Drugs and Poisons in Humans Volume 5070 || β-Blockers
8
4.7 4.7 © Springer-Verlag Berlin Heidelberg 2005 II.4.7 β-Blockers by Makoto Ueki Introduction β-Blockers ( β-adrenergic receptor antagonists) block the effects of catecholamines on signal transmission through β-receptors; they cause hypotension by decreasing the heart beat rate and cardiac output, and prevent the attacks of arrhythmia and angina pectoris. In the brain, the drugs attenuate migraine by suppressing the dilation of blood vessels; in the eye, they decrease intraocular pressure by suppressing the production of aqueous humor. Since the drugs are also effective in suppressing muscle quivering and in suppressing overreaction of the thyroid gland upon being too nervous, they are used as doping drugs in competitive sports such as shooting and archery, which require psychic powers of concentration rather than aerobic performance. As untoward effects of these drugs, chill of extremities due to the contraction of vessels and aggravation of bronchial asthma due to contraction of the bronchi can be mentioned. e drugs can be classified into β 1 - and β 2 -blockers; the β 1 -receptors are mainly located in the heart muscle, while the β 2 -receptors located in the smooth muscles of the airways and blood vessels. e β 1 -blockers specifically exert blocking action on the β 1 -receptors; otherwise, the β-blockers act on both β 1 - and β 2 -receptors. e β-blockers are structurally classified into isopropylamino drugs such as propranolol and tertiary butylamino drugs such as nadolol; and many products containing 26 kinds of β-blockers are commercially available in Japan. e metabolism of β-blockers depends upon the hydrophobicity of their side chain structures. e drugs with hydrophilic side chains, such as atenolol, labetalol and nadolol, are excreted into urine in unchanged forms, while the drugs with hydrophobic side chains are excreted into urine in the glucuronide-conjugated forms aſter their hydroxylation. erefore, it is almost difficult to detect unchanged forms of drugs from urine for such hydrophobic β-blockers. e concentration ratio of a metabolite to its precursor drug in urine and the location to be hydroxylated in a drug structure are different according to races and individuals; care should be taken especially when the foreign literature is searched on the metabolism of β-blockers. HPLC analysis Reagents and their preparation • Many of the authentic standards of β-blockers can be purchased from Sigma (St. Louis, MO, USA); when compounds are not commercially available, they were directly obtained from their manufacturers with request. Ethyltheophylline a , to be used as internal standard (IS), is synthesized by heating theophylline (Sigma) and twice-molar ethyl iodide at 60 °C overnight in acetone in the presence of potassium carbonate. Other common chemicals used were of the highest purity commercially available
Transcript of Drugs and Poisons in Humans Volume 5070 || β-Blockers

4.74.7
© Springer-Verlag Berlin Heidelberg 2005
II.4.7 β-Blockers by Makoto Ueki
Introduction
β-Blockers ( β-adrenergic receptor antagonists) block the eff ects of catecholamines on signal transmission through β-receptors; they cause hypotension by decreasing the heart beat rate and cardiac output, and prevent the attacks of arrhythmia and angina pectoris. In the brain, the drugs attenuate migraine by suppressing the dilation of blood vessels; in the eye, they decrease intraocular pressure by suppressing the production of aqueous humor. Since the drugs are also eff ective in suppressing muscle quivering and in suppressing overreaction of the thyroid gland upon being too nervous, they are used as doping drugs in competitive sports such as shooting and archery, which require psychic powers of concentration rather than aerobic performance. As untoward eff ects of these drugs, chill of extremities due to the contraction of vessels and aggravation of bronchial asthma due to contraction of the bronchi can be mentioned.
Th e drugs can be classifi ed into β1- and β2-blockers; the β1-receptors are mainly located in the heart muscle, while the β2-receptors located in the smooth muscles of the airways and blood vessels. Th e β1-blockers specifi cally exert blocking action on the β1-receptors; otherwise, the β-blockers act on both β1- and β2-receptors.
Th e β-blockers are structurally classifi ed into isopropylamino drugs such as propranolol and tertiary butylamino drugs such as nadolol; and many products containing 26 kinds of β-blockers are commercially available in Japan. Th e metabolism of β-blockers depends upon the hydrophobicity of their side chain structures. Th e drugs with hydrophilic side chains, such as atenolol, labetalol and nadolol, are excreted into urine in unchanged forms, while the drugs with hydrophobic side chains are excreted into urine in the glucuronide-conjugated forms aft er their hydroxylation. Th erefore, it is almost diffi cult to detect unchanged forms of drugs from urine for such hydrophobic β-blockers. Th e concentration ratio of a metabolite to its precursor drug in urine and the location to be hydroxylated in a drug structure are diff erent according to races and individuals; care should be taken especially when the foreign literature is searched on the metabolism of β-blockers.
HPLC analysis
Reagents and their preparation
• Many of the authentic standards of β-blockers can be purchased from Sigma (St. Louis, MO, USA); when compounds are not commercially available, they were directly obtained from their manufacturers with request. Ethyltheophyllinea, to be used as internal standard (IS), is synthesized by heating theophylline (Sigma) and twice-molar ethyl iodide at 60 °C overnight in acetone in the presence of potassium carbonate. Other common chemicals used were of the highest purity commercially available

370 β-Blockers
• Solid carbonate buff er: the powder of sodium carbonate is mixed with a half-weight of the powder of sodium bicarbonate, and the mixture is well ground in a mortar and stored in a dry state
• IS solution: ethyltheophylline is dissolved in methanol to prepare 100 µg/mL solution• Mobile phases for HPLC: mobile phase A, acetonitrile/phosphoric acid/distilled water
(15:0.1:85, v/v); mobile phase B, acetonitrile/phosphoric acid/distilled water (60:0.1:40, v/v).
HPLC conditions
Separation column: Nucleosil7C18 (250 × 4.6 mm i. d., Macherey-Nagel, Düren, Germany).HPLC conditions; instrument: L-6200 typeb (Hitachi Ltd., Tokyo, Japan); autosampler:
WISP 714 plus (Waters, Milford, MA, USA); fl ow rate: 1.5 mL/min. Gradient elution is linearly made from 100 % A to 100 % B during 8 min aft er injection. Detector: HP1040DAD (Agilent Technologies, Palo Alto, CA, USA); detection wavelengths: 216, 254 and 275 nm, because of low specifi city of the detection by ultraviolet absorbance.
Procedure
i. A 1-mL volume of a specimen, 50 µL IS solution (containing 5 µg ethyltheophylline) and 0.5 g of solid carbonate buff er are placed and mixed well in a glass centrifuge tube with a ground-in stopper, followed by the addition of 5 mL diethyl ether and gentle shaking for 5 min.
ii. Aft er centrifugation at 1,000 g for 5 min, the ether phase is transferred to a vial and evapo-rated to dryness under a stream of nitrogen.
iii. Th e residue is dissolved in 300 µL methanol and a fi xed aliquot of it is injected into HPLC c.
iv. Blank specimens are spiked with various concentrations of the authentic standard of a drug and the IS, and are processed according to the above procedure to construct each calibra-tion curve. By applying the peak area ratio of a specimen to the calibration curve, the concentration of a target compound is calculated.
Assessment of the method
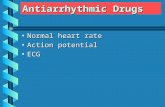
> Figure 7.1 shows HPLC chromatograms for atenolol, nadolol and labetalol extracted from urine of their users. Atenolol is eluted just aft er the void volume; however, since it has a couple of asymmetric carbon atoms in its structure and produces two peaks due to the isomers, its identifi cation is relatively easy. Nadolol could be detected until about 7 h aft er single adminis-tration, but it has no characteristic absorbance maximum and lacks in specifi city; it should be careful to identify nadolol by HPLC. Th e detection limit of the β-blockers was about 100 ng/mL (10 ng on-column).

371
Simultaneous GC/MS analysis of β-blockers and their metabolites [1–3]
Reagents and their preparation
• Acquisition of the authentic standard drugs and their preparation are the same as described in the HPLC analysis section
• 1 M Phosphate buff er solution (pH 7.0): a 34.0-g aliquot of potassium dihydrogenphos-phate is dissolved in distilled water, followed by adjustment of the solution to pH 7.0 with 10 M NaOH; then the fi nal volume is adjusted to 250 mL
• Solid carbonate buff er: the powder of sodium bicarbonate is mixed with a half-weight of potas-sium carbonate powder, and the mixture is well ground in a mortar and stored in a dry state
• Derivatization reagents: N-methyl-N-(trimethylsilyl)trifl uoroacetamide ( MSTFA) and N-methyl-bis(trifl uoroacetamide) ( MBTFA) were purchased from Macherey-Nagel (Düren, Germany)
• IS solutiond: bupranolol is dissolved in ethanol to prepare 0.2 mg/mL solution.
GC/MS conditions
Instrumente: HP-5970MSD (Agilent Technologies)GC column: Ultra-II (12.5 m × 0.25 mm i. d., fi lm thickness 0.33 µm, Agilent Technologies)
HPLC chromatograms for β-blockers extracted from urine of subjects, who had ingested each of them. The results were obtained after single oral intake of each drug. In the analysis of atenolol, double peaks appeared for this drug, because of two asymmetrical carbon atoms present in its structure.
⊡ Figure 7.1
Simultaneous GC/MS analysis of β-blockers and their metabolites

372 β-Blockers
Flow rate: 1 mL/min (about 20 kPa/cm2 of He pressure at 100 °C); injection temperature: 300 °C; split ratio = 11:1; sample volume to be injected: 2 µL; ionization mode: EI; electron energy: 70 eV; ion multiplier: auto tune + 300 V
Th e range in the scan mode: m/z 50–600; dwell time of each ion in the SIM mode: 30 ms/ion. Th e measurements are made for the following 3 groups by switching them according to retention times.
Ion group 1: from 2.5 min of retention timem/z 86, 129, 200, 284, 365, 373, 427, 478, 479, 505, 526 and 559Ion group 2: from 5.1 min of retention timem/z 86, 129, 235, 250, 284, 344, 348, 421, 448, 478, 488, 497, 510 and 526Ion group 3: from 6.0 min of retention timem/z 86, 91, 129, 284, 292, 478 and 515.
Procedure
i. A 5-mL volume of urine, 50 µL IS solution (containing 10 µg bupranolol), 1 mL of 1 M phosphate buff er (pH 7) and 30 µL of β-glucuronidase K-2 (3 nuits, Roche Diagnostics GmbH, Mannheim, Germany) are placed in a glass centrifuge tube with a ground-in stop-per, and incubated at 50 °C for 60 min for hydrolysis.
ii. Th e hydrolyzed solution is mixed with 5 mL diethyl ether and gently shaken for 5 min for washing the aqueous phase. Aft er removal of the organic phase, 1 mL 2-methylpropanol and about 0.1 g of solid carbonate buff er are added to the aqueous phase and mixed well.
iii. A 5 mL volume of diethyl etherf and 3 g anhydrous sodium sulfate are added to the above aqueous phase, gently shaken for 20 min and centrifuged at 1,000 g for 5 min. Th e resulting ether phase is transferred to a glass vial with a screw cap and evaporated to dryness under a stream of nitrogen.
iv. Th e residue is dissolved in 50 µL MSTFA, followed by heating at 50 °C for 5 min aft er cap-ping the vial for TMS derivatization. Aft er cooling to room temperature, 15 µL MBTFA is added to the mixture, followed by heating at 50 °C for 15 min for TFA derivatization. Since the reactions are dependent upon equilibrium, the reaction solution should not be evapo-rated, but directly injected into GC/MS.
v. Th e calibration curves are constructed for quantitation in the same way as that of HPLC analysis.
Assessment and some comments on the method
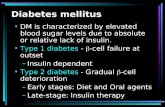
> Figure 7.2 shows an example of mass chromatograms of GC/MS for the extract of urine, into which β-blockers and their metabolites had been spiked. In the automatic searching system of the author, the presence or absence of a β-blocker is displayed aft er calculating the expected retention time of a candidate drug from the actually measured retention time of IS and the relative retention time of the compound listed in > Table 7.1. Isopropylamino β-blockers and their metabolites, such as alprenolol, oxprenolol, metoprolol, atenolol, propranolol and acebutolol, can be detected in mass chromatograms at m/z 284 and 129

373
( > Fig. 7.2). By examining a pattern (abundance ratios among diagnostic ion traces) of a mass spectrum of a compound, it is easy to discriminate a target compound from a impurity peak. Th e tertiary butylamino β-blockers are simultaneously detected by mass chromatography at m/z 86; the β-blockers with characteristic structures, such as sotalol and labetalol, can be de-tected with high sensitivity using their proper ions.
Th e detection limit of β-blockers obtained by mass chromatography of GC/MS is about 10 ng/mL (about 150 pg on column), while that by HPLC was 100 ng/mL (10 ng on-column).
> Table 7.1 summarizes the names of β-blockers and their metabolites detected, the struc-tures of derivatives, relative retention times to that of IS, molecular weights of derivatives and two representative fragment ions each, obtained from urine extracts of volunteers, who had received single oral administration of each β-blocker under informed consent. Th e metabolites hydroxy-lated at the aromatic rings followed by its glucuronide conjugation are found in common with most β-blockers; especially for alprenolol, metoprolol, penbutolol and propranolol, the amounts of metabolites to be excreted into urine are larger than those of their unchanged forms.
⊡ Table 7.1Indicators for GC/MS analysis of β-blockers
β-Blocker Compound(s) to be detected
Derivatization Relative retention time*
M. W. Monitor ions (m/z)
acebutolol acebutolol acetylacebutolol
N-TFA-O-TMSN-TFA-O-TMS
2.3132.196
504476
284284
129129
alprenolol hydroxyl aprenolol N-TFA-bis-O-TMS 1.618 505 284 505
atenolol atenolol N-TFA-bis-O-TMS 1.630 559 284 559
betaxolol betaxolol N-TFA-O-TMS 2.039 475 284 129
bisoprolol bisoprolol N-TFA-O-TMS 2.027 493 284 129
carteolol carteolol bis-O-TMS 1.871 436 235 421
celiprolol celiprolol bis-O-TMS 1.643 450 86 200
esmolol esmolol N-TFA-O-TMS 1.871 448 284 448
labetalol labetalol(racemic mixture)
nitril-N-TFA-bis-O-TMSnitril-N-TFA-bis-O-TMS
2.4422.476
550550
292292
91 91
levobunolol levobunolol O-TMS 1.792 363 86 348
metoprolol hydroxyl metoprolol N-TFA-bis-O-TMS 1.793 523 284 478
mepindolol mepindolol bis-N, N-TFA-O-TMS 1.781 526 284 526
nadolol nadolol tris-O-TMS 1.970 525 86 510
oxprenolol oxprenolol hydroxyl oxprenolol
N-TFA-O-TMSN-TFA-bis-O-TMS
1.2781.160
433521
284284
129129
penbutolol hydroxyl penbutolol N-TFA-bis-O-TMS 1.797 451 86 250
pindolol pindolol N-TFA-bis-N,O-TMS 2.061 488 284 488
propranolol hydroxyl propranolol 4- hydroxyl propranolol
N-TFA-O-TMSN-TFA-O-TMS
1.7082.148
427515
284284
427515
sotalol sotalol N-TFA-bis-N,O-TMS 1.851 512 344 497
timolol timolol O-TMS 1.627 388 86 373
IS bupranolol N-TFA-O-TMS 1.000 439 86
* Relative retention time: retention times of each compound, when that of IS is assumed as 1.000.
Simultaneous GC/MS analysis of β-blockers and their metabolites

374 β-Blockers
β-Blockers are usually derivatized with MSTFA/MBTFA to form N-TFA-O-TMS deriva-tives; when they are analyzed by GC/MS in the EI mode, intense fragment peaks can be de-tected at m/z 284 and 129 for the isopropylamino drugs and at m/z 86 for the tertiary butylamino drugs in common ( > Table 7.1). By using these ions, it becomes possible to make simultaneous detection of unchanged forms and metabolites of many β-blockers using a small number of ions.
When a β-blocker used can be estimated, various additional informations can be obtained by optimizing analytical conditions for the target compound. For example, when the ionization mode is changed into the CI mode, a protonated molecular ion appears, which is useful to confi rm its molecular weight. When the derivatization reagents are changed into trifl uoroacetic anhydride, a base peak at a higher mass number due to a TFA derivative of a β-blocker can be obtained aft er heating and evaporation of the excess reagent; for example, the mass spectrum of nadolol-tris-O-TMS gives the base peak at m/z 86, while that of nadolol-tris-O-TFA gives the base peak at m/z 266, which can be used for sensitive quantitation.
Toxic and fatal concentrations [4]
As usual cautions for use of β-blockers, their administration should not be stopped suddenly, because it causes aggravation of symptoms and occasionally cardiac infarction; the suppression of respiration of a neonate may take place, when a mother had been taking a β-blocker during
Mass chromatograms of GC/MS for β-blockers extracted from urine of subjects, who had ingested each drug. Many of β-blockers and their hydroxylated metabolites can be simul-taneously detected in the mass chromatograms at m/z 284, 126 and 86. It is possible to confirm the presence or absence of a target compound by displaying the location of chromatograms, where the target compound should appear, using a targeting software.
⊡ Figure 7.2

375
pregnancy. As relatively frequent untoward eff ects of the drugs, exanthemas due to hypersen-sitivity, bradycardia, headache, diarrhea and decrease in secretion of tears can be mentioned.
LD50 values vary from 190 (alprenolol hydrochloride) to 4,000 mg/kg (acebutolol hydro-chloride) with oral administration to mice; the values are 17–57 mg/kg with intravenous ad-ministration of the same drugs to rats, depending on each drug.
Although in Japan reports on β-blocker poisoning are not many, Kiyota et al. [5] reported a fatal poisoning case due to intake of multiple drugs including oxprenolol; the case showed marked circulatory disturbance. Th e victim had ingested about 11 g of oxprenolol, 96 mg chlor-promazine, a tricyclic antidepressant, a benzodiazepine and other drugs together with wine to attempt suicide. She died of hypotension and circulatory disturbance 34 h aft er hospitalization. Th e concentration of oxprenolol in urine sampled several hours aft er admission was about 20 µg/mL, which was very high. Th erefore, it was diagnosed that her death was due to poison-ing by multiple drugs (mainly oxprenolol).
> Table 7.2 shows β-blockers and the numbers of their detection disclosed by doping con-trol tests in 1995–2000. Th e most frequently used drug was atenolol, followed by metoprolol, bisoprolol, sotalol and carteolol; the numbers of acebutolol, betaxolol and carvedilol were a few.
Notes
a) When the synthesis of ethyltheophylline is diffi cult, proxyphylline (Sigma) can be used as IS.b) Any type of HPLC instruments, which enables gradient elution and is equipped with a UV-
or photodiode array detector, can be used.c) To enhance the sensitivity, the amount of the fi nal solution can be reduced; in that case, the
amount of IS to be spiked should be reduced appropriately. To monitor contamination by environmental compounds, mutual contamination among specimens and interference by endogenous components, the same amount samples of distilled water, blank serum (urine) and spiked serum (urine) (for quality assurance) are preferably processed simultaneously.
⊡ Table 7.2The numbers of doping tests conducted for sport athletes and the numbers of positive cases of doping with β-blockers in 1995–2000
Year 1995 1996 1997 1998 1999 2000
Total number of tests 93,937 96,454 106,561 105,250 118,259 117,314 Total
atenolol 2 2 3 4 4 6 21
metoprolol 1 1 2 4 3 2 13
bisoprolol 1 1 2 1 2 7
sotalol 1 4 1 6
carteolol 2 2 4
acebutolol 1 1 2
betaxolol 2 2
carvedilol 1 1
Total number of positive cases
4 4 9 10 16 13 56
Toxic and fatal concentrations

376 β-Blockers
d) As IS, one of other β-blockers can be used. Th e most desirable IS is the deuterated form of the target compound, in which more than two deuterium atoms are labeled.
e) Any type of GC/MS instruments with the EI ionization can be used. To simultaneously detect many ions in the SIM mode, it is convenient to use an instrument, which supports a soft ware to change an ion group into another group according to retention time intervals for analysis.
f) For extraction of β-blockers, various solvents much polar than diethyl ether can be used, resulting in a higher peak of a target compound due to higher extraction effi ciency; but the impurity peaks are also increased and thus the S/N ratio is sometimes not improved. When a target compound is fi rmly bound with proteins in a blood specimen, deproteinization or alkalinization treatment should be made; the pH of the resulting clear solution should also be adjusted before extraction with an organic solvent. Th ese treatments may give much better results.
References
1) Ueki M (1997) Application to doping tests. In: Ueno T, Hirayama K, Harada K (eds) Biological Mass Spectrometry. Tokyo Kagaku Dojin, Tokyo, pp 204–214 (in Japanese)
2) Leloux MS, Maes RAA (1990) The use of electron impact and positive chemical ionization MS in the screening of beta blockers and their metabolites in human urine. Biomed Environ Mass Spectrom 19:137–142
3) Hemmersbach P, de la Torre R (1996) Stimulants, narcotics and beta-blockers: 25 years of development in ana-lytical techniques for doping control. J Chromatogr B 687:221–238
4) Osaka Prefectural Society of Hospital Pharmacists (ed) (1988) Guide Book for Ethical Drugs, 4th edn. Jiho Inc., Tokyo, p 466 (in Japanese)
5) Kiyota K, Ono K, Maekawa K et al. (1997) A fatal poisoning case with multiple drugs including oxprenolol, a β-blocker. Jpn J Toxicol 10:425–426 (in Japanese)