Asmah Nasser, M.D.. Alpha blockers Beta blockers Alpha plus beta blockers.
Upload
hoangtuongCategory
view
212download
0
THERAPY
Two studies of 'major clinical relevance' have established that calcium antagonists and ~blockers produce similar outcomes in terms of symptomatic benefit, mortality and serious cardiovascular morbidity in patients with stable angina, say L Ryden and K Malmberg from Karolinska Hospital , Stockholm, Sweden. I This is reassuring considering the recent concerns about the safety of calcium antagonists for patients with ischaemic heart disease, they say.
News from TIBET The Total Ischaemic Burden European Trial2.3 was
a double-blind, multi centre study that randomised 682 patients with mild chronic stable angina pectoris to receive treatment with atenolol 50mg twice daily, slow-release nifedipine 20mg twice daily, or both drugs in combination. There was a 2-week placebo run-in period, and exercise testing was conducted after 6 weeks of treatment. The dosage of nifedipine could be increased to 40mg twice daily if required after 6 weeks.
Ischaemic burden reduced Compared with baseline, all treatments
significantly improved time to pain, total exercise time, time to 1 mm ST segment depression and maximal ST segment depression on treadmill and bicycle exercise testing.2 The number of patients experiencing ischaemic episodes during 48-hour ambulatory ST segment monitoring was also reduced. There were no significant differences in any of these variables between the treatment groups.
Hard end-points assessed There were also no statistically significant
differences between the treatment groups in terms of the incidence of various 'hard'* or 'so/t'** end-points during a mean of 2 years of follow-up [see figure IV The presence of ambulatory ischaemia was not found to be predictive of outcome.
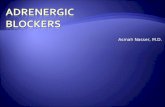
Fig 1. Incidence of end-points· in TIBET
Cardiac death
Non·fatal MI
Unstable angina
CABG orPlCA
Treatment failure
o t 234 567
Percentage of patients
• the moat IMV." end-poinl for _ch pal_"t wu analyMd CABG • coronary artery byp ... graft MI - myocardial infarction; PTCA • percutaneous lran.luminal coronary anoioplaaty
• Atenolol
~ Nifediplne
• Comblnallon
Although the use of combination therapy cannot be justified on the grounds of greater reduction in ischaemic burden,2 there was a trend toward this approach improving prognosis.3 However, confirmation of prognostic improvement is needed before combination therapy can be recommended, say the researchers.3
0156·270319611 Q33.000171$01 .00o Adl. Internetlol1lll Limited 19116. Ali rights r~
Confumation from APSIS No clinically important differences between the
effects of metoprolol and verapamil on the prognosis of patients with stable angina pectoris were found in another similar study, the Angina Prognosis Study in Stockholm [APSIS; (see figure 2)] .4
Fig 2. Incidence of fatal and non-fatal cardiovascular events in APSIS
CABG or
Unstable Inall .. .."""
CerabrovasCIllar
• Me\optOiQI
e:::aVerlPlmll
o 2 4 6 8 10 12 14 16
• without ,..y .. ~.rlaatlon Percentage 01 patients
CABG : coronary .".ry bypua graft; MI • myocardtal infamion; PTeA .. percutaneou. tran.lum inal coronary angiopla.ty; pvo = peripheral vucular di .... e
This study involved 809 patients with stable angina who were randomised to receive treatment with metoprolol (maximum dosage 200mg once daily) or verapamil (maximum dosage 240mg twice daily). Patients were followed for a median of 3.4 years.
Tolerability differences important? In TIBET, 27% of atenolol monotherapy recipients
and 29% of combination therapy recipients withdrew from therapy, compared with 40% of nifedipine monotherapy recipients.3 1n APSIS, ILl % of metoprolol and 14.6% of verapamil recipients, respectively, withdrew from treatment because of adverse effects.4
As calcium antagonists and ~-blockers seem to produce similar outcomes in patients with stable angina, it is important to carefully assess measures other than efficacy in this indication, say Drs Ryden and Malmberg. I
* carrJioc death, nonjaJaJ myocardial infamion or unstahIe angina
** need/or coronary artery bypass surgery and/or angWplarty. or persistence of symptoms despite optimal therapy
1. Ryd&! L, ct a1. Calcium channel blockers 01' beta receptor antagonists for patients with ischaemic bean disease. What is tbe best choice? European Heart
Journal 17: 1·2, Jan 19961. Fox KM. ct aI. The ToIaIlschaemic Burden European Trial (TIBET): effects of atenolol, nifedipine SR and their combination
on the exercise test and the total ischaemic burden in 608 patients with stable
angina. European Heart Journal 17: 96-103. Jan 1996 3. Dargie HJ, ct a1. Total
Iscbacmic Burden European Trial (TIBET): effects of ischaemia and treatment with aICDOlol, nifodipine SR and tbeir combination on outcome in patients with
chronic stable angina. European Heart Journal 17: 104-122, Jan 1996
4. Rdmqvist N, ct aI. Effects of mctoprolol vs verapamil in patients with stable
angina pectoris: tbe Angina Prognosis Study in Stockbolm (APSIS). European
Heart Journal 17: 76-81. Jan 1996 100"'.31
• EtIitorilll COI1llM1It: Concern over the safety of the use of calcium antagonists in patients with ischaemic heart disease was triggered by the results of a meta-analysis of the effects of slwrt-acting nifedipine in patients with unstable angina, stable angiTlLl and/or myocardial infarr:tion {see Inpharma 1005: 20. 23 Sep 1995; 8oo314666J. Altlwugh the meta-analysis indicated that moderate to high dosages of nifedipine were associated with a higher risk of death tlwn placebo. this effect may be specific to short-actingformulations.
Inphannas 20 Apr 1l1li6 No. 1033
17