Beuerle, John - POWERPOINT Emergency Department...
31
8/30/2011 1 Emergency Department Misadventures (Cases You Don’t Want to Miss) John Beuerle, M.D., M.S.
Transcript of Beuerle, John - POWERPOINT Emergency Department...

8/30/2011
1
Emergency Department Misadventures(Cases You Don’t Want to Miss)
John Beuerle, M.D., M.S.
8/30/2011
2
I’m brilliant.You’re the only one not looking at the
screen.

8/30/2011
3
These guys worship me.I worship him.
I can’t hear a thing.
I can’t believe I forgot to bring
my stethescope.
I gotta pee.
If I don’t eat something soon, I’m gonna pass out.
If my purse goes missing, I’m calling security.
I’m here for knee pain.
This coffee tastes horrible. That’s a urine sample.
8/30/2011
4
What’s next?Geriatric Medicine
NASCAR pit crew
Sports Medicine
Anesthesiology
Tarot Card Reader
Neurology
Neurosurgery
Batman
Orthopedics
Pediatrics
Family Practice
Physical Rehabilitation
Emergency Medicine
Surgery
OB/GYN
Veterinary Medicine
Just try not . . .
to kill anyone!
Let’s begin.
8/30/2011
5
Case # 1: Lights on. Nobody home.
• 3 y.o. female
• Lights on. Nobody home.• Blank stare. Rotary nystagmus.
Case # 1: Lights on. Nobody home.
• Initial treatment?• Labs?
• CBC: normal• BMP: normal• UA: normal• Tylenol / Salicylate:
negative
• CT head?normal
• Tox screen:Positive for PCP
Case # 1: Lights on. Nobody home.
• What now?– Child Protective Services?– PICU?
– Strangle theparents with your bare hands?
Case # 2: Tequila Jane
• 16 y.o. female, arrives by EMS• HPI:
– Found unresponsive at home.– Empty bottle of tequila in room. – Family reports patient
“may have been drinking.”– Family called 911.
• PMHx: none• SocHx: Nonsmoker, occasional EtOH,
No illicit drug use• FmHx: HTN, asthma, hyperlipidemia
8/30/2011
6
Case # 2: Tequila Jane
• Physical Exam:– Strong odor of alcohol to breath.– Moans / withdraws to deep painful stimuli– BP 96/68, HR 56, RR 12, Temp 98 F, 96%
on room air– PERRL– Small amount of emesis in oropharynx.– No external signs of trauma.
Case # 2: Tequila Jane
• Initial management?– Airway management
(suction)– Check fingerstick glucose !!!– EtOH level, tox screen
– CBC, CMP, UA, HCG? – EKG, CXR, CT head?– What else??
Normal !!
Case # 3: Whiskey Joe
• 54 y.o. self-proclaimed concert pianist
• Wife called 911 because patient was “drunker than usual”.
• PMHx: HTN, DM, a-fib, and . . . wife reports: “He’s a pathological liar.”
• “He can’t even play a kazoo.”
?Case # 3: Whiskey Joe
• Physical Exam– Dissheveled.– Strong odor of alcohol
. . . and feet.– No external signs of trauma.– Mutters incoherently.– Kazoo found in back pocket.
8/30/2011
7
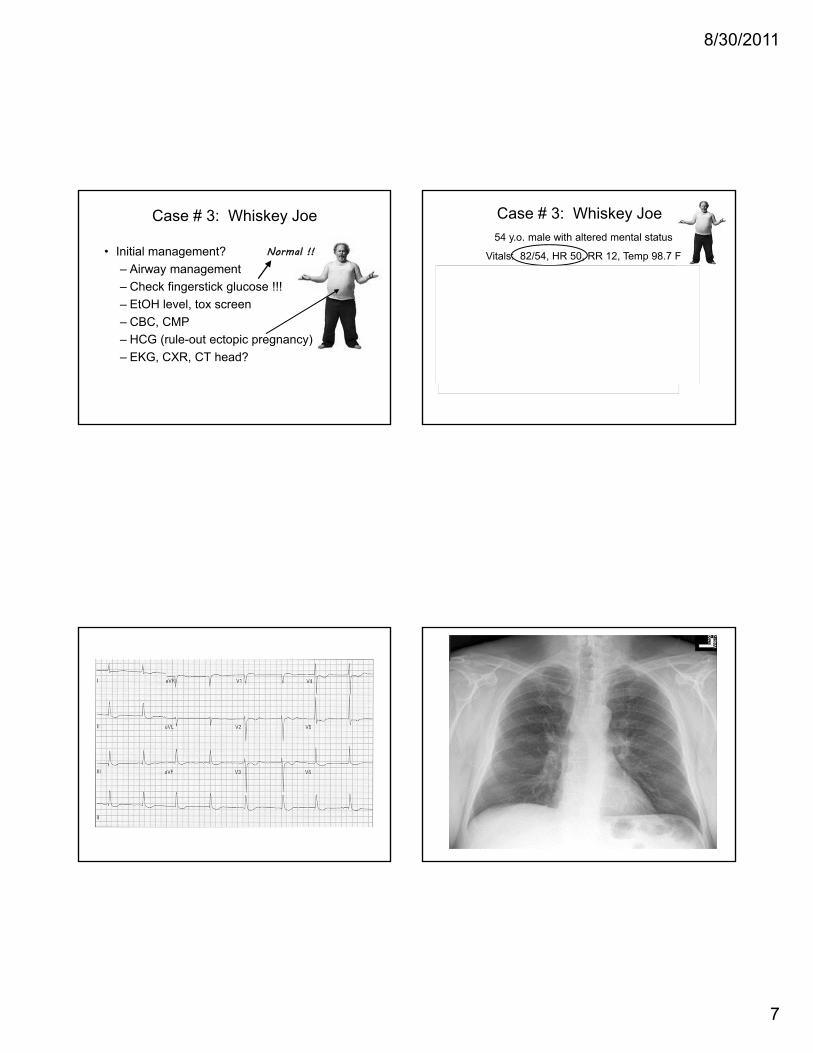
Case # 3: Whiskey Joe
• Initial management?– Airway management – Check fingerstick glucose !!!– EtOH level, tox screen– CBC, CMP– HCG (rule-out ectopic pregnancy) – EKG, CXR, CT head?
Normal !!
Case # 3: Whiskey Joe
10.411.4
34.8298
137
6.2
98
25
13
0.9118
96
32
42
0.6
6.7
3.6UA: nml
Tox screen: negativeBAL 210
54 y.o. male with altered mental status
Vitals: 82/54, HR 50, RR 12, Temp 98.7 F
Urine hcg: positive !!!2.423.2
45.6
8/30/2011
8
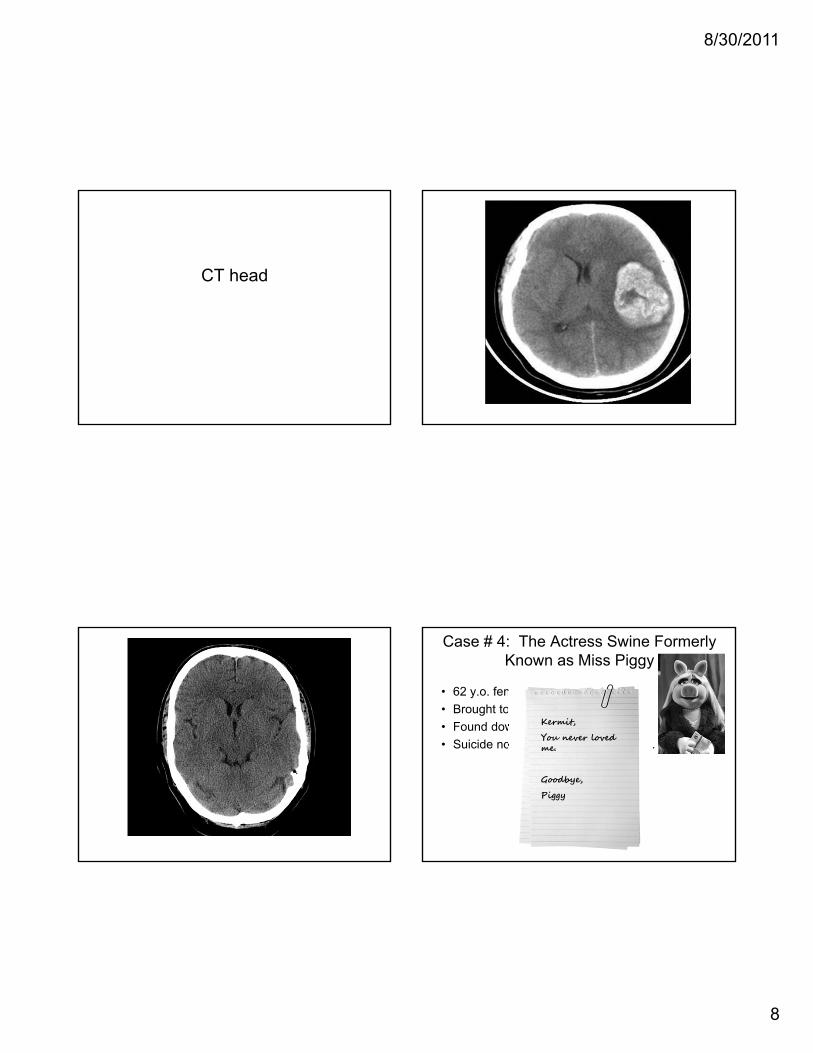
CT head (Just kidding.)
• 62 y.o. female pig• Brought to ED by ambulance.• Found down in trough.• Suicide note paper-clipped to her tail.
Case # 4: The Actress Swine Formerly Known as Miss Piggy
Kermit,
You never loved me.
Goodbye,
Piggy

8/30/2011
9
Case # 4: The Actress Swine Formerly Known as Miss Piggy
8.210.4
32.7289
134
4.3
97
25
18
0.8108
26
38
42
0.6
6.8
4.1
Tox screen: BAL 82
HCG: neg
62 y.o. suicidal pig with altered mental status
Vitals: 70/42, HR 160, RR 14, Temp 99 F
Lightweight !!(Even for a pig.)
Positive for bacon !!
We need you in Room 8!!
STAT !!!
Case # 2: Tequila Jane
10.212.4
36.7301
136
4.2
97
25
11
0.8211
26
38
42
0.6
6.8
4.1UA: nml
Tox screen: negativeBAL 154
HCG: neg
16 y.o. female with altered mental status
Vitals: 68/36, HR 38, RR 14, Temp 98 F
8/30/2011
10
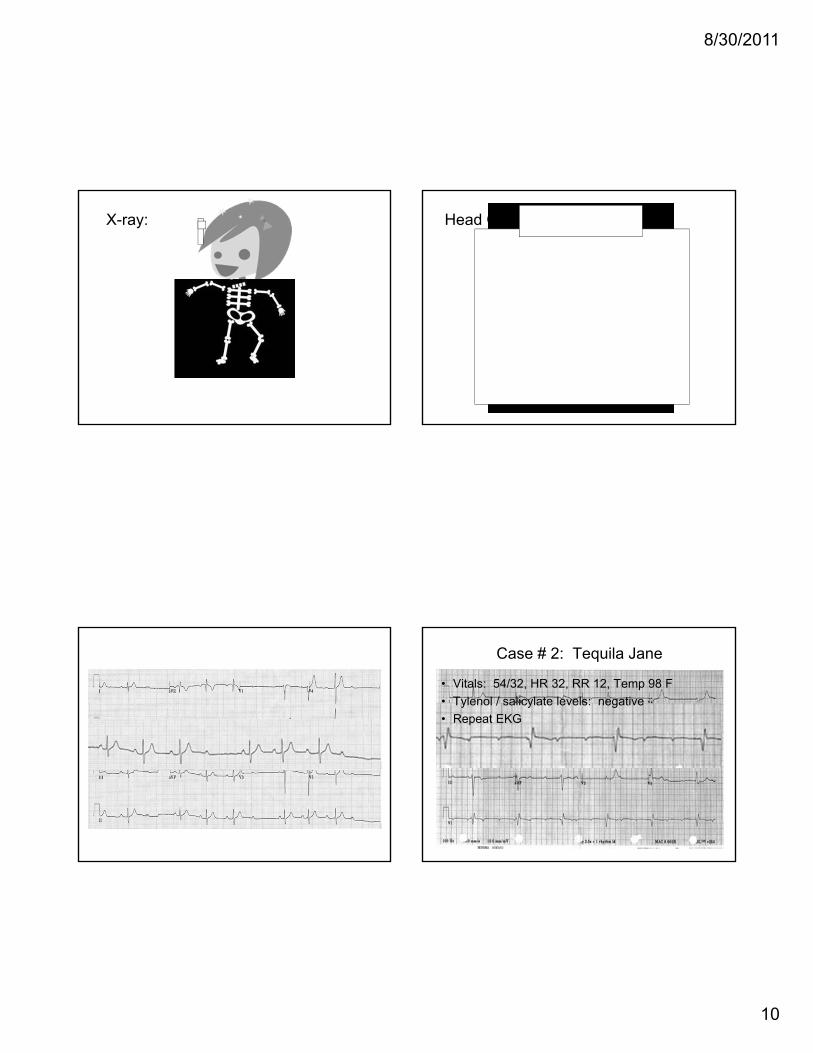
X-ray: Head CT:
Case # 2: Tequila Jane
• Vitals: 54/32, HR 32, RR 12, Temp 98 F• Tylenol / salicylate levels: negative• Repeat EKG
8/30/2011
11
We need you in Room 4!!
STAT !!!
Case # 3: Whiskey Joe
I wanna sandwich.
Vitals: 74/50, HR 48
What’s wrong with these patients?!!• Just plain drunk• Faking it• Conversion Disorder• Minding their own business . . .
when all of a sudden . . . TWO DUDES jumped out of the bushes and gave them hypotension and cardiac arrhythmias!!
• Could they have overdosed?!!• If so, on what?!!
• What commonly prescribed medications are cardiotoxic?– Digoxin– β-blockers– Calcium channel blockers– Clonidine
8/30/2011
12
How can we tell the difference?– Check a level.– Ask the family. Check the medicines.
Patient’s meds include . . . . . . atenolol !!!
. . . and enalapril !!. . . and digoxin !!
. . . and clonidine !!. . . and Preparation H !!!
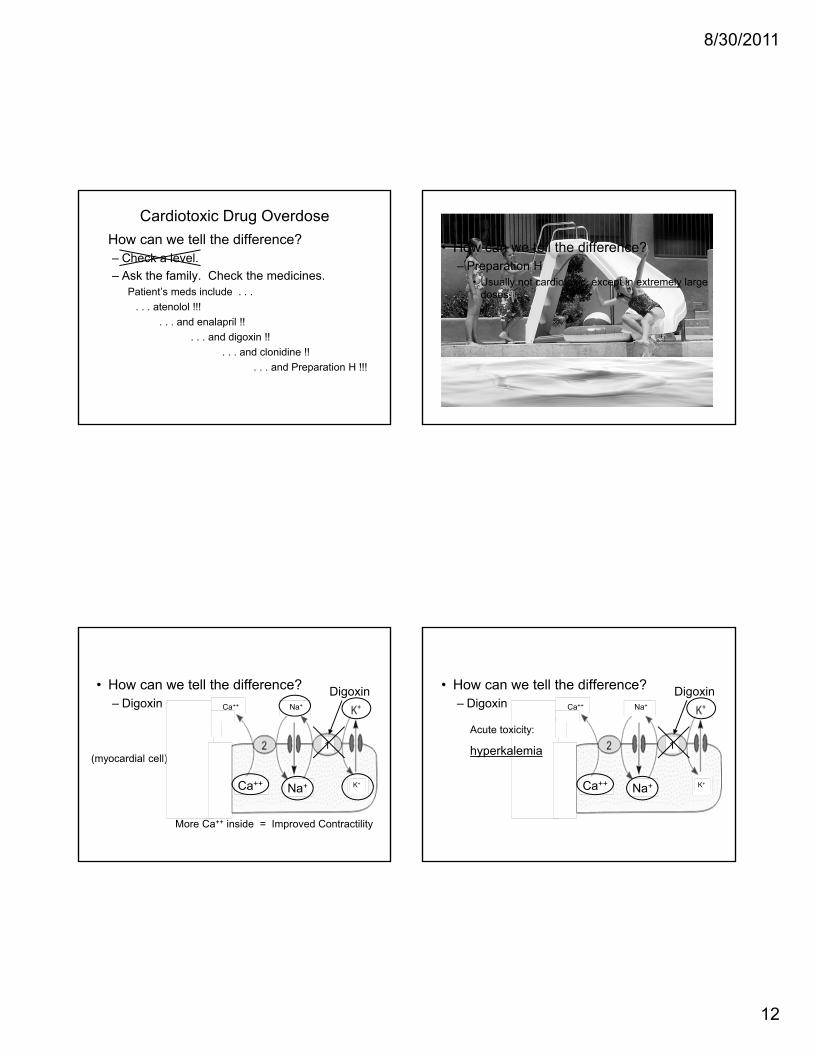
Cardiotoxic Drug Overdose
• How can we tell the difference?– Preparation H
• Usually not cardiotoxic, except in extremely large doses.
• How can we tell the difference?– Digoxin
(myocardial cell)
Digoxin
K+
Na+
Ca++
Ca++
Na+
More Ca++ inside = Improved Contractility
1
• How can we tell the difference?– Digoxin
Digoxin
K+
Na+
Ca++
Ca++
Na+
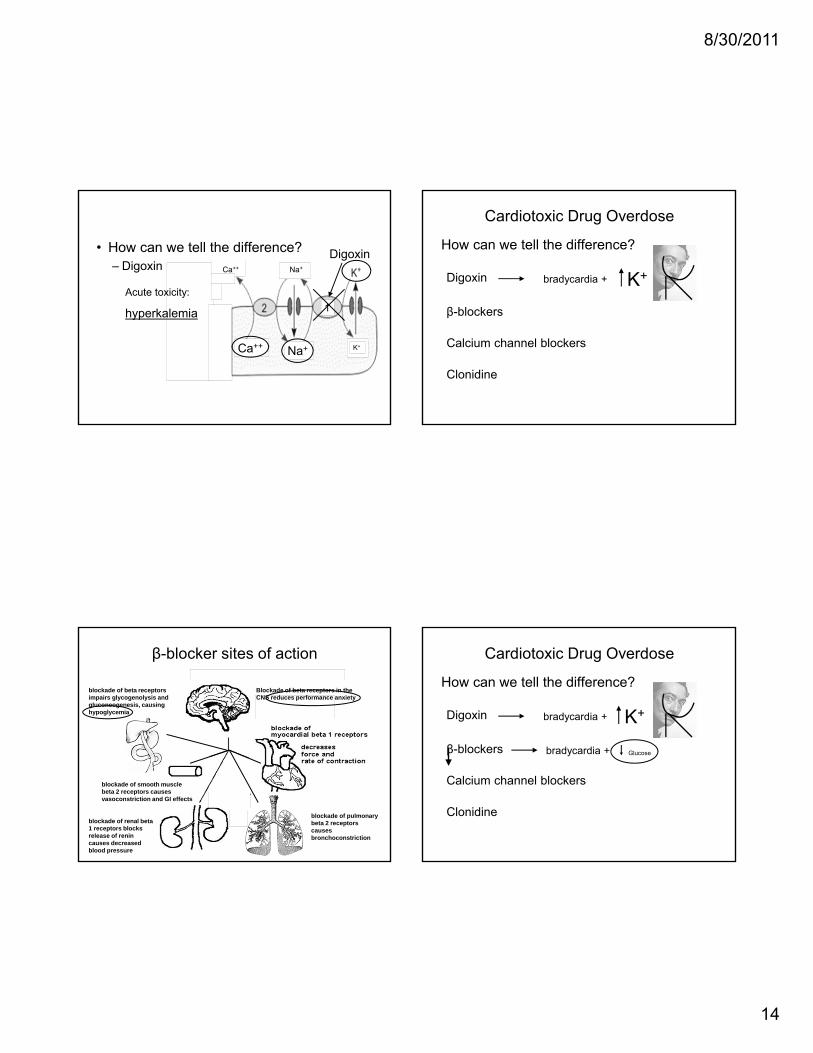
1Acute toxicity:
hyperkalemia
8/30/2011
13
– Large Volume of Distribution
• In acute poisoning, a low level is not necessarily reassuring.
• In symptomatic patients, do not wait for a level to treat!!
Total amount of drug in the body
Blood plasma concentration of drug VD =
Digoxin
• Symptoms of acute toxicity:– First 6 hours: GI symptoms– At 3-4 hours: cardiac effects
• bradycardia, PVCs• AV node effects:
– atrial fibrillation / flutter– high degree AV blocks
Digoxin
DigoxinThe “Salvador Dali sign” on EKG correlates with digoxin use, not necessarily with digoxin toxicity. How can we tell the difference?
Digoxin
β-blockers
Calcium channel blockers
Clonidine
Cardiotoxic Drug Overdose
8/30/2011
14
• How can we tell the difference?– Digoxin
Digoxin
K+
Na+
Ca++
Ca++
Na+
1Acute toxicity:
hyperkalemia
How can we tell the difference?
Digoxin
β-blockers
Calcium channel blockers
Clonidine
bradycardia +
Cardiotoxic Drug Overdose
K+
β-blocker sites of action
blockade of pulmonary beta 2 receptors causes bronchoconstriction
blockade of renal beta 1 receptors blocks release of renin causes decreased blood pressure
Blockade of beta receptors in the CNS reduces performance anxiety
blockade of smooth muscle beta 2 receptors causes vasoconstriction and GI effects
blockade of beta receptors impairs glycogenolysis and gluconeogenesis, causing hypoglycemia
How can we tell the difference?
Digoxin
β-blockers
Calcium channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
8/30/2011
15
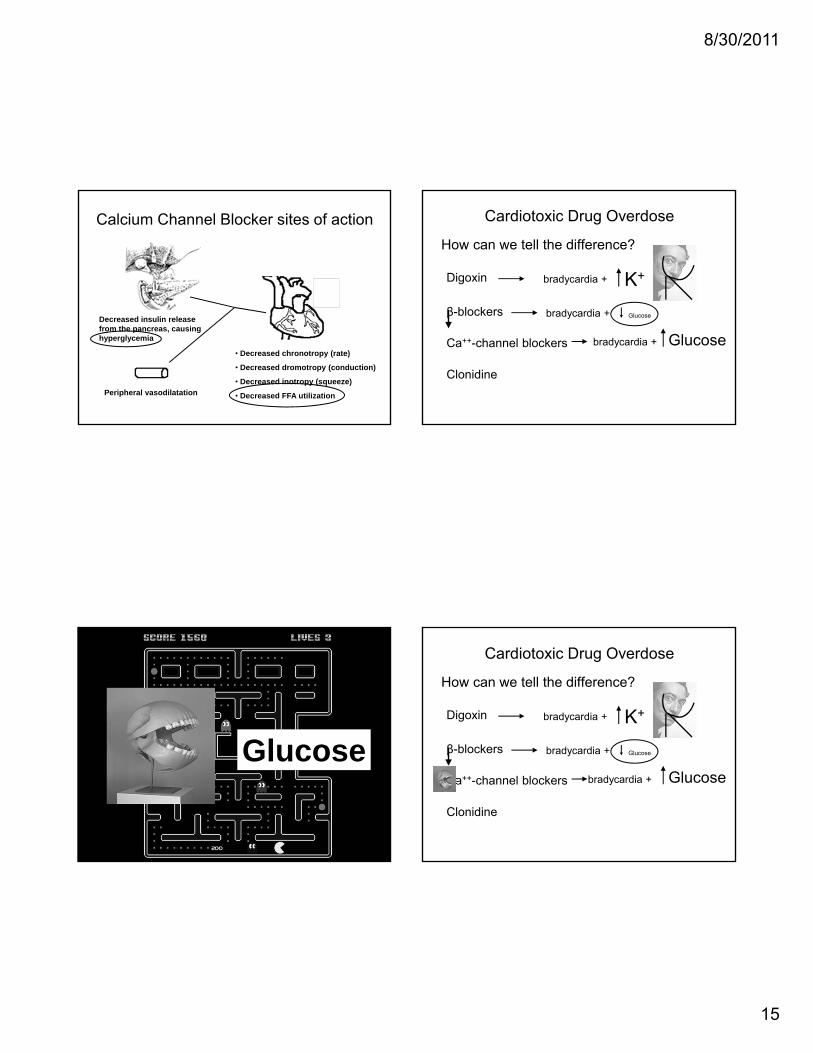
Calcium Channel Blocker sites of action
Peripheral vasodilatation
• Decreased chronotropy (rate)
• Decreased dromotropy (conduction)
• Decreased inotropy (squeeze)
• Decreased FFA utilization
Decreased insulin release from the pancreas, causing hyperglycemia
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
Glucose
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
8/30/2011
16
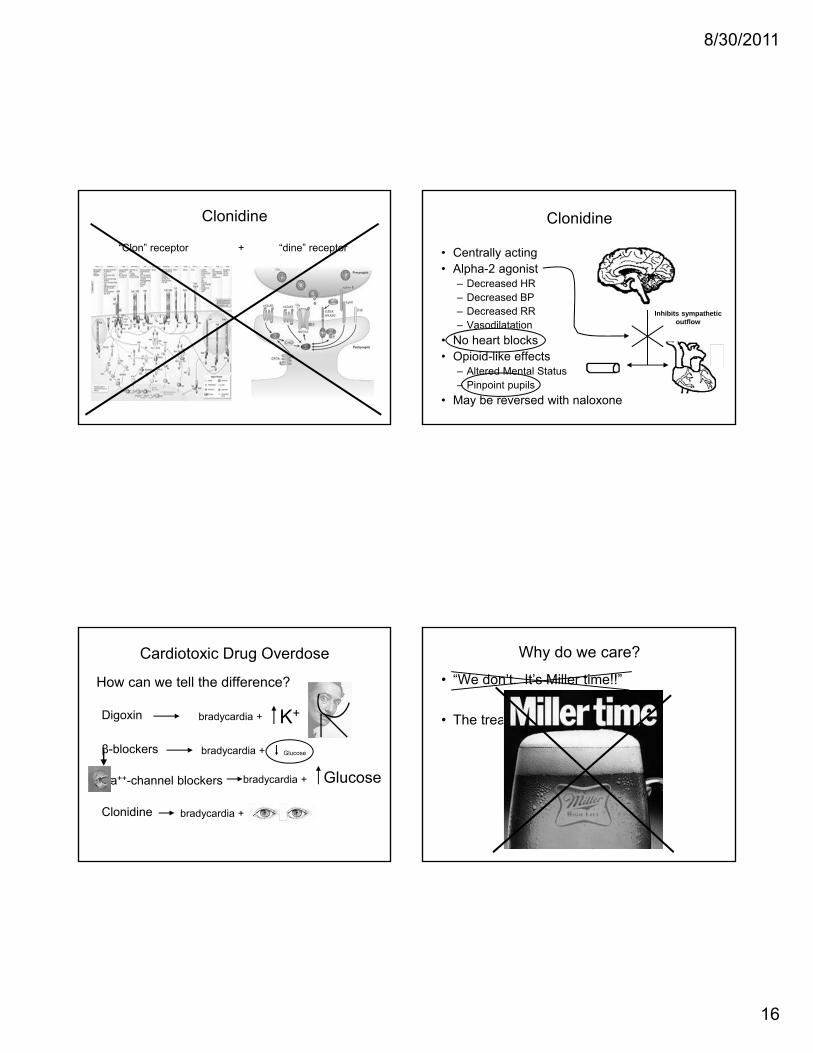
Clonidine
“Clon” receptor “dine” receptor+
Clonidine
• Centrally acting• Alpha-2 agonist
– Decreased HR– Decreased BP– Decreased RR– Vasodilatation
• No heart blocks• Opioid-like effects
– Altered Mental Status– Pinpoint pupils
• May be reversed with naloxone
Inhibits sympathetic outflow
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
Why do we care?
• “We don’t. It’s Miller time!!”
• The treatment is different !!!
8/30/2011
17
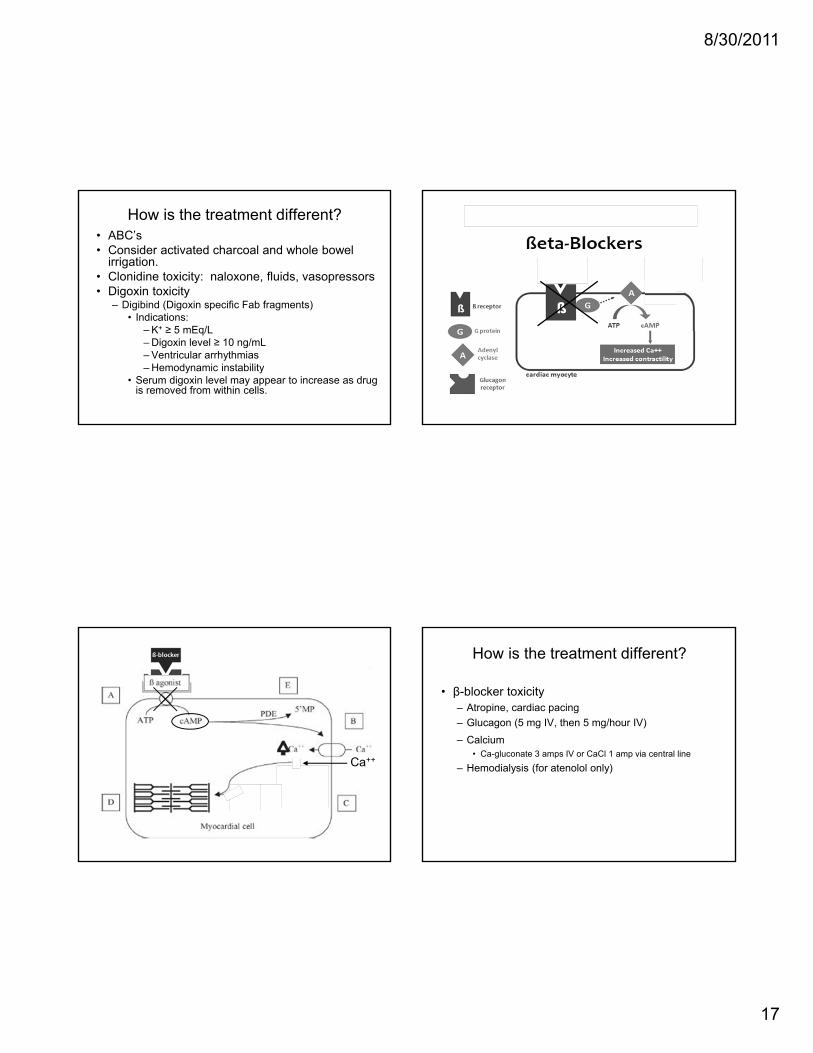
How is the treatment different?• ABC’s• Consider activated charcoal and whole bowel
irrigation.• Clonidine toxicity: naloxone, fluids, vasopressors• Digoxin toxicity
– Digibind (Digoxin specific Fab fragments)• Indications:
– K+ ≥ 5 mEq/L– Digoxin level ≥ 10 ng/mL– Ventricular arrhythmias– Hemodynamic instability
• Serum digoxin level may appear to increase as drug is removed from within cells.
How is the treatment different?
• β-blocker toxicity– Atropine, cardiac pacing– Glucagon (5 mg IV, then 5 mg/hour IV)– Calcium
• Ca-gluconate 3 amps IV or CaCl 1 amp via central line
Ca++
How is the treatment different?
• β-blocker toxicity– Atropine, cardiac pacing– Glucagon (5 mg IV, then 5 mg/hour IV)– Calcium
• Ca-gluconate 3 amps IV or CaCl 1 amp via central line
– Hemodialysis (for atenolol only)

8/30/2011
18
How is the treatment different?
• Ca++-channel blocker toxicity– High mortality !!! Why??
Atropine
Ca++
How is the treatment different?
• Ca++-channel blocker toxicity– High mortality !!! – Atropine– Glucagon– Calcium
• Ca-gluconate 3 amps IV or CaCl 1 amp via central line
– Hemodialysis?(Ineffective.)
Is there no hope??!
Treatment: Calcium ChannelBlocker Toxicity
• High-dose insulin therapy– 1 unit/kg IV, then 0.5 units/kg/hour IV– Ten-fold higher dose than used for DKA !!
Calcium Channel Blocker sites of action
Peripheral vasodilatation
• Decreased chronotropy (rate)
• Decreased dromotropy (conduction)
• Decreased inotropy (squeeze)
• Decreased FFA utilization
Decreased insulin release from the pancreas, causing hyperglycemia
8/30/2011
19
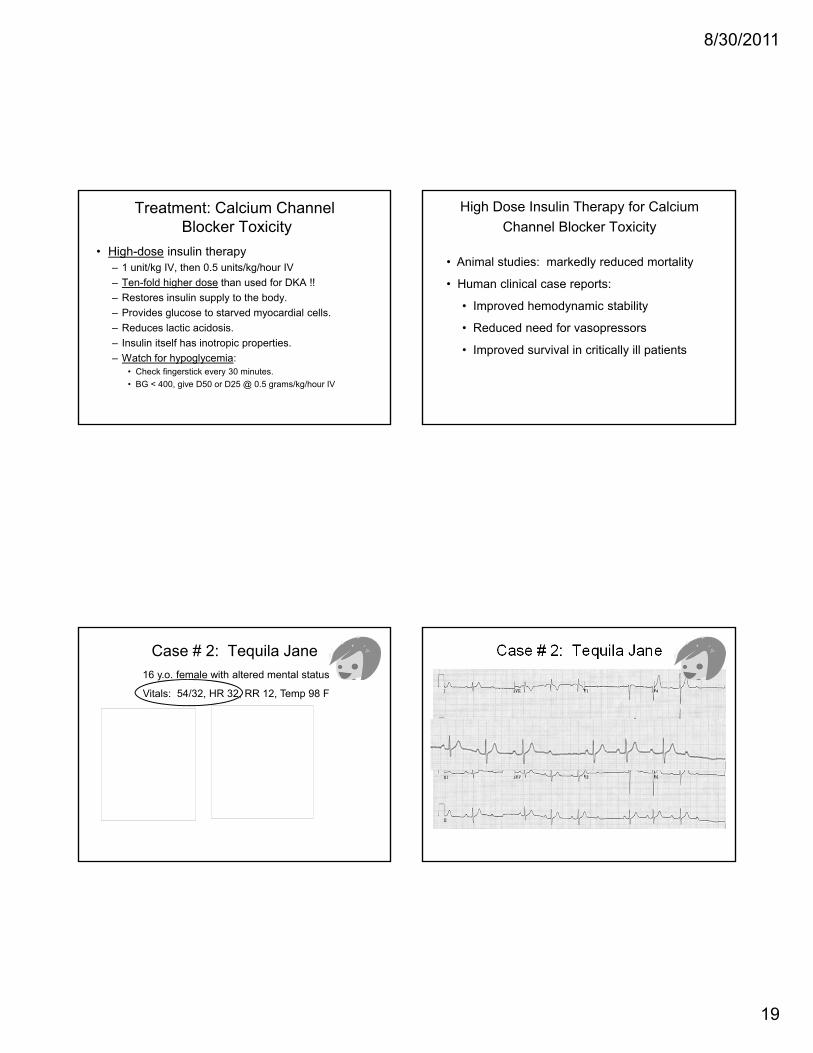
Treatment: Calcium ChannelBlocker Toxicity
• High-dose insulin therapy– 1 unit/kg IV, then 0.5 units/kg/hour IV– Ten-fold higher dose than used for DKA !!– Restores insulin supply to the body.– Provides glucose to starved myocardial cells.– Reduces lactic acidosis.– Insulin itself has inotropic properties.– Watch for hypoglycemia:
• Check fingerstick every 30 minutes.• BG < 400, give D50 or D25 @ 0.5 grams/kg/hour IV
High Dose Insulin Therapy for Calcium Channel Blocker Toxicity
• Animal studies: markedly reduced mortality
• Human clinical case reports:
• Improved hemodynamic stability
• Reduced need for vasopressors
• Improved survival in critically ill patients
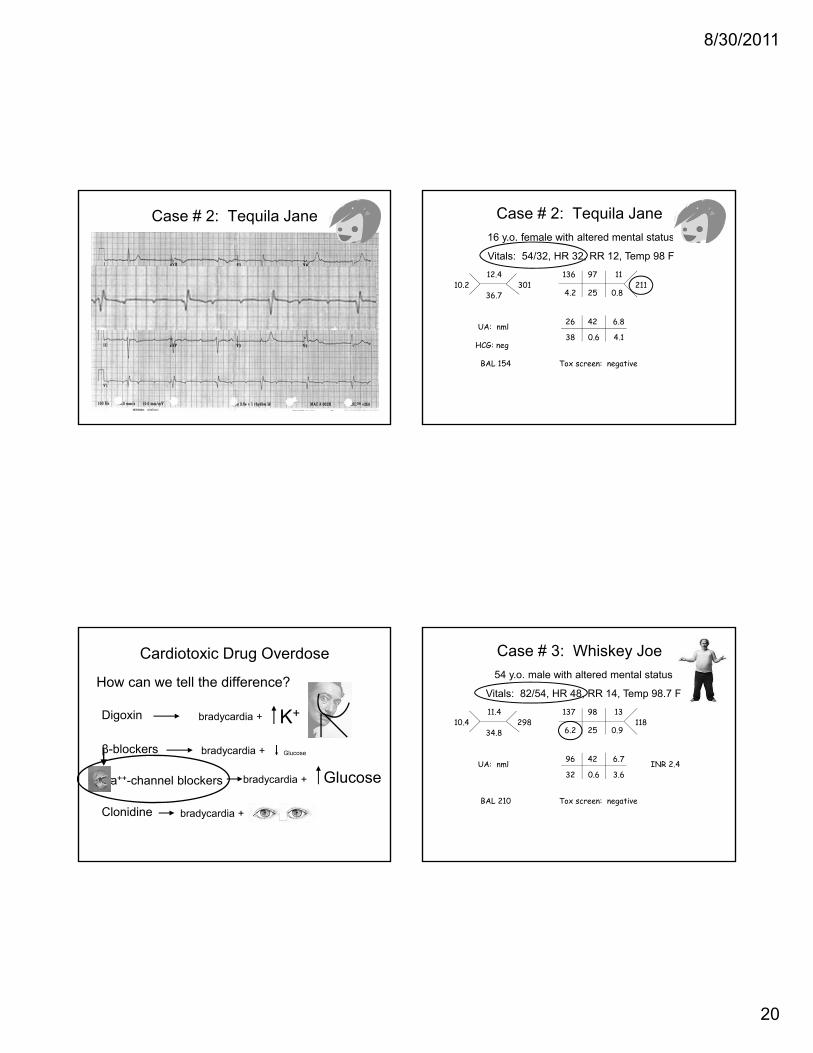
Case # 2: Tequila Jane
10.212.4
36.7301
136
4.2
97
25
11
0.8211
26
38
42
0.6
6.8
4.1UA: nml
Tox screen: negativeBAL 154
HCG: neg
16 y.o. female with altered mental status
Vitals: 54/32, HR 32, RR 12, Temp 98 F
Case # 2: Tequila Jane
8/30/2011
20
Case # 2: Tequila Jane Case # 2: Tequila Jane
10.212.4
36.7301
136
4.2
97
25
11
0.8211
26
38
42
0.6
6.8
4.1UA: nml
Tox screen: negativeBAL 154
HCG: neg
16 y.o. female with altered mental status
Vitals: 54/32, HR 32, RR 12, Temp 98 F
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
Case # 3: Whiskey Joe
10.411.4
34.8298
137
6.2
98
25
13
0.9118
96
32
42
0.6
6.7
3.6UA: nml
Tox screen: negativeBAL 210
54 y.o. male with altered mental status
Vitals: 82/54, HR 48, RR 14, Temp 98.7 F
INR 2.4
8/30/2011
21
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
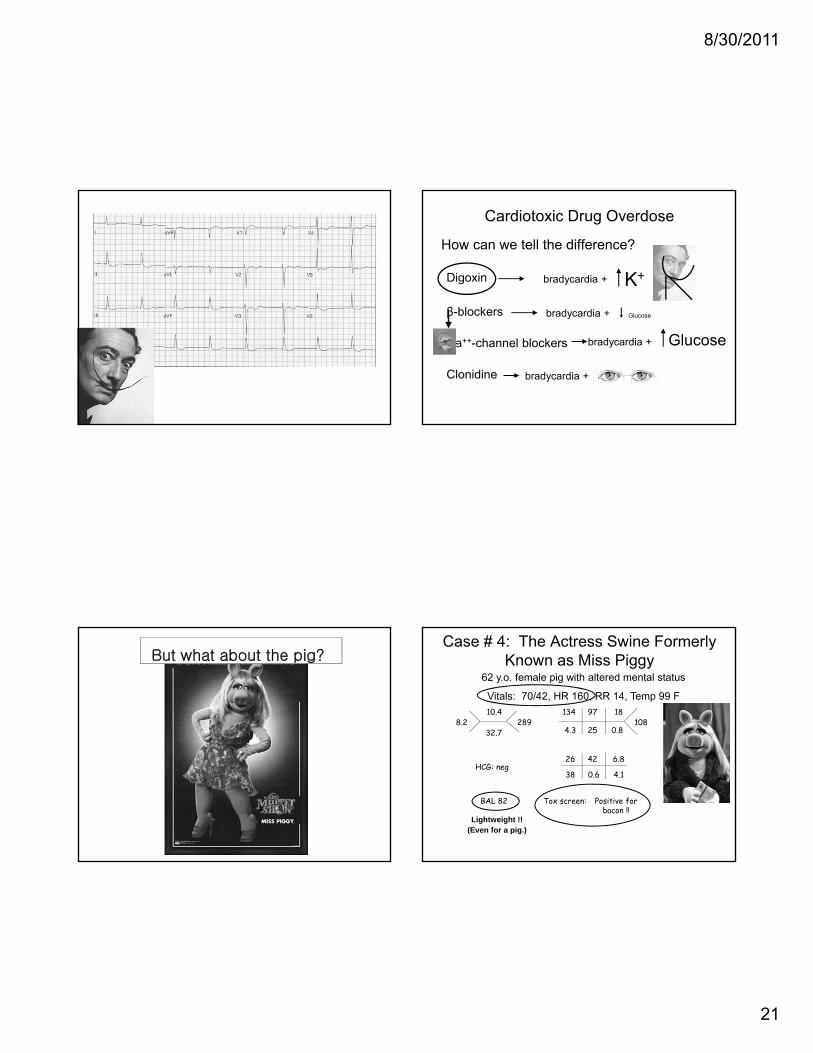
But what about the pig?Case # 4: The Actress Swine Formerly
Known as Miss Piggy
8.210.4
32.7289
134
4.3
97
25
18
0.8108
26
38
42
0.6
6.8
4.1
Tox screen: BAL 82
HCG: neg
62 y.o. female pig with altered mental status
Vitals: 70/42, HR 160, RR 14, Temp 99 F
Lightweight !!(Even for a pig.)
Positive for bacon !!
8/30/2011
22
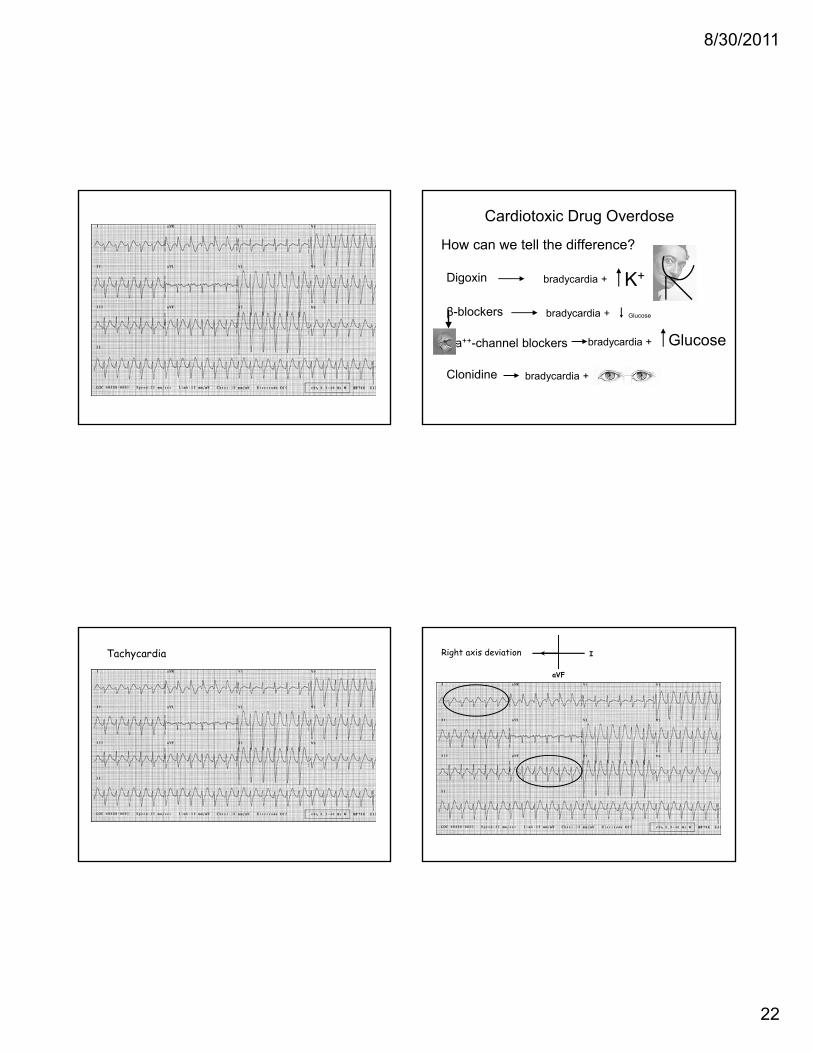
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
Tachycardia I
aVF
Right axis deviation
8/30/2011
23
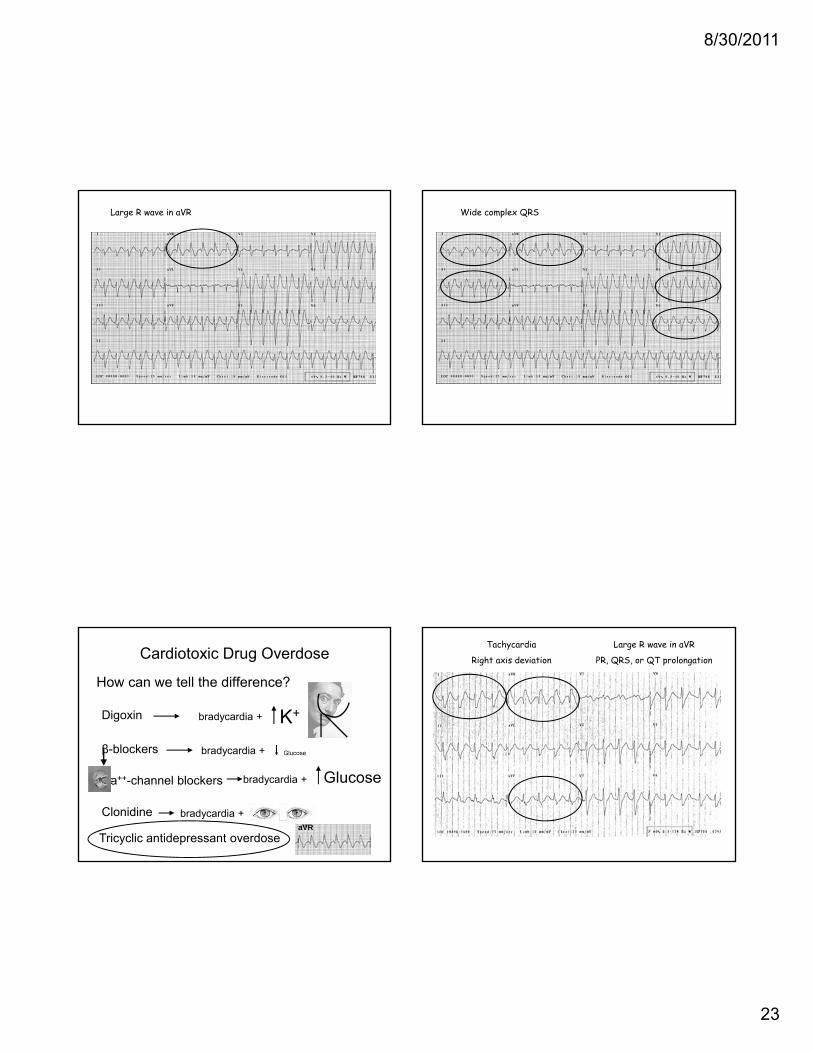
Large R wave in aVR Wide complex QRS
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
Tricyclic antidepressant overdoseaVR
Tachycardia
Right axis deviation
Large R wave in aVR
PR, QRS, or QT prolongation
8/30/2011
24
Tricyclic Antidepressant Overdose•
QRS widening• associated with development of seizures and
arrhythmias• can be used to assess severity of TCA toxicity• QRS < 100 ms: unlikely to develop seizures and
arrhythmias• QRS > 100 ms:
• 34% of patients develop seizures• 14% of patients develop serious arrhythmias
• QRS > 160 ms: 50% of patients develop ventriculararrhythmias
Tricyclic Antidepressant Overdose
• A large R wave in aVR is a highly sensitive screening tool for TCA toxicity.
• Amplitude of R wave in aVR may be even more predictive of seizure and arrhythmia than QRS prolongation.• Liebelt, et al: R wave > 3 mm in aVR was 81% sensitive
and 73% specific for the development of seizures and arrhythmias
Tricyclic Antidepressant Overdose
• Treatment of TCA Overdose:• Airway management• Activated charcoal• Sodium bicarbonate
• Indications: • QRS widening, hypotension, dysrhythmias, seizures
• 1-2 amps IV bolus, then• 3 amps in 1 Liter D5W, infuse at 250 mL/hour IV
• Treat seizures with benzodiazepines• Treat hypotension with IV fluids and Levophed• Dopamine is usually ineffective
(TCAs deplete NE stores by blocking re-uptake.)
Tricyclic Antidepressant Overdose
• Use of anti-arrhythmic agents
• Avoid class Ia, Ic, II, and III
• Lidocaine (Ib), magnesium, and Dilantin may be useful

8/30/2011
25
Case # 1: Lights on. Nobody home.
• 3 y.o. female
• Lights on. Nobody home.• Blank stare. Rotary nystagmus.
Case # 1: Lights on. Nobody home.
• Initial treatment• Labs
• CBC: normal• BMP: normal• UA: normal• Tylenol / Salicylate:
negative
• CT head?normal
• Tox screen:Positive for PCP
Case # 1: Lights on. Nobody home.
• What now?– Child Protective Services– PICU
– Strangled theparents with our bare hands.
• Child recovered uneventfully in PICU.
• Parents sent to trauma center after being strangled.
• Child removed from home and sent to foster care.
Case #1: Follow-up

8/30/2011
26
8 months later . . .
• Court Summons
“Hello, attorney?”
Case # 1: Lights on. Nobody home.
• Toxicology expert for Defense:
“This was a classic case of . . .. . . dextromethorphan overdose, not PCP intoxication.”
Case # 1: Lights on. Nobody home.
“The patient broke into a medicine cabinet with a lead pipe in the conservatory, and was discovered by the maid, Ms. White.”

8/30/2011
27
Case # 1: Lights on. Nobody home.
“Dextromethorpan is present in many cough and cold medications.
“Accidental overdose inchildren is common.”
Case # 1: Lights on. Nobody home.
“Intentional recreational overdose in adolescents and young adults is also common.
“I’ve never touched the stuff.
“Honest.”
Case # 1: Lights on. Nobody home.
“An ingestion of 5-10 times the recommended dose of dextromethorphan can be toxic and induce a dissociative state, much like ketamine.”
Case # 1: Lights on. Nobody home.
“Oof!! Someone just hit me over the head with a wrench!”
“Trying to suppress my testimony, no doubt.”

8/30/2011
28
Case # 1: Lights on. Nobody home.
“The chemical structures of dextromethorphan and PCP are very similar, and may cause a false positive result for PCP on hospital toxicology screens.”
Case # 1: Lights on. Nobody home.
“Confirmatory testing by an outside laboratory is always recommended in cases of suspected child abuse.”
Case # 1: Lights on. Nobody home.
“Dextromethorphan can also induce Seratonin Syndrome in patients who are taking an SSRI.”
Case # 1: Lights on. Nobody home.
“Symptoms include muscle rigidity, hyperthermia, altered mental status, and hyperreflexia which is more profound in the lower extremities.”

8/30/2011
29
Case # 1: Lights on. Nobody home.
“Agghpphcchtt!!!
“Someone just tried to strangle me with a rope!!
“Trying to suppress my testimony, no doubt.”
Case # 1: Lights on. Nobody home.
“Treatment for dextromethorphan overdose is mostly supportive.”
Case # 1: Lights on. Nobody home.
“Treatment for Seratonin Syndrome includes benzodiazepines, cooling, and for severe cases, cyproheptadine.”
Case # 1: Lights on. Nobody home.
“Treatment for wounds sustained by this revolverthat’s being pointed at me by Ms. Scarlett may be more extensive.”
8/30/2011
30
What did we learn?
• Alcohol isn’t the only drug that can cause altered mental status.
• Be very careful with intoxicated patients.– Poor historians.– Poor judgement.– Prone to trauma.– Smelly and obnoxious = no physical exam– Delayed diagnosis of life-threatening
conditions.
What did we learn?
• Prescription medication overdoses are common.
• They are also more likely to be missed.– Often not suspected.– Most meds don’t show up on a tox screen.– Most don’t have levels to check.
What did we learn?
• Many prescription medication overdoses can be lethal.
• Many commonly prescribed medications can be cardiotoxic in overdose.– Digoxin– β-blockers– Calcium channel blockers– Clonidine– Tricyclic antidepressants
How can we tell the difference?
Digoxin
β-blockers
Ca++-channel blockers
Clonidine
bradycardia +
bradycardia +
K+
Glucose
Cardiotoxic Drug Overdose
bradycardia + Glucose
bradycardia +
Tricyclic antidepressant overdoseaVR

8/30/2011
31
What did we learn?• Treatment differs depending on the drug.
– Digoxin• Digibind
– β-blockers• Atropine, pacing, glucagon, calcium
– Calcium channel blockers• Atropine, pacing, glucagon, calcium• High-dose insulin therapy
– Clonidine• Naloxone
– Tricyclic antidepressants• NaHCO3, benzodiazepines, Levophed, lidocaine
What did we learn?• Don’t jump to conclusions. • Many drugs can trigger
false positives ontoxicology screens.
• Admit to the PICU
• Notify CPS
• Reserve judgment of the parents for another day.
Thanks for listening.