IRCCS Istituto delle Scienze Neurologiche di Bologna ... · – “hot cross bun” in the pons...
55
Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna
Transcript of IRCCS Istituto delle Scienze Neurologiche di Bologna ... · – “hot cross bun” in the pons...

Pietro Cortelli
IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna

HYSTORY• 1900descriptionofOPCA(Dejerine,Thomas)
• 1960descriptionofShy-Dragersyndrome
• 1964descriptionofSND(Adams,VanBogaert,VanderEecken)
Human α-synucleinopathies
• Parkinson’sdisease(sporadic,geneticswitha-synorotherthanα-synmutation)
• Dementiawithlewybodies– PureDLB– FamilialAlzheimerdisease(APP,PS-1,PS-2mutation,Downsyndrome)
• MultiplesystemAtrophy(MSAp,MSAc)• Pure/isolatedautonomicfailure(PAF)• Disesasesthatmayhaveα-synimmunoreactivelesion
– HallevordenSpatz,NeuroaxonalDystrophy,traumaticbarininjury,Pickdisease,ALS
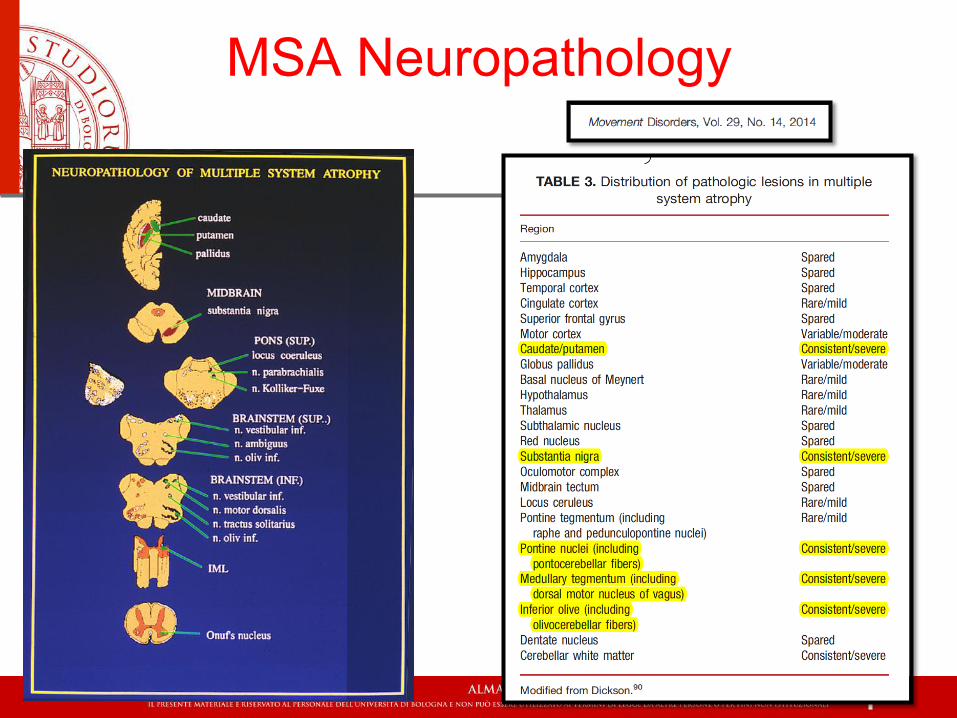
MSA Neuropathology
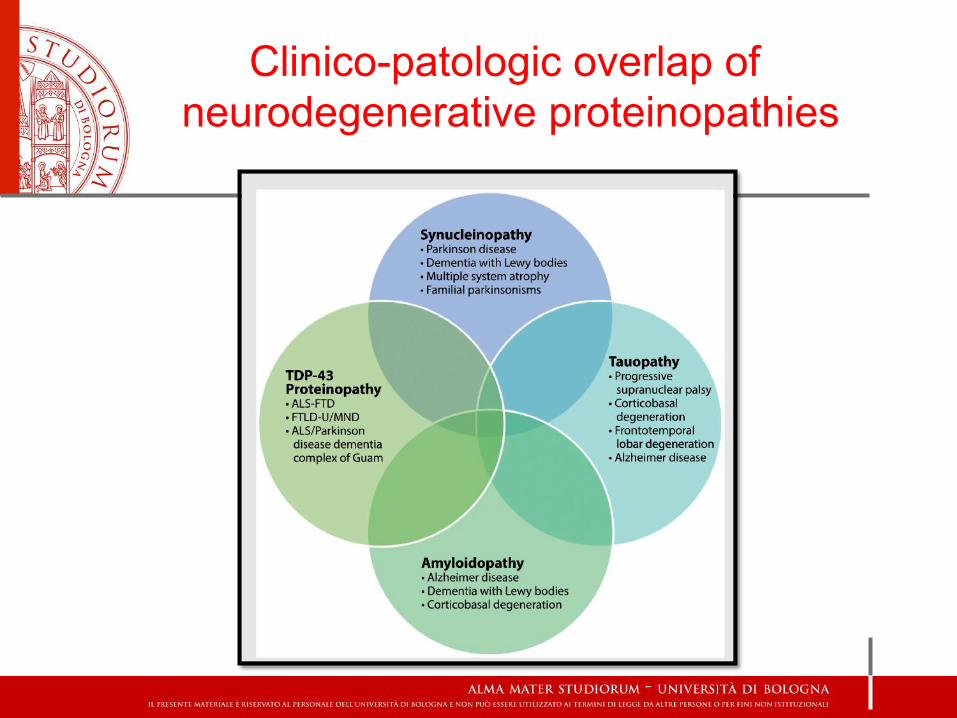
Clinico-patologic overlap of neurodegenerative proteinopathies
MSASTUDYGROUPS
� EuropeanMSAStudyGroup(1999,Innsbruck,27centres)
� NorthAmericaMSAStudyGroup(2003,USA,11centres)
� JapaneseMSAStudyGroup
� ChineseMSAStudyGroup
� MulticentreregistryoftheGermanCompetenceNetworkonParkinson’sdisease(2005,30centres)
EPIDEMIOLOGY
� Ararediseasewithannualincidenceabout0,6per100.000peryear
� 3per100.000peryearinpopulationolderthan50yrs
� Prevalencerangesfrom1,9to4,9per100.000inhabitants(similartothoseofHuntingtonandmotorneurondiseases)
CLINICALHALLMARKS
• Parkinsonism
• Cerebellarataxia
• Autonomicfailure
• Pyramidalsymptoms/signs
� MSA-p=predominantparkinsonian(68%)
� MSA-c=predominantcerebellar(32%)
NONMOTORSLEEP
AUTONOMIC
MOTORPARKINSONIANCEREBELLAR
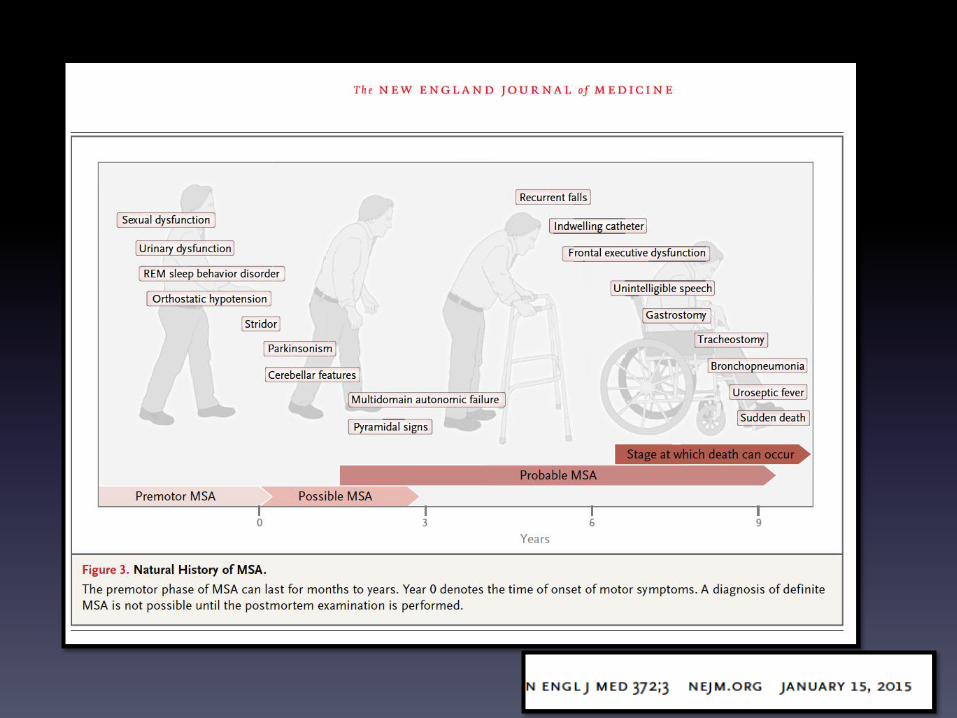
CLINICALPRESENTATIONOFMSA
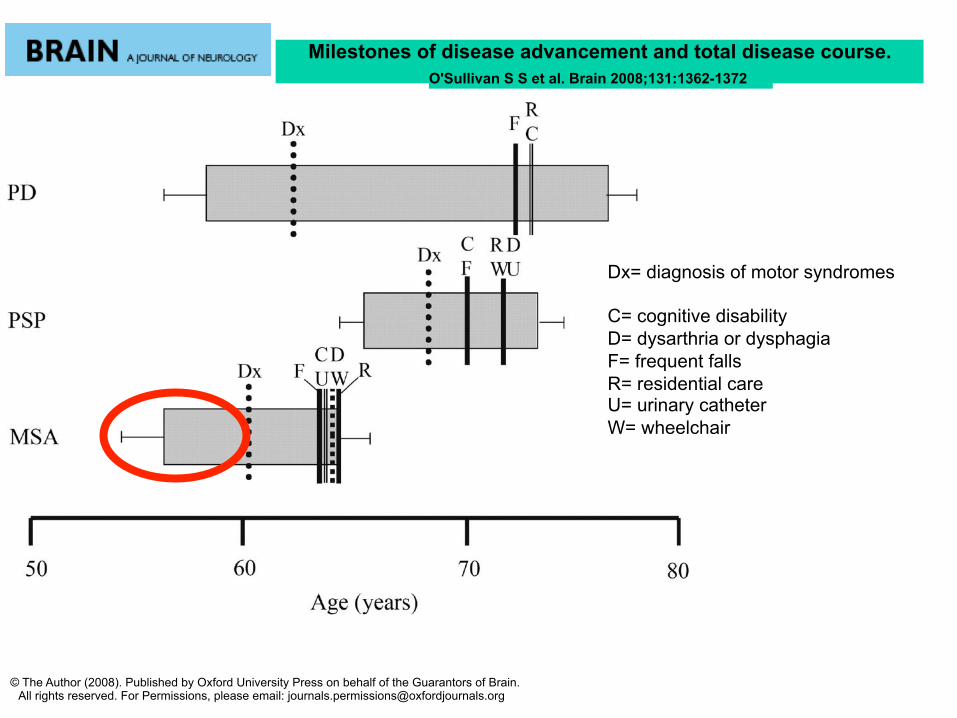
Milestones of disease advancement and total disease course. O'Sullivan S S et al. Brain 2008;131:1362-1372
© The Author (2008). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected]
Dx= diagnosis of motor syndromes C= cognitive disability D= dysarthria or dysphagia F= frequent falls R= residential care U= urinary catheter W= wheelchair
DIAGNOSIS
� NiallQuinn1989:“Thenatureofthebeast”
� FirstConsensusCriteria1998
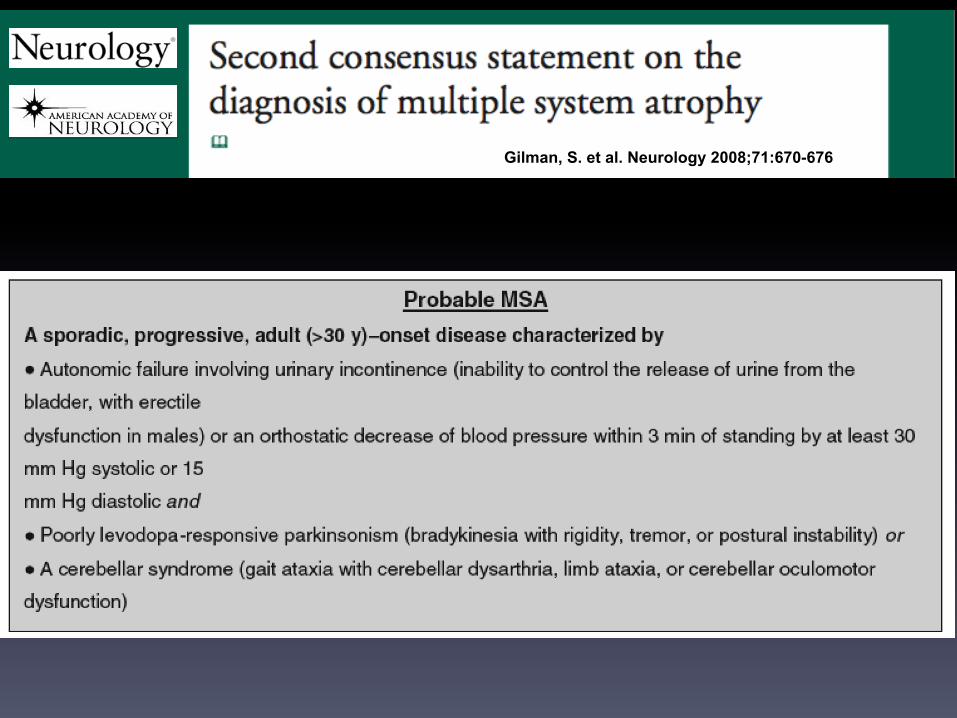
� SecondConsensusCriteria2008(simpleandincludeneuroimagingfeatures)
� Validation2009:sensitivitywithnewconsensus“possiblecategory”washigher,andPPVmarginallyhigher,thanforclinicaldiagnosiswitholdconsensus“possiblecategory”(sensitivityofnew=41%vs28%ofold)
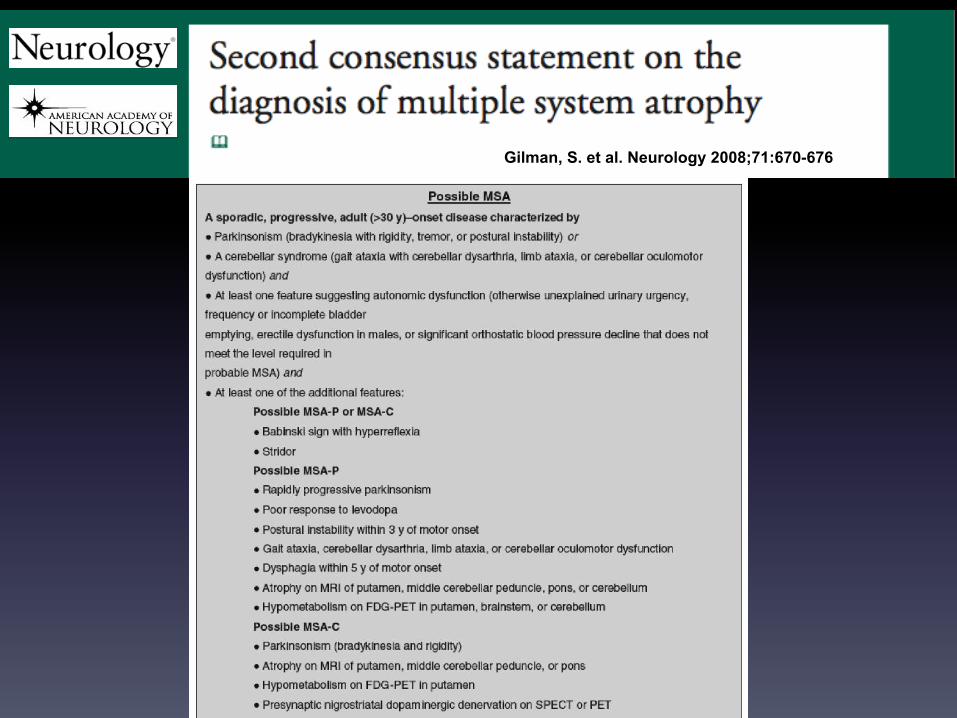
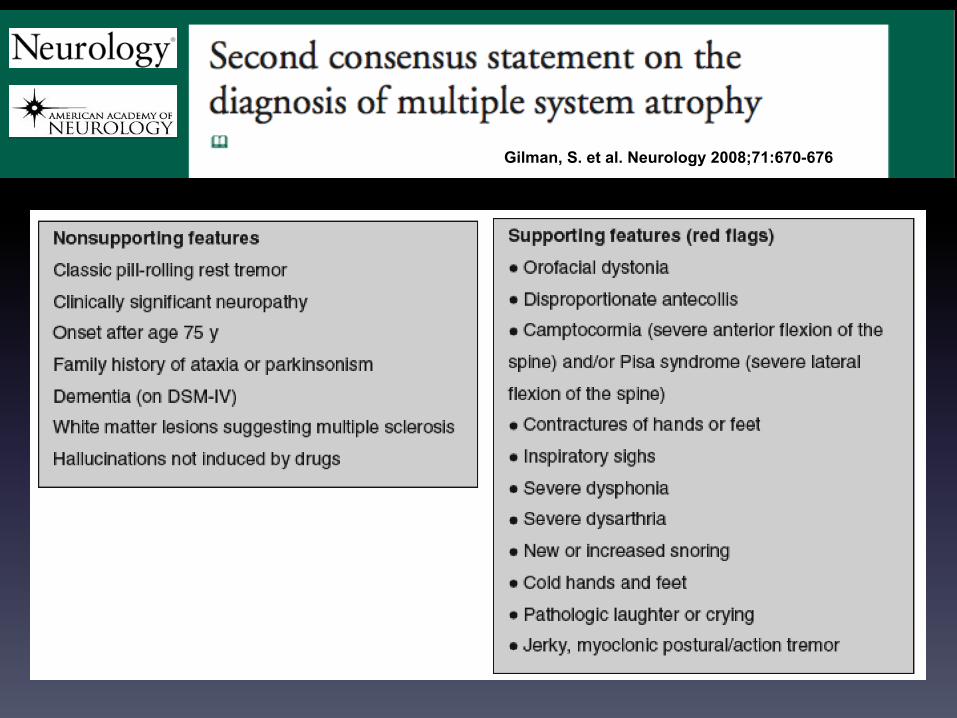
Gilman, S. et al. Neurology 2008;71:670-676
Gilman, S. et al. Neurology 2008;71:670-676
Gilman, S. et al. Neurology 2008;71:670-676
Gilman, S. et al. Neurology 2008;71:670-676
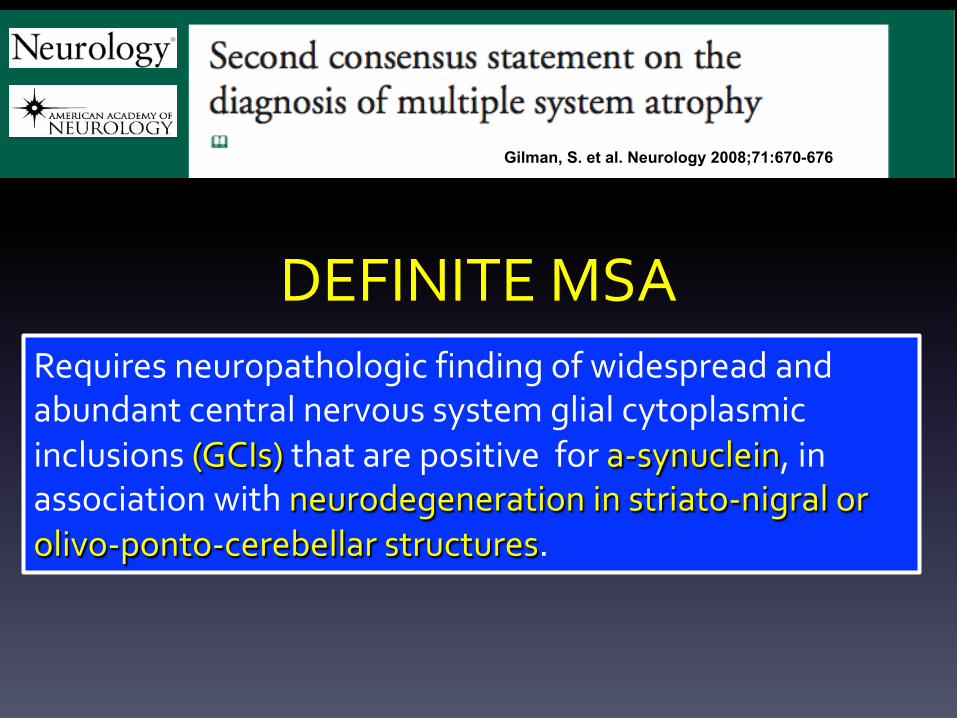
Requiresneuropathologicfindingofwidespreadandabundantcentralnervoussystemglialcytoplasmicinclusions(GCIs)thatarepositivefora-synuclein,inassociationwithneurodegenerationinstriato-nigralorolivo-ponto-cerebellarstructures.
DEFINITEMSA
PROGNOSIS� MoresevereanddisablingthanPD(4%ofprolonged
survival,Petrovich2012,Calandra2013)
� Themostimportantearlyclinicalprognosticfeatureregardingsurvivalis“earlyautonomicdysfunction”
� Suddendeathis7timesascommoninpatientswithautonomicpredominanceandmayoccureveninptwithtracheostomy
� Female,olderageofonset,shorterintervaluntilclinicalmilestonesarereachedpredictshortersurvivaltime
� NodifferencesbetweenMSA-pandMSA-c
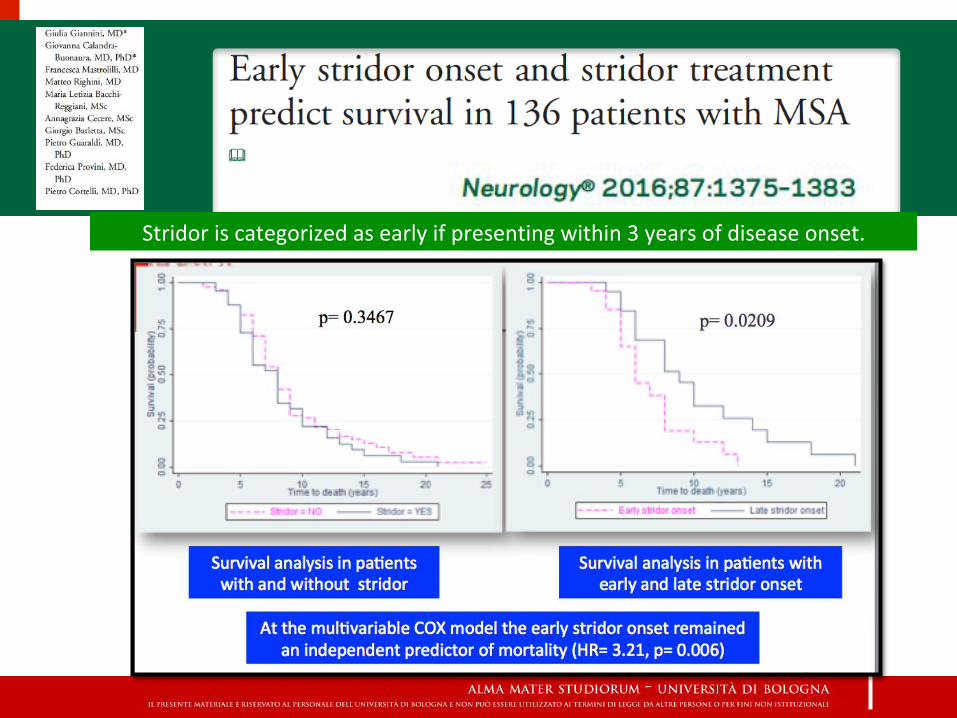
Stridoriscategorizedasearlyifpresentingwithin3yearsofdiseaseonset.
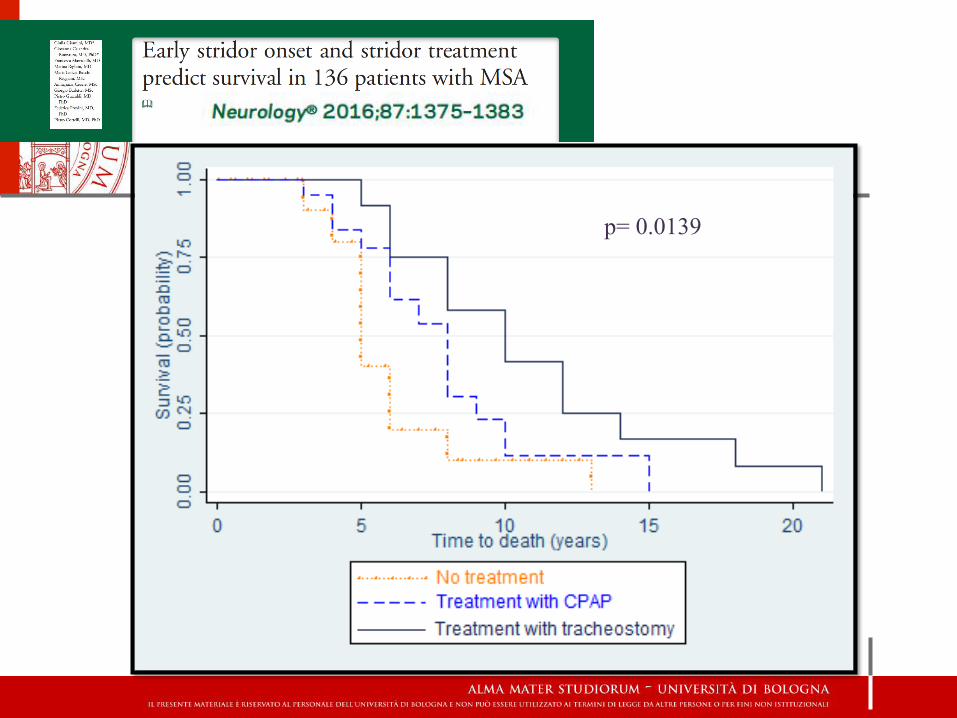
p= 0.0139

CLINICALPRESENTATION&NATURALHISTORY
� Motor(Parkinsonianorcerebellar)presentationismorecommonthanautonomicexcepturogenitaldysfunction
� Onset55-60yrs(range=33-83yrs)
� Meansurvival7-9yrswithsubstantialvariation
� InEuropeandUSA,MSA-pismorecommonthanMSA-c(60%vs40%)
� InJapanMSA-cismorecommonthanMSA-p(84%vs16%)
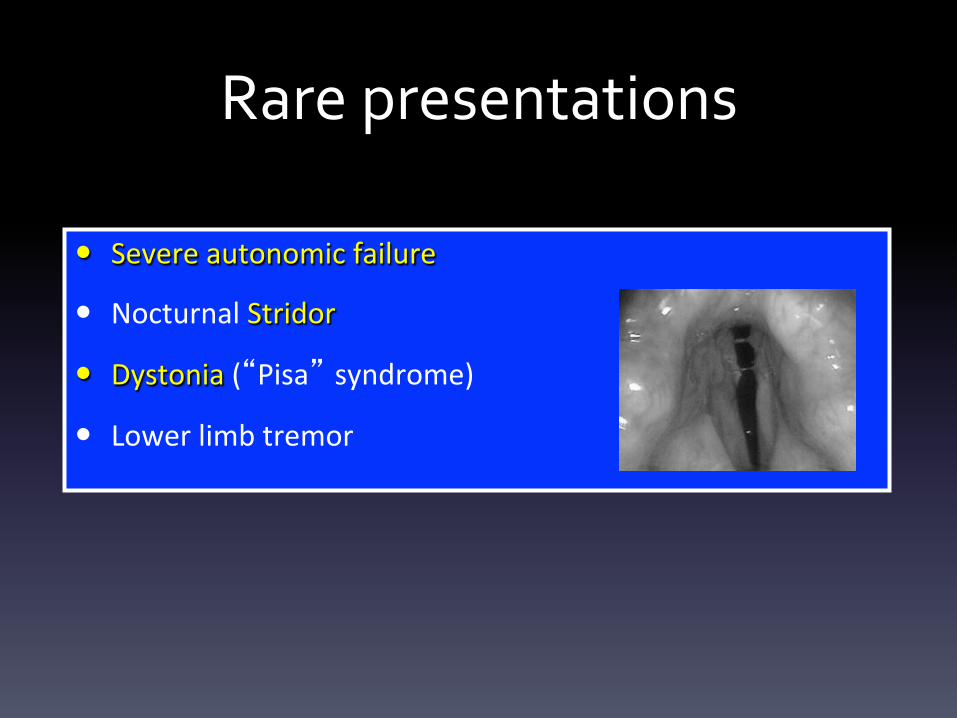
Rarepresentations
� Severeautonomicfailure
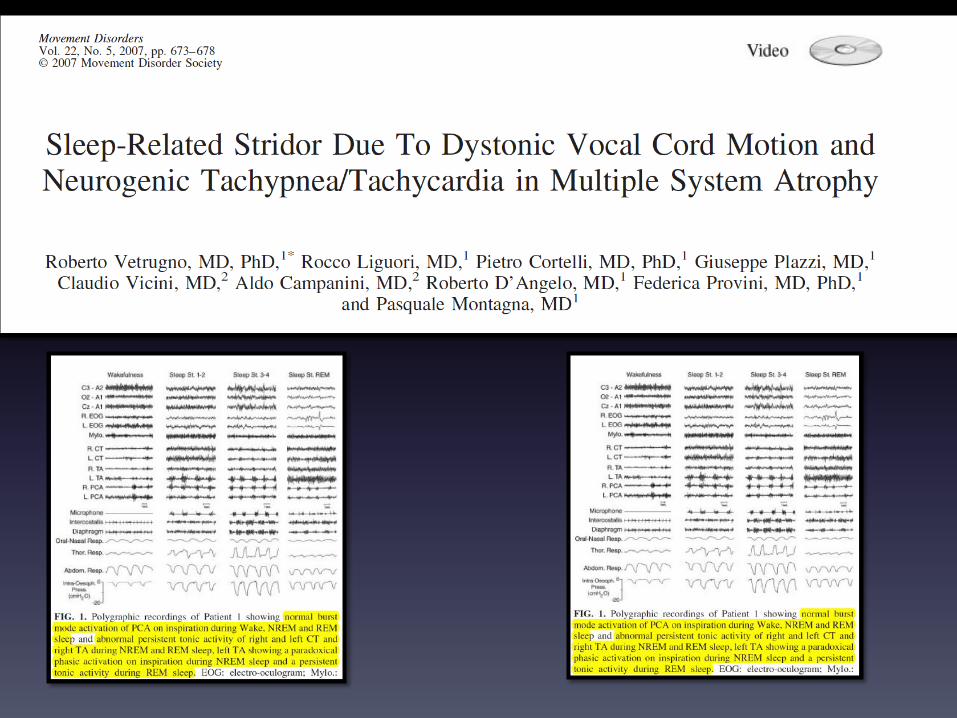
� NocturnalStridor
� Dystonia(“Pisa” syndrome)
� Lowerlimbtremor
Earlydiagnosis(<3yrs)
• Diagnosisiseasybutafter5yearsofdisease!
• Parkinsonianonset:“redflags”with>95%
specificityforMSA-Poccurafter3years
• Cerebellaronset:SCA1,2,3,6,7,12,17;ataxiawith
oculomotorapraxia(aprataxinmutation;fragile-X-
associatedtremorataxiasyndrome;FMR1genemutation
in4%ofMSA-c)
• Autonomiconset:synucleinopathies
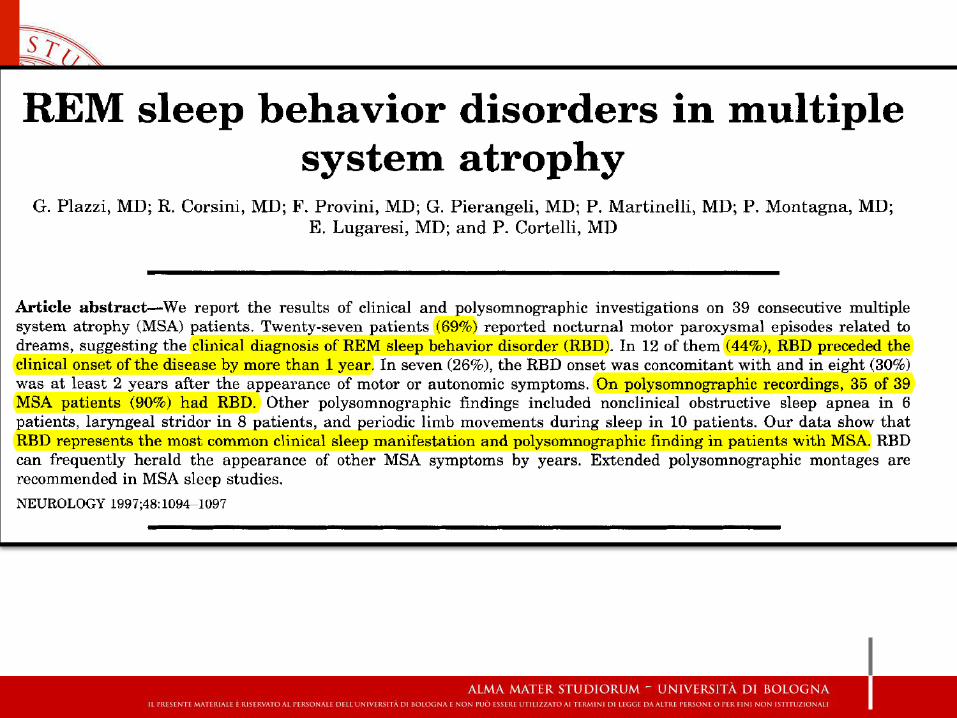
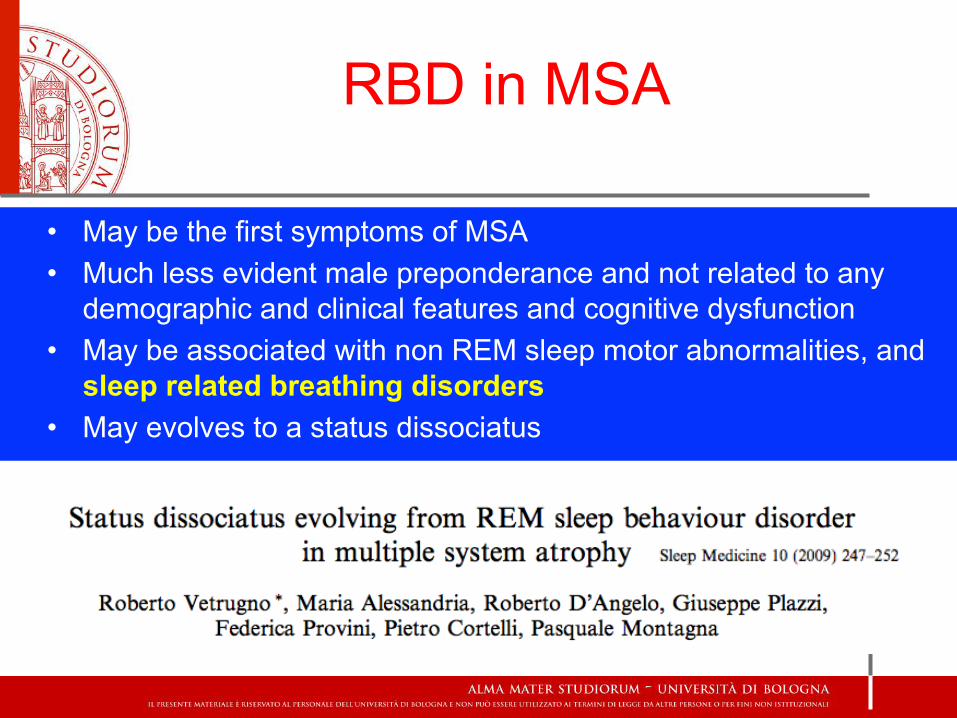
RBD in MSA
• May be the first symptoms of MSA • Much less evident male preponderance and not related to any
demographic and clinical features and cognitive dysfunction • May be associated with non REM sleep motor abnormalities, and
sleep related breathing disorders • May evolves to a status dissociatus
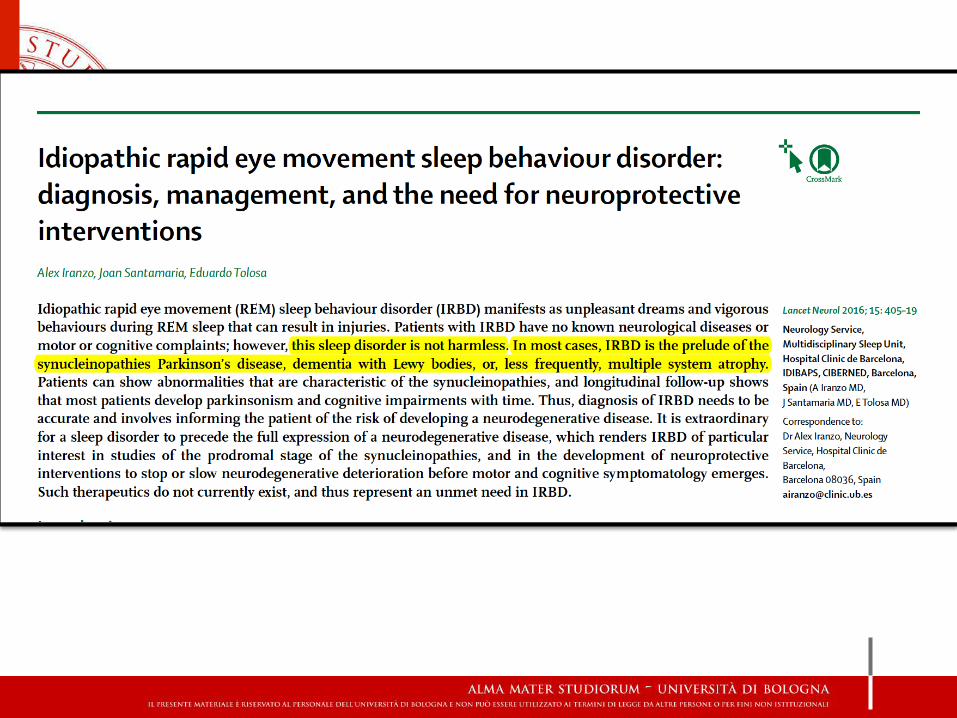
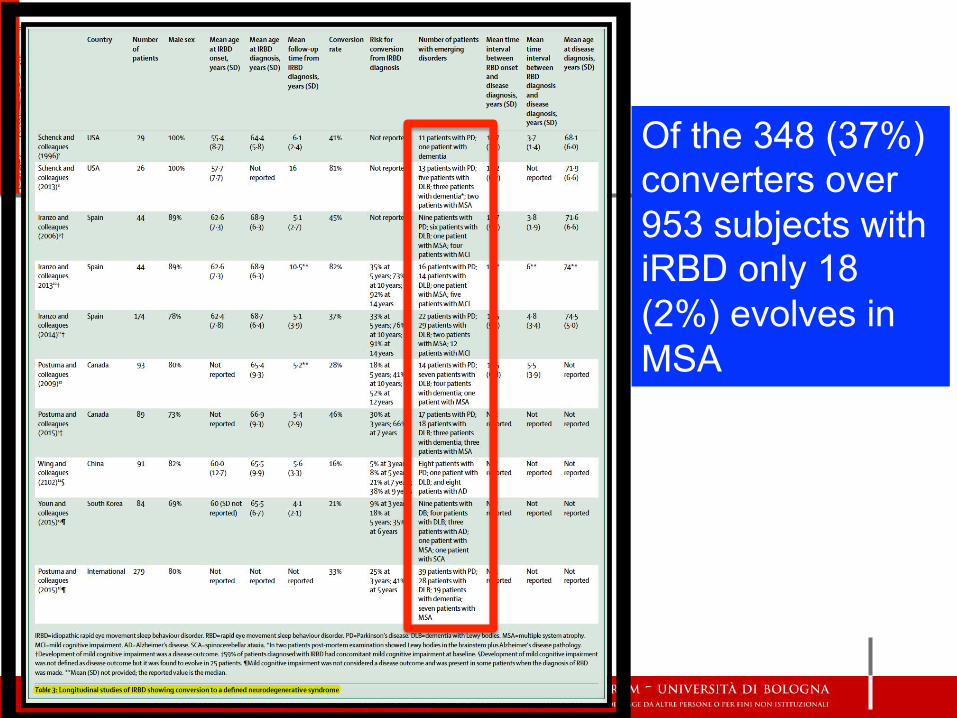
Of the 348 (37%) converters over 953 subjects with iRBD only 18 (2%) evolves in MSA
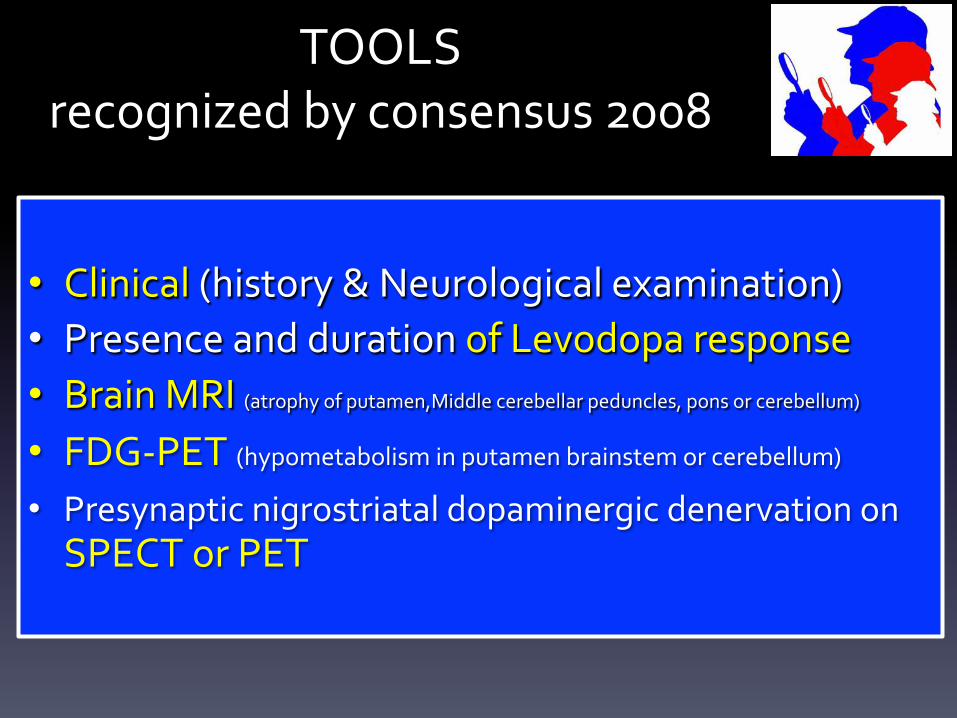
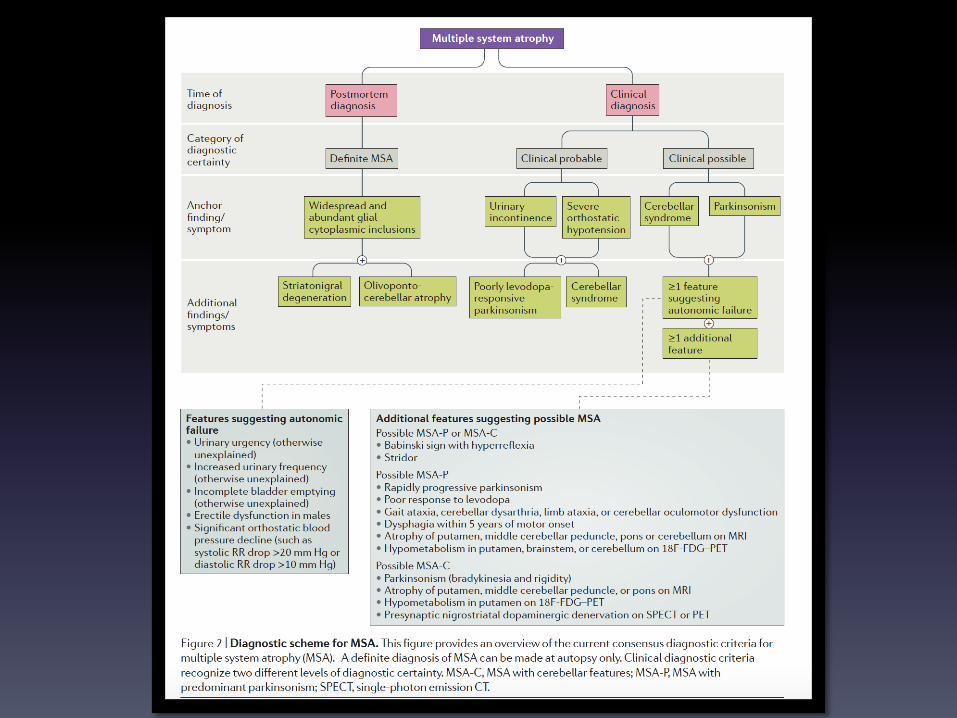
TOOLSrecognizedbyconsensus2008
• Clinical(history&Neurologicalexamination)• PresenceanddurationofLevodoparesponse• BrainMRI(atrophyofputamen,Middlecerebellarpeduncles,ponsorcerebellum)
• FDG-PET(hypometabolisminputamenbrainstemorcerebellum)
• PresynapticnigrostriataldopaminergicdenervationonSPECTorPET
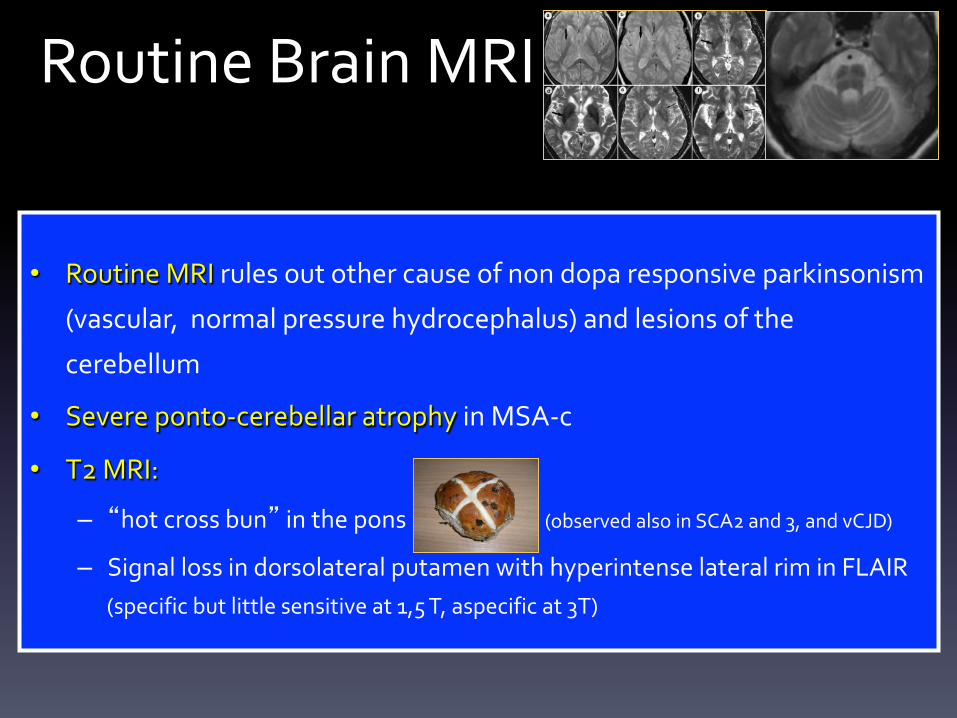
RoutineBrainMRI
• RoutineMRIrulesoutothercauseofnondoparesponsiveparkinsonism
(vascular,normalpressurehydrocephalus)andlesionsofthe
cerebellum
• Severeponto-cerebellaratrophyinMSA-c
• T2MRI:
– “hotcrossbun”inthepons(observedalsoinSCA2and3,andvCJD)
– SignallossindorsolateralputamenwithhyperintenselateralriminFLAIR(specificbutlittlesensitiveat1,5T,aspecificat3T)
BrainMRIDWI,spectroscopy,morphometry
• FractionalanisotropyandapparentdiffusioncoefficientchangesarepresentpriorofT2MRIalterationsandareusefultodifferentiateMSAfromPDandincaseofcerebellarpresentation
• Magneticresonancespectroscopy• Voxelbasedmorphometryandtractographyarenot
appropriatefordiagnosticwork-upbutofferresearchinsights
• Morphometricmeasurementsofmidbrain,ponscandistinguishMSA-pfromPSPandofsuperiorcerebellarpeduncleMSA-pfromPD
Functionalimaging
• PETwith18F-dopa(presynapticdopaminergicmarker)andwithraclopride(D1striatal)poorlydistinghishMSA-pfromPDandotherparkinsonism
• PET-FDGshowlowmetabolisminthebrainstemandcerebelluminMSA-c
• SPECT-DATSCAN(dopaminetransporter,nigro-striatalpathway)isuselessinMSA-pmaybeusefulincaseofcerebellar(MSA-c),autonomicandsleeponset
• SPECT-IBZM(D2striatalligand)littlevalue
OTHERTOOLS
• Autonomicfunctiontests– cardiovascularfunction– Bladder
• Sleepevaluation(polysomnography)• Olfactoryevaluation
• CardiacSPECT–MIBG(post-ganglioniccardiacdenervation)• Transcranialsonography
INVESTIGATIONS
• Eachofthemethodslistedhas
– onlysuboptimalaccurancyattheonsetofthedisease
– moststudieshavebeendoneinclinicallydefiniteMSAwhen
investigationshavelittlesignificanceinthediagnosisofMSA
Theconundrumoftheearlydiagnosis(<3yrs)ofMSA
ONSET
• SLEEP(RBD,others)
POSSIBLEDIAGNOSIS
• iRBD,PD,DLB,MSA
Theconundrumoftheearlydiagnosis(<3yrs)ofMSA
ONSET
• AUTONOMIC
POSSIBLEDIAGNOSIS
• PAF,AAG,PD,DLB,MSA
Theconundrumoftheearlydiagnosis(<3yrs)ofMSA
ONSET
• CEREBELLAR
POSSIBLEDIAGNOSIS
• ILOCA,SCA,FXTAS,MSA-C
Cerebellarsigns
• CerebellarAtaxiaoccursin64%ofMSA
• Limbkineticataxia,scanningdysarthriaandcerebellar
oculomotordisturbancesarealsocommon
Theconundrumoftheearlydiagnosis(<3yrs)ofMSA
ONSET
• PARKINSONISM
POSSIBLEDIAGNOSIS
• PD,MSAP,PSP,CBD
Parkinsonism
• Rigidity,bradykinesia,posturalinstabilityoccurin90%ofMSA• Restingtremorislessfrequent(10-30%comparedto60-70%
ofPD)• BenefitfromlevodopaisNOTsustainedbuttransientresponse
occurin30-40%ofMSAusinglargerdosagesthaninPD(facialdystoniaoccursmorefrequentlythanlimbdyskinesia)
• Progressionisfast(UPDRSIIImotorscore28%peryearinMSAvs4%inPD,Seppi2005;UMSARSIhystoryreview35%,UMSARSIIImotorscore57%,Geser2006)
Cognitive and MSA
• Cognitive impairment is not a feature of MSA and until recently would have been regarded as a reason to reconsider the diagnosis
• Studies with neuropathological ascertainment
of MSA, cognitive impairment has been recorded in 14–18% of cases
Cognitive and MSA
Cognitive impairment, consisting of visuospatial and constructional dysfunction, impairment of verbal fluency, dysexecutive syndrome and depression has been described to be more severe and widespread in patients with MSA-P than in patients with MSA-C.
MakinganearlydiagnosisofMSAisdifficultbutyoucangetitifyouhaveknowledge
ofsleep,autonomic,cerebellarandparkinsonian
disorders!!!
Takehomemessage