Computational Fluid Dynamics: From Lab to Bedside · 2012. 7. 17. · Computational Fluid Dynamics:...
94
Computational Fluid Dynamics: From Lab to Bedside Δημοσθένης Γ. Κατρίτσης, MD, PhD (London), FRCP Athens Euroclinic, Athens Greece St Thomas’ Hospital, London UK City University, London UK
Transcript of Computational Fluid Dynamics: From Lab to Bedside · 2012. 7. 17. · Computational Fluid Dynamics:...
-
Computational Fluid Dynamics:From Lab to Bedside
Δημοσθένης Γ. Κατρίτσης, MD, PhD (London), FRCP
Athens Euroclinic, Athens Greece
St Thomas’ Hospital, London UK
City University, London UK
-
• Coronary artery disease (CAD) is the single most common cause of death in the developed world, responsible for about 1 in every 5 deaths. In 2002, out of 57 million deaths worldwide, approximately 16.7 million were due to cardiovascular disease (as compared with
approximately 5 million due to tuberculosis, human immunodeficiency virus, and malaria combined).
• Mortality from cardiovascular disease is estimated to reach 23.4 million in 2030. Coronary artery disease (including acute MI) is responsible for about half of these cardiovascular deaths.
Computational Fluid Dynamics: From Lab to Bedside
One death every two sec
-
Atherosclerosis in Ancient Egyptian MummiesAllam AH et al. The Horus Study J Am Coll Cardiol Img 2011;4:315–27
-
Atherosclerosis in Ancient Egyptian MummiesAllam AH et al. The Horus Study J Am Coll Cardiol Img 2011;4:315–27
-
Coronary atherosclerosis in patients
-
Computational Fluid Dynamics: From Lab to BedsideLAD stable stenosis
RAO Cranial
-
Determinants of thrombosis in coronary atherosclerotic plaques.
Computational Fluid Dynamics: From Lab to Bedside
-
Computational Fluid Dynamics: From Lab to Bedside
Stenotic lesions have smaller lipid cores, more fibrosis, and calcification;
thick fibrous caps; and less compensatory enlargement (positive remodeling).
Nonstenotic lesions have large lipid cores and thin,
fibrous caps susceptible to rupture and thrombosis.
-
Computational Fluid Dynamics: From Lab to Bedside PCI vs MEDICAL THERAPY In Stable CAD
Katritsis and Ioannidis. Circulation 2005; 111:2906-2912.
PCI not recommended in stable IHD in recent GLs
-
Update of Meta-Analysis of PCI, as Compared with Medical Treatment,for Stable Coronary Artery Disease
PCI vs MEDICAL THERAPY In Stable CADKatritsis and Ioannidis. New Engl J Med 2007;357:414-5 .
-
Intervention is indicated as soon as possible in ACSKatritsis DG, et al. Optimal timing of coronary angiography and potential intervention in non-ST-elevation
acute coronary syndromes. Eur Heart J. 2011;32:32-40.
-
MIs often occur at sites of mild-to-moderate stenosesAmbrose et al. J Am Coll Cardiol. 1988;12:56-62
Little et al. Circulation. 1988;78:1157-1166
Ruptured plaques leading to acute coronary syndrome
more likely occur within the segment of significant
stenosesFalk E. B Heart J. 1983;50:127-134
Richardson et al. Lancet. 1989;2:941-944
Qia et al. J Am Coll Cardiol. 1991;17:1138-1142
Computational Fluid Dynamics: From Lab to Bedside
-
Computational Fluid Dynamics: From Lab to BedsideKaski JC, Chen L, Chester M, Katritsis D. Circulation 1995;92:2058-2065
Characteristics of Stenosis Progressing to Total Occlusion
-
Computational Fluid Dynamics: From Lab to BedsideAnatomy and Haemodynamics May Affect Plaque Rupture
el Fawal MA, et al. Sudden coronary death in Glasgow:
nature and frequency of acute coronary lesions. Br Heart J 1987;57:329-335.
Fox B, et al. Atherosclerosis 1982;41:337-347.
Gibson CM, et al. J Thromb Thrombolysis 2003;15:189-196.
Hochman JS, et al. Am Heart J 1988;116:1217-1222.
Vieweg WV, et al. Cathet Cardiovasc Diagn 1979;5:319-330.
-
LAD LCx RCA
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
Wang, J. C. et al. Circulation 2004;110:278-284
-
RAO 28.5 CAUD 18
RAO 12.3 CRAN 35.3
Computational Fluid Dynamics: From Lab to Bedside3-D coronary reconstruction
-
RAO 28 CAUD 0
LAO 47 CRAN
0
Computational Fluid Dynamics: From Lab to Bedside3-D coronary reconstruction
-
3D
reconstruction2D acquisition
Coronary geometry is acquired by two 2-D images of the coronary tree from different projection angles
Using the concept of epipolar geometry 3-D reconstruction is performed by identifying identical points at the two projections
Andriotis A, Zifan A, Gavaises M, Liatsis P, Pantos I, Theodorakakos A, Efstathopoulos EP, Katritsis D.
A new method of three-dimensional coronary artery reconstruction from X-ray angiography: validation against
a virtual phantom and multislice computed tomography. Catheter Cardiovasc Interv. 2008;71:28-43.
Computational Fluid Dynamics: From Lab to Bedside
-
Computational Fluid Dynamics: From Lab to Bedside
Visual representation of the method used for determining the vessel diameterAndriotis A, Zifan A, Gavaises M, Liatsis P, Pantos I, Theodorakakos A, Efstathopoulos EP, Katritsis D.
A new method of three-dimensional coronary artery reconstruction from X-ray angiography: validation against
a virtual phantom and multislice computed tomography. Catheter Cardiovasc Interv. 2008;71:28-43.
-
The reconstruction algorithm has been validated against multislice detector CT coronary angiography which is considered now days the most accurate non-invasive means to visualize and
characterize the epicardial coronary arteries
Andriotis A, Zifan A, Gavaises M, Liatsis P, Pantos I, Theodorakakos A, Efstathopoulos EP, Katritsis D.
A new method of three-dimensional coronary artery reconstruction from X-ray angiography: validation against
a virtual phantom and multislice computed tomography. Catheter Cardiovasc Interv. 2008;71:28-43.
Computational Fluid Dynamics: From Lab to Bedside
-
Computational Fluid Dynamics: From Lab to Bedside Andriotis A, Zifan A, Gavaises M, Liatsis P, Pantos I, Theodorakakos A, Efstathopoulos EP, Katritsis D.
A new method of three-dimensional coronary artery reconstruction from X-ray angiography: validation against
a virtual phantom and multislice computed tomography. Catheter Cardiovasc Interv. 2008;71:28-43.
-
Katritsis DG, et al. Three-dimensional analysis of the left anteriordescending coronary artery: comparison with
conventional coronary angiograms. Coronary Artery Disease 2008, 19:265–270
Conventional coronary angiography cannot provide accurate estimates of
anatomical parameters, such as distance of a coronary stenosis from the ostium of
the vessel, coronary artery curvature at the site of stenosis, axial deformity and
bending because of ventricular contraction.
Distance of lesion from LAD ostium 14.6mm and vessel curvature at lesion
14.6 mm and 137.20 on 2-D, whereas on 3-D 21.9mm and 1600, respectively
Computational Fluid Dynamics: From Lab to Bedside
-
145 patients were identified with
a LAD lesion, 54 patients with a LCx lesion, and 76
patients with a RCA lesion responsible for the clinical
presentation.
Katritsis et al. Anatomic Characteristics of Culprit Sites in Acute Coronary Syndromes. J Interven
Cardiol 2008;21:140–150
The presence of angulation on the lesion increased the risk of an ACS 1.92
times (95% confidence interval [CI] 1.9–3.07)
The presence of bifurcation after the lesion increased the risk 1.65 times (95%
CI1.04–2.62)
Angulated lesions located within the first 40 mm from the ostium and before a
bifurcation presented an 11-fold increased risk for an ACS.
Computational Fluid Dynamics: From Lab to Bedside
-
RAO CranialRAO Caudal
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
-
RAO Cranial LAO Caudal
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
-
Diastole Systole
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
-
Katritsis DG et al. Three-dimensional analysis of vulnerable segments in the left
anterior descending artery. Coron Artery Dis. 2009;20:199-206.
Coronary angiograms of 76 consecutive patients with an
anterior STEMI and a recanalized LAD were reconstructed
in the three-dimensional space, and compared with
angiograms of 76 patients with stable coronary artery
disease (SCAD) and significant LAD stenosis.
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
-
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
Katritsis DG et al. Three-dimensional analysis of vulnerable segments in the left
anterior descending artery. Coron Artery Dis. 2009;20:199-206.
-
Dominant anatomic models of STEMI and stable coronary artery disease
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
Katritsis DG et al. Three-dimensional analysis of vulnerable segments in the left
anterior descending artery. Coron Artery Dis. 2009;20:199-206.
-
Hemodynamic and mechanical forces acting on
vulnerable plaque:1. Wall shear stress
2. Circumferential wall stress and shear failure
3. Mechanical shear failure
4. Arterial wall collapse
5. Circumferential bending
6. Longitudinal flexion
7. Vasospasm
8. Fatigue failure
Computational Fluid Dynamics: From Lab to Bedside Anatomy and Haemodynamics May Affect Plaque Rupture
-
The hemodynamic factor that has been
most extensively studied and associated
with the localization, generation and
growth of atherosclerotic lesions is wall
(or endothelial) shear stress (WSS), ie
the tangential force exerted on the vessel
wall by blood flow due to the viscous
properties of blood (μ).
Illustration of the WSS acting on the
vascular endothelium
dr
duWSS
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Katritsis DG, Kaiktsis L, Chaniotis A, Pantos J, Efstathopoulos EP, Marmarelis V.
Wall shear stress: theoretical considerations and methods of measurement. Prog Cardiovasc Dis. 2007;49:307-29.
-
Circumferential Wall Stress
The circumferential wall stress is a tensile stress which is induced on the vessel wall by the transmural blood pressure and it is several orders of magnitude stronger than the wall shear stress
. For a given intraluminal pressure, the circumferential stress on a 50% stenosis is five times greater than on a 90% stenosis.Consequently, mildly or moderately stenotic plaques are generally stressed more than severely stenotic plaques and could therefore be more prone to rupture
Circumferential Stress Failure
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Katritsis DG, Kaiktsis L, Chaniotis A, Pantos J, Efstathopoulos EP, Marmarelis V.
Wall shear stress: theoretical considerations and methods of measurement. Prog Cardiovasc Dis. 2007;49:307-29.
-
Mechanical Shear Failure
Mechanical shear stress is the shearing stress that is exerted between adjacent layers of the vessel induced by the circumferential elongation due to circumferential stresses
Mechanical shear failure of the vessel occurs when vessel layers separate and slide relative to one another and when the extracellular matrix, which functions as the glue holding these layers together, cannot withstand the shear stress
Shear Failure
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Katritsis DG, Kaiktsis L, Chaniotis A, Pantos J, Efstathopoulos EP, Marmarelis V.
Wall shear stress: theoretical considerations and methods of measurement. Prog Cardiovasc Dis. 2007;49:307-29.
-
Arterial Wall CollapseAccording to the Bernoulli principle, at sites of artery stenosis, blood flow causes a
drop in static pressure within the throat of the stenosis.
The collapse of arteries may produce highly compressive stresses which arteries cannot withstand since they are typically constructed for tension only. Compressive stress is particularly determinant in that it may induce a crack or cavity
Experimental study of wall
collapse using a latex tube model
with induced stenosis
Stenosis
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Katritsis DG, Kaiktsis L, Chaniotis A, Pantos J, Efstathopoulos EP, Marmarelis V.
Wall shear stress: theoretical considerations and methods of measurement. Prog Cardiovasc Dis. 2007;49:307-29.
-
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Chatzizisis YS, et al. J Am Coll Cardiol. 2007;49:2379-93
-
The endothelial cytoskeleton transmits the shear forces to the focal adhesions located at
the basal endothelial surface, where a downstream intracellular signaling cascade starts.
Computational Fluid Dynamics: From Lab to BedsideFlow Must Have a Role
Davies KA, et al Annu Rev Physiol 19977; 59:527–549
-
Low endothelial shear stress promoting atherogenesis, atherosclerotic plaque formation
and progression, and vascular remodeling.
Computational Fluid Dynamics: From Lab to BedsideLow SS promotes atherogenesis
Chatzizisis YS, et al. J Am Coll Cardiol. 2007;49:2379-93
-
WSS is an important determinant of endothelial function and phenotype. High WSS induces endothelial
quiescence and an atheroprotective gene expression profile while low WSS stimulates an atherogenic
phenotype.
Low shear– mediated recruitment and activation of monocytes, increased
vasoconstriction and paracrine growth stimulation of the vessel wall constituents,
increased oxidant state, and increased apoptosis and cellular turnover.
Illustration of the arterial phenotype switch from atheroprotective (left) to atherogenic (rightl) induced by low WSS
conditions
Malek et al. Jama.1999;282:2035-2042
Computational Fluid Dynamics: From Lab to Bedside
-
The complex three-dimensional vascular geometry, the blood molecular viscosity and the
flow pulsation constitute the major determinants of intravascular blood flow patterns and
shear stress.
In relatively straight vessel segments WSS is
pulsatile and unidirectional and yields a positive
time-averaged value over the cardiac cycle
In geometrically irregular regions, pulsatile
flow generates low or oscillatory WSS
Low and oscillatory WSS
-Direction: bidirectional
-Magnitude: low time-
averaged
Normal and
pulsatile WSS
-Direction:
uniderectional
-Magnitude:
physiologic time-
averaged
Ku DN et al. Arteriosclerosis. 1985;5: 293-302
Computational Fluid Dynamics: From Lab to Bedside
-
Atherogenesis preferentially involves the outer
walls of vessel bifurcations, the inner walls of
arterial curvature and points of blood flow
recirculation and stasis. In these geometrically
predisposed locations, WSS is significantly lower
in magnitude than adjacent regions.
Asakura T, Karino T. Circ Res. 1990;66:1045-1066
Computational Fluid Dynamics: From Lab to Bedside
Atherosclerotic lesions co-localize with regions of low and oscillatory WSS
-
Chatzizisis et al. Journal of the American College of Cardiology; 2007, 49:2379-
2393.
•In susceptible to atherosclerosis regions
(e.g. branches, arterial curvatures) where
WSS is low, an early fibroatheroma is
formed
•The vascular response (compensatory
expansive, constrictive or excessive
expansive remodelling) to that early
fibroatheroma likely determines the
subsequent natural history of the plaque
•% reported are based on IVUS studies
Computational Fluid Dynamics: From Lab to BedsideTHE EVOLUTION OF CORONARY PLAQUES
-
Computational Fluid Dynamics: From Lab to Bedside
High SS is associated with plaque erosion and rupture
and causes platelet activation
Bluestein D, et al. Annals of biomedical engineering. 1999;27:763-773
Nesbitt WS, et al. Journal of molecular medicine (Berlin, Germany). 2006;84:989-995
-
Computational Fluid Dynamics: From Lab to BedsideKoskinas KC, Chatzizisis YS, Antoniadis AP, Giannoglou GD. Role of endothelial shear stress in stent
restenosis and thrombosis: pathophysiologic mechanisms and implications for clinical translation.
J Am Coll Cardiol. 2012;59:1337-49.
-
Specific anatomic conditions identified at sites of coronary occlusions, such as the presence of bifurcation branches, create zones of vortices and flow recirculation.
These flow disturbances promote atherosclerosis and plaque development as well as thrombus formation and may affect the clinical outcome of coronary plaque rupture and potentially the incidence of MI.
Identification of such coronary segments may indicate targets of preventive intervention (plaque passivation?).
Computational Fluid Dynamics: From Lab to Bedside It is the flow stupid…..
-
Computational Fluid Dynamics: From Lab to BedsideThe Navier Stokes Equations
0uρt
ρ
0uuρt
uρ
S
TuuμIuμ3
2PS
Mass conservation equation:
where ρ is the density, t the time,u the velocity vector.
Momentum conservation equation:
-
-20
0
20
40
60
80
100
120
0.0 0.2 0.4 0.6 0.8
Time (s)
Flo
w R
ate
(m
l/m
in)
Steady -state
-20
0
20
40
60
80
100
120
0.0 0.2 0.4 0.6 0.8
Time (s)
Flo
w R
ate
(m
l/m
in)
Steady -state
0.0 0.25 0.5 0.75
Non Dimensional Time
1.0
Computational Fluid Dynamics: From Lab to BedsideComputer Models
-
Computational Fluid Dynamics: From Lab to BedsideComputational Fluid Dynamics (CFD) is a powerful tool
which can mathematically access important hemodynamic features such as local velocity, shear stress and flow patterns (vortices, recirculation)
Katritsis D et al. Prog Cardiovasc Dis. 2007;49:307-29.
-
Computational Fluid Dynamics: From Lab to Bedside
Katritsis D et al. Prog Cardiovasc Dis. 2007;49:307-29.
Wall Shear Stress Distribution
-
Vortex Formation and Recirculation
Blood Flow Streamlines
Computational Fluid Dynamics: From Lab to Bedside
Katritsis D et al. Prog Cardiovasc Dis. 2007;49:307-29.
-
Computational Fluid Dynamics: From Lab to Bedside
Katritsis D et al. Prog Cardiovasc Dis. 2007;49:307-29.
Real-time Flow Real-time Shear stress
-
Myocardial infarctionPlaque rupture AND Thrombosis
IVUS studies have suggested that plaque rupture itself
may not necessarily lead to clinical events.
A high incidence of multiple plaque ruptures remote
from the culprit lesion in ACS patients has been reported,
and plaque ruptures have also been identified in patients
with stable angina or asymptomatic ischemia.
Rioufol G et al.. Circulation. 2002;106:804-808
Hong et al. Circulation. 2004;110:928-933
Maehara et al. J Am Coll Cardiol. 2002;40:904-910
Maehara et al. J Am Coll Cardiol. 2002;40:904
Computational Fluid Dynamics: From Lab to Bedside
-
Effect of Flow on Potential Thrombosis?
Computational Fluid Dynamics: From Lab to BedsideFrom plaque rupture to thrombosis
-
Coronary angiograms of 186 consecutive patients (original sample) with an
anterior ST elevation myocardial infarction (STEMI) and a recanalized LAD
were reconstructed in the three-dimensional space. Culprit lesions were
compared with 293 stable LAD coronary stenoses on the same patients.
Katritsis DG, Efstathopoulos EP, Pantos I, Tzanalaridou E, De Waha A, Siontis GC, Toutouzas K, Redwood S, Kastrati A,
Stefanadis C. Ruptured versus stable plaques in human coronary arteries. Coron Artery Dis. 2011;22:345-51.
Computational Fluid Dynamics: From Lab to BedsideFrom plaque rupture to thrombosis
-
Anatomic parametersStable lesions
N=293
Culprit
lesions
N=186
P
Lesion reference diameter (mm) 2.8 ± 0.7 3.1 ± 0.6
-
• The majority of culprit lesions occurred between 20 and 40 mm from the LAD ostium while the majority of stable lesions were found
in distance >60 mm (p
-
Points
Lesion length
15 mm
0
1.5
Curvature on systole
>165o
-
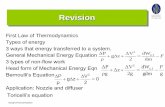
Figure 1. General model of the
LAD and side branches
Model of stenosis
associated with MI. The
stenosis involves two side
branches, one upstream
and one downstream the
most stenotic site.
Model of stenosis
associated with MI. The
stenosis involves one side
branch downstream the
most stenotic site.
Model of stenosis
associated stable CAD.
The stenosis does not
involve any side branch.
Derived dominant models of vulnerable and stable coronary lesions
Katritsis DG, Efstathopoulos EP, Pantos I, Tzanalaridou E, De Waha A, Siontis GC, Toutouzas K, Redwood S, Kastrati A,
Stefanadis C. Ruptured versus stable plaques in human coronary arteries. Coron Artery Dis. 2011;22:345-51.
Computational Fluid Dynamics: From Lab to BedsideFrom plaque rupture to thrombosis
-
• Vulnerable plaque
– Characteristic histology
• Vulnerable blood
– Platelet hyperactivity, procoagulant states
• Vulnerable patient
– Prominent risk factors for IHD
• Vulnerable coronary segment
Computational Fluid Dynamics: From Lab to BedsideFrom plaque rupture to thrombosis
-
Scope:
To study intracoronary hemodynamics and particularly the formation of zones of flow recirculation and stagnation
Facts:
o The relationship of hemodynamic factors and thrombus formation due to platelet deposition has been previously investigated in various experimental and computational studies
o These studies showed that the flow condition at the stenosis promote platelet activation and aggregation
o If recirculation zones are present downstream the stenosis, the aggregation of platelets is further promoted and the motion of the platelets bring them into contact with the arterial wall
-
Based on the analysis of the anatomical characteristics of 152 coronary angiograms of
vulnerable and stable coronary lesions, the following three dominant models were derived
3D geometries were consequently generated incorporating a lesion with varying diameter
% stenosis
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
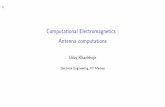
STEMI 1
50% stenosis
50% stenosis
SCS
50% stenosis
STEMI 2
Computational Fluid Dynamics: From Lab to BedsideEffect of % stenosis on flow
Katritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
For the 50% stenosis there is flow recirculation at
the ostium of the side branch in both STEMI
geometries (blue arrows), whereas no recirculation
is seen in the SCS model
No recirculation zones are noted at STEMI for
0% and 20% stenosis
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
No recirculation zones are noted at STEMI for 0% and 20% stenosis
-
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
No recirculation zones are noted at SCAD for 50% stenosis
-
For the 50% stenosis there is flow recirculation at the ostium of the side branch in both STEMI geometries
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
For the 50% stenosis there is flow recirculation at the ostium of the side branch in both STEMI geometries
-
For the 50% stenosis, in STEMI 2 geometry the recirculation vortex virtually blocks the
entry into the side branch
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
For the 90% stenosis, flow recirculation
occurs in both main (red arrow) and side
branch (blue arrow) after the stenosis.
In the SCS geometry, recirculation is also
seen in the post-stenotic lumen of the main
branch (red arrow) despite the absence of
bifurcation
Computational Fluid Dynamics: From Lab to BedsideEffect of % stenosis on flow
Katritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
For the 90% stenosis, flow recirculation occurs in both main and side branch after the
stenosis.
Computational Fluid Dynamics: From Lab to BedsideEffect of % stenosis on flow
Katritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
In the SCS geometry, recirculation is also seen in the post-stenotic lumen of the main branch
despite the absence of bifurcation
Computational Fluid Dynamics: From Lab to BedsideEffect of % stenosis on flow
Katritsis DG, Theodorakakos A, Pantos I, Andriotis A, Efstathopoulos EP, Siontis G, Karcanias N, Redwood S, Gavaises M.
Vortex formation and recirculation zones in left anterior descending artery stenoses: computational fluid dynamics analysis.
Phys Med Biol. 2010;55:1395-411.
-
BIFURCATION STENTINGClassifications
Chen-Gao
-
BIFURCATION STENTINGTreatment Modes
T-stenting
Y-stenting
Culotte
Crush
Reverse Crush
Kissing Stents
Main branch stenting
Main branch stenting with kissing
balloons
-
CulotteSKSCrush
BIFURCATION STENTINGTreatment Modes
-
Computational Fluid Dynamics: From Lab to BedsideDouble Stenting in Bifurcations
Katritsis DG, Siontis GC, Ioannidis JP. Double versus single stenting for coronary bifurcation lesions: a meta-
analysis. Circ Cardiovasc Interv. 2009;2:409-15.
-
Computational Fluid Dynamics: From Lab to BedsideDouble Stenting in Bifurcations
Katritsis DG, Siontis GC, Ioannidis JP. Double versus single stenting for coronary bifurcation lesions: a meta-
analysis. Circ Cardiovasc Interv. 2009;2:409-15.
-
Considered bifurcation model
Considered single (left panel) and double
(right panel) bifurcation stenting techniques
Considered coronary DES
Computational Fluid Dynamics: From Lab to BedsideKatritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
-
High TAWSS values, low OSI values, and low tr values are considered hemodynamically favorable
Katritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
Computational Fluid Dynamics: From Lab to Bedside
-
Streamlines WSS distribution
Computational Fluid Dynamics: From Lab to Bedside
Main branch stentingKatritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
-
Katritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
Computational Fluid Dynamics: From Lab to Bedside
Main branch stenting
-
BIFURCATION STENTINGFate of side branches
- Dissected or even occluded side branches are usually clinically silent
- Probably do not affect long-term clinical event-free survival
- The majority of side branches (up to 90%) reappear at follow-up
Alfonso et al. J Am Coll Cardiol. 2000;36:1549-1556.
Tanabe et al. Am J Cardiol. 2002;90:937-941
Pan et al. Am Heart J. 2004;148:857-864.
-
Computational Fluid Dynamics: From Lab to Bedside
Culotte - Stenting
Katritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
-
Computational Fluid Dynamics: From Lab to Bedside
T - StentingKatritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
-
Katritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
Computational Fluid Dynamics: From Lab to Bedside
Crush Stenting
-
Katritsis DG, Theodorakakos A, Pantos I, Gavaises M, Karcanias N,. Efstathopoulos EP. Flow Patterns at
Stented Coronary Bifurcations: Computational Fluid Dynamics Analysis. Circulation AE (In press)
Computational Fluid Dynamics: From Lab to Bedside
Results:
Single stenting of the main branch with our without balloon angioplasty of the
side branch offers hemodynamic advantages over double stenting.
When double stenting is considered, the crush technique with the use of a thin
strut stent results in improved hemodynamics compared to culotte or T stenting.
-
Computational Fluid Dynamics: From Lab to BedsideKoskinas KC, Chatzizisis YS, Antoniadis AP, Giannoglou GD. Role of endothelial shear stress in stent
restenosis and thrombosis: pathophysiologic mechanisms and implications for clinical translation.
J Am Coll Cardiol. 2012;59:1337-49.
Role of endothelial shear stress
in stent restenosis and thrombosis
-
1. Non-newtonian fluid (proteins, blood cells, paltelets, fibrinogen…).
1. Pulsatile flow
3. Cardiac motion has minimal impact on CFD-assessed flowTheodorakakos A, Gavaises M, Andriotis A, Zifan A, Liatsis P, Pantos I, Efstathopoulos EP, Katritsis D.
Simulation of cardiac motion on non-Newtonian, pulsating flow development in the human left anterior
descending coronary artery. Phys Med Biol. 2008;53:4875-92.
Computational Fluid Dynamics: From Lab to BedsideExperimental Conditions
-
Left: superimposed centerlines at coronary angiography at diastole, systole and one intermediate time
and Right: layout of the moving geometry simulated for 5 time steps as seen from two different views
Theodorakakos A, Gavaises M, Andriotis A, Zifan A, Liatsis P, Pantos I, Efstathopoulos EP, Katritsis D. Simulation of cardiac
motion on non-Newtonian, pulsating flow development in the human left anterior descending coronary artery. Phys Med Biol.
2008;53:4875-92.
Computational Fluid Dynamics: From Lab to Bedside
-
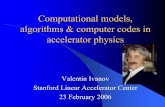
Flow streamlines colored with the velocity magnitude in the location downstream of the
atheromatous stenosis during the heart cycle; the recirculation zones induced at the
trifurcation point just downstream of the stenosis due to the pulsating flow are observed
Systole
Diastole
Computational Fluid Dynamics: From Lab to BedsideTheodorakakos A, Gavaises M, Andriotis A, Zifan A, Liatsis P, Pantos I, Efstathopoulos EP, Katritsis D. Simulation of cardiac
motion on non-Newtonian, pulsating flow development in the human left anterior descending coronary artery. Phys Med Biol.
2008;53:4875-92.
-
Shear stress distribution at systole and diastole as seen from two different views for the
moving and non-moving arterial tree
Systole
Diastole
Non-moving Non-movingMoving Moving
Computational Fluid Dynamics: From Lab to BedsideTheodorakakos A, Gavaises M, Andriotis A, Zifan A, Liatsis P, Pantos I, Efstathopoulos EP, Katritsis D. Simulation of cardiac
motion on non-Newtonian, pulsating flow development in the human left anterior descending coronary artery. Phys Med Biol.
2008;53:4875-92.
-
The spatial distribution of WSS at the area of the stenosis is very similar
between the stationary and the moving coronary trees. However, the absolute
values of WSS differ in the two cases.
Predictions indicate that myocardial motion has only a minor effect on flow
distribution within the arterial tree relative to the effect of the blood pressure
pulse
Computational Fluid Dynamics: From Lab to BedsideTheodorakakos A, Gavaises M, Andriotis A, Zifan A, Liatsis P, Pantos I, Efstathopoulos EP, Katritsis D. Simulation of cardiac
motion on non-Newtonian, pulsating flow development in the human left anterior descending coronary artery. Phys Med Biol.
2008;53:4875-92.
-
PIV study - laser sheet and two high resolutiondigital cameras view the intersection of the vessel with the laser beam
(a) Scanning electron microscopy image of fibrin mesh (blue) with trapped platelets (purple)
and red blood cells (red) and
(b) b) Multi-scale model of thrombus development
(a) (b)
1 - Computational 2 - Experimental
The Future: Computational vs Experimental
Flow Analysis
-
Blood flow and WSS (3 methodologies) throughout the cardiac cycle for a specific patient
WSS measurements based on the maximum blood velocity show large deviations with respect to the measurements that use the mean blood volume flow or the mean blood velocity.
Therefore, in-vivo WSS measurements require careful selection of the applied methodology
The Future: MRI vs CFD
-
Coronary Flow Research Unit, Athens Euroclinic (D. Katritsis, J. Pantos)
Dept of Radiology, Attikon Hosp, Athens Univ Med School (E. Efstathopoulos)
Fluid Research Co. Athens (A. Theodorakakos)
The City University, London, UK (M. Gavaises, N. Karcanias, D. Katritsis)
St Thomas’ Hospital, London, UK (S. Redwood, D. Katritsis)
Cardiology Dept, Munich University, Germany ( A. Kastrati)
University of Athens Medical School, Greece (C. Stefanadis)
Computational Fluid Dynamics: From Lab to BedsideThe Team
-
Computational Fluid Dynamics: From Lab to BedsideConclusions
Myocardial infarction, the leading cause of death in the developed world has not been studied from the perspective of coronary flow.
CFD and MRI allow studying of coronary flow.
Novel techniques and models that allow simulation of physiologic conditions are necessary for this purpose.
A new era has begun….