CD34 + fibrocytes in normal cervical stroma, cervical intraepithelial neoplasia III, and invasive...
5
Abstract CD34 + fibrocytes are widely distributed in normal connective tissues but have been reported to be absent within the stroma associated with invasive carci- nomas. In the present study we investigated the presence and distribution of CD34 + fibrocytes and α-smooth mus- cle actin (α-SMA) positive myofibroblasts in cervical in- traepithelial neoplasia III (CIN III; n=8), invasive carci- noma of the cervix (n=18) and adjacent normal cervical stroma. Normal cervical stroma and the stroma adjacent to CIN III disclosed a dense network of CD34 + fibro- cytes, whereas the stroma of invasive carcinoma was virtually free of this cell population. Early stromal inva- sion by squamous carcinoma was characterized by a focal loss of CD34 + fibrocytes. α-SMA-positive myofi- broblasts were not seen in the normal cervical stroma but occurred in six of eight cases of CIN III adjacent to the atypical epithelium. The stroma of invasive carcinoma was made up of large amounts of haphazardly arranged α-SMA-positive myofibroblasts. In the setting of the present study, a loss of CD34 + fibrocytes was specific for stromal alterations associated with invasive carcinoma and proved to be a sensitive tool in detecting small foci of stromal invasion. Therefore, detection of a loss of CD34 + fibrocytes may constitute an adjunctive tool in detecting (1) early stromal invasion and (2) invasive carcinoma in small biopsy specimens. Moreover, the present study shows that CD34 + fibrocytes and myofi- broblasts play an important role in stromal remodeling associated with invasive squamous cell carcinoma of the cervix. Keywords Cervix · Fibrocytes · Intraepithelial neoplasias · Squamous cell carcinoma · CD34 Introduction CD34 + fibrocytes, also referred to as dendritic interstitial cells [11, 12, 20], occur in the connective tissue compart- ment of various anatomical locations such as the skin [7, 12, 18], gastrointestinal [10, 11, 13, 15] and urogenital [8] tracts, breast [1, 9, 14, 19], pancreas [2], thyroid [21], salivary glands [16] and peripheral nervous system [6]. Morphologically CD34 + fibrocytes show slender cyto- plasmic processes closely interwoven with those of neighboring CD34 + fibrocytes leading to the descriptive term “CD34-positive reticular network” [1, 2, 3, 17, 19, 20, 21]. At the electron microscopic level, CD34 + fibro- cytes and mononuclear cells disclose a close spatial association leading to the hypothesis that CD34 + fibro- cytes might be involved in specific immune surveillance [19, 20]. The latter assumption is highlighted by the fact that at least a subpopulation of CD34 + fibrocytes ex- presses MHC II molecules and CD80 [4]. Moreover, the stroma of invasive carcinomas lacks CD34 + fibrocytes whereas the corresponding normal tissues harbor large amounts of this cell type [1, 2, 10, 11]. Recently, similar findings were reported for salivary gland tumors leading to the authors’ suggestion that CD34 + fibrocytes might be associated with the regulation of tumor growth by mechanisms that remain to be elucidated [16]. However, the loss of CD34 expression in the stroma associated with invasive carcinoma is in part accompanied by a gain of α-smooth muscle actin (α-SMA) positive myofi- broblasts which have been detected in the stroma of colorectal adenocarcinoma [10], ductal adenocarcinoma of the pancreas [2] and invasive ductal breast cancer [1]. In accordance with the aforementioned anatomical sites, the stroma of the uterine cervix has also been report- ed to be in part composed of CD34 + fibrocytes [8]. The significance of this finding has to be further evaluated since the cited study was exclusively based on the analysis of normal cervical tissues. We therefore undertook the present study to analyze the occurrence of CD34 + fibro- cytes in the cervical stroma with special respect to under- lying pre-invasive and invasive carcinomas of the cervix. P.J. Barth ( ✉ ) · A. Ramaswamy · R. Moll Institute of Pathology, Philipps-University Marburg, Baldingerstrasse, 35033 Marburg, Germany e-mail: [email protected] Tel.: +49-06421-2862465, Fax: +49-06421-2865640 Virchows Arch (2002) 441:564–568 DOI 10.1007/s00428-002-0713-y ORIGINAL ARTICLE Peter J. Barth · Annette Ramaswamy · Roland Moll CD34 + fibrocytes in normal cervical stroma, cervical intraepithelial neoplasia III, and invasive squamous cell carcinoma of the cervix uteri Received: 21 May 2002 / Accepted: 12 August 2002 / Published online: 16 October 2002 © Springer-Verlag 2002
Transcript of CD34 + fibrocytes in normal cervical stroma, cervical intraepithelial neoplasia III, and invasive...

Abstract CD34+ fibrocytes are widely distributed innormal connective tissues but have been reported to beabsent within the stroma associated with invasive carci-nomas. In the present study we investigated the presenceand distribution of CD34+ fibrocytes and α-smooth mus-cle actin (α-SMA) positive myofibroblasts in cervical in-traepithelial neoplasia III (CIN III; n=8), invasive carci-noma of the cervix (n=18) and adjacent normal cervicalstroma. Normal cervical stroma and the stroma adjacentto CIN III disclosed a dense network of CD34+ fibro-cytes, whereas the stroma of invasive carcinoma was virtually free of this cell population. Early stromal inva-sion by squamous carcinoma was characterized by a focal loss of CD34+ fibrocytes. α-SMA-positive myofi-broblasts were not seen in the normal cervical stroma butoccurred in six of eight cases of CIN III adjacent to theatypical epithelium. The stroma of invasive carcinomawas made up of large amounts of haphazardly arrangedα-SMA-positive myofibroblasts. In the setting of thepresent study, a loss of CD34+ fibrocytes was specific forstromal alterations associated with invasive carcinomaand proved to be a sensitive tool in detecting small fociof stromal invasion. Therefore, detection of a loss ofCD34+ fibrocytes may constitute an adjunctive tool indetecting (1) early stromal invasion and (2) invasive carcinoma in small biopsy specimens. Moreover, thepresent study shows that CD34+ fibrocytes and myofi-broblasts play an important role in stromal remodelingassociated with invasive squamous cell carcinoma of thecervix.
Keywords Cervix · Fibrocytes · Intraepithelial neoplasias · Squamous cell carcinoma · CD34
Introduction
CD34+ fibrocytes, also referred to as dendritic interstitialcells [11, 12, 20], occur in the connective tissue compart-ment of various anatomical locations such as the skin [7,12, 18], gastrointestinal [10, 11, 13, 15] and urogenital[8] tracts, breast [1, 9, 14, 19], pancreas [2], thyroid [21],salivary glands [16] and peripheral nervous system [6].Morphologically CD34+ fibrocytes show slender cyto-plasmic processes closely interwoven with those ofneighboring CD34+ fibrocytes leading to the descriptiveterm “CD34-positive reticular network” [1, 2, 3, 17, 19,20, 21]. At the electron microscopic level, CD34+ fibro-cytes and mononuclear cells disclose a close spatial association leading to the hypothesis that CD34+ fibro-cytes might be involved in specific immune surveillance[19, 20]. The latter assumption is highlighted by the factthat at least a subpopulation of CD34+ fibrocytes ex-presses MHC II molecules and CD80 [4]. Moreover, thestroma of invasive carcinomas lacks CD34+ fibrocyteswhereas the corresponding normal tissues harbor largeamounts of this cell type [1, 2, 10, 11]. Recently, similarfindings were reported for salivary gland tumors leadingto the authors’ suggestion that CD34+ fibrocytes mightbe associated with the regulation of tumor growth bymechanisms that remain to be elucidated [16]. However,the loss of CD34 expression in the stroma associatedwith invasive carcinoma is in part accompanied by again of α-smooth muscle actin (α-SMA) positive myofi-broblasts which have been detected in the stroma of colorectal adenocarcinoma [10], ductal adenocarcinomaof the pancreas [2] and invasive ductal breast cancer [1].
In accordance with the aforementioned anatomicalsites, the stroma of the uterine cervix has also been report-ed to be in part composed of CD34+ fibrocytes [8]. Thesignificance of this finding has to be further evaluatedsince the cited study was exclusively based on the analysisof normal cervical tissues. We therefore undertook thepresent study to analyze the occurrence of CD34+ fibro-cytes in the cervical stroma with special respect to under-lying pre-invasive and invasive carcinomas of the cervix.
P.J. Barth (✉) · A. Ramaswamy · R. MollInstitute of Pathology, Philipps-University Marburg, Baldingerstrasse, 35033 Marburg, Germanye-mail: [email protected].: +49-06421-2862465, Fax: +49-06421-2865640
Virchows Arch (2002) 441:564–568DOI 10.1007/s00428-002-0713-y
O R I G I N A L A RT I C L E
Peter J. Barth · Annette Ramaswamy · Roland Moll
CD34+ fibrocytes in normal cervical stroma, cervical intraepithelialneoplasia III, and invasive squamous cell carcinoma of the cervix uteri
Received: 21 May 2002 / Accepted: 12 August 2002 / Published online: 16 October 2002© Springer-Verlag 2002
Verwendete Distiller 5.0.x Joboptions
Dieser Report wurde automatisch mit Hilfe der Adobe Acrobat Distiller Erweiterung "Distiller Secrets v1.0.5" der IMPRESSED GmbH erstellt. Sie koennen diese Startup-Datei für die Distiller Versionen 4.0.5 und 5.0.x kostenlos unter http://www.impressed.de herunterladen. ALLGEMEIN ---------------------------------------- Dateioptionen: Kompatibilität: PDF 1.2 Für schnelle Web-Anzeige optimieren: Ja Piktogramme einbetten: Ja Seiten automatisch drehen: Nein Seiten von: 1 Seiten bis: Alle Seiten Bund: Links Auflösung: [ 600 600 ] dpi Papierformat: [ 595 785 ] Punkt KOMPRIMIERUNG ---------------------------------------- Farbbilder: Downsampling: Ja Berechnungsmethode: Bikubische Neuberechnung Downsample-Auflösung: 150 dpi Downsampling für Bilder über: 225 dpi Komprimieren: Ja Automatische Bestimmung der Komprimierungsart: Ja JPEG-Qualität: Mittel Bitanzahl pro Pixel: Wie Original Bit Graustufenbilder: Downsampling: Ja Berechnungsmethode: Bikubische Neuberechnung Downsample-Auflösung: 150 dpi Downsampling für Bilder über: 225 dpi Komprimieren: Ja Automatische Bestimmung der Komprimierungsart: Ja JPEG-Qualität: Mittel Bitanzahl pro Pixel: Wie Original Bit Schwarzweiß-Bilder: Downsampling: Ja Berechnungsmethode: Bikubische Neuberechnung Downsample-Auflösung: 600 dpi Downsampling für Bilder über: 900 dpi Komprimieren: Ja Komprimierungsart: CCITT CCITT-Gruppe: 4 Graustufen glätten: Nein Text und Vektorgrafiken komprimieren: Ja SCHRIFTEN ---------------------------------------- Alle Schriften einbetten: Ja Untergruppen aller eingebetteten Schriften: Nein Wenn Einbetten fehlschlägt: Warnen und weiter Einbetten: Immer einbetten: [ ] Nie einbetten: [ ] FARBE(N) ---------------------------------------- Farbmanagement: Farbumrechnungsmethode: Alle Farben zu sRGB konvertieren Methode: Standard Arbeitsbereiche: Graustufen ICC-Profil: RGB ICC-Profil: sRGB IEC61966-2.1 CMYK ICC-Profil: U.S. Web Coated (SWOP) v2 Geräteabhängige Daten: Einstellungen für Überdrucken beibehalten: Ja Unterfarbreduktion und Schwarzaufbau beibehalten: Ja Transferfunktionen: Anwenden Rastereinstellungen beibehalten: Ja ERWEITERT ---------------------------------------- Optionen: Prolog/Epilog verwenden: Nein PostScript-Datei darf Einstellungen überschreiben: Ja Level 2 copypage-Semantik beibehalten: Ja Portable Job Ticket in PDF-Datei speichern: Nein Illustrator-Überdruckmodus: Ja Farbverläufe zu weichen Nuancen konvertieren: Nein ASCII-Format: Nein Document Structuring Conventions (DSC): DSC-Kommentare verarbeiten: Nein ANDERE ---------------------------------------- Distiller-Kern Version: 5000 ZIP-Komprimierung verwenden: Ja Optimierungen deaktivieren: Nein Bildspeicher: 524288 Byte Farbbilder glätten: Nein Graustufenbilder glätten: Nein Bilder (< 257 Farben) in indizierten Farbraum konvertieren: Ja sRGB ICC-Profil: sRGB IEC61966-2.1 ENDE DES REPORTS ---------------------------------------- IMPRESSED GmbH Bahrenfelder Chaussee 49 22761 Hamburg, Germany Tel. +49 40 897189-0 Fax +49 40 897189-71 Email: [email protected] Web: www.impressed.de
Adobe Acrobat Distiller 5.0.x Joboption Datei
<< /ColorSettingsFile () /AntiAliasMonoImages false /CannotEmbedFontPolicy /Warning /ParseDSCComments false /DoThumbnails true /CompressPages true /CalRGBProfile (sRGB IEC61966-2.1) /MaxSubsetPct 100 /EncodeColorImages true /GrayImageFilter /DCTEncode /Optimize true /ParseDSCCommentsForDocInfo false /EmitDSCWarnings false /CalGrayProfile () /NeverEmbed [ ] /GrayImageDownsampleThreshold 1.5 /UsePrologue false /GrayImageDict << /QFactor 0.9 /Blend 1 /HSamples [ 2 1 1 2 ] /VSamples [ 2 1 1 2 ] >> /AutoFilterColorImages true /sRGBProfile (sRGB IEC61966-2.1) /ColorImageDepth -1 /PreserveOverprintSettings true /AutoRotatePages /None /UCRandBGInfo /Preserve /EmbedAllFonts true /CompatibilityLevel 1.2 /StartPage 1 /AntiAliasColorImages false /CreateJobTicket false /ConvertImagesToIndexed true /ColorImageDownsampleType /Bicubic /ColorImageDownsampleThreshold 1.5 /MonoImageDownsampleType /Bicubic /DetectBlends false /GrayImageDownsampleType /Bicubic /PreserveEPSInfo false /GrayACSImageDict << /VSamples [ 2 1 1 2 ] /QFactor 0.76 /Blend 1 /HSamples [ 2 1 1 2 ] /ColorTransform 1 >> /ColorACSImageDict << /VSamples [ 2 1 1 2 ] /QFactor 0.76 /Blend 1 /HSamples [ 2 1 1 2 ] /ColorTransform 1 >> /PreserveCopyPage true /EncodeMonoImages true /ColorConversionStrategy /sRGB /PreserveOPIComments false /AntiAliasGrayImages false /GrayImageDepth -1 /ColorImageResolution 150 /EndPage -1 /AutoPositionEPSFiles false /MonoImageDepth -1 /TransferFunctionInfo /Apply /EncodeGrayImages true /DownsampleGrayImages true /DownsampleMonoImages true /DownsampleColorImages true /MonoImageDownsampleThreshold 1.5 /MonoImageDict << /K -1 >> /Binding /Left /CalCMYKProfile (U.S. Web Coated (SWOP) v2) /MonoImageResolution 600 /AutoFilterGrayImages true /AlwaysEmbed [ ] /ImageMemory 524288 /SubsetFonts false /DefaultRenderingIntent /Default /OPM 1 /MonoImageFilter /CCITTFaxEncode /GrayImageResolution 150 /ColorImageFilter /DCTEncode /PreserveHalftoneInfo true /ColorImageDict << /QFactor 0.9 /Blend 1 /HSamples [ 2 1 1 2 ] /VSamples [ 2 1 1 2 ] >> /ASCII85EncodePages false /LockDistillerParams false >> setdistillerparams << /PageSize [ 595.276 841.890 ] /HWResolution [ 600 600 ] >> setpagedevice

565
Materials and methods
This study comprised a total of 25 females ranging in age between21 years and 82 years (average 42.5 years) who underwent cervi-cal cone biopsy (n=12) or hysterectomy (n=14) and in whom thediagnosis of cervical intraepithelial neoplasia III (CIN III) or inva-sive carcinoma of the cervix was made. In one patient, the biopsyspecimen and subsequent hysterectomy specimen were investigat-ed. Invasive carcinomas were mostly squamous cell carcinomas;in one patient an invasive adenocarcinoma of the cervix was diag-nosed. The epidemiological data of the patients investigated arelisted in Table 1.
Cone biopsy specimens were completely embedded and stepsections were performed. For hysterectomy specimens at least tworepresentative blocks of the ecto- and endocervix were chosen.
Immunohistochemistry
Immunohistochemistry was performed using the standard avidin biotin complex (ABC)-peroxidase method (ABC Elite Kit; Vector,Burlingame, Calif.) and 3,3′-diaminobenzidine (DAB) as chromo-gen. CD34 antigen was detected by means of a monoclonal antibody(QBEND10, Dako, Hamburg, Germany, dilution 1:50) after micro-wave pretreatment. Microwave pretreatment was performed by heat-ing the deparaffinized and rehydrated sections, immersed in 10 mMsodium citrate buffer (pH 6.0), in a microwave oven at 600 W, threetimes for 5 min each. α-SMA was detected using a monoclonal anti-body (ASM-1, Progen, Heidelberg, Germany; dilution 1:200) aftertissue pretreatment with 0.1% trypsin for 15 min at 37°C.
Simultaneous labeling of CD34 and α-SMA
In order to detect CD34 and α-SMA on a single slide, sequentialimmunohistochemical staining of the two antigens was performed.As a first procedural step, CD34 was detected by means of a monoclonal antibody (QBEND10, Immunotech, Marseille,France) which was applied as purchased by the supplier withoutfurther dilution or tissue pretreatment. The specific reaction was detected using the standard ABC-peroxidase method using3,3′-DAB as chromogen as described above. Thereafter, α-SMAwas detected by incubating the slides with the monoclonal anti-body (ASM-1, Progen; dilution 1:200) as described above. Detec-tion of the primary antibody was then performed by means of theABC-alkaline phosphatase method (Vector) using AS-bi-Naphthol(Sigma, Taufkirchen, Germany) as chromogen.
Results
Normal cervical stroma
In the normal cervical stroma CD34+ fibrocytes werepredominantly found in subepithelial and perivascularsites where they formed a dense reticular network(Fig. 1a, Table 2). With increasing distance from theoverlying epithelium and vascular structures, the densityof CD34+ fibrocytes decreased. The CD34+ fibrocytesshowed thin, bi- or multipolar dendrite-like cytoplasmicprocesses communicating with those of neighboringCD34+ fibrocytes. In the deep cervical stroma CD34+
fibrocytes were also found surrounding fascicles ofsmooth muscle which showed a strong reactivity with α-SMA. The subepithelial stroma was free of smoothmuscle and disclosed no α-SMA-positive myofibroblasts(Fig. 1b, Table 3).
CIN III and invasive carcinoma
In CIN III the distribution of CD34+ fibrocytes was simi-lar to that observed in the normal cervical stroma(Fig. 1c, Table 2). In six of eight cases investigated, thesubepithelial cervical stroma associated with CIN III disclosed α-SMA-positive myofibroblasts (Fig. 1d, Table 3). In the remaining two cases the stroma adjacentto CIN III was free of α-SMA-positive myofibroblasts.Early stromal invasion was characterized by a loss of subepithelial CD34+ fibrocytes in the vicinity of in-vading tumor cells (Fig. 1c, inset), whereas no alterationin the distribution of α-SMA-positive myofibroblasts occurred.
The stroma associated with invasive squamous cellcarcinoma of the cervix was free of CD34+ fibrocytes in10 of 18 cases (Fig. 1e, Table 2). In these cases the tran-sition from tumor-free stroma to invasive carcinoma was
Table 1 Epidemiological data of the patients investigated. CIN IIIcervical intraepithelial neoplasia III
Patientsn=25 femalesAge: range 24–82 years, arithmetic mean: 42.5 years
Type of specimenHysterectomy specimens: 14Cone biopsies: 12*
Histologic diagnosesCIN III: 8**
Invasive carcinoma: 18*pT1a 5pT1b 10pT2a 1pT2b 2
* In one patient the cone biopsy specimen and subsequent hyster-ectomy specimen were included** CINIII associated with invasive carcinoma was not evaluated
Table 2 Distribution of CD34+ fibrocytes in the cervical stroma. 0 no CD34+ fibrocytes, + focal accumulations of CD34+ fibro-cytes, ++ diffusely scattered CD34+ fibrocytes
0 + ++
Normal cervical stroma 0 0 26Cervical intraepithelial neoplasia III 0 0 8Invasive carcinoma 10 7 1
Table 3 Distribution of α-smooth muscle actin (α-SMA) positivemyofibroblasts in the cervical stroma. 0 no α-SMA-positive myo-fibroblasts detectable, + focal accumulations of α-SMA-positivemyofibroblasts, ++ diffusely scattered and densely packed α-SMA-positive myofibroblasts
0 + ++
Normal cervical stroma 26 0 0CIN III 2 6 0Invasive carcinoma 0 9 9

566
clear-cut and appeared to be made up of a population ofmore densely packed CD34+ fibrocytes. In seven cases afocal residual population of CD34+ fibrocytes could bedetected at the periphery of the infiltrating carcinoma. Inone case the CD34+ fibrocytes appeared to be completelypreserved. The residual CD34+ fibrocytes showed nomorphological alterations in comparison with CD34+
fibrocytes found in the normal, tumor-free cervical stro-ma. Adjacent tumor-free cervical stroma disclosed acompletely unaltered population of CD34+ fibrocytes.
α-SMA-positive myofibroblasts were detected in thestroma of all cases of invasive carcinoma irrespective ofthe presence or absence of CD34+ fibrocytes (Table 3).The myofibroblasts were haphazardly arranged, spindle-
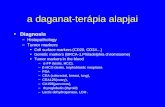
Fig. 1 The normal stroma of the cervix uteri harbors a dense network of CD34+ fibrocytes (a), whereas α-smooth muscle actin(α-SMA) positive myofibroblasts are absent (b). The walls ofmuscularized vessels stain positive for α-SMA (b). The stromaadjacent to cervical intraepithelial neoplasia III (CIN III) includeshuge numbers of CD34+ fibrocytes (c), early stromal invasion by atypical cells is characterized by a loss of CD34+ fibrocytes (c, inset). In CIN III, the subepithelial stroma also expresses α-SMA (d). The stroma of invasive squamous cell carcinomas is free of CD34+ fibrocytes (e) and contains huge numbers of haphazardly arranged α-SMA-positive myofibroblasts (f)

shaped and showed plump cigar-shaped nuclei and acharacteristic “tram-tracking” of α-SMA-positive intra-cytoplasmic fibers (Fig. 1f).
Double staining for CD34 and α-SMA
Double staining for CD34 and α-SMA revealed the subepithelial CD34+ fibrocytes of the normal cervicalstroma to be exclusively reactive for CD34. In the deeperlayers α-SMA-reactive smooth muscle cells and CD34+
fibrocytes could be clearly distinguished by means ofCD34 and α-SMA double staining. In those cases ofCIN III that showed subepithelial CD34+ fibrocytes andα-SMA-positive myofibroblasts, double labeling showedclosely intermingled CD34+ and α-SMA-positive fibers.By means of light microscopy it was not possible to decide whether CD34 and α-SMA were coexpressed in a single cell population or in two distinct cell types.However, taken together with the results of single stain-ing for CD34 and α-SMA, this finding was assumed tobe highly suggestive of a population expressing bothCD34 and α-SMA. In contrast, double labeling of inva-sive carcinomas clearly distinguished between α-SMA-positive myofibroblasts and CD34-reactive endothelialcells as well as CD34+ fibrocytes. No CD34+ fibrocytesor cells double stained for CD34 and α-SMA were foundin the stroma of the majority of infiltrating squamouscell carcinomas. In invasive carcinomas with a residualCD34+ fibrocyte population, double labeling showed anaspect similar to that observed in the vicinity of CIN III.
Discussion
The cervical stroma harbors large amounts of CD34+
fibrocytes [8]. Although this cell population has been described in the normal cervical stroma, data concerningalterations of this cell population in relation to certaindisease processes are not published in the pertinent literature. The present study confirms the findings ofLindenmayer and Miettinen who were the first to reportCD34+ fibrocytes in the cervix [8]. In addition, the stroma of invasive cervical squamous cell carcinoma isvirtually free of CD34+ fibrocytes and is mainly com-posed of a population of α-SMA-positive myofibroblastswhich are almost completely absent from the normal cer-vical stroma. The loss of CD34+ fibrocytes in invasivecarcinomas is not site specific for the cervix since similar findings have been reported for stromal altera-tions occurring in ductal carcinomas of the breast [1],pancreas [2], colon [10] and skin [7].
Although this phenomenon appears to be ubiquitous,the mechanisms that mediate this process are far frombeing understood. Two alternative mechanisms might beresponsible for the immunophenotypic alterations of thestroma associated with invasive carcinoma. On the onehand, the tumor might induce apoptosis of CD34+ fibro-cytes which subsequently are replaced by α-SMA-posi-
tive myofibroblasts; on the other hand, the immunophe-notypic change may occur in one cell population thatdownregulates CD34 and gains α-SMA expression. Thefirst assumption may be strengthened by the finding thatcell culture supernatants of pulmonary endocrine tumorsare capable of inducing apoptosis in dendritic interstitialcells [5] which appear to be closely related to CD34+
fibrocytes. It remains questionable whether these in vitrofindings also occur in vivo. Considering the results ofthe present study it appears to be more likely that CD34+
fibrocytes gain α-SMA expression and in turn downreg-ulate CD34 expression. This assumption is based on thefinding that expression of CD34 and α-SMA is notstrictly exclusive since a simultaneous expression ofthese markers was found in the subepithelial cells adja-cent to CIN III. These cells appear to constitute an inter-mediate population between CD34+ and α-SMA-nega-tive fibrocytes and CD34-negative and α-SMA-positivemyofibroblasts.
While the mechanisms leading to a reduction andcomplete loss of CD34+ fibrocytes remain to be eluci-dated, the practical advantages of the findings presentedhere are obvious. Taking into account that tangential sec-tioning of atypical surface epithelium and occupation ofdeep-seated glandular structures by atypical epitheliummay cause significant problems in establishing the diag-nosis of stromal infiltration, the diagnosis of invasivecervical cancer is not trivial. The loss of stromal CD34+
expression paralleled by a gain of α-SMA expression appears to be a sensitive indicator of early stromal inva-sion. Therefore, the detection of a loss of CD34+ fibro-cytes appears to be a valuable tool in detecting earlystromal invasion and stromal invasion in general. Thelatter might be of certain significance when small biopsyparticles of the cervix are submitted. We concede that theabsence or loss of immunohistochemical expression of acertain marker is regarded to be less valuable than an im-munohistochemically positive signal since reduction orcomplete loss of immunohistochemical marker expres-sion might be related to technical flaws. In the case ofCD34 immunohistochemistry, however, the stroma con-tains mostly small vascular structures providing a reli-able internal positive control.
References
1. Barth PJ, Ebrahimsade S, Ramaswamy A, Moll R (2002)CD34+ fibrocytes in invasive ductal carcinoma, ductal carci-noma in situ, and benign breast lesions. Virchows Arch440:298–303
2. Barth PJ, Ebrahimsade S, Ramaswamy A, Moll R (2002)CD34+ fibrocytes in ductal adenocarcinoma of the pancreas,chronic pancreatitis and normal pancreatic parenchyma. Virchows Arch 440:128–133
3. Bucala R, Spiegel LA, Chesney J, Hogan M, Cerami A (1994)Circulating fibrocytes define a new leukocyte subpopulationthat mediates tissue repair. Mol Med 1:71–81
4. Chesney J, Bacher M, Bender A, Bucala R (1997) The periph-eral blood fibrocyte is a potent antigen-presenting cell capableof priming naive T cells in situ. Proc Natl Acad Sci USA94:6307–6312
567

14. Silverman JS, Tamsen A (1996) Mammary fibroadenoma andsome phyllodes tumour stroma are composed of CD34+ fibro-blasts and factor XIIIa+ dendrophages. Histopathology 29:411–419
15. Sircar K, Hewlett BR, Huizinga JD, Chorneyko K, Berezin I,Riddell RH (1999) Interstitial cells of Cajal as precursors ofgastrointestinal stromal tumors. Am J Surg Pathol 23:377–389
16. Soma L, LiVolsi VA, Baloch ZW (2001) Dendritic interstitialand myofibroblastic cells at the border of salivary gland tumors. Arch Pathol Lab Med 125:232–236
17. Suster S, Fisher C (1997) Immunoreactivity for the human hematopoietic progenitor cell antigen (CD34) in lipomatoustumors. Am J Surg Pathol 21:195–200
18. Swanson PE, Fitzpatrick MM, Ritter JH, Glusac EJ, Wick MR(1998) Immunohistologic differential diagnosis of basal cellcarcinoma, squamous cell carcinoma, and trichoepithelioma insmall cutaneous biopsy specimens. J Cutan Pathol 25:153–159
19. Yamazaki K, Eyden BP (1995) Ultrastructural and immunohis-tochemical observations on intralobular fibroblasts of humanbreast, with observations on the CD34 antigen. J SubmicroscCytol Pathol 27:309–323
20. Yamazaki K, Eyden BP (1996) Ultrastructural and immunohis-tochemical studies of stromal cells in lamina propria of humanfallopian tube ampullar mucosa: the recognition of “CD34-positive reticular network” and its putative function in immune surveillance. J Submicrosc Cytol Pathol 28:325–337
21. Yamazaki K, Eyden BP (1997) Interfollicular fibroblasts in thehuman thyroid gland: recognition of a CD34-positive stromal cellnetwork communicated by gap junctions and termineated by autonomic nerve endings. J Submicrosc Cytol Pathol 29:461–467
568
5. Katsenelson NS, Shurin GV, Bykosvkaia SN, Shogan J,Shurin MR (2001) Human small cell lung carcinoma and car-cinoid tumor regulate dendritic cell maturation and function.Mod Pathol 14:40–45
6. Khalifa MA, Montgomery EA, Ismiil N, Azumi N (2000)What are CD34+ cells in benign peripheral nerve sheath tumors? Am J Clin Pathol 114:123–126
7. Kirchmann TT, Prieto VG, Smoller BR (1994) CD34 stainingpattern distinguishes basal cell carcinoma from trichoepithe-lioma. Arch Dermatol 130:589–592
8. Lindenmayer AE, Miettinen M (1995) Immunophenotypicfeatures of uterine stromal cells. CD34 expression in endocer-vical stroma. Virchows Arch 426:457–460
9. Magro G, Michal M, Bisceglia M (2001) Benign spindle celltumors of the mammary stroma: diagnostic criteria, classifica-tion, and histogenesis. Pathol Res Pract 197:453–466
10. Nakayama H, Enzan H, Miyazaki E, Kuroda N, Naruse K, Hiroi M (2000) Differential expression of CD34 in normal colorectal tissue, peritumoral inflammatory tissue, and tumourstroma. J Clin Pathol 53:626–629
11. Nakayama H, Enzan H, Miyazaki E, Kuroda N, Naruse K, Kiyoku H, Toi M, Hiroi M (2001) CD34 positive stromal cellsin gastric adenocarcinomas. J Clin Pathol 54:846–848
12. Narvaez D, Kanitakis J, Faure M, Claudy A (1996) Immuno-histochemical study of CD34-positive dendritic cells of humandermis. Am J Dermatopathol 18:283–288
13. Seidal T, Edvardsson H (1999) Expression of c-kit (CD117)and Ki67 provides information about the possible cell of ori-gin and clinical course of gastrointestinal stromal tumours.Histopathology 34:416–424