ERYTHROPOIESIS AND ANAEMIA IN HETEROZYGOUS β-THALASSAEMIA
2
Click here to load reader
-
Upload
phaedon-fessas -
Category
Documents
-
view
218 -
download
3
Transcript of ERYTHROPOIESIS AND ANAEMIA IN HETEROZYGOUS β-THALASSAEMIA

British journal of HaPmutology, 1 98 7, 6 7, 24 5-2 5 3
Correspondence
ERYTHROPOESIS AND ANAEMIA IN HETEKOZYGOIJS lA1,ASSAEMTA
We read with interest the careful study on ‘Erythrokinetics and iron status in heterozygous /3-thalassaemia . . . ’ (British Journal of HaematIogy. 66, 12 3-1 2 7. 198 7). Kevising pre- vious views (Weatherall & Clegg. 198 1) Pippard & Wainscoat found only a minor degree of ineffective erythropoiesis insufficient to account for the anaemia of the carriers of the trait. Therefore the authors raise again the old question ‘why there is little or no increase in erythropoiesis to compensate for the mild anaemia’ of hetcrozygous /3-thalassaemia. An increase of the value of Pso could explain this phenomenon; but no change was detected, ‘which might have accounted for any lack of increased stimulus for erythropoiesis’; in support of this finding they cite one single study (Pearson e f
We would like to bring to your attention that all other studies, prior or subsequent to the paper of Pearson et al, unanimously report a n increase of the P511 relative to normal controls; the essencc of these reports has been concentrated in Table I. Although the differences of P jo vary from 1.2 up to 3.1 mmHg, they are all in the same direction and within the range expected for the degree of anaemia or even higher. Even Pearson et al report a small increase; their study, however, can be criticized for failing to provide their own normal controls. Pippard & Wainscoat do not mention number, sex and haemoglobin level of their controls for P jO: a few such omissions may be noted in some of the other reports which, however, rover a total of 92 patients and 135 controls.
Calculations based on our own data have shown that the shift of the dissociation curve to the right is sufficient to compensate for the mild haemoglobin deficit of the heterozy- gotes, which cannot be considered as truly anaemic, at least at rest; there is no anoxic stimulus and no need for further
ul. 1977).
Table 1.
intensification of erythropoiesis (Fessas & Tassiopoulos, 1983). The fresh erythrokinetic data of Pippard & Wainscoat do not contradict this hypothesis. Of course there is more evidence that 8-thalassaemia heterozygotes are capable of increasing their erythropoiesis when necessary, as for instance in the association of fi-thalassaemia with high-O2- affinity /3-chain variants.
Pippard & Wainscoat state: ‘its seems conceivable that the increased number of small red cells might increase the efficiency of oxygen delivery to the tissues . . . etc.’. Apart from anaemic and nori-anaemic P-thalassaemia heterozy- gotes (Tassiopoulos ef al, 1982). our studies on microcytosis of different aetiology, such as non-anaemic iron deficiency of phlebotomized polycythaemia Vera (Tassiopoulos et d, 1983) and childhood anaemia (Tassiopoulos et al, 1987), indicate that microcytes may indeed improve oxygen delivery because of the associated increase of the 2,3-DPG/Hb ratio: erythro- cytes born smaller than normal tend to maintain the 2,3-DPG content of normocytes. Unpublished data from our labora- tory suggest that in P-thalassaemia heterozygotes this effect is obtained through an increased glycolytic rate. Of course, we do not exclude a priori the possibility that microcytosis may work through yet other mechanisms, for instance by creating different rheological conditions at the site of the ‘anoxia sensors‘.
Irrespective to such hypotheses, the discrepancies concern- ing PjO. between the study of Pippard & Wainscoat and all other reports, need to be explained.
First Department of lnternal Medicine. THOMAS TASSIOPOIJLOS University of Athens, ‘Laiko’ General Hospital, 17 Aghiou Thoma, Athens 11 5 27, Greece
PHAEDON FFSSAS
Controls ~~
Keferencc* Sex n Hb (g/dl) P5f1
Fiorelli P t a/ . 1973 MF 26 14.4&0.23 25.9fO.14
~~ ~~
de Furia et al. 1974 MF 9 - 26.4 Ricci et al, 1982 hfF 20 13 .6 f1 .5 25.8 Tassiopoulosetal, 19x2 M I h 15.7f1 .47 26.3+0.66
F 16 13 .3 f0 .73 27.0It0.48 Alvarez-Sala et al, 1983 lilF 48 - 26.4+ 1.4
16 11 .010 .52 27.1 &0.25 1.2 <0,001 7 - 29.5 3.1
30 12.4&1.4 27.1 1.3 <0.05 18 12.811.0 28 .4 f1 .52 2.1 < 0 . 0 0 7 19 1 1 . 0 r l . 0 29-211.35 2.2 <0.001 12 - 27-9 f2 .5 1.5 <0.01
* All values represent m + 1 SD exept for the study of Fiorelli et a1 which provides m f S E As provided by the authors .
245

246 Correspondence
REFERENCES
Alvarex-Sala, J.L., Villegas. A., Alarccin. C. & Espinos. D. (1983) Intraerythrocytic adaptation to anaemia in thalassaemia. Nuuvelle Revue Frunpise d'Hemuiulugiu, 25, 267-2658.
Fessas. Ph. & Tassiopoulos, Th. (1983) On the 'anaemia' of heterozygous thalassaemia and on the possible relation of micro- cytosis to haemoglobin concentration. Biomedica Biuchimica Acta.
Fiorelli, C., Gerli. G.C.. Bernasconi. C.. Bianchi, C. 8: Matuonto, V. (1 97 3 ) L'afinita dell'emoglobina per I'ossigeno in sindromi talasse- niiche: Interaxione tra 2,3-difosfoglicerato ed emoglobina fetale. Att i Vu Congressu Sulk Micrucitemie, pp. 145-1 54. Edit. Inst. Ital. di Medicina Sociale.
de Furia. F.G.. Miller, D.R. & Canale, V.C. (1974) Red blood cell metabolism and function in transfused P-thalassemia. Annals ufthe New York Academy of Sciences, 232, 323-332.
Pearson. HA. . Motoyama. E., Genel. M.. Kramer. M. & Zigas, C.J. (1 977) Intraerythrocytic adaptation (2,3-DPG,P50) in thalasse- mia minor. Blood, 49, 463465 .
42,258-262.
Ricci. G.. Castaldi. G., Zavagli. (2.. Lupi, G., Turati, A. & Rezzi, T. (1982) Red cell 2.3-diphosphoglycerate contents and oxygen affinity in heterozygous beta-thalassaemia. Acta Haemato~ogicu.
Tassiopoulos, Th.. Kaltsoya-Tassiopoulos. A.. Alchanati, N.. Rom- bos, J., Rournaras. N. & Fessas, Ph. (1982) Anemie, 2,3-DPG et oxygenation tissulaire chez les hetkozygotes de P-thalassemie. Nuuvelle Revue Franpise d'Himatulogir, 24, 359-362.
Tassiopoulos, Th., Fessas, Ph., Pangalis, G., Andreopoulos. A. & Loukopoulos, D. (1983) Volume des erythrocytes et concentration en 2.3-DPG. Etude sur le modkle de la polyglobulie primitivc. Nouvelle Revue Frunquise d'Himatologie, 25, 263-266.
Tassiopoulos, Th., Stamatelos, G., Filippidou, E., Filippidis, F., Laoutaris. N. & Fessas, Ph. (1987) The anemia of childhood revisited. Blut, 54, 147-1 52.
Weatherall, D.J. & Clegg, J.B. (198 1) The Thulassuemiu Syndromes, 3rd edn. p. 240. Blackwell Scientific Publications, Oxford.
68, 63-64.
AGGRESSIVE CHEMOTHERAPY IN THE TREATMENT OF SUBACUTE MYELOMONOCYTIC TXUKAEMIA WITH SKIN INFILTRATION
In a recent paper Fenaux et al (1987) reported 60 cases of chronic (CMML) and subacute (SMML) myelomonocytic leukaemia. Media survival of the CMML subjects was 49 months but for the SMML subjects was 8 . 5 months. At diagnosis the mean percentage of blast cells in the marrow was 6.8% in CMML and 15.5% in SMML. The mean haemoglobin levels were 10.6 g/dl in CMML and 7.0 g/dl in SMML arid the mean blood monocytoid cells were 3.6 x 10y/l in CMML and 7.6 x 1OY/1 in SMML. Duguin et al (1983) reported four cases of CMML who during the course of the disease developed skin infiltration by monocytoid cells. At the appearance of skin lesions the disease evolved rapidly and all
Table I. Clinical and laboratory features at the onset of leukaemia
Peripheral blood Hb (g/W WBC ( x 1OY/1)
Monocytoid cells (%) Blasts (%) Platelets ( x loy/l) Bone marrow
Blasts (%) Monocytoid cclls (%)
Hepatomegaly Splenomegaly Lymphadenopathy Run (S.I. units) Creatinine (S.I. units)
Case 1 Case 2 Case 3
8.9 59.9 67 1 1
112
30 50
2 cm 1 cm -
13.209 25752
6 .6 17.2 45 2 5 90
35 27 2 cm -
16.065 256.36
6 . 5 65.4 7 0 10
140
40 40
12.852 229.84
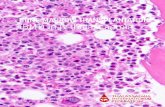
Fig 1. Skin biopsy (case 1 ) (haematoxylin and eosin x 200).