
nguyennguyet -
Category
Documents
-
view
222 -
download
0
Transcript of Non-Carbapenem Therapy for Bacteremia Caused by...

Non-Carbapenem Therapy for Bacteremia Caused by Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae:
When Can We Afford to Bench the Big Three?
Manuel Escobar, Pharm.D. PGY2 Infectious Diseases Pharmacy Resident
South Texas Veterans Health Care System Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center University of Texas Health Science Center at San Antonio
October 4, 2013
Learning Objectives: 1. Understand the epidemiologic importance of limiting carbapenem use 2. Understand the mechanisms and clinical implications of extended-spectrum β-lactamase
(ESBL) production in Enterobacteriaceae 3. Describe the in-vitro and human primary literature available for therapy of bacteremia due
to ESBL-producing organisms 4. Describe the situations where non-carbapenem agents are an acceptable option for
treatment of ESBL bacteremia
IMI ERTA
MERO
Escobar Page 1
I. CARBAPENEMS: A CRITICAL MEMBER OF OUR ANTIBIOTIC ARMAMENTARIUM
A. The unique nature of carbapenems1 i. Cabapenems are relatively resistant to hydrolysis by most β-lactamases
ii. Regarded as first-line therapy for serious infections caused by Extended Spectrum β-Lactamase (ESBL)-producing organisms
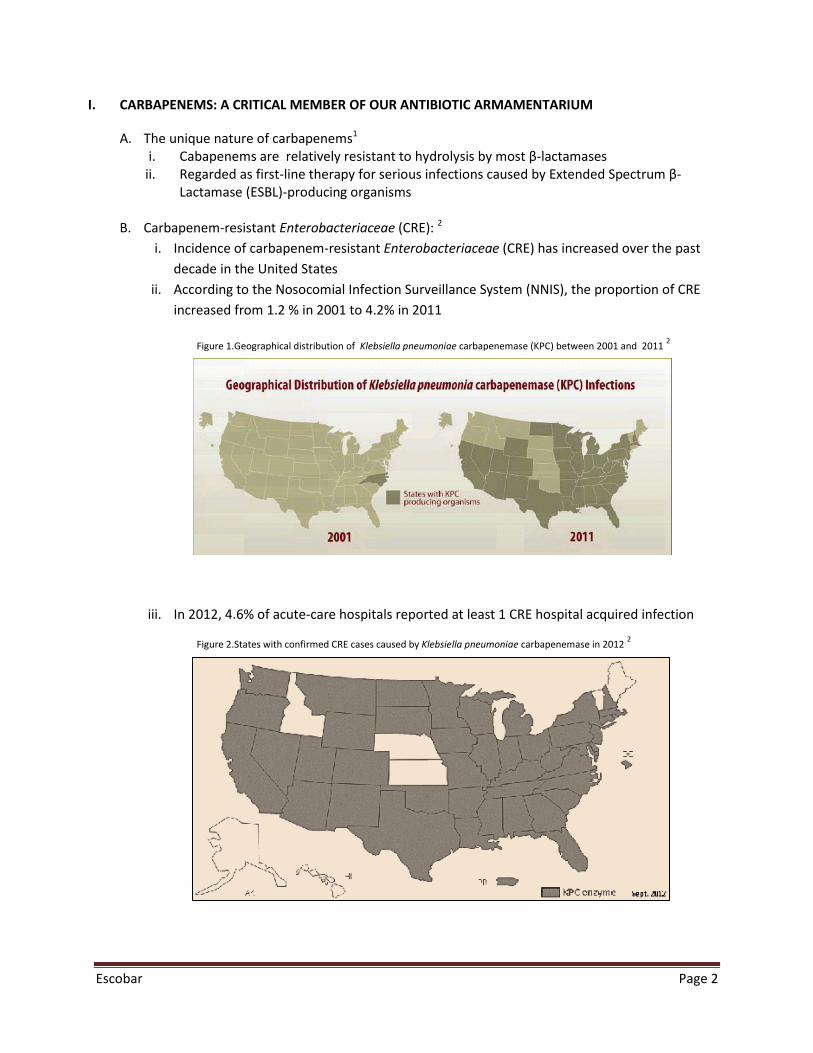
B. Carbapenem-resistant Enterobacteriaceae (CRE): 2
i. Incidence of carbapenem-resistant Enterobacteriaceae (CRE) has increased over the past decade in the United States
ii. According to the Nosocomial Infection Surveillance System (NNIS), the proportion of CRE increased from 1.2 % in 2001 to 4.2% in 2011
iii. In 2012, 4.6% of acute-care hospitals reported at least 1 CRE hospital acquired infection
Figure 2.States with confirmed CRE cases caused by Klebsiella pneumoniae carbapenemase in 2012 2
Figure 1.Geographical distribution of Klebsiella pneumoniae carbapenemase (KPC) between 2001 and 2011 2
Escobar Page 2
C. Clinical Implications of carbapenem resistance in infections caused by Enterobacteriaceae 3-5 i. The presence of β-Lactamases that confer resistance to carbapenems is also associated
with mechanisms of resistance to other antibiotic classes that together result in highly multidrug resistant organisms
ii. Treatment of these infections is difficult given many isolates are also resistant to all β-lactam antibiotics, fluoroquinolones, and aminoglycosides
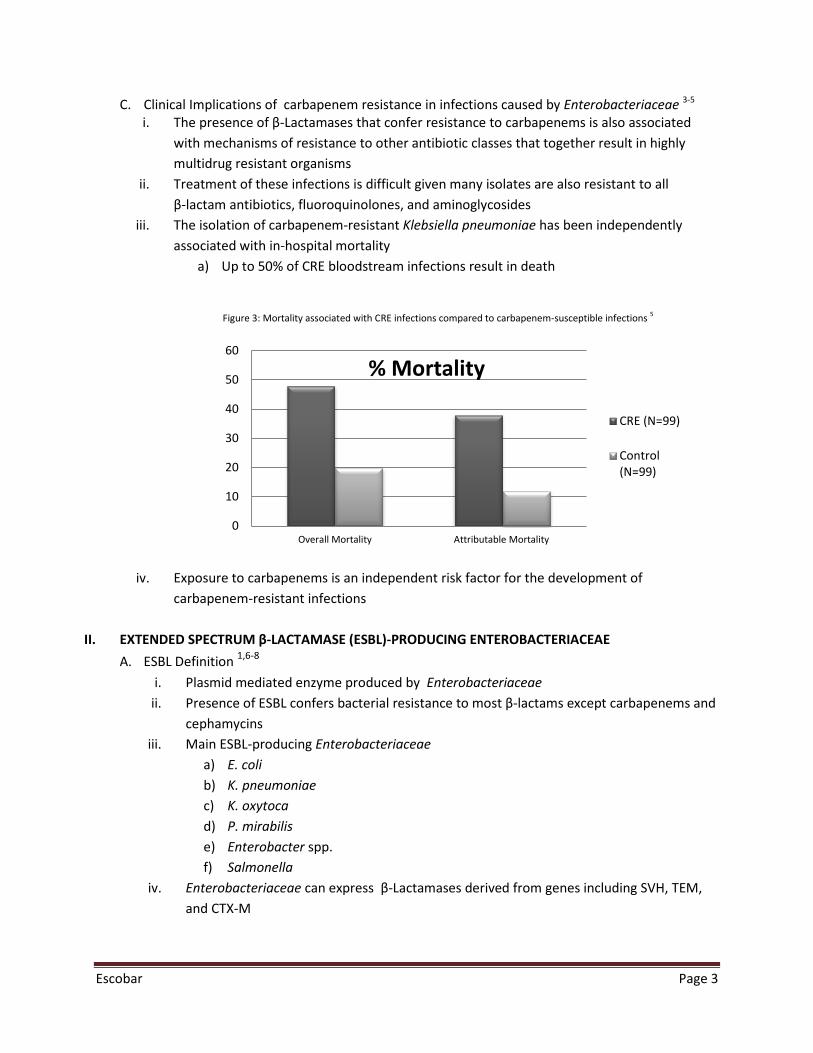
iii. The isolation of carbapenem-resistant Klebsiella pneumoniae has been independently associated with in-hospital mortality
a) Up to 50% of CRE bloodstream infections result in death
iv. Exposure to carbapenems is an independent risk factor for the development of
carbapenem-resistant infections
II. EXTENDED SPECTRUM β-LACTAMASE (ESBL)-PRODUCING ENTEROBACTERIACEAE A. ESBL Definition 1,6-8
i. Plasmid mediated enzyme produced by Enterobacteriaceae ii. Presence of ESBL confers bacterial resistance to most β-lactams except carbapenems and
cephamycins iii. Main ESBL-producing Enterobacteriaceae
a) E. coli b) K. pneumoniae c) K. oxytoca d) P. mirabilis e) Enterobacter spp. f) Salmonella
iv. Enterobacteriaceae can express β-Lactamases derived from genes including SVH, TEM, and CTX-M
0
10
20
30
40
50
60
Overall Mortality Attributable Mortality
% Mortality
CRE (N=99)
Control(N=99)
Figure 3: Mortality associated with CRE infections compared to carbapenem-susceptible infections 5
Escobar Page 3
B. Emergence and epidemiology1 i. The first large outbreak of ESBL-producing organisms was reported in France in 1986
ii. The first reports in the United States occurred in 1988
C. ESBL Diagnosis9 i. ESBL phenotypic confirmatory test takes advantage of the ability of clavulanate to inhibit
growth of ESBL-producing bacteria a) The Clinical and Laboratory Standards Institute (CLSI) recommends the use of
cephalosporins/clavulanate combination disks on isolate growth in Mueller-Hinton agar
b) A difference of ≥5 mm between the zone diameters of the cephalosporin disks and their respective cephalosporins/clavulanate disk is taken to be phenotypic confirmation of ESBL production
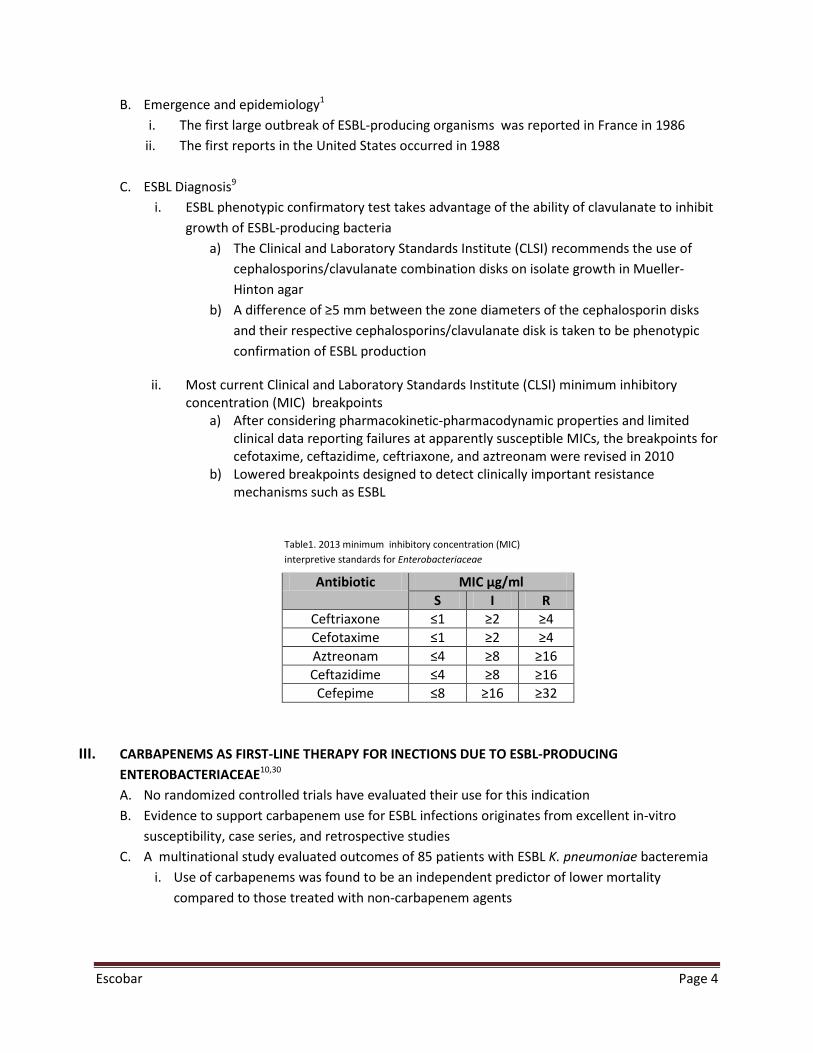
ii. Most current Clinical and Laboratory Standards Institute (CLSI) minimum inhibitory concentration (MIC) breakpoints
a) After considering pharmacokinetic-pharmacodynamic properties and limited clinical data reporting failures at apparently susceptible MICs, the breakpoints for cefotaxime, ceftazidime, ceftriaxone, and aztreonam were revised in 2010
b) Lowered breakpoints designed to detect clinically important resistance mechanisms such as ESBL
Antibiotic MIC µg/ml
S I R Ceftriaxone ≤1 ≥2 ≥4 Cefotaxime ≤1 ≥2 ≥4 Aztreonam ≤4 ≥8 ≥16 Ceftazidime ≤4 ≥8 ≥16
Cefepime ≤8 ≥16 ≥32
III. CARBAPENEMS AS FIRST-LINE THERAPY FOR INECTIONS DUE TO ESBL-PRODUCING ENTEROBACTERIACEAE10,30 A. No randomized controlled trials have evaluated their use for this indication B. Evidence to support carbapenem use for ESBL infections originates from excellent in-vitro
susceptibility, case series, and retrospective studies C. A multinational study evaluated outcomes of 85 patients with ESBL K. pneumoniae bacteremia
i. Use of carbapenems was found to be an independent predictor of lower mortality compared to those treated with non-carbapenem agents
Table1. 2013 minimum inhibitory concentration (MIC) interpretive standards for Enterobacteriaceae
Escobar Page 4
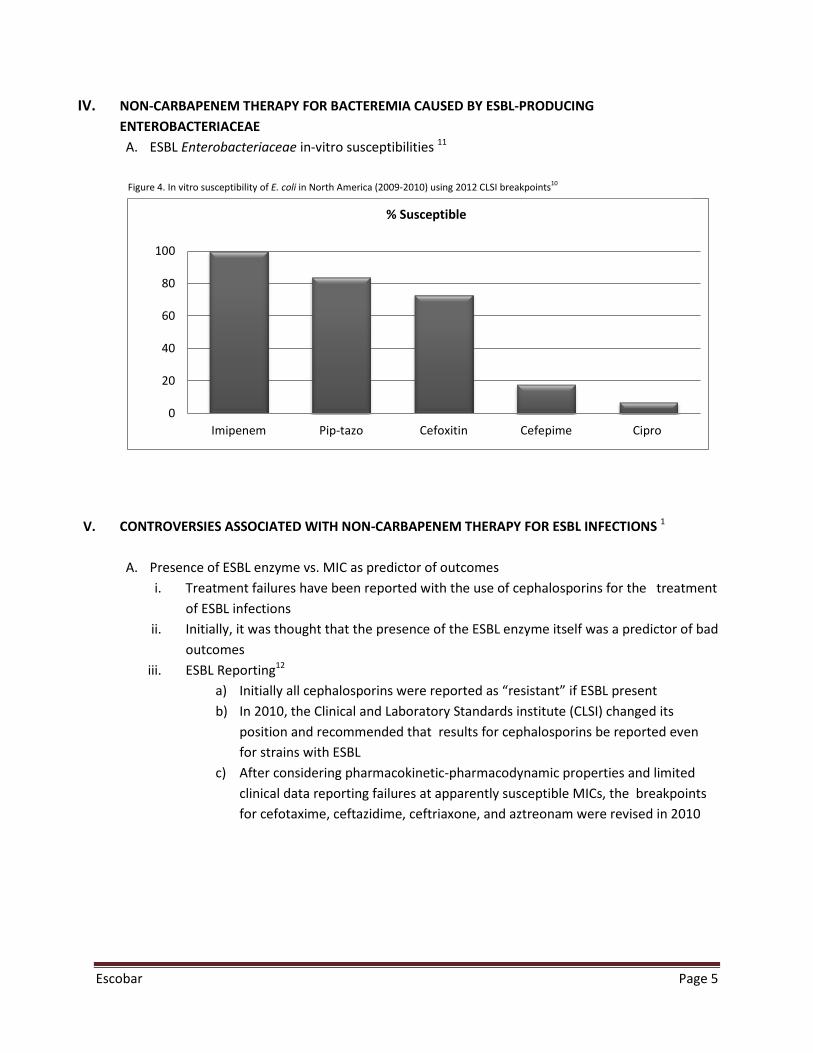
IV. NON-CARBAPENEM THERAPY FOR BACTEREMIA CAUSED BY ESBL-PRODUCING ENTEROBACTERIACEAE A. ESBL Enterobacteriaceae in-vitro susceptibilities 11
V. CONTROVERSIES ASSOCIATED WITH NON-CARBAPENEM THERAPY FOR ESBL INFECTIONS 1
A. Presence of ESBL enzyme vs. MIC as predictor of outcomes i. Treatment failures have been reported with the use of cephalosporins for the treatment
of ESBL infections ii. Initially, it was thought that the presence of the ESBL enzyme itself was a predictor of bad
outcomes iii. ESBL Reporting12
a) Initially all cephalosporins were reported as “resistant” if ESBL present b) In 2010, the Clinical and Laboratory Standards institute (CLSI) changed its
position and recommended that results for cephalosporins be reported even for strains with ESBL
c) After considering pharmacokinetic-pharmacodynamic properties and limited clinical data reporting failures at apparently susceptible MICs, the breakpoints for cefotaxime, ceftazidime, ceftriaxone, and aztreonam were revised in 2010
0
20
40
60
80
100
Imipenem Pip-tazo Cefoxitin Cefepime Cipro
% Susceptible
Figure 4. In vitro susceptibility of E. coli in North America (2009-2010) using 2012 CLSI breakpoints10
Escobar Page 5
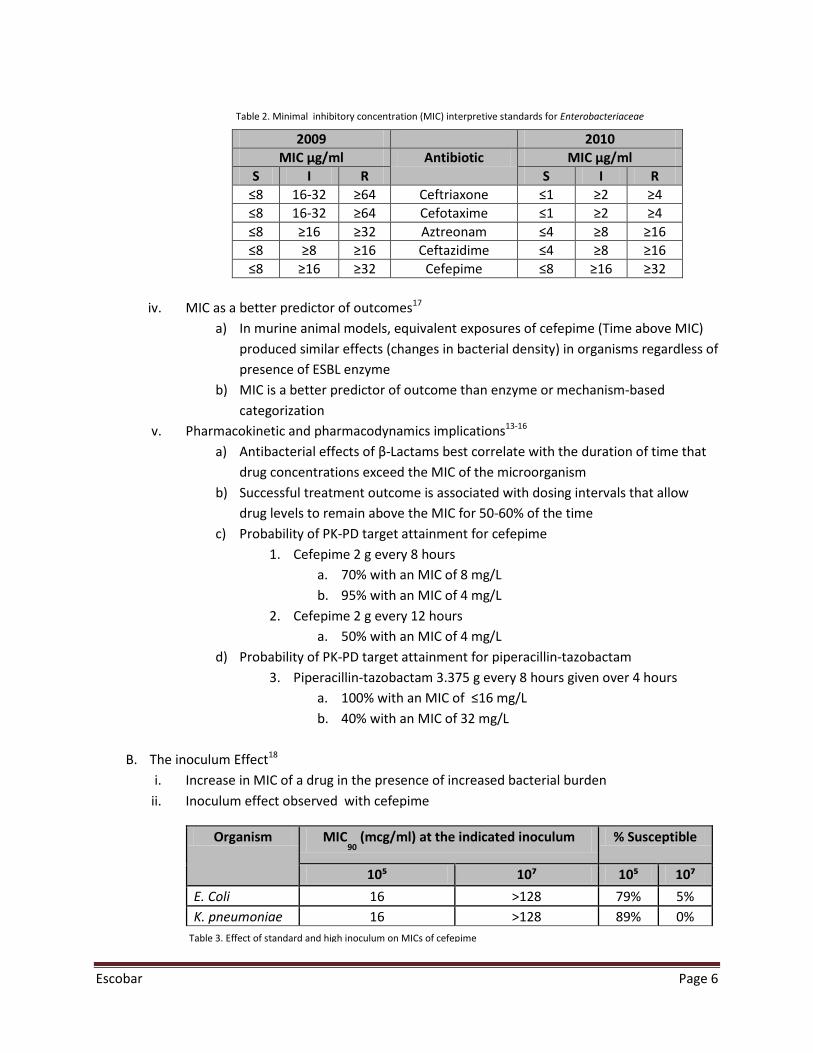
2009 2010 MIC µg/ml Antibiotic MIC µg/ml
S I R S I R ≤8 16-32 ≥64 Ceftriaxone ≤1 ≥2 ≥4 ≤8 16-32 ≥64 Cefotaxime ≤1 ≥2 ≥4 ≤8 ≥16 ≥32 Aztreonam ≤4 ≥8 ≥16 ≤8 ≥8 ≥16 Ceftazidime ≤4 ≥8 ≥16 ≤8 ≥16 ≥32 Cefepime ≤8 ≥16 ≥32
iv. MIC as a better predictor of outcomes17
a) In murine animal models, equivalent exposures of cefepime (Time above MIC) produced similar effects (changes in bacterial density) in organisms regardless of presence of ESBL enzyme
b) MIC is a better predictor of outcome than enzyme or mechanism-based categorization
v. Pharmacokinetic and pharmacodynamics implications13-16 a) Antibacterial effects of β-Lactams best correlate with the duration of time that
drug concentrations exceed the MIC of the microorganism b) Successful treatment outcome is associated with dosing intervals that allow
drug levels to remain above the MIC for 50-60% of the time c) Probability of PK-PD target attainment for cefepime
1. Cefepime 2 g every 8 hours a. 70% with an MIC of 8 mg/L b. 95% with an MIC of 4 mg/L
2. Cefepime 2 g every 12 hours a. 50% with an MIC of 4 mg/L
d) Probability of PK-PD target attainment for piperacillin-tazobactam 3. Piperacillin-tazobactam 3.375 g every 8 hours given over 4 hours
a. 100% with an MIC of ≤16 mg/L b. 40% with an MIC of 32 mg/L
B. The inoculum Effect18
i. Increase in MIC of a drug in the presence of increased bacterial burden ii. Inoculum effect observed with cefepime
Organism MIC90
(mcg/ml) at the indicated inoculum % Susceptible
10⁵ 10⁷ 10⁵ 10⁷ E. Coli 16 >128 79% 5% K. pneumoniae 16 >128 89% 0%
Table 3. Effect of standard and high inoculum on MICs of cefepime
Table 2. Minimal inhibitory concentration (MIC) interpretive standards for Enterobacteriaceae
Escobar Page 6
iii. Piperacillin-tazobactam is less subject to an inoculum effect compared to the cephalosporins and aztreonam
VI. HUMAN STUDIES EVALUATING THE EFFICACY OF CEFEPIME AND OTHER CEPHALOSPORINS FOR ESBL BACTEREMIA
i. Body of literature consists of mostly observational retrospective studies ii. Designed to observe mortality or clinical failure with for cephalosporins given for empirical
and definitive therapy
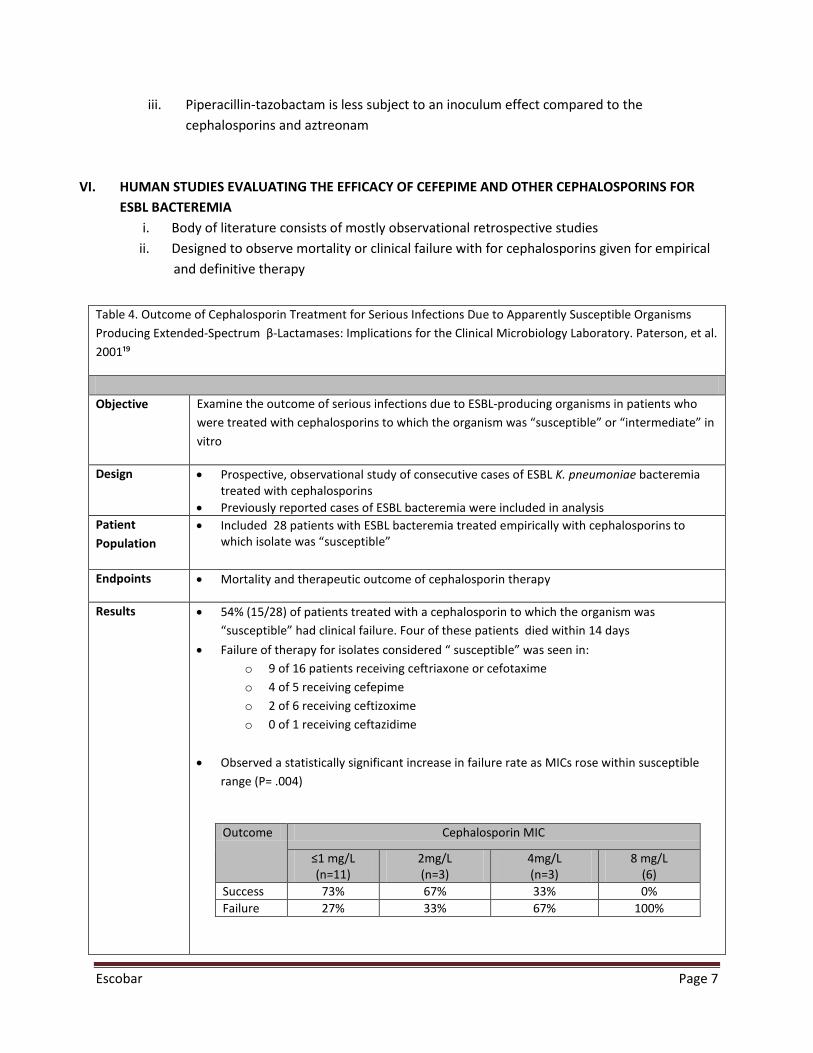
Table 4. Outcome of Cephalosporin Treatment for Serious Infections Due to Apparently Susceptible Organisms Producing Extended-Spectrum β-Lactamases: Implications for the Clinical Microbiology Laboratory. Paterson, et al. 2001¹⁹
Objective Examine the outcome of serious infections due to ESBL-producing organisms in patients who
were treated with cephalosporins to which the organism was “susceptible” or “intermediate” in vitro
Design • Prospective, observational study of consecutive cases of ESBL K. pneumoniae bacteremia treated with cephalosporins
• Previously reported cases of ESBL bacteremia were included in analysis Patient Population
• Included 28 patients with ESBL bacteremia treated empirically with cephalosporins to which isolate was “susceptible”
Endpoints • Mortality and therapeutic outcome of cephalosporin therapy
Results • 54% (15/28) of patients treated with a cephalosporin to which the organism was “susceptible” had clinical failure. Four of these patients died within 14 days
• Failure of therapy for isolates considered “ susceptible” was seen in: o 9 of 16 patients receiving ceftriaxone or cefotaxime o 4 of 5 receiving cefepime o 2 of 6 receiving ceftizoxime o 0 of 1 receiving ceftazidime
• Observed a statistically significant increase in failure rate as MICs rose within susceptible
range (P= .004)
Outcome Cephalosporin MIC
≤1 mg/L (n=11)
2mg/L (n=3)
4mg/L (n=3)
8 mg/L (6)
Success 73% 67% 33% 0% Failure 27% 33% 67% 100%
Escobar Page 7
A. Take home points:
i. Cephalosporins may not be appropriate agents to treat serious ESBL-bacteremia infections
ii. There is an increase in failure rate as MICs of cephalosporins rise within susceptible range
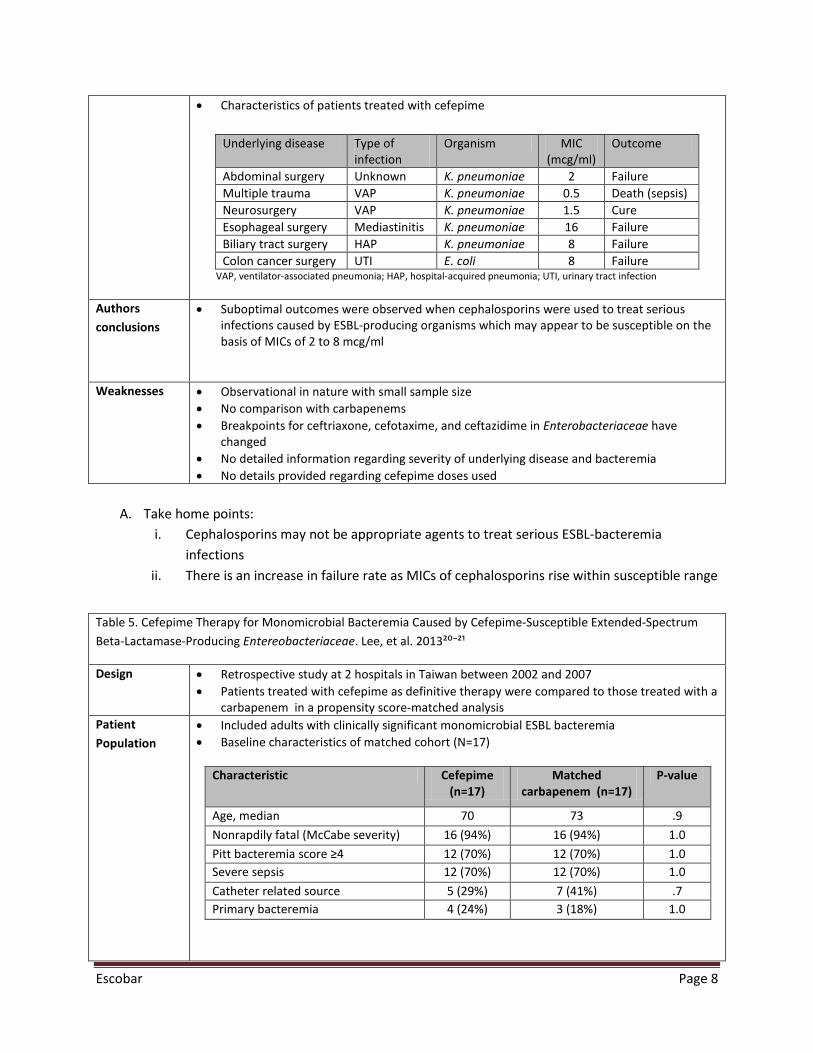
• Characteristics of patients treated with cefepime Underlying disease Type of
infection Organism MIC
(mcg/ml) Outcome
Abdominal surgery Unknown K. pneumoniae 2 Failure Multiple trauma VAP K. pneumoniae 0.5 Death (sepsis) Neurosurgery VAP K. pneumoniae 1.5 Cure Esophageal surgery Mediastinitis K. pneumoniae 16 Failure Biliary tract surgery HAP K. pneumoniae 8 Failure Colon cancer surgery UTI E. coli 8 Failure
VAP, ventilator-associated pneumonia; HAP, hospital-acquired pneumonia; UTI, urinary tract infection
Authors conclusions
• Suboptimal outcomes were observed when cephalosporins were used to treat serious infections caused by ESBL-producing organisms which may appear to be susceptible on the basis of MICs of 2 to 8 mcg/ml
Weaknesses • Observational in nature with small sample size • No comparison with carbapenems • Breakpoints for ceftriaxone, cefotaxime, and ceftazidime in Enterobacteriaceae have
changed • No detailed information regarding severity of underlying disease and bacteremia • No details provided regarding cefepime doses used
Table 5. Cefepime Therapy for Monomicrobial Bacteremia Caused by Cefepime-Susceptible Extended-Spectrum Beta-Lactamase-Producing Entereobacteriaceae. Lee, et al. 2013²⁰⁻²¹
Design • Retrospective study at 2 hospitals in Taiwan between 2002 and 2007 • Patients treated with cefepime as definitive therapy were compared to those treated with a
carbapenem in a propensity score-matched analysis Patient Population
• Included adults with clinically significant monomicrobial ESBL bacteremia • Baseline characteristics of matched cohort (N=17)
Characteristic Cefepime
(n=17) Matched
carbapenem (n=17) P-value
Age, median 70 73 .9 Nonrapdily fatal (McCabe severity) 16 (94%) 16 (94%) 1.0 Pitt bacteremia score ≥4 12 (70%) 12 (70%) 1.0 Severe sepsis 12 (70%) 12 (70%) 1.0 Catheter related source 5 (29%) 7 (41%) .7 Primary bacteremia 4 (24%) 3 (18%) 1.0
Escobar Page 8
B. Take home points: i. Cefepime cannot be recommended for therapy of ESBL bacteremia in the setting of:
a) Severe bacteremia and underlying disease b) Elevated MICs
ii. Successful outcomes with cefepime therapy may be possible when MICs are less than 1 iii. Definitive conclusions about cefepime’s effectiveness cannot be made
a) Study did not report dosing regimens used in association with MICs
C. Cefepime outcomes compared to carbapenems for E. cloacae ESBL bacteremia in an 8-year retrospective study 22
i. Methods: a) Included 121 patients with E. cloacae ESBL bacteremia b) Compared relationship between definitive or empirical treatment and clinical
outcomes for carbapenems vs. non-carbapenem therapy c) 80% of non-carbapenem therapy was cefepime
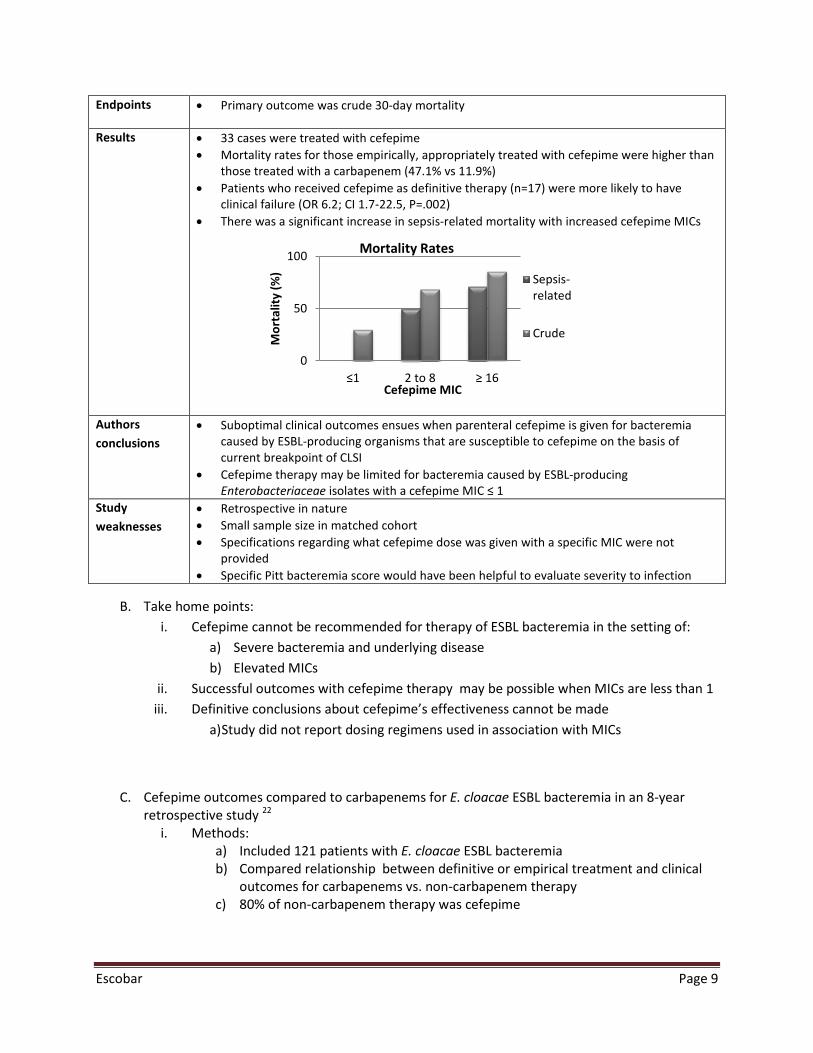
Endpoints • Primary outcome was crude 30-day mortality
Results
• 33 cases were treated with cefepime • Mortality rates for those empirically, appropriately treated with cefepime were higher than
those treated with a carbapenem (47.1% vs 11.9%) • Patients who received cefepime as definitive therapy (n=17) were more likely to have
clinical failure (OR 6.2; CI 1.7-22.5, P=.002) • There was a significant increase in sepsis-related mortality with increased cefepime MICs
Authors conclusions
• Suboptimal clinical outcomes ensues when parenteral cefepime is given for bacteremia caused by ESBL-producing organisms that are susceptible to cefepime on the basis of current breakpoint of CLSI
• Cefepime therapy may be limited for bacteremia caused by ESBL-producing Enterobacteriaceae isolates with a cefepime MIC ≤ 1
Study weaknesses
• Retrospective in nature • Small sample size in matched cohort • Specifications regarding what cefepime dose was given with a specific MIC were not
provided • Specific Pitt bacteremia score would have been helpful to evaluate severity to infection
0
50
100
≤1 2 to 8 ≥ 16
Mor
talit
y (%
)
Cefepime MIC
Mortality Rates
Sepsis-related
Crude
Escobar Page 9
ii. Population (N=121) a) 64% bacteremic onset in ICU b) 50% Pittsburgh bacteremic score ≥ 4
iii. Underlying sources of bacteremia (n=121) a) 40% vascular catheter related infections b) 27% primary bacteremia c) 10% pneumonia d) 7% urinary tract infection
iv. Findings a) The in-hospital sepsis-related mortality in patients definitively treated by a
carbapenem (5/53 or 9.4%) was lower than that of patients treated by non-carbapenem agents (16/61 or 26%) P=0.02
VII. HUMAN STUDIES EVALUATING THE EFFICACY OF PIPERACILLIN-TAZOBACTAM FOR ESBL BACTEREMIA
i. Body of literature consists of observational retrospective or post-hoc analysis of prospective studies
ii. Designed to observe mortality or clinical failure with for piperacillin-tazobactam given for empirical and definitive therapy
A. Successful outcomes have been reported with use of piperacillin-tazobactam in the treatment of
ESBL bacteremia:23 i. Gavin, et al. 200627
a) Successful outcomes reported in 14 of 15 ESBL infections with MIC ≤ 16/4 mg/L, including 10 of 11 non-urinary infections
b) Failure reported in 4 out of 5 patients when piperacillin-tazobactam MIC > 16/4 mg/L
ii. Rodriguez-Baño, et al. 200624 a) Analyzed outcome of 43 episodes of ESBL E. coli bacteremia b) Mortality was lower when patients were given a β-Lactam/β-Lactamase
Inhibitor combination or carbapenem, compared to other antibiotics
Table 6. Predictors of Mortality in Patients with Bloodstream Infections Caused by Extended Spectrum-β-Lactamase-Producing Enterobacteriaceae: Importance of Inadequate Initial Antimicrobial Treatment. Tumbarello, et al. 2007²⁸ Objective Identify the risk factors for mortality in patients with bloodstream infections caused by ESBL-
producing strains of E. coli, Klebsiella spp., and Proteus mirabilis
Design • 6-year retrospective cohort analysis
Escobar Page 10
A. Take home points regarding use of β-Lactam/β-Lactamase Inhibitor combinations vs.
carbapenems: i. Effective empiric antimicrobial therapy is essential in serious infections caused by ESBL-
producing isolates ii. β-Lactam/β-Lactamase Inhibitor combinations, when susceptible, have the potential for
a successful outcomes in serious infections, however, carbapenems displayed best outcomes in this setting
Patient Population
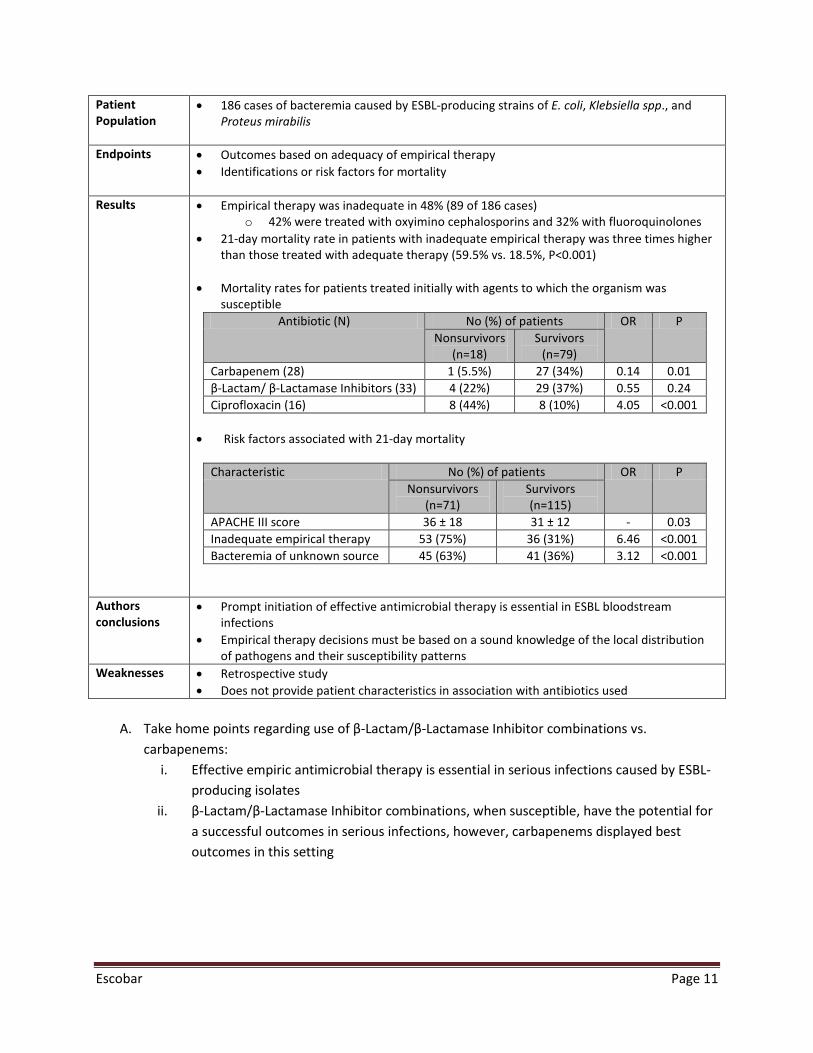
• 186 cases of bacteremia caused by ESBL-producing strains of E. coli, Klebsiella spp., and Proteus mirabilis
Endpoints • Outcomes based on adequacy of empirical therapy • Identifications or risk factors for mortality
Results
• Empirical therapy was inadequate in 48% (89 of 186 cases) o 42% were treated with oxyimino cephalosporins and 32% with fluoroquinolones
• 21-day mortality rate in patients with inadequate empirical therapy was three times higher than those treated with adequate therapy (59.5% vs. 18.5%, P<0.001)
• Mortality rates for patients treated initially with agents to which the organism was susceptible
Antibiotic (N) No (%) of patients OR P Nonsurvivors
(n=18) Survivors
(n=79) Carbapenem (28) 1 (5.5%) 27 (34%) 0.14 0.01 β-Lactam/ β-Lactamase Inhibitors (33) 4 (22%) 29 (37%) 0.55 0.24 Ciprofloxacin (16) 8 (44%) 8 (10%) 4.05 <0.001
• Risk factors associated with 21-day mortality
Characteristic No (%) of patients OR P Nonsurvivors
(n=71) Survivors (n=115)
APACHE III score 36 ± 18 31 ± 12 - 0.03 Inadequate empirical therapy 53 (75%) 36 (31%) 6.46 <0.001 Bacteremia of unknown source 45 (63%) 41 (36%) 3.12 <0.001
Authors conclusions
• Prompt initiation of effective antimicrobial therapy is essential in ESBL bloodstream infections
• Empirical therapy decisions must be based on a sound knowledge of the local distribution of pathogens and their susceptibility patterns
Weaknesses • Retrospective study • Does not provide patient characteristics in association with antibiotics used
Escobar Page 11
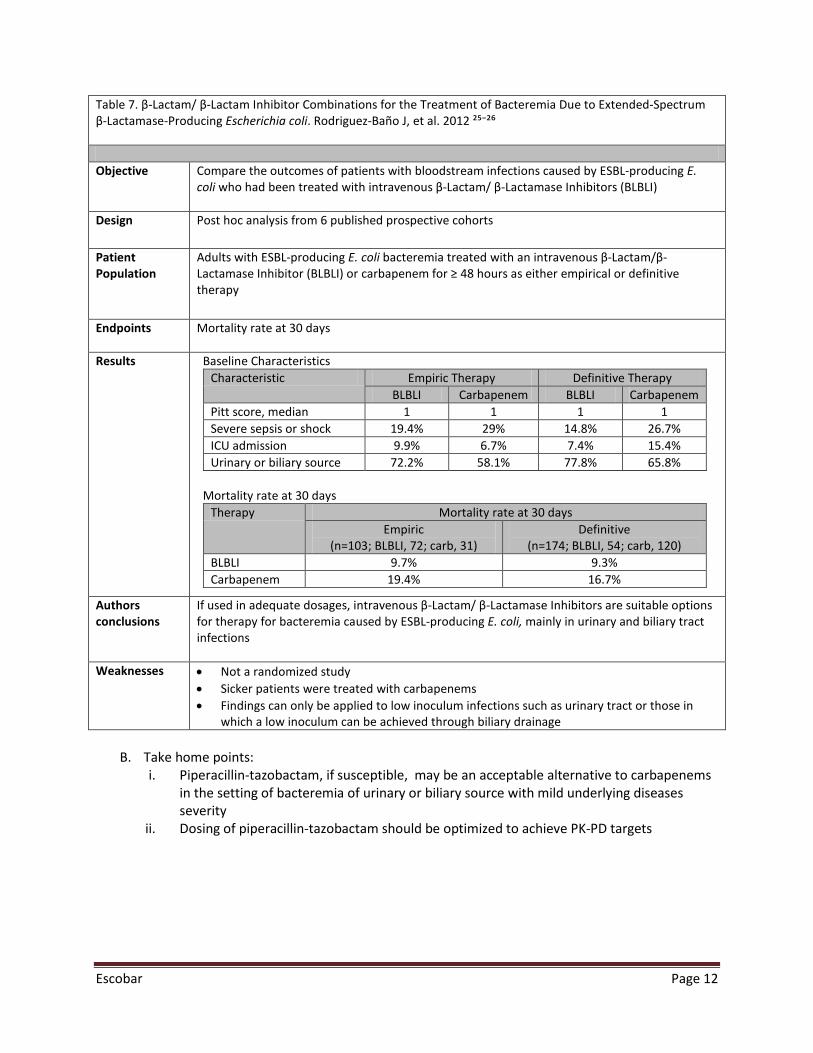
Table 7. β-Lactam/ β-Lactam Inhibitor Combinations for the Treatment of Bacteremia Due to Extended-Spectrum β-Lactamase-Producing Escherichia coli. Rodriguez-Baño J, et al. 2012 ²⁵⁻²⁶ Objective Compare the outcomes of patients with bloodstream infections caused by ESBL-producing E.
coli who had been treated with intravenous β-Lactam/ β-Lactamase Inhibitors (BLBLI)
Design Post hoc analysis from 6 published prospective cohorts
Patient Population
Adults with ESBL-producing E. coli bacteremia treated with an intravenous β-Lactam/β-Lactamase Inhibitor (BLBLI) or carbapenem for ≥ 48 hours as either empirical or definitive therapy
Endpoints Mortality rate at 30 days
Results
Baseline Characteristics Characteristic Empiric Therapy Definitive Therapy
BLBLI Carbapenem BLBLI Carbapenem Pitt score, median 1 1 1 1 Severe sepsis or shock 19.4% 29% 14.8% 26.7% ICU admission 9.9% 6.7% 7.4% 15.4% Urinary or biliary source 72.2% 58.1% 77.8% 65.8%
Mortality rate at 30 days
Therapy Mortality rate at 30 days Empiric
(n=103; BLBLI, 72; carb, 31) Definitive
(n=174; BLBLI, 54; carb, 120) BLBLI 9.7% 9.3% Carbapenem 19.4% 16.7%
Authors conclusions
If used in adequate dosages, intravenous β-Lactam/ β-Lactamase Inhibitors are suitable options for therapy for bacteremia caused by ESBL-producing E. coli, mainly in urinary and biliary tract infections
Weaknesses • Not a randomized study • Sicker patients were treated with carbapenems • Findings can only be applied to low inoculum infections such as urinary tract or those in
which a low inoculum can be achieved through biliary drainage
B. Take home points: i. Piperacillin-tazobactam, if susceptible, may be an acceptable alternative to carbapenems
in the setting of bacteremia of urinary or biliary source with mild underlying diseases severity
ii. Dosing of piperacillin-tazobactam should be optimized to achieve PK-PD targets
Escobar Page 12
VIII. USE OF OTHER ANTIMICROBIALS FOR ESBL BACTEREMIA A. Fluoroquinolones 29-30
i. High rates of concurrent resistance and the potential for emergence of resistance on treatment often limits use
ii. Ciprofloxacin was less effective than imipenem used empirically in a study evaluating 17 patients with ESBL K. pneumoniae bacteremia
a) 2 out of 10 (20%) patients failed therapy with imipenem vs. 5 out of 7 (71%) patients treated with ciprofloxacin
B. Cephamycins 31 i. High in-vitro susceptibility
ii. Relevant clinical data is limited iii. Porin loss mutations limit their value
IX. RISK FACTORS FOR MORTALITY AND IMPORTANCE OF ADEQUATE EMPIRIC THERAPY 1, 28 A. Risk factors for acquisition of infections caused by ESBL-producing bacteria
i. Serious illness ii. History of lengthy hospital stay
iii. Prolonged exposure to invasive medical devices or procedures a) Urinary catheters, endotracheal tubes, and central venous lines
iv. Prior exposure to antimicrobial therapy v. High local prevalence of ESBL organisms
B. Risk factors associated with 21-day mortality in ESBL bacteremia i. Failure to provide adequate antimicrobial therapy within the first 72 hours of infection
ii. Failure to identify the source of the ESBL bacteremia and provide adequate source control
iii. Nature and severity of underlying disease state present at initiation of antimicrobial therapy
C. Empiric therapy considerations in patients with high risk of mortality in ESBL bacteremia i. Empiric therapy when ESBL-infections are suspected should be based on local
susceptibility data ii. Regimens most commonly classified as inadequate for empiric therapy in this setting are
cephalosporins and fluoroquinolones iii. Empiric therapy with carbapenems is associated with lowest mortality in this setting
Escobar Page 13
X. CONCLUSIONS AND RECOMMENDATIONS: A. Carbapenem-sparing therapy options are urgently needed to reduce development of resistance B. Cefepime for ESBL Bacteremia
i. Based on current studies, cefepime may not be a safe option for severe ESBL bloodstream infections
ii. Worse outcomes are seen as MICs for cefepime increase within susceptible range iii. Further studies are required to evaluate:
a) More aggressive dosing regimens of cefepime b) Less severe and easier to treat infections c) Low MICs
C. Piperacillin-tazobactam for ESBL Bacteremia i. Piperacillin-tazobactam is a reasonable alternative to carbapenems if susceptible in:
a) Urinary or biliary sources with adequate drainage b) Mild in severity of underlying disease
ii. Further studies are necessary to investigate the role of piperacillin-tazobactam for serious infections
iii. Doses must be optimized to achieve target PK-PD targets D. Empirical therapy with a carbapenem is most appropriate when ESBL infection is suspected in
the setting of high risk for mortality
Escobar Page 14
References:
1. Paterson DL, Bonomo RA. Extended-Spectrum β-Lactamase: a Clinical Update. CMR 2005;18.4.657-686 2. Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae.
MMWR 2013;62:165-170 3. Schwaber MJ, Klarfeld-Lidji S, Navon-Venezia S, Schwartz D, Leavitt A, Carmeli Y. Predictors of
carbapenem-resistant Klebsiella pneumonia acquisition among hospitalized adults and effect of acquisition on mortality. Antimicrob Agents Chemother 2008; 52:1028–33
4. Bratu S, Landman D, Haag R, et al. Rapid spread of carbapenem-resistant Klebsiella pneumoniae in New York City: A new threat to our antibiotic armamentarium. Arch Intern Med 2005; 165:1430–5.
5. Patel G, Huprikar S, Factor SH, et al. Outcomes of Carbapenem-Resistant Klebsiella pneumoniae Infection and the Impact of Antimicrobial and Adjunctive Therapies. Infect Control Hosp Epidemiol 2008; 29: 1099-1106
6. Rawat D, Nair D. Extended Spectrum β-Lactamases in Gram Negative Bacteria. J Glob Infect Dis. 2010; 2 (3): 263-274
7. Babic M, Hujer AM, Bonomo RA. What’s new in antibiotic resistance? Focus on beta-lactamases. Drug Resistance Updates 2006; 9: 142-156
8. Jacoby GA, Munoz-Price LS. The New β-Lactamases. N engl J Med 2005; 352(4): 380-91 9. Clinical and Laboratory Standards institute. Performance Standards for Antimicrobial susceptibility
Testing: Twenty-Third Informational Supplement M100-S23. CLSI, Wayne, PA, USA, 2013 10. Paterson DL, Ko WC, Von Gottberg A, et al. Antibiotic therapy for Klebsiella pneumoniae bacteremia:
implications of production of extended spectrum β-Lactamases. Clin Infect Dis 2004; 39:31-37 11. Hoban DJ, Lascols C, Nicolle LE, et al. Antimicrobial susceptibility of Enterobacteriaceae, including
molecular characterization of ESBL-producing species, in urinary tract isolates from hospitalized patients in North America and Europe: results from the SMART study 2009-2010. Diag Microb Infect Dis 2012; 74;: 62-67
12. Livermore DM, Andrews JM, Hawkey PM, et al. Are susceptibility tests enough, or should laboratories still seek ESBLs and carbapenemases dierectly? J Antimicrob Chemother 2012; 10.1093
13. Andes D, Craig WA. Treatment of infections with ESBL-producing organisms: pharmacokinetic and pharmacodynamics considerations. Clin Microbiol Infect 2005: 11(6):10-17
14. Ambrose GP, Bhavnani SM, Jones RN. Pharmacokinetics-Pharmacodynamics of cefepime and piperacillin-Tazobactam against Escherichia coli and Klebsiella pneumoniae Strains Producing Extended-Spectrum β-Lactamases: Report from the ARREST Program. Antimic Agen and Chemo 2003; 47(5): 1643-1646
15. Roos JF, Rulitta J, Lipman J, et al. Pharmacokinetic-pharmacodynamic rationale for cefepime dosing regimens in intensive care units. J Clin Microbiol 2006; 58; 987-993
16. Lodise TP, Lomaestro B, Drusano GL. Piperacillin-tazobactam for Pseudomonas aeruginosa Infection: Clinical Implications of an Extended Infusion Dosing Strategy. Clin Infect Dis 2007; 44:357-63
17. Maglio D, Ong C, Banevicious MA, et al. Determination of the In Vivo Pharmacodynamic Profile of Cefepime against Extended-Spectrum-Beta-Lactamase-Producing Eschirichia coli at Various Inocula. Antimic Agents Chemother 2004; 48(6): 1941-1947
18. Thomson KS, Ellen SM. Cefepime, Piperacillin-Tazobactam, and the Inoculum Effect in Tests with Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae 2001; 45(12): 3548-3554
19. Paterson DL, Ko W, Gottberg AV, et al. Outcome of Cephalosporin Treatment for Serious Infections Due to Apparently Susceptible Organisms Producing Extended-Spectrum β-Lactamases: Implications for the Clinical Microbiology Laboratory. J Clin Microbiol 2001; 39:2206-12
Escobar Page 15
20. Lee NY, Le CC, Huang WH, et al. Cefepime Therapy for Monomicrobial Bacteremia Caused by Cefepime-Susceptible Extended-Spectrum Beta-Lactamase-Producing Entereobacteriaceae: MIC Matters. Clin Infect Dis 2013; 56(4): 488-95
21. Alshuler J, Aitken S, Guervil D, et al. Treatment of Extended-Spectrum Beta-Lactamase Enterobacteriaceae with Cefepime: The Dose Matters, too. Clin Infect Dis 2013; 57(6): 915-16
22. Lee CC, Lee NY, Yan JJ et al. Bacteremia due to Extended-Spectrum β-Lactamase-producing Enterobacter cloacae: role of carbapenem therapy. Antimicrob Agents Chemoth 2010; 54:3551-6
23. Peterson LR. Antibiotic policy and prescribing strategies for therapy of extended-spectrum β-Lactamase-producing Enterobacteriaceae: the role of piperacillin-tazobactam. Clin Microbiol Infect 2008; 14(1): 181-184
24. Rodrigez-Baño J, Navarro, MD, Romero L, et al. Bacteremia Due to Extended Spectrum β-Lactamase- Producing Escherichia coli in the CTX-M Era: a New Clinical Challenge. Clin Infect Dis 2006; 43: 1407-14
25. Rodrigez-Baño J, Dolores Navarro M, Retamar P, et al. β-Lactam/ β-Lactam Inhibitor Combinations for the Treatment of Bacteremia Due to Exteded-Spectrum β-Lactamase-Producing Escherichia coli: A Post Hoc Analysis of Prospective Cohorts. Clin Infect Dis 2012; 54:167-74
26. Perez F, Bonomo RA. Can We Really Use β-Lactam/ β-Lactam Inhibitor Combinations for the Treatment of Infections Caused by Extended-Spectrum β-Lactamase-Producing Bacteria? Clin Infect Dis 2012; 54(2):175-177
27. Gavin PJ, Suseno MT, Thomson RB, et al. Clinical correlation of the CLSI susceptablity breakpoint for piperacillin-tazobactam against extended-spectrum β-Lactamase-Producing Escherichia coli and Klebsiella species. Antimicrob Agents Chemother 2006; 50; 2244-2247
28. Tumbarello M, Sanguinetti M, Montuori E et al, Predictors of mortality in patients with bloodstream infections caused by extended-spectrum-β-lactamase-producing Enterobacteriaceae: importance of inadequate initial antimicrobial treatment. Antimicrob Agents Chemother 2007; 51: 1987-94
29. Endimiani A, Luzzaro F, Perillli M, et al. Bacteremia Due to Klebsiella pneumoniae Isolates Producing the TEM-52 Extended-Spectrum β-Lactamase: Treatment Outcome of Patients Receiving Imipenem or Ciprofloxacin. Clin Infect Dis 2004; 38:243-51
30. Souha SK, Kanafani Z. Current concepts in Antimicrobial Therapy Against Gram-Negative Organisms: Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae, and Multidrug-Resistant Pseudomonas aeurginosa. Mayo Clin Proc. 2011; 86(3): 250-259
31. Lee, C. H., L. H. Su, Y. F. Tang, and J. W. Liu. 2006. Treatment of ESBL-producing Klebsiella pneumoniae bacteremia with carbapenems or flomoxef: a retrospective study and laboratory analysis of the isolates. J. Antimicrob. Chemother. 58:1074-1077
Escobar Page 16