EXPERTから学ぶTLA(Tumescent Local Anesthesia) 皮膚切開 「希釈麻酔液法」 生理的食塩水500-80ml=420mlとし リドカイン(キシロカイン) 40ml

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 94 Thai Journal of Anesthesiology 95Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
°“√„À⬓√–ß—∫§«“¡√Ÿâ÷°„πºŸâªÉ«¬∑’Ë¡’‰¢—πÀ≈—ß∫“¥‡®Á∫
‡√◊Õß√Õß ‰∑¬ÿ¡‘µ√ æ.∫.,*
¿—≥±‘≈“ √ÿ®‘‚√®πå®‘π¥“°ÿ≈ æ.∫., ««. *
*¿“§«‘™“«‘—≠≠’«‘∑¬“ §≥–·æ∑¬»“µ√å ¡À“«‘∑¬“≈—¬ß¢≈“π§√‘π∑√å ®.ߢ≈“ 90110
Table 1 American Spinal Injury Association Impairment Scale (ASIA)1,4
Grade Category Description
A Complete No sensory or motor function is preserved in the sacral segments S4-S5 B Incomplete Sensory but not motor function is preserved below the neurologic level and extends through the sacral segments S4-S5 C Incomplete Motor function is preserved below the neurologic level, and the majority of key muscles below the neurologic level have a muscle grade < 3 D Incomplete Motor function is preserved below the neurologic level, and the majority of key muscles below the neurologic level have a muscle grade ≥ 3 E Normal Sensory or motor function are normal
°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß¡—°∑”„À⇰‘¥°“√æ‘°“√Õ¬à“ß
∂“«√ ∑”„ÀâµâÕߟ≠‡’¬∑√—欓°√·≈–§à“„™â®à“¬®”π«π¡“°„π
°“√¥Ÿ·≈√—°…“ °“√¥Ÿ·≈ºŸâªÉ«¬∑’Ë∂Ÿ°µâÕß®”‡ªìπµâÕ߇¢â“„®æ¬“∏‘
√’√«‘∑¬“ (pathophysiology) ¢Õß°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß
´÷Ëß“¡“√∂≈¥Õÿ∫—µ‘°“√≥å°“√µ“¬‰¥â∂÷ß√âÕ¬≈– 5-7 „πªï·√°
·≈–≈¥°“√‡°‘¥¿“«–·∑√°´âÕπµà“ß Ê ‰¥â1, 2
Õÿ∫—µ‘°“√≥å „π·µà≈–ªï∑—Ë«‚≈°æ∫ª√–¡“≥ 28-55 §πµàÕª√–™“°√
≈â“π§π ¡’ºŸâªÉ«¬„À¡à‡°‘¥¢÷Èπ 10,000 √“¬„π∑ÿ° Ê ªï æ∫¡“°
ÿ¥„π°≈ÿà¡Õ“¬ÿ 15-25 ªï ‚¥¬æ∫∂÷ß√âÕ¬≈– 45 ·≈–—¥à«π
‡æ»™“¬µàÕ‡æ»À≠‘߇∑à“°—∫ 4 µàÕ 1
“‡Àµÿ à«π„À≠à‡°‘¥®“°Õÿ∫—µ‘‡Àµÿ∑“ß√∂¬πµå (√âÕ¬≈– 36-
48) √Õß≈ß¡“§◊Õµ°®“°∑’ËŸß (√âÕ¬≈– 17-21) ∂Ÿ°∑”√⓬
√à“ß°“¬ (√âÕ¬≈– 5-29) ·≈–®“°“‡ÀµÿÕ◊Ëπ Ê ‡™àπ Õÿ∫—µ‘‡Àµÿ
®“°°“√‡≈àπ°’Ó ·≈–°“√ª√–°Õ∫Õ“™’æ1 ‚¥¬°√–¥Ÿ°—πÀ≈—ß
à«π§Õ∑’Ë 4 ∂÷ß 7 (C4-C7) ‰¥â√—∫∫“¥‡®Á∫∫àÕ¬ÿ¥ °√–¥Ÿ°-
—πÀ≈—ßà«π‡Õ«·≈–à«πÕ°‡°‘¥‰¥âπâÕ¬°«à“‡æ√“–¡’°√–¥Ÿ°´’Ë‚§√ß
·≈–°≈â“¡‡π◊ÈÕ intercostal ™à«¬ª√–§—∫ª√–§Õß3
™π‘¥¢Õß°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß American Spinal Injury Association (ASIA)1,4
®”·π°™π‘¥°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ßÕÕ°‡ªìπ 2 ·∫∫ §◊Õ
1. ·∫àßµ“¡§«“¡√ÿπ·√ߢÕß°“√Ÿ≠‡’¬∑“ß√–∫∫
ª√–“∑ (severity of neurological deficits) ¥—ßµ“√“ß∑’Ë 1
2. ·∫àßµ“¡Õ“°“√·¥ß (clinical syndrome) ÕÕ°
‡ªìπ 2 ™π‘¥ §◊Õ
∫∑§«“¡øóôπ«‘™“
Thai J Anesthesiology 2006 ; 32(2) : 94-101.
94

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 94 Thai Journal of Anesthesiology 95Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
2.1 °“√∫“¥‡®Á∫‰¢—πÀ≈—ßÕ¬à“ß¡∫√Ÿ≥å (com-
plete spinal cord injury) ¡’°“√Ÿ≠‡’¬∑—Èß motor ·≈– sen-
sory √–¥—∫∑’˵˔°«à“√–¥—∫∑’ˉ¥â√—∫°“√∫“¥‡®Á∫≈ß¡“∑—ÈßÀ¡¥
2.2 °“√∫“¥‡®Á∫‰¢—πÀ≈—ßÕ¬à“߉¡à¡∫√Ÿ≥å (in-
complete spinal cord injury) ¡’Õ“°“√‰¥âÀ≈“¬√Ÿª·∫∫‡™àπ
central cord syndrome, Brown-sequard syndrome ·≈–
cauda equina lesions ‡ªìπµâπ
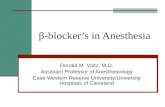
°≈‰°°“√‡°‘¥°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß Denis ·≈–§≥–5 ·∫àßµ“¡‚§√ß√â“ߢÕß vertebral
column ÕÕ°‡ªìπ 3 column §◊Õ anterior, middle ·≈– pos-
terior ‡√’¬°«à“ three column concept ¥—ß√Ÿª∑’Ë 1 ´÷Ëß“¡“√∂
∫Õ°°≈‰°°“√∫“¥‡®Á∫‰¥â ‡™àπ extension injury ∑”„À⇰‘¥
°“√·µ°À—°¢Õß anterior column (√Ÿª∑’Ë 1a), flexion injury
∑”„À⇰‘¥°“√·µ°À—°¢Õß posterior column (√Ÿª∑’Ë 1c) ´÷Ëß
∂â“¡’°“√·µ°À—°¡“°°«à“ 2 column ¢÷Èπ‰ª°Á®–∑”„Àâ°√–¥Ÿ°-
—πÀ≈—߉¡à¡—Ëπ§ß (instability) ‡°‘¥°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß
„π‡¥Á°‡≈Á°®π∂÷ßÕ“¬ÿ 10 ªï °√–¥Ÿ°—πÀ≈—߬—߇µ‘∫‚µ‰¡à
‡µÁ¡∑’Ë·≈– ligament ¬—߉¡à·¢Áß·√ß ‡°‘¥°“√‡§≈◊ËÕπ∑’Ë¢Õß
°√–¥Ÿ°—πÀ≈—߉¥âßà“¬ æ∫Õÿ∫—µ‘°“√≥凰‘¥°“√∫“¥‡®Á∫¢Õß
‰¢—πÀ≈—ß ‚¥¬‰¡àæ∫§«“¡º‘¥ª°µ‘¢Õß¿“æ∂à“¬√—ß’ ‡√’¬°«à“
SCIWORA (spinal cord injury without radiographic ab-
normality) ‡æ‘Ë¡¢÷Èπ ´÷ËßÕ“®∑”„Àâ«‘π‘®©—¬º‘¥æ≈“¥‰¥â πÕ°
®“°π’È°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ßÕ“®‡°‘¥®“°“‡ÀµÿÕ◊Ëπ Ê ∑’ˉ¡à
‰¥â‡°‘¥®“°Õÿ∫—µ‘‡Àµÿ‡™àπ ‚√§∑’ˇªìπ¡“·µà°”‡π‘¥ °“√Õ—°‡∫
µ‘¥‡™◊ÈÕ ‡π◊ÈÕßÕ° ‡ªìπµâπ
欓∏‘√’√«‘∑¬“¢Õß°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß °“√∫“¥‡®Á∫ª∞¡¿Ÿ¡‘ (primary injury) ‡°‘¥‡¡◊ËÕ¡’·√ß
°√–·∑°À√◊Õ°¥∑’ˉ¢—πÀ≈—ß‚¥¬µ√ß∑”„Àâ¡’‡≈◊Õ¥ÕÕ°¿“¬„π
‰¢—πÀ≈—ß ‡°‘¥°“√Ÿ≠‡’¬ autoregulation ·≈–‡´≈≈å∫«¡
∑”„À⧫“¡¥—π„π™àÕß°√–¥Ÿ°—πÀ≈—߇æ‘Ë¡ º≈§◊Õ ‰¢—πÀ≈—ß
¢“¥‡≈◊Õ¥ ‡°‘¥°“√°√–µÿâπ∑“ß™’«‡§¡’ (biochemical) ´÷Ë߇ªìπ
®ÿ¥‡√‘Ë¡µâπ¢Õß°“√∫“¥‡®Á∫∑ÿµ‘¬¿Ÿ¡‘ (secondary injury) À“°
‡°‘¥°“√∫“¥‡®Á∫∑ÿµ‘¬¿Ÿ¡‘®–¡’°“√Ÿ≠‡’¬°“√∑”ß“π¢Õ߉¢—π-
À≈—ßÕ¬à“ß∂“«√‡æ√“–‡°‘¥°“√µ“¬¢Õ߇π◊ÈÕ‡¬◊ËÕ‰¢—πÀ≈—ß®“°
°“√¢“¥‡≈◊Õ¥ ´÷Ë߇°‘¥‰¥âµ—Èß·µàπ“∑’·√°À√◊ÕÀ≈“¬™—Ë«‚¡ßÀ≈—ß
°“√∫“¥‡®Á∫ª∞¡¿Ÿ¡‘
®“°°≈‰°°“√‡°‘¥°“√∫“¥‡®Á∫∑ÿµ‘¬¿Ÿ¡‘¥—ß°≈à“« ¡’°“√
»÷°…“°“√„™â¬“‡æ◊ËÕ≈¥Õ“°“√º‘¥ª°µ‘∑“ß√–∫∫ª√–“∑ ´÷Ëß
‡°‘¥ª√–‘∑∏‘¿“楒‡¡◊ËÕ„Àâ∑—π∑’À≈—ß°“√∫“¥‡®Á∫ ‚¥¬‡©æ“–
¿“¬„π 8 ™¡. ¬“‡À≈à“π’ȉ¥â·°à naloxone, thyrotropin
releasing hormone, calcium channel blockers, NMDA
receptor antagonist ·≈– corticosteroids ·µàæ∫«à“¡’‡æ’¬ß
steroids „π¢π“¥Ÿßµ—«‡¥’¬«‡∑à“π—Èπ∑’Ë¡’ª√–‘∑∏‘¿“楒 ®“°
°“√»÷°…“„πÀ≈“¬∂“∫—π°≈à“««à“°“√©’¥ methylpredniso-
lone 30 ¡°./°°. ∑“߇âπ‡≈◊Õ¥¥”·≈â«À¬¥µàÕ„π¢π“¥ 5.4
¡°./°°./™¡. „π 23 ™¡.µàÕ¡“6 “¡“√∂∑”„Àâ°“√∑”ß“π
¢Õß√–∫∫ª√–“∑ sensory ·≈– motor ∑’Ë 6 —ª¥“Àå·≈–
6 ‡¥◊ÕπÀ≈—ßºà“µ—¥¥’¢÷Èπ5,7-9
º≈¢Õß°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß (Systemic effects of spinal cord injury)3, 4,10-12
¡’º≈µàÕ∑ÿ°√–∫∫¢Õß√à“ß°“¬‚¥¬‡©æ“–√–∫∫‰À≈‡«’¬π
‡≈◊Õ¥·≈–√–∫∫À“¬„® “¡“√∂√ÿª‰¥â¥—ßµ“√“ß∑’Ë 2
Autonomic hyperreflexia (mass reflex)3,10,13
‡°‘¥‰¥âÀ≈—ßøóôπ®“° spinal shock ´÷ËßÕ“®Õ¬Ÿàπ“πÀ≈“¬
«—πÀ√◊ÕÀ≈“¬—ª¥“Àå ‚¥¬™à«ß∑’ˇ°‘¥ spinal shock ∑—Èß sym-
pathetic ·≈– parasympathetic ®–À¬ÿ¥∑”ß“π À≈—ß®“°π—Èπ
°“√∑”ß“π®–°≈—∫¡“Õ¬à“ß√«¥‡√Á«·≈– sympathetic ∫√‘‡«≥∑’Ë
µË”°«à“°“√∫“¥‡®Á∫®–∑”ß“π·¬°ÕÕ°¡“¥â«¬µ—«‡Õ߉¡à¢÷Èπ°—∫
¡Õßà«π brain stem ·≈– hypothalamus ‡°‘¥°“√Ÿ≠‡’¬
Figure 1 Three column concept5 a anterior column injury b : middle column injury c : posterior column injury SSL : supraspinous ligament, PLL : pos- terior longitudinal liga mnet, ALL : anterior longitudinal ligament

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 96 Thai Journal of Anesthesiology 97Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
Table 2 The systemic effects following spinal cord injury 3,4, 11-13
1) Cardiovascular system • Initial sympathetic stimulation with increase in blood pressure • Followed by onset of spinal shock with Loss of sympathetic tone Decrease in systemic vascular resistance Increase in venous capacitance and pooling Resultant profound hypotension Bradycardia and decrease ventricular function in lesion above T5
• Autonomic reflexia in chronic stage with lesion above T7
2) Respiratory system • Total diaphragmatic paralysis and apnea in lesion above C4
• Variable loss of intercostals and abdominal functions in lesion below C5
• Decrease in functional residual capacity, forced vital capacity, maximal inspiratory and expiratory pressure • Hypoventilation with hypercapnia and hypoxia • Neurogenic pulmonary edema may occur • Pneumonia from atelectasis and impaired cough3) Gastrointestinal system • Paralytic ileus, delayed gastric emptying time, neurogenic megacolon • Fecal incontinence, flaccid anal sphincter and loss of anal reflex in lesion at conus medullaris and cauda equina4) Genitourinary system • Urinary incontinence, incomplete voiding, vesicoureteric reflux and chronic renal infection5) Musculoskeletal system • Contracture of joint, osteoporosis, muscular atrophy and involuntary skeletal muscle spasm • Pressure necrosis of the skin below level of the spinal transaction • Secondary osteomyelitis at the site of the ulcers 6) Thermal regulation • Poikilothermic below level of the spinal transaction7) Psychological status • Severe depression and emotional instability
sympathetic integration °“√∑”ß“π∑’ˇ°‘¥¢÷Èπ®÷ߥŸ‡À¡◊Õπ‡ªìπ
reflex ´÷Ëß∂Ÿ°°√–µÿâπ‰¥âßà“¬ ¢“¥°“√µÕ∫πÕ߇©æ“–∑’Ë
(local response) ·≈–ªØ‘°‘√‘¬“°«â“ߢ«“ß (widespread reac-
tion) ‡√’¬°«à“ mass reflex ‚¥¬ª√–¡“≥√âÕ¬≈– 85 ¢Õß
ºŸâ∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ߟ߰«à“°√–¥Ÿ°—πÀ≈—ß√–¥—∫Õ°∑’Ë 5 ®–
‡°‘¥ª√“°Ø°“√≥åπ’ȉ¥â ‡æ√“– main splanchnic outflow Õ¬Ÿà
√–À«à“ß°√–¥Ÿ°—πÀ≈—ß√–¥—∫Õ°∑’Ë 5 ∂÷ß°√–¥Ÿ°‡Õ«∑’Ë 2 ·µà∂â“
°“√∫“¥‡®Á∫Õ¬ŸàµË”°«à“°√–¥Ÿ°—πÀ≈—ß√–¥—∫Õ°∑’Ë 10 °Á®–‡°‘¥
‰¥âπâÕ¬≈ß °“√„™â¬“™“‡©æ“–∑’Ë (topical anesthesia) Õ“®‰¡à
‡æ’¬ßæÕ„π°“√ªÑÕß°—π¿“«–π’È ·µà general anesthesia ∑’Ë¡’
§«“¡≈÷°‡æ’¬ßæÕÀ√◊Õ regional anesthesia “¡“√∂ªÑÕß°—π
¿“«–¥—ß°≈à“«‰¥â
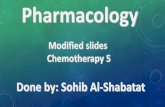
°≈‰°°“√‡°‘¥ autonomic hyperreflexia ·¥ß¥—ß
√Ÿª∑’Ë 2

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 96 Thai Journal of Anesthesiology 97Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
°“√¥Ÿ·≈√–¬–·√° (Early supportive care)3,5
°“√√—°…“„ÀâªØ‘∫—µ‘µ“¡·π«∑“ߢÕß Advanced trau-
ma life support (ATLS) ·≈–ªÑÕß°—πÕ¬à“„À⇰‘¥¿“«–ÕÕ°-
´‘‡®π„π‡≈◊Õ¥µË”‡æ√“–®–∑”„Àâ°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß
·¬à≈ß ¥—ßπ—Èπ§«√„ÀâÕÕ°´‘‡®π„πºŸâªÉ«¬∑’Ë¡’‰¢—πÀ≈—ß∫“¥‡®Á∫
∑ÿ°√“¬
‡ªÑ“À¡“¬¢Õß°“√√—°…“ (The goal of treatment of spinal cord injury)5
1. ªÑÕß°—π‰¢—πÀ≈—߉¡à„À⇰‘¥§«“¡‡’¬À“¬µàÕ‡π◊ËÕß
(Protection of the spinal cord from further damage)
2. °√≥’∑’Ë¡’°“√∫“¥‡®Á∫‰¢—πÀ≈—ßÕ¬à“߉¡à¡∫√Ÿ≥å
欓¬“¡‰¡à„Àâ·π«‰¢—πÀ≈—߇§≈◊ËÕπ‡æ◊ËÕ„À⇰‘¥°“√øóôπµ—«¡“°
∑’Ëÿ¥ (Maintenance of spinal alignment to allow maxi-
mal recovery in incomplete lesions)
3. 欓¬“¡®—¥„Àâ°√–¥Ÿ°—πÀ≈—ßÕ¬Ÿà„π¿“æ§ßµ—«‡æ◊ËÕ
„Àâ°≈—∫Ÿà¿“懥‘¡ (Establishment of stability to allow
rehabilitation)
°“√¥Ÿ·≈∑“߇¥‘πÀ“¬„®„π√–¬–·√° (Management of airway in acute phase) °“√„à∑àՙ૬À“¬„®µâÕß„™â«‘∏’∑’ˉ¡à∑”„À≢—πÀ≈—ß
∫“¥‡®Á∫‡æ‘Ë¡¢÷Èπ ®–‡≈◊Õ°«‘∏’„¥¢÷Èπ°—∫¿“溟âªÉ«¬ √–¥—∫§«“¡
√Ÿâ÷°µ—« (level of co-operation) ·≈–§«“¡™”π“≠¢Õß«‘—≠≠’
´÷Ëß¡’¢âÕ·π–π” ¥—ßπ’È15,16
1. °√≥’‰¡à‡√àߥà«π (elective) ‰¡à¡’¿“«–¢“¥ÕÕ°´‘‡®π
·≈–¿“«–§“√å∫Õπ‰¥ÕÕ°‰´¥å§—Ëß æ‘®“√≥“∂à“¬¿“æ√—ß’¢Õß
°√–¥Ÿ°µâπ§Õ¥â“π¢â“ß (lateral cervical spine) °àÕπ‡æ√“–°“√
‡ÀÁπ¿“æ√—ß’µ—Èß·µà∫√‘‡«≥°√–¥Ÿ°µâπ§Õ∑’Ë 1 ∂÷ß°√–¥Ÿ°∑√«ßÕ°
∑’Ë 1 ®–™à«¬≈¥§«“¡º‘¥æ≈“¥„π°“√«‘π‘®©—¬·≈–∫Õ°§«“¡º‘¥
ª°µ‘‰¥â√âÕ¬≈– 70-8317,18 ·≈–·π–π”„Àâ„à∑àՙ૬À“¬„®
¢≥–¬—ß√Ÿâ÷°µ—« (awake) ¥â«¬ fiberoptic bronchoscope À√◊Õ
«‘∏’ blind nasal
2. °√≥’©ÿ°‡©‘𠇙àπ ºŸâªÉ«¬‰¡à√Ÿâ÷°µ—« ‰¡à„À⧫“¡
√à«¡¡◊Õ „Àâ„à∑àՙ૬À“¬„®¥â«¬«‘∏’ manual in line stabiliza-
tion ‚¥¬„À⺟â™à«¬®—∫»’√…–‰¡à„À⇧≈◊ËÕπ‰À«¡“°‡°‘π‰ª¢≥–„à
∑àՙ૬À“¬„® ·µàæ÷ß√–≈÷°‰«â«à“Õ“®„à∑àՙ૬À“¬„®‰¥â¬“°¢÷Èπ
‡æ√“–¡Õ߇ÀÁπ glottic opening ‰¥â‰¡à™—¥‡®π
°“√√—°…“¿“«– autonomic hyperreflexia 1) °”®—¥‘Ëß∑’Ë°√–µÿâπ„À⇰‘¥ autonomic hyperreflexia
‡™àπ °“√°√–µÿâπµà“ß Ê „π√–¥—∫∑’˵˔°«à“∫√‘‡«≥∑’ˉ¥â√—∫
∫“¥‡®Á∫
2) ‡æ‘Ë¡√–¥—∫§«“¡≈÷°¢Õ߬“√–ß—∫§«“¡√Ÿâ÷° ´÷Ëß∑”„Àâ
≈¥§«“¡¥—π‡≈◊Õ¥≈߉¥â À√◊Õ∂â“∑” epidural anesthesia „Àâ
‡æ‘Ë¡√–¥—∫°“√™“ (sensory level)
3) ∂ⓧ«“¡¥—π‡≈◊Õ¥¬—ßŸß Õ“®µâÕß„™â¬“≈¥§«“¡¥—π
‡≈◊Õ¥ ´÷ËßÕÕ°ƒ∑∏‘Ï∑’˵”·Àπàßµà“ß Ê °—π¢Õß reflex arch ‡™àπ
ÕÕ°ƒ∑∏‘Ï∑’˪¡ª√–“∑ (ganglia) ª≈“¬ª√–“∑ postgan-
glionic À√◊ÕÕ«—¬«– effector (À≈Õ¥‡≈◊Õ¥) ‚¥¬ sodium ni-
troprusside ‡ªìπ¬“∑’Ëπ‘¬¡„™â‡π◊ËÕß®“°ª√—∫¬“‰¥âßà“¬ ‰¥âº≈¥’
à«π nifedipine ‡ªìπ¬“∑’Ëπ‘¬¡„™â”À√—∫ªÑÕß°—π autonomic
hyperreflexia14
Figure 2 Schematic diagram of the pathophysiology of autonomic hyperreflexia.26 Dashed line indicates inability of brainstem to communicate neuro- logically with the lower spinal cord

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 98 Thai Journal of Anesthesiology 99Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
«‘∏’™à«¬‡ªî¥∑“߇¥‘πÀ“¬„®„π°√≥’∑’Ë°√–¥Ÿ°—πÀ≈—߉¡à¡—Ëπ- §ß (Airway maneuvers on unstable spine)19-25
1. «‘∏’™à«¬‡ªî¥∑“߇¥‘πÀ“¬„®æ◊Èπ∞“π (Basic airway
maneuvers) ∑—Èß«‘∏’ head tilt ·≈– chin lift ¡’º≈„Àâ disc
space „πµ”·Àπàß∑’Ë∫“¥‡®Á∫¢¬“¬‰¥â ¡“°°«à“ 5 ¡¡. ∂â“
®”‡ªìπ·π–π”„Àâ„™â jaw thrust
2. «‘∏’ blind nasotracheal Õ“®‡°‘¥°“√‡§≈◊ËÕπ∫√‘‡«≥
¥â“πÀ≈—ß (posterior subluxation) „πµ”·Àπàß∑’Ë∫“¥‡®Á∫
‰¥â¡“°°«à“ 5 ¡¡.
3. Advanced airway maneuvers ‡™àπ °“√„à∑àÕ
endotracheal ‰¡à«à“®–„™â laryngoscope blade ™π‘¥µ√ß
À√◊Õ‚§âß ®–∑”„Àâ disc space „πµ”·Àπàß∫“¥‡®Á∫¢¬“¬‰¥â
3-4 ¡¡.
4. Alternative airway management ‡™àπ eso-
phageal combitube, laryngeal mask airway (LMA), in-
tubating laryngeal mask airway (ILMA), lightwand ¡’
¢âÕ¡Ÿ≈°“√„™âπâÕ¬‚¥¬‡©æ“–„π°√≥’∑’Ë¡’°“√∫“¥‡®Á∫¢Õ߉¢—π-
À≈—ß∫√‘‡«≥§Õ∑’Ë√ÿπ·√߇π◊ËÕß®“°‰¡à“¡“√∂°≈à“«‰¥â«à“‰¡à¡’
°“√°â¡ (flexion) À√◊Շ߬ (extension) ¢Õß»’√…–¢≥–„à
µ—«Õ¬à“߇™àπ esophageal combitube °“√„à≈¡®”π«π¡“°
„π pharyngeal cuff ∑”„Àâ¡’·√ß°¥µ√ßµ”·Àπàß vertebral
bodies ¢Õß°√–¥Ÿ°§Õ∑’Ë 2-3 À√◊Õ 4
°“√„À⬓√–ß—∫§«“¡√Ÿâ÷°„πºŸâªÉ«¬∑’Ë¡’‰¢—πÀ≈—ß∫“¥‡®Á∫ (Anesthesia for Spinal cord Injury Patients)6,12
°“√ª√–‡¡‘π°àÕπºà“µ—¥
°“√´—°ª√–«—µ‘·≈–µ√«®√à“ß°“¬∑’Ë¥’ ¡’§«“¡”§—≠
‚¥¬¡’§”·π–π”„π°“√ª√–‡¡‘πºŸâªÉ«¬°àÕπ°“√ºà“µ—¥ ¥—ßµ“√“ß
∑’Ë 3
Premedication ¢÷Èπ°—∫§«“¡«‘µ°°—ß«≈¢ÕߺŸâªÉ«¬ ∂â“欓∏‘¿“æ√–¥—∫
Ÿß®–‰«µàÕ¬“ premedication ‡¡◊ËÕ„Àâ„π¢π“¥ª°µ‘ ®÷ߧ«√
≈¥¢π“¥≈ß ·¡â¡’°“√°≈à“««à“º≈¢Õ߬“®–≈¥≈߇π◊ËÕß®“°¡’
delayed gastric emptying time °Áµ“¡ ‚¥¬à«π„À≠à ‰¡à
π‘¬¡„À⬓‡æ◊ËÕ sedation ·µà®–„À⬓‡æ◊ËÕªÑÕß°—π¿“«– au-
Table 3 Checklist for assessment of spinal cord injured patients before surgery7
1. Sensory level compared with surgical field 2. Complete or incomplete lesion? 3. Time since injury. Spinal shock or reflex phase? Risk of hyperkalaemic response to suxamethonium 3 days- 9 months. 4. Previous anaesthetic history especially use of ‘standby’ anaesthesia. Previous anaesthetic records should be located. 5. Airway and neck movements : particularly after cervical spine surgery. 6. Respiratory assessment : particularly high lesions. History of respiratory tract infections, intensive care unit admissions, etc. Tracheostomy past or present. Vital capacity should be measured in all patients with lesion above C7. When in doubt, chest X-ray and arterial blood gases should be ordered. 7. Cardiovascular assessment : baseline blood pressure, heart rate. History of postural hypotension. History of autonomic dysreflexia-suggested by symptoms of headache and sweating when bladder full. 8. Musculoskeletal : spasms, contractures, pressure sores. 9. Medications : especially anticoagulants, baclofen and dantrolene. 10. Allergies. 11. Full blood count : anaemia is common, especially in the presence of pressure sores or chronic sepsis. 12. Urea and electrolytes : to exclude renal impairment. 13. Liver functions tests : especially where there is chronic sepsis.

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 98 Thai Journal of Anesthesiology 99Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
tonomic hyperreflexia ‡™àπ nifedipine 10 ¡°. 1 ™¡. °àÕπ
ºà“µ—¥10
General anesthesia Monitoring5,24
§«√¡’ basic monitoring µ—Èß·µà°àÕπ induction ®π∂÷ß
™à«ß recovery ‰¥â·°à §≈◊Ëπ‰øøÑ“À—«„® pulse oximetry, cap-
nometry Õÿ≥À¿Ÿ¡‘°“¬·≈–§«“¡¥—π‡≈◊Õ¥´÷Ëߧ«√‡ªìπ·∫∫
Õ—µ‚π¡—µ‘‡æ◊ËÕµ√«®«—¥¿“«–°“√‡ª≈’ˬπ·ª≈ߧ«“¡¥—π‡≈◊Õ¥‰¥âÕ¬à“ß
√«¥‡√Á« °√≥’∑’ˉ¡à stable ‡™à𠧫“¡¥—π‡≈◊Õ¥µË” À√◊Õ∑”ºà“µ—¥
„À≠à∑’Ë¡’°“√‡’¬‡≈◊Õ¥®”π«π¡“° ®πµâÕß„Àâ“√πÈ”À√◊Õà«π
ª√–°Õ∫¢Õ߇≈◊Õ¥ Õ“®µâÕß¡’ invasive monitor ‡™à𠧫“¡
¥—π‡≈◊Õ¥·¥ß (arterial blood pressure) §«“¡¥—π‡≈◊Õ¥¥”
(central venous pressure) À√◊Õ pulmonary capillary wedge
pressure
Somatosensory evoked potentials (SSEP) ·≈–
motor evoked potentials (MEP) „™â‡æ◊Ëՙ૬∫Õ°°“√‡ª≈’ˬπ
·ª≈ßÕ¬à“߇©’¬∫æ≈—π„π°√≥’∑’ˇªìπ°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß
·∫∫‰¡à¡∫√Ÿ≥å ´÷ËßÕ“®‡ªìπº≈®“°°“√¢“¥ÕÕ°´‘‡®π ‡≈◊Õ¥
‰ª‡≈’Ȭ߉¡à‡æ’¬ßæÕÀ√◊Õ‚¥π°¥®“°°“√ºà“µ—¥
Induction °√≥’∑’Ë stable “¡“√∂„™â thiopental À√◊Õ propofol
‰¥â à«π„π√“¬∑’ˉ¡à stable À√◊Õ¡’ spinal shock §«√„™â
ketamine ·µà§«√≈¥¢π“¥¬“≈ß·≈–„Àâ“√πÈ”ª√‘¡“≥¡“°π”
‰ª°àÕπ ‡æ√“–¬“¡’ƒ∑∏‘Ï°¥°“√∑”ß“π¢Õß°≈â“¡‡π◊ÈÕÀ—«„®·≈–
ºŸâªÉ«¬‡À≈à“π’È¡—°¡’°“√Ÿ≠‡’¬°“√∑”ß“π¢Õß reflex sympa-
thetic ∑”„Àâ‰¡à“¡“√∂ª√—∫µ—«‡¡◊ËÕ¡’°“√°¥°“√∑”ß“π¢Õß
°≈â“¡‡π◊ÈÕÀ—«„®®“°¬“ ketamine √à«¡°—∫¡—°¡’ renal impair-
ment ∑”„Àâ clearance ¢Õ߬“≈¥≈ß
succinylcholine “¡“√∂„™â‰¥â∂Ⓣ¥â√—∫∫“¥‡®Á∫πâÕ¬
°«à“ 24-48 ™¡. ·≈–∂◊Õ‡ªìπ muscle relaxant of choice
„π¿“«–∫“¥‡®Á∫‡©’¬∫æ≈—π à«π°“√∫“¥‡®Á∫‡√◊ÈÕ√—ßπ—Èπ„™â‰¥â
Õ¬à“ߪ≈Õ¥¿—¬À≈—ß∫“¥‡®Á∫ 9 ‡¥◊Õπ ·µà∫“ß√“¬ß“π·π–π”
„Àℙ≥âÀ≈—ß∫“¥‡®Á∫ 18 ‡¥◊Õπ Õ¬à“߉√°Áµ“¡‰¡àπ‘¬¡„™â‡ªìπ
Õ—π¥—∫·√°∂Ⓣ¡à¡’¢âÕ∫àß™’È∑’Ë™—¥‡®π ‡æ√“–Õ“®‡°‘¥Õ—πµ√“¬
‡π◊ËÕß®“° membrane ∑—ÈßÀ¡¥¢Õ߇´≈≈å°≈â“¡‡π◊ÈÕ®–∑”µ—«‡ªìπ
motor end-plate ¥—ßπ—Èπ succinylcholine ®– depolarize
membrane ∑—ÈßÀ¡¥¢Õ߇´≈≈å°≈â“¡‡π◊ÈÕ‡°‘¥‚æ·∑‡´’¬¡®”π«π
¡“°À≈—Ëߟà°√–·‡≈◊Õ¥ ∑”„À⇰‘¥ ventricular fibrillation
·≈–À—«„®À¬ÿ¥‡µâπ (cardiac arrest) µ“¡¡“‰¥â
Maintenance ®ÿ¥ª√–ߧå∑’Ë”§—≠ §◊Õ „Àâ‡≈◊Õ¥‰ª‡≈’Ȭ߉¢—πÀ≈—ß
Õ¬à“߇撬ßæÕ ‡π◊ËÕß®“°¡’°“√Ÿ≠‡’¬ autoregulation ∑”„Àâ
‡≈◊Õ¥∑’ˉª‡≈’Ȭß∑’ˉ¢—πÀ≈—ߢ÷Èπ°—∫§«“¡¥—π‡≈◊Õ¥∑’ˉª‡≈’Ȭß√à“ß
°“¬ (systemic perfusion) ¥—ßπ—Èπ°“√¡’§«“¡¥—π‡≈◊Õ¥µË”
®–∑”„À⇰‘¥°“√∫“¥‡®Á∫∑ÿµ‘¬¿Ÿ¡‘¡“°¢÷Èπ „π∑“ßµ√ߢⓡ∂â“
§«“¡¥—π‡≈◊Õ¥Ÿß¡“°‡°‘π‰ª°Á®–‡°‘¥‡≈◊Õ¥ÕÕ° (hemorrhage)
·≈–‰¢—πÀ≈—ß∫«¡ (spinal cord edema) ‰¥â‡™àπ°—π ¥—ßπ—Èπ
§«√√—°…“§«“¡¥—π‡©≈’ˬ„ÀâÕ¬Ÿà„π‡°≥±åª°µ‘
°“√·≈°‡ª≈’ˬπ·°ä¡’§«“¡”§—≠ ‡π◊ËÕß®“°°“√‰À≈
‡«’¬π‡≈◊Õ¥¢Õ߉¢—πÀ≈—ß (spinal cord circulation) ¡’≈—°…≥–
‡À¡◊Õπ°“√‰À≈‡«’¬π‡≈◊Õ¥¢Õß¡Õß (cerebral circulation)
°“√ hyperventilation “¡“√∂ decompress spinal cord ·µà
µâÕß√–«—߉¡à hyperventilation ¡“°‡°‘π‰ª ‡æ√“–®–‡°‘¥
hypocarbia ∑”„Àâ‡≈◊Õ¥‰ª‡≈’Ȭ߉¢—πÀ≈—ß≈¥≈ß·≈–‡°‘¥°“√
¢“¥‡≈◊Õ¥ √ÿª§◊Õ·π–π”„Àâ normocapnia À√◊Õ mild hy-
pocapnia
¿“«–πÈ”µ“≈„π‡≈◊Õ¥Ÿß®–°√–µÿâπ„À⇰‘¥°“√¢“¥‡≈◊Õ¥‰¥â
¡“°¢÷Èπ®“°°“√‡°‘¥¿“«– lactic acidosis ¥—ßπ—Èπ§«√À≈’°‡≈’ˬß
“√πÈ”∑’Ë¡’πÈ”µ“≈‡ªìπà«πª√–°Õ∫·≈–§«√√—°…“¥â«¬Õ‘π´Ÿ≈‘π
‡¡◊ËÕæ∫«à“πÈ”µ“≈„π‡≈◊Õ¥¡“°°«à“ 200 ¡°./¥≈.
ªí®®ÿ∫—π‰¡à¡’°“√√ÿª«à“«‘∏’°“√„À⬓√–ß—∫§«“¡√Ÿâ÷°«‘∏’„¥
¥’∑’Ëÿ¥ ∑’Ë”§—≠§◊ÕµâÕß„À⬓√–ß—∫§«“¡√Ÿâ÷°∑’Ë≈÷°æÕ (ade-
quate depth of anesthesia) ‡æ◊ËÕªÑÕß°—π°“√‡°‘¥ autonomic
hyperreflexia ·≈–‰¡àπ‘¬¡„™â«‘∏’≈¥§«“¡¥—π‡≈◊Õ¥ (induced
hypotensive) ‡æ√“–‡æ‘Ë¡§«“¡‡’ˬ߄π°“√¢“¥‡≈◊Õ¥¢Õß
‰¢—πÀ≈—ß
°“√¥Ÿ·≈™à«ß emergence ·≈–À≈—ßºà“µ—¥ à«π„À≠à¡—°¡’√–∫∫‰À≈‡«’¬π‡≈◊Õ¥·≈–√–∫∫À“¬„®
unstable ¥—ßπ—Èπ‰¡à§«√∂Õ¥∑àՙ૬À“¬„®À≈—߇√Á®ºà“µ—¥·≈–
§«√µ‘¥µ“¡Õ“°“√µàÕ∑’ËÀÕ∫√‘∫“≈ºŸâªÉ«¬Àπ—° ·µà°√≥’∑’Ë¡’°“√
∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß√–¥—∫‡Õ«·≈–‰¡à¡’§«“¡º‘¥ª°µ‘¢Õß√–∫∫
À“¬„®“¡“√∂∂Õ¥∑àՙ૬À“¬„®‰¥âÀ≈—߇√Á®ºà“µ—¥

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 100 Thai Journal of Anesthesiology 101Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
Regional Anesthesia6
‡∑§π‘§π’È¡’¢âÕ¥’§◊Õ ªÑÕß°—π¿“«– autonomic hyper-
reflexia ·≈–À≈’°‡≈’ˬßÕ—πµ√“¬∑’ˇ°‘¥®“°°“√¥¡¬“≈∫ ·µà¡’
¢âÕ®”°—¥µ√ß∑’Ë Õ“®‡°‘¥§«“¡¥—π‡≈◊Õ¥µË”¡“°¢÷Èπ‚¥¬‡©æ“–°√≥’
∑’Ë¡’¿“«–æ√àÕß“√πÈ”√à«¡°—∫‰¡à∑√“∫«à“µâÕß„™â¢π“¥¬“‡∑à“‰√
®÷ß®–∑”„À≥â√–¥—∫°“√™“∑’˵âÕß°“√ ·≈–°“√ª√–‡¡‘π√–¥—∫
°“√™“∑”‰¥â¬“° ¡’∫“ß√“¬ß“π·π–π”„Àâª√–‡¡‘π‚¥¬¥Ÿ®“°
√–¥—∫∑’Ë∑”„Àâ spastic paraparesis °≈“¬‡ªìπ flaccid para-
paresis À√◊Õ√–¥—∫∑’Ë°≈â“¡‡π◊ÈÕ‡°√ÁßÀ“¬‰ª πÕ°®“°π’ÈÕ“®
∑”°“√„À⬓√–ß—∫§«“¡√Ÿâ÷°‡©æ“–∑’ˉ¥â¬“°‡π◊ËÕß®“°ªí≠À“¢Õß
spinal column ‡™àπ kyphoscoliosis ‡§¬ºà“µ—¥‰¢—πÀ≈—ß¡“
°àÕπ √à«¡°—∫°“√®—¥∑à“∑”‰¥â¬“°‡æ√“–‰¡à“¡“√∂ßÕµ—«‰¥â
®“°¿“«–°≈â“¡‡π◊ÈÕ‰¢—πÀ≈—ßÀ¥‡°√Áß·≈–°√–¥Ÿ°º‘¥√Ÿª (bony
deformities)
”À√—∫°“√ºà“µ—¥∫√‘‡«≥°√–‡æ“–ªí“«–·≈– peri-
neum °“√∑” spinal ¥’°«à“ epidural ‡π◊ËÕß®“°“¡“√∂
complete block ¢Õß∫√‘‡«≥ sacral root ‰¥â¡“°°«à“·≈–
°“√∑” epidural ¡’‚Õ°“≈⡇À≈«‰¥â®“°°“√ missed seg-
ments ‡æ√“–¡’ distortion of epidural space °“√‰¡à“¡“√∂
∑¥Õ∫√–¥—∫°“√™“‰¥âÕ¬à“ß·πàπÕπ °“√‰¡à‡ÀÁπº≈®“°°“√
test dose ∑’Ë™—¥‡®π´÷ËßÕ“®∑”„À⇰‘¥ total spinal block ‰¥â
®÷ß∑”„Àâ¡’°“√„™â®”°—¥‡©æ“–„π™à«ß∑’Ë¡’°“√‡®Á∫§√√¿å·≈–°“√
§≈Õ¥‡æ◊ËÕªÑÕß°—π¿“«– autonomic hyperreflexia „πÀ≠‘ß
µ—Èߧ√√¿å
°“√∑” brachial plexus block “¡“√∂∑”‰¥â °“√
„™â nerve stimulator „πºŸâªÉ«¬∑’ˉ¥â√—∫∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß
√–¥—∫§Õ Õ“®‰¡à‡ÀÁπ°“√°√–µÿ°¢Õß¡◊ÕÀ√◊Õ‰¡à‡°‘¥ pares-
thesia ‡π◊ËÕß®“° root ¢Õß brachial plexus Õ“®‰¥â√—∫
∫“¥‡®Á∫√à«¡¥â«¬27
Standby, local anesthesia and sedation6
∑”‰¥â‚¥¬¢÷ÈπÕ¬Ÿà°—∫ªí®®—¬¥—ßπ’È (·µàµâÕß¡’ IV line,
monitor ·≈–¡’«‘—≠≠’·æ∑¬åÕ¬Ÿà¥â«¬µ≈Õ¥°“√∑”À—µ∂°“√)
1) ∂â“‚Õ°“‡°‘¥ autonomic hyperreflexia Ÿß‰¡à
·π–π”„Àâ∑” ‡™àπ ¡’°“√∫“¥‡®Á∫¢Õ߉¢—πÀ≈—ß√–¥—∫§Õ
¡’ª√–«—µ‘°“√‡°‘¥ª√“°Ø°“√≥åπ’È¡“°àÕπ À√◊Õ¡“∑”ºà“µ—¥√–∫∫
∑“߇¥‘πªí“«–·≈– perineum
2) Sedation, local anesthesia ·≈– topical anes-
thesia ‰¡à“¡“√∂ªÑÕß°—π¿“«– autonomic hyperreflexia ‰¥â
3) ∂â“¡’°≈â“¡‡π◊ÈÕ‡°√Áß∫àÕ¬ Ê ·π–π”„Àâ∑”°“√√–ß—∫
§«“¡√Ÿâ÷°«‘∏’ general À√◊Õ regional ‡æ◊ËÕ§«∫§ÿ¡°“√‡°√Áß
√–À«à“ßºà“µ—¥
4) §«“¡µâÕß°“√¢ÕߺŸâªÉ«¬ ‡™àπ µâÕß°“√À≈—∫√–À«à“ß
°“√ºà“µ—¥´÷ËßÕ“®∑”„ÀâµâÕ߇≈◊Õ°„™â«‘∏’√–ß—∫§«“¡√Ÿâ÷°·∫∫ general
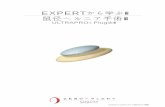
“¡“√∂√ÿª·π«∑“ß°“√„À⬓√–ß—∫§«“¡√Ÿâ÷°‰¥â¥—ß
√Ÿª∑’Ë 3
°“√¥Ÿ·≈√–¬–¬“« (Long-term Management)10
ªÑÕß°—π‰¡à„À⇰‘¥ autonomic hyperreflexia ‚¥¬°”®—¥
‘Ëß°√–µÿâπ √à«¡°—∫„À⬓ nifedipine ªÑÕß°—π‡¡◊ËÕ∑√“∫«à“
®–¡’‘Ëß°√–µÿâπ‡°‘¥¢÷Èπ à«π°“√√—°…“„π√–¬–¬“«¥â«¬°“√ºà“µ—¥
radical ‰¥â·°à cordectomy, pelvic neurectomy ∑”„πºŸâªÉ«¬
∑’ˇ°‘¥Õ“°“√∫àÕ¬ Ê ¢≥–∑’Ë°“√∑” bilateral paravertebral
sympathetic blocks æ∫«à“‰¡à‰¥âº≈
Figure 3 Flow chart for the anesthetic management of spinal cord injury patients6

ªï∑’Ë 32 ©∫—∫∑’Ë 2 ‡¡…“¬π-¡‘∂ÿπ“¬π 2549 100 Thai Journal of Anesthesiology 101Vol. 32, No. 2, April-June 2006«‘—≠≠’“√
√ÿª °“√¥Ÿ·≈ºŸâªÉ«¬∑’ˉ¢—πÀ≈—ß∫“¥‡®Á∫ ®–µâÕ߇√‘Ë¡µâπµ—Èß·µà
«‘π“∑’·√°∑’Ëæ∫ºŸâªÉ«¬ ¥—ß∑’Ë°≈à“«‰«â„πµÕπµâπ«à“‡¡◊ËÕ¡’°“√∫“¥
‡®Á∫®–¡’欓∏‘¿“懰‘¥¢÷Èπ ´÷ËßµâÕ߉¥â√—∫°“√¥Ÿ·≈√—°…“∑—π∑’
‡æ◊ËÕªÑÕß°—π‰¡à„Àâ欓∏‘¿“懰‘¥√ÿπ·√ߢ÷Èπ °“√¥Ÿ·≈·≈–√—°…“
ºŸâªÉ«¬§ßµâÕßÕ“»—¬°“√∑”ß“π‡ªìπ∑’¡ ‰¡à«à“®–‡ªìπ»—≈¬·æ∑¬å
«‘—≠≠’·æ∑¬å √«¡∂÷ß欓∫“≈·≈–‡®â“Àπâ“∑’Ë∑’ˇ°’ˬ«¢âÕ߇æ◊ËÕ„Àâ
ºŸâªÉ«¬‰¥â√—∫ª√–‚¬™πåŸßÿ¥
‡Õ°“√Õâ“ßÕ‘ß 1. Sadowsky C, Volshteyn O, Schultz L, McDonald JW. Spinal
cord injury. Disabil Rehabil 2002 ; 24 : 680-7. 2. Sekhon LH, Fehlings MG. Epidemiology, demographics,
and pathophysiology of acute spinal cord injury. Spine 2001 ; 26 : S2-12.
3. Dutton RP, McCunn M. Anesthesia for Trauma. In : Miller RD, editor. Anesthesia, 6th ed. Phildelphia : Churchill Livingstone ; 2005 : 2473-6.
4. Nockels RP. Nonoperative management of acute spinal cord injury. Spine 2001 ; 26 : S31-S37.
5. Grover VK, Tewari MK, Gupta SK, Kumar KV. Anaesthetic and intensive care aspects of spinal injury. Neurol India 2001 ; 49 : 11-8.
6. Dangor A, Lam AM. Perioperative management of patients with head and spinal cord trauma. Anesthesiol Clin North Am 1999 ; 17 : 155-70.
7. Hurlbert RJ. Methylprednisolone for acute spinal cord injury : an inappropriate standard of care. J Neurosurg 2000 ; 93 : 1-7.
8. Short DJ, El Masry WS, Jones PW. High dose methyl-prednisolone in the management of acute spinal cord injury - a systematic review from a clinical perspective. Spinal Cord 2000 ; 38 : 273-86.
9. Matsumoto T, Tamaki T, Kawakami M, Yoshida M, Ando M, Yamada H. Early complications of high-dose methylprednisolone sodium succinate treatment in the follow-up of acute cervical spinal cord injury. Spine 2001 ; 26 : 426-30.
10. Amzallag M. Autonomic hyperreflexia. Int Anesthesiol Clin 1993 ; 31 : 87-102.
11. Mirza SK, Krengel WF, III, Chapman JR, Anderson PA, Bailey JC, Grady MS, et al. Early versus delayed surgery for acute cervical spinal cord injury. Clin Orthop Relat Res 1999 ; 359 : 104-14.
12. Mehr EH, Poznak AV. Spinal Cord Tumor. In : Yao FS. Yao & Artusio’s Anesthesiology (Problem-Oriented Patient Management), 4th ed. Philadelphia : Lippincott-Raven ; 1998 : 483-91.
13. American Association of Neurological Surgeons. Blood pressure management after acute spinal cord injury. Neurosurgery 2002 ; 50 : S58-S62.
14. Habibi A, Schmeising C, Gerancher JC. Interscalene regional anesthesia in the prevention of autonomic hyper- reflexia in a quadriplegic patient undergoing shoulder sur- gery. Anesth Analg 1999 ; 88 : 98-9.
15. Catz A, Thaleisnik M, Fishel B, Ronen J, Spasser R, Fred- man B, et al. Survival following spinal cord injury in Israel. Spinal Cord 2002 ; 40 : 595-8.
16. EAST Practice Parameter Workgroup for Cervical Spine Clearance. Practice Management Guidelines for Identify- ing Cervical Spine Injuries Following Trauma. Eastern Association for the Surgery of Trauma 1998. URL: http//east.org/tpg.html.
17. McCrory C, Blunnie WP, Moriarty DC. Elective tracheal intubation in cervical spine injuries. Ir Med J 1997 ; 90 : 234-5.
18. Blackmore CC, Emerson SS, Mann FA, Koepsell TD. Cer- vical spine imaging in patients with trauma : determination of fracture risk to optimize use. Radiology 1999 ; 211 : 759-65.
19. Lennarson PJ, Smith D, Todd MM, Carras D, Sawin PD, Brayton J, et al. Segmental cervical spine motion during orotracheal intubation of the intact and injured spine with and without external stabilization. J Neurosurg 2000 ; 92 : 201-6.
20. Brimacombe J, Keller C, Kunzel KH, Gaber O, Boehler M, Puhringer F. Cervical spine motion during airway ma- nagement : a cinefluoroscopic study of the posteriorly des-tabilized third cervical vertebrae in human cadavers. Anesth Analg 2000 ; 91 : 1274-8.
21. Lennarson PJ, Smith DW, Sawin PD, Todd MM, Sato Y, Traynelis VC. Cervical spinal motion during intubation : efficacy of stabilization maneuvers in the setting of com- plete segmental instability. J Neurosurg 2001 ; 94 : 265-70.
22. Hastings RH, Vigil AC, Hanna R, Yang BY, Sartoris DJ. Cervical spine movement during laryngoscopy with the Bullard, Macintosh, and Miller laryngoscopes. Anesthesio- logy 1995 ; 82 : 859-69.
23. Kihara S, Watanabe S, Brimacombe J, Taguchi N, Yaguchi Y, Yamasaki Y. Segmental cervical spine movement with the intubating laryngeal mask during manual in-line sta-bilization in patients with cervical pathology undergoing cervical spine surgery. Anesth Analg 2000 ; 91 : 195-200.
24. Keller C, Brimacombe J, Keller K. Pressures exerted against the cervical vertebrae by the standard and intubating laryn-geal mask airways : a randomized, controlled, cross-over study in fresh cadavers. Anesth Analg 1999 ; 89 : 1296- 300.
25. Hambly PR, Martin B. Anaesthesia for chronic spinal cord lesions. Anaesthesia 1998 ; 53 : 273-89.
26. Moss J, Glick D. The Autonomic Nervous System. In : Miller RD, editor. Anesthesia, 6th ed. Philadelphia : Chur- chill Livingstone ; 2005 : 665-6.
27. Pereira L. Obstetric management of the patient with spinal cord injury. Obstet Gynecol Surv 2003 ; 58 :678-87.