Digital photogrammetry and histomorphometric assessment of the effect of non-coherent light...
10
ORIGINAL ARTICLE Digital photogrammetry and histomorphometric assessment of the effect of non-coherent light (light-emitting diode) therapy (l640±20 nm) on the repair of third-degree burns in rats Silvana Maria Véras Neves & Renata Amadei Nicolau & Antônio Luiz Martins Maia Filho & Lianna Martha Soares Mendes & Ana Maria Veloso Received: 28 July 2012 / Accepted: 15 March 2013 / Published online: 13 April 2013 # Springer-Verlag London 2013 Abstract Recent studies have demonstrated the efficacy of coherent light therapy from the red region of the electro- magnetic spectrum on the tissue-healing process. This study analysed the effect of non-coherent light therapy (light- emitting diode—LED) with or without silver sulfadiazine (sulpha) on the healing process of third-degree burns. In this study, 72 rats with third-degree burns were randomly divid- ed into six groups (n=12): Gr1 (control), Gr2 (non-contact LED), Gr3 (contact LED), Gr4 (sulfadiazine), Gr5 (sulfadi- azine + non-contact LED) and Gr6 (sulfadiazine + contact LED). The groups treated with LED therapy received treat- ment every 48 h (l =640±20 nm, 110 mW, 16 J/cm 2 ; 41 s with contact and 680 s without contact). The digital photo- metric and histomorphometric analyses were conducted after the burn occurred. The combination of sulpha and LED (contact or non-contact) improved the healing of burn wounds. These results demonstrate that the combination of silver sulfadiazine with LED therapy (l =640±20 nm, 4 J/cm 2 , without contact) improves healing of third-degree burn wounds, significantly reduces the lesion area and increases the granulation tissue, increases the number of fibroblasts, promotes collagen synthesis and prevents burn infections by accelerating recovery. Keywords Light-emitting diode . Healing . Third-degree burns . Rats Introduction Burns are an important public health problem in Brazil and throughout the world. The healing process for these lesions is highly complex and can be divided into three phases: inflammation, proliferation and maturation [1]. Research using experimental models has suggested that phototherapy positively modulates cellular prolifer- ation and activity, angiogenesis and collagen synthesis [2–4]. The therapeutic effects of electromagnetic radia- tion (coherent and non-coherent) on biological tissue are fundamentally dependent on the measured parameters [5]. Some studies have demonstrated that skin lesions in non- diabetic and diabetic rats are repaired more quickly when S. M. V. Neves (*) : A. L. M. M. Filho Faculdade Integral Diferencial—FACID, Rua Veterinário Bugyja Brito, 1354—Bairro Horto Florestal, 64052-410, Teresina, Piauí, Brazil e-mail: [email protected] S. M. V. Neves : R. A. Nicolau : A. L. M. M. Filho Universidade do Vale do Paraíba, São José dos Campos, São Paulo, Brazil L. M. S. Mendes Universidade Federal do Piauí, Teresina, Piaui, Brazil A. M. Veloso Pathology and Cytopathology Laboratory, São Marcos Hospital, Teresina, Piaui, Brazil Lasers Med Sci (2014) 29:203–212 DOI 10.1007/s10103-013-1312-7
Transcript of Digital photogrammetry and histomorphometric assessment of the effect of non-coherent light...

ORIGINAL ARTICLE
Digital photogrammetry and histomorphometric assessmentof the effect of non-coherent light (light-emitting diode) therapy(l640±20 nm) on the repair of third-degree burns in rats
Silvana Maria Véras Neves & Renata Amadei Nicolau &
Antônio Luiz Martins Maia Filho &
Lianna Martha Soares Mendes & Ana Maria Veloso
Received: 28 July 2012 /Accepted: 15 March 2013 /Published online: 13 April 2013# Springer-Verlag London 2013
Abstract Recent studies have demonstrated the efficacy ofcoherent light therapy from the red region of the electro-magnetic spectrum on the tissue-healing process. This studyanalysed the effect of non-coherent light therapy (light-emitting diode—LED) with or without silver sulfadiazine(sulpha) on the healing process of third-degree burns. In thisstudy, 72 rats with third-degree burns were randomly divid-ed into six groups (n=12): Gr1 (control), Gr2 (non-contactLED), Gr3 (contact LED), Gr4 (sulfadiazine), Gr5 (sulfadi-azine + non-contact LED) and Gr6 (sulfadiazine + contactLED). The groups treated with LED therapy received treat-ment every 48 h (l=640±20 nm, 110 mW, 16 J/cm2; 41 swith contact and 680 s without contact). The digital photo-metric and histomorphometric analyses were conducted
after the burn occurred. The combination of sulpha andLED (contact or non-contact) improved the healing of burnwounds. These results demonstrate that the combination ofsilver sulfadiazine with LED therapy (l=640±20 nm,4 J/cm2, without contact) improves healing of third-degreeburn wounds, significantly reduces the lesion area andincreases the granulation tissue, increases the number offibroblasts, promotes collagen synthesis and preventsburn infections by accelerating recovery.
Keywords Light-emitting diode . Healing . Third-degreeburns . Rats
Introduction
Burns are an important public health problem in Brazil andthroughout the world. The healing process for these lesionsis highly complex and can be divided into three phases:inflammation, proliferation and maturation [1].
Research using experimental models has suggestedthat phototherapy positively modulates cellular prolifer-ation and activity, angiogenesis and collagen synthesis[2–4]. The therapeutic effects of electromagnetic radia-tion (coherent and non-coherent) on biological tissue arefundamentally dependent on the measured parameters[5].
Some studies have demonstrated that skin lesions in non-diabetic and diabetic rats are repaired more quickly when
S. M. V. Neves (*) :A. L. M. M. FilhoFaculdade Integral Diferencial—FACID, Rua Veterinário BugyjaBrito, 1354—Bairro Horto Florestal,64052-410, Teresina, Piauí, Brazile-mail: [email protected]
S. M. V. Neves : R. A. Nicolau :A. L. M. M. FilhoUniversidade do Vale do Paraíba, São José dos Campos,São Paulo, Brazil
L. M. S. MendesUniversidade Federal do Piauí, Teresina, Piaui, Brazil
A. M. VelosoPathology and Cytopathology Laboratory, São Marcos Hospital,Teresina, Piaui, Brazil
Lasers Med Sci (2014) 29:203–212DOI 10.1007/s10103-013-1312-7

light-emitting diode (LED) therapy is employed because itfacilitates the healing process, promotes collagen proteinsynthesis and aids wound recovery [6–9].
Several studies have employed coherent light to optimisethe process of tissue repair [10–15] because it has importantbiomodulatory effects. However, more research on non-coherent light therapy is needed to scientifically test itseffects on cutis burn lesions with and without medications.
The objective of this study was to test the biomodulatoryeffects of LED therapy with and without 1 % silver sulfadi-azine on healing of third-degree burns in rats.
Materials and methods
Ethical aspects
After the Research Ethics Committee of Faculdade IntegralDiferencial granted approval (under protocol number496/2008), 72 male Wistar rats weighing 250±25 g wereused in the study. The International Norms for BiomedicalResearch in Animals were followed.
Induction of experimental burn
Anaesthesia was administered intraperitoneally using 10 %ketamine and 2 % xylazine chloride (0.1 ml/100 g of bodyweight). A dorsal trichotomy was performed on the animals(6 cm from the skull to the tail and 4 cm from side to side). Toinduce the third-degree burns, a test tube with a 2.44-cmdiameter containing 50 ml of distilled water was heated to100ºC and then placed in contact with the skin for 20 s [16].After these procedures, the animals were placed in polypro-pylene cages during the experiment. They were kept underideal hygienic, light and temperature conditions and fed thestandard animal house diet and water ad libitum.
Experimental groups
The animals included in the study were randomly dividedinto six experimental groups. Each group was subdividedinto two groups (n=6) for euthanasia and analysed after 7 or14 days (Table 1).
Treatment parameters and equipment
The first irradiations occurred 24 h after the burns wereinduced at 48-h intervals in Gr2, Gr3, Gr5 and Gr6. (Table 2).The LED equipment was used [gallium–aluminium–arsenide(GaAlAs)] with 40 nm bandwidth (full width at half maxi-mum), centred at 640 nm, which was a prototype built for theexperiment. The optical output power of the light source wasfound before the experiments with the use of a broadband
power and energy metre: System 13 PEM 001/J (Melles GriotPhotonics Components Group, Carlsbad, CA, USA).
For the irradiations of Gr2 and Gr5, the LED was fixedon a tripod at a distance of 2.44 cm from the animal's dorsalso that the LED beam covered the entire affected area, butthe equipment did not make direct contact with the lesionregion. Thirty-six animals were euthanised 7 days after thelesion was induced. The animals' euthanised on the 7th dayreceived three therapy sessions, whereas the animals'euthanised on the 14th day received six sessions.
Silver sulfadiazine topical use
Applications of 0.5 g of 1 % silver sulfadiazine (Prati,Donaduzzi, Toledo, Paraná, Brazil) were performed in Gr4,Gr5 and Gr6 covering the entire lesion area every 48 h until theday before euthanasia.
Digital photogrammetry—macroscopic analysis
The digital photogrammetry was performed immediately afterthe burn and on the 7th and 14th days of treatment. The digitalimage was obtained using a Sony model DSC-S730 camera(Cyber-shot © 2008, Sony Corporation, São Paulo, Brazil)with a resolution of 7.2 megapixels. The camera was fixedon a tripod and kept at a constant distance of 12 cm from thebase. The diameter of the wounds was measured using ImageJ
Table 1 Distribution of the experimental groups
Group (n=12) Treatment
Gr1 Control
Gr2 Non-contact LED
Gr3 Contact LED
Gr4 Sulfadiazine only
Gr5 Sulfadiazine + non-contact LED
Gr6 Sulfadiazine + contact LED
Table 2 LED irradiation parameters used in the experiment
Parameters LED contact LED without contact
Wavelength (nm) 640±20 640±20
Power (W) 0.11 0.11
Irradiation area (cm2) 1.13 4.67
Irradiation time (seconds) 41 680
Energy density (J/cm2)/point 4 16
Energy (J)/point 4.51 74.8
Number of points 4 1
Energy density (J/cm2) total 16 16
Total energy (J) 74.8 74.8
204 Lasers Med Sci (2014) 29:203–212

software (version 1.39u), and the programme calibrationguidelines were followed to determine the area of the lesion.
Histological analysis
Longitudinal histological cuts with a thickness of 5 μm wereobtained for analysis. For each animal, eight cuts wereobtained: four cuts stained with haematoxylin and eosin andfour cuts stained with Masson's trichrome for specific collagencoloration.
The histological analysis of inflammatory reactions wasconducted using optical microscopy following the protocolof Meirelles et al. [16].
Histomorphometric analysis
The histological laminas were submitted to analysis usingcaptured images evaluated with a system of optical microsco-py. The image capture was taken with a Samsung Super VisionSVIII digital camera (1280×1024 pixels) attached to a NikonEclipse Microscope E 400 (Japan) and a Samsung Synmastercomputer 740n. The images were standardised according to themicroscope light intensity and magnification level (×40 objec-tive) and stored in tagged image file format for subsequent cellcounting. For quantitative analysis, inflammatory cells, fibro-blasts and blood vessels from the experimental periods (days 7and 14) were counted using the ImageJ programme. Thequalitative evaluation analysed the evolution of lesion repairby investigating the degree of collagen fibre remodelling usingthe same software.
Statistical analysis
The variables measured in the study were analysed with the aidof GraphPad Prism software 3.0 (Platform Windows, 3.0 ver-sion). A nonparametric Kruskal–Wallis test and Dunn's post-testwere used to analyse the differences between groups. P≤0.05was considered statistically significant.
Results
Macroscopic evolution of wound repair
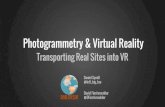
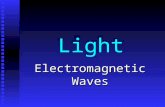
Seven days after burning (DAB), thermal necrosis with thepresence of crusts that extended to the subcutaneous tissuewas still observed in all of the specimens in the six groups(Fig. 1).
Intragroup analysis The intragroup analysis showed that thelesion area was significantly smaller (p<0.001) in all groups 7and 14 DAB compared with the lesion area at baseline(0 DAB). It was observed that the injury area was significantly
smaller 14 DAB compared with the area 7 DAB (p<0.05) inall groups.
Intergroup analysis There was no significant difference in theburn area between the groups 7 DAB (p>0.05). Gr4 had asignificantly smaller lesion area (p<0.01) than Gr1, Gr3 andGr5 (Fig. 2). The area of the legions in Gr4 was not signifi-cantly different than the area in Gr2 andGr6. The lesion area inGr6 was significantly smaller than in Gr2. The lesion area inGr2 was significantly larger than in Gr1 (p=0.0206), whileGr4 had a significantly smaller legion area than Gr1 (p=0.0011). Fourteen DAB, Gr1 (p=0.0079), Gr2 (p=0.0111),Gr3 (p=0.0183) and Gr6 (p=0.0325) had significantly largerlesion areas than Gr4. However, 14 DAB, the lesion area wassimilar between Gr4 and Gr5.
Microscopic evolution of wound repair The inflammatorycells, blood vessels and fibroblasts were counted in the areadelimited by the ImageJ software. On day 7, acute inflam-mation and neovascularisation were intense in the majorityof analysed specimens, and chronic inflammation was gen-erally moderate. Re-epithelisation was absent in the majorityof analysed samples and was present in more than 50 % ofspecimens in only Gr1, Gr2 and Gr5. The presence of gran-ulation tissue was moderate in all specimens of the controlgroup and mild in the majority of animals in the other groups.The number of fibroblasts was low in the majority of animalsin all of the experimental groups. In all of the animals, thecollagen deposits were also mild in this phase. On day 14,granulation tissue was generally moderate in the sulpha groupand intense in the other groups. Neovascularisationwas intensein nearly all of the animals. The number of fibroblasts wasmoderate in Gr1 and Gr3, moderate to intense in Gr2 andintense in Gr4 and Gr5. Collagen deposition was mild in themajority of the animals. Re-epithelisation was predominantlymild in Gr2 and Gr5, varied from mild to moderate in Gr1 andGr3 and varied from moderate to intense in Gr4 and Gr6(Table 3, Fig. 3).
Intragroup analysis There was a significant reduction in thenumber of inflammatory cells from 7 to 14 DAB in Gr1 (p=0.0073), Gr4 (p=0.0297) and Gr6 (p=0.0159). There were nosignificant differences (p>0.05) between the two time points inGr2, Gr3 or Gr5. Gr2 and Gr5 showed similar results at bothexperimental time points (7 and 14DAB), but there were fewerinflammatory cells in Gr1 and Gr3 (Fig. 4). There were nosignificant differences in the number of vessels from 7 to 14DAB in any of the experimental groups. An increase in thenumber of fibroblasts from 7 to 14 DAB was observed in Gr2(p=0.0004) and Gr4 (p=0.0208).
Intergroup analysis The number of inflammatory cells 7DAB was greater in Gr1 than in Gr2 (p=0.0040), Gr4
Lasers Med Sci (2014) 29:203–212 205

(p=0.0060) and GR5 (p=0.0060). The number of inflam-matory cells 14 DAB was significantly lower in Gr4 com-pared with Gr1 (p=0.0079), Gr2 (p=0.0111), Gr3 (p=0.0183) and Gr6 (p=0.0325). There were no significantdifferences between Gr4 and Gr5 (p=0.2035) in the numberof inflammatory cells. The number of blood vessels 7 DABwas significantly lower in Gr5 than in Gr1 (p=0.0169). Thenumber of blood vessels 14 DAB was significantly higher inGr1 than in Gr3 (p=0.0153) and Gr4 (p=0.0352). Gr4 andGr3 had significantly fewer vessels than Gr2 (p=0.0175 andp=0.0098, respectively). The number of vessels in Gr3 wassignificantly lower than in Gr6 (p=0.0448). The number offibroblasts 7 DAB was significantly lower in Gr4 than inGr1 (p=0.0386) and Gr5 (p=0.033). Although differenceswere observed between Gr4 and Gr2 (p=0.1137), Gr3 (p=0.0534) and Gr6 (p=0.0996), these differences were not
significant. The number of fibroblasts 14 DAB in Gr4was significantly higher than in Gr1 (p=0.0357) andGr5 (p=0.0297).
Discussion
The beneficial effects of coherent and non-coherent light forhealing tissue burns in diabetic and non-diabetic rats and humanshave been reported in several studies [6, 11, 13, 16–19].However, some studies are contradictory, and some do not showpositive results for phototherapy [20–22]. Burns were chosen asthe woundmodel because there is a great need for more researchon the biomodulation effects of laser or LED therapy. Therewere no significant differences in burn area between thedifferent groups, indicating that the effects of third-degree
GroupsDays after burns
0 7 14
No sulfadiazine
Control
Non-contact LED
Contact LED
With sulfadiazine
Control
Non-contact LED
Contact LED
3 cm
Fig. 1 Burn injury during theexperimental periods (days 0, 7and 14) in animals treated withor without sulfadiazine and/orLED
206 Lasers Med Sci (2014) 29:203–212

burns were consistent, as previously described by Meirelleset al. [16]. There is evidence that coherent light therapydecreases the number of inflammatory cells [2, 3].Photobiomodulation helps increase the quantity of growthfactors and cytokines liberated by monocytes, which playan important role in the inflammatory phase of healing [23,24]. There have been no studies to date on LED therapywith silver sulfadiazine for burns, although some recentstudies have suggested an association of low-intensity coher-ent light with other medicines [25–28]. The effectivenessof phototherapy in dosages between 1 and 6 J/cm2 inaccelerating the healing process has been demonstratedpreviously [4, 10, 24, 29–32]. From this perspective, thebenefits of phototherapy were evident in this study; theLED energy employed at the cellular level acceleratedthe inflammatory response in the initial healing phase.Phototherapy in elevated dosages (above 16 J/cm2) mayinhibit the inflammatory response and harm the healingprocess [33–36].
The presence of crusts was observed in all the groups onday 7. Some authors say that crusts are necessary becausethey serve as a mechanical barrier between the externalenvironment and lesion tissue, facilitating cell migration tothe healing tissue and producing better conditions for cellu-lar repair [17]. All of the groups showed significant burnreduction in the first and second weeks after the burn oc-curred. We suggest that there is no negative change in thetissue repair process after LED therapy (contact or non-
contact) with or without silver sulfadiazine. Previous studieshave observed similar results for wounds treated with non-coherent light (LED) or coherent light (laser) as the radiationsource [2, 3, 34, 35]. The results of the lesion area analysis 7DAB suggest that non-contact LED had an effect that wassimilar to sulpha therapy but less pronounced than thecombination of sulpha and contact LED. Confirming thedata obtained in this study, Minatel et al. [37] observed theeffect of phototherapy on the healing of leg ulcers in twodiabetic patients. The combination of a laser (660/890 nm)with topical sulfadiazine was effective for surgical healingas a non-invasive, biostimulatory therapy and had an addi-tional analgesic effect. There is no significant differenceassociated with changes in the electromagnetic spectrum ofthe LED used in coherent light (laser) therapy in the resultsobtained in cultures or tissue when they are irradiated inhomeostasis [38, 39]. Diabetic and immunosuppressed ani-mals, for example, have no systemic homeostasis. Unlikeprevious studies, when phototherapy was used on diabeticanimals with damaged skin, it promoted an area reduction ofmore significant injuries [2, 3].
Seven DAB, the lesion area in Gr2 was larger than inthe control group (Gr1). This result suggests that non-contact LED therapy can promote effective control ofthe inflammatory cascade, resulting in less oedema andleading to a larger area of injury because of the swell-ing and oedema of the lower edges. Other studies haveoffered evidence of a significant reduction in cytokines
0
2
4
6
8
Gr1 Gr2 Gr3 Gr4 Gr5 Gr6
Groups
Les
ion
area
(cm
2 )
0 days
7 days
14 days
¥
§
¥
§#
¥ ¥¥§†
¥
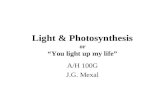
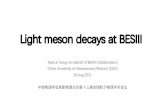
Fig. 2 Lesion area during the experiment. Gr1 (control), Gr2 (non-contact LED), Gr3 (contact LED), Gr4 (sulfadiazine), Gr5 (sulfadia-zine + non-contact LED) and Gr6 (sulfadiazine + contact LED). Thevalues are presented as the mean ± SEM for the six groups. Intragroup
significant difference (p<0.05); (asterisk) vs. day 0, (yen) vs. day 7,Intergroup; (section sign) vs. Gr1, (black diamond) vs. Gr2, (numbersign) vs. Gr3, (dagger) vs. Gr6
Lasers Med Sci (2014) 29:203–212 207

after irradiation with red region light [40], and thus, wecould obtain the same energy density in the groups thatwere irradiated. The irradiation time employed for Gr2was higher than for Gr3, suggesting that the irradiationtime may have been an important factor in the positivephotobiomodulator effect and control of inflammation.This conclusion is strongly supported by the significant-ly lower number of inflammatory cells in Gr2 comparedwith the control and contact LED therapy groups. Thesimilarity of the results related to the inflammatory cellsin Gr1, Gr4 and Gr5 (in the parameters tested) maysuggest that non-contact LED therapy promotes localantimicrobial control and activates the immune system,as shown in a recent review by Piva et al. [40].
The presence of granulation tissue was intense and accom-panied by a large number of fibroblasts and low number ofcollagen fibres in Gr4, Gr5 and Gr6 14 DAB. These findings
confirm the results of a previous study [30] that used the sameperiod of observation, wavelengths from 660 and 780 nm andan energy density of 5 J/cm2 per point.
Intense neovascularisation was observed in 100 % of theanimals in Gr2, Gr3, Gr5 and Gr6 on day 7, which suggestpositive effects of photo induction on vascular formationbased on the parameters used. These data corroborate aprevious study [24] that found that blood vessel prolifera-tion on days 3, 7 and 14 was superior to the non-treatedgroup in all of the irradiated groups (p<0.05). For theseauthors, irradiation with 5 J/cm2 fluency stimulated moreintense angiogenesis than the 20 J/cm treatment. On day 14,the tissue therapy with a non-contact LED (Gr2) showed ahigher number of blood vessels compared with Gr4 (p<0.05).Thus, the LED therapy may have generated and increasedblood vessels, contributing to the re-establishment of localblood flow. These data corroborate the results of the authors
Table 3 Summary of the results of the histological analysis (%) on days 7 and 14
CriterionControl Non-contact LED Contact LED
I M Md I M Md I M Md
Day 7
No sulfadiazine Acute inflammation 83 17 – 83 17 – 100 – –
Chronic inflammation – 100 – – 83 17 – 100 –
Fibroblasts – – 100 – – 100 – – 100
Granulation tissue – 100 – – – 100 – – 100
Neoangiogenesis 100 – – 100 – – 100 – –
Collagen – – 100 – – 100 – – 100
With sulfadiazine Acute inflammation 50 33 17 50 33 17 66 17 17
Chronic inflammation – 83 17 – 50 50 – 66 33
Fibroblasts 17 17 66 – – 100 – – 100
Granulation tissue 17 33 50 – – 100 – – 100
Neoangiogenesis 83 17 – 100 – – 100 – –
Collagen – 17 83 – – 100 – – 100
Day 14
No sulfadiazine Acute inflammation – 67 33 33 50 17 17 67 17
Chronic inflammation – 83 17 – 33 67 – 33 67
Fibroblasts – 100 – 33 67 – 17 83 –
Granulation tissue – 100 – 50 50 – 83 17 –
Neoangiogenesis 100 – – 83 17 – 100 – –
Collagen – – 100 – – 100 – – 100
With sulfadiazine Acute inflammation – 67 33 – 100 – – 50 50
Chronic inflammation – 67 33 – 100 – – 17 83
Fibroblasts 100 – – 100 – – 100 – –
Granulation tissue 100 – – 100 – – 100 – –
Neoangiogenesis 67 33 – 100 – – 67 33 –
Collagen – 17 83 – – 100 – – 100
I Intense, M Moderate, Md Mild
208 Lasers Med Sci (2014) 29:203–212

that have employed a laser in repairing third-degreeburns [16, 17, 19].
Fibroblasts play a decisive role in healing. Three and 4DAB, fibroblasts originated from mesenchymal cells. Theyproliferated and became dominant around the 10th day, whenthey became involved in collagen production. The resultsindicated that non-coherent light had better stimulatory effectswhen combined with sulpha and was superior to it when usedalone. On the cellular level, coherent and non-coherent lightmodulates fibroblast proliferation, increases collagen bondand synthesis, promotes angiogenesis, improves energy me-tabolism and produces biological effects during the healing
phase [3, 33–36]. The collagen deposition varied according tothe period and according to the group analysed; it was minorin the great majority of animals in the six groups on the14th day of observation. Our results concur with the findingsof previous research that employed wavelengths of 660 and780 nm and a dosage of 5 J/cm2 on four points [16, 30] andfound a small and moderated number of immature and frag-mentary collagen fibres on the 14th day of treatment usingoptical microscopy. The studies indicated that the 660 nmlaser produced better results than the 780 nm laser in acceler-ating the healing process of third-degree burns in diabetic andnon-diabetic rats.
GroupsDay
7 14
No sulfadiazine
Control(Gr1)
Non-contact LED (Gr2)
Contact LED(Gr3)
With sulfadiazine
Control(Gr4)
Non-contact LED (Gr5)
Contact LED(Gr6)
Fig. 3 Microscopy showingwound healing on the 7th and14th day after the burn.Masson's trichrome (×400)
Lasers Med Sci (2014) 29:203–212 209

The results obtained in this study demonstrate thatthe majority of the treated groups (Gr2 to Gr5) had asmaller concentration of inflammatory cells at the lesionsite in the initial phase of repair, especially in the LEDgroups combined with sulpha compared with the controlgroup, which corroborated some studies that haveemployed laser therapy [2, 31]. Gr1, Gr2, Gr3 andGr6 had significantly larger lesion areas than Gr4. How-ever, the lesion area was similar 14 DAB for Gr4 andGr5. These results demonstrate the cumulative effects ofsulpha drug therapy and occurred in association with
non-contact LED and sulpha. The positive resultsobtained in this study regarding the reduction in thelesion area (7 and 14 DAB) corroborate previous studiesthat have found an effect of phototherapy using a doseof 4 J/cm2. To evaluate the interference of the laser(GaAlAs, 670 nm) on the elastic and collagen fibres,the researchers induced standardised skin wounds on theback of Wistar rats and then performed regular applica-tions of laser therapy with different energy densities.The animals were sacrificed after 5, 7 and 14 days.The results showed that there was a greater reduction
0
10
20
30
40
50
Infl
amm
ator
y ce
lls (
n) ..
7 days 14 days
0
2
4
6
8
Ves
sels
(n)
0
10
20
30
40
Gr1 Gr2 Gr3 Gr4 Gr5 Gr6Groups
Fib
robl
asts
(n)
‡
¥
*
¥*
‡
*† *†¥
¥*§
¥*
‡
*§†*§
*
Fig. 4 Number ofinflammatory cells, bloodvessels and fibroblasts presentin the repair area of the differentgroups 7 and 14 DAB. Gr1(control), Gr2 (non-contactLED), Gr3 (contact LED), Gr4(sulfadiazine), Gr5(sulfadiazine + non-contactLED) and Gr6 (sulfadiazine +contact LED). The values arepresented as the mean ± SEMfor the six groups. Intragroupsignificant difference (p<0.05);(yen) vs. day 7. Intergroupsignificant difference (p<0.05);(asterisk) vs. Gr1, (section sign)vs. Gr2, (double dagger) vs.Gr4, (dagger) vs. Gr6
210 Lasers Med Sci (2014) 29:203–212

in oedema and inflammatory infiltration and increasedexpression of collagen and elastic fibres in the experi-mental group, although the difference was not statisti-cally significant (p>0.05). Treatment with a dose of4 J/cm2 yielded better results than a dose of 8 J/cm2
[29].On 7 DAB of healing, there were significantly fewer in-
flammatory cells in the groups treated with contact LED (Gr3and Gr6) compared with the non-contact LED groups (Gr2and Gr4). This result suggests that the pressure exerted by theequipment in Gr3 and Gr6 may have generated a greaterinflammatory response in these groups. This information con-tributes to knowledge about treating wounds with photother-apy because it guides decisions about the type of lightapplication. The loss of radiation from reflection under non-contact treatment did not decrease the positive biomodulatoryeffects of phototherapy.
Conclusion
The combination of sulpha and LED (contact or non-contact) improves the healing of burn wounds. These resultsdemonstrate that the combination of silver sulfadiazine withLED therapy (l=640±20 nm, 4 J/cm2 without contact)improves the quality of the wound healing after third-degree burns, promotes a significant reduction in the lesionarea and granulation tissue, increases the number offibroblasts, improves collagen synthesis and preventsburn infections by encouraging wound repair.
Acknowledgments R. A. Nicolau thanks the National Council forScientific and Technological Development (CNPq, Brazil) for theproductivity fellowship (process no. 314455/2009-4).
References
1. Martins CBG, Andrade SM (2007) Burns in children and adolescents:hospital morbidity and mortality analysis. Acta Paul Enferm20(4):464–469. doi:10.1590/S0103-21002007000400013
2. Rabelo SB, Villaverde AB, Nicolau RA, Salgado MC, MeloMS, Pacheco MT (2006) Comparison between wound healingin induced diabetic and nondiabetic rats after low-level lasertherapy. Photomed Laser Surg 24:474–479. doi:10.1089/pho.2006.24.474
3. Dall-Agnol MA, Nicolau RA, Lima CJ, Munin E (2009) Compar-ative analysis of coherent light action (laser) versus non-coherentlight (light-emitting diode) for tissue repair in diabetic rats. LasersMed Sci 2009. doi:10.1007/s10103-009-0648-5
4. Mello PB, Sampedro RMF, Piccinini AM (2007) Effects of theHe–Ne laser and of the application mode on healing burns in rats.Fisioter Pesq 4:6–13
5. Bispo LB (2007) Light emitting diodes: the wave length and itsimportance. Rev Dent on line.16, jul/dec, 110-113. http://www.ufsm.br/dentisticaonline. Accessed 01 Jun 2009
6. Al-Watban FAH, Andres BL (2003) Polychromatic LED therapyin burn healing of non-diabetic and diabetic rats. J Clin Laser MedSurg 21:249–258. doi:10.1089/pho.2006.24.10
7. Vinck EM, Cagnie BJ, Cornelissen MJ, Declercq HA, Cambier DC(2003) Increased fibroblast proliferation induced by light emittingdiode and low power laser irradiation. Lasers Med Sci 18:95–99.doi:10.1007/s10103-003-0262-x
8. Whelan HT, Buchmann EV, Dhokalia A, Kane MP, Whelan NT,Wong-Riley MTT, Eells JT, Gould LJ, Hammamieh R, Das R, JettM (2003) Effect of NASA light-emitting diode irradiation onmolecular changes for wound healing in diabetic mice. J ClinLaser Med Surg 21:67–74. doi:10.1089/104454703765035484
9. Al-Watban FA, Andres BL (2006) Polychromatic LED in oval full-thickness wound healing in non-diabetic and diabetic rats.Photomed Laser Surg 24(1):10–16. doi:10.1089/pho.2006.24.10
10. Byrnes KR, Barna L, Chenault VM, Waynant RW, Ilev IK, LongoL, Miracco C, Johnson B, Anders JJ (2004) Photobiomodulationimproves cutaneous wound healing in an animal model of type IIdiabetes. Photomed Laser Surg 22:281–290. doi:10.1089/pho.2004.22.281
11. Al-Watban FAH, Delgado GD (2005) Burn healing with a diodelaser: 670 nm at different doses as compared to a placebo group.Photomed Laser Surg 23:245–250. doi:10.1089/pho.2005.23.245
12. Gál P, Vidinsky B, Toporcer T, Mokry M, Mozes S, Longauer F,Sabo J (2006) Histological assessment of the effect of laser irradi-ation on skin wound healing in rats. Photomed Laser Surg 24:480–488. doi:10.1089/pho.2006.24.480
13. Al-Watban FA, Zhang XY, Andres BL, Al-Anize A (2009) Visiblelasers were better than invisible lasers in accelerating burn healingon diabetic rats. Photomed Laser Surg 27(2):269–272.doi:10.1089/pho.2008.2310
14. Al-Watban FA (2009) Laser therapy converts diabetic woundhealing to normal healing. Photomed Laser Surg 27(1):127–135.doi:10.1089/pho.2008.2406
15. Al-Watban FA, Zhang XY, Andres BL (2007) Low-level lasertherapy enhances wound healing in diabetic rats: a comparison ofdifferent lasers. Photomed Laser Surg 25(2):72–77. doi:10.1089/pho.2006.1094
16. Meirelles GCS, Santos JN, Chagas PO, Moura AP, Pinheiro ALB(2008) Effectiveness of laser photobiomodulation as 660 or780 nm on the repair of third-degree burns in diabetic rats.Photomed Laser Surg 26(1):47–54. doi:10.1089/pho.2007.2051
17. Oliveira PC, Meireles GCS, dos Santos NR, de Carvalho CM, deSouza APC, dos Santos JN, Pinheiro ALB (2008) The use of lightphotobiomodulation on the treatment of second-degree burns: ahistological study of a rodent model. Photomed Laser Surg26(4):289–299. doi:10.1089/pho.2007.2148
18. Ribeiro MS, da Silva DdFT, de Araújo CEN, De Oliveira SF,Pelegrini CMR, Zorn TMT, Zezell DM (2004) Effects of low-intensity polarised visible laser radiation on skin burns: a lightmicroscopy study. J Clin Laser Med Surg 22(1):59–66.doi:10.1089/104454704773660994
19. Vashegani MMV, Bayat M, Rezaei F, Bayat A, Karimipour M(2008) Effect of low-level laser therapy on mast cells in second-degree burns in rats. Photomed Laser Surg 26(1):1–5. doi:10.1089/pho.2007.2103
20. Erdle BJ, Brouxhon S, Kaplan M, Vanbuskirk J, Pentland AP(2008) Effects of continuous-wave (670 nm) red light on woundhealing. Dermatol Surg 34:320–325. doi:10.1111/j.1524-4725.2007.34065.x
21. Schlager A, Oehler K, Huebner KU, Schmuth M, Spoetl L (1999)Healing of burns treatment with 670-nm low power laser light.Plast Reconstr Surg 105(5):1635–1639. doi:10.1097/00006534-200004050-00006
22. Schlager A, Kronberger P, Petschke F, Ulmer H (2000) Low-powerlaser light in the healing of burns: a comparison between two
Lasers Med Sci (2014) 29:203–212 211

different wavelengths (635 and 690 nm) and a placebo group.L a s e r s S u r g Me d 2 7 : 3 9 – 4 2 . d o i : 1 0 . 1 0 0 2 / 1 0 9 6 –9101(2000)27:1<39::AID-LSM5>3.0.CO;2–4
23. Yu W, Naim JO, Lanzafame RJ (1997) Effects of photo-stimulation on wound healing in diabetic mice. Lasers Surg Med20:56–63. doi:10.1002/(SICI)1096–9101(1997)20:1<56::AID-LSM9>3.0.CO;2-Y
24. Corazza AV, Jorge J, Kurachi C, Bagnato VA (2007)Photobiomodulation on the angiogenesis of skin wounds in ratsusing different light sources. Photomed Laser Surg 25(2):102–106. doi:10.1089/pho.2006.2011
25. Gonçalves WLS, Souza FM, Conti CL, Cirqueira JP, Rocha WA,Pires JGP, Barros LAP, Moysés MR (2007) Influence of He–Nelaser therapy on the dynamics of wound healing in mice treatedwith anti-inflammatory drugs. Braz J Med Biol Res 40:877–884.doi:10.1590/S0100-879X2007000600018
26. Reis SRA, Medrado AP, Marchionni AMT, Figueira C,Fracassi LD, Knop LAH (2008) Effect of 670-nm laser ther-apy and dexamethasone on tissue repair: a histological andultrastructural study. Photomed Laser Surg 26(4):307–313.doi:10.1089/pho.2007.2151
27. Gál P, Mokrý M, Vidinský B, Kilík R, Depta F, Harakaľová M,Longauer F, Mozeš S, Sabo J (2009) Effect of equal daily dosesachieved by different power densities of low-level laser therapy at635 nm on open skin wound healing in normal and corticosteroid-treated rats. Lasers Med Sci 24:539–547. doi:10.1007/s10103-008-0604-9
28. Sommer AP (2007) Antiinfectives and low-level light: a newchapter in photomedicine. Photomed Laser Surg 25(3):150–158.doi:10.1089/pho.2007.2058
29. Pugliese LS, Medrado AP, Reis SRA, Andrade ZA (2003) Theinfluence of low-level laser therapy on biomodulation of collagenand elastic fibres. Pesq Odont Bras 17(4):307–313. doi:10.1590/S1517-74912003000400003
30. Meirelles GCS, Santos JN, Chagas PO, Moura AP, Pinheiro ALB(2008) A compara t ive s tudy of the effec ts of laserphotobiomodulation on the healing of third-degree burns-a histo-logical study in rats. Photomed Laser Surg 26(2):159–166.doi:10.1089/pho.2007.2052
31. Busnardo VL, Biondo-Simões MLP (2010) Effects of low-levelhelium–neon laser on induced wound healing in rats. Rev BrasFisiot 14(1):45–51. doi:10.1590/S1413-35552010000100008
32. Enwemeka CS, Parker JC, Dowdy DS, Harkness EE, Sanford LE,Woodruff LD (2004) The efficacy of low-power lasers in tissuerepair and pain control: a meta-analysis study. Photomed LaserSurg 22:323–329. doi:10.1089/pho.2004.22.323
33. Houreld N, Abrahamse H (2007) In vitro exposure of woundeddiabetic fibroblast cells to a helium–neon laser at 5 and 16 J/cm2.Photomed Laser Surg 20(2):78–84. doi:10.1089/pho.2006.990
34. Houreld N, Abrahamse H (2008) Laser light influences cellularviability and proliferation in diabetic-wounded fibroblast cells in adose- and wavelength-dependent manner. Lasers Med Sci 23:11–18. doi:10.1007/s10103-007-0445-y
35. Hawkins D, Abrahamse H (2005) Biological effects ofhelium–neon laser irradiation on normal and wounded humanskin fibroblasts. Photomed Laser Surg 23(3):251–259.doi:10.1089/pho.2005.23.251
36. Hawkins D, Abrahamse H (2006) Effect of multiple exposures oflow-level laser therapy on the cellular responses of woundedhuman skin fibroblasts. Photomed Laser Surg 24(6):705–714.doi:10.1089/pho.2006.24.705
37. Minatel DG, Franca SC, Enwemera CS, Frade MAC (2009) Pho-totherapy (LEDs 660/890nm) in the treatment of leg ulcers indiabetic patients: case study. An Bras Dermatol 84(3):279–283.doi:10.1590/S0365-05962009000300011
38. Almeida-Lopes L, Rigau J, Jaeger MMM, Brugnera AJr, Vélez-González M (1998) Acción del láser a baja densidad de potencia enla proliferación in vitro de fibroblastos de encía humana. BolSELMQ 14(5):14–18
39. El Sayed SO, Dyson M (1990) Comparison of the effect ofmultiwavelength light produced by a cluster of semiconductordiodes and each individual diode on Mast cell number and degran-ulation in intact and injured skin. Lasers Surg Med 10:559–568.doi:10.1002/lsm.1900100608
40. Piva JAAC, Abreu EMC, Silva VS, Nicolau RA (2011) Effect oflow-level laser therapy on the initial stages of tissue repair: basicprinciples. An Bras Dermatol 86(5):947–954. doi:10.1590/S0365-05962011000500013
212 Lasers Med Sci (2014) 29:203–212