Gene Therapy of Collagen-Induced Arthritis by Electrotransfer of Human Tumor Necrosis Factor- ...
13
HUMAN GENE THERAPY 15:189–201 (February 2004) © Mary Ann Liebert, Inc. Gene Therapy of Collagen-Induced Arthritis by Electrotransfer of Human Tumor Necrosis Factor-a Soluble Receptor I Variants CAROLE BLOQUEL, 1,2, * NATACHA BESSIS, 1, * MARIE-CHRISTOPHE BOISSIER, 1 DANIEL SCHERMAN, 2 and PASCAL BIGEY 2 ABSTRACT Electrotransfer is a simple and efficient strategy of nonviral gene delivery. We have used this method to de- liver plasmids encoding three human tumor necrosis factor-a soluble receptor I variants (hTNFR-Is) a monomeric hTNFR-Is, a chimeric hTNFR-Is/mIgG1, and a dimeric (hTNFR-Is) 2 form. Electrotransfer pa- rameters were studied and because anti-TNF strategies have proven efficient for the treatment of rheumatoid arthritis in clinics, we used a collagen-induced arthritis (CIA) mouse model to assess the efficacy of our con- structs in the treatment of the disease. All proteins were proven bioactive, both in vitro and ex vivo. Plasmid intramuscular electrotransfer in mice resulted in a local expression of the three variants for at least 6 months; systemic expression lasted also more than 6 months for the hTNFR-Is/mIgG1 form, while it was shorter for the two other forms. This expression was plasmid dose-dependent. Electrotransfer of 50 mg of hTNFR- Is/mIgG1 at the onset of a CIA induced a clear-cut decrease in both clinical and histologic signs of the dis- ease; the dimeric form also showed some efficacy. Moreover, the long-lasting protective effect was observed for more than 5 weeks. Comparison of this electrotransfer approach with repeated recombinant protein (etan- ercept) injections highlighted the potential practical interest of gene therapy approach for CIA, which leads to sustained therapeutic effect after single treatment. These results show that electrotransfer may be a useful method to deliver cytokine or anticytokine therapy in rheumatoid arthritis and also illustrate the potential- ity of plasmid intramuscular electrotransfer for the rapid screening and assessment of different variant forms of secreted proteins. 189 OVERVIEW SUMMARY We used in vivo electrotransfer, a powerful method of non- viral gene therapy, to deliver plasmids encoding three hu- man tumor necrosis factor- a soluble receptor I variants (hTNFR-Is): a monomeric hTNFR-Is, a chimeric hTNFR- Is/mIgG1, and a dimeric (hTNFR-Is) 2 form. We show that all three proteins are secreted in a bioactive form. Plasmid intramuscular electrotransfer in mice resulted in a local (at least 6 months for all variants) and systemic (at least 6 months for the hTNFR-Is/mIgG1 form, and shorter time for the two other forms) production of proteins. This ex- pression was plasmid dose-dependent. Electrotransfer of 50 mg of hTNFR-Is/mIgG1 at the onset of collagen-induced arthritis (CIA) in mice was clinically and histologically highly effective; the dimeric form also showed some effi- cacy. Comparison of this electrotransfer approach with re- peated recombinant protein (etanercept) injections high- lighted the potential practical interest of gene therapy approach for CIA. 1 UPRES EA-3408 and Service de Rhumatologie, UFR Léonard de Vinci, Université Paris 13 and Hopital Avicenne (AP-HP), 93017 Bobigny Cedex, France. 2 Laboratoire de Pharmacologie Chimique et Génétique, U266 INSERM FRE 2463 CNRS, Faculté de Pharmacie Paris 5/ENSCP, 75270 Paris, France. *Both of these authors contributed equally to this work.
Transcript of Gene Therapy of Collagen-Induced Arthritis by Electrotransfer of Human Tumor Necrosis Factor- ...

HUMAN GENE THERAPY 15:189–201 (February 2004)© Mary Ann Liebert, Inc.
Gene Therapy of Collagen-Induced Arthritis by Electrotransfer of Human Tumor Necrosis
Factor-a Soluble Receptor I Variants
CAROLE BLOQUEL,1,2,* NATACHA BESSIS,1,* MARIE-CHRISTOPHE BOISSIER,1
DANIEL SCHERMAN,2 and PASCAL BIGEY2
ABSTRACT
Electrotransfer is a simple and efficient strategy of nonviral gene delivery. We have used this method to de-liver plasmids encoding three human tumor necrosis factor-a soluble receptor I variants (hTNFR-Is) amonomeric hTNFR-Is, a chimeric hTNFR-Is/mIgG1, and a dimeric (hTNFR-Is)2 form. Electrotransfer pa-rameters were studied and because anti-TNF strategies have proven efficient for the treatment of rheumatoidarthritis in clinics, we used a collagen-induced arthritis (CIA) mouse model to assess the efficacy of our con-structs in the treatment of the disease. All proteins were proven bioactive, both in vitro and ex vivo. Plasmidintramuscular electrotransfer in mice resulted in a local expression of the three variants for at least 6 months;systemic expression lasted also more than 6 months for the hTNFR-Is/mIgG1 form, while it was shorter forthe two other forms. This expression was plasmid dose-dependent. Electrotransfer of 50 mg of hTNFR-Is/mIgG1 at the onset of a CIA induced a clear-cut decrease in both clinical and histologic signs of the dis-ease; the dimeric form also showed some efficacy. Moreover, the long-lasting protective effect was observedfor more than 5 weeks. Comparison of this electrotransfer approach with repeated recombinant protein (etan-ercept) injections highlighted the potential practical interest of gene therapy approach for CIA, which leadsto sustained therapeutic effect after single treatment. These results show that electrotransfer may be a usefulmethod to deliver cytokine or anticytokine therapy in rheumatoid arthritis and also illustrate the potential-ity of plasmid intramuscular electrotransfer for the rapid screening and assessment of different variant formsof secreted proteins.
189
OVERVIEW SUMMARY
We used in vivo electrotransfer, a powerful method of non-viral gene therapy, to deliver plasmids encoding three hu-man tumor necrosis factor-a soluble receptor I variants(hTNFR-Is): a monomeric hTNFR-Is, a chimeric hTNFR-Is/mIgG1, and a dimeric (hTNFR-Is)2 form. We show thatall three proteins are secreted in a bioactive form. Plasmidintramuscular electrotransfer in mice resulted in a local (atleast 6 months for all variants) and systemic (at least 6
months for the hTNFR-Is/mIgG1 form, and shorter timefor the two other forms) production of proteins. This ex-pression was plasmid dose-dependent. Electrotransfer of 50mg of hTNFR-Is/mIgG1 at the onset of collagen-inducedarthritis (CIA) in mice was clinically and histologicallyhighly effective; the dimeric form also showed some effi-cacy. Comparison of this electrotransfer approach with re-peated recombinant protein (etanercept) injections high-lighted the potential practical interest of gene therapyapproach for CIA.
1UPRES EA-3408 and Service de Rhumatologie, UFR Léonard de Vinci, Université Paris 13 and Hopital Avicenne (AP-HP), 93017 BobignyCedex, France.
2Laboratoire de Pharmacologie Chimique et Génétique, U266 INSERM FRE 2463 CNRS, Faculté de Pharmacie Paris 5/ENSCP, 75270 Paris,France.
*Both of these authors contributed equally to this work.

INTRODUCTION
PLASMID ELECTROTRANSFER is a recently introduced physicaltechnique for in vivo nonviral gene delivery. Optimized
electric pulses have been applied to various tissues, such as tu-mors and skeletal muscle, leading to high-level gene transfer(Aihara et al., 1998; Mir et al., 1998; Rols et al., 1998; Math-iesen, 1999; Mir et al., 1999; Bettan et al., 2000; Tamura et al.,2001). Electrotransfer improves transfection efficiency and du-ration of transgenic protein expression. In particular, the ad-vantage of using electrotransferred skeletal muscle as an endo-crine tissue for therapeutic proteins plasmatic secretion has beenlargely illustrated (Tripathy et al., 1996; Kon et al., 1999; Kreisset al., 1999; Bettan et al., 2000; Maruyama et al., 2000; Hannaet al., 2001; Kishida et al., 2001; Maruyama et al., 2001;Nakano et al., 2001; Payen et al., 2001; Vilquin et al., 2001;Saidenberg-Kermanac’h et al., 2003). Electrotransfer leads toalmost stable blood levels, for more than a year (Bettan et al.,2000), and therapeutic effects in a model of b-thalassemia andof rheumatoid arthritis have been reported (Payen et al., 2001;Saidenberg-Kermanac’h et al., 2003).
Rheumatoid arthritis (RA) is a chronic disabling diseasecharacterized by joint inflammation, synovitis, destruction ofcartilage and bone, and ultimately loss of joint function (Har-ris, 1990). Although RA etiology is not fully understood, pro-gresses in deciphering RA pathogenic mechanism have high-lighted that tumor necrosis factor (TNF)-a is critically involved(Feldmann et al., 1996) and elevated levels of TNF-a were de-tected in the serum of patients with RA (al-Janadi et al., 1993;Klimiuk et al., 2001). TNF-a acts by binding to membrane-bound receptors TNFR-I (p55; 55 kd) or TNFR-II (p75; 75 kd).The naturally occurring soluble forms of these two receptorsblock TNF-a proinflammatory activity by trapping the cytokinebut are highly unstable. Recombinant proteins, in which TNF-a soluble receptors are stabilized by an immunoglobulin frag-ment, have proven efficient both in animal models of arthritis(Williams et al., 1992; Wooley et al., 1993; Mori et al., 1996;Joosten et al., 1999), and in clinical studies (Moreland et al.,1997; Weinblatt et al., 1999). TNFR-IIs/Fc-immunoglobulindomain fusion protein (etanercept) is currently used in clinics(Bathon et al., 2000) as well as monoclonal antibodies againstTNF-a (infliximab and adalimumab) (Maini et al., 1999; Lip-sky et al., 2000; Weinblatt et al., 2003). However, these re-combinant proteins are expensive to produce, require repetitiveinjections, and lead to high systemic levels of TNF-a neutral-izing activity on parenteral delivery, which may result in un-desirable effects by excessive inhibition of the TNF-a physio-logic functions. In addition, antibodies against infliximab havebeen detected in patients (Baert et al., 2003).
Gene therapy appears to be an alternative to overcome prob-lems linked to recombinant protein therapy (Evans et al., 1999;Bessis et al., 2002b). Currently, only one phase 2 clinical trialis being considered with retroviral delivery of human IL-1Ra.Gene therapy strategies have been investigated in various mousemodels of RA such as collagen-induced arthritis (CIA), spon-taneous arthritis transgenic mice, in a rat model of streptococ-cal cell wall-induced arthritis (SCW), and in a rabbit model ofantigen-induced arthritis (Le et al., 1997; Ghivizzani et al.,1998; Quattrocchi et al., 1999; Cottard et al., 2000; Kim et al.,2000, 2002; Zhang et al., 2000; Chan et al., 2002). Consider-
ing the clinical efficacy of TNF-a blockade and the advantagesof nonviral gene therapy, we considered the feasibility and ef-ficiency of anti-TNF-a gene delivery by electrotransfer.
In the present report, we investigated three different formsof the TNFR-Is: the chimeric form of the protein (hTNFR-Is/mIgG1), which has proven efficiency as a recombinant pro-tein but has never been tested by electrotransfer; the physio-logic form of the type I TNFRs (monomeric form), which isknown to be highly unstable but could nevertheless have someefficiency when produced by an electrotransferred muscle; anda more original form made by association of two TNFR-Islinked by a polyglycine polylinker, which we hoped could bemore easily produced by the muscle because it is smaller andkeeps a good affinity for the TNF-a trimer compared to themonomeric form because of its two subunits. We decided touse the type I TNF-a soluble receptor for its higher affinity to-ward TNF-a, leading to a nearly irreversible binding (Grell etal., 1998), thus avoiding a prolonged TNF-a plasma appear-ance and action as a ligand passer (Evans et al., 1994; Frish-man et al., 2000). The aim of the study was to compare the ca-pacity of skeletal muscle to secrete proteins of various sizes,bearing the same functional moiety present either at a ratio ofone receptor unit per molecule (monomer) or two (dimeric andchimeric forms of the TNF-a soluble receptor). We also as-sessed the steady-state plasmatic level obtained, taking into ac-count differences in transgenic protein secretion rate and in kid-ney clearance. The three different plasmid-encoded proteinswere then compared after intramuscular electrotransfer for theirefficiency to block TNF-a effect and for the treatment of CIAin mice.
MATERIALS AND METHODS
Plasmids
Human type I soluble TNF receptor cDNA (hTNFR-Is), wasobtained from HeLa cells (Peppel et al., 1991), and subclonedinto a pCOR expression plasmid (Soubrier et al., 1999) to yieldpCORhTNFR-Is. To construct the chimeric pCOR hTNFR-Is/mIgG1, the cDNA of the murine immunoglobulin G1 (IgG1)heavy chain was cloned as follows. Mice were stimulated byan intraperitoneal injection of ovalbumin (100 mg) emulsifiedin 60 ml of Freund’s incomplete adjuvant and were boosted atday 7 with the same emulsion. Spleens were removed at day12, and leucocytes were recovered in RPMI medium using acellular sieve. Extracted cells were then placed in ACK bufferfor erythrocyte lysis. After RPMI addition to stop lysis and twowashes, leukocytes total RNA was extracted. The mIgG1 con-stant fragment was amplified by reverse transcription (RT-PCR)with IgG59-Thr primer (59-ctggttccgcgtggatccGTGCCCAG-GGATTGTGGT) and IgG39 primer (59-actggctcgagTCATT-TACCAGGAGAGTG ), and was subcloned into the pCR2.1 plas-mid (Invitrogen, Carlsbad, CA). The chimeric hTNFR-Is/mIgG1 cDNA was then obtained as described (Peppel et al.,1991), subcloned in a pCR2.1 plasmid, and finally inserted intoa pCOR plasmid after KpnI and XhoI digestion, and ligation,giving the pCOR hTNFR-Is/mIgG1 plasmid, whose sequencewas controlled. To construct the dimeric pCOR (hTNFR-Is)2,the 59-terminal and the 39-terminal domain of the human TNFR-
BLOQUEL ET AL.190

Is dimer encoding construct were amplified by polymerasechain reaction (PCR) from the PCR2.1 hTNFR-Is-Thr plasmid,respectively, with primer TNFR59 (agcattctagaTCTGGC-ATGGGCCTCTCCACC) and with primer TNFR39-PG (actac-caccacctccggaaccaccaccaccTGTGGTGCCTGAGTC), and withTNFR39 (59-actggctcgagctaTGTGGTGCCTGAGTCCTC) andTNFR59-PG (ggtggtggtggttccggaggtggtggtagtTCTGGCATG-GGCCTC) primers. The two amplified fragments were insertedin pCR2.1 to give pCR2.1 hTNR-Is39-PG and pCR2.1 hTNR-Is59-PG, respectively. A BspEI-NotI fragment of PCR2.1 hT-NFR-Is39-PG was ligated into pCR2.1 hTNR-Is59-PG digestedby the same enzymes, giving pCR2.1 (hTNFR-Is)2 plasmid. Fi-nally, a KpnI-XhoI fragment from pCR2.1 (hTNFR-Is)2 wassubcloned into a KpnI-XhoI–digested pCOR, giving the pCOR(hTNFR-Is)2 plasmid.
hTNFR-Is ELISA in cell culture supernatant, musclelysates, or serum
Briefly, muscles were removed from the hind limbs, crushed,and resuspended in 400 ml of lysis buffer (Tris 0.25 mM, pH 58). After 1 min vortex, the resulting tissue suspensions werefreeze/thawed five times, and lysates were cleared by two 10-min centrifugation at 12,000g. Supernatants were stored at220°C until assayed. The total amount of protein was deter-mined by lysate absorbance at 280 nm. hTNFR-Is concentra-tion in muscles was expressed as picograms of hTNFR-Is permilligram of protein. The blood was collected by cardiac punc-ture, serum was separated by centrifugation for 10 min at 3000rpm and 4°C, and stored at 280°C until assayed. hTNFR-Iswas measured in the samples using a commercially availableenzyme-liked immunosorbent assay (ELISA) kit for humanTNFR-Is (Duoset, R&D Systems, Abingdon, UK). Results wereexpressed as equivalent of monomeric recombinant hTNFR-Is,as mean 6 standard error of the mean (SEM).
Assays of TNF inhibitory activity
Inhibition of TNF-a cytotoxicity by hTNFR-Is on the murinecell line L929 was assessed. L929 cells were grown in RPMI1640 with glutamax 1 supplemented with 7% fetal calf serum(FCS) and 1% penicillin-streptomycin (Kolls et al., 1994; Quat-trocchi et al., 1999); 4 3 104 cells per well were seeded in 96-well plates in 100 ml of medium and incubated overnight in 5%CO2 at 37°C. The hTNFR-Is–containing samples were seriallydiluted in 100 ml of medium and incubated overnight at 37°Cwith TNF-a at a concentration of 200 pg/ml (which generates100% cytotoxicity) and actinomycin D at 4 mg/ml (to allow hTNFR-Is and TNF-a binding). Then, 20 ml 3-[4,5-dimethyl-thiazol-2-yl]-2,5-diphenyltetrazolium bromide (thiazolyl blue)(MTT; 5 mg/ml) in 80 ml of medium was added for 4 hr at37°C. Viable cells quantities were measured by solubilizing for-mazan crystals with 150 ml of propan-1-ol/HCl 0.04 N. Thestaining was quantified by absorbance at 570 nm. A viabilityof 100% was attributed to the wells with L929 cells withoutTNF-a, and the percentage of inhibition was determined in thelinear region of the dose-response curve.
In vivo plasmid electrotransfer
DBA/1 mice (8–10 weeks old) were obtained from HarlanOlac (Bicester, UK). Mice were anesthetized with avertin
(1.25% [v/w] tribromoethanol, 2.5% [v/v] 2-methyl-butan-2-ol). Plasmid DNA (15 mg in 30 ml of sodium chloride [NaCl]150 mM) or NaCl 150 mM (30 ml) was unilaterally injectedinto the tibial-cranial muscle of a shaved hind limb. When 50mg of plasmid was used, both hind limbs were injected with 25mg of plasmid in 30 ml NaCl 150 mM, and control mice werethen injected with 30 ml NaCl 150 mM in both hind limbs. Eightelectric pulses (200 V/cm, 2 Hz, 20 ms) were delivered as pre-viously described by an ECM 930 BTX electropulsator (Gene-tronics, San Diego, CA; Mir et al., 1998, 1999).
Induction and assessment of arthritis
Arthritis was induced with native bovine collagen type II(CII) as previously described (Boissier et al., 1990). MaleDBA/1 mice were injected subcutaneously at the base of thetail with 100 mg of CII emulsified in Freund’s adjuvant. Onday 21, mice were boosted with a subcutaneous injection ofCII in incomplete Freund’s adjuvant. Mice were monitoredfor evidence of arthritis using a blind procedure. Clinicalseverity of arthritis in each joint or group of joints (toes, tar-sus, and ankle) was scored as follows: 0, normal; 1, erythema;2, swelling; 3, deformity; and 4, necrosis. These scores weresummed to obtain the arthritic score; the mean arthritic scoreon each clinical observation day and in each group was usedto evaluate CIA severity (Boissier et al., 1990). For clinicalscores, an analysis of variance method (ANOVA test) wasused. For histologic analysis, the animals were killed 62 daysafter induction of CIA, and their legs were dissected free andprocessed for histologic studies as described elsewhere(Boissier et al., 1990). The severity of synovial proliferationand the severity of inflammatory cell infiltration were eachscored using a four-point scale (0–3, where 0 is normal and3, severe).
Statistical analysis
Results were compared using Student’s t tests. For repeatedmeasures (clinical scores), we used an ANOVA test.
RESULTS
In vitro and ex vivo bioactivity of monomeric, dimeric,and chimeric TNF-a soluble receptor I
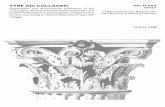
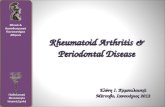
We constructed three plasmids: pCOR hTNFR-Is, pCOR hT-NFR-Is/mIgG1, pCOR (hTNFR-Is)2, encoding, respectively,for a monomeric (hTNFR-Is), chimeric (hTNFR-Is/mIgG1) ordimeric (hTNFR-Is)2 form of TNF-a human soluble receptor I(Fig. 1). The hTNFR-Is production in the supernatant ofDBA/Tst cells (Bessis et al., 2002a), which are syngeneic fi-broblasts conditionally immortalized by the temperature sensi-tive SV40 large T antigen (gift from Yuti Chernajovsky, St.Bartholomew’s Hospital, London, UK), posttransfection was165.5 6 5.8 ng per 24 hr per 106 cells with pCOR hTNFR-Is;114.2 6 8.0 ng per 24 hr per 106 cells with pCOR hTNFR-Is/mIgG1; and 23.2 6 0.8 ng per 24 hr per 106 cells with pCOR(hTNFR-I)2, as determined by using a specific ELISA kit (Duoset; data not shown). All results were expressed as equiv-alent of TNF-a monomeric receptor.
GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 191

In vitro bioactivity
To study the bioactivity of the expressed proteins, super-natants from DBA/Tst cells transfected with the three plasmidswere tested for the inhibition of TNF-a cytotoxicity on L929cells. Results shown in Table 1A highlight the strong bioactiv-ity of chimeric and dimeric forms of hTNFR-Is. The monomericform of hTNFR-Is was less efficient neutralizing TNF-a, as ex-pected.
Ex vivo bioactivity
The bioactivity of the hTNF-a soluble receptors variantsproduced in vivo in mouse by intramuscular plasmid electro-transfer as previously described (Mir et al., 1998, 1999), wasassayed on the capacity of muscle lysates to prevent TNF-a cy-totoxicity on L929 cells. This quantification was not possiblein the circulation because of the global effect of the serum. Mus-cle lysate from naïve mice or empty pCOR electrotransferred
BLOQUEL ET AL.192
Chimera hTNFR-Is/mIgG1
Monomer hTNFR-Is Dimer (hTNFR-Is)2
human
TNFR-Is
murine IgG1heavy chain
S SS S
thrombincleavage site
human
TNFR-Is
polyglycine linker
human
TNFR-Is
FIG. 1. Schematic description of the three variants of the tumor necrosis factor (TNF)-a soluble receptor I.
TABLE 1. ANTI-TNF-a ACTIVITY PRODUCED BY TRANSFECTED DBA/Tst CELLS (A) AND BY IN VIVO ELECTROTRANSFERRED MUSCLE (B)
Soluble receptor Surviving cellsTransfected plasmid (ng/ml)a (% of control)
(A) Saline Nondetectable NondetectableDBA/Tst cells Monomer 02 06
transfection Chimera 02 65Dimer 02 71
(B) Saline Nondetectable 14 6 00Intramusclar electrotransfer Empty pCOR Nondetectable 14 6 10
Monomer 96 73 6 2Chimera 45 84 6 12Dimer 04 52 6 15
A: TNF-a (200 pg/ml) was incubated with the supernatant of DBA/Tst cells transfected 48 hr before with the indicated plas-mids (3 mg, lipofectamine-transfecting agent, DBA/Tst cells in RPMI 1640 medium with glutamax 1, supplemented with 10%FCS and 1% penicillin-streptomycin). This solution was assayed for its cytolytic effect on target L929 cells. Cell survival wasquantified using a MTT assay and is expressed as percent of control in the absence of TNF-a. A representative result from threeexperiments is shown. B: TNF-a (200 pg/ml) was incubated with the lysates of tibial cranial muscles (n 5 2), that were elec-trotransferred 14 days before with 15 mg of the indicated plasmids. This solution was assayed for its cytolytic effect on targetL929 cells as in (A). Cell survival was quantified using a MTT assay and is expressed as percent of control in the absence ofTNF-a. Results are mean 6 SEM of duplicate determinations.
aIn both experiments, soluble receptor concentration was measured in the cell supernatants (A) or in muscle lysates (B) usinga specific ELISA.
TNF-a, tumor necrosis factor-a; FCS, fetal calf serum; MTT, 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide(thiazolyl blue); SEM, standard error of the mean; ELISA, enzyme-linked immunosorbent assay.

mice both resulted in a slight 14% inhibition of cytotoxicity(Table 1B). On the other hand, lysates of mice electrotrans-ferred with the three plasmids resulted in a marked inhibitionof TNF-a cytotoxicity, which demonstrates the bioactivity ofthe three proteins produced in mouse muscle. Unlike DBA/Tstsupernatants (Table 1A), the monomeric form of hTNFR-Is in-hibited hTNF-a cytotoxicity, but approximately 50 times moresoluble receptor monomer was produced in muscle lysate thanin DBA/Tst supernatant and was used in the hTNF-a protec-tion assay.
Expression of hTNFR-Is in muscle and serum afterintramuscular electrotransfer
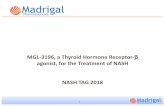
At day 10 after electrotransfer, dose-dependent expressionof hTNFR-Is was detected in both muscle and serum (Fig. 2)by using the same ELISA kit as above. With 15 mg of injected
plasmid, the level of immunoreactive hTNFR-Is in muscle wasof the same order of magnitude with the three constructs (ap-proximately 10,000 pg/mg protein). A very low production ofhTNFR-Is was detected in the contralateral control muscle ofeach group. In the serum, as shown in Figure 2B, plasmatic hTNFR-Is immunoreactivity was drastically higher with thechimeric hTNFR-Is/mIgG1 protein (approximately 5,600 pg/mlfor 15 mg of electrotransferred plasmid) than with the two otherconstructs, pCOR hTNFR-Is and pCOR (hTNFR-Is)2. No sys-temic production of hTNFR-Is was observed in control non-plasmid-injected mice.
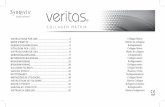
Figure 3A shows that a peak of expression is reached intoelectrotransferred muscles between day 7 and day 14 for themonomeric and dimeric hTNFR-Is (11,600 and 11,200 pg/mgprotein, respectively). For hTNFR-Is/mIgG1, the maximumconcentration in muscle was reached after 1 month (42,400pg/mg protein). The levels of detected proteins then declined
GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 193
B
hT
NF
R-I
s m
on
om
eric
eq
uiv
alen
t (p
g/m
g p
rote
in)
8000
pCOR
0
2000
4000
6000
1 3 5 15
pCOR hTNFR-Is
0
100
200
300
1 3 5 1502000
6000
10000
14000 pCOR hTNFR-Is
electrotransferred musclecontralateral control
1 3 5 15
pCOR hTNFR-Is/mIgG1
0
2000
6000
10000
14000
1 3 5 15
pCOR (hTNFR-Is)2
0
2000
6000
10000
14000
1 3 5 15
pCOR (hTNFR-Is)2
0
100
200
300
400
1 3 5 15Injected plasmid (mg)
hT
NF
R-I
s m
on
om
eric
eq
uiv
alen
t (p
g/m
l)A
Soluble receptor in muscle Soluble receptor in plasma
pCOR hTNFR-Is/mlgG1
FIG. 2. Dose-dependent expression of hTNFR-Is variants in the muscle (A) and in the serum (B) after intramuscular electro-transfer. The hTNFR-Is concentration was assayed by enzyme-linked immunosorbent assay (ELISA) 10 days after intramuscu-lar electrotransfer of increasing plasmid dose (n 5 2). A: hTNFR-Is production in the muscle. In muscles electrotransferred withempty pCOR, nonsignificant control values were detected. B: hTNFR-Is production in serum. Serum from mice electrotrans-ferred with empty pCOR do not express hTNFR-Is.

and stabilized at values of approximately 1000 pg/mg proteinfor both monomer and dimer, and at approximately 30,000pg/mg protein for hTNFR-Is/mIgG1. In the serum, the mono-meric and dimeric proteins were detectable for 2 or 4 weeks,respectively, and reached a maximum of 180 pg/ml for hTNFR-Is, and 310 pg/ml for (hTNFR-Is)2 (Fig. 3B). These two pro-teins were then detected episodically in a few mice serum, atapproximately 50 pg of hTNFR-Is per milliliter. The secretedchimeric hTNFR-Is/mIgG1 reached peak value at days 15–30after electrotransfer (approximately 16,500 pg/ml). It then grad-ually declined, but was still approximately 3000 pg/ml 6 monthsafter electrotransfer.
A 50-mg dose of electrotransferred plasmid was also testedusing the dimeric encoding construct and led to a circulatingrate of 1314 6 415 pg/ml 14 days after electrotransfer (n 5 2),instead of 313 6 313 pg/ml by electrotransfer of 15 mg of thesame plasmid. This result shows that the systemic dose-re-sponse relationship is worthwhile up to at least 50 mg of elec-trotransferred plasmid.
Electrotransfer of hTNFR-Is plasmid variants in micewith CIA
In a preliminary experiment, male DBA/1 mice were elec-trotransferred with 15 mg of plasmid at the onset of the disease.This treatment resulted in a mild improvement of the clinicalevolution of the disease (data not shown), so a higher dose wasstudied in order to highlight more clearly the therapeutic po-tentiality of the constructs. Thus, male DBA/1 mice were elec-trotransferred with 50 mg of plasmid or similar volume of NaClat the onset of clinical symptoms of CIA (day 25). Clinicalscores of control groups treated with NaCl and empty pCORexhibited a slightly different evolution during the progressionof the disease (Fig. 4). This may be explained by a small in-flammatory stimulation by injecting this high plasmid dose.Only the hTNFR-Is/mIgG1 construct led to an important de-crease of arthritis clinical symptoms. This protection was highlysignificant (p 5 0.0001 vs. NaCl or empty pCOR groups). Nev-ertheless, mice treated with pCOR (hTNFR-Is)2 also displayed
BLOQUEL ET AL.194
0
4000
8000
12000
16000
0 40 80 120 160
0
20000
40000
60000
0 40 80 120 160
0
200
400
600
0 40 80 120 160
0
10000
20000
30000
0 40 80 120 160
0
100
200
300
0 40 80 120 160
hT
NF
R-I
s m
on
om
eric
eq
uiv
alen
t (p
g/m
g p
rote
in)
Time after electrotransfer (days)
BApCOR hTNFR-Is
0
4000
8000
12000
0 40 80 120 160
electrotransferred musclecontralateral control
Soluble receptor in muscle Soluble receptor in plasma
pCOR hTNFR-Is/mlgG1
pCOR (hTNFR-Is)2
hT
NF
R-I
s m
on
om
eric
eq
uiv
alen
t (p
g/m
l)
pCOR hTNFR-Is
pCOR hTNFR-Is/mlgG1
pCOR (hTNFR-Is)2
FIG. 3. Kinetics of hTNFR-Is variants, in the muscle (A) and in the serum (B) after intramuscular electrotransfer. Fifteen micro-grams of the indicated plasmid was electrotransferred in two mice for each date. Experimental parameters were as in Figure 1.

a decreased disease severity (p 5 0.0378 vs. empty pCORgroup). As a positive control, a group of mice was treated with200 mg of etanercept per mouse 3 times per week (a conditionthat has proven efficiency [Williams et al., 1995; Quattrocchiet al., 1999]), from day 25 to day 42, and twice or once perweek to day 60. These mice were well protected from arthritisuntil day 42, but the clinical score started to increase as injec-tions were spaced. Of note, the clinical score of etanercept-treated mice sharply increased when injections were stoppedfor a single week, thus reaching higher values than the clinicalscore of pCOR hTNFR-Is/mIgG1–electrotransferred mice, whichhad only been treated once at the onset of disease, at day 25.Histologic evaluation showed a clear-cut decrease of arthritisin pCOR hTNFR-Is/mIgG1–treated mice compared to control(p , 0.05 vs. NaCl and p , 0.05 vs. empty pCOR; Table 2 andFig. 5). Moreover, as expected, etanercept treatment also re-sulted in a strong reduction of histologic scores even if treat-ment with the recombinant protein was stopped 8 days before
GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 195
days after immunizationElectrotransfer
21 26 36 41 51 56 61
clin
ical
sco
res
0
2
4
6
8
10
12
14
31 46
pCOR hTNFR-Is
pCOR hTNFR-Is /mIgG1* #
pCOR (hTNFR-Is)2**
etanercept * #
NaClempty pCOR
FIG. 4. Effect of electrotransfer of 50 mg of plasmid encoding hTNFR-Is variants and of TNFR-IIs/Fc-immunoglobulin do-main fusion protein (etanercept) on the clinical score of collagen-induced arthritis. The gene therapy treatment was administeredat the onset of the disease (day 25, thick arrow) into the tibial cranial muscle of both hind limbs (2 3 25 mg). A group of micewas treated by injection of 200 mg intraperitoneally of etanercept at dates indicated by fine arrows. As controls, 50 mg of emptypCOR were electrotransferred in one group, and another group was injected and electrotransferred with 2 3 30 ml of NaCl. Arthri-tis scores were evaluated in the four paws. Each point represents the mean arthritis score in the corresponding group (n 5 10,except 50 mg of empty pCOR: n 5 15 and NaCl: n 5 14) on a given day. *p 5 0.0001 vs. empty pCOR (analysis of variance[ANOVA]); **p 5 0.0378 vs. empty pCOR (ANOVA); #p 5 0.0001 vs. NaCl (ANOVA).
the leg sampling (p , 0.02 vs. NaCl and p , 0.02 vs. emptypCOR, Table 2 and Fig. 5). No difference in histologic scoreswas observed between monomer- or dimer-treated mice andcontrol groups.
DISCUSSION
The present report shows that electrotransferred muscle isable to produce the three forms of human TNF-a soluble re-ceptor I (monomeric, dimeric, and the IgG chimera) and, mostimportantly, to secrete these proteins under a bioactive form,which binds to and inactivates TNF-a. Previous studies withTNF-a soluble receptors using an adenoviral vector encodingthe IgG soluble receptor chimera have shown systemic expres-sion for only 4 weeks after injection (Kolls et al., 1994). A sys-temic production of chimeric protein has been reached for sixmonths using an adeno-associated virus (AAV) vector (Chan et

al., 2002). In another study using intra-articular injection of anAAV encoding the monomeric soluble receptor I, the proteinwas detected during 2 months in the joint but never in the serum(Zhang et al., 2000). In the present electrotransfer experiment,the monomeric, dimeric, and chimeric hTNFR-Is variants weredetected in the muscle for at least 6 months.
Nevertheless we have observed different kinetic profiles inthe electrotransferred muscle. Intramuscular concentration ofTNF-a soluble receptor is higher and more stable for the chi-meric protein, whereas it is decreased by one order of magni-tude between day 7 to 15 for the dimeric and monomeric forms.The origin of this time-dependent decrease in intramusculartransgene expression during the first weeks after electrotrans-fer is still unclear, but has been commonly seen including inimmunodeficient severe combined immunodeficiency disorders(SCID) mice (Bettan et al., 2000; Deleuze et al., 2002; Kim etal., 2003). Several hypotheses can be proposed. First, the se-cretion profile differences of the three variants might be attrib-uted to the differences of sizes between the proteins, resultingin different features of crossing of the endothelial barrier. Thus,the chimeric protein that is the biggest (M <100 kd) must re-main longer in the interstitial media (Michel, 1972), and as aresult, accumulates into the muscle up to 40 days after electro-transfer. Intramuscular proteases may also have different be-havior toward the variants and hardly degrade the chimeric formbecause it is bigger (Dice et al., 1973). The hypothesis of genesilencing can be discarded because we previously showed along-lasting expression (more than 270 days) after electro-transfer of a luciferase-encoding plasmid with the same back-bone (pCOR) as our constructs (Mir et al., 1999). Likewise, hu-man secreted alkaline phosphatase can also be detected for morethan 168 days in SCID mice after electrotransfer of the corre-sponding plasmid (our unpublished results). It is possible thatsome of the transfected fibers are lost as a result of partial degra-dation of the transfected myofibers, local inflammation afterelectrotransfer (Hartikka et al., 2001), or immune responseagainst the transfected cells. Nevertheless, at least a part of thesecells remain functional because approximately 10% of the max-imum of monomeric or dimeric protein is still detected after 6
months, and this level of detection is well above the back-ground. A possible immune response against plasmid DNA can-not either explain the decrease of expression. It actually wouldalso lead to the elimination of the cells transfected with the plas-mid encoding the chimeric protein, and also result in a decreaseof the production of this form of soluble receptor, which is notthe case. Moreover, we used a pCOR backbone (Soubrier et al.,1999), which contains few viral sequences and was designedspecifically to avoid immune reaction against plasmid vector.
We cannot discard the possibility of an immune responseagainst the monomeric and dimeric forms of the protein, andnot the chimeric protein, because of conformation differences.Previous results highlight the low immunogenicity of a hTNFR-Is/mIgG1 protein (Kolls et al., 1994), similar to the one pro-duced with our construct. Concerning an immune response inhuman, studies have been done by use of recombinant proteins.Thus, IgG and IgM have been found against a recombinant hu-man TNFR-Is/IgG1 fusion protein, but no neutralizing activityof these antibodies has been detected (Christen et al., 1999). Aphase 2 clinical trial using PEGylated recombinant human sol-uble TNF-a receptor I has highlighted that 5% of patients wereseropositive for antibodies against PEG TNFR-Is, but no neu-tralizing antibody has been found (Davis et al., 2000). How-ever, this antibody response affected the half-life and clearanceof the protein, which would thus not be used for treating pa-tients with RA (Moreland et al., 2000). A phase 1 study is alsoongoing with onercept (hTNFR-Is; Serono SA, Rockland, MA),and no antibodies against the molecule have been found (Trin-chard-Lugan et al., 2001). Likewise, all antibodies against etan-ercept were non-neutralizing (Calabrese, 2003).
Regarding circulating rates, chimeric and dimeric solubleTNF-a receptors I were also detected in the serum during the6 months of the kinetic study, whereas the monomer was onlydetected during 2 weeks. Electrotransfer of pCOR hTNFR-Is/mIgG1 induced a stable seric concentration (approximately3000 pg hTNFR-Is per milliliter) from the third month afterelectrotransfer. The chimeric protein was detected in the serumof all mice, while the dimeric receptor was detected in half ofthe mice (9/18). Previous studies have shown that the chimericIgG-protein is stable in serum (Kolls et al., 1994) (half-life 5
29 hours by using an adenoviral vector). Thus, although the chi-meric soluble TNF-a receptor is quite large because it is prob-ably secreted as a dimer (M <100 kd) it appears to be effi-ciently secreted by skeletal muscle cells and to readily diffusethrough muscle extracellular basal lamina. The monomericTNF-a soluble receptor I (M <25 kd) is well known as a highlyunstable molecule, unusable clinically. Moreover, its small sizetheoretically allows fast kidney elimination. Accordingly, thismonomeric receptor was no longer detected in the serum 2weeks after intramuscular electrotransfer. We had envisionedthat the more original dimeric form of the soluble TNF-a re-ceptor could be more stable in serum than the monomer, withrespect to protease attack and renal filtration, because of itslarger molecular weight (M <50 kd). However, the dimeric re-ceptor, while detected in the serum, was at a much lower con-centration than the chimeric hTNFR-Is/mIgG1 receptor, indi-cating either seric protease degradation, consequent kidneyelimination, because the molecular weight of the dimer is stilllower than kidney filtration size threshold, or immune reactionagainst the protein.
BLOQUEL ET AL.196
TABLE 2. EFFECT OF hTNFR-Is VARIANTS ON HISTOLOGIC
PARAMETER OF COLLAGEN-INDUCED ARTHRITIS
Electrotransferred plasmid Hindleg scorea
Sodium chloride 1.87 6 0.29**empty pCOR 1.77 6 0.23**pCOR hTNFR-Is 1.72 6 0.37**pCOR hTNFR-Is/mIgG1 0.94 6 0.32**pCOR (hTNFR-Is)2 1.71 6 0.350*Etanercept 0.75 6 0.30**
Experiment shown in Figure 4. An amount of 25 mg of theindicated plasmids or 30 ml of NaCl 150 mM was injected intoboth tibial cranial muscle hind limbs, prior to electric pulsesdelivery. The treatment was administered at the onset of thedisease (day 25).
aMean 6 SEM.*p , 0.05 vs. empty pCOR or NaCl.**p , 0.02 vs. empty pCOR or NaCl.NaCl, sodium chloride; SEM, standard error of the mean.

GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 197
FIG. 5. Examples illustrating histologic analysis. Hematoxylin and eosin (H&E) staining, 1003 magnification, showing theknee. A: Empty pCOR-treated mouse: synovitis and cartilage destruction. B: pCOR hTNFR-Is–treated mouse: synovitis and car-tilage destruction. C: pCOR (hTNFR-Is)2–treated mouse: synovitis and cartilage destruction. D: pCOR hTNFR-Is/mIgG1–treatedmouse: aspect of normal synovial and cartilage. E: Etanercept-treated mouse: aspect of normal synovial and cartilage. (black ar-row: synovial membrane, white arrow: cartilage).

The dose response observed in transgenic protein level in thepresent work confirms earlier results obtained with other genessuch as erythropoietin, proinsulin, or luciferase (Kon et al., 1999;Payen et al., 2001; Blair-Parks et al., 2002) and is relevant to fu-ture therapeutic development. This is especially important in thecase of anti-inflammatory cytokine treatment, because uncon-trolled TNF-a inhibition might increase infection or tumor risk.Relevant also to the biosafety of the electrotransfer method, aPCR study of the triceps next to the electrotransferred muscleand of organs distant from this muscle (liver, kidney, spleen,heart, lung, brain, gonads) indicated that there was no diffusionof the injected plasmid (unpublished results).
The three forms of receptors produced in the electrotrans-ferred muscle were able to bind TNF-a and to inhibit its cyto-toxic activity. However, from in vitro results using a low con-centration of soluble TNF-a receptor equivalent, we can assume that the monomeric receptor, because it can only bindone subunit of the TNF-a trimer, poorly prevents TNF-a bind-ing to the transmembrane TNF receptor, and hence only weaklyprevents the effect of this cytokine. On the other hand, thedimeric receptor exhibited quite the same bioactivity as the chi-meric receptor. This suggests the same mode of action, i.e.,binding to 2 of the 3 subunits of TNF-a trimer, thus prevent-ing activation of transmembrane TNF receptor, because the re-maining TNF subunit is unable to activate this receptor (Adamet al., 1995). Concerning the ex vivo bioactivity of the proteins(i.e., using transfected muscle homogenate), results highlightthat the three proteins produced in vivo by electrotransferredmuscle were biologically active. These results suggest that ex-pression in muscle cells allows for normal TNFR-Is glycosyla-tion and leads to production of clinically relevant proteins.
A major purpose of our study was to assess whether block-ade of TNF-a activity through electrotransfer-mediated plas-mid delivery of different TNF-a–binding proteins is feasibleand effective in a chronic inflammatory disease model such asCIA. Previous studies on TNFRs in RA models have been per-formed using an TNFR-Is/mIgG1 encoding adenoviral vectorinjected at the onset of the disease (Quattrocchi et al., 1999).Quattrocchi and colleagues (1999) reported a transitory im-provement only during 10 days, followed by a 10-day escala-tion of clinical symptoms, even though the TNFRs-IgG chimerawas still detected in the serum. Another study in rats, using thesame construct, was efficient by intravenous injection, but notby intra-articular injection (Le et al., 1997). An Adeno Asso-ciated Virus (AAV) encoding the monomeric form of the re-ceptor was also used by intra-articular injection in TNF-a trans-genic mice (Zhang et al., 2000), leading to arthritis inhibition.Another AAV encoding a TNFR-Fc protein was efficient by in-tramuscular or intra-articular administration in the SCW-in-duced rat arthritis model (Chan et al., 2002). Recently, a studyusing electrotransfer delivery of a hTNFR-IIs/hIgG1–encodingplasmid has shown efficacy in the treatment of CIA for at least18 days (Kim et al., 2003). Ours results highlight that one sin-gle electrotransfer of 50 mg of plasmid encoding a chimericprotein hTNFR-Is/mIgG1, at the onset of the disease, is clini-cally and histologically effective in a model of RA. Moreover,the long-lasting protective effect is observed for more than 5weeks. The same dose of the dimeric construct leads to a lessimportant, but nonetheless significant inhibition of the arthriticdisease. We also proved the importance of the electrotransfer
method because the injection of pCOR hTNFR-Is/mIgG1 with-out electrotransfer was unable to prevent the development ofthe disease (data not shown). Interestingly, the comparison be-tween multiple, repeated injection of recombinant solubleTNFR-II (etanercept), and a unique pCOR hTNFR-Is/mIgG1electrotransfer at the onset of the disease, leads to similar re-sults. Protein injection remained the most efficient treatmentwhen frequently administered 3 times per week, but clinicalscore rapidly increased as soon as injection became spaced.Moreover, after stopping recombinant protein treatment, theclinical score rapidly became higher than that observed in thegroup that had been electrotransferred with a single dose ofpCOR hTNFR-Is/mIgG1 5 weeks before. These results are inagreement with observations concerning patients with RA un-dergoing etanercept treatment where disease pathology returnsunabated immediately on termination of the protein treatment(Robbins et al., 2003). This highlights the potential practicaladvantage of gene therapy, which leads to sustained therapeu-tic effect after single treatment, which is especially importantfor chronic diseases, such as RA, which require long-term ther-apy. It could also be of interest for the patient’s quality of life.Finally, a single injection of plasmid DNA also has an eco-nomic advantage: the treatment would be less expensive thanrepeated recombinant protein injections (which are expensiveto produce) to achieve the same benefits.
In conclusion, the present work illustrates the relevance ofelectrotransfer of plasmids encoding monomeric, dimeric, orchimeric human soluble receptor I in an arthritis model. Thethree TNF-a soluble receptor variants are bioactive, producedin a dose-dependent manner, and, for the first time, a systemicproduction of chimeric and dimeric receptors has been observedfor at least 6 months. Moreover, our results highlight the effi-ciency of two of these proteins in CIA treatment. To our knowl-edge, for the first time, some superiority (of a practical and eco-nomical kind) over recombinant protein treatment has beenobserved using nonviral gene therapy with a hTNFR-Is/mIgG1chimera. Finally, from a methodological point of view, the pres-ent work illustrates the general potentiality of plasmid intra-muscular electrotransfer for the rapid screening and compara-tive assessment of different variant forms of secreted proteinssuch as plasmatic factors, cytokines, or cytokine inhibitors.
ACKNOWLEDGMENTS
This work was supported by the CNRS, INSERM, the ENSCP,Paris 5 Pharmacy René Descartes University, Gencell S.A., theAssociation de Recherche sur la Polyarthrite (ARP), the SociétéFrançaise de Rhumatologie (SFR), and the Association ClaudeBernard. We are grateful to Virginie Deleuze, Delphine Lemeiter(UPRES EA-3408), Monique Etienne, and Simone Beranger (UP-RES EA-3410) for their outstanding technical assistance and toStéphane Chambris for his expert care of the animals.
REFERENCES
ADAM, D., KESSLER, U., and KRONKE, M. (1995). Cross-linkingof the p55 tumor necrosis factor receptor cytoplasmic domain by adimeric ligand induces nuclear factor-kappa B and mediates celldeath. J. Biol. Chem. 270, 17482–17487.
BLOQUEL ET AL.198

AIHARA, H., and MIYAZAKI, J. (1998). Gene transfer into muscleby electroporation in vivo. Nat. Biotechnol. 16, 867–870.
AL-JANADI, M., AL-BALLA, S., AL-DALAAN, A., and RAZIUD-DIN, S. (1993). Cytokine profile in systemic lupus erythematosus,rheumatoid arthritis, and other rheumatic diseases. J. Clin. Immunol.13, 58–67.
BAERT, F., NOMAN, M., VERMEIRE, S., VAN ASSCHE, G.,D’HAENS, G., CARBONEZ, A., and RUTGEERTS, P. (2003). In-fluence of immunogenicity on the long-term efficacy of infliximabin Crohn’s disease. N. Engl. J. Med. 348, 601–608.
BATHON, J.M., MARTIN, R.W., FLEISCHMANN, R.M., TESSER,J.R., SCHIFF, M.H., KEYSTONE, E.C., GENOVESE, M.C.,WASKO, M.C., MORELAND, L.W., WEAVER, A.L., MARKEN-SON, J., and FINCK, B.K. (2000). A comparison of etanercept andmethotrexate in patients with early rheumatoid arthritis. N. Engl. J.Med. 343, 1586–1593.
BESSIS, N., COTTARD, V., SAIDENBERG-KERMANACH, N.,LEMEITER, D., FOURNIER, C., and BOISSIER, M.C. (2002a).Syngeneic fibroblasts transfected with a plasmid encoding inter-leukin-4 as non-viral vectors for anti-inflammatory gene therapy incollagen-induced arthritis. J. Gene Med. 4, 300–307.
BESSIS, N., DOUCET, C., COTTARD, V., DOUAR, A.M., FIRAT, H.,JORGENSEN, C., MEZZINA, M., and BOISSIER, M.C. (2002b). Genetherapy for rheumatoid arthritis. J. Gene Med. 4, 581–591.
BETTAN, M., EMMANUEL, F., DARTEIL, R., CAILLAUD, J.M.,SOUBRIER, F., DELAERE, P., BRANELEC, D., MAHFOUDI, A.,DUVERGER, N., and SCHERMAN, D. (2000). High-level proteinsecretion into blood circulation after electric pulse-mediated genetransfer into skeletal muscle. Mol. Ther. 2, 204–210.
BETTAN, M., IVANOV, M.A., MIR, L.M., BOISSIERE, F., DE-LAERE, P., and SCHERMAN, D. (2000). Efficient DNA electro-transfer into tumors. Bioelectrochemistry 52, 83–90.
BLAIR-PARKS, K., WESTON, B.C., and DEAN, D.A. (2002). High-level gene transfer to the cornea using electroporation. J. Gene Med.4, 92–100.
BOISSIER, M.C., CHIOCCHIA, G., RONZIERE, M.C., HERBAGE,D., and FOURNIER, C. (1990). Arthritogenicity of minor cartilagecollagens (types IX and XI) in mice. Arthritis Rheum. 33, 1–8.
CALABRESE, L.H. (2003). Molecular differences in anticytokine ther-apies. Clin. Exp. Rheumatol. 21, 241–248.
CHAN, J.M., VILLARREAL, G., JIN, W.W., STEPAN, T., BURSTEIN,H., and WAHL, S.M. (2002). Intraarticular gene transfer of TNFR:Fcsuppresses experimental arthritis with reduced systemic distributionof the gene product. Mol. Ther. 6, 727–736.
CHRISTEN, U., THUERKAUF, R., STEVENS, R., and LESSLAUER,W. (1999). Immune response to a recombinant human TNFR55-IgG1fusion protein: auto-antibodies in rheumatoid arthritis (RA) and mul-tiple sclerosis (MS) patients have neither neutralizing nor agonist ac-tivities. Hum. Immunol. 60, 774–790.
COTTARD, V., MULLEMAN, D., BOUILLE, P., MEZZINA, M.,BOISSIER, M.C., and BESSIS, N. (2000). Adeno-associated virus-mediated delivery of IL-4 prevents collagen-induced arthritis. GeneTher. 7, 1930–1939.
DAVIS, M.W., FEIGE, U., BENDELE, A.M., MARTIN, S.W., and ED-WARDS, C.K. (2000). Treatment of rheumatoid arthritis with PEG-ylated recombinant human soluble tumour necrosis factor receptor typeI: A clinical update. Ann. Rheum. Dis. 59(Suppl 1), i41–43.
DELEUZE, V., SCHERMAN, D., and BUREAU, M.F. (2002). Inter-leukin-10 expression after intramuscular DNA electrotransfer: kineticstudies. Biochem. Biophys. Res. Commun. 299, 29–34.
DICE, J.F., DEHLINGER, P.J., and SCHIMKE, R.T. (1973). Studieson the correlation between size and relative degradation rate of sol-uble proteins. J. Biol. Chem. 248, 4220–4228.
EVANS, C.H., GHIVIZZANI, S.C., KANG, R., MUZZONIGRO, T.,WASKO, M.C., HERNDON, J.H., and ROBBINS, P.D. (1999).Gene therapy for rheumatic diseases. Arthritis Rheum. 42, 1–16.
EVANS, T.J., MOYES, D., CARPENTER, A., MARTIN, R.,LOETSCHER, H., LESSLAUER, W., and COHEN, J. (1994). Pro-tective effect of 55- but not 75-kD soluble tumor necrosis factor re-ceptor-immunoglobulin G fusion proteins in an animal model ofgram-negative sepsis. J. Exp. Med. 180, 2173–2179.
FELDMANN, M., BRENNAN, F., and MAINI, R.N. (1996). Roleof cytokines in rheumatoid arthritis. Annu. Rev. Immunol. 14,397–440.
FRISHMAN, J.I., EDWARDS, C.K., SONNENBERG, M.G., KOHNO,T., COHEN, A.M., and DINARELLO, C.A. (2000). Tumor necro-sis factor (TNF)-alpha–induced interleukin-8 in human blood cul-tures discriminates neutralization by the p55 and p75 TNF solublereceptors. J. Infect. Dis. 182, 1722–1730.
GHIVIZZANI, S.C., LECHMAN, E.R., KANG, R., TIO, C., KOLLS,J., EVANS, C.H., and ROBBINS, P.D. (1998). Direct adenovirus-mediated gene transfer of interleukin 1 and tumor necrosis factor al-pha soluble receptors to rabbit knees with experimental arthritis haslocal and distal anti-arthritic effects. Proc. Natl. Acad. Sci. U.S.A.95, 4613–4618.
GRELL, M., WAJANT, H., ZIMMERMANN, G., and SCHEURICH,P. (1998). The type 1 receptor (CD120a) is the high-affinity recep-tor for soluble tumor necrosis factor. Proc. Natl. Acad. Sci. U.S.A.95, 570–575.
HANNA, E., ZHANG, X., WOODLIS, J., BREAU, R., SUEN, J., andLI, S. (2001). Intramuscular electroporation delivery of IL-12 genefor treatment of squamous cell carcinoma located at distant site. Can-cer Gene Ther. 8, 151–157.
HARRIS, E.D. (1990). Rheumatoid arthritis. Pathophysiology and im-plications for therapy. N. Engl. J. Med. 322, 1277–1289.
HARTIKKA, J., SUKHU, L., BUCHNER, C., HAZARD, D., BOZOU-KOVA, V., MARGALITH, M., NISHIOKA, W.K., WHEELER,C.J., MANTHORP, M., and SAWDEY, M. (2001). Electroporation-facilitated delivery of plasmid DNA in skeletal muscle: Plasmid de-pendence of muscle damage and effect of poloxamer 188. Mol. Ther.4, 407–415.
JOOSTEN, L.A., HELSEN, M.M., SAXNE, T., VAN-DE-LOO, F.A.,HEINEGARD, D., and VAN DEN BERG, W.B. (1999). IL-1 alphabeta blockade prevents cartilage and bone destruction in murine typeII collagen-induced arthritis, whereas TNF-alpha blockade only ame-liorates joint inflammation. J. Immunol. 163, 5049–5055.
KIM, J.M., HO, S.H., HAHN, W., JEONG, J.G., PARK, E.J., LEE,H.J., YU, S.S., LEE, C.S., LEE, Y.W., and KIM, S. (2003). Electro-gene therapy of collagen-induced arthritis by using an expressionplasmid for the soluble p75 tumor necrosis factor receptor-Fc fusionprotein. Gene Ther. 10, 1216–1224.
KIM, K.N., WATANABE, S., MA, Y., THORNTON, S., GIANNINI,E.H., and HIRSCH, R. (2000). Viral IL-10 and soluble TNF recep-tor act synergistically to inhibit collagen-induced arthritis followingadenovirus-mediated gene transfer. J. Immunol. 164, 1576–1581.
KIM, S.H., LECHMAN, E.R., KIM, S., NASH, J., OLIGINO, T.J., andROBBINS, P.D. (2002). Ex vivo gene delivery of IL-1Ra and solu-ble TNF receptor confers a distal synergistic therapeutic effect inantigen-induced arthritis. Mol. Ther. 6, 591–600.
KISHIDA, T., ASADA, H., SATOH, E., TANAKA, S., SHINYA, M.,HIRAI, H., IWAI, M., TAHARA, H., IMANISHI, J., and MAZDA,O. (2001). In vivo electroporation-mediated transfer of interleukin-12 and interleukin-18 genes induces significant antitumor effectsagainst melanoma in mice. Gene Ther. 8, 1234–1240.
KLIMIUK, P.A., SIERAKOWSKI, S., LATOSIEWICZ, R., CYLWIK,B., SKOWRONSKI, J., and CHWIECKO, J. (2001). Serum cyto-kines in different histological variants of rheumatoid arthritis. J.Rheumatol. 28, 1211–1217.
KOLLS, J., PEPPEL, K., SILVA, M., and BEUTLER, B. (1994). Pro-longed and effective blockade of tumor necrosis factor activitythrough adenovirus-mediated gene transfer. Proc. Natl. Acad. Sci.U.S.A. 91, 215–219.
GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 199

KON, O.L., SIVAKUMAR, S., TEOH, K.L., LOK, S.H., and LONG,Y.C. (1999). Naked plasmid-mediated gene transfer to skeletal mus-cle ameliorates diabetes mellitus. J. Gene Med. 1, 186–194.
KREISS, P., BETTAN, M., CROUZET, J., and SCHERMAN, D.(1999). Erythropoietin secretion and physiological effect in mouseafter intramuscular plasmid DNA electrotransfer. J. Gene Med. 1,245–250.
LE, C.H., NICOLSON, A.G., MORALES, A., and SEWELL, K.L.(1997). Suppression of collagen-induced arthritis through adenovi-rus-mediated transfer of a modified tumor necrosis factor alpha re-ceptor gene. Arthritis Rheum. 40, 1662–1669.
LIPSKY, P.E., VAN DER HEIJDE, D.M., ST. CLAIR, E.W., FURST,D.E., BREEDVELD, F.C., KALDEN, J.R., SMOLEN, J.S., WEIS-MAN, M., EMERY, P., FELDMANN, M., HARRIMAN, G.R., andMAINI, R.N. (2000). Infliximab and methotrexate in the treatmentof rheumatoid arthritis. Anti-Tumor Necrosis Factor Trial in Rheu-matoid Arthritis with Concomitant Therapy Study Group. N. Engl.J. Med. 343, 1594–1602.
MAINI, R., ST. CLAIR, E.W., BREEDVELD, F., FURST, D.,KALDEN, J., WEISMAN, M., SMOLEN, J., EMERY, P., HARRI-MAN, G., FELDMANN, M., and LIPSKY, P. (1999). Infliximab(chimeric anti-tumour necrosis factor alpha monoclonal antibody)versus placebo in rheumatoid arthritis patients receiving concomitantmethotrexate: A randomised phase III trial. ATTRACT Study Group.Lancet 354, 1932–1939.
MARUYAMA, H., SUGAWA, M., MORIGUCHI, Y., IMAZEKI, I.,ISHIKAWA, Y., ATAKA, K., HASEGAWA, S., ITO, Y.,HIGUCHI, N., KAZAMA, J.J., GEJYO, F., and MIYAZAKI, J.I.(2000). Continuous erythropoietin delivery by muscle-targetedgene transfer using in vivo electroporation. Hum. Gene Ther. 11,429–437.
MARUYAMA, H., ATAKA, K., GEJYO, F., HIGUCHI, N., ITO, Y.,HIRAHARA, H., IMAZEKI, I., HIRATA, M., ICHIKAWA, F., NE-ICHI, T., KIKUCHI, H., SUGAWA, M., and MIYAZAKI, J. (2001).Long-term production of erythropoietin after electroporation-medi-ated transfer of plasmid DNA into the muscles of normal and ure-mic rats. Gene Ther. 8, 461–468.
MATHIESEN, I. (1999). Electropermeabilization of skeletal muscle en-hances gene transfer in vivo. Gene Ther. 6, 508–514.
MICHEL, C.C. (1972). Flows across the capillary wall. In Cardiovas-cular Fluid Dynamics. D.H. Bergel (Academic Press, New York) pp.241–298.
MIR, L.M., BUREAU, M.F., RANGARA, R., SCHWARTZ, B., andSCHERMAN, D. (1998). Long-term, high level in vivo gene ex-pression after electric pulse-mediated gene transfer into skeletal mus-cle. C R Acad Sci III 321, 893–899.
MIR, L.M., BUREAU, M.F., GEHL, J., RANGARA, R., ROUY, D.,CAILLAUD, J.M., DELAERE, P., BRANELLEC, D., SCHWARTZ,B., and SCHERMAN, D. (1999). High-efficiency gene transfer intoskeletal muscle mediated by electric pulses. Proc. Natl. Acad. Sci.U.S.A. 96, 4262–4267.
MORELAND, L.W., BAUMGARTNER, S.W., SCHIFF, M.H.,TINDALL, E.A., FLEISCHMANN, R.M., WEAVER, A.L., ET-TLINGER, R.E., COHEN, S., KOOPMAN, W.J., MOHLER, K.,WIDMER, M.B., and BLOSCH, C.M. (1997). Treatment of rheu-matoid arthritis with a recombinant human tumor necrosis factorreceptor (p75)-Fc fusion protein. N. Engl. J. Med. 337, 141–147.
MORELAND, L.W., MCCABE, D.P., CALDWELL, J.R., SACK, M.,WEISMAN, M., HENRY, G., SEELY, J.E., MARTIN, S.W., YEE,C.L., BENDELE, A.M., FRAZIER, J.L., KOHNO, T., COSENZA,M.E., LYONS, S.A., DAYER, J.M., COHEN, A.M., and ED-WARDS, C.K. (2000). Phase I/II trial of recombinant methionyl hu-man tumor necrosis factor binding protein PEGylated dimer in pa-tients with active refractory rheumatoid arthritis. J. Rheumatol. 27,601–609.
MORI, L., ISELIN, S., DE-LIBERO, G., and LESSLAUER, W. (1996).Attenuation of collagen-induced arthritis in 55-kDa TNF receptortype 1 (TNFR1)-IgG1-treated and TNFR1-deficient mice. J. Im-munol. 157, 3178–3182.
NAKANO, A., MATSUMORI, A., KAWAMOTO, S., TAHARA, H.,YAMATO, E., SASAYAMA, S., and MIYAZAKI, J.I. (2001). Cy-tokine gene therapy for myocarditis by in vivo electroporation. Hum.Gene Ther. 12, 1289–1297.
PAYEN, E., BETTAN, M., ROUYER-FESSARD, P., BEUZARD, Y.,and SCHERMAN, D. (2001). Improvement of mouse beta-tha-lassemia by electrotransfer of erythropoietin cDNA. Exp. Hematol.29, 295–300.
PEPPEL, K., CRAWFORD, D., and BEUTLER, B. (1991). A tumornecrosis factor (TNF) receptor-IgG heavy chain chimeric proteinas a bivalent antagonist of TNF activity. J. Exp. Med. 174,1483–1489.
QUATTROCCHI, E., WALMSLEY, M., BROWNE, K., WILLIAMS,R.O., MARINOVA-MUTAFCHIEVA, L., BUURMAN, W., BUT-LER, D.M., and FELDMANN, M. (1999). Paradoxical effects of ad-enovirus-mediated blockade of TNF activity in murine collagen-in-duced arthritis. J. Immunol. 163, 1000–1009.
ROBBINS, P.D., EVANS, C.H., and CHERNAJOVSKY, Y. (2003).Gene therapy for arthritis. Gene Ther. 10, 902–911.
ROLS, M.P., DELTEIL, C., GOLZIO, M., DUMOND, P., CROS,S., and TEISSIE, J. (1998). In vivo electrically mediated proteinand gene transfer in murine melanoma. Nat. Biotechnol. 16,168–171.
SAIDENBERG-KERMANAC’H, N., BESSIS, N., DELEUZE, V.,BLOQUEL, C., BUREAU, M., SCHERMAN, D., and BOISSIER,M.C. (2003). Efficacy of interleukin-10 gene electrotransfer intoskeletal muscle in mice with collagen-induced arthritis. J. Gene Med.5, 164–171.
SOUBRIER, F., CAMERON, B., MANSE, B., SOMARRIBA, S., DU-BERTRET, C., JASLIN, G., JUNG, G., CAER, C.L., DANG, D.,MOUVAULT, J.M., SCHERMAN, D., MAYAUX, J.F., andCROUZET, J. (1999). pCOR: A new design of plasmid vectors fornonviral gene therapy. Gene Ther. 6, 1482–1488.
TAMURA, T., NISHI, T., TAKESHIMA, H., DEV, S.B., USHIO, Y.,and SAKATA, T. (2001). Intratumoral delivery of interleukin 12 ex-pression plasmids with in vivo electroporation is effective for colonand renal cancer. Hum. Gene Ther. 12, 1265–1276.
TRINCHARD-LUGAN, I., HO-NGUYEN, Q., BILHAM, W.M.,BURAGLIO, M., YTHIER, A., and MUNAFO, A. (2001). Safety,pharmacokinetics and pharmacodynamics of recombinant human tu-mour necrosis factor-binding protein-1 (Onercept) injected by intra-venous, intramuscular and subcutaneous routes into healthy volun-teers. Eur. Cytokine Network 12, 391–398.
TRIPATHY, S.K., SVENSSON, E.C., BLACK, H.B., GOLD-WASSER, E., MARGALITH, M., HOBART, P.M., and LEIDEN,J.M. (1996). Long-term expression of erythropoietin in the systemiccirculation of mice after intramuscular injection of a plasmid DNAvector. Proc. Natl. Acad. Sci. U.S.A. 93, 10876–10880.
VILQUIN, J.T., KENNEL, P.F., PATURNEAU-JOUAS, M.,CHAPDELAINE, P., BOISSEL, N., DELAERE, P., TREMBLAY,J.P., SCHERMAN, D., FISZMAN, M.Y., and SCHWARTZ, K. (2001). Electrotransfer of naked DNA in the skeletal muscles of animal models of muscular dystrophies. Gene Ther. 8,1097–1107.
WEINBLATT, M.E., KREMER, J.M., BANKHURST, A.D., BUL-PITT, K.J., FLEISCHMANN, R.M., FOX, R.I., JACKSON, C.G.,LANGE, M., and BURGE, D.J. (1999). A trial of etanercept, a re-combinant tumor necrosis factor receptor:Fc fusion protein, in pa-tients with rheumatoid arthritis receiving methotrexate. N. Engl. J.Med. 340, 253–359.
WEINBLATT, M.E., KEYSTONE, E.C., FURST, D.E., MORE-LAND, L.W., WEISMAN, M.H., BIRBARA, C.A., TEOH, L.A.,
BLOQUEL ET AL.200

FISCHKOFF, S.A., and CHARTASH, E.K. (2003). Adalimumab,a fully human anti-tumor necrosis factor alpha monoclonal anti-body, for the treatment of rheumatoid arthritis in patients takingconcomitant methotrexate: the ARMADA trial. Arthritis Rheum.48, 35–45.
WILLIAMS, R.O., FELDMANN, M., and MAINI, R.N. (1992).Anti-tumor necrosis factor ameliorates joint disease in murine collagen-induced arthritis. Proc. Natl. Acad. Sci. U.S.A. 89,9784–9788.
WILLIAMS, R.O., GHAYEB, J., FELDMANN, M., and MAINI, R.(1995). Successful therapy of collagen-induced arthritis with TNFreceptor-IgG fusion protein and combination with anti-CD4. Immu-nology 84, 433–439.
WOOLEY, P.H., DUTCHER, J., WIDMER, M.B., and GILLIS, S.(1993). Influence of a recombinant human soluble tumor necrosisfactor receptor FC fusion protein on type II collagen-induced arthri-tis in mice. J. Immunol. 151, 6602–6607.
ZHANG, H.G., XIE, J., YANG, P., WANG, Y., XU, L., LIU, D., HSU,H.C., ZHOU, T., EDWARDS, C.K., and MOUNTZ, J.D. (2000).
Adeno-associated virus production of soluble tumor necrosis factorreceptor neutralizes tumor necrosis factor alpha and reduces arthri-tis. Hum. Gene Ther. 11, 2431–2442.
Address reprint requests to:Dr. Daniel Scherman
Unité de Pharmacologie Chimique et GénétiqueUniversité René Descartes
Faculté de Pharmacie4, avenue de l’Observatoire
75270 Paris Cedex 06France
E-mail: [email protected]
Received for publication July 2, 2003; accepted after revisionJanuary 7, 2004.
Published online: January 22, 2004.
GENE THERAPY OF COLLAGEN-INDUCED ARTHRITIS BY ELECTROTRANSFER 201