Effective Treatment with Interferon-α in Chronic Recurrent Multifocal Osteomyelitis
2
JOURNAL OF INTERFERON AND CYTOKINE RESEARCH 15:837-838 (1995) Mary Ann Liebert, Inc. CASE REPORT Effective Treatment with Interferon-a in Chronic Recurrent Multifocal Osteomyelitis RUNE ANDERSSON ABSTRACT Chronic recurrent multifocal osteomyelitis (CRMO) is a rare disease of unknown etiology characterized by multiple osteomyelitic changes in the predominantly metaphysial regions of long bones.'1-2' It was first de- scribed by Giedon et al. in 1972.'" Cultures for all known microorganisms are negative. Pain is the most com- mon symptom, and sometimes soft tissue swelling is present. Patients are usually treated with nonsteroidal antiinflammatory drugs (NSAIDs) or corticosteroids(4> and respond, at least partly, to these treatments. CRMO is most commonly seen in children and is in the majority of cases self-limiting but has a protracted course of several years. Some patients have a more prolonged disease period, as in the patient reported here. Treatment with corticosteroids in children has the risk of causing growth retardation as a potential adverse effect, and alternative treatments are of great interest. In the actual paper, a successful treatment with interferon-a2b in a 34-year-old man with CRMO is presented. CASE REPORT A boy was referred to the hospital with an osteomyelitic le- sion in the right tibia at the age of 14 years. Repeated cultures were negative. Biopsy of the affected bone showed a periostal reaction and a chronic inflammation in the bone marrow with lymphocytes and some giant cells. There were no signs of spe- cific infection or malignancy. Treatment with flucloxacillin and tuberculostatic therapy were without effect. The disease pro- gressed with osteomyelytic lesions in both femoral bones. He later suffered from severe pain, sometimes disturbing his sleep. Radiograms of the femoral bones and right tibia are shown in Fig. 1, demonstrating osteomyelitic changes with periostal re- actions and formation of new bone between tibia and fibula. He has been treated with 12.5-20 mg prednisolone and 3-6 g acetylsalicylic acid daily, with incomplete pain relief. The pa- tient noted for several years that he had less pain when he had a cold and told me that "it would have been better to have a cold all the time!" This made me think of treatment with in- terferon (IFN). When he was 34 years old he started with in- terferon-a2b (Introna; Schering-Plough), 3 MU subcutaneously three times per week, in September 1992. He responded well to the treatment, and it was possible to decrease the pred- nisolone dose gradually and stop it after 7 weeks. It was pos- sible to reduce the acetylsalicylic acid to about 1 g in the af- ternoon the 3 days of the week he injected himself with the Department of Infectious Diseases, Ostra Hospital, Göteborg, Sweden. interferon. The acetylsalicylic acid prevented his chills and the increased tiredness he experienced a few hours after the injec- tions. A scintigraph of the osteomyelitic lesions in the legs after 10 months of IFN-ot treatment showed decreased activity. Radio- graphs of the legs after 1 year of treatment did not show any difference from pretreatment x-rays. Erythrocyte sedimentation rate and C-reactive protein were in the normal range before, during, and after treatment with IFN-a. The most important side effect was a moderate tiredness, which the patient preferred compared with the previous pain. IFN therapy was stopped after 1 year; the patient had a re- lapse of the CRMO with pain after about 1 week and had to restart the prednisolone treatment and gradually increase it to 15 mg daily and acetylsalicylic acid to 6 g daily. Despite the treatment with prednisolone and acetylsalicylic acid, he again had severe pain periods every day and difficulties in sleeping. A scintigraph 2 months after withdrawing the IFN-a treatment showed a marked increase in the activity in the osteomyelitic lesions. He restarted the IFN-a treatment 2 months and 9 days after stopping the previous treatment, and with the same dosage he responded again and was completely free from pain the same day the IFN therapy was initiated. It was again possible to stop the prednisolone treatment and reduce the acetylsalicylic acid to 1 g after each IFN-a injection. It has until now been possi- ble to reduce the dosage to 0.5 MU IFN-a three times per week. 837
Transcript of Effective Treatment with Interferon-α in Chronic Recurrent Multifocal Osteomyelitis

JOURNAL OF INTERFERON AND CYTOKINE RESEARCH 15:837-838 (1995)Mary Ann Liebert, Inc. CASE REPORT
Effective Treatment with Interferon-a in Chronic RecurrentMultifocal Osteomyelitis
RUNE ANDERSSON
ABSTRACT
Chronic recurrent multifocal osteomyelitis (CRMO) is a rare disease of unknown etiology characterized bymultiple osteomyelitic changes in the predominantly metaphysial regions of long bones.'1-2' It was first de-scribed by Giedon et al. in 1972.'" Cultures for all known microorganisms are negative. Pain is the most com-mon symptom, and sometimes soft tissue swelling is present. Patients are usually treated with nonsteroidalantiinflammatory drugs (NSAIDs) or corticosteroids(4> and respond, at least partly, to these treatments. CRMOis most commonly seen in children and is in the majority of cases self-limiting but has a protracted course ofseveral years. Some patients have a more prolonged disease period, as in the patient reported here. Treatmentwith corticosteroids in children has the risk of causing growth retardation as a potential adverse effect, andalternative treatments are of great interest. In the actual paper, a successful treatment with interferon-a2b ina 34-year-old man with CRMO is presented.
CASE REPORT
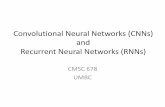
A boy was referred to the hospital with an osteomyelitic le-sion in the right tibia at the age of 14 years. Repeated cultureswere negative. Biopsy of the affected bone showed a periostalreaction and a chronic inflammation in the bone marrow withlymphocytes and some giant cells. There were no signs of spe-cific infection or malignancy. Treatment with flucloxacillin andtuberculostatic therapy were without effect. The disease pro-gressed with osteomyelytic lesions in both femoral bones. Helater suffered from severe pain, sometimes disturbing his sleep.Radiograms of the femoral bones and right tibia are shown inFig. 1, demonstrating osteomyelitic changes with periostal re-actions and formation of new bone between tibia and fibula.
He has been treated with 12.5-20 mg prednisolone and 3-6g acetylsalicylic acid daily, with incomplete pain relief. The pa-tient noted for several years that he had less pain when he hada cold and told me that "it would have been better to have a
cold all the time!" This made me think of treatment with in-terferon (IFN). When he was 34 years old he started with in-terferon-a2b (Introna; Schering-Plough), 3 MU subcutaneouslythree times per week, in September 1992. He responded wellto the treatment, and it was possible to decrease the pred-nisolone dose gradually and stop it after 7 weeks. It was pos-sible to reduce the acetylsalicylic acid to about 1 g in the af-ternoon the 3 days of the week he injected himself with the
Department of Infectious Diseases, Ostra Hospital, Göteborg, Sweden.
interferon. The acetylsalicylic acid prevented his chills and theincreased tiredness he experienced a few hours after the injec-tions.A scintigraph of the osteomyelitic lesions in the legs after 10
months of IFN-ot treatment showed decreased activity. Radio-graphs of the legs after 1 year of treatment did not show anydifference from pretreatment x-rays. Erythrocyte sedimentationrate and C-reactive protein were in the normal range before,during, and after treatment with IFN-a. The most important sideeffect was a moderate tiredness, which the patient preferredcompared with the previous pain.IFN therapy was stopped after 1 year; the patient had a re-
lapse of the CRMO with pain after about 1 week and had torestart the prednisolone treatment and gradually increase it to15 mg daily and acetylsalicylic acid to 6 g daily. Despite thetreatment with prednisolone and acetylsalicylic acid, he againhad severe pain periods every day and difficulties in sleeping.A scintigraph 2 months after withdrawing the IFN-a treatmentshowed a marked increase in the activity in the osteomyeliticlesions. He restarted the IFN-a treatment 2 months and 9 daysafter stopping the previous treatment, and with the same dosagehe responded again and was completely free from pain the same
day the IFN therapy was initiated. It was again possible to stopthe prednisolone treatment and reduce the acetylsalicylic acidto 1 g after each IFN-a injection. It has until now been possi-ble to reduce the dosage to 0.5 MU IFN-a three times per week.
837

838 ANDERSSON
abcFIG. 1. Radiograms of both femoral bones and the right lower leg before the start of IFN-a treatment in a 34-year-old man.The patient has suffered from CRMO from the age of 14 years, (a) Left femoral bone, (b) Right femoral bone, (c) Right lowerleg.
When we tried to reduce the dose to 0.5 MU two times perweek, the patient had a relapse of bone pain.
Because the disease mainly affects children and corticos-teroids cause retardation of growth, it will be of great interestto evaluate in a controlled trial IFN-a treatment in patients notresponding to acetylsalicylic acid or NSAIDs.
3. GIEDION, A., HOLTHUSEN, W., MASEL, L.F., and VISCHER,D. (1972). Subacute and chronic "symmetrical" osteomyelitis. Ann.Radiol. 15, 329-342.
4. STANTON, R.P., LOPEZ-SOSA, F.H., and DOIDGE, R. (1993).Chronic recurrent multifocal osteomyelitis. Orthop. Rev. 22, 229-233.
REFERENCES
1. BJÖRKSTEN, B., and BOQUIST, L. (1980). Histopathological as-pects of chronic recurrent multifocal osteomyelitis. J. Bone JointSurg. [Br] 62, 376-380.
2. SOLHEIM, L.F., PAUS, B., LIVERUD, K, and ST0EN, É. (1980).Chronic recurrent multifocal osteomyelitis. A new clinical-radio-logical syndrome. Acta Orthop. Scand. 51, 37-41.
Address reprint requests to:Dr. Rune Andersson
Department of Infectious DiseasesÖstra University Hospital
S-416 85 Göteborg, Sweden
Received 14 December 1994/Accepted 12 June 1995