Immunoreactive trypsin and a comparison of two ΔF508 mutation analyses in newborn screening for...
11
Screening, 2 (1993) 1-l 1 0 1993 Elsevier Science Publishers B.V. All rights reserved 0925-6164/93/$06.00 SCREEN 00047 Immunoreactive trypsin and a comparison of two AF508 mutation analyses in newborn screening for cystic fibrosis: An anonymous pilot study in Denmark Bent Nmgaard-Pedersen”, Estrid Hargdall”, Antti Iitigb, Jmgen Arendsa, Patrik Dahlen” and Jens Vuusta “Laboratory of Molecular Biology and Department of Clinical Biochemistry, Statens Seruminstitut. Copenhagen, Denmark, bDepartment of Biochemistry, University of Turku, Turku, Finland and c Wdac Oy, Tietokatu 2, Turku, Finland (Accepted 7 December 1992) A total of 1081 newborn screening cards were anonymously selected for cystic fibrosis (CF) screening by quantitation of immunoreactive trypsin (IRT, Delfia) and by AF508 mutational analyses using polymerase chain reaction followed by both gel retardation test and time- resolved fluorescence hybridization assay (Delfia). The IRT values showed a log normal distribution and was significantly higher in girls than boys and ic 28 carriers compared with 1052 normals. In 12 newborns corresponding to 1.02% an IRT concentration greater than 70 pg/l was found. One of these was a AF508 homozygote with an IRT concentration of 380 pg/l. A comparison between the two types of AF’508 mutational analyses gave identical results (1052 normals, 28 heterozygotes, and one homozy- gote), i.e., a carrier frequency of 1:38.6. However, the Delfia AF508 assay was easier to perform and the various controls makes the assay more reliable. In future newborn CF screening programs we therefore recommend Delfia IRT followed by Delfia AF508 analyses for IRT values greater than 70 pg/l. Key wor&: Cystic fibrosis; Newborn; Immunoreactive trypsin; Polymerase chain reaction Introduction Quantitation of immunoreactive trypsin (IRT) in dried filter paper blood speci- mens from newborns taken 4-6 days after birth has been used in screening for cystic Correspondence: Dr. Bent Nergaard-Pedersen, Statens Seruminstitut, Department of Clinical Biochem- istry, Artillerivej 5, DK-2300 Copenhagen S, Denmark.
Transcript of Immunoreactive trypsin and a comparison of two ΔF508 mutation analyses in newborn screening for...

Screening, 2 (1993) 1-l 1 0 1993 Elsevier Science Publishers B.V. All rights reserved 0925-6164/93/$06.00
SCREEN 00047
Immunoreactive trypsin and a comparison of two AF508 mutation analyses in newborn screening for
cystic fibrosis: An anonymous pilot study in Denmark
Bent Nmgaard-Pedersen”, Estrid Hargdall”, Antti Iitigb, Jmgen Arendsa, Patrik Dahlen” and Jens Vuusta
“Laboratory of Molecular Biology and Department of Clinical Biochemistry, Statens Seruminstitut. Copenhagen, Denmark, bDepartment of Biochemistry, University of Turku, Turku, Finland and c Wdac
Oy, Tietokatu 2, Turku, Finland
(Accepted 7 December 1992)
A total of 1081 newborn screening cards were anonymously selected for cystic fibrosis (CF) screening by quantitation of immunoreactive trypsin (IRT, Delfia) and by AF508 mutational analyses using polymerase chain reaction followed by both gel retardation test and time- resolved fluorescence hybridization assay (Delfia).
The IRT values showed a log normal distribution and was significantly higher in girls than boys and ic 28 carriers compared with 1052 normals. In 12 newborns corresponding to 1.02% an IRT concentration greater than 70 pg/l was found. One of these was a AF508 homozygote with an IRT concentration of 380 pg/l. A comparison between the two types of AF’508 mutational analyses gave identical results (1052 normals, 28 heterozygotes, and one homozy- gote), i.e., a carrier frequency of 1:38.6. However, the Delfia AF508 assay was easier to perform and the various controls makes the assay more reliable.
In future newborn CF screening programs we therefore recommend Delfia IRT followed by Delfia AF508 analyses for IRT values greater than 70 pg/l.
Key wor&: Cystic fibrosis; Newborn; Immunoreactive trypsin; Polymerase chain reaction
Introduction
Quantitation of immunoreactive trypsin (IRT) in dried filter paper blood speci- mens from newborns taken 4-6 days after birth has been used in screening for cystic
Correspondence: Dr. Bent Nergaard-Pedersen, Statens Seruminstitut, Department of Clinical Biochem- istry, Artillerivej 5, DK-2300 Copenhagen S, Denmark.

2
fibrosis (CF) [1,4,7,14]. However, about 1% unaffected infants have raised IRT levels in the neonatal period (false positives) leading to new blood sampling, sweat tests and considerable anxiety. As a result of the characterization of the cystic fibrosis gene [8] and the discovery of the common mutation AF508 [9] a new screening strategy is possible [7]. The newborn CF screening protocol, also called the two- tiered IRT and DNA approach, involves primary IRT analyses of all filter paper blood samples followed by mutational examination only of samples with elevated IRT levels. This novel approach is especially interesting in Denmark where this mutation has been found among 88% of the CF patients [lo].
We have, therefore, carried out an anonymous pilot study in newborns with simultaneous analysis of IRT and AF508 on filter paper blood specimens in order to make a basis for the design of a future non-anonymous prospective screening in newborns. Furthermore, we have compared two different types of mutation analyses.
Materials and Methods
Blood spot specimens A total of 1081 filter paper blood spots were collected consecutively and anony-
mously from the routine newborn screening cards (PKU cards) used for PKU and TSH screening in Denmark. The newborn screening laboratory receives about 60,000 samples per year. These samples are taken 4-6 days after birth and received in the laboratory 1 day later. After analyses the samples are stored at - 20°C.
Quantitation of IRT Filter paper discs with a diameter of 3 mm were punched from the blood spots
and IRT was measured using a solid phase, two-site sandwich immunofluorometric method (Delfia, neonatal IRT assay kit, Wallac Oy, Finland). The assay was carried out as described by the manufacturer with a recommended cut-off value of 70 ug/l. Control samples were also included to ensure the day-to-day reproducibility. Stan- dards and controls were prepared by addition of trypsin. The assay is measuring both the complexed active form (trypsin) and the uncomplexed form (trypsinogen).
Polymerase chain reaction For the Delfia test a disc, 3 mm in diameter, was punched from the blood spots
into a microcentrifuge tube and treated according to Iitil et al. [5] with some modifications. Briefly, 50 ul of 10 mM NaOH, 1% Nonidet P-40 was added above the disc and the sample was boiled for 10 min. Fifty ul of 10 mM CH,COOH, 100 mM Tris (pH 8.5) was added to neutralize the sample. After centrifugation a 20 ul sample was taken from the supernatant into the PCR reaction. Pretreated samples were stored at - 20°C.
The region around the AF508 mutation was amplified using the primers 5’- AAGCACAGTGGAAGAATTTC-3’, and 5’-CTCTTCTAGTTGGCATGCT-3’ in a Hybaid Thermal Reactor. A cycle program of 95°C 50 s, 53°C 2 min, 73°C 2 min, and 28 amplification cycles were used. The final amplification reaction (100 ~1)

3
contained 10 mM Tris-HCl (pH 8.4), 5.0 mM MgCl,, 200 uM dNTP, 0.1 mg/ml BSA, 50 mM NaCl, and Taq Polymerase (Perkin Elmer) 1 unit per 100 ul.
For the gel retardation test, PCR was carried out in the same way, except that the primers were 5’-AGTTTGCATGCTTTGATGAC and 3’-GCCTGGCACCAT- TAAACAA, the reaction buffer contained 10 mM Tris-HCl (pH 8.3), 50 mM HCl, 1.5 mM MgCl,, 0.0001% w/v gelatine, 200 uM dNTP, and Taq polymerase (Perkin Elmer), 1 unit per 100 ~1, and the cycle program was 94°C for 30 s, 51°C for 1 min, and 72°C for 2 min for a total of 30 cycles.
The gel retardation test Heteroduplex analysis of the PCR amplified DNA with the gel retardation test
was carried out as follows: Ten ~1 of the PCR product was mixed with the PCR product from a known homozygous wild-type sample and the mixture was incubated at 94°C for 5 minutes. After rehybridization at 65°C for 5 minutes, the mixtures were electrophoresed on 12% polyacrylamide gel in parallel with the original I?CR product and analyzed by observation of ETBR-stained bands.
The Del&a AF508 test Analysis of the amplified DNA with time-resolved fluorescence was performed in
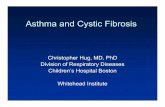
streptavidin coated microtitration wells [2] utilizing a capture/reporter oligonucleo- tide probe system [6]. The Eu-labelled reporter probe 5’-(EU modC)30 TCT- CAGTTTTCCTGGATTATGCCTGGCACC-3’ is complementary to a sequence outside the AF508 site in the amplified fragment, while two biotinylated capture probes are complementary to the normal 5’-AAATATCATCTTTGGTGTTTCm- odC-bio-3’ or the AF508 mutant S’AAA ATATCATTGGTGTTTCCTmodC-bio-3’ allele, respectively. The assay flow diagram is shown in Fig. 1. After washing at stringent conditions, Eu is released from the probe by adding Delfia Enhancement solution (Wallac Oy, Turku, Finland) into the wells. Time-resolved fluorescense is measured from the Enhancement solution using a time-resolved fluorometer (model 1230 Arcus, Wallac Oy, Turku, Finland). Function of the hybridization step was controlled using synthetic double-stranded oligonucleotide controls corresponding to the DNA fragments, either the normal or mutant alleles, between the PCR primer sequences. In addition, samples from clinically known normal persons (homozygous normal and a carrier of AF508 mutation) as well as samples from patients with cystic fibrosis homozygous for AF508, were run together as controls with unknown samples. All hybridizations were performed as duplicates. In all experiments, PCR reactions with water or pretreatment solution instead of sample were include:d as negative controls.
Ethics The study has been accepted by the Scientific ethical committee for Copenhagen
and Frederiksberg, J. No. V.100 2210,/91.

MUTANT SAMPLE
I SAMPLE TREATMENT AND AMPLIFICATION
DENATURATION AND ADDITION OF PROBES
MUTANT PROBE NORMAL PROBE
WASH UNDER STRINGENT CONDITIONS
MEASURE Eu-FLUORESCENCE
Fig. 1. Principle of the Delfia AF508 assay. Discs from the dried blood spots are boiled in alkaline conditions to liberate the DNA from cells, after which the region around the mutation site is amplified. The product is then analyzed in two separate, allele-specific hybridizations in microtitration wells coated with streptavidin (SA). One of two biotinylated capture probes, one specific for the normal and one specific for the mutant allele, are used. In addition a common Eu-labelled reporter probe is used in both
of the reactions.

5
Results
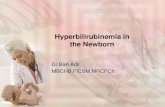
The 1081 PKU cards were all assayed for IRT and the AF508 mutation. PCR product from the region of the AF508 mutation were analyzed by both the gel retardation and the Delfia methods. The results are shown in the flow diagram in Fig. 2. In 12 newborns, corresponding to 1.02%, a concentration of IRT greater than 70 Kg/l was found. One of these 12 cases was a homozygote for AF508 and the IRT concentration was 380 ug/l. A total number of 28 heterozygotes was found giving a carrier frequency of 1:38.6 (Table 1).
108 1 - PKU Cards
1 IRT test
l~~N~12_l.02%~ S70 ug/I (N = 1069)
1 1 A508 A508
NOllTlal Heteroz. Homoz. Normal Heteroz. Homoz.
1042 27 0 10 1 1
Fig. 2. Newborn screening in Denmark for CF by combined IRT and AF508 he results of the IRT analyses of 1081 mutational analyses. Flow diagram for the results of the IRT analyses of 1081 newborn
infants.
TABLE 1
IRT values @g/l) in normals, heterozygotes and one case of AF508 homozygote
IRT &z/l)
No. median min. max.
Normals 1052 19.8 4.8 135.9 Heterozygotes 28 25.8 13.0 12.7 Homozygotes 1 380

6
The IRT analyses
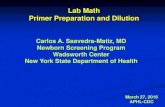
The reproducibility has been examined by coefficient of variation (CV) between replicates for IRT calibrator solutions and for filter paper blood spots. The CV was greatest for filter paper duplicates (Fig. 3). The majority of blood spots had IRT concentrations below the cut-off value. Of the 12 blood spots which had values higher than 70 ug/l, one had a CV of 12%, the others less than 10%. Of 35 samples with an IRT concentration between 50 and 70 ug/l, two had CV between 20 and 30%, and 9 samples had CV between 10% and 20%, 24 samples had CV less than 10%. The intra- and interassay precision profiles showed a coefficient of variation between 3.6% and 14.2% at three different IRT levels. The detection limit was 4 us/l. The IRT values showed a log normal distribution as shown in Fig. 4 and the concentrations were slightly but significantly higher in girls than in boys (Student t- test P=O.O02) Fig. 5. The IRT levels were also significantly higher in 28 AF508 heterozygotes (Student t-test P= 0.001) (median: 25.8 ug/l, and range: 13.0-72.7) than in 1052 normals (Fig.6) (median: 19.8 ug/l, and range: 4.8-135.9 w/l).
The gel and Deljia test for AF508
For all 1081 PKU cards the mutational analyses for AF508 showed identical results for the gel retardation test and the Delfia test, namely 1052 normals, 28
% CU brtwrrn rrplicrtrr
Fig. 3. Cumulative relative frequencies. Frequency of coefficient of variations (CV%) between replicates for 1: IRT Calibrator solution 25 pg/l, 2: IRT calibrator solution 100 pg/l, and 3: filter paper blood spots
(n= 1081).
1

6
I , * I / , , , , , , , , L 1.6 2.6 3.6 4.6
LOG IRT ng/ml
Fig. 4. Normal probability plot for logarithmic IRT concentration (n= 1081).
I , , I / , / , , , , , , , ,
1.. 7.4 a.4 . . . s.1
Log IRT ng/ml
Fig. 5. Comparison of frequency histograms for logaritmic IRT concentrations in normal girls (n = 527 (13 heterozygotes), median: 20.5 pg/l) and boys (n= 519 (15 heterozygotes), median 19.0 pg/l).

8
heterozygotes and one homozygote. However, the Delfia test was much easier to carry out and one technician can analyze twice as many samples per day than with the gel retardation test. In the Delfia AF508 assay, the synthetic oligonucleotide controls made it possible to follow the function of the detection part separately from the function of the amplification. Additional reliability was obtained by including background control along with known normal carrier and mutant samples in each amplification run.
Discussion
This anonymous CF screening study in newborns by IRT and AF508 mutational analyses was carried out to make a basis for the design of a future newborn screening program based upon this two-tiered approach. We have confirmed that a cut-off by Delfia IRT at 70 ug/l corresponds to about 1% false positives and have shown that the IRT levels in newborns follow a log normal distribution. The IRT concentration is significantly higher in newborn girls than in boys (P= 0.002) and also slightly but significantly higher in heterozygotes than in normals (P=O.OOl). One case was a homozygote for the AF508 mutation and in this CF patient the IRT concentration was 380 ug/l.
The Delfia IRT assay was easy to perform and one person can easily examine 200 samples for both Delfia TSH and Delfia IRT per day. The reproducibility in terms
1
norm.,.
- I.1 P.. 3.1 . . . s..
Log IRT ng/ml
Fig. 6. Comparison of frequency histograms for logarithmic IRT concentrations in normals (n = 1052) and carriers (n = 28).

9
of intra- and interassay coefficient of variation was less than 14.2%. Also the coefficient of variation between duplicates was acceptable as shown in Fig. 3 especi- ally since the CV above the cut-off level of 70 ug/l was less than 12%.
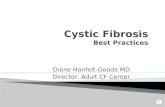
The AF508 mutational analyses showed identical results for all 108 1 PKU samples both with the gel test and the Delfia test, e.g., 1052 normals, 28 heterozygotes and one homozygote. The carrier frequency was thus found to be 1:38.6. This is the same frequency as found in a recent prenatal carrier screening project for AF5~08 in Denmark [ll]. Delfia AF508 assay was more practical to perform than the gel retardation assay and various controls also made the assay more reliable. Numerical results from the Delfia AF508 assay are easier to interpret, store and present (Fig. 7).
At present several models for CF screening are explored. Carrier screening by AF508 analyses can be carried out as a preconceptional screening or a prenatal screening. If the woman is a carrier for the AF508 mutation then the partner could
400
350
300
100
50
0
. 8
: .
. .
. . . .
. . mm= b
. . .. 10x
m .
.
I I
10x
0 50 lco 150 200 250 3w 2.53 400
Normal probe (CPSxlOOO)
Fig. 7. Results obtained with the Delfia AF508 analysis. Values for one homozygous mutant (arrow) and twenty-eight carriers found in the study, together with 50 homozygous normal samples are shown. Hybridization signals obtained with PCR background control was subtracted from the hybridization signals and values for normal probe were plotted against values obtained with the mutant probe. Lines (10 x ) represent theoretical cut-off if ten times higher signal was obtained with specific probe over the
crossreacting probe.

10
be examined [3,11,13]. If he is also a carrier, prenatal diagnosis could be offered, e.g., chorion villus sampling or amniocentesis, since the risk for CF foetus is 25%. If the CF diagnosis is made, the couple could be offered therapeutic abortion.
Newborn CF screening is a completely different approach where the assumption is that early diagnosis improves the treatment of CF resulting in less morbidity and longer life expectancy. This is still a matter of controversy, but recent progress in understanding the metabolic abnormality of the disease certainly seems promising for symptomatic as well as causal therapy of the disease [12]. Therefore, newborn CF screening is more in focus than just a few years ago. Furthermore, in the two- tiered IRT/DNA strategy there is only a theoretical possibility of having a false- positive result and also the rate of false-negative results should be low. This is true especially in Denmark, where the AF508 mutation is found in 88% of the CF chromosomes, meaning that 98.6% of the CF patients have the AF508 mutation in one or two of their CF genes. Use of the two-tiered approach could reduce the number of sweat tests and possibly also the length of initial hospitalization periods. In addition there is no need for a second IRT sample. With the two-tiered approach it should be also possible to reduce the cost for diagnosis of CF.
Acknowledgements
We want to thank Timo Liivgren, Kim Pettersson, and Harri Siitari for scientific support. We also want to thank Jette Rasmussen and Kirsten Lindboe for the expert technical assistance and Ingelise Laybourn for typing the manuscript. We also thank Irma Suvisuo for preparing the picture of the Delfia AF508 assay flow.
References
1 Crossley JR, Elliot R, Smith PA. Dried-Blood spot screening for cystic fibrosis in the newborn. Lancet 1979;i: 472-474.
2 Dahlen PO, Iitia AJ, Skagius G, Frostell A, Nunn MF, Kwiatkowski M. Detection of human immunodeficiency virus type 1 by using the polymerase chain reaction and a time-resolved fluorescence based hybridization assay. Clin Microbial 1991;29: 798-804.
3 Editorial. Screening for Cystic Fibrosis. Lancet 1992;ii: 209-210. 4 Hammond KB, Abman SH, Sokol RJ, Accurso FJ. Efficacy of statewide neonatal screening for cystic
fibrosis by assay of trypsinogen concentrations. N Engl J Med 1991;325: 769-774. 5 Iitia A, Hsgdall E, Dahlen P, Hurskainen P, Vuust J, Siitari H. Detection of mutation AF508 in the
cystic fibrosis gene using allele-specific PCR primers and time-resolved fluorometry. PCR Methods Applications 1992;2: 157-162.
6 Liivgren T, Hurskainen P, Dahlen P. Detection of Lanthanide chelates by time-resolved fluorescence. In: Kricka LJ, ed. Nonisotopic DNA probe techniques. New York: Academic Press, 1992.
7 Ranieri E, Ryall RG, Morris CP, Nelson PV, Carey WF, Pollard AC, Robertson EF. Neonatal screening strategy for cystic fibrosis using immunoreactive trypsin and direct gene analysis. Br Med J 1991;302:1237-1240.
8 Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Gizelczak Z, Zielenski J, Lok S, Plavsic N, Chou JL, Drumm M, Iannuzzi M, Collins F, Tsui LC. Identification of the cystic fibrosis gene: Cloning and characterization of complementary DNA. Science 1989;245:1066-1073.

11
9 Rommens JM, Iannuzzi M, Kerem B, Drumm ML, Melmer G, Dean M, Rozmahel R, Cole JL, Kennedy D, Hidaka N, Zsiga M, Buchwald M, Riordan JR, Tsui LC, Collins FS. Identification of the cystic fibrosis gene: chromosome walking and jumping. Science 1989;245:1059-1065.
10 Schwartz M, Johansen HK, Koch C, Brandt NJ. Frequency of the AF508 mutation on cystic fibrosis chromosomes in Denmark. Hum Genet 1990;85:427-428.
11 Schwartz M, Brandt NJ, Skovby F. Screening for carrier of cystic fibrosis among pregnant women. Eur J Hum Genet 1993; in press.
12 Tizzano EF and Buchwald M. Cystic fibrosis: Beyond the gene to therapy. J Pediatr 1992;120:337-349, 13 Wald NJ. Couple screening for cystic fibrosis. Lancet 1991;ii:l318-1319. 14 Wilcken B, Urwin R, Brown DA. Cystic fibrosis screening by dried blood spot trypsin assay. RI:sults
in 75,000 newborn infants. J Pediatr 1983;102:383-387.