Ectopic Pregnancy Case study 1: s A 22-year-old woman, para 0, was admitted with mild vaginal...
37
Ectopic Pregnancy
-
Upload
ethel-elliott -
Category
Documents
-
view
219 -
download
0
Transcript of Ectopic Pregnancy Case study 1: s A 22-year-old woman, para 0, was admitted with mild vaginal...
Ectopic Pregnancy
Case study 1: A 22-year-old woman, para 0, was admitted with mild
vaginal bleeding after 7 weeks of amenorrhoea. She had had a positive home pregnancy test. Ultrasound scan showed an empty uterus, with an adnexal mass around 2 cm. quantitative β-hCG was 2000 iu/ml.
At laparoscopy ectopic pregnancy was confirmed in the ampulary part of the right tube.
Linear salpengotomy was performed. The patient was discharged home the following day in good condition.
Case study 2: A 22-year-old woman, para 0, was admitted with vaginal
bleeding after 8 weeks of amenorrhoea. She had had a positive home pregnancy test, and described passing some tissue per vaginum. Ultrasound scan showed an empty uterus, although urinary B-hCG was still positive.
A presumptive diagnosis of incomplete abortion was made, and evacuation of the uterus carries out uneventfully. She was discharged the following day
Was readmitted that night with lower abdominal pain; a ruptured ampullary ectopic was found at laparotomy. Histology of curettage “ decidua with Arias-Stella type reaction, no
chorionic villi seen”.
Case study 3: An 33-year old woman para 4, was brought into
E.R. collapsed with lower abdominal pain. On admission she was shocked with blood pr. Of 60/40, a pulse of 120 bpm and tender rigid abdomen. Vaginal exam. Revealed a slight red loss, bulky uterus and marked cervical excitation with a tender mass in the right fornix.
At laparotomy, 3000 ml of fresh blood was removed from the peritoneal cavity and a ruptured right tubal ectopic pregnancy was found. The patient was in irreversible D.I.C. with Hb =0 .5 gm/dl and eventually died
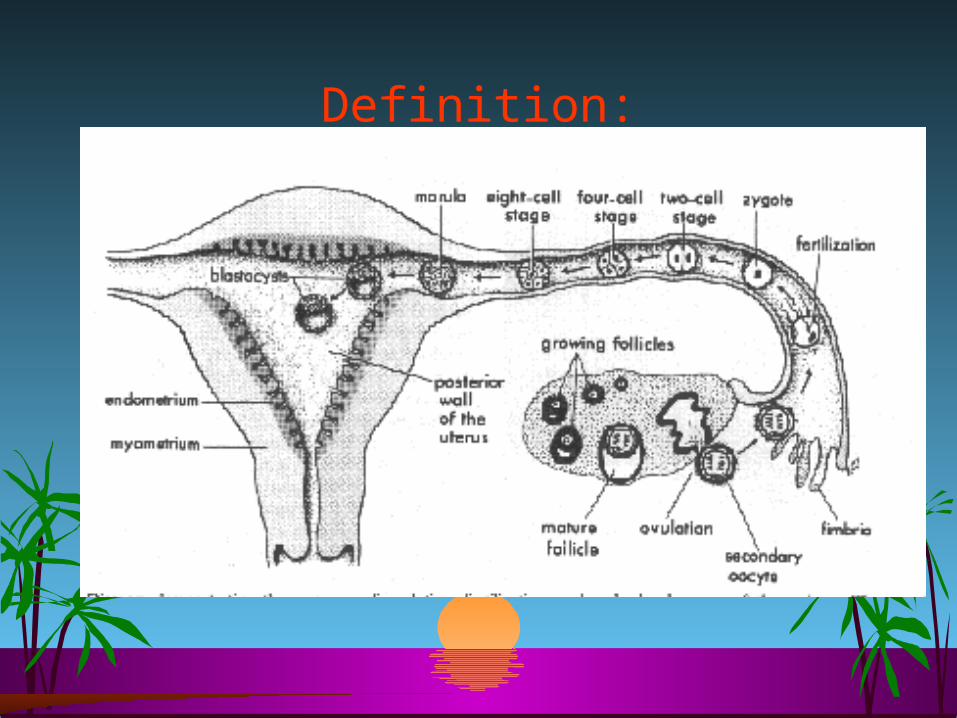
Definition:“ Any pregnancy occurring outside the uterus”
Incidence: Increasing due to P.I.D./ infertility
1-2% of all births
9% after IVF-ET
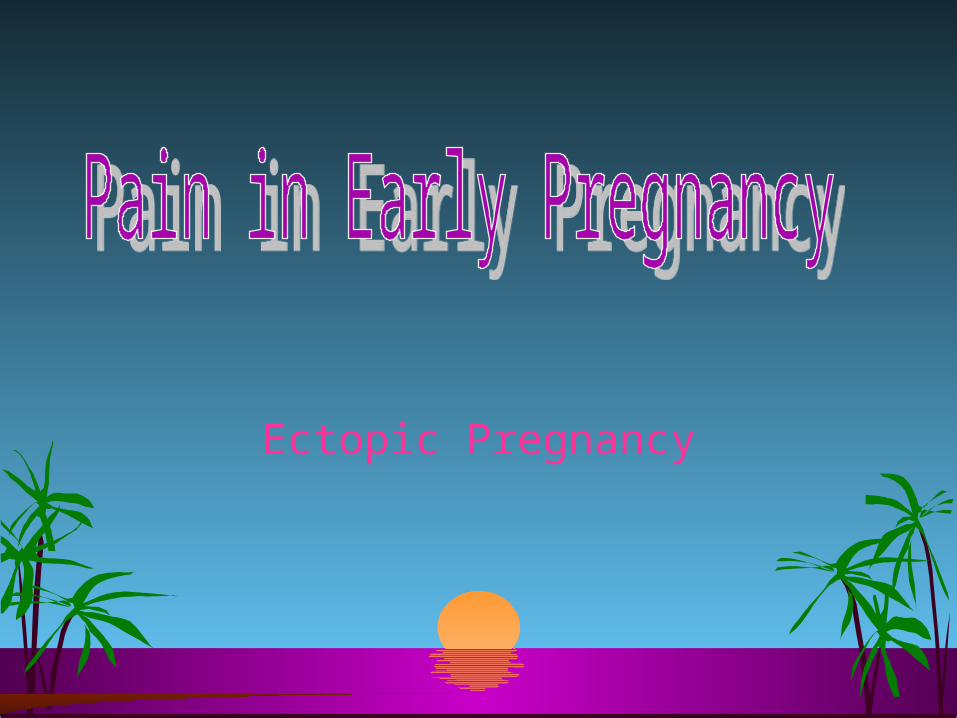
Site of implantation:

SITES OF ECTOPIC PREGNANCY
1)Fimbrial 2)Ampullary 3)Isthemic 4)Interstitial 5)Ovarian 6)Cervical 7)Cornual-Rudimentary horn 8)Secondary abdominal 9)Broad ligament 10)Primary abdominal
Ampulla (>85%)Isthmus (8%)
Cornual (< 2%)
Ovary (< 2%)
Abdomen (< 2%)
Cervix (< 2%)
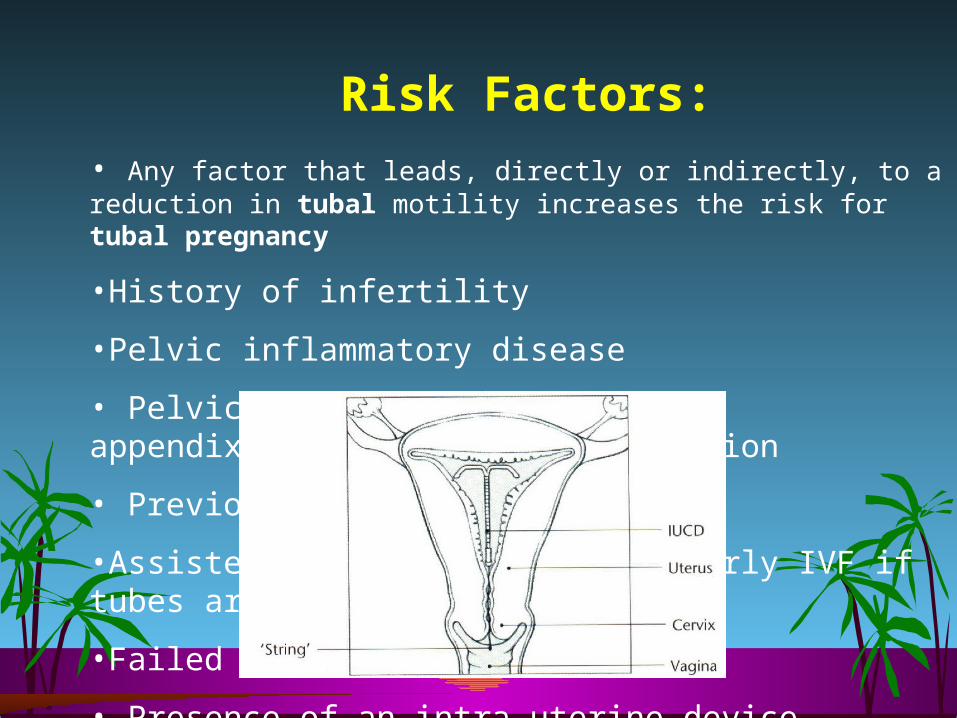
Risk Factors:
• Any factor that leads, directly or indirectly, to a reduction in tubal motility increases the risk for tubal pregnancy
•History of infertility
•Pelvic inflammatory disease
• Pelvic operations { tubal … appendix }failed tubal sterilization
• Previous tubal pregnancy
•Assisted conception { particularly IVF if tubes are patent and damaged }
•Failed contraceptive methods
• Presence of an intra uterine device.
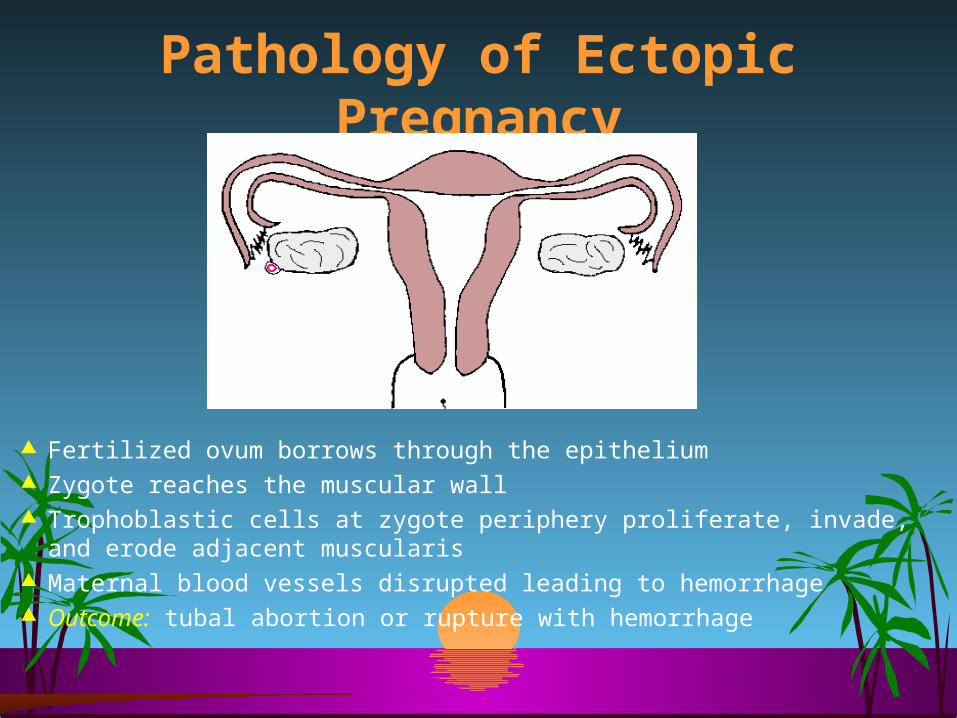
Pathology of Ectopic Pregnancy
Fertilized ovum borrows through the epithelium Zygote reaches the muscular wall Trophoblastic cells at zygote periphery proliferate, invade, and erode adjacent
muscularis Maternal blood vessels disrupted leading to hemorrhage Outcome: tubal abortion or rupture with hemorrhage

Tubal Pregnancy Commonest site of ectopic pregnancy (99%)
The ampulla is the most frequent location of implantation (64%)
Symptoms: Onset occurs ~7 weeks after LMP Abdominal pain Vaginal bleeding
Signs: Abdominal tenderness (91%) 1st trimester bleeding (79%)
Common associated findings: Adnexal tenderness (54%) , Amenorrhea Early pregnancy symptoms Cullen’s sign (Periumbilical bruising) Nausea, vomiting, diarrhea, dizziness
Other Signs: Tachycardia, Low grade fever Chadwick’s sign (cervix and vaginal cyanosis) Hegar’s sign (softened uterine isthmus) Hypoactive bowel sounds Cervical Motion Tenderness Enlarged uterus Tender pelvic or adnexal mass Cul-de-sac fullness Decidual cast (Passage of decidua in one piece)
Signs suggestive of ruptured ectopic pregnancy: Usually between 6 and 12 weeks gestation Severe abdominal tenderness with rebound, guarding Orthostatic hypotension
Differential Diagnosis Appendicitis Threatened Abortion Ruptured ovarian cyst PID Salpingitis Endometritis Nephrolithiasis Ovarian torsion Intrauterine pregnancy
Alternative diagnoses:
• Dysmenorrhea• Dysfunctional uterine bleed• UTI• Diverticulitis• Mesenteric lymphadenitis
Symptoms & Signs:
In a woman of child bearing age with pelvi-abdominal pain and/ or vaginal bleeding …… ALWAYS….think

DIAGNOSIS In recent years, inspite of an increase in the
incidence of ectopic pregnancy there has been a fall in the case fatality rate.
This is due to the widespread introduction of diagnostic tests and an increased awareness of the serious nature of this disease.
This has resulted in early diagnosis and effective treatment.
Now the rate of tubal rupture is as low as 20%.
METHODS OF EARLY DIAGNOSIS
Immunoassay utilising monoclonal antibodies to beta HCG
Ultrasound scanning – Abdominal & Vaginal including Colour Doppler
Laparoscopy Serum progesterone estimation not
helpful A combination of these methods may have to be employed.

Diagnostic modalities1. Pregnancy test.
a) Urinary B-hCG… sensitive, detects 25-50 ml I.U/ml.. Positive before missing the next period
b) Serum B-hCG…… Mainly used for quantitative rather than qualitative purposes
2. Pelvic ultrasound scan
a) Abdominal. Sac at 5 wks F.H. at 7 wks.. Needs full bladder
b) Transvaginal. A wk earlier than abdo… empty bladder
In 85% normal pregnancy B-hCG doubles every 2-3 days
In 85% ectopic pregnancy B-hCG 65% Increase every 2-3 days
METHODS OF EARLY DIAGNOSIS
TVS can visualise a gestational sac as early as 4-5 weeks from LMP.
During this time the lowest serum beta HCG is 2000 IU/Lt.
When beta HCG level is greater than this and there is an empty uterine cavity on TVS, ectopic pregnancy can be suspected.
In such a situation, when the value of beta HCG does not double in 48 hours ectopic pregnancy will be confirmed.
At 4-5 weeks-


METHODS OF EARLY DIAGNOSIS
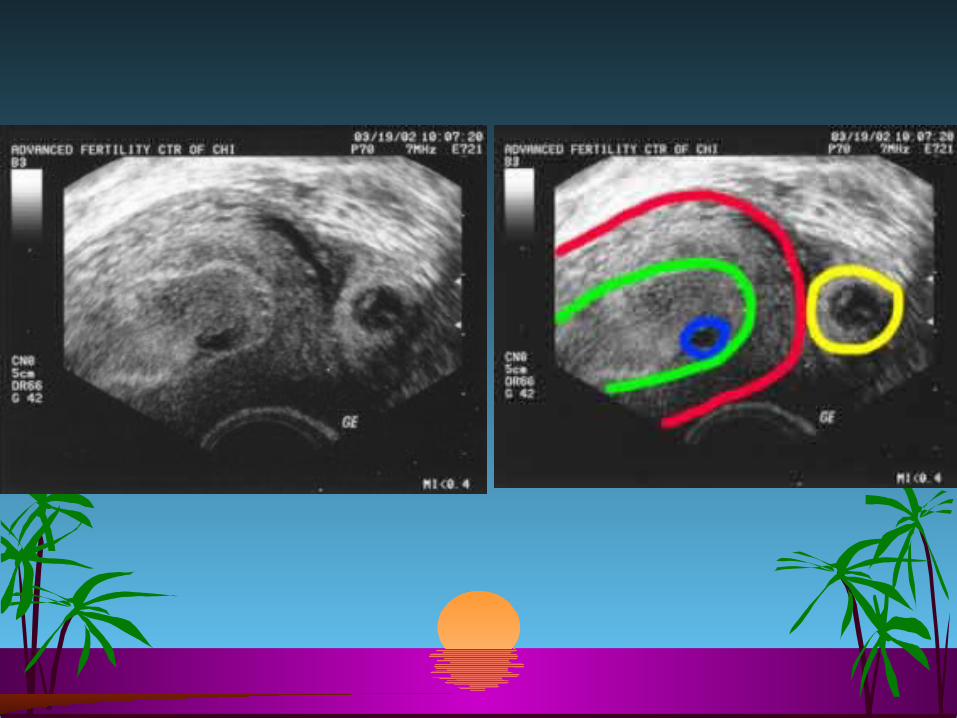
2. Poorly defined tubal ring possibly containing echogenic structure and POD typically containing fluid or blood.
3. Ruptured ectopic with fluid in the POD and an empty uterus.
4. In Colour Doppler, the vascular colour in a characteristic placental shape, the so-called fire pattern, can be seen outside the uterine cavity while the uterine cavity is cold in respect to blood flow
The USG features of ectopic pregnancy after 5 weeks can be any of the following-
Diagnostic modalities
Early Pregnancy Assessment Clinic {EPAC}:
If early pregnancy problems…. Urine B-hCG + AScan
Intra-uterine pregnancy …….GOOD
No Intra-uterine gestation Seen…… serum B-hCG + TVS.
with serum B-hCG of 1500-2000 ml I.U/ml Intra uterine gestation should be seen using TVS…… otherwise suspect Ectopic pregnancy
3. Diagnostic Laparoscopy.
Diagnostic modalitiesEarly Pregnancy Assessment Clinic {EPAC}:
.
With Advance in diagnosis and improvement in patient awareness ectopic pregnancy is more and more being diagnosed in its early stages. So, to reduce the incidence of maternal mortality and serious morbidity this dedicated clinic is a must in regional hospitals.
• Patients with early pregnancy problems to report to
• Facilities to perform urine and serum P.T. onsite
• Facilities and expertise in performing TVS
• Access to operating theatre and blood bank

MANAGEMENT
Depending on the presentation:
Acute… with ruptured ectopic and intra-abdominal bleeding…. ABC,,, + surgical approach.
Early stages, with intact ectopic:
1. Expectant… decreasing B-hCG …. Tubal abortion
2. Medical… Depending on size of ectopic and level of B-hCG….. Use methotrexate….. Not common approach
3. Surgical
Surgical Management Conservative,
Open vs laparoscopic….. Linear salpengotomy vs milking of the tube
Radical,
laparoscopic vs open ……. salpengectomy
Fertility post ectopic surgery…

SURGICAL TREATMENT OF ECTOPIC PREGNANCY
LAPAROTOMY?
VS.
LAPAROSCOPY?
SALPINGECTOMY?
VS
SALPINGOSTOMY / SALPINGOTOMY?
The debate goes on

COMPARING LAPAROTOMY Vs LAPAROSCOPY
L’tomy L’scopyHospital cost More? Less?Post operative adhesions More LessRisk of future ectopic Same SameFuture fertility Same SameExperience of Surgeon Trained Special Instruments General Special
SALPINGECTOMY VS
SALPINGOSTOMY / SALPINGOTOMY
All tubal pregnancies can be treated by partial or total Salpingectomy
Salpingostomy / Salpingotomy is only indicated when: 1. The patient desires to conserve her fertility2. Patient is haemodinmically stable3. Tubal pregnancy is accessible4. Unruptured and < 5Cm. In size5. Contralateral tube is absent or damaged
The choice of surgical treatment does not influence the post treatment fertility, but prior history of infertility is associated with a marked reduction in fertility after treatment
Making the choice – Chapron et al (1993) have described a scoring system, based on the patient’s previous gynaecological history and the appearance of the pelvic organs, to decide between salpingostomy / salpingotomy and salpingectomy.
SALPINGECTOMY VS
SALPINGOSTOMY / SALPINGOTOMY
Fertility reducing factor Score• Antecedent one Ectopic pregnancy 2• Antecedent each further
Ectopic pregnancy 1• Antecedent Adhesiolysis 1• Antecedent Tubal micro surgery 2• Antecedent Salpingitis 1• Solitary tube 2• Homolateral Adhesions 1• Contralateral Adhesions 1
SALPINGECTOMY VS
SALPINGOSTOMY / SALPINGOTOMY
• The rationale behind the scoring system is to decide the risk of recurrent ectopic pregnancy.
• Conservative surgery is indicated with a score of 1-4 only, while radical treatment is to be performed if the score is 5 or more.
SALPINGECTOMY VS
SALPINGOSTOMY / SALPINGOTOMY

Fertility post ectopic surgery…
The overall subsequent conception rate in women with ectopic pregnancies is about 60%less than half of these pregnancies result in another ectopic or spontaneous abortion, so only about one third of women with ectopic pregnancies have subsequent live births. The subsequent fertility rate is significantly higher in parous women younger than 30 years. If the ectopic pregnancy is a women's first pregnancy, her subsequent conception rate is only about 35%. On the other hand, women with high parity (more than three pregnancies) who develop an ectopic pregnancy have a relatively high rate of conception (80%). The subsequent conception rate is lower in women who have a history of salpingitis and in those who have gross evidence of damage to the opposite oviduct as a result of previous salpingitis. Future fertility is significantly higher in women who have unruptured tubal pregnancies than in those who have ruptured ectopic pregnancies; hence, early diagnosis with serial hCG and ultrasound is desirable.

Repeat Ectopic Pregnancy
The rate of repeat ectopic pregnancy after a single ectopic pregnancy ranges from 8% to 20%, with a mean of 15%. Only about one of three nulliparous women who have an ectopic pregnancy ever conceives again (35%), and about one third have another ectopic pregnancy (13%). After two ectopic pregnancies, infertility rates as high as 90% have been reported
Ectopic pregnancy is a life threatening condition & on the increase
Not all cases present with a classical picture
ALWAYS suspect ectopic pregnancy in a woman of a child-bearing age c/o pain and/or p.v. bleeding
Early diagnosis and management is feasible {EPAC}, which should be available in referral centers
Tailor your management on the patient presentation.+/_ F.up















![Mycobacteria-specific CD4IFN- cell expresses naïve-surface … · SCM) [15, 16]. These cells have been detected in BCG vaccinated infected subjects [17]. We had previously identified](https://static.fdocument.org/doc/165x107/5fa54c277baf7c74b671181f/mycobacteria-specific-cd4ifn-cell-expresses-nave-surface-scm-15-16-these.jpg)
