Guide to CGD | CGD Pathways · PDF fileANC 4,235 Cell/μL 1,700-7,000* 5,987 ... FORM SAMPLE...
8
CHRONIC GRANULOMATOUS DISEASE ( CGD ) Clinical Manifestations, Testing, and Management
Transcript of Guide to CGD | CGD Pathways · PDF fileANC 4,235 Cell/μL 1,700-7,000* 5,987 ... FORM SAMPLE...

CHRONICGRANULOMATOUSDISEASE (CGD)
Clinical Manifestations, Testing, and Management

Chronic granulomatous disease (CGD) is a primary immunodeficiency disorder of phagocytes that results from impaired killing of fungi and bacteria, which can lead to severe and recurrent infections. CGD may become apparent at any time from infancy to late adulthood; however, most affected individuals are diagnosed before age 5 years.1 Approximately 1 out of every 200,000 people in the United States has CGD.2
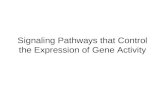
Most frequent sites of infection, common infectious complications, and common inflammatory complications1
Lung(pneumonia)
Stomach(gastrointestinal granulomas)
Colon(colitis)
Urinary tract(genitourinary granulomas)
Lymph nodes(lymphadenitis)
Liver(abscess)
Bone(osteomyelitis)
Skin(abscess or cellulitis)
RECOGNIZING THE SIGNS AND SYMPTOMS CAN LEAD TO DIAGNOSIS
SUSPECT CGD IN A PATIENT WITH:FREQUENT, REPEAT
INFECTIONSUNUSUALLY SEVERE
INFECTIONS
INFECTIONS FROM A SPECIFIC GROUP OF
PATHOGENS

Aspergillus speciesCOMMON PRESENTATIONPneumonia, lymphadenitis, osteomyelitis, brain abscess
Nocardia speciesCOMMON PRESENTATIONPneumonia, osteomyelitis, brain abscess
Serratia marcescensCOMMON PRESENTATIONMore common: osteomyelitis, soft tissue infections Less common: pneumonia, sepsis
Burkholderia (pseudomonas) cepacia complexCOMMON PRESENTATIONPneumonia, sepsis
Candida speciesCOMMON PRESENTATIONSepsis, soft tissue infection, liver abscess
Klebsiella speciesCOMMON PRESENTATIONPneumonia, skin infections, lymphadenitis
Staphylococcus aureusCOMMON PRESENTATIONSoft tissue infections, lymphadenitis, liver abscess, perirectal abscess, osteomyelitis, pneumonia, sepsis
Patients with primary immunodeficiencies present frequently with chronic and/or recurrent infections caused by a broad array of pathogens, and do so early in life. Most severe infections in patients with CGD in North America are caused by a select group of organisms, both bacterial and fungal.1,3-8
Most frequent pathogens and common presentations associated with CGD*
LOOK FOR THE PATHOGENS THAT MAY INDICATE CGD
FUNGAL
BACTERIAL
*This is not a complete list of pathogens. Infections may also be caused by other species of bacteria and fungi not listed here.

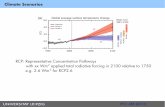
Examples of pre- and postactivation DHR histograms
M1
M1
THE DHR TEST IS THE PREFERRED TEST FOR CGD
X-linked female CGD carriers have 2 populations of cells: cells that respond to the stimulus and cells that don’t. X-linked carriers commonly exhibit discoid lupus, photosensitivity rashes, and aphthous ulcers. Diagnosis of an X-linked CGD carrier can help confirm an X-linked diagnosis in her son.
M2
M1
M1
250
200
150
100
50
0
Cel
l cou
nt
MFI PMA ox-DHR
100 104101 102
Before
103
TYPICAL X-LINKED CGD CARRIERb
100 104101 102 103
After PMA stimulationa
M1M1
In a normal individual, neutrophils respond to the stimulus, meaning the cells are functioning.
250
200
150
100
50
0
Cel
l cou
nt
MFI PMA ox-DHR
100 104101 102
Before
103
NORMAL
100 104101 102 103
After PMA stimulationa
M1
M1
An autosomal recessive patient with CGD demonstrates a reduced response to the stimulus. Both males and females can present with autosomal recessive CGD.
250
200
150
100
50
0
Cel
l cou
nt
MFI PMA ox-DHR
100 104101 102
Before
103
AUTOSOMAL RECESSIVE PATIENT WITH CGD
100 104101 102 103
After PMA stimulationa
In an X-linked patient with CGD, cells do not respond to the stimulus, meaning they are not functioning as they should. If they do not respond to the stimulus, then they also don’t respond to specific bacteria and fungi, suggesting an immune deficiency.
250
200
150
100
50
0
Cel
l cou
nt
MFI PMA ox-DHR
100 104101 102
Before
103
X-LINKED PATIENT WITH CGD
100 104101 102 103
After PMA stimulationa
Abbreviations: MFI, mean fluorescence intensity; PMA, phorbol myristate acetate. Adapted from Leiding et al (2013)7 and Jirapongsananuruk et al.11
aPMA is an activator used to stimulate neutrophil NADPH oxidase activity. bUsually a female with a healthy and a mutated allele for gp91phox.
*The DHR test is also referred to as the neutrophil oxidative burst (NOXB1) assay for assessing neutrophil superoxide production.10
Historically, the nitroblue tetrazolium (NBT) test has been the recognized diagnostic test for CGD. Relying on light microscopy, the NBT test provides only a qualitative determination of phagocyte nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activity. The NBT test is also open to operator subjectivity and can produce false-negative results.
The dihydrorhodamine (DHR) test* is the preferred method for diagnosing CGD because it produces fewer false-negative test results than the NBT method. The DHR test is known for its1,9:
• Relative ease of use
• Objectivity without requiring significant operator experience
• Ability to distinguish between X-linked and autosomal recessive forms of CGD
• Ability to detect gp91phox carriers
• High sensitivity
• Ability to quantitatively assess residual superoxide production

Sample reportsX-linked CGD patient
VARIABLE VALUE (PATIENT) UNIT NORMAL CUTOFF VALUE (UNRELATED HEALTHY DONOR)
ANC 4,235 Cell/μL 1,700-7,000* 5,987% PMA ox-DHR+ 4.1 % ≥ 95% 100.0MFI PMA ox-DHR+ 6.73 MFI ≥ 60 78.25
300
250
200
150
100
50
0
Cel
l cou
nt
DHR @ FITC-A
101 102100
Before stimulation
103 104 101 102100 103 104
300
250
200
150
100
50
0
Cel
l cou
nt
DHR @ FITC-A
After PMA stimulation
Results: Result is consistent with associated X-linked CGD in a male patient.
Abbreviations: ANC, absolute neutrophil count; FITC, fluorescein isothiocyanate; MFI, mean fluorescence intensity; PMA, phorbol myristate acetate.
Autosomal recessive CGD patient
Before stimulation300
250
200
150
100
50
0
Cel
l cou
nt
DHR @ FITC-A
101 102100 103 104
After PMA stimulation
101 102100 103 104
300
250
200
150
100
50
0
Cel
l cou
nt
DHR @ FITC-A
Results: Result is consistent with associated autosomal recessive CGD in a female patient.
Abbreviations: ANC, absolute neutrophil count; FITC, fluorescein isothiocyanate; MFI, mean fluorescence intensity; PMA, phorbol myristate acetate.
VARIABLE VALUE (PATIENT) UNIT NORMAL CUTOFF VALUE (UNRELATED HEALTHY DONOR)
ANC 2,743 Cell/μL 1,700-7,000* 5,987% PMA ox-DHR+ 53.8 % ≥ 95% 100.0MFI PMA ox-DHR+ 31.34 MFI ≥ 60 78.25
*The appropriate age-related reference values for absolute neutrophil count will be provided on the report.
These values are representations of possible DHR outcomes. Because of heterogeneity in disease severity and genotype, outcomes will vary.

IF YOU HAVE A PATIENT YOU SUSPECT MAY HAVE CGD, REQUEST A DHR TEST KIT
The DHR Test Kit includes:
To help ensure appropriate patients are diagnosed, Horizon Pharma is sponsoring the DHR Test Kit. The test kit is:
• Easy to use: It includes labeling and shipping materials for the sample
• Easy to process: Comprehensive test results will be sent via fax, including a link to an enhanced report and histogram
LABORATORY REQUISITION
FORM
SAMPLE VIALS AND LABELS
SHIPPING MATERIALS
To get a DHR Test Kit, visit CGDPathways.comFor for more information, contact your Horizon clinical science associate or call the Horizon Patient Services line at 1 (877) 305-7704 between the hours of 8 am EST and 6 pm EST.

For the chronic medical management of CGD, the American Academy of Allergy, Asthma & Immunology, the American College of Allergy, Asthma & Immunology, and the Immune Deficiency Foundation recommend interferon gamma-1b in combination with prophylactic antimicrobials. For the treatment of active infections, they recommend using appropriate antimicrobials based on pathogen likelihood or identification.3,7
Recommended chronic treatment paradigm12,13
COMBINATION IMMUNOMODULATORY AND ANITMICROBIAL PROPHYLAXIS THERAPY*
*This does not include all options for managing CGD.
Adapted from Gallin et al.12
Interferon gamma-1b
IMMUNOMODULATORY THERAPY
Eg, trimethoprim/ sulfamethoxazole
ANTIBIOTIC THERAPY
Eg, itraconazole
ANTIFUNGAL THERAPY

©HZNP USA Inc. All rights reserved. August 2017 DA-UNBR-00356-02
TEST AND DIAGNOSETest patients presenting with unusual infections in unusual places to help diagnose a possible immune deficiency, including CGD.
1
ADVOCATE COMBINATION THERAPYReinforce to your CGD patients the importance of adherence to prescribed medications to reduce the frequency and severity of serious infections.
2
*These steps do not include all the options for managing CGD.
COUNSEL CAUTIONEducate patients about making careful lifestyle choices to avoid activities and areas with bacteria, fungi, or yeasts that could put them at risk for serious infection. Encourage patients to schedule routine checkups to facilitate early intervention when necessary.
3
STEPSFOR HELPING YOUR PATIENTSLIVING WITH CGD*,1 3
References: 1. Leiding JW, Holland SM. Chronic granulomatous disease. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews. Seattle, WA: University of Washington, Seattle;1993-2016. 2. Winkelstein JA, Marino MC, Johnston RB, et al. Chronic granulomatous disease: report on a national registry of 368 patients. Medicine (Baltimore). 2000;79(3):155-169. 3. Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015;136(5):1186-1205.e1-e78. 4. Marciano BE, Spalding C, Fitzgerald A, et al. Common severe infections in chronic granulomatous disease. Clin Infect Dis. 2015;60(8):1176-1183. 5. Bortoletto P, Lyman K, Camacho A, Fricchione M, Khanolkar A, Katz BZ. Chronic granulomatous disease: a large, single-center US experience. Pediatr Infect Dis J. 2015;34(10):1110-1114. 6. van den Berg JM, Van Koppen E, Ahlin A, et al. Chronic granulomatous disease: the European experience. PLoS ONE. 2009;4(4):e5234. 7. Leiding JW, Malech HL, Holland SM. Chronic granulomatous disease. Clinical Focus on Primary Immunodeficiencies. 2013;15:1-9. 8. Song E, Jaishankar GB, Saleh H, Jithpratuck W, Sahni R, Krishnaswamy G. Chronic granulomatous disease: a review of the infectious and inflammatory complications. Clin Mol Allergy. 2011;9(1):10. 9. Kuhns DB, Alvord WG, Heller T, et al. Residual NADPH oxidase and survival in chronic granulomatous disease. N Engl J Med. 2010;363(27):2600-2610. 10. Test ID: NOXB. Mayo Medical Laboratories website. http://www.mayomedicallaboratories.com/test-notifications/attachment.php?id=35440. Published October 8, 2014. Accessed March 4, 2014. 11. Jirapongsananuruk O, Malech HL, Kuhns DB, et al. Diagnostic paradigm for evaluation of male patients with chronic granulomatous disease, based on the dihydrorhodamine 123 assay. J Allergy Clin Immunol. 2003;111(2):374-379. 12. Gallin JI, Alling DW, Malech HL, et al. Itraconazole to prevent fungal infections in chronic granulomatous disease. N Engl J Med. 2003;348(24):2416-2422. 13. Holland SM. Chronic granulomatous disease. Hematol Oncol Clin North Am. 2013;27(1):89-99.