Intracoronary 17 β -Estradiol and the Inotropic Response to Dobutamine...
5
JOURNAL OF WOMEN’S HEALTH Volume 17, Number 9, 2008 © Mary Ann Liebert, Inc. DOI: 10.1089/jwh.2007.0768 Intracoronary 17-Estradiol and the Inotropic Response to Dobutamine in Postmenopausal Women Susanna Mak, M.D., Ph.D. Abstract Background: Gender differences with respect to clinical presentation and outcome of cardiovascular disease have prompted examination of sex-specific factors that may influence cardiovascular physiology and patho- physiology. The rationale for evaluating control of contractility by estrogen derives from preclinical data demon- strating that 17-estradiol (17-E 2 ) can attenuate the myocardial response to adrenergic stimulation. Methods: The effects of two doses of intracoronary 17-E 2 (150 and 300 ng/min) were tested on the left ven- tricular (LV) inotropic response to intravenous dobutamine in postmenopausal women who had undergone diagnostic cardiac catheterization. Peak positive LVdP/dt (LVdP/dt max ) was obtained from analysis of LV pressure recorded by a micromanometer catheter. Results: The study was terminated prematurely after the manufacturer stopped production of 17-E 2 , and data from 7 patients who had completed the study were analyzed. Intracoronary 17-E 2 had no effect on basal LVdP/dt max (1299 60 mm Hg/sec [mean SE] at control vs, 1299 46 mm Hg/sec with 17-E 2 ). Intra- coronary 17-E 2 also had no significant effect on the LVdP/dt max response to dobutamine (1672 95 mm Hg/sec with dobutamine alone vs. 1639 73 with dobutamine and 17-E 2 , p 0.51). Conclusions: In humans, no evidence of an acute moderate or large effect of 17-E 2 on adrenergically stimu- lated contractility was documented; a small effect size could not be excluded. 1499 Introduction G ENDER DIFFERENCES WITH RESPECT to clinical presentation and outcome of cardiovascular disease 1–4 have prompted examination of sex-specific factors that may in- fluence cardiovascular physiology. Sex steroid hormones, particularly estrogens, have generated significant attention, given the apparent link between menopause and the delayed development of disease in women. The presence of estrogen receptors (ER and ER) in human myocardium suggests that the heart may be subject to control by either genomic or nongenomic effects of ER stimulation. 5–8 The rationale for evaluating control of contractility by es- trogen derives from preclinical data demonstrating that ex- ogenous 17-estradiol (17-E 2 ) at supraphysiological con- centration decreases myocyte Ca 2 transients and exerts a negative inotropic effect in experimental myocardial prepa- rations. 5,9–11 At more physiologically relevant concentration, 17-E 2 can limit the increased availability of Ca 2 for con- traction in response to adrenergic stimulation. 5,12,13 A pur- ported mechanism for this observation is that the nonge- nomic stimulation of nitric oxide synthase 3 (NOS3) activity by estrogen, well described in the endothelium, 13–16 may be relevant in the myocyte. 17,18 In vivo, NOS activation is a well- understood mechanism that limits the contractile response to adrenergic stimulation. 19,20 A single human study 21 demonstrated that micronized sublingual 17-E 2 did not affect the basal left ventricular (LV) pressure-volume relationships in postmenopausal women. Thus far, no examination of the effect of estrogen on stimulated, directly measured cardiac function has been reported in humans. It was, therefore, hypothesized that administration of 17-E 2 , the most potent ligand of the ER, 22,23 would negatively modify the inotropic response to adrenergic stimulation with dobutamine in postmeno- pausal women. To minimize any systemic effect on load- ing conditions, 17-E 2 was administered by the intracoro- nary (i.c.) route. Clinical Cardiovascular Research Laboratory, Mount Sinai Hospital, and Division of Cardiology, Department of Medicine, University of Toronto, Ontario, Canada. This work is supported by a Grant-in-Aid, NA 5579, Heart and Stroke Foundation of Ontario. S.M. is supported by a New Investigator Award, Heart and Stroke Foundation of Ontario.
Transcript of Intracoronary 17 β -Estradiol and the Inotropic Response to Dobutamine...

JOURNAL OF WOMEN’S HEALTHVolume 17, Number 9, 2008© Mary Ann Liebert, Inc.DOI: 10.1089/jwh.2007.0768
Intracoronary 17�-Estradiol and the Inotropic Response to Dobutamine in Postmenopausal Women
Susanna Mak, M.D., Ph.D.
Abstract
Background: Gender differences with respect to clinical presentation and outcome of cardiovascular diseasehave prompted examination of sex-specific factors that may influence cardiovascular physiology and patho-physiology. The rationale for evaluating control of contractility by estrogen derives from preclinical data demon-strating that 17�-estradiol (17�-E2) can attenuate the myocardial response to adrenergic stimulation.Methods: The effects of two doses of intracoronary 17�-E2 (150 and 300 ng/min) were tested on the left ven-tricular (LV) inotropic response to intravenous dobutamine in postmenopausal women who had undergonediagnostic cardiac catheterization. Peak positive LV�dP/dt (LV�dP/dtmax) was obtained from analysis of LVpressure recorded by a micromanometer catheter.Results: The study was terminated prematurely after the manufacturer stopped production of 17�-E2, and datafrom 7 patients who had completed the study were analyzed. Intracoronary 17�-E2 had no effect on basalLV�dP/dtmax (1299 � 60 mm Hg/sec [mean � SE] at control vs, 1299 � 46 mm Hg/sec with 17�-E2). Intra-coronary 17�-E2 also had no significant effect on the LV�dP/dtmax response to dobutamine (1672 � 95 mmHg/sec with dobutamine alone vs. 1639 � 73 with dobutamine and 17�-E2, p � 0.51).Conclusions: In humans, no evidence of an acute moderate or large effect of 17�-E2 on adrenergically stimu-lated contractility was documented; a small effect size could not be excluded.
1499
Introduction
GENDER DIFFERENCES WITH RESPECT to clinical presentationand outcome of cardiovascular disease1–4 have
prompted examination of sex-specific factors that may in-fluence cardiovascular physiology. Sex steroid hormones,particularly estrogens, have generated significant attention,given the apparent link between menopause and the delayeddevelopment of disease in women. The presence of estrogenreceptors (ER� and ER�) in human myocardium suggeststhat the heart may be subject to control by either genomic ornongenomic effects of ER stimulation.5–8
The rationale for evaluating control of contractility by es-trogen derives from preclinical data demonstrating that ex-ogenous 17�-estradiol (17�-E2) at supraphysiological con-centration decreases myocyte Ca2� transients and exerts anegative inotropic effect in experimental myocardial prepa-rations.5,9–11 At more physiologically relevant concentration,17�-E2 can limit the increased availability of Ca2� for con-
traction in response to adrenergic stimulation.5,12,13 A pur-ported mechanism for this observation is that the nonge-nomic stimulation of nitric oxide synthase 3 (NOS3) activityby estrogen, well described in the endothelium,13–16 may berelevant in the myocyte.17,18 In vivo, NOS activation is a well-understood mechanism that limits the contractile responseto adrenergic stimulation.19,20
A single human study21 demonstrated that micronizedsublingual 17�-E2 did not affect the basal left ventricular(LV) pressure-volume relationships in postmenopausalwomen. Thus far, no examination of the effect of estrogenon stimulated, directly measured cardiac function has beenreported in humans. It was, therefore, hypothesized thatadministration of 17�-E2, the most potent ligand of theER,22,23 would negatively modify the inotropic response toadrenergic stimulation with dobutamine in postmeno-pausal women. To minimize any systemic effect on load-ing conditions, 17�-E2 was administered by the intracoro-nary (i.c.) route.
Clinical Cardiovascular Research Laboratory, Mount Sinai Hospital, and Division of Cardiology, Department of Medicine, Universityof Toronto, Ontario, Canada.
This work is supported by a Grant-in-Aid, NA 5579, Heart and Stroke Foundation of Ontario. S.M. is supported by a New InvestigatorAward, Heart and Stroke Foundation of Ontario.

Materials and Methods
Postmenopausal women referred for elective diagnosticheart catheterization to evaluate a chest pain syndrome par-ticipated in this study. Patients with any history of uterine,ovarian, or breast cancer were specifically excluded. Post-menopausal women were clinically defined as being � 50years of age with cessation of menses � 1 year or as havinghad bilateral surgical oophorectomy; status was subse-quently confirmed by measurement of the sex hormone pro-file. All patients underwent two-dimensional echocardiog-raphy to exclude valvular heart disease and any evidence ofLV systolic and diastolic dysfunction. Patients were excludedif they received hormone replacement therapy (HRT) or re-lated agents within the preceding year. All medications werewithheld for 24 hours prior to the study.
This study was approved by the Mount Sinai Ethics Re-view Board for experimentation involving human subjects,and all patients gave written informed consent.
Cardiac catheterization procedure and hemodynamic measurements
Patients were studied after diagnostic left and right heartcatheterization via the femoral approach. A 7F micro-manometer-tipped catheter (Millar Instruments, Houston,TX) was advanced via the right femoral artery into the LVfor measurement of LV pressure. A 6F angiographic cathe-ter was advanced from the opposite femoral artery to the os-tium of the left main coronary artery. When 17�-E2 was notinfusing, the catheter was continuously flushed with the ve-hicle for hormone infusion (0.9% saline) at a rate of 1.5mL/min with a Harvard infusion pump. Femoral arterypressure was monitored via the 7F sidearm sheath that wasused to insert the 6F angiographic catheter.
The electrocardiogram (ECG), femoral artery pressure, LVpressure, and LV peak positive dP/dt (LV�dP/dtmax) wererecorded on a strip-chart recorder. Each description of heartrate (HR) and blood pressure (systolic blood pressure [SBP],diastolic blood pressure [DBP], mean arterial pressure[MAP]) represents the mean of � 15 consecutive beats. TheECG, LV pressure, and LV�dP/dtmax were also continu-ously digitally recorded (1000 Hz) online. LV�dP/dtmax LVsystolic pressure (LVSP) LV end-diastolic pressure (LVEDP)were calculated offline with a customized software program(Labview version 5.0; National Instruments Corp, Austin,TX). The time constant of isovolumic relaxation (tau, �) wasalso recorded by the logarithmic method. The mean of � 50consecutive beats was used for analysis. These methods arewell established in our laboratory.
Study protocol
All patients received heparin (5000 U i.v.) and a rest pe-riod after placement of the catheters. Measurements weremade at each of five sequential conditions. Condition 1 (con-trol), the intracoronary infusion of the vehicle solution (0.9%saline) at 1.5 mL/min. Condition 2 (Dob); dobutamine (EliLilly and Co., Indianapolis, IN) diluted in 5% dextrose in wa-ter infused via a systemic vein at a rate of 2.5 mg/kg/min.This dose achieved a �25% or more increase in LV�dP/dt-max in all patients and was infused until LV�dP/dtmax re-mained stable (�5%) for three consecutive measurements,
each separated by 1 min. Condition 3 (recontrol), after dobu-tamine infusion was stopped for � 10 minutes and peakLV�dP/dtmax was similar to baseline (within 10%). Condi-tion 4 (17�-E2), 17�-E2 (17�OH-estradiol, Clinalfa, micellarpreparation, 100 �g vial) diluted in vehicle solution and in-fused into the left main coronary artery for 10 minutes at arate of 1.5 mL/min and at a dose of either 150 ng/min or300 ng/min. It has been demonstrated previously that theintracoronary infusion of 17�-E2 at 150 ng/min yields phys-iological levels of 17�-E2 in the coronary sinus, similar to val-ues found in premenopausal women during the late follicu-lar and early luteal phase of the menstrual cycle.14 Condition5 (Dob � 17�-E2): During the continued infusion of 17�-E2,dobutamine (2.5 mg/kg/min) was reinfused i.v. until peakLV�dP/dtmax remained stable (�5%) for three consecutivemeasurements, each separated by 1 minute. We have previ-ously demonstrated in patients with normal LV function thatthere is no change in the inotropic response to sequential in-fusions of dobutamine.24 Final measurements of peakLV�dP/dtmax during the reinfusion of dobutamine occurredafter 17�-E2 had infused for at least 15 minutes in total.
Measurement of sex hormone profile
Serum was obtained at control and after the Dob � 17�-E2 condition for determination of 17�-E2, progesterone, andtestosterone levels. Testosterone, which is normally presentin postmenopausal women, was measured to ensure thatsubjects were not abnormally androgenized and erroneouslydefined as postmenopausal. All samples were stored frozenat �70°C prior to analysis. Measurements were made withstandard radioimmunoassay (RIA) methods.
Statistical analysis
All data are presented as mean � SEM. A statistical soft-ware package was used for the analysis (Statview, Cary, NC).Hemodynamic measurements at each condition were com-pared using a one-way ANOVA for repeated measures. Posthoc pairwise comparisons of each condition to control wereperformed with a Bonferroni/Dunn test (p � 0.005 requiredfor significance). Dobutamine responses (Dob vs. Dob � 17�-E2) were also compared using a paired t test. A value of p �0.05 was required for statistical significance.
We have demonstrated previously that the infusion ofdobutamine yields at least a 30 � 15% (SD) increase inLV�dP/dtmax. A sample size of 15 patients would havepower of � 0.8 to detect a 30% change in the LV�dP/dtmax
response to dobutamine.
Results
The study was stopped prematurely in 2006 after pro-duction of the micellar preparation of 17�-E2 was stopped.The micellar preparation enabled reconstitution of 17�-E2 inaqueous solution; otherwise, 17�-E2 is lipophilic and re-quires dissolution in absolute ethanol. No other similarpreparation of 17�-E2 suitable for intracoronary infusion inhumans is available. Results from 7 postmenopausal women(age 67 � 1 years) who completed the protocol prior to de-pletion of the supply of 17�-E2 are presented here.
In these patients, the mean LV internal dimension in di-astole was 46 � 4 mm, posterior wall thickness in diastole
MAK1500

was 9.0 � 0.3 mm, interventricular septum thickness was 9.0mm, and LV mass index25 was 80.4 � 11.2 g/m2. Three pa-tients had a single stenosis of �50% of the right coronaryartery, and 4 patients had no evidence of epicardial coronaryartery disease. None of the patients had diabetes mellitus,and all patients were nonsmokers. Three patients had treatedhypertension, and four had hypercholesterolemia controlledby medical therapy. Mean body mass index (BMI) was 27.5 �1.7 kg/m2. Five patients received medical therapy with as-pirin, 5 with HMG CoA reductase inhibitors, 3 with beta-blockers, and 3 with angiotensin-converting enzyme (ACE)inhibitors or angiotensin receptor blocking agents.
Effect of estrogen on serum sex hormone profile
All patients at the control condition had 17�-E2 levels be-low the detection limit of our assay (�20 pmol/L). Serumprogesterone was below the detection limit of the assay in 4patients (�0.64 nmol/L) and 0.79 � 0.06 in the 3 others.Serum testosterone was 0.9 � 0.1 nmol/L. Three patients re-ceived 150 ng/min and 4 patients received 300 ng/min of17�-E2. In the Dob � 17�-E2 condition, with the intracoro-nary infusion of 17�-E2, the serum 17�-E2 level increased to
59 � 29 pmol/L in patients receiving 150 ng/mL and to142 � 21 pmol/L in patients receiving 300 ng/mL 17�-E2.
In 1 postmenopausal woman, to understand the organ-spe-cific concentration of 17�-E2 achieved, 17�-E2 was measuredin effluent from the coronary sinus (CS) in response to the i.c.infusion of 17�-E2. At 150 ng/min, CS 17�-E2 was 185 pmol/L,whereas at 300 ng/min, CS 17�-E2 was 1361 pmol/L.
Effect of estrogen on basal LV�dP/dtmax
and hemodynamics
The i.c. infusion of 17�-E2 at either 150 or 300 ng/mL hadno effect on resting LV�dP/dtmax At control, LV�dP/dtmax
was 1299 � 60 mm Hg/sec, and after the infusion of 17�-E2,LV�dP/dtmax was 1299 � 46 mm Hg/sec. The mean ab-solute difference in LVdP/dtmax between the control and17�-E2 condition was �0.2 � 31 mm Hg/sec, p � 0.99 Therewere also no effects of i.c. 17�-E2 on HR, SBP, DBP, MAP,LVSP, LVEDP, or tau (Table 1).
Effect of estrogen on inotropic response to dobutamine
Intravenous dobutamine was associated with the antici-pated significant increase in LV�dP/dtmax (28 � 7%) (Table
ESTROGEN AND CONTRACTILITY 1501
TABLE 1. EFFECT OF DOBUTAMINE WITH AND WITHOUT INTRACORONARY 17�-ESTRADIOL
Control Dobutamine Recontrol 17�-estradiol 17�-estradiol � dobutamine
Heart rate (min�1) 61 � 4 68 � 5* 61 � 4 61 � 3 67 � 4*SBPa (mm Hg) 151 � 5 149 � 9 145 � 6 150 � 6 148 � 8DBP (mm Hg) 62 � 2 57 � 2 59 � 2 62 � 2 59 � 2MAP (mm Hg) 95 � 3 90 � 4 91 � 3 94 � 3 92 � 3LVSP (mm Hg) 148 � 5 147 � 9 143 � 6 148 � 6 150 � 8LVEDP (mm Hg) 16 � 2 17 � 2 17 � 2 17 � 2 17 � 2LV � dP/dt (mm Hgs�1) 1299 � 60 1672 � 95* 1306 � 56 1299 � 46 1639 � 73*Tau (msec) 49 � 3 42 � 3* 47 � 2 47 � 2 41 � 3*
aSBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; LVSP, left ventricular systolic pressure; LVEDP,left ventricular end-diastolic pressure; LV � dP/dt, left ventricular peak dP/dt.
*p � 0.05 vs. control.
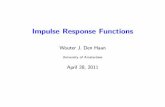
FIG. 1. The effect of two doses of intracoronary (i.c.) 17�-estradiol (open circles, 150 ng/min; filled circles, 300 ng/min)on left ventricular peak positive dP/dt (LV�dP/dtmax) responses to intravenous dobutamine. Individual data, mean, andSEM are shown.

1). The i.c. infusion of 17�-E2 had no effect on theLV�dP/dtmax response to dobutamine (Fig. 1). The mean in-crease in LV�dP/dtmax was 373 � 47 mm Hg/sec withdobutamine alone and 340 � 24 mm Hg/sec with dobuta-mine and 17�-E2, p � 0.51. The absolute difference inLV�dP/dtmax between the inotropic response to dobuta-mine alone and the response to dobutamine and 17�-E2
[(Dob � 17�-E2) � Dob] was �32 � 47 mm Hg/sec. Therewas no evidence of a dose-response relationship between pa-tients receiving 150 ng/min or 300 ng/min 17�-E2 and theinotropic response to dobutamine (Fig. 1). There was also noapparent relationship between the presence of coronaryartery disease and the effect of 17�-E2 on dobutamine re-sponses (data not shown).
Intravenous dobutamine was associated with a small in-crease in HR, a shortening of tau, and no significant effecton blood pressure. The i.c. infusion of 17�-E2 at either 150or 300 ng/mL had no effect on the HR, blood pressure, ortau responses to dobutamine.
Discussion
This experiment was terminated after production of themicellar preparation of 17�-E2 was summarily discontinuedby the manufacturer, necessitating evaluation of the data af-ter enrollment of 7 patients. Although short of the antici-pated sample size of 15 patients, the central finding of thisstudy is that the acute i.c. administration 17�-E2 to post-menopausal women did not discernibly influence basal con-tractility or the inotropic response to adrenergic stimulationwith dobutamine. A small effect of 17�-E2 on the inotropicresponse to dobutamine could not be excluded.
The concept that estrogen may exert a negative inotropiceffect on basal and stimulated LV function has been estab-lished in nonhuman studies.5,9–13 In humans however, Hay-ward et al.21 found no effect of micronized sublingual 17�-E2 at supraphysiological concentration on the resting LVpressure-volume relationship. In the current study, 17�-E2
was also employed as the most potent ligand of the ER,22,23
and administered at two doses by the i.c. route to minimizesystemic effects. Similar to Hayward’s results, no apparenteffect on basal LV�dP/dtmax was observed. Extending theobservations to examine the inotropic response to dobuta-mine, the addition of i.c. 17�-E2 to dobutamine yielded amean decrease in LV�dP/dtmax of 32 mm Hg/sec comparedwith dobutamine alone. The observed difference representsattenuation of the inotropic response to dobutamine by 17�-E2 of approximately 10%, an effect size that was smaller thanhypothesized and did not reach statistical significance. Basedon the response to dobutamine observed, the probability oftype II error thus falsely accepting the null hypothesis is ap-proximately 0.1. If these observations represented a small butreal effect, to have adequate power, a sample size of over 70patients would have been required.
The rationale to study postmenopausal women was thatmyocardial ERs were more likely to be present, but at lowlevels of endogenous stimulation.14,26 The concentration of17�-E2 employed has been shown previously to enhance en-dothelium-dependent vasodilatation in the coronary circu-lation via an NO-dependent mechanism in a population ofwomen similar to those in the present study.14,15 I also con-firmed that infusion of 17�-E2 as performed in the current
study achieved the anticipated supraphysiological 17�-E2
concentration measured in the CS effluent. The lack of a re-lationship between the concentration of 17�-E2 administeredand the inotropic response to dobutamine further diminishesthe possibility that a small treatment effect was missed. Thus,17�-E2 has no or minimal nongenomic effects on modulationof adrenergically stimulated contractility in humans withnormal LV function.
The absence of an acute effect of estrogen does not indi-cate that sex hormone status is irrelevant to cardiac function.Determinants of EC coupling may be influenced by extendedexposure to estrogen.27 Perhaps the most significant influ-ence that estrogen may exert over LV function is by meansof the likely genomic effect on LV mass and chamber re-modeling.28,29 The apparent permissive effect of age andpostmenopausal status on increases in LV mass and hyper-trophy30 is supportive of estrogen-mediated limitation of re-modeling demonstrated in preclinical experiments. In hu-mans, pressure overload hypertrophy8 and myopathicdisease7 are associated with upregulation of myocardial ER�;moreover, specific polymorphisms of ER� may be determi-nants of LV mass.31 These observations invoke the questionof whether an acute, nongenomic ER-mediated effect on car-diac function might be observed in these populations at aphysiologically relevant 17�-E2 concentration. The womenin the current study had no evidence of LV hypertrophy, andLV mass was documented to be in the normal range. Finally,the potential role of sex steroid hormones and differences incardiac function between men and women are also likely notlimited with estrogen. Testosterone appears to exert diver-gent effects compared to estrogen on LV function andmass.30,32,33
There are limitations to the current study. The effect ofpremature termination of this study and resultant samplesize have been discussed. The assumption that postmeno-pausal women are most likely to have myocardial ER at lowlevels of endogenous stimulation may be challenged, giventhat the ER expression was not directly measured. Preclini-cal experiments demonstrating a negative inotropic effect of17�-E2 used supraphysiological concentrations that may nothave been achieved in this study. Additionally, the durationof the 17�-E2 was approximately 15 minutes and may havebeen too brief to observe an effect.
Sex hormone milieu is likely important to LV chambermorphology and adaptation to hemodynamic overload. Inthe current study, however, no evidence for an acute effectof 17�-E2 on adrenergically stimulated contractility in post-menopausal women with normal LV function was docu-mented; a small effect size could not be excluded.
Disclosure Statement
There are no conflicts of interest to disclose.
References
1. Vaccarino V, Rathore SS, Wenger NK, et al. Sex and racialdifferences in the management of acute myocardial infarc-tion, 1994 through 2002. N Engl J Med 2005;353:671–682.
2. Albert CM, McGovern BA, Newell JB, Ruskin JN. Sex dif-ferences in cardiac arrest survivors. Circulation 1996;93:1170–1176.
MAK1502

3. Ho KK, Pinsky JL, Kannel WB, Levy D. The epidemiologyof heart failure: The Framingham Study. J Am Coll Cardiol1993;22:6A–13A.
4. Johansen H, Strauss B, Arnold JM, Moe G, Liu P. On the rise:The current and projected future burden of congestive heartfailure hospitalization in Canada. Can J Cardiol 2003;19:430–435.
5. Meyer R, Linz KW, Surges R, et al. Rapid modulation of L-type calcium current by acutely applied oestrogens in iso-lated cardiac myocytes from human, guinea-pig and rat. ExpPhysiol 1998;83:305–321.
6. Brandenberger AW, Tee MK, Lee JY, Chao V, Jaffe RB. Tis-sue distribution of estrogen receptors alpha (ER-alpha) andbeta (ER-beta) mRNA in the midgestational human fetus. JClin Endocrinol Metab 1997;82:3509–3512.
7. Mahmoodzadeh S, Eder S, Nordmeyer J, et al. Estrogen re-ceptor alpha up-regulation and redistribution in humanheart failure. FASEB J 2006;20:926–934.
8. Nordmeyer J, Eder S, Mahmoodzadeh S, et al. Upregulationof myocardial estrogen receptors in human aortic stenosis.Circulation 2004;110:3270–3275.
9. Jiang C, Poole-Wilson PA, Sarrel PM, Mochizuki S, CollinsP, Macleod KT. Effect of 17 beta-oestradiol on contraction,Ca2� current and intracellular free Ca2� in guinea-pig iso-lated cardiac myocytes. Br J Pharmacol 1992;106:739–745.
10. Raddino R, Manca C, Poli E, Bolognesi R, Visioli O. Effectsof 17 beta-estradiol on the isolated rabbit heart. Arch IntPharmacodyn Ther 1986;281:57–65.
11. Sitzler G, Lenz O, Kilter H, La Rosee K, Bohm M. Investi-gation of the negative inotropic effects of 17 beta-oestradiolin human isolated myocardial tissues. Br J Pharmacol1996;119:43–48.
12. Li HY, Bian JS, Kwan YW, Wong TM. Enhanced responsesto 17beta-estradiol in rat hearts treated with isoproterenol:Involvement of a cyclic AMP-dependent pathway. J Phar-macol Exp Ther 2000;293:592–598.
13. Patterson E, Ma L, Szabo B, Robinson CP, Thadani U.Ovariectomy and estrogen-induced alterations in myocar-dial contractility in female rabbits: Role of the L-type cal-cium channel. J Pharmacol Exp Ther 1998;284:586–591.
14. Gilligan DM, Quyyumi AA, Cannon RO. Effects of physio-logical levels of estrogen on coronary vasomotor function inpostmenopausal women. Circulation 1994;89:2545–2551.
15. Guetta V, Quyyumi AA, Prasad A, Panza JA, Waclawiw M,Cannon RO. The role of nitric oxide in coronary vascular ef-fects of estrogen in postmenopausal women. Circulation1997;96:2795–2801.
16. Kim HP, Lee JY, Jeong JK, Bae SW, Lee HK, Jo I. Nonge-nomic stimulation of nitric oxide release by estrogen is me-diated by estrogen receptor alpha localized in caveolae.Biochem Biophys Res Commun 1999;263:257–262.
17. Nuedling S, Kahlert S, Loebbert K, et al. 17 Beta-estradiolstimulates expression of endothelial and inducible NO syn-thase in rat myocardium in vitro and in vivo. Cardiovasc Res1999;43:666–674.
18. Nuedling S, Karas RH, Mendelsohn ME, et al. Activation ofestrogen receptor beta is a prerequisite for estrogen-depen-dent upregulation of nitric oxide synthases in neonatal ratcardiac myocytes. FEBS Lett 2001;502:103–108.
19. Hare JM. Nitric oxide and excitation-contraction coupling. JMol Cell Cardiol 2003;35:719–729.
20. Hare JM, Givertz MM, Creager MA, Colucci WS. Increasedsensitivity to nitric oxide synthase inhibition in patients withheart failure. Potentiation of �-adrenergic inotropic respon-siveness. Circulation 1998;97:161–166.
21. Hayward CS, Kalnins WV, Kelly RP. Acute effects of 17beta-estradiol on ventricular and vascular hemodynamics in post-menopausal women. Am J Physiol Heart Circ Physiol2000;279:H2277–2284.
22. Weihua Z, Andersson S, Cheng G, Simpson ER, Warner M,Gustafsson JA. Update on estrogen signaling. FEBS Lett2003;546:17–24.
23. Gustafsson JA. What pharmacologists can learn from recentadvances in estrogen signalling. Trends Pharmacol Sci2003;24:479–485.
24. Mak S, Newton GE. Vitamin C augments the inotropic re-sponse to dobutamine in humans with normal left ventric-ular function. Circulation 2001;103:826–830.
25. Park SH, Shub C, Nobrega TP, Bailey KR, Seward JB. Two-dimensional echocardiographic calculation of left ventricu-lar mass as recommended by the American Society ofEchocardiography: Correlation with autopsy and M-modeechocardiography. J Am Soc Echocardiogr 1996;9:119–128.
26. Gilligan DM, Badar DM, Panza JA, Quyyumi AA, CannonRO. Acute vascular effects of estrogen in postmenopausalwomen. Circulation 1994;90:786–791.
27. Johnson BD, Zheng W, Korach KS, Scheuer T, Catterall WA,Rubanyi GM. Increased expression of the cardiac L-type cal-cium channel in estrogen receptor-deficient mice. J GenPhysiol 1997;110:135–140.
28. van Eickels M, Grohe C, Cleutjens JP, Janssen BJ, WellensHJ, Doevendans PA. 17Beta-estradiol attenuates the devel-opment of pressure-overload hypertrophy. Circulation2001;104:1419–1423.
29. Babiker FA, De Windt LJ, van Eickels M, et al. 17Beta-estra-diol antagonizes cardiomyocyte hypertrophy by au-tocrine/paracrine stimulation of a guanylyl cyclase A re-ceptor-cyclic guanosine monophosphate-dependent proteinkinase pathway. Circulation 2004;109:269–276.
30. Hayward CS, Webb CM, Collins P. Effect of sex hormoneson cardiac mass. Lancet 2001;357:1354–1356.
31. Peter I, Shearman AM, Vasan RS, et al. Association of es-trogen receptor beta gene polymorphisms with left ventric-ular mass and wall thickness in women. Am J Hypertens2005;18:1388–1395.
32. Golden KL, Marsh JD, Jiang Y, Brown T, Moulden J. Go-nadectomy of adult male rats reduces contractility of iso-lated cardiac myocytes. Am J Physiol Endocrinol Metab2003;285:E449–E453.
33. Golden KL, Marsh JD, Jiang Y, Moulden J. Acute actions oftestosterone on contractile function of isolated rat ventricu-lar myocytes. Eur J Endocrinol 2005;152:479–483.
Address reprint requests to:Susanna Mak, M.D., Ph.D.
Mount Sinai Hospital, Suite 1542600 University Avenue
Toronto, OntarioCanada M5G 1X5
E-mail: [email protected]
ESTROGEN AND CONTRACTILITY 1503