Normal Respiratory Microanatomy - ΒΙΟΪΣΤΟΛΟΓΙΟ · Normal Respiratory Microanatomy ......
68
Normal Respiratory Microanatomy Conducting Portion- tubular passageways that serve to warm or cool, humidify and clean air Nasal Cavities • Vestibular region has a lightly keratinized, stratified squamous epithelium with coarse hairs (vibrissae) and sebaceous glands. The vibrissae act as coarse filters and are richly supplied with nerve endings. • Respiratory region has a ciliated pseudostratified columnar epithelium (respiratory epithelium) with numerous goblet cells o Cell types: Goblet Ciliated- projections to snag mucus flow Brush- innervated by CN V (unknown secretory or sensory function) Basal- stem cells EEC (enteroendocrine)- hormone secreting; origin of oat cell carcinomas • Mucus moistens air and traps particles, while cilia beat towards pharynx causing about one pint of mucus to be swallowed per day • Turbinate bones on lateral walls help make airflow more turbulent • Swell bodies are venous cavernous plexuses which function for heat exchange and alternate left to right every half-hour • Vessels have intimal cushions so when the tunica media relaxes, the vessel opens (erectile characteristic similar to that of the penis) • Blood supply is arranged in redundant loops (counter-current system) • Olfactory region has an epithelium similar to respiratory epithelium but lacking goblet cells. The glands associated with olfactory epithelium produce only serous fluid, no mucous. o Olfactory cells are bipolar neurons that are structurally but not functionally identical; they have non-motile cilia that increase surface area o Basal cells may be stem cells for olfactory cells (do replace other cells) o Sustentacular cells form mesaxons around the olfactory cell axons (function similarly to glial cells) and are also secretory o Brush cells are rich in microvilli and serve an unknown function (probably sensory) Paranasal Sinuses (Frontal, Sphenoidal, Ethmoidal, Maxillary) • Epithelium is similar to respiratory epithelium but with fewer cilia, fewer goblet cells and relatively few glands • Compromised drainage of the sinuses causes congestion and irritation of nerve endings within the lamina propria o Can be treated with drugs like epinephrine that constrict vessels, decrease blood flow, reduce swelling and allow drainage Trachea • Lined with respiratory epithelium, with cilia beating up toward pharynx • Abundant serous and mucous glands within the submucosa • Has 16-20 C-shaped rings of cartilage in the adventitia, all of which open posteriorly
Transcript of Normal Respiratory Microanatomy - ΒΙΟΪΣΤΟΛΟΓΙΟ · Normal Respiratory Microanatomy ......

Normal Respiratory Microanatomy Conducting Portion- tubular passageways that serve to warm or cool, humidify and clean air Nasal Cavities • Vestibular region has a lightly keratinized, stratified squamous epithelium with coarse hairs
(vibrissae) and sebaceous glands. The vibrissae act as coarse filters and are richly supplied with nerve endings.
• Respiratory region has a ciliated pseudostratified columnar epithelium (respiratory epithelium) with numerous goblet cells o Cell types:
Goblet Ciliated- projections to snag mucus flow Brush- innervated by CN V (unknown secretory or sensory function) Basal- stem cells EEC (enteroendocrine)- hormone secreting; origin of oat cell carcinomas
• Mucus moistens air and traps particles, while cilia beat towards pharynx causing about one pint of mucus to be swallowed per day
• Turbinate bones on lateral walls help make airflow more turbulent • Swell bodies are venous cavernous plexuses which function for heat exchange and alternate left to
right every half-hour • Vessels have intimal cushions so when the tunica media relaxes, the vessel opens (erectile
characteristic similar to that of the penis) • Blood supply is arranged in redundant loops (counter-current system) • Olfactory region has an epithelium similar to respiratory epithelium but lacking goblet cells. The
glands associated with olfactory epithelium produce only serous fluid, no mucous. o Olfactory cells are bipolar neurons that are structurally but not functionally identical; they have
non-motile cilia that increase surface area o Basal cells may be stem cells for olfactory cells (do replace other cells) o Sustentacular cells form mesaxons around the olfactory cell axons (function similarly to glial
cells) and are also secretory o Brush cells are rich in microvilli and serve an unknown function (probably sensory)
Paranasal Sinuses (Frontal, Sphenoidal, Ethmoidal, Maxillary) • Epithelium is similar to respiratory epithelium but with fewer cilia,
fewer goblet cells and relatively few glands • Compromised drainage of the sinuses causes congestion and
irritation of nerve endings within the lamina propria o Can be treated with drugs like epinephrine that
constrict vessels, decrease blood flow, reduce swelling and allow drainage
Trachea • Lined with respiratory epithelium,
with cilia beating up toward pharynx
• Abundant serous and mucous glands within the submucosa
• Has 16-20 C-shaped rings of cartilage in the adventitia, all of which open posteriorly

Bronchi • Identical to trachea, except hyaline cartilage is arranged in
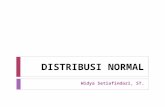
plates • Picture shows small portions of hyaline cartilage (on left
and right edges of picture), substantial glandular tissue, and bands of smooth muscle just beneath the lamina propria
Bronchioles • Encircled by a complete layer of smooth muscle, which
plays an important role in regulating the diameter of the bronchiole
o This is the smooth muscle that spasms in asthmatics
• Lined by ciliated simple columnar epithelium • Contain sparse glands in the submucosa
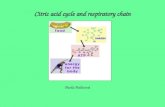
Respiratory Portion- segments of the respiratory tract in which gas exchange occurs
Respiratory Bronchioles • Can be differentiated from terminal bronchiole (also
pictured) by the openings of alveoli • Lined by ciliated simple cuboidal and simple squamous
epithelium • Contain no glands
Alveoli • Lined by simple squamous epithelium • Type I cells cover about 95% of the alveolar surface
o Not mitotically capable o Can share basal lamina with capillary, creating thinnest
part of the respiratory minimal barrier (type I cell, basal lamina, endothelial cell)
• Type II cells cover about 5% of the alveolar surface (bulge) o Are mitotically capable (reserve for Type I and II cells)o Produce and release surfactant, which decreases
alveolar surface tension Surfactant is first produced by the fetus at about 24
weeks gestation Surfactant increases with ventilation and is
stimulated by corticosteroids • Alveolar macrophages (dust cells) are monocyte-derived
cells that phagocytose debris and surfactant • Interalveolar wall contains collagen for support and to
limit expansion and elastic fibers to accommodate inspiration
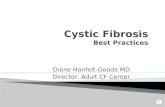
Type II cell
Dust cell


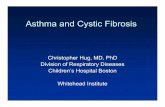
Gas exchange first occurs at the respiratory bronchioles due to the appearance of alveoli (arrows).
Respiratory Minimal Barrier
Respiratory Conducting

Chronic Obstructive Pulmonary Disease A disease state characterized by progressive development of airflow limitation that is not fully reversible and usually results from an abnormal response of the lungs to noxious particles or gases Prevalence
• 16 million people in the U.S. have COPD • Rare in people under 40 years old • WHO predicts that by 2020, COPD will rise from 6th to 3rd place worldwide as the most
common cause of death Etiology
• Important contributing factors to the genesis of COPD are cigarette smoking and air pollution • Four major conditions cause COPD
o Emphysema o Chronic bronchitis/bronchiolitis o Asthma o Bronchiectasis
Clinical Findings
• Patients with COPD often have overlapping symptoms of chronic bronchitis, chronic asthma and emphysema
• Cough with mucoid to mucopurulent sputum • Dyspnea, first on exertion and later in the disease
at rest • Prolonged expiration, with or without wheezes • Decreased breath sounds • Hyperresonance to percussion • FVC, FEV1 and FEV1/FVC are all decreased • TLC, RV and RV/TLC are all increased • Hypoxemia and hypercapnia can occur later in the disease (when FEV1
falls below 1.0 L) • Chest x-ray shows hyperinflation with flat, depressed diaphragms, a long
and narrow heart shadow, and increased space behind the sternum Complications
• Hypoxic pulmonary hypertension • Right heart failure (cor pulmonale) • Frequent intercurrent respiratory tract infections (>2 per year) • Weight loss and loss of appetite • Respiratory failure with severe hypoxemia, hypercapnia, and respiratory acidosis
Management
• Smoking cessation • Oxygen therapy • Bronchodilators (mainly inhaled) • Steroids (for acute episodes) • Antibiotics • Mechanical ventilation • Surgery (LVRS, transplantation)
Normal chest x-ray (left) and chest x-ray of COPD (right) showing flat, depressed diaphragms and long,
narrow heart shadow
Lateral chest x-ray showing increased space
behind the sternum

Emphysema A condition of the lung characterized by abnormal permanent enlargement of the airspaces distal to the terminal bronchiole, accompanied by the destruction of their walls and without obvious fibrosis Pathogenesis
• Hypothesis is that alveolar wall destruction is due to an imbalance between proteases (especially elastase) and antiproteases (especially α1-antitrypsin)
o Low serum levels of the protease inhibiter (Pi) α1-antitrypsin lead to the development of emphysema
90% of the population has the normal phenotype PiMM
Indiviudals with the PiZZ phenotype are at high risk for developing emphysema
o Smokers have increased numbers of PMNs in their alveoli These PMNs secrete free radicals that inhibit α1-antitrypsin Oxidants in cigarette smoke also inhibit α1-antitrypsin
Panacinar Emphysema (panlobular emphysema)
• Dilation and destruction of entire acini • Characterized by multiple small cystic spaces which, on cut section, give
the lung a ragged fishnet appearance • Lesions tend to be in the lower and anterior zones of the lung bilaterally • This form is quite common, especially in older adults • Noxious environmental factors facilitate panacinar emphysema • This form is also seen with α1-antitrypsin deficiency
Centriacinar Emphysema (proximal acinar emphysema)
• Most common form of emphysema (strongly linked to cigarette smoking) • Dilation and destruction primarily involving the proximal portion of the
acinus (respiratory bronchioles) • Characterized by spotty, multifocal, cystic spaces with interstitial deposits
of anthracotic pigment • Lesions tend to be more prominent in the upper lobes
Paraseptal Emphysema (distal acinar emphysema)
• Dilation and destruction primarily involving the peripheral portion of the acinus (distal alveolar ducts and sacs)
• Cystic or bullous lesions are most common in the apices, anterior margins of upper lobes, and diaphragmatic surfaces of lower lobes
o A bulla is a dilation of an air space that is 1cm or greater • Since distal acini attach to relatively rigid
structures (pleura or septa) a shearing effect is facilitated under stress
o This can cause leakage of air from the lung airways into the interstitium and pleura, creating subpleural collections of air (“blebs”) which are prone to rupture
Panacinar emphysema, showing destruction of most of the lung lobule
In emphysema, alveolar walls are destroyed and air spaces are dilated
Bullous disease of the lung, a cyst-like enlargement of the airspace that can be a manifestation of paraseptal emphysema
Centriacinar emphysema, showing diseased spots
surrounded by spared acinic tissues
Pleural bleb

Chronic Bronchitis A clinical diagnosis requiring a chronic cough that produces sputum for 3 months or more in at least 2 consecutive years, without any other disease that could account for this symptom Etiology
• Smoking is a major etiological factor o Only 5-10% of chronic bronchitis cases occur in non-smokers
• Environmental factors such as pollution can play a role in causing chronic bronchitis • Weather conditions and infectious agents can also contribute to chronic bronchitis
Clinical Findings
• Chronic cough that produces sputum • Bronchitis is especially likely to cause right ventricular hypertrophy and lung congestion (“blue
bloater” syndrome and cor pulmonale) Pathogenesis
• Inflammatory cells are present in the wall and lumen of the bronchus and mucus glands are increased in number
• The resulting increased level of secretions leads to airway obstruction o There is no bronchoconstriction (in contrast to asthma)
Pathologic Findings
• Hypertrophy and hyperplasia of submucosal glands in the bronchi
• Goblet cell increase in the epithelial lining of the small airways
o Causes hypersecretion of mucous (with plugging), inflammation and fibrosis
• Reid Index greater than 0.5 o Reid index is a ratio of submucosal gland thickness to
the distance between the epithelial basement membrane and the inner surface of the perichondrium
Chronic Bronchiolitis
• Chronic inflammation involving bronchioles, particularly the terminal and respiratory bronchioles
• The most common lesion with viral infections, inhalation of chemicals, air pollutants, and smoking
• Can result in physiologically significant airway obstruction
The bronchial wall shows many inflammatory cells, mostly lymphocytes
In chronic bronchiolitis, inflammatory cells are seen in the smaller airways

Asthma A chronic inflammatory disorder of the airways characterized by episodic, reversible attacks of respiratory obstruction due to bronchoconstriction Etiology
• Development of asthma is linked to atopy and allergies • “Allergic asthma” is associated with elevated IgE levels and may be linked to specific antigens • “Intrinsic asthma” is associated with only slightly elevated IgE levels and no specific antigen
o This variant is frequently associated with reaction to certain drugs, cold or stress Clinical Findings
• Symptoms usually begin in childhood and continue into adulthood (50% of patients become asymptomatic in adulthood)
• Episodes of dyspnea, coughing and wheezing • If the cough is productive, the sputum may contain:
o Prominent eosinophils o Charcot-Leyden crystals derived from plasma membranes of the
eosinophils o Curschmann’s spirals (casts of small airways) o Creole bodies (aggregates of columnar cells) o Sloughed ciliated cells
• Inhalation challenge is positive • During auscultation of blood pressure, may see a greater than 15 mmHg reduction in amplitude
in systolic arterial pressure with inspiration (pulsus paradoxus) • Status asthmaticus is the most severe form of asthma and may result in severe cyanosis
Pathogenesis
• Allergic asthma o Allergen causes B-lymphocytes to produce IgE o IgE attaches to mast cells or basophils o 2nd stimulus causes release of mediators
(histamines, leukotriene B4) o Bronchoconstriction, mucous secretion,
flushing and hypotension develop • Asthma is an entirely obstructive phenomenon with no
associated destruction of airways Pathological Findings
• The bronchial wall is thickened by edema and subacute inflammation with prominent eosinophil and lymphocyte infiltration
• There is some hypertrophy and hyperplasia of mucous cells and submucosal glands
• There is some hyperplasia of bronchial smooth muscle • The epithelial basement membrane appears thickened due to
deposition of collagen II and V in the lamina reticularis • On autopsy, the lung fails to collapse due to mucous plugs
obstructing the outflow of air
Charcot-Leyden crystals
Bronchial mucous cast removed from an asthmatic lung at autopsy
Bronchial wall, showing prominent eosinophils
Bronchial wall, showing thickened basement membrane and inflammatory infiltrate
Curschmann’s spirals

Bronchiectasis The abnormal dilation of bronchi and bronchioles associated with chronic, necrotizing infection Etiology
• Infectious: o Before vaccinations, pertussis and measles were strongly linked to bronchiectasis o Adenovirus and tuberculosis infections remain major causes o Immunologic deficiencies are also associated with bronchiectasis
• Hereditary o Cystic fibrosis and Kartagener immotile cilia syndrome
• Bronchial obstruction: o Aspiration of poorly soluble substances or foreign objects (eg. peanuts) o Compression of bronchi by tumors or enlarged lymph nodes o Mucous impaction or bronchitis
Pathologic Findings
• Bronchi are enlarged and dilated while the surrounding lung is poorly-aerated and collapsed o Usually involves primarily the lower lobes
• Fusiform, saccular and varicose distortions are recognized
The bronchi are enlarged, dilated, and extend out to nearly the pleural surface while the surrounding lung is non-
aerated, collapsed and has areas of consolidation
Bronchiectasis can become a chronic infectious process that involves bronchi, but secondarily produces pneumonia in
the surrounding lung

Pneumonia Infection of the pulmonary parenchyma by any of a variety of pathogens Prevalence
• Community-acquired pneumonia is the 6th leading cause of death in the US o Number 1 cause of infection-related mortality o 3rd most frequent hospital diagnosis in patients over 65 years old
Etiology
• Streptococcus pneumoniae o Most commonly identified cause of community-acquired pneumonia o Gram-positive cocci in pairs (diplococci) o Catalase-negative o α-hemolytic o Sensitive to optochin o About 90 immunologically distinct polysaccharide capsules exist
Types 19, 57, 58, and 59 are most common • Haemophilus influenzae
o More common in smokers and the elderly o Small, Gram-negative coccobacillus o Grows aerobically and anaerobically o Requires two growth factors:
X factor (Hematin) V factor (Nicotinamide adenine dinucleotide)
• Moraxella catarrhalis o Causes pneumonia in the elderly and patients with underlying
disease o Gram-negative coccobacillus o Commonly carried in the upper respiratory tract
50% of children 7% of adults
• Klebsiella pneumoniae o Gram-negative bacillus o Causes “necrotizing pneumonia”
May be hospital-acquired Alcoholics and patients with COPD are at risk Patients have currant jelly sputum and bulging fissure sign
• Staphylococcus aureus o Gram-positive cocci o Facultatively anaerobic o Catalase-positive and coagulase-positive o Uncommon cause of community-acquired pneumonia o Most common cause of hospital-acquired pneumonia o Causes lung necrosis and abscess formation
• “Atypical organisms” o Intracellular bacteria that cause diffuse interstitial disease, rather than lobar and alveolar
Mycoplasma pneumoniae Chlamydophila pneumoniae (seen in younger patients) Legionella species
• Viruses • Fungi
Streptococcus pneumoniae (sputum)
Haemophilus influenzae (culture)
Moraxella catarrhalis (culture)
Klebsiella pneumoniae (culture)
Staphylococcus aureus (sputum)

Typical Pneumonia Atypical Pneumonia Symptoms Fever, chills, pleuritic pain (acute) Fever, headache, myalgias Cough Productive Non-productive X-ray Lobar, dense Bronchopneumonia, interstitial pattern
Transmission
• Aspiration of organisms colonizing the oropharynx is the most common cause of pneumonia o About 50% of healthy adults aspirate oropharyngeal secretions during sleep o More frequent with impaired consciousness or neurologic disorder
• Inhalation of infected aerosols is a common mode of transmission o Particles larger than 10 µm deposit in upper airways o Particles smaller than 5 µm deposit in small bronchioles and alveoli
Stay suspended in air for long periods • Hematogenous spread is also possible
Clinical Findings
• Cough that may be productive or non-productive • Fever (over 100°F with bacterial pneumonia) and
shaking chills • Pleuritic chest pain • Headache and myalgias • Physical examination reveals signs of consolidation
of the lung parenchyma (increased tactile fremitus, bronchophony, egophony, bronchial breath sounds, and fine rales over the consolidated area)
• Chest x-ray shows lobar (typical) or diffuse (atypical) infiltrate
• Sputum Gram stain may identify causative organism in a purulent sample produced by a deep cough and uncontaminated by oral secretions
Pathologic Findings
• On autopsy, abnormal lung retains its shape while normal lung collapses
o Pale consolidation is observed (may be lobar or diffuse)
• Microscopically, typical pneumonias show an alveolar filling process
o Viral pneumonitis or atypical pneumonia is more likely to show an interstitial inflammatory process
Gross bronchopneumonia (diffuse), showing
characteristic multifocal pattern of consolidation
Lobar pneumonia, showing diffuse alveolar filling process and intraalveolar
PMNs
Bronchopneumonia, showing patchy alveolar filling process with an acute
inflammatory infiltrate
Lobar pneumonia Diffuse pneumonia, showing characteristic
“ground glass” appearance
Viral pneumonitis, showing an enlarged interstitium with predominantly
lymphocytic infiltration while the alveoli remain clear (in contrast to bacterial
pneumonias)
Gross lobar pneumonia, showing normal lung tissue on the right and
consolidated tissue on the left

Treatment • Treatment is ideally based on the causative
organism, but in practice must be started before organism can be identified (blood/sputum cultures should still be performed)
• Drugs should be chosen based on most likely causative organism and more than one drug should be used
o Trimethoprim-sulfamethoxazole o Doxycycline o Beta-lactam antibiotics (penicillins,
cephalosporins, carbapenems) o Macrolides o Quinolones
Pneumocystis Pneumonia A lung infection caused by the fungus Pneumocystis joriveci and occurring exclusively in immunocompromised patients, particularly those with AIDS Etiology
• Pneumocystis joriveci (formerly Pneumocystic carinii) is present in the lungs of many animals o Causes disease exclusively in immunocompromised patients o 70% of healthy individuals have antibodies against P. jiroveci
Pathogenesis • Cysts filled with sprorozoites are inhaled • Sporozoites emerge from cysts and replicate as
trophozoites, which then form new cysts Pathologic Findings
• Grossly, the lung shows consolidation, but with a pink appearance
• Histology shows alveoli filled with a pink, foamy or granular exudate with very few inflammatory cells
o Inflammation is primarily interstitial Treatment
• Trimethoprim-sulfamethoxazole
P. jiroveci (carinii) in a sample from a bronchial lavage, showing round cyst
with several pink sporozoites inside and some free sporozoites
P. jiroveci (carinii), methenamine silver stain
P. jiroveci (carinii), silver stain, showing cluster of cysts that is infrequent in clinical samples
Common Causes of Pneumonia, by age Neonates (0-6 wks):
• S. agalactiae (GBS), E. coli, C. trachomatis Children (6 wks-18 yrs):
• Viruses (RSV), mycoplasma Young adults (18-40 yrs):
• Mycoplasma, C. pneumoniae Adults (40-65 yrs):
• S. pneumoniae, H. influenzae Elderly (>65 yrs):
• S. pneumoniae, viruses, H. influenzae

Histoplasmosis Etiology
• Histoplasma capsulatum or Ajellomyces capsulatum o Both pathogens have been isolated from soil
exposed to bird and bat feces o Common in southeastern and midwestern US
(Mississippi and Ohio Rivers) Pathogenesis
• Inhalation of the fungal microconidia leads to transformation to yeast at 37°C
o Yeast evade phagocytosis by PMNs o Yeast survive and multiply within
phagolysosome of non-activated macrophages Clinical Findings
• Pulmonary infection is usually flu-like or asymptomatic o In 5% of cases, severe pneumonia develops
• In immunocompromised hosts, disseminated disease will usually follow
• In immunocompetent hosts, lung lesions will usually calcify but disseminated disease may occur
• Disseminated disease usually involves leucopenia, hepatosplenomegaly and irregular fevers and can become a mild chronic disease affecting one organ (99% survival) or a severe chronic disease affecting multiple organs (50% survival)
• Chest x-rays show diffuse infiltrates in primary disease and calcifications similar to TB in disseminated disease
• Antigen can be detected by latex agglutination in urine or serum in disseminated disease • Skin test is available for histoplasmin exo-antigen
Pathologic Findings
• Giemsa stain of biopsy shows organism growing inside of macrophages Treatment
• Amphotericin B, voriconazole, itraconazole, fluconazole
Histoplasma capsulatum (mycelial form), shows septate hyphae with small, round
conidia
Histoplasma capsulatum (yeast form), shows oval or round, small single cells with buds at
the narrow end of the parent cell

Blastomycosis Etiology
• Blastomyces dermatitidis or Ajellomyces dermatitidis o Isolated from moist soil with high organic content
and exposed to animal excreta o Common in southeastern and midwestern US,
including Wisconsin and Minnesota Pathogenesis
• Inhalation of the fungal conidia leads to transformation to yeast in lung
o Yeast evade phagocytosis by alveolar macrophages
Clinical Findings
• Primary pulmonary infection is asymptomatic in most patients
• Acute pneumonia is followed by hematogenous spread to bone (25-50%), genitourinary system (especially prostate) and rarely to the CNS
o Sometimes the fungus does not disseminate and establishes localized chronic disease
• Sub-acute respiratory infection leads to fever, cough and chest pain
• Skin lesions develop into ulcerated granulomas • Budding yeast cells with characteristic broad base can be seen in 10% KOH preparation of
sputum, skin lesions, prostate fluid, etc. • Chest x-ray shows non-specific pulmonary lesions • Antibody to the A-antigen can be detected in 77% of cases with enzyme immuno assay
Treatment
• Amphotericin B, voriconazole, itraconazole
Blastomyces dermatididis (myecelial form), showing numerous round or pear-shaped
single-celled conidia
Blastomyces dermatididis (yeast form), showing large, spherical, thick-walled yeast
with broad-based buds

Coccidioidomycosis “San Joaquin Valley Fever” Etiology
• Coccidioides immitis is a saprophyte found primarily in the soil of the southwestern US
Pathogenesis
• After inhalation, arthrospores swell and develop into spherules filled within endospores, which in turn develop into new spherules
o Arthrospores possess anti-phagocytic activity o Spherules are too large to be phagocytosed
Clinical Findings
• Pulmonary infection is asymptomatic in 60% of cases • Mild to severe flu-like symptoms are seen in 40% of cases • Erythema nodosum is seen in 5% of cases • Disseminated disease is seen in 5% of cases
o Includes skin manifestations, soft tissue abscesses, bone and joint disease, and meningitis
• Chest x-ray may show a coin-shaped lesion • Sputum preparation in 10% KOH shows characteristic
spherules • Skin test is available for coccidion exo-antigen
Pathologic Features
• Microscopy shows granulomas with giant cells o Caseous necrosis may be present
Treatment
• Amphotericin B, voriconazole, itraconazole, fluconazole
Coccidioides immitis arthrospores, stained with lactophenol cotton blue
Mature sporangium of Coccidioides immitis
Biopsy showing epithelioid cells, lymphocytes, a giant cell and a C. immitis spherule

Aspergillosis Etiology
• Aspergillus fumigatus and Aspergillus flavius are ubiquitous opportunistic pathogens
Pathogenesis
• Pathogens are molds (no yeast form) that only infect immunocompromised hosts, especially neutropenic ones
• Produce numerous toxins (eg. haemolysin) and extracellular enzymes (eg. proteases and lipases) that lead to hemorrhage and tissue necrosis and may aid in tissue invasion
• Also produce toxins that slow ciliary beat frequency of human respiratory epithelium
• Possess cell wall components that aid in adherence to different host proteins
• Possess cell wall pigments (melanin) that interfere with phagocytosis by scavenging reactive oxidants
Clinical Findings
• Fever, malaise and cough • Hematogenous spread to the brain, kidney, liver, heart and bone can lead to meningitis,
hematuria, endocarditis and bone pain • Chest x-ray may show characteristic fungus balls (aspergillomas) that are mycelium-filled
pulmonary cavities that were initially caused by another lung disease • Sputum preparation in 10% KOH shows Y-shaped filaments
Treatment
• Intravenous amphotericin B, caspofungin, micafungin, voriconazole • Surgical removal of aspergillomas
Aspergillus, showing sunflower-like arrangements of conidiophores

Zygomycosis Etiology
• Rhizopus, Mucor, and Absidia are ubiquitous (ie. bread molds) Pathogenesis
• Pathogens are molds (no yeast form) that only infect immunocompromised hosts, especially neutropenic ones and particular diabetic patients after a ketoacidotic episode
• Pathogens have angioinvasive properties • Infection begins in paranasal sinuses and spreads to eyes, brain, CNS, lungs and GI tract
Clinical Findings
• Signs and symptoms vary widely based on the organs involved Pathologic Findings
• Biopsy shows organisms with large, non-septate hyphae which branch at right angles, growing through cells and blood vessels
Treatment
• Surgery (debridement) • Amphotericin B
Cryptococcosis Etiology
• Cryptococcus neoformans and Filobasidiella neoformans are found in soil contaminated with pigeon feces
Pathogenesis
• Pathogens are yeast that form a capsule to prevent phagocytosis and opsonization (acapsular mutants are avirulent)
• Produce melanin and D-mannitol to inactivate hydroxyl radicals and superoxides produced by monocytes and granulocytes
Clinical Findings
• Majority of pulmonary infections are asymptomatic with ultimate resolution of the primary lesion
• Minority of cases develop fulminating pneumonia o Hematogenous spread to the CNS causes meningitis
• CSF stained with India ink shows characteristic encapsulated yeast o CSF that is positive for Cryptococcus neoformans is AIDS-defining
Treatment
• Amphotericin B in combination with 5-fluocytosine • Fluconazole to prevent relapse

Influenza A contagious respiratory illness caused by influenza viruses Prevalence
• 5-20% of the US population gets the flu every year Etiology
• Influenza viruses are negative-strand RNA viruses o They are enveloped o Influenza A, B and C viruses can all infect humans
Influenza A viruses also infect birds and swine • Since other reservoirs exist there can be a re-assortment of viral genes in
these reservoirs, creating a virus that has not been seen by humans and for which humans have no immunity (this is basis for concern about an “avian flu pandemic”)
o Transmission is airborne Clinical Findings
• Fever (usually high) • Headache • Extreme tiredness • Dry cough • Sore throat • Runny or stuffy nose • Muscle aches • Stomach symptoms, such as nausea, vomiting, and diarrhea (more common in children) • Infectious period in otherwise healthy adults begins one day before symptoms and ends 5 days
after symptoms Vaccinations Live Attenuated Inactivated Route of administration Intranasal spray Intramuscular injection Type of vaccine Live virus Killed virus # of included virus strains 3 (2 influenza A, 1
influenza B) Same as LAIV
Vaccine virus strains updated Annually Annually Frequency of administration Annually Annually Approved age and risk group Healthy persons aged 5-49
years Persons ≥6 months; sick or not
Can be administered to family members or close contacts of immunosuppressed persons not requiring a protected environment
Yes Yes
Can be administered to family members or close contacts of immunosuppressed persons requiring a protected environment (e.g. hematopoietic stem cell transplant recipient)
Inactivated influenza vaccine preferred (live can be shed)
Yes
Can be administered to family members or close contacts of persons at high risk but not severely immunosuppressed
Yes Yes
If not simultaneously administered can be administered within 4 weeks of another live vaccine
Prudent to space 4 weeks apart
Yes
If not simultaneously administered can be administered within 4 weeks of another inactivated vaccine
Yes Yes
Effectiveness 85% 70 – 90%

Severe Acute Respiratory Syndrome A viral respiratory illness caused by a coronavirus that was first reported in Asia in February 2003 and is associated with high-grade fever and pneumonia Etiology
• SARS Corona-virus (SARS-CoV) o An enveloped virus with spikes (corona) o Reservoir is in horseshoe bats o Both humans and civets are hosts o Transmission is airborne
Clinical Findings
• Incubation period of 2-12 days (4 days mean) • Acute interstitial pneumonia • Fever, myalgia, cough, headache, dizziness • Normal or low WBC count • Elevated LDH
Treatment
• Ribavirin o RNA virus mutagen o Used in infants with RSV infections o High toxicity
• Interferon • Immune globulin
Virus Life Cycle and Potential Drug Targets

Sarcoidosis A multisystemic disorder characterized by an increased cellular immune response to an unknown antigen and the formation of non-caseating granulomas in affected tissues Prevalence
• Prevalence of 10-40 per 100,000 in the U.S. • May occur at any age, but most commonly in patients 20-40 years old • Blacks affected more than whites in the U.S. (10-17:1) • Women are affected more than men
Etiology
• Various infectious and non-infectious agents have been implicated • Evidence suggests that the disease results from an exaggerated cellular immune response
(acquired, inherited, or both) to a limited class of persistent antigens or self-antigens Clinical Findings
• Often asymptomatic • Mild dyspnea on exertion may be seen • Disease most commonly affects the lungs and lymph nodes
o May also present in skin, eyes, bone marrow, liver, spleen, kidneys and other organs • Chest x-ray may show hilar lymphadenopathy and
pulmonary infiltrates Pathologic Findings
• Grossly, honeycomb fibrosis of the lung may be seen in advanced disease
• Microscopy reveals non-caseating granulomatous inflammation with giant cells
o Giant cells may have inclusion bodies
Gross lung, showing honeycomb fibrosis
Non-caseating granuloma with Langhans-type giant cells, surrounded by a rim of lymphocytes
Giant cells with Schaumann body inclusions
A giant cell with an asteroid body inclusion can be seen in the center of
this image

Tuberculosis Prevalence
• It is estimated that at least 30% of the world’s population is infected with M. tuberculosis • Most new TB cases occur in Southeast Asia, the Western Pacific and Africa • Disease is more common in blacks, Eskimos and native Americans • Disease is more common in patients with diabetes, alcoholism, malnutrition,
congenital heart disease, chronic lung disease and AIDS Etiology
• Tuberculosis is caused by the acid fast bacilli of the genus Mycobacterium o Mycobacterium tuberculosis is the most common etiologic agent
Pathogenesis
• The pathologic features of the disease relate to a type IV delayed hypersensitivity response and granulomatous reaction by the host
o Mycobacterium sp. have no endotoxins, exotoxins, or enzymes, but are resistant to intracellular digestion
o The intensity of the host reaction causes tissue necrosis (caseating granulomas) Clinical Findings
• Prolonged cough with hemoptysis • Fatigue, malaise, weight loss, fever and night sweats • Sputum smears may be positive for acid-fast bacilli (65%) • Positive tuberculin skin test (purified protein derivative; PPD) indicates exposure and type IV
T-cell delayed hypersensitivity reaction to the organism o Negative PPD may occur in active TB due to anergy (non-responsive T-cells) or recent
infection (<6 weeks) o Positive PPD does not indicate disease activity o PPD is considered positive based on the size of the induration after 48 hours
• ≥5 mm is positive with suspected HIV or immunosuppression, recent contact with active TB, organ transplant, or chest x-ray consistent with prior TB
• ≥10 mm is positive with high risk medical conditions, recent immigration from high-prevalence countries, intravenous drug abuse, crowded home or workplace, children less than 4 years old, and mycobacteriology lab personnel
• ≥15 mm is positive in persons with no risk factors for TB • QuantiFERON-TB is a whole blood IFN-γ release assay for the detection of TB infection
o Indirectly assesses presence of TB-specific antigens ESAT-6 and CFP-10 • These antigens induce IFN-γ release and are absent from BCG vaccination and
most environmental strains of Mycobacterium Disease Progression
• An individual who is exposed to someone with active tuberculosis can become infected by inhaling the tubercle bacilli present in infectious droplets
o Wet sputum organisms are viable for months o Dry sputum organisms are viable for weeks
• Most people do not immediately develop progressive disease, but rather mount an effective immune response and limit the growth of the TB bacilli (this stage is called “primary TB”)
o Primary TB usually affects the lower and middle lungs and heals with no clinical symptoms in more than 90% of cases, often by fibrosis and calcification
Sputum smears showing acid-fast bacilli

o These people have long-lasting partial immunity and a positive tuberculin skin test o Later, the partial immunity may wane, putting them at risk of developing active TB o The lifetime risk of someone infected with the TB bacilli developing disease is 10% o “Latent TB” refers to the state in which a person has the organism
in their body but experiences no symptoms or measurable damage • Active Pulmonary TB typically develops 2 years after infection (if at all)
o The early lesion is a small granulomatous bronchopneumonic infiltration
o Typically affects upper lobes and apical portions of lower lobes o Caseation can occur and the necrotic center may be discharged
into the bronchi, leaving a “cavity” in the lung o Infected sputum can be aspirated to other segments in the lung and
cause bronchogenic spread
Pathologic Findings
• Caseating granulomatous reactions in the lung (Ghon focus) and lymph nodes (Ghon complex)
o Caseating granulomas show central necrosis surrounded by a rim of epithelioid cells with giant cells and lymphocytes
o Primary pulmonary site and lymph nodes generally undergo calcification
Treatment
• Latent TB may be treated with 9 months of isoniazid to reduce risk of developing active TB o Monitor liver function, especially if HIV-positive, pregnant, age >35, or liver disease
• Active TB is treated with 6 months of directly observed therapy (DOT) o Isoniazid, rifampin, ethambutol and pyrazinamide (or streptomycin) for first 2 months o Isoniazid and rifampin for subsequent 4 months
• Treatment of multidrug-resistant TB (MDR-TB) is much more problematic because it requires the use of second line anti-TB agents, which are usually more toxic and less effective
o Treatment usually takes more than one year and there is still high mortality o New molecular genetic techniques are helpful to distinguish related cases of TB in the
community (“clusters”) and to potentially predict drug resistance patterns
Gross lung showing consolidation and a caseous granuloma
Gross lung showing miliary (like millet seed) pattern of
tuberculosis, which may be a reactivation form of disease or
primary with immune deficiency

Immunology of Granulomas • Granuloma formation is the end result of a complex interplay of factors, including antigen
invasion, prolonged antigenemia, macrophage processing and presentation, CD4+ T-helper cell response, B-cell overactivity, circulating immune complexes, and biochemical mediators
• Antigen-presenting cells with MHC class II molecules present antigens to T-helper cells • T-cells induce macrophages to produce interleukin-1 (IL-1)
o Th-1 cells produce IL-2, IFN-γ, and TNF-α, and participate in delayed hypersensitivity o Th-2 cells produce IL-4, IL-5, and IL-10, which are important for development of B-
cells and eosinophilic inflammation Differentiating Granulomatous Diseases by Histology Tuberculosis Sarcoidosis Hypersensitivity
Pneumonitis Fungi Brucellosis
Caseation Present Absent Rare Absent Absent Necrosis Present Rare Rare Present Maybe Inclusions Rare Present (70%) Rare Rare Rare Eosinophils Minimal Present Prominent Absent Absent Vasculitis Rare Rare Maybe Maybe Maybe Bronchiolitis Rare Rare Present Absent Absent Differentiating Granulomatous Diseases by Chest X-ray Tuberculosis Sarcoidosis Hypersensitivity
Pneumonitis Wegener’s Granulomatosis
Hodgkin Disease
Fungi
Hilar Adenopathy
Unilateral Bilateral Absent Absent Unilateral Unilateral
Parenchymal Infiltrate
Localized, miliary
Lower, middle fields
Diffuse Rare, nodular Uncommon Common
Cavity Formation
Common Rare Rare Common Rare Rare
Mediastinal Adenopathy
May occur May occur Absent Absent Common May occur
Pleural Effusion
Common Unusual Absent Rare May occur May occur
Large Nodules
May occur May occur Absent Common Common May occur

Pulmonary Embolism Obstruction of one or more branches of the pulmonary artery by a blood clot or foreign material Etiology
• Vast majority of emboli originate from thrombi formed in the deep veins of the legs o Thrombi from the heart, pelvic veins, renal veins and veins of
the arms are less common o Fat, tumor cells, amniotic fluid, septic vegetations or foreign
materials can also embolize to the pulmonary circulation Pathogenesis
• Vessel occlusion results in decreased perfusion to distal lung, resulting in increased dead space
o Decreased blood flow leads to decreased surfactant production, decreased alveolar ventilation and decreased CO2 excretion
o Compensatory hyperventilation leads to decreased pCO2 o Reduced pCO2 leads to bronchoconstriction, atelectasis and
hypoxemia o Bronchoconstriction due to release of mediators shifts
ventilation away from normal lung • Vessel occlusion and release of mediators may result in increased
vascular resistance usually after 50-70% of vascular bed occluded o Large increase in vascular resistance results in right ventricular
failure with decreased cardiac output, hypotension, syncope and death
Clinical Findings
• Signs and symptoms are non-specific (may be asymptomatic) • May see dyspnea, tachypnea, pleuritic chest pain, fever, cough,
hemoptysis, wheezing and syncope • EKG may show sinus tachycardia, right axis deviation, right bundle
branch block, and inverted T waves in leads V1-V3 • May have history of stasis, endothelial injury or hypercoagulable state • Chest x-ray findings vary and may be normal
o May show atelectasis, elevated hemidiaphragm, wedge-shape infiltrate (Hampton’s hump), decreased perfusion (Westermarks’ sign), or other findings
• Decreased or normal pO2, decreased pCO2, and increased pH • Characteristic finding in pulmonary embolism is an area that has no
perfusion but normal ventilation (V/Q mismatch) o Normal ventilation and perfusion effectively rules out
pulmonary embolism o V/Q scan showing multiple segmental or larger perfusion
defects with normal ventilation gives a high probability of pulmonary embolism
o Matched ventilation and perfusion defects or mismatched defects less than segmental are considered intermediate probability of PE and require further studies
Studies are aimed at diagnosis of DVT (eg. Doppler ultrasound)
• Pulmonary angiogram is the gold standard for diagnosis of PE
Atelectasis
Hampton’s hump
Westermarks’ sign
Pulmonary angiogram showing vessel cut-off

Complications • Acute mortality is usually due to right heart failure • Major long-term complication is pulmonary hypertension
Treatment
• Standard treatment is anticoagulant therapy o Intravenous heparin followed by coumadin
• Thrombolytic agents are used for massive embolism or hemodynamic compromise (RV strain) o Streptokinase or recombinant tissue plasminogen activator (rTPA)
• Inferior vena cava filter may be used if anticoagulation therapy is contraindicated Fat Embolism
• Usually occurs after traumatic fracture of long bones o Delay of 24-48 hours
• Fat in venous circulation obstructs capillaries of lung, skin, brain • Clinical triad of dyspnea, petechiae, and mental status changes • Therapy is supportive with oxygen and mechanical ventilation
o No anticoagulation Septic Embolism
• Associated with intravenous drug use and indwelling vascular catheters • Composed of purulent material mixed with thrombus • Chest x-ray shows patchy infiltrates that cavitate • Treat with antibiotics (and line removal, if appropriate)
Pneumothorax Accumulation of air in the pleural space Clinical Findings
• Pleuritic chest pain • Dyspnea • Cough (occasionally) • Decreased breath sounds • Hyperresonant percussion note • Evidence of shift of the mediastinum to the contralateral side of a
tension pneumothorax o A tension pneumothorax results from a wound in the chest
wall that acts as a valve, permitting air to enter the pleural cavity but preventing its escape
o Tension pneumothorax is also associated with decreased blood pressure
o Tension pneumothorax is a true medical emergency Treatment
• Oxygen and observation • Chest tube • Surgery • Pleurodesis (surgical creation of a fibrous adhesion between the visceral and parietal layers of
the pleura, thus obliterating the pleural cavity)
Chest x-ray of septic embolism
Chest x-ray of a large, right-sided tension pneumothorax showing a leftward shift of the mediastinum

Pleural Effusion Accumulation of fluid in the pleural space Types of Pleural Effusion
• Transudative pleural effusion is one that develops secondary to a disease process not directly involving the pleura (eg. congestive heart failure)
• Exudative pleural effusions are produced by disease processes directly involving the pleura (eg. tumor)
• Hemothorax is a bloody effusion generally developing after trauma (hematocrit exceeds 1%) • Hemorrhagic pleural effusion is a bloody effusion with a hematocrit less than 1%, often related
to a tumor but may also be seen in tuberculosis • Chylous pleural effusion generally develops after obstruction of the lymphatics, often in
association with tumors • Empyema is pus in the pleura, generally related to anaerobic infection of the pleura • Parapneumonic effusions develop in association with pneumonia but without direct infection of
the pleura • Lobulated pleural effusions develop in localized areas of the pleura without demonstrable free
fluid Clinical Findings
• Dyspnea • Pleuritic chest pain (stabbing, inspiratory chest pain over entire chest) • Cough with sputum production • Fever and weight loss • Decreased breath sounds • Dullness to percussion • Decreased movement of hemithorax • Egophony • Tachypnea • Thoracentesis should be performed to differentiate exudates from transudates
o With an exudate, the pleural fluid will have one or more of the following characteristics:
LDH greater than 2/3 of serum LDH Protein greater than 1/2 of serum protein LDH greater than 0.6 times the high end of the normal serum range
Common Causes of Transudates and Exudates Transudates: Exudates:
• Congestive heart failure • Cirrhosis of the liver • Nephrotic syndrome • Myxedema (rare)
• Neoplasm • Tuberculosis • Pancreatitis • Empyema • Rheumatoid arthritis • Systemic lupus erythematosus • Parapneumonic effusions
Treatment
• Primarily directed toward underlying disease process • Tube thoracostomy or, rarely, open surgical drainage may be needed to drain the fluid from the
pleural space

Diffuse Interstitial Lung Disease A family of restrictive lung diseases that share the finding of fibrosis or inflammation of the pulmonary interstitium with the final common pathway of honeycomb fibrosis Etiology
• There are over 130 causes of DILD: o Infectious causes such as bacteria, mycobacteria, fungi, viruses and parasites o Inhalants such as organic dusts, inorganic dusts and toxic fumes o Neoplastic causes such as metastases and broncho-alveolar cell neoplasms o Cardiovascular causes such as heart failure and embolism o Immunologic causes such as connective tissue disease, Goodpasture disease and
Wegener granulomatosis o Iatrogenic causes such as drugs and radiation o Idiopathic causes such as sarcoidosis, UIP, NSIP, DIP, AIP, LIP and BOOP o Aspiration o Adult respiratory distress syndrome
• Only 35% of patients with DILD have an identifiable cause Clinical Findings
• Dyspnea is a cardinal sign o Due to the increased work of breathing in poorly compliant lungs
• Tachypnea with shallow respirations • Hypoxemia • Non-productive cough is common • Weight loss, anorexia and fever may be present • Increased A-a O2 gradient is the most sensitive measurement for presence of DILD
o Vital capacity is decreased o Total lung capacity is decreased o Diffusing capacity (DL) is decreased o Compliance is decreased
• Chest x-ray is normal in 10% of patients

Idiopathic Pulmonary Fibrosis A chronic fibrosing interstitial pneumonitis of undetermined etiology Prevalence
• Most common of the idiopathic interstitial pneumonias • Most patients are 40-70 years old • Men are more affected than women (2:1)
Pathogenesis
• Pathogenesis appears to involve multifocal injury to the lung over a period of years, resulting in an accumulation of minute scars in the pulmonary interstitium
• Studies indicate the presence of an alveolitis in the form of increased neutrophils within alveolar lumens and lavage fluid shows the presence of inflammatory mediators
Clinical Findings
• Patients usually present with dyspnea and dry cough of months or years duration
• Clubbing of fingers, hypoxemia, and restrictive pulmonary function studies are typical
• May have rheumatoid factor or antinuclear antibodies in blood • Chest X-ray shows bilateral reticular or reticulonodular infiltrates
affecting predominantly lower lobes, with production of peripheral lung honeycombing
Pathologic Findings
• Grossly, the lung is firm, gray, and contracted due to fibrosis o Often shows honeycomb cysts beneath the pleura o The fibrosis is typically predominant in the lower lobes,
or the lower aspects of all lobes • Microscopically, IPF shows the usual interstitial pneumonia (UIP)
pattern characterized by: o Patchy involvement of lung by fibrosing interstitial
pneumonitis (“geographic heterogeneity”) o Variation in the age of the fibrosis with areas of young fibrosis
(fibroblast foci) and older fibrosis (“temporal heterogeneity”) Fibroblast foci may represent the advancing or
progressive edge of the disease, areas of organization of acute lung injury with myofibroblasts present
These foci are not pathognomonic of UIP pattern, but they are necessary for the diagnosis
o Interstitial chronic inflammation composed of lymphocytes and plasma cells
o Alveolar inflammation composed of macrophages and some neutrophils
o Cellular proliferation of type 2 cells, bronchiolar cells, fibroblasts, myofibroblasts, and smooth muscle
o Honeycombing cysts lined by bronchiolar epithelium, caused by destruction of alveolar spaces
Treatment
• Steroids, with or without cyclophosphamide (poorly effective) or lung transplantation
Chest x-ray showing bilateral reticular infiltrates, largely involving the lower lobes
Gross lung showing cystic spaces (honeycombing)
predominantly in the lower lobe and anterior aspect of
the upper lobe

Rheumatoid Interstitial Pneumonitis Prevalence
• Found in up to 17% of patients with rheumatoid arthritis • Usually occurs in men over 60 years old
Clinical Findings
• Tachypnea • Rales and rhonchi on auscultation • Elevated RA titers • Chest x-ray shows diffuse, interstitial process involving
both lung fields Pathologic Findings
• Grossly, honeycombing cysts are apparent beneath the pleura • Microscopically, rheumatoid interstitial pneumonitis shows the usual interstitial pneumonia
(UIP) pattern, with honeycombing
Drug-Induced Pneumonitis A variety of toxic manifestations in lung caused by drug use, ranging from chronic interstitial pneumonitis, diffuse alveolar damage, eosinophilic pneumonia, pulmonary hemorrhage, edema or pulmonary hypertension (Bleomycin will be used as an example) Clinical Findings of Bleomycin Toxicity
• Cough and dyspnea • Chest x-ray shows diffuse pulmonary infiltrates
Pathologic Findings of Bleomycin Toxicity
• Histologic findings are most often those of diffuse alveolar damage o Characterized by hyaline membranes, replicating type 2 cells, and interstitial edema
• Later stages of the disease show interstitial scarring or interstitial fibrosis o Often there are markedly atypical alveolar lining cells, produced by the cytotoxic
effects of the drug itself • Acute pulmonary hemorrhage and eosinophilic pneumonia are less common manifestations
High-resolution CT showing numerous cysts bilaterally, consistent with honeycombing
Gross lung showing numerous cysts and tan-gray tissue, consistent with honeycombing fibrosis
Interstitial chronic inflammation with fibrosis and honeycombing

Hypersensitivity Pneumonitis (Extrinsic Allergic Alveolitis) An inflammatory reaction in the distal lung caused by hypersensitivity to a variety of inhaled antigens Etiology
• Hypersensitivity is most frequently to organic proteins derived from birds, mammals, fungi and thermophillic bacteria, but rarely inorganic antigens
• Classic examples are due to common occupations (“farmer’s lung”), unusual occupations (“maple bark stripper’s lung,” “malt worker’s lung”), hobbies (“bird fancier’s lung”), and, in the urban environment, “air conditioner lung” and “home humidifier lung”
Pathogenesis
• Inhaled insoluble particulates measuring 1-3 micra in diameter reach the distal lung, where they evoke an immune reaction in a susceptible host
• Cellular immunity mediated by T cells and possibly humoral mediators (immune complexes) may both play a role in the production of the inflammatory reaction
Clinical Findings
• Fever, chills, and a flu-like syndrome occur 2-9 hours after exposure to antigen
• Chronic exposure to antigens can be associated with gradual onset of cough and exertional dyspnea
• Chest x-ray shows a diffuse reticular or reticulonodular pattern Pathologic Findings
• Interstitial pneumonitis characterized by interstitial lymphoplasmacytic infiltrate
• Poorly-formed interstitial and peribronchiolar granulomas (in 2/3 of cases)
• Tufts of organizing fibrous tissue in terminal and respiratory bronchioles and alveolar ducts
o These are sites where the antigen is deposited and evokes an inflammatory response
• Foci of foamy alveolar macrophages may be seen in the distal alveolar lumens due to airway obstruction (most prominently in pigeon breeder’s lung)
Treatment
• Treatment of choice is early diagnosis and avoidance of the antigen
• Corticosteroids can be used to treat acute exacerbations
High-power microscopy shows an interstitial
pneumonitis, with lymphocytes and other mononuclear cells in the interstitium, and an ill-formed granuloma
Low-power microscopy shows a uniform interstitial disease, with preservation of the alveoli and an inflammatory infiltrate within the interstitium

Asbestosis Interstitial fibrosis occurring as a result of inhalation of asbestos fibers Pathogenesis
• Fibers deposit preferentially at respiratory bronchioles, where they may be phagocytosed by alveolar macrophages or penetrate the epithelium
• The development of interstitial scarring can take 15 years to several decades and progresses long after initial exposure because the fibers, particularly amphiboles, are hard to break down and may remain for prolonged periods in lung
Clinical Findings
• Shortness of breath progressing to respiratory failure • Dyspnea and cough • Patients generally have a history of long, relatively intense
exposure to asbestos • Chest x-ray shows bibasilar reticular infiltrates involving
predominantly the lower lobes o Parietal and diaphragmatic pleura typically show bilateral
calcified plaques Pathologic Findings
• Grossly, the lung is small with a gray/white fibrous appearance in lower lobes, often with honeycombing cysts
• Microscopically, early disease shows fibrosis around respiratory bronchioles with subsequent extension into the alveolar interstitium, producing a UIP pattern
• At least one ferruginous (asbestos) body should be present o Ferruginous bodies are long asbestos fibers that are coated
with iron and mucopolysaccharides o Can be seen lying among macrophages within alveoli or in a
peri-bronchiolar location o Occur as a result of an interaction of macrophages and giant
cells with large fibers in which iron is derived from the macrophages, presumably to wall off the toxic asbestos
Iron stain showing iron-positive macrophages
Ferruginous bodies

Neoplasms of the Lung Prevalence
• Lung cancer accounts for 13% of all new cancers • Lung cancer is the leading cause of cancer deaths for both sexes
o Overall 5-year survival rate is only 14% • More common in African Americans, less common in Asians and Hispanics • Peak incidence in ages 60-79
Staging
• Survival is related to disease stage • Staging is based on number of tumors, nodes, and metastases (TNM staging) • Surgery with curative intent is limited to stages IA, IB, IIA, and IIB • No surgery for either stage IIIB or IV disease
o Four tumors or three nodes involved equals stage IIIB disease o Any metastasis equals stage IV disease
• Always sample the potentially highest staging lesion (eg. likely metastases, over lymph nodes) Histologic Classification of Lung Carcinoma
• Squamous carcinoma (35-40% of all lung cancers) o Usually develops in a central location in a main, lobar, segmental or subsegmental
bronchus, but may occur anywhere o Grossly, squamous carcinoma is usually a firm, off-white mass that may protrude into
the lumen of the bronchus Central cavitation of the lesion due to necrosis is common Microcalcification may be present
o Well-differentiated squamous carcinoma is characterized by polygonal, pink-staining cells showing keratinization with keratin pearls and intercellular bridges (prickles)
o Poorly-differentiated tumors will show desmosomes and cytokeratin filaments by electron microscopy
o Associated with paraneoplastic condition of ectopic PTH and hypercalcemia o Death is often due to local extension into the mediastinum and chest
Squamous carcinoma, showing polygonal, pink cells with keratinizing
features
High-power view of squamous carcinoma, showing intracellular bridges
(prickles) and keratinizing features
Papillary variant of squamous carcinoma, which typically carries a better prognosis

Adenocarcinoma (40%) o Usually occurs in the periphery of the lung, but may arise in
the glandular epithelium of the large bronchi o Grossly, adenocarcinomas exhibit pleural puckering and may
show a black anthracotic pigment May glisten on cut section due to mucin production Often associated with peripheral scars in the lung
parenchyma o Microscopically, papillary, acinar or solid patterns may be
seen Mucin production is common Giant cell variants and mixed forms may also be seen
o Death is usually caused by metastatic rather than local disease
• Undifferentiated small cell carcinoma (“oat cell carcinoma”) (10-25%)
o Strongly associated with smoking o Arises from the neuroendocrine cells of the bronchial
mucosa (Kulchitsky cells) o Almost always found centrally, due to cell of origin
Tends to arise in a large bronchus but invade around the bronchus and into surrounding structures such as hilar lymph nodes
Rarely produces an intraluminal mass Circumferential extension may stenose the bronchial
lumen o Grossly, the tumors are gray-white, soft and fleshy
Necrotic areas may be present o Microscopically, the tumors are composed of cells with
intermediate (15-25 micron) nuclei which are round, oval or fusiform (oat-like)
Nuclei are stippled with absent or inconspicuous nucleoli
Cells have scant cytoplasm o Associated with most lung cancer paraneoplastic syndromes o Small cell carcinomas are highly malignant and metastasize
early and widely, often to the brain and bone marrow
Gross adenocarcinoma, showing a nodular pleural tumor with
slight dimpling over the surface
Acinar pattern of adenocarcinoma, showing irregular-shaped glands (acini) with hyperchromatic and irregular nuclei
Papillary pattern of adenocarcinoma, showing growth in a papillary pattern on
fibrovascular cores
Signet ring pattern of adenocarcinoma, showing tumor cells with abundant
intracellular mucin and peripheral nuclei
Small cell carcinoma, showing nuclear stippling, inconspicuous
nucleoli, and mitotic figures
Small cell carcinoma, showing a fusiform (spindle-shaped) pattern

• Undifferentiated large cell carcinoma (5-20%) o A wastebasket term for tumors composed of large
cells, usually with abundant cytoplasm, that show no obvious squamous or glandular differentiation by light microscopy
Electron microscopy and immunohistochemistry can usually demonstrate such differentiation and this diagnosis is becoming less common
The important distinction is from small cell carcinomas, which are likely to be chemosensitive
• Bronchioloalveolar carcinoma (3-5%) o A less common distinct subtype of adenocarcinoma o Always occurs in the periphery of the lung, arising in the
terminal bronchioles and alveolar air spaces and spreading along the fibrous septae of the alveolar air spaces
o Nonmucinous bronchioloalveolar carcinomas are derived from either type II alveolar pneumocytes or Clara cells
Tend to be singular lesions with a good prognosis o Mucinous bronchioalveolar carcinomas consist of uniform,
tall columnar epithelium with abundant apical mucin and extremely bland nuclei
Tumors are often multifocal and may spread aerogenously (within lung by normal respiration)
• Carcinoid tumors (1-2%) o Low-grade tumors of bronchial origin, related to
Kulchitsky cells o Like small cell carcinomas, these occur centrally, often with only a small ulcerated
tumor area visible in the bronchus 90% or more of the tumor mass is below the bronchus, extending into the
pulmonary parenchyma o Tumors are well-circumscribed and slow-growing o May cause endocrine symptoms such as Cushing syndrome
So-called “carcinoid syndrome” due to serotonin excretion is rare in pulmonary carcinoids
o Microscopically, tumors consist of small, uniform cells arranged in clusters, cords or tubules
Cells have round, even nuclei and well-defined cytoplasm Neurosecretory granules are visible by electron microscopy
Carcinoid tumor, showing an organoid nesting pattern surrounded by a fine
vascular stroma (“Zellballen”)
Carcinoid tumor, showing a trabecular pattern
Atypical carcinoid tumor, showing a small focus of necrosis
Large cell carcinoma, showing large epithelial cells with no evidence of
squamous or glandular differentiation
Non-mucinous (top) and mucinous (bottom) bronchioloalveolar carcinomas

• Malignant mesothelioma o Strongly associated with asbestos exposure
Smoking is also a contributing factor o A deadly malignant neoplasm arising from the
mesothelial linings of body cavities, especially the pleural surfaces
o The tumor commonly spreads over the lung surfaces, enclosing them in a strangling, firm, gray, partially gelatinous fibrous mass
o Invasion of both the lung parenchyma and chest wall is common, with the ultimate formation of a rind of unyielding tumor that suffocates the patient by restricting respiratory motion
o Microscopically, the tumor usually exhibits both spindle-cell and epithelioid elements Electron microscopy shows the presence of long microvilli and tonofilaments
Clinical Findings
• Central carcinomas (arising in the first, second or third order bronchi, of any of the above histological types) generally present with cough, hemoptysis and shortness of breath
o Weight loss and chest pain tend to occur later in the disease • Peripheral carcinomas are often free of symptoms until late in the disease
Special Clinical Presentations
• Bronchial obstruction can lead to unresolving pneumonia, lung abscess, and bronchiectasis • Local invasion of the pleura or pericardium causes pleural effusion • Local invasion of the thoracic duct may cause chylothorax • Blockage of the superior vena cava causes edema of the face, neck and brain (“superior vena
cava syndrome”) • Destruction of the T1 intercostal nerve and cervical sympathetic trunk due to invasion of the
apical pleura causes “Pancoast syndrome” o T1 motor and sensory deficit o Weakness and wasting of small muscles of the hand o Numbness of the medial side of the arm o Horner syndrome (ptosis of the eyelid, papillary constriction and absence of sweating
on the side of the lesion)
Mesothelioma, showing a biphasic pattern of both spindle cell and
epithelioid components
Tubulopapillary variation of the epithelial pattern of mesothelioma
Monophasic spindle cell variant of mesothelioma
Gross appearance of mesothelioma, showing a thick rind of dense adherent tumor covering the pleural surface of
the lung

Metastatic Cancer • Cancer metastasizing from another part of the body is the number
one type of cancer found in the lung • Cancer metastasizing to the lung often has a “cannonball”
appearance grossly Paraneoplastic Syndromes
• Hypercalcemia o Due to ectopic PTH-like secretion, most commonly in
squamous cell carcinoma o May also be due to bone metastasis
• Hyponatremia and SIADH o Most commonly seen in small cell carcinoma
• Cushing Syndrome o Due to ectopic ACTH or CRH, most commonly in small
cell carcinoma or carcinoid • Neurologic syndromes
o Neuromyopathies, peripheral neuropathies, subacute cerebellar degeneration, dementia o All most commonly seen in small cell carcinoma
• Hypertrophic pulmonary osteoarthropathy o Painful symmetric arthropathy due to proliferative periostitis involving ankles, wrists
and elbows o Most commonly seen in large cell carcinoma and adenocarcinoma (but does not rule out
small cell carcinoma) • Eaton-Lambert Myasthenic Syndrome
o Muscle weakness, hyporeflexia, and autoimmune dysfunction o Antibody to peripheral cholinergic nerve terminal voltage-gated channel o Commonly associated with small cell carcinoma
Gross appearance of metastases in the lung

Adult Respiratory Distress Syndrome A clinical syndrome whose hallmark is non-cardiogenic pulmonary edema resulting in severe respiratory distress and hypoxemic respiratory failure Etiology
• Systemic inflammation, commonly due to trauma, sepsis or pancreatitis
• Direct injury to the lung, commonly due to aspiration of gastric contents, severe pneumonia or toxic gas inhalation
Pathogenesis
• ARDS results from increased capillary permeability due to endothelial damage • The injured capillary bed leaks protein-rich fluid into the interstitial space, eventually causing
alveolar flooding and impaired gas exchange • Obliteration of the pulmonary microvasculature by platelet aggregates, leukoagglutination,
thrombosis and endothelial swelling accompanied by hypoxic vasoconstriction produces pulmonary hypertension and worsens gas exchange
• Loss of surfactant leads to increased alveolar surface tension and atelectasis Clinical Findings
• Chest x-ray shows diffuse bilateral infiltrates • PaO2 less than 60 mmHg on FiO2 of 0.5
o Accompanied by low PaCO2 in the early stages of disease • Normal pulmonary capillary pressure • Reduced functional residual capacity (FRC), due to stiffened lungs
Pathologic Findings
• Grossly, lungs are heavy and red with congestion and edema • In the acute phase, the alveolar wall and interlobular septum are
thickened by edema fluid o The hallmark of this phase is the presence of eosinophilic
hyaline membranes composed of fibrin and cellular debris, found lining the alveolar ducts in particular
o Hyaline membranes are usually associated with damaged type I alveolar epithelial cells or areas where the epithelial lining has been sloughed away, leaving a bare basal lamina
• In the subacute or proliferative phase (4-10 days) the severity of edema is generally lessened o Hyaline membranes are less frequently encountered o Many alveoli are lined with type II pneumocytes that have proliferated to cover the
denuded basement membrane o Mild interstitial fibrosis occurs
• In the chronic phase, alveolar architecture gradually returns to normal o In a minority of cases, fibrosis continues to the point of obliteration of the alveolar and
bronchiolar spaces Treatment
• Treat the underlying cause • Supplemental O2 to increase PaO2 • Mechanical ventilation may be required (with positive end-expiratory pressure)
ARDS NRDS (neonatal) Causes Shock, infection,
trauma, aspiration Lack of surfactant
Pathophysiology Impaired gas exchange caused by pulmonary hemorrhage, pulmonary edema or atelectasis
Surfactant production begins at 24 weeks gestation and is complete at 37; without surfactant the infant can clear lungs of fluids, but can’t fill lungs with air
Acute ARDS, showing alveoli lined by hyaline membranes

Obstructive Sleep Apnea-Hypopnea Syndrome A sleep breathing disorder characterized by repetitive obstructive apneas or hypopneas resulting in sleep fragmentation and intermittent hypoxia and hypercarbia Prevalence
• 2-4% of middle-aged adults suffer from OSAHS • More common in males and obese patients
Etiology
• Collapse of the pharyngeal airway • Predisposing factors include tonsillar hypertrophy, pharyngeal mass, severe nasal obstruction,
hypothyroidism, and use of ethanol or sedatives Clinical Findings
• Habitual snoring with or without witnessed apneas • Nocturnal gasping or snorting episodes • Morning headaches and daytime hypersomnolence • Memory loss and decreased mental function • Diagnosis is by standard overnight polysomnogram demonstrating an apnea-hypopnea index of
greater than 5 events per hour o An obstructive apnea pattern is cessation of respiratory airflow for
greater than 10 seconds associated with continued respiratory effort o Hypopnea is a significant reduction in airflow that is associated
with respiratory effort, oxygen desaturation and an EEG arousal Treatment
• Address reversible causes of OSAHS • Oral appliances and dental devices to maintain patent airway • Continuous positive airway pressure (CPAP) is the most effective non-
invasive therapy • Tracheostomy is the most effective invasive treatment
Central Sleep Apnea Syndrome A sleep breathing disorder characterized by simultaneous cessation of respiratory effort and airflow Etiology
• Neurologic disorders or congestive heart failure Clinical Findings
• Patients rarely snore • Insomnia and frequent nighttime arousal • Diagnosis is by standard overnight polysomnogram demonstrating an apnea index of greater
than 5 events per hour o Central sleep apnea shows a pattern of simultaneous cessation of respiratory airflow for
greater than 10 seconds and cessation of respiratory effort Treatment
• Treat the underlying cause • Acetazolamide, low flow O2, and nasal CPAP/BIPAP are commonly used
Nasal CPAP

Acquired Immune Deficiency Syndrome A secondary form of immune deficiency caused by the human immunodeficiency virus (HIV) Laboratory Diagnosis of HIV Infection
• Screening test is performed by enzyme-linked immunosorbent assay (ELISA) o Tests for multiple HIV-associated antigens including p24, a major structural protein that
may be measurable before any antibody formation • Confirmatory test is commonly performed by Western blot analysis
o Identification of a matching band from two of the three main viral product regions (env, gag and pol) is generally considered positive
Categorization of HIV Infection Based on CD4+ T-cell Counts
• ≥ 500 per mm3 Category 1 • 200-499 per mm3 Category 2 • < 200 per mm3 Category 3 (AIDS)
Categorization of HIV Infection Based on Indicator Conditions
• Group A o Asymptomatic HIV infection o Acute seroconversion syndrome (primary HIV infection) o Generalized lymphadenopathy
• Group B o Candidiasis (oral or vulvovaginal) o Herpes zoster, involving at least two distinct episodes or more than one dermatome o Listeriosis o Peripheral neuropathy o Idiopathic thrombocytopenic purpura o Oral hairy leukoplakia
Virtually 100% of patients with oral hairy leukoplakia are HIV-positive Lesions present as asymptomatic white to yellow patches along the lateral
border and inferior surface of the tongue, often with a hairy or corrugated appearance
o Bacillary epithelioid angiomatosis A skin disease characterized by red papules due to proliferations of small round
vessels with well-defined lumens lined by plump endothelial cells Associated with Bartonella henseli bacteria
o Cervical dysplasia or carcinoma-in-situ • Group C (AIDS)
Fungal Infections: o Pneumocystis carinii pneumonia
Initial manifestation of AIDS in 60% of patients Clinical features include shortness of breath, fever, hypoxia and non-productive
cough X-ray may show diffuse interstitial infiltrate or solitary or multiple nodules Histology shows alveoli full of foamy eosinophilic material Cysts are ovoid to cup-shaped, often with a dot-like cyst wall thickening
• Budding is never seen
Note: Once a patient has met the criteria for one group or category, he or she can never return to an earlier categorization (even if CD4+ count improves or indicator condition resolves)

o Cryptococcosis, extrapulmonary Cryptococcus neoformans is the second most common form of fungal
pneumonia (not AIDS-defining) Cryptococcus neoformans is a round, pleomorphic, budding yeast
• It’s thick capsule retracts in tissue sections leaving a halo around the organism
• Can be stained by Mayer mucicarmine because of mucopolysaccharide capsule
o Histoplasmosis, disseminated or extrapulmonary Histoplasma capsulatum is a tiny yeast, characterized by narrow-based budding
• Intracellular organisms usually show a thin halo • Can be differentiated from Cryptococcus by their small size and uniform
shape o Coccidioidomycosis, disseminated or extrapulmonary
Coccidioides immitis is not a yeast and does not bud • Characterized by large spherules with thick wall, filled with endospores
o Candidiasis of bronchi, trachea, lungs or esophagus Oral (thrush) and vulvovaginal candidiasis are frequent early in the course of
HIV infection (not AIDS-defining) Candida pneumonia occurs later and is associated with disseminated disease Endoscopy shows characteristic cheesy white plaques on an erythematous base
progressing to ulceration and pseudomembrane formation Histology shows a mixture of both budding yeast forms and segmented
pseudomycelial forms invading into mucosal surfaces Bacterial Infections: o Mycobacterium tuberculosis
TB occurring late in HIV disease may be characterized by negative tuberculin reaction and atypical x-ray findings including massive intrathoracic adenopathy, involvement of the lower lung zones and diffuse infiltration
Extrapulmonary dissemination is common and extensive Histology may show granulomas or minimal inflammation
• In late disease, clusters of foamy histiocytes filled with acid-fast bacilli may be seen
o Mycobacterium avium intracellulare complex or Mycobacterium kansasii, disseminated or extrapulmonary
Acid-fast, PAS-positive, GMS-positive organisms are found almost entirely within histiocytes
• Likely to be seen in areas with many histiocytes, like spleen, lymph nodes, liver, bone marrow and lamina propria of the GI tract
These organisms are ubiquitous and normally do not cause disease MAI is the most common systemic bacterial pathogen in AIDS Respiratory involvement is relatively insignificant
o Salmonella septicemia, recurrent

Viral Infections: o Cytomegalovirus, other than liver, lymph nodes or spleen
50-95% of the population has some evidence of CMV infection, but it is normally latent
CMV infection is characterized by the presence of large cells with basophilic or eosinophilic nuclear inclusions separated from the nuclear membrane by a clear halo that imparts an “owl’s eye” appearance to the infected cells
In HIV, CMV is associated with interstitial pneumonias causing shortness of breath and dry cough
GI involvement of the esophagus, stomach, colon, gall bladder, liver and pancreas can cause pain, obstructive symptoms, bleeding, and watery diarrhea
CMV is an important opportunistic pathogen of the brain and may cause severe necrotizing inflammation of the brain, meninges and cerebral ventricles
CMV retinitis causes an irregular flat yellow lesion along the vessels of the eye o Herpes simplex, chronic ulcers (> 1 month duration) or bronchitis, pneumonitis, or
esophagitis Histology shows a ground-glass nucleus, possibly accompanied by
multinucleation and nuclear molding or a fluffy eosinophilic inclusion surrounded by a clear halo (Cowdry type A inclusion)
HSV typically infects and destroys squamous epithelial cells, causing cutaneous, oral, esophageal and genital ulcerations
o Progressive multifocal leukoencephalopathy PML is a demyelinating disease associated with patches of irregular, ill-defined
granular destruction of white matter • Lesions are said to resemble astronomic images of galaxies • Lesions include a star-shaped area of demyelination with lipid-laden
macrophages surrounded by a somewhat hypercellular rim of oligodendrocytes
• Oligodendrocyte nuclear chromatin is replaced by a glassy amphophilic viral inclusion associated with the JC-polyoma virus
Parasitic Diseases: o Toxoplasmosis of brain
Subacute symptoms develop over 1-2 weeks Multiple focal abscesses form in the cerebral cortex near the gray-white matter
junction and deep gray nuclei Histology shows central foci of necrosis and hemorrhage surrounded by acute
and chronic inflammation • Ovoid or crescent-shaped Toxoplasma gondii organisms may be seen in
cysts (bradyzoites) or free (tachyzoites) • Giemsa stain shows blue cytoplasm and a red-purple nucleus near the
blunted end of the organism o Cryptosporidiosis, chronic intestinal (> 1 month duration)
Cryptosporidia infection causes a severe watery diarrhea, electrolyte imbalance, malabsorption, severe pain and weight loss
Endoscopy shows small erosions on thickened mucosal folds Biopsy shows tiny, dark blue, spherical organisms in the brush borders of
intestinal villi Cryptosporidia may also cause inflammation of the gallbladder, without stones
o Isosporidiosis, chronic intestinal (> 1 month duration) Isospora is an intestinal protozoan parasite similar to Cryptosporidia

Tumors: o Kaposi Sarcoma
Forms an infiltrative lesion composed of spindle-shaped tumor cells of endothelial (capillary lining cell) origin
• Tumor cells tend to form poorly-defined “vascular slits” • Red cells are usually present within these slits and tend to spill out
(erythrocyte extravasation) • Brown hemosiderin pigment usually accompanies the proliferation • Factor VIII stains are positive, demonstrating vascular endothelial origin
Lesions may occur in skin, mucous membranes, lymph nodes, GI tract, lungs or abdominal viscera
Much more common in homosexual patients, for unknown reasons May be associated with Human Herpesvirus 8 (HHV-8)
o Lymphomas, Burkitt, immunoblastic or primary in brain Malignant lymphomas in AIDS are usually high-grade, of B-cell origin, and of
extranodal origin o Cervical cancer, invasive Degenerative States: o HIV-related wasting syndrome
Patients with AIDS frequently experience profound involuntary weight loss associated with chronic diarrhea, weakness, or fever
o HIV-related encephalopathy (AIDS dementia complex) Progressive dementia is common and begins insidiously with impaired memory,
decreased concentration and slow thought, accompanied by motor deficits, weakness, ataxia and behavioral changes
Progresses to profound dementia, paraplegia and incontinence Histology shows cellular infiltrates including macrophages, microglia,
astrocytes and multinucleated histiocytic cells throughout the brain • Infiltrates are seen most easily around small blood vessels • Demyelination is common • HIV antigen is demonstrated in the multinucleated cells
o Pneumonia, recurrent (of any origin)

Pharyngitis Inflammation of the mucous membranes and underlying parts of the pharynx Etiology
• Viral o Rhinovirus, coronavirus, parainfluenza, adenovirus, enterovirus, influenza, measles,
HSV, HIV, Epstein Barr, CMV • Bacterial
o Streptococcus pyogenes and other β-hemolytic Streptococci, anaerobic pharyngitis, Arcanobacterium haemolyticum, Mycoplasma pneumoniae (hominis), Chlamydia pneumoniae, Carynbacterium diphtheriae, mixed anaerobic infection (Vincent’s angina), Neisseria gonorrheae, Treponema pallidum
• Fungal o Candida
• Non-infectious o Behcet’s disease, Kawasaki disease
• Autoimmune o Aphthous, SLE, bullous pemphigoid
Clinical Findings
• Throat discomfort or pain • Pain on swallowing • Fever, headache, malaise • Mouth breathing, snoring, sleep apnea • Nasopharyngitis associated with coryza (common cold) suggests viral cause • Physical examination of the throat may reveal erythema, exudates, vesicles, ulcerations
o Pseudomembrane may be present o May be paralysis of muscles of mastication (trismus) due to deep neck space infection o May be deviation of uvula in peritonsillar abscess (quinsy)
Strep Throat (Streptococcus pyogenes)
• Strep. Pyogenes causes a wide range of diseases, including pharyngitis
o M protein contributes to virulence and complications • Usually spread by close contact, with outbreaks occurring
especially in the winter • Severe disease is characterized by marked pharyngeal pain,
odynophagia and high fever • The pharyngeal membrane becomes intensely erythematous • Patchy exudate is usually present on the tonsils and lymphoid nodules of the posterior pharynx • Treat with Benzathine PCN, PCNVK, Erythromycin, Azithromycin, or oral cephalosporins
o Treatment reduces morbidity and prevents rheumatic fever if given early Scarlet Fever (Group A Streptococci)
• Erythematous sandpaper rash on cheeks and trunk
• Caused by streptococcal erythrogenic toxin • Usually has benign course • Patients have strawberry tongue,
circumoral pallor and Pastia’s lines
Gram stain (left) and blood agar culture (right) of Streptococcus pyogenes

Vincent’s Angina • Ulcerative infection of the tonsils and pharynx caused by fusiform and spirochetal organisms • Most common in adolescents and young adults • Purulent exudate coats the pharyngeal membrane • Foul odor usually present • Can be associated with necrotizing ulcerative gingivitis (especially with HIV) and septic
jugular thrombophlebitis (fusobacterium necrophorum) Epstein Barr Virus
• Herpesvirus causing chronic infection in humans • Spread by close contact
o Commonly acquired in adolescence by kissing, causing mononucleosis
• Acute manifestations include fever and malaise o Adenopathy including tonsillar enlargement sometimes
causes respiratory compromise o Pharyngitis is sometimes exudative, making it difficult to distinguish from infection
with Group A Streptococcus o Hepatosplenomegaly can occur
Diphtheria (Corynebacterium diphtheriae)
• Corynebacterium diphtheriae is a pleomorphic Gram-positive bacillus
o Exotoxin causes both local and distant manifestations Inhibits RNA translocase, causing tissue necrosis
o Spread by contact and airborne droplets • Major cause of morbidity and mortality worldwide
o Rare in US due to immunization, but outbreaks occur • Cutaneous form of disease is usually benign
o Shallow ulcer with grayish necrotic membrane • Respiratory form of disease is more severe
o Initial symptoms include sore throat, low-grade fever, hoarseness, shallow ulceration of nares and upper lip, and dysphagia
o Grayish pseudomembrane develops, accompanied by cervical swelling and enlarged lymph nodes
o May cause respiratory compromise, especially in laryngeal disease
Patient develops palatal and hypopharyngeal paralysis Suffocation is a frequent cause of death in children
o Hematogenous spread of toxin causes distant organ damage Accounts for most morbidity and mortality Myocarditis is common
• Treat with antitoxin and antibacterials

Irritation Fibroma Clinical Findings
• Nodular mass of fibrous tissue with minimal inflammation • Usually arises at the bite line of the mouth or gingivodental junction
Treatment
• Surgical excision Pyogenic Granuloma Etiology
• Benign vascular neoplasm (type of hemangioma) • This lesion is neither pyogenic nor granulomatous
Prevalence
• Lesions commonly arise in gingiva of children, young adults, and pregnant women
Clinical Findings
• Solitary, rapidly growing, bright red papule that may or may not be pedunculated • Lesions ulcerate with very little provocation, leading to profuse and repetitive bleeding that
may be refractory to pressure or cautery Pathologic Findings
• Histology shows a dense vascular proliferation similar to granulation tissue • Lesion may undergo fibrous maturation or develop into a peripheral ossifying fibroma
Treatment
• Pregnancy-associated lesions may regress spontaneously • Other lesions often require electrocautery or laser treatment
Peripheral Ossifying Fibroma Prevalence
• Peak incidence is seen in young females Etiology
• Common reactive gingival growth of uncertain etiology • Some lesions arise secondary to maturation of persistent pyogenic granulomas
Clinical Findings
• Red, ulcerated, nodular lesion Treatment
• Complete deep surgical excision is recommended, as recurrence rate is 15-20%

Aphthous Ulcers “Canker sores” Prevalence
• Seen in 40% of the population, usually during the first two decades Clinical Findings
• Lesions are painful, shallow, red ulcerations with a thin mononuclear exudate and a zone of hyperemia that may develop secondary to bacterial infection
• Lesions persist for weeks and are often recurrent Glossitis Inflammation of the tongue, and also a descriptive term for the characteristic beefy-red appearance seen in the tongue in conjunction with certain nutritional deficiencies Etiology
• Deficiency in vitamin B12, niacin, riboflavin, or pyridoxine • Similar findings may also be seen in patients with sprue or iron-deficiency anemia
Pathogenesis
• Papillae atrophy and the mucous membrane thins o Bright red color occurs due to exposure of the underlying vasculature
Plummer-Vinson Syndrome
• Iron deficiency, angular stomatitis, glossitis and dysphagia • Associated with increased risk of oral squamous cell carcinoma and esophageal cancer
Cold Sores Etiology
• Herpes Simplex Virus 1 (HSV-1) is most common in the oral cavity, but HSV-2 may also cause lesions
Pathogenesis
• Primary infection occurs in 2- to 4-year-old children and is often asymptomatic • HSV-1 localizes to the regional nerves and lies dormant within the local ganglia (ie. trigeminal) • Virus becomes reactivated to produce the common “cold sore” lesion
o Reactivation is usually associated with allergies, upper respiratory infections, UV light exposure, immunosuppression, or intense heat or cold exposure
Clinical Findings
• 10-20% of first infections demonstrate acute herpatic gingivostomatitis with abrupt eruption of vesicles and ulcerations throughout the oral cavity, particularly within the gingival
• Vesicles typically resolve spontaneously in 3-4 weeks • Microscopic examination of vesicular fluid using the Tzanck test may demonstrate epidermal
cells that contain eosinophilic intranuclear viral inclusions, or fusion of several of these cells to produce giant cells

Oral Candidiasis Infection of the mucous membranes of the mouth with Candida albicans Etiology
• Caused by the fungus Candida albicans, normal oral flora in 50% of the population • Factors influencing development of a clinical infection include:
o Immune status o Particular strain of Candida o Overall composition of oral flora
Clinical Findings
• There are three clinical forms of oral candidiasis: o Pseudomembranous (“thrush”) o Erythematous o Hyperplastic
• Thrush, the most common form, represents a superficial, thick, curdy, white to grayish membrane composed of organisms enmeshed within a fibropurulent inflammatory exudate
o The exudate is easily scraped away (in contrast to leukoplakia) o Scraping of the exudate may reveal an erythematous,
inflamed tissue base Hairy Leukoplakia Etiology
• Caused by Epstein-Barr virus, but the lesion is reflective of an underlying systemic condition o 80% of patients have associated HIV infection o Remaining 20% have alternate cause of immunosuppression
Clinical Findings
• White, confluent, hyperkeratotic thickened patches having a feathery, corrugated, or fluffy pattern that predominantly occur on the lateral borders of the tongue
o This lesion cannot be scraped off, unlike the exudate associated with thrush Pathologic Findings
• Histology shows hyperparakeratosis and acanthosis (thickening of the prickle cell layer of the skin) with occasional koilocytosis
Pseudomembranous oral candidiasis (“thrush”)

Leukoplakia A white patch or plaque that can neither be scraped off nor otherwise classified as a specific disease Prevalence
• 3% of the global population has leukoplakia • 5-25% of lesions are premalignant • More common in men than women (2:1)
Etiology
• Precancerous lesion associated with tobacco use Clinical Findings
• Lesions are most commonly found on the buccal mucosa, floor of the mouth, ventral surface of the tongue, palate and gingiva
• Lesions may be solitary or multiple white patches or plaques with either indistinct or sharply-defined borders
o High variability is seen in plaque thickness, smoothness, elevation, ulceration, fissuring and corrugation
• Most lesions are painless Pathologic Findings
• Histology shows hyperkeratosis ranging from an orderly squamous mucosal epithelium to a markedly dysplastic epithelium
Erythroplakia Prevalence
• More common in men than women (2:1) Etiology
• Precancerous lesion associated with tobacco use Clinical Findings
• Red, velvety plaque in the oral cavity o Lesion is occasionally depressed compared to surrounding mucosa o May show erosions
• Lesion may arise on tongue or buccal mucosa (common in women) or on the floor of the mouth (common in men)
Pathologic Findings
• Histology is much more atypical than leukoplakia, so there is higher risk of malignancy • Majority of lesions display evidence of dysplasia or worse

Chondrodermatitis Nodularis Helicis (CNH) Common inflammatory condition of the skin and cartilage caused by minor trauma, sun damage, and prolonged and excessive pressure or cold Prevalence
• Most common in middle-aged to elderly men and fair-skinned people with sun damage
Clinical Findings
• Lesion typically appears as a painful, flesh-colored or erythematous nodule on the prominent projections of the ear (helix or antihelix)
o Nodules range from 2-20mm in size and are firm, tender, round or oval, and have raised edges
o Lesions may contain a central area of crusting or ulceration
o Lesions may become secondarily infected • With repeated injury, chronic inflammation, necrosis of
cartilage, and subsequent fibrosis will occur and may result in significant deformity
Pathologic Findings
• Microscopy often demonstrates epidermal ulceration o The intact epidermis may be edematous and acanthotic o Below the area of ulceration, collagen degeneration of
the dermis is often present, accompanied by a prominent lymphocytic infiltration and some granulation tissue
o The perichondrium often is inflamed Treatment
• Lesions persist if untreated and surgical intervention is frequently required

Neoplasms of the External Ear Keratoses
• Premalignant lesions occurring in the exposed auricular areas • Lesions represent an overgrowth of skin layers resulting from extended sun exposure • Present as an irregular scaly plaque varying from gray to deep brown in color • Usually smaller than one centimeter in diameter • The hyperkeratotic scale may become nodular and project to form a cutaneous horn
Squamous Cell Carcinoma
• A malignant lesion first appearing as a papule that enlarges and ulcerates
o “Infection that fails to resolve” • Well-differentiated lesions seldom metastasize,
whereas poorly-differentiated lesions tend to metastasize widely
• Lesions that extend and involve the bony portion of the external ear canal are difficult to eradicate
Basal Cell Carcinoma
• Most common malignant neoplasm of the external ear • A malignant lesion with a pearly raised border of epithelium surrounding a
“rodent ulceration” which is usually covered with crusty material • May also present as a flesh-colored or pigmented nodule
Melanomas
• Malignant lesions occurring on the exposed portions of the external ear • Prognosis depends on the extent of involvement of the skin and underlying
structures • These are aggressive lesions that metastasize to lymph nodes and distant sites
rapidly

Otitis Externa Inflammation of the external auditory canal Etiology
• Can be bacterial or fungal Pathogenesis
• Caused by an alteration of the host defense mechanisms of the external ear canal, such as an altered immune status in a diabetic patient
• Susceptibility to infections may be caused by disruption of the protective layers of skin, as by trauma from a q-tip
• In swimmers, divers and surfers, chronic cold water exposure can lead to the growth of bony swellings in the canal called exostoses, which may interfere with the drainage of wax and predispose to otitis externa
Clinical Findings
• Pain and thick discharge from the ear Swimmer’s Ear
• A specific localized infection of the external ear canal caused by the trapping of moisture, wax and debris resulting in obstruction, swelling and severe pain
o An alkaline pH lays the environment for infecting organisms such as E. coli and Pseudomonas sp.
• Treatment is by debridement and application of acidic antibiotic drops with steroids to reduce inflammation
Otitis externa caused by Aspergillus
“Swimmer’s ear”

Otitis Media Prevalence
• 90% of children between the ages of one and six have had at least one episode of otitis media • Otitis media is the leading cause of hearing loss in children
Etiology
• Acute otitis media is commonly caused by (in decreasing order of frequency) Streptococus pneumococcus, H. influenzae, other Strep species, B. catarrhalis, and Staphylococcus sp.
Pathogenesis
• Predisposing factors to otitis media include young age, maleness, bottle feeding, heredity and crowded living conditions
• Barotrauma due to sudden changes in atmospheric pressure compared to a relatively low middle ear space may cause the lining of the middle ear cleft to produce a clear, watery exudate
o This is called serous otitis media (SOM) or otitis media with effusion (OME) • Persistent or recurring bouts of acute otitis media can produce mucosal and goblet cell
hyperplasia and increased serous secretions o Over time, an adhesive and gelatinous material accumulates in the middle ear space
(“glue ear”) Clinical Findings
• Acute otitis media produces signs and symptoms of acute infection
• Early in the disease, there is hyperemia, congestion and formation of exudates, with pain and plugging of the ear canal
o As the disease progresses, the middle ear fills with pus
• Chronic otitis media is the result of prolonged infection of the middle ear and can have the following complications:
o Tympanic membrane perforation o Erosion of the ossicles o Mastoiditis o Tympanosclerosis
• Masses of hard, dense connective tissue around the ossicles in the tympanic membrane and submucosal areas of the middle ear
o Cholesteatoma o Conductive or neurosensory hearing loss
Early and late stages of acute otitis media
Chronic otitis media

Cholesteatoma A benign cyst consisting of desquamating layers of scaly or keratinized epithelium from the tympanic membrane, which may also contain cholesterol crystals Etiology
• May be acquired, as a complication of acute or chronic otitis media • May be congenital
Pathogenesis
• The fundamental pathologic mechanism in both acquired and congenital cholesteatoma is accumulation of the desquamated keratin of the tympanic membrane
o In acquired disease, retraction pockets in the pars flaccida and pars tensa of the tympanic membrane enlarge and perforate and the skin of the tympanic membrane grows through the perforation and into the middle ear
o In congenital disease, small remnants of skin become trapped in the middle ear
Clinical Findings
• Ear drainage, sometimes with a foul odor • Complications include facial paralysis, erosion of the ossicles and brain abscess
Pathologic Findings
• Histology shows an advancing edge of squamous epithelium with laminated keratinaceous material resulting from squamous exfoliation
• Acicular clefts formed by the precipitation of cholesterol in the tissues and flecks of calcific material may be seen
Autoimmune Inner Ear Disease A clinical syndrome of probable autoimmune pathogenesis, characterized by rapidly progressive bilateral sensorineural hearing loss Clinical Findings
• Rapidly progressive bilateral sensorineural hearing loss • May observe some vestibular symptoms • Circulating autoantibodies against inner ear antigens are observed in 71% of patients with
bilateral sensorineural hearing loss of unknown etiology Treatment
• Patients with detectable antibodies in their serum may respond to corticosteroid therapy • Cochlear implantation is the most likely outcome of the progressive hearing loss
Acquired cholesteatoma
Congenital cholesteatoma
Cholesteatoma, showing laminated keratinaceous material
Cholesteatoma, showing prominent acicular clefts

Menier Disease (Endolymphatic Hydrops) An inner ear disease of unknown etiology characterized by vertigo and intraaural fullness or pressure Clinical Findings
• Unilateral or bilateral sense of intraaural fullness or pressure • Vertigo, nausea and vomiting that last for hours • Fluctuating low frequency sensorineural hearing loss and tinnitus
Acoustic Neuroma A benign tumor of the cerebellar pontine angle associated with hearing loss Pathogenesis
• Most tumors originate from the Schwann cells surrounding the superior vestibular nerve • Symptoms are caused by the growing tumor compressing the eighth cranial nerve
Clinical Findings
• Unilateral sensorineural hearing loss • Unilateral tinnitus • Trigeminal nerve symptoms

Vestibulitis Inflammation of the slight dilatation just inside the anterior aperture of the nasal cavity Etiology
• Focal infections involving the hair follicles of the vestibule or adjacent tissues may result from nose-picking, drying and fissuring of the nasal tissues from forced air heat in homes, and fumes in certain industrial plants
Pathologic Findings
• Nonspecific acute inflammation with hemorrhage, infiltrate of PMNs, and hyperemic granulation tissue
Complications
• Cavernous sinus thrombosis is the most serious complication o This can occur when a soft tissue infection around the face and
nose involves the veins that drain the area o The infection spreads retrograde into the cavernous sinus, since
these veins do not have valves Septal Hematoma An accumulation of blood within the nasal septum, usually due to trauma Clinical Findings
• Symptoms of obstruction, pressure, dull frontal headache • Patient may have a slight fever • Septal hematoma can cause a septal abscess to form (also can occur
with measles) Treatment
• Septal hematomas must be drained early to avoid destruction of the septal a cartilage o If the hematoma is bilateral, the septal cartilage can die within 24 hours resulting in a
saddle nose deformity Nasal Septal Perforation Etiology
• Trauma, infection, chronic nose-picking or surgery on the septum o Syphillis, tuberculosis, leprosy, diphtheria and Wegener
granulomatosis can all cause nasal septal perforations o Common causes seen clinically include cocaine abuse,
intranasal steroids used for allergies, and collagen vascular disorders (eg. SLE)
Pathogenesis
• Blood flow to the septal cartilage is compromised due to chronic nasal vascular constriction, resulting in cartilage necrosis and perforation
Unilateral left septal hematoma, one week old

Nasopharyngeal Carcinoma Prevalence
• Accounts for 4% of head and neck cancers in the US • More common in China (Hong Kong and Taiwan), possibly due to environmental factors
Etiology
• Carcinoma of the nasopharynx is associated with the Epstein-Barr virus o High levels of antibody to the virus are identified in 70% of US patients
Clinical Findings
• Neck mass (60%) • Aural fullness (41%) • Conductive hearing loss due to middle ear effusion
(37%) • Epistaxis (30%) • Most common site of lesion is just posterior to the
Eustachian tube Pathologic Findings
• Three histologic classes: o Keratinizing squamous cell carcinoma (25%)
Well-differentiated o Non-keratinizing squamous cell carcinoma (12%) o Undifferentiated carcinoma (63%)
Includes lymphoepithelialoma Demonstrates large epithelial cells with round vesicular nuclei, prominent
nucleoli and indistinct cell borders in a syncytium-like display There is a marked infiltrate of mature lymphocytes
Treatment
• Radiation therapy is associated with a 50-70% 3-year survival rate o Undifferentiated variant is most radiosensitive o Keratinizing variant is least radiosensitive
Nasopharyngeal carcinoma, showing predominant non-neoplastic lymphocytic infiltrate and syncitial-like appearance of indistinctly-
demarcated cells in the center

Nasopharyngeal Angiofibroma Benign vascular tumor occurring in the posterior nasal cavity Prevalence
• Seen almost exclusively in adolescent males o Suggests that tumor growth is associated with male sex
hormone stimulation Clinical Findings
• May see recurrent epistaxis or obstruction with persistent rhinorrhea
• Tumor displaces and distorts surrounding soft tissue structures, and may cause pressure necrosis and extension into bone
Pathologic Findings
• Congested polypoid mass microscopically demonstrates proliferation of endothelial-lined blood vessels and myofibroblasts within a fibrous stroma
Sinonasal Papillomas Benign epithelial tumor arising in the nose or paranasal sinuses Etiology
• Squamous papillomas arise from the epithelium of the nasal vestibule • Inverting papillomas (Schneiderian papillomas) arise from respiratory epithelium
o This lesion is associated with human papilloma viruses 6 and 11 Clinical Findings
• Squamous papillomas grow outward (exophytic)
• Inverting papillomas extend downward into the musosa
o Can invade orbit or cranial vault o High rate of recurrence if not
completely excised Infectious Rhinitis “Common cold” Etiology
• Usually caused by adenoviruses, echoviruses, and rhinoviruses Clinical Findings
• Thickened, red, edematous nasal mucosa with narrowed nasal cavities o May have serous or catarrhal discharge o Secondary bacterial infections may occur, producing muropurulent discharge
Gross and microscopic inverted papillomas

Allergic Rhinitis “Hay fever” Prevalence
• 20% of the US population is affected Etiology
• IgE-mediated allergic reaction, usually to plant/animal allergens, fungi or dust mites Clinical Findings
• Early changes include marked nasal mucosa hyperemia, edema and mucus secretion Pathologic Findings
• Late allergic response is characterized by a mixed leukocytic inflammatory infiltration with predominance of eosinophils
Nasal Polyps Chronic edematous projections of nasal or nasal sinus mucosa usually composed of fibroedematous tissue covered with pseudostratified ciliated columnar epithelium Etiology
• Nasal polyps are caused by chronic nasal allergy, with or without superimposed chronic inflammatory edema from infections
• In children, nasal polyps may be seen in patients with cystic fibrosis Clinical Findings
• Nasal obstruction, altered smell, sneezing, and anterior or posterior nasal discharge
• Most nasal polyps originate from the middle meatus, from the anterior or posterior ethmoid region or maxillary sinus cavity
• Epithelium can become ulcerated and bacterially infected • “Allergic polyps” usually occur bilaterally
o Nasal mucus smears show many eosinophils • “Infection polyps” usually occur unilaterally
Pathologic Findings
• Microscopy demonstrates edematous mucosa, loose stroma, and a mixed inflammatory infiltrate with a preponderance of PMNs and eosinophils
Nasal polyp, lined by respiratory epithelium and showing an
edematous stroma with scattered inflammatory cells
Nasal polyp, higher magnification, with predominantly eosinophilic
infiltrate that is seen in a variety of allergic reactions

Sinusitis Etiology
• Acute sinusitis is caused by the impairment of normal sinus drainage and aeration via the normal opening or ostia
o The sinus ostia may be obstructed due to edema from allergy, viral infection, a deviated septum, nasal polyps or tumor
• Commonly follows acute or chronic rhinitis, with normal oral flora as causative agents • Bacterial etiologies include Streptococcus pneumoniae, H. influenzae, Staphylococcus aureus,
Streptococcus pyogenes, and Moraxella catarrhalis o Chronic sinusitis is more likely to involve anaerobic organisms
Pathogenesis
• Ostia blockage causes lack of oxygen in the sinus, stagnation of secretions, ciliary dysfunction, fluid collection and a favorable environment for bacterial overgrowth and a nonspecific inflammatory reaction
Clinical Findings
• Symptoms of an upper respiratory infection, but more severe and protracted • Nasal obstruction, purulent discharge, sinus/facial pain or headache • Pain may be referred to the eyes, ears, teeth or vertex • Complication of sinusitis include mucocele (mucus retention cyst of the sinus), osteomyelitis
(usually in the frontal bone) and CNS infections • Empyema may occur due to blockage of sinus drainage
Treatment
• Chronic sinusitis usually requires endoscopic sinus surgery

Vocal Cord Nodules/Polyps “Singer’s nodules” Etiology
• A reactive lesion, more common in men, occurring in heavy smokers or individuals who place great strain on their vocal cords
Clinical Findings
• Nodules may be unilateral or bilateral • Nodules are typically small sessile or pedunculated lesions located on
the true vocal cords • Lesions frequently cause hoarseness, but do not undergo malignant
transformation Pathologic Findings
• Lesions are covered by squamous epithelium that may become keratotic, hyperplastic, or slightly dysplastic
• Nodule core is composed of myxoid connective tissue with numerous dilated blood vessels and variable degrees of fibrosis
Laryngeal Papilloma Benign squamous cell neoplasm usually located on the true vocal cords Prevalence
• May occur in all ages o Usually occurs as a single lesion in adults o Often occurs as multiple lesions in children (juvenile
laryngeal papillomatosis) Etiology
• Caused by human papilloma virus types 6 and 11 Clinical Findings
• Hoarseness is common • Trauma to lesions on free edge of cords may cause ulceration and
hemoptysis • Lesions are often recurrent, but malignant transformation is rare
Pathologic Findings
• Grossly, the lesions are soft, small (<1 cm), raspberry-like lesions
• Histology shows multiple slender, finger-like projections supported by central fibrovascular cores
o Projections are covered by well-differentiated, stratified squamous epithelium

Laryngeal Carcinoma Prevalence
• Most commonly presents in patients over 40 years old • Males more affected than females (7:1) • 95% of laryngeal carcinomas are squamous cell carcinomas
o Rarely, adenocarcinomas arise from the mucous glands Etiology
• Strongly associated with smoking o Additional risk factors include alcohol use, asbestos
exposure, and irradiation • HPV present in 5% of cases
Clinical Findings
• Persistent hoarseness is a common symptom • More advanced lesions may cause pain, dysphagia and hemoptysis • Lesions may be classified anatomically
o Supraglottic lesions arise in the epiglottis, false cord area, and aryepiglottic folds o Glottic lesions arise within the true vocal cords
Most common lesion Carries low risk of metastasis due to poor lymphatic supply and early
presentation o Subglottic lesions arise below the vocal cords
Pathologic Findings
• Grossly, lesions range from smooth or wrinkled pearly white areas of thickened mucosa (suggestive of noninvasive lesions) to irregular, verrucous and sometimes ulcerating or fungating
• Histologically, most lesions are well-differentiated
Laryngeal squamous cell carcinoma, showing an ulcerative lesion on the left
true vocal cord (glottic lesion)
Laryngeal squamous cell carcinoma, showing nests of cells infiltrating the underlying supportive connective tissue and
keratin pearls (the top left corner shows normal tissue)
Squamous cell carcinoma of the larynx

Thyroglossal Duct Cyst A congenital cyst in the midline connection between the foramen caecum and the thyroid gland Complications
• Congenital carcinomas occasionally arise in thyroglossal duct cysts
o These cancers are characteristic of papillary carcinomas of the thyroid gland
Treatment
• Excision of the cyst, tract, and middle portion of the hyoid bone
Branchial Cleft Cyst/Sinus A congenital defect arising on the lateral part of the neck from a failure of obliteration of the second branchial cleft in embryonic development, which may present as an epithelial cyst or draining sinus Clinical Findings
• Cutaneous openings of the branchial sinuses, if present, are anterior to the sternocleidomastoid muscle
o The tract lies deep to the platysma muscle • Cysts may not present until adulthood
Pathologic Findings
• Branchial cleft cysts are usually lined by stratified squamous epithelium
o Occassionally, ciliated columnar epithelium is present
o Lymphoid tissue with germinal centers forms the outer coat
Treatment
• Excision, which must include the tract Laryngomalacia A congenital abnormality of the laryngeal cartilages, commonly causing airway obstruction Clinical Findings
• Stridor is the primary symptom, and other causes of stridor need to be ruled out
• Deformation is present at birth and will manifest as several weeks of age
• Usually resolves spontaneously within one-and-a-half years
Cutaneous openings of branchial cleft sinuses
External and CT views of a branchial cleft cyst
Normal larynx, mild laryngomalacia and severe laryngomalacia

Acute Supraglottitis (Acute Epiglottitis) A form of acute laryngitis where the inflammatory changes involve the entire supraglottic larynx Prevalence
• Affects children ages 2-7 Etiology
• The etiologic agent is Haemophilis influenzae, type B Clinical Findings
• Rapidly progressive dyspnea that may progress to complete airway destruction
• Swollen, bright red epiglottis o Obstructs the pharynx at the base of the tongue
• Child prefers the upright position with the neck extended • Diagnosis is made in the operating room, where airway
control is necessary Treatment
• Intubation for 24-48 hours • Sedation and muscle relaxation • Intravenous antibiotics
Laryngotracheal Bronchitis (Croup) An acute lower respiratory infection that extends from the larynx to the smaller divisions of the bronchial tree Prevalence
• Usually seen in children 3-5 years old, but may be seen earlier Etiology
• Etiology is viral, usually parainfluenza virus, types 1 through 4 o Bacterial species (Haemophilus, Streptococcus, and
Staphylococcus) are frequently cultured Clinical Findings
• Disease begins like a common cold • Barking cough (like a seal) is characteristic • Mucosal inflammation from subglottic space into the trachea • X-ray of the upper airway shows subglottic tracheal narrowing,
producing an inverted V appearance (steeple sign) Treatment
• May require hospitalization with intravenous steroids, antibiotics, humidification and oxygen therapy
• Intubation may be required
Acute supraglottitis (bottom of image is anterior)

Normal Salivary Gland Microanatomy Parotid Gland
• Largest of the major glands (20g) • Composed primarily of serous cells
(which stain blue) • Adipose tissue is often associated with
the parotid • Pale-staining oval zones are ducts
draining the acini • To the left of the image is a larger duct
containing some mucous cells in its epithelium
Submandibular Gland • Second largest gland (10g) • Composed of mixed cell types, with a
preponderance of serous cells • Serous demilunes are present
o A serous demilune is a crescent-shaped cluster of serous cells enveloping the more centrally placed mucous cells in an acinus
Sublingual Gland • Composed primarily of mucous cells
(which stain pink) o Accessory salivary glands are
similarly composed o Mucous cells are typically
columnar with basally located nuclei and pale vacuolated cytoplasm on the apical side of the cell due to loss of contents from their secretory granules
• Serous demilunes are present

Sialadenitis Inflammation of a salivary gland Mucocele
• Most common inflammatory salivary gland lesion • Caused by blockage or rupture of the salivary gland
duct with subsequent leakage of saliva into the surrounding connective tissues
• Most occur in lower lip, secondary to trauma • Present as swellings with blue discoloration
o Lesion size may fluctuate in association with meals • Histology shows cyst-like spaces filled with mucin and inflammatory cells
o Spaces may be lined by granulation tissue or fibrous connective tissue • Complete resection of cyst and associated gland is required
Mumps
• The most common viral infection of the salivary glands • Caused by a paramyxovirus • Edema and inflammation of ductal epithelial cells causes pain and
swelling • Parotid gland is most commonly affected • Also affects testes, pancreas and kidneys • Common cause of sensorineural hearing loss in children and adults
Suppurative Parotitis
• Most commonly caused by Staphylococcal infection • Especially common in dehydrated and debilitated hosts • Commonly affects major salivary glands, especially submandibular • Can be induced by ductal obstruction due to stones • Suppurative sialadenitis can lead to dangerous soft tissue infections of the
head and neck Salivary Gland Calculi
• 70-80% are found in the submandibular gland or duct (due to gravity) o 20-39% are found in the parotid or sublingual glands or ducts
• 65-75% contain enough calcium phosphate and carbonate to be radiopaque
o Parotid gland stones are mostly translucent • Stone formation may be related to ductal obstruction by
food debris or ductal orifice edema secondary to trauma • With calculi, restriction of flow leads to stasis of saliva
o Stasis results in trapped bacteria o Local infection develops o Local infection can progress to chronic state

Neoplasms of the Salivary Gland 75% of salivary gland neoplasms are benign Pleomorphic Adenoma (85% of benign neoplasms)
• A benign mixed tumor o Believed to be derived from a mixture of ductal and
myoepithelial cells • Comprises 60% of parotid tumors and is less common in
submandibular glands • Radiation exposure is known to increase risk • Presents as a painless, slow-growing, mobile, discrete mass • Grossly, tumors are rounded, well-demarcated masses usually less
than 6 cm in diameter with incomplete encapsulation and a gray-white cut surface demonstrating myxoid areas
• Histologically, epithelial (ductal) and myoepithelial elements appear arranged in cords
o Acini and sheets are dispersed throughout a background of myxoid stroma containing cartilaginous areas
o Dysplasia and mitotic activity are not usually seen
• Recurrence is low with adequate parotidectomy • Malignant transformation (carcinoma ex pleomorphic adenoma) increases with duration of
tumor Warthin’s Tumor (Papillary Cystadenoma Lymphomatosum) (10% of benign neoplasms)
• Almost exclusively arises in parotid gland • More common in males • Typical age of patient is 50-70 years • 10% are multifocal • 10% are bilateral • Eight times higher risk in smokers • Grossly, tumors are encapsulated, 2-5 cm oval
masses with pale gray cut surface punctuated by narrow cystic or cleft-like spaces filled with mucinous or serous secretions
• Histology reveals cystic spaces lined by a uniform double-layered epithelial lining composed of large cells (oncocytes) with abundant granular cytoplasm due to numerous mitochondria
o Epithelial cells are very eosinophilic and frequently thrown into papillary folds
o Epithelial cells rest on a dense lymphocytic stroma that may contain germinal centers

Mucoepidermoid Carcinoma (33% of malignancies) • Most commonly seen in the parotid gland • Grossly, tumors may grow up to 8cm
o Tumors appear circumscribed, but lack well-defined capsules and may show marginal infiltration
o Cut surface is gray-white with small, mucin-containing cysts • Histology shows cords, sheets, and cysts of squamous, mucous or intermediate cells with a
wide range of dysplasia Adenoid Cystic Carcinoma (25% of malignancies)
• 50% arise in minor salivary glands • Grossly, tumors are small, poorly-encapsulated, infiltrative, gray-pink lesions with a bluish hue • Histology shows small cells with dark, compact nuclei and scant cytoplasm
o Cells are arranged in tubules, solid sheets, or cribiform (“cookie cutter”) patterns
• Tumor commonly shows perineural invasion, leading to high recurrence
• 50% metastasize to bone, liver or brain, often years after excision
• Tumors from minor salivary glands have a worse prognosis than parotid tumors
Benign Vascular Neoplasms Hemangiomas
• Congenital hamartomas that are mesodermal nests of vasoformative tissue • May be capillary, cavernous or mixed • Present at birth or within first year of life • Bluish mass increases in size with straining or crying • Many regress spontaneously, especially the cavernous form • Strawberry hemangiomas are raised above the surrounding skin and
blanch with pressure o Account for 90% of infant hemangiomas
• Steroid therapy is the first line of treatment o Surgery is delayed as long as possible
• Hemangiomas are a common salivary gland tumor in children •
Lymphangiomas (Cystic Hygromas)
• 80% involve the neck • Present at birth or within first six months of life • Surgical excision sparing vital structures is the mainstay of treatment • Spontaneous regression is extremely rare

Neoplasms of the Oral Cavity Locations
• Carcinoma of the lip accounts for 25-30% of oral carcinoma o 95% of these involve the lower lip
• The oral tongue (anterior two-thirds) accounts for 20% of oral carcinomas o Many tongue cancers present with occult bilateral lymph node metastases and can be
quite invasive Squamous Cell Carcinoma
• Squamous cell carcinoma of the lips, tongue or other oral mucous membranes is usually related to tobacco and alcohol use
o 50% of cases are associated with human papilloma virus • Squamous cell carcinoma is the most common cancer of the lower
lip o In the case of lip cancer, sun exposure plays a role
• Tumor usually presents on the ventral surface of the tongue, floor of the mouth, lower lip, soft palate or gingival
o Tumor is often preceded by a premalignant lesion • Early lesions are typically raised, firm, pearly plaques or rough,
irregular mucosal thickenings o Lesions eventually enlarge and ulcerate o The mass may have an irregular, firm, and indurated
border • Histology shows dysplasia with or without full epithelial thickness
dysplasia before invasion o Degree of differentiation and keratinization are not related
to prognosis • Tumors invade locally before they metastasize
o Local metastases usually involve cervical lymph nodes o Distant metastases often involve mediastinum, lungs, liver
or bones Basal Cell Carcinoma
• Basal cell carcinoma is the most common cancer of the upper lip • Basal cell carcinomas tend to grow in rather than out • Histology shows nests of malignant cells with palisading nuclei
Squamous cell carcinoma of the lower lip
Squamous cell carcinoma with a keratin pearl (arrow)
Low (left) and high (right) power views of basal cell carcinoma, showing nests of malignant cells with palisading nuclei (“picket fence” pattern)