
Analysis of an Interferon-γ Gene ( IFNG ) Polymorphism in Danish and...
7
JOURNAL OF INTERFERON AND CYTOKINE RESEARCH 17:87-93 (1997) Mary Ann Liebert, Inc. Analysis of an Interferon-y Gene (IFNG) Polymorphism in Danish and Finnish Insulin-Dependent Diabetes Mellitus (IDDM) Patients and Control Subjects FLEMMING POCIOT,1 RIITTA VEIJOLA,2 JESPER JOHANNESEN,1 PERNILLE M. HANSEN,1 TOVE LORENZEN,1 ALLAN E. KARLSEN,1 HELENA REIJONEN,3 MIKAEL KNIP,2 J0RN NERUP,1 and THE DANISH STUDY GROUP OF DIABETES IN CHILDHOOD ABSTRACT A CA-repeat polymorphism within the first intron of the interferon (IFN)-y gene was analyzed. This poly- morphism was recently demonstrated to be associated with insulin-dependent diabetes mellitus (IDDM) in Japanese subjects. We typed 266 IDDM patients and 195 control subjects of Danish Caucasoid origin. No sig- nificant differences in alíele or genotype frequencies between patients and control were observed. In addition, we typed 168 IDDM and 110 control subjects of Finnish origin. A significant disease association of the studied IFN-y allelic pattern was found (p = 0.029). Analysis of data according to HLA-DQB1 susceptibility status did not reveal heterogeneity of risk at the IFN-y locus in either of the populations. Fifty-five Danish and 94 Finnish IDDM multiplex families with at least two affected siblings (660 individuals) were typed to test for transmis- sion disequilibrium (TDT). No evidence for overall transmission disequilibrium using either an alíele-wise (p = 0.42; combined data) or a genotype-wise analysis (p = 0.21; combined data) could be detected. Thus, the mod- est significance level observed in the Finnish case-control study and the failure to replicate it by the TDT pro- vide little support for the hypothesis that the IFN-y gene microsatellite is associated with IDDM. I INTRODUCTION hesion molecules*18-19' on various cells, including pancreatic beta cells. It may also modulate the processing of exogenous nsulin-dependent diabetes mellitus (IDDM) is caused by (MHC class II) antigens by human monocytes.(20) Transgenic an immune-mediated, selective destruction of the pancreatic mice expressing IFN-y by pancreatic beta cells develop au- beta cells triggered by unknown environmental factors in ge- toimmune diabetes/21>22) and postnatal anti-IFN-y treatment netically susceptible individuals. Recent studies have affirmed prevents pancreatic inflammation in this model.<23) Antibodies the polygenic nature and genetic heterogeneity of IDDM/1^1' to IFN-y also protect against diabetes development in NOD Cytokines may mediate pancreatic beta cell damage during mice(24,25) and in BB rats/26' Finally, IFN-y is expressed in the early stages of IDDM/5_7) The cytokine interferon (IFN)- late-stage insulitis of recent-onset IDDM patients.(27) The re- y, alone or in combination with interleukin-1 (IL-1) or tumor ported actions of IFN-y are consistently diabetes promoting, necrosis factor (TNF)-cdß or both, was suggested to be cyto- and, therefore, the IFN-y gene (IFNG) is an obvious candidate toxic to beta cells by our model of pathogenesis of IDDM/5,6) gene for conferring susceptibility to IDDM. This has been shown subsequently to be the case in rat, mouse, The IFNG is a single copy gene that contains three introns and human pancreatic islets in vitro(8~13) at least in part via gen- and four exons encoding a polypeptide of 166 amino acids, 20 eration of nitric oxide/8,14' IFN-y is a product of T lympho- of which constitute the signal peptide/28,29' and has been as- cytes and natural killer (NK) cells, possesses unique im- signed to 12q24.12.(30) A dinucleotide repeat polymorphism of munomodulatory properties, and can affect also nonlymphoid this gene has been reported/31' This polymorphism was subse- tissues. In addition to the direct effect on beta cells, IFN-y may quently demonstrated to be associated with IDDM in a Japanese play a role in the pathogenesis of IDDM for the following rea- population*32' where the IDDM incidence is low. sons: IFN-y upregulates MHC class I,(15> class H/16'17' and ad- In the present study, we analyzed this polymorphism in an 'Steno Diabetes Center, DK-2820 Gentofte, Denmark. 2University of Oulu, Department of Pediatrics, FIN-90220 Oulu, Finland. 'University of Turku, Department of Virology, FIN-20520 Turku, Finland. 87
Transcript of Analysis of an Interferon-γ Gene ( IFNG ) Polymorphism in Danish and...

JOURNAL OF INTERFERON AND CYTOKINE RESEARCH 17:87-93 (1997)Mary Ann Liebert, Inc.
Analysis of an Interferon-y Gene (IFNG) Polymorphism inDanish and Finnish Insulin-Dependent Diabetes Mellitus
(IDDM) Patients and Control Subjects
FLEMMING POCIOT,1 RIITTA VEIJOLA,2 JESPER JOHANNESEN,1 PERNILLE M. HANSEN,1TOVE LORENZEN,1 ALLAN E. KARLSEN,1 HELENA REIJONEN,3 MIKAEL KNIP,2 J0RN NERUP,1
and THE DANISH STUDY GROUP OF DIABETES IN CHILDHOOD
ABSTRACT
A CA-repeat polymorphism within the first intron of the interferon (IFN)-y gene was analyzed. This poly-morphism was recently demonstrated to be associated with insulin-dependent diabetes mellitus (IDDM) inJapanese subjects. We typed 266 IDDM patients and 195 control subjects of Danish Caucasoid origin. No sig-nificant differences in alíele or genotype frequencies between patients and control were observed. In addition,we typed 168 IDDM and 110 control subjects of Finnish origin. A significant disease association of the studiedIFN-y allelic pattern was found (p = 0.029). Analysis of data according to HLA-DQB1 susceptibility status didnot reveal heterogeneity of risk at the IFN-y locus in either of the populations. Fifty-five Danish and 94 FinnishIDDM multiplex families with at least two affected siblings (660 individuals) were typed to test for transmis-sion disequilibrium (TDT). No evidence for overall transmission disequilibrium using either an alíele-wise (p =
0.42; combined data) or a genotype-wise analysis (p = 0.21; combined data) could be detected. Thus, the mod-est significance level observed in the Finnish case-control study and the failure to replicate it by the TDT pro-vide little support for the hypothesis that the IFN-y gene microsatellite is associated with IDDM.
IINTRODUCTION hesion molecules*18-19' on various cells, including pancreatic
beta cells. It may also modulate the processing of exogenousnsulin-dependent diabetes mellitus (IDDM) is caused by (MHC class II) antigens by human monocytes.(20) Transgenican immune-mediated, selective destruction of the pancreatic mice expressing IFN-y by pancreatic beta cells develop au-
beta cells triggered by unknown environmental factors in ge- toimmune diabetes/21>22) and postnatal anti-IFN-y treatmentnetically susceptible individuals. Recent studies have affirmed prevents pancreatic inflammation in this model.<23) Antibodiesthe polygenic nature and genetic heterogeneity of IDDM/1^1' to IFN-y also protect against diabetes development in NOD
Cytokines may mediate pancreatic beta cell damage during mice(24,25) and in BB rats/26' Finally, IFN-y is expressed inthe early stages of IDDM/5_7) The cytokine interferon (IFN)- late-stage insulitis of recent-onset IDDM patients.(27) The re-
y, alone or in combination with interleukin-1 (IL-1) or tumor ported actions of IFN-y are consistently diabetes promoting,necrosis factor (TNF)-cdß or both, was suggested to be cyto- and, therefore, the IFN-y gene (IFNG) is an obvious candidatetoxic to beta cells by our model of pathogenesis of IDDM/5,6) gene for conferring susceptibility to IDDM.This has been shown subsequently to be the case in rat, mouse, The IFNG is a single copy gene that contains three intronsand human pancreatic islets in vitro(8~13) at least in part via gen- and four exons encoding a polypeptide of 166 amino acids, 20eration of nitric oxide/8,14' IFN-y is a product of T lympho- of which constitute the signal peptide/28,29' and has been as-
cytes and natural killer (NK) cells, possesses unique im- signed to 12q24.12.(30) A dinucleotide repeat polymorphism ofmunomodulatory properties, and can affect also nonlymphoid this gene has been reported/31' This polymorphism was subse-tissues. In addition to the direct effect on beta cells, IFN-y may quently demonstrated to be associated with IDDM in a Japaneseplay a role in the pathogenesis of IDDM for the following rea- population*32' where the IDDM incidence is low.sons: IFN-y upregulates MHC class I,(15> class H/16'17' and ad- In the present study, we analyzed this polymorphism in an
'Steno Diabetes Center, DK-2820 Gentofte, Denmark.2University of Oulu, Department of Pediatrics, FIN-90220 Oulu, Finland.'University of Turku, Department of Virology, FIN-20520 Turku, Finland.
87

88 POCIOT ET AL.
IDDM intermediate-risk population of Danish origin and in an
IDDM high-risk Finnish population.
MATERIALS AND METHODS
SubjectsThe study population comprised the following subgroups: ( 1 )
266 IDDM patients of Danish Caucasoid origin. Of these, 55were identified as probands of IDDM multiplex families in a
nationwide population-based survey/33' All family members(257 individuals) from these families were typed in order toevaluate a possible distortion in transmission of disease-asso-ciated alíeles/34' The other IDDM patients were identifiedthrough the outpatient clinic at Steno Diabetes Center. They allfulfilled the WHO criteria for IDDM, and all were diagnosedbefore the age of 30 years. (2) The second group was 195 eth-nically matched, unrelated control individuals. None had a fam-ily history of IDDM or other endocrinopathies. (3) The thirdgroup was made up of 168 Finnish IDDM patients with youngage at diagnosis (mean age ± SD at diagnosis: 5.04 ± 3.28years). Of these, 94 were probands from IDDM multiplex fam-ilies identified at pédiatrie units in Finland. Parents and IDDM-affected siblings from these families (403 individuals) were
typed to evaluate transmission of disease-associated alíeles/34'The sporadic cases represent all the IDDM patients youngerthan 10 years at diagnosis (mean age ± SD at diagnosis: 6.3 ±3.2 years) who were admitted to the Department of Pediatrics,University of Oulu, Oulu, for initial treatment of IDDM since1989. (4) The fourth group was 110 Finnish healthy school-children from five municipalities in the Province of Oulu, whoserved as control subjects.
GenotypingDNA was prepared by standard procedures from leuko-
cytes/35' A CA repeat polymorphism of intron 1 of the IFN-ygene<31) was analyzed in the present study. The CA repeat was
amplified by PCR using the following primers: 5'-Biotin-AATTGA TTT TAT TCT TAC-3' and 5'-TTG CTG TAG GGTATT ATT-3'. PCR amplification was 94°C for 5 min, then 30cycles each consisting of 94°C for 60 sec, 42°C for 30 sec, and72°C for 40 sec, followed by 72°C for 10 min, performed in a
Perkin Elmer Cetus Thermal Cycler. The PCR mixture con-
tained 100 ng genomic DNA, 50 pM of each dNTP, 1 pM ofeach primer, and 1 U Taq polymerase/sample in 1 X PCR buffer(Promega Corp., Madison, WI) with 2 mM MgCb in a 20 mlreaction volume. Twenty microliters of stop buffer (98% for-mamide) was added to the PCR product, and the sample washeated for 2 min at 94°C and placed on ice. Eight microlitersof this mixture was analyzed on an 8% polyacrylamide gel at65 W. Afterward, the PCR products were transferred to an un-
charged nylon membrane (IMMOBILON-S, Millipore Corp.,Bedford, MA) and UV cross-linked (UV Stratalinker 2400,Stratagene, La Jolla, CA). The membrane was then blocked by10% SDS, 0.9% NaCl for 2-5 min, and then covered with 0.5%SDS, 0.9% NaCl containing 1 mg/ml streptavidin-HRP (Sigma,St. Louis, MO) for 4 min with gentle shaking. The membranewas washed twice in 0.5% SDS, 0.9% NaCl and once in wa-ter. The PCR products were detected using the ECL gene de-
tection reagents (Amersham, Buckinghamshire, UK) accordingto the manufacturer's directions. The membrane was exposedto x-ray film for 1-5 min.
SequencingFor preparation of single-stranded templates of PCR prod-
ucts, Dynabeads M-280 (Dynal A.S., Oslo, Norway) with chem-ically bound streptavidin were used according to the manufac-turer's instructions. Briefly, 20 pi of washed beads suspensionwas used per sequence reaction. The PCR product was incu-bated with the beads for 15 min at room temperature, with fre-quent resuspension. Then, the beads were washed with TE-buffer (10 mM Tris-HCl, pH 7.5, 1 mM EDTA, pH 8.0),resuspended in 10 pi 0.1 M NaOH, and incubated for 5 min atroom temperature. The beads were pelleted in an MPC-E mag-net (Dynal AS), washed, and resuspended in 7 pi dH^O.Sequencing was performed using the Sequenase kit, version 2.0(U.S. Biochemical Corp., Cleveland, OH) and 35S-dATP(Amersham).
HLA-DQB1 typingDQB1 typing of the Danish material was performed using
standard procedures, as previously reported/4' The DQB 1 typ-ing of the Finnish material was based on solution hybridizationwith lanthanide-labeled oligonucleotide probes detected withtime-resolved fluorometry, as described in detail elsewhere/36'Sequence-specific oligonucleotide probes for identification ofthe DQB 1*0302, 0201, 0301, and 0602/3 alíeles were used inthe analysis.
Statistical analysisCategorical comparisons were made by the ^-test or Fisher's
exact test, whichever was appropriate. Five percent (two-tailed)was chosen as level of significance. Odds ratios (OR) were cal-culated by Woolf s formula/37' An extended transmission dis-equilibrium test (TDT) for multiallele marker loci was used toassess transmission from heterozygous parents to offspring bythe software package EDTD version 1.1Z38'
RESULTS
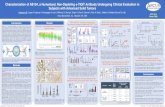
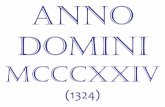
A total of five different sized alíeles were identified in thepresent study (Fig. 1 ). Each of these alíeles varied with one CArepeat (11-15), as verified by sequence analysis (Fig. 2). In ad-dition, we identified a single nucleotide substitution, just up-stream of the CA repeat sequence, in position 1348 of the pub-lished sequence/28' This T —» A transversion, which introducedan extra CA repeat, did not show disease restriction or absolutelinkage to any of the CA-repeat alíeles and was not further in-vestigated.
No differences were found between familial and nonfamil-ial IDDM cases in either of the populations, and these sub-groups were analyzed together. The global allelic distributionin the Danish population is shown in Table 1. No significantdifferences in allelic or genotype frequencies (not shown) were
observed (p = 0.73 and p = 0.53, respectively). As thestrongest association with IDDM was reported in Japanese sub-

IFN-y GENE POLYMORPHISM IN IDDM 89
FIG. 1. PCR products of the CA repeat within the first intronof the IFN-y gene. Five alíeles were detected and designatedA11-A15 according to the number of repeats. Genotypes rep-resenting all five alíeles are shown.
jects with clinical onset £ 10 years of age, the Danish popula-tion was stratified accordingly (Table 1). Still, no significantdifferences in allelic and genotype frequencies were observed(p = 0.7 and p = 0.5, respectively).
The allelic distribution in the Finnish population is shown inTable 2. A significant difference in the global allelic distribu-tion was observed between patients and controls (p = 0.029),and a trend for difference in genotype distribution (not shown)was found (p = 0.077). The difference in allelic distribution
A12/A12 A13/13 A13/13TGCA TGCA TGCA
^Hh WKbb <MMPK «• 1 - p —•* Si
-
—
[CA]n
was due to an increased frequency of the A12 allel and a de-creased frequency of the A14 and A15 alíeles in patients.Consequently, different frequencies of various genotypes were
observed in the two groups: 61.9% A12 positive patients vs.
49.1% controls (p = 0.035) (OR 1.7, 95% CI 1.05-2.7) and25.0% A14-positive and/or A15-positive patients vs. 41.8%controls (p = 0.003) (OR 0.46, 95% CI 0.31-0.67). The geno-type frequencies in both Danish and Finnish control and IDDMpopulations did not deviate from the expected values by Hardy-Weinberg equilibrium.
To investigate if there was any difference at IFNG accordingto HLA-DQB associated susceptibility in the Finnish population,a direct comparison was made of the DQB 1*0201/DQB 1*0302-positive, the DQB 1 *0302-positive/DQB 1*0201 -negative, theDQBl*0201-positive/DQBl*0302-negative, and the DQB1*-0201-negative/DQBl*0302-negative diabetic subjects. No het-erogeneity of risk at IFNG according to the HLA-DQB 1 statuscould be demonstrated (p = 0.36, x2 = 13.06, 12df) (Table 3),although the DQB1*0201/X group had a higher frequency of theA12 alíele compared with the other groups (p = 0.02, uncor-
rected). Individuals positive for DQB 1*0602/3 (n = 14) were
studied separately and did not differ from IDDM patients withother studied HLA-DQB 1 specificities (data not shown). In theDanish population, HLA-DQB 1 data were available from 156IDDM subjects. Stratifying for DQB1 status did not reveal anysignificant differences in this material (data not shown).
To further investigate the IFNG polymorphism in relation toIDDM, we typed 55 Danish and 94 Finnish IDDM multiplexfamilies with at least two IDDM-affected offspring and per-formed an extended TDT for a marker with multiple alíeles/38'One hundred eighteen and 218 transmissions from Ijeterozy-gous patients were observed in the Danish and the Finnish fam-ily material, respectively. First, a genotype-wise analysis was
performed. In this analysis, every heterozygous parental geno-type was considered separately, and it was determined if eachalíele of the genotype was transmitted to affected offspring on
50% of occasions. Second, an analysis was performed to testfor preferential transmission of certain alíeles across genotypes.Initially, the Danish and Finnish family data sets were analyzedseparately. No differences between the two data sets were ob-served, and the data were pooled (Table 4). No evidence foroverall transmission disequilibrium using either the allele-wise(p = 0.42) or the genotype-wise (p = 0.21) analysis was found.Also, no evidence for a distorted transmission of individual al-íeles was found (Table 5).
When comparing the two populations, differences were
found between control subjects (p < 0.00001) as well as be-tween IDDM patients (age at onset :£ 10 years) (p = 0.03).
DISCUSSION
FIG. 2. Sequence of the CA repeat region from three indi-viduals. Two individuals are A13/A13 homozygous and one isA12/A12 homozygous. The CA repeats are indicated at the left.A new polymorphism, aA^T transition, was detected by se-
quencing this region. The position of this single base substitu-tion is indicated with an arrow. The first individual is A/A, thenext is A/T, and the individual to the right is T/T.
In the present study, we found evidence for an associationof a CA-repeat polymorphism within the first intron of the IFN-y gene and IDDM in a Finnish but not in a Danish population.We were able to identify only 5 alíeles of this polymorphismdespite typing a very large number of unrelated individuals (n =
888), control and IDDM subjects, from two Scandinavian pop-ulations. This was in contrast to the original report describingthe polymorphism/31' where 6 alíeles were reported with the

90 POCIOT ET AL.
Table 1. Allelic Distribution and Frequencies of CA-Repeat Polymorphismof IFN-y Gene in Danish Control and IDDM Subjects"
Alíele All A12 A13 A14 A15
Control subjects (n = 390) 0 183 166 27 140 0.469 0.426 0.069 0.036
IDDM patients (n = 532) 2 253 222 30 250.004 0.476 0.417 0.056 0.047
IDDM patients diagnosed 0 149 127 18 16<10 years (n = 310) 0 0.481 0.410 0.058 0.052
an is number of chromosomes, x2—
2-78 (4 df); p = 0.6 for comparing control subjects and IDDM patients.X2 = 1.48 (3 df); p = 0.7 for comparing control subjects and IDDM patients with age at onset before 10 years.
apparent lack of the A14 alíele (our nomenclature) but the ad- We were not able to demonstrate any association of IFNGditional identification of alíeles corresponding to Al 6 and A17. polymorphism with IDDM in the Danish population. TheThat study was based on analysis of 54 chromosomes of unre- strongest association with IDDM in Japanese individuals was
lated individuals of African, Asian, and European origin/31' In reported for patients with young age at diagnosis, that is, ^10the Japanese population, the presence of 8 alíeles was re- years/32'Therefore, the Danish data were analyzed with respectported/32' However, the exact length of the PCR-identified al- to age at diagnosis of IDDM. Still, no evidence for an IDDMleles or the number of CA repeats of the different alíeles were association of IFNG polymorphism was found. In contrast, datanot reported, and comparison of data, including evaluation of from the Finnish population demonstrated a significant IDDMthe IDDM association, from the different studies is, therefore, association based on allelic frequency and a trend based on
difficult. Nevertheless, the CA repeat polymorphism of the first genotypic frequency. The frequency of the A12 alíele was in-intron of the IFNG locus seems to vary considerably between creased in patients, and A12-positive genotypes were signifi-ethnically different populations. In the present study, a highly cantly more frequent in patients, whereas the frequency of thesignificant difference in allelic distribution was observed be- AI*4 alíele was increased in controls, and A14-positive geno-tween the Danish and Finnish control subjects. types were significantly more frequent in controls.
Table 2. Allelic Distribution and Frequencies of IFN-y GenePolymorphism in Finnish Control and IDDM Subjects"
Alíele All A12 A13 A14 A15
Control subjects (n = 220) 5 67 99 27 220.023 0.305 0.450 0.123 0.100
IDDM patients (n = 336) 9 139 143 25 200.027 0.414 0.426 0.074 0.060
an is number of chromosomes, x2 = 10.75 (4 df); p = 0.029 for comparing control subjects and IDDM pa-tients.
Table 3. Comparison of Allelic Frequencies of IFNG in Finnish IDDMSubjects According to HLA-DQB 1 Status (Heterogeneity of Risk)
Alíele AU A12 A13 A14 A15
DQB 1*0201-DQB l*0302(n = 53)a 4 46 43 6 70.038 0.434 0.406 0.057 0.066
DQB1*0302/Xb(n = 81) 4 59 77 11 110.025 0.364 0.475 0.068 0.068
DQB1*0201/XC (n = 22) 0 26 12 4 20.591 0.273 0.091 0.045
Xd/Xd (n = 12) 1 10 10 3 00.042 0.417 0.417 0.125
an is number of individuals.bNon-DQB 1*0201.cNon-DQB 1*0302.dNon-DQB 1*0201, non-DQB 1 *0302.X2 = 13.06 (12 df); p = 0.36.

IFN-y GENE POLYMORPHISM IN IDDM 91
Table 4. Observed Heterozygous Parental Genotypesand Frequencies of Transmitted Alleles in Combined
Danish and Finnish Family Material
Parental genotype*
A11/A12A11/A13A11/A15A12/A13A12/A14A12/A15A13/A14A13/A15A14/A15
411
2184
25392939
3
First alíele ofgenotype transmitted0
(n)
232
1039
231517
2
"X2 for genotype TDT = 12.03 (9 df); p = 0.21.V TDT = 3.88 (4 df); p = 0.42.
in the Finnish case-control study and the failure to replicate itby TDT provide little support for the hypothesis that the IFNGmicrosatellite is associated with IDDM.
However, to firmly establish or exclude the possible role ofIFNG polymorphism in IDDM susceptibility, other ethnic pop-ulations need to be studied. Furthermore, it is necessary to con-
firm whether it is the same alíele demonstrating disease asso-
ciation in the Finnish and the Japanese populations, and, finally,the possible functional significance of this polymorphismshould be studied.
ACKNOWLEDGMENTS
The skillful technical assistance of Bodil Bosmann is greatlyappreciated. The Danish material was in part collected by theDanish Study Group of Diabetes in Childhood (DSGD). F.P. isthe recipient of a research grant from the Danish MedicalResearch Council (J.no. 12-1857-1).
We found no heterogeneity of risk at IFNG according toHLA-DQB 1 status, although we cannot ignore the fact that theA12 alíele is more frequent in the DQB1*0201/X group.Previous reports have observed that non-MHC susceptibilitygenes exert their maximum effect in diabetic subjects with thelowest MHC class Il-associated susceptibility/39^*2' This in-cludes studies of populations of Finnish origin/41'42' The pre-sent case-control data may suggest an independent (of MHC),although minor, contribution of IFNG to IDDM susceptibilityin the Finnish population. However, analysis of 55 Danish and94 Finnish families with multiple children affected with IDDMrevealed no evidence for linkage by the TDT of the studiedpolymorphism. Based on this analysis, the observed differencein A12 alíele (or other alleles) frequency is likely to be of lim-ited relevance with regard to conferring susceptibility to IDDM.There is substantial reason to believe that techniques for test-
ing for association, such as the TDT, that use family-based con-
trols are much more sensitive and less prone to error than are
case-control studies/43^15' The differences observed in theFinnish case-control study may, therefore, derive from (an un-
known) population stratification. If the data of Awata et al/32'claiming a highly significant association between IFNG andJapanese IDDM patients diagnosed before 10 years of age, are
reconsidered once the p values are corrected (both for allelesanalyzed and number of tests performed), the statistical signif-icance would be substantially reduced to almost marginal sig-nificance. In conclusion, the modest significance level observed
REFERENCES
BENNETT, S.T., LUCASSEN, A.M., GOUGH, S.C.L., POWELL,E.E., UNDLIEN, D.E., PRITCHARD, L.E., MERRIMAN, M.E.,KAWAGUCHI, Y., DRONSFIELD, M.J., POCIOT, F., NERUP,J., BOUZEKRI, N, CAMBON-THOMSEN, A., R0NNINGEN,K,S., BARNETT, A.H., BAIN, S.C., and TODD, J.A. (1995).Susceptibility to human type 1 diabetes at IDDM2 is determinedby tandem repeat variation at the insulin gene minisatellite locus.Nature Genet. 9, 284-291.COPEMAN, J.B., HEARNE, C, CORNALL, R.J., REED, P.W.,CUCCA, F., R0NNINGEN, K.S., UNDLIEN, D.E., BÚZZETTI,R., NISTICÖ, L., TOSI, R„ POCIOT, F., NERUP, J., CORNELIS,F., BARNETT, A.H., BAIN, S.C., and TODD, J.A. (1995). Finelocalisation of a type 1 diabetes susceptibility gene (IDDM7) tohuman chromosome 2q by linkage disequilibrium mapping. NatureGenet. 9, 80-85.DAVIES, J.L., KAWAGUCHI, Y., BENNETT, ST., COPEMAN,J.B., CORDELL, H.J., PRITCHARD, L.E., REED, P.W., GOUGH,S.C.L., JENKINS, S.C., PALMER, S.M., BALFOUR, K.M.,ROWE, B.R., FARRALL, M., BARNETT, A.H., BAIN, S.C., andTODD, J.A. (1994). A genome-wide search for human suscepti-bility genes. Nature 371, 130-136.POCIOT, F„ R0NNINGEN, K.S., BERGHOLDT, R., LOREN-ZEN, T., JOHANNESEN, J., YE, K, DINARELLO, CA.,NERUP, J., and THE DANISH STUDY GROUP OF DIABETESIN CHILDHOOD. (1994). Genetic susceptibility markers in Danishpatients with type 1 (insulin-dependent) diabetes—Evidence forpolygenecity in man. Autoimmunity 19, 169-178.
Table 5. Transmission for Individual Alleles inCombined Danish and Finnish Data Sets"
Alíele All A12 A13 A14 A15
PassedNot passedX2p values
7100.5290.47
137115
1.9210.17
121142
1.6770.20
3225
0.8600.35
3944
0.3010.58
"Table provides the total number of times each alíele was transmitted or not transmitted fromheterozygous parents; i.e., each transmission is included twice: once for the alíele that is trans-mitted and once for the alíele that is not. p values are not corrected for multiple testing.

92 POCIOT ET AL.
5. MANDRUP-POULSEN, T., HELQVIST, S., WOGENSEN, L.D.,M0LVIG, J., POCIOT, F., JOHANNESEN, J., and NERUP, J.(1990). Cytokines and free radicals as effector molecules in the de-struction of pancreatic beta cells. Curr. Top. Microbiol. Immunol.164, 169-193.
6. NERUP, J., MANDRUP-POULSEN, T., HELQVIST, S., AN-DERSEN, H.U., POCIOT, F., REIMERS, J.I., CUARTERO, B.G.,KARLSEN, A.E., BJERRE, U., and LORENZEN, T. (1994). Onthe pathogenesis of IDDM. Diabetologia 37 (Suppl. 2), S82-S89.
7. RABINOVITCH, A. (1993). Roles of cytokines in IDDM patho-genesis and islet B-cell destruction. Diabetes Rev. 1, 215-240.
8. CETKOVIC-CVRLJE, M., and EIZIRIK, D.L. (1994). TNF-a andIFN-y potentiate the deleterious effects of IL-Iß on mouse pan-creatic islets mainly via generation of nitric oxide. Cytokine 6,399-406.
9. CAMPBELL, I.L., ISCARO, A., and HARRISON, L.C. (1988).IFN-y and tumor necrosis factor«. Cytotoxicity to murine isletsof Langerhans. J. Immunol. 141, 2325-2329.
10. PUKEL, C, BAQUERIZO, H., and RABINOVITCH, A. (1988).Destruction of rat islet cell monolayers by cytokines. Synergisticinteractions of interferon- y, tumor necrosis factor, lymphotoxin,and interleukin 1. Diabetes 37, 133-136.
11. RABINOVITCH, A., SUAREZ-PINZON, W.L., SHI, Y., MOR-GAN, A.R., and BLEACKLEY, R.C. (1994). DNA fragmentationis an early event in cytokine-induced islet beta-cell destruction.Diabetologia 37, 733-738.
12. CORBETT, J.A., SWEETL, M.A., WANG, J.L., LANCASTER,J., and McDANIEL, M.I. (1993). Nitric oxide mediates cytokine-induced inhibition of insulin secretion by human islets ofLangerhans. Proa Nati. Acad. Sei. USA 90, 1731-1735.
13. EIZIRIK, D.L., SANDLER, S., WELSH, N., CETKOVIC-CVRLJE, M., NIEMAN, A., GELLER, D.A., PIPELEERS, D.G.,BENUTZEN, K., and HELLERSTRÖM, C. (1994). Cytokine sup-press human islet function irrespective of their effects on nitric ox-
ide generation. J. Clin. Invest. 93, 1968-1974.14. CORBETT, J.A., and McDANIEL, M.L. (1995). Intraislet release
of interleukin 1 inhibits ß cell expression of inducible nitric oxidesynthase. J. Exp. Med. 181, 559-568.
15. CAMPBELL, I.L., WONG, G.H.W., SCHRADER, J.W., andHARRISON, L.C. (1985). Interferon-y enhances the expression ofthe major histocompatibility class I antigens on mouse pancreaticbeta cells. Diabetes 34, 1205-1209.
16. CAMPBELL, I.L., OXBROW, L., WEST, J., and HARRISON,L.C. (1988). Regulation of MHC protein expression in pancreaticß-cells by interferon y and tumor necrosis factor-a. Mol.Endocrinol. 2, 101-107.
17. PUJOL-BORELL, R., TODD, I., DOSHI, M., BOTTAZZO, G.F.,SUTTON, R., GRAY, D., ADOLF, G.R., and FELDMANN, M.(1987). HLA class II induction in human islet cells by interferon-y plus tumour necrosis factor or lymphotoxin. Nature 326,304-306.
18. CAMPBELL, I.L., CUTRI, A., WILKINSON, D., BOYD, A.W.,and HARRISON, L.C. (1989). Intercellular adhesion molecule 1 isinduced on isolated endocrine islet cells by cytokines but not byreovirus infection. Proc. Nati. Acad. Sei. USA 86, 4282-4286.
19. VIVES, M., SOLDEVILA, G, ALCALDE, L., LORENZO, C,SOMOZA, N., and PUJOL-BORRELL, R. (1991). Adhesion mol-ecules in human islet /3-cells. De novo induction of ICAM-1 butnot LFA-3. Diabetes 40, 1382-1390.
20. NADLER, S.G., RANKIN, B.M., MORAN-DAVIS, P., CLEVE-LAND, J.S., and KIENER, P.A. (1994). Effect of interferon-? on
antigen processing in human monocytes. Eur. J. Immunol. 24,3124-3130.
21. SARVETNICK, N., LIGGITT, D., PITTS, S.L., HANSEN, S.E.,and STEWART, T.A. (1988). Insulin-dependent diabetes mellitus
induced in transgenic mice by ectopic expression of class II MHCand interferon-gamma. Cell 52, 773-782.
22. SARVETNICK, N., SHIZURU, J., LIGGITT, D., MARTIN, L.,McINTYRE, B., GREGORY, A., PARSLOW, T., and STEWART,T. (1990). Loss of pancreatic islet tolerance induced by /3-cell ex-
pression of interferon-y. Nature 346, 844-847.23. WOGENSEN, L., MOLONY, L., GU, D., KRAHL, T., ZHU, S„
and SARVETNICK, N. (1994). Postnatal anti-interferon-y treat-ment prevents pancreatic inflammation in transgenic mice with ß-cell expression of interferon-y. J. Interferon Res. 14, 111-116.
24. CAMPBELL, I.L., KAY, T.W.H., OXBROW, L., and HARRI-SON, L.C. (1991). Essential role for interferon-y and interleukin-6 in autoimmune insulin-dependent diabetes in NOD/Wehi mice.J. Clin. Invest. 87, 739-742.
25. DEBRAY-SACHS, M., CARNAUD, C, BOITARD, C, COHEN,H., GRESSER, I., BEDOSSA, P., and BACH, J.-F. (1991).Prevention of diabetes in NOD mice treated with antibody tomurine IFNy. J. Autoimmunity 4, 237-248.
26. NICOLETTI, F., MERONI, P.L., LANDOLFO, S., GARAGLIO,M., GUZZARDI, S., BARCELLINI, W., LUNETTA, M., MUGH-INI, L., and ZANUSSI, C. (1990). Prevention of diabetes inBB/Wor rats treated with monoclonal antibodies to interferon-y.Lancet 336, 319.
27. FOULIS, A.K., McGILL, M., and FARQUHARSON, M.A. (1991).Insulitis in type 1 (insulin-dependent) diabetes mellitus in man—
Macrophages, lymphocytes, and interferon-y containing cells. J.Pathol. 165, 97-103.
28. GRAY, P.W., and GOEDDEL, D.V. (1982). Structure of the hu-man immune interferon gene. Nature 298, 859-863.
29! TAYA, Y., DEVOS, R., TAVERNIER, J., CHEROUTRE, H., EN-GLER, G, and FIERS, W. (1982). Cloning and structure of the hu-man interferon-y chromosomal gene. EMBO J. 1, 953-958.
30. TRENT, J.M., OLSON, S., and LAWN, R.M. (1982).Chromosomal localization of human leukocyte, fibroblast, and im-mune interferon genes by means of in situ hybridization. Proc. Nati.Acad. Sei. USA 79, 7809-7813.
31. RUIZ-LINARES, A. (1993). Dinucleotide repeat polymorphism inthe interferon-gamma (IFNG) gene. Hum. Mol. Genet. 2, 1508.
32. AWATA, T., MATSUMOTO, C, URAKAMI, T., HAGURA, R„AMEMIYA, S., and KANAZAWA, Y. (1994). Association ofpolymorphism in the interferon g gene with IDDM. Diabetologia37, 1159-1162.
33. POCIOT, F., N0RGAARD, K„ HOBOLTH, N., ANDERSEN, O.,NERUP, J., and THE DANISH STUDY GROUP OF DIABETESIN CHILDHOOD. (1993). A nationwide population-based studyof the familial aggregation of insulin-dependent diabetes inDenmark. Diabetologia 36, 870-875.
34. SPIELMAN, R.S., McGINNIS, R.E., and EWENS, W.J. (1993).Transmission test for linkage disequilibrium: The insulin gene re-
gion and insulin-dependent diabetes mellitus (IDDM). Am. J. Hum.Genet. 52, 506-516.
35. POCIOT, F., M0LVIG, J., WOGENSEN, L., WORSAAE, H.,DALB0GE, H., BAEK, L., and NERUP, J. (1991). A tumournecrosis factor beta gene polymorphism in relation to monokinesecretion and insulin-dependent diabetes mellitus. J. Scand.Immunol. 33, 37-49.
36. SJÖROOS, M., DTIA, A., ILONEN, J., REUONEN, H., andLÖVGREN, T. (1995). Triple-label hybridization assay for type-1diabetes-related HLA alleles. Biotechniques 18, 870-877.
37. WOOLF, B. (1955). On estimating the relation between bloodgroup and disease. Ann. Hum. Genet. 19, 251-253.
38. SHAM, P.C., and CURTIS, D. (1995). An extended transmis-sion/disequilibrium test (TDT) for multi-allele marker loci. Ann.Hum. Genet. 59, 323-336.
39. OWERBACH, D., and GABBAY, K.H. (1995). The HOXD8 lo-

IFN-y GENE POLYMORPHISM IN IDDM
cus (2q31) is linked to type I diabetes. Interaction with chromo-some 6 and 11 disease susceptibility genes. Diabetes 44, 132-136.
40. POCIOT, F., M0LVIG, J., WOGENSEN, L., WORSAAE, H., andNERUP, J. (1992). A TaqI polymorphism in the human interleukin-1/3 (IL-1/3) gene correlates with IL-1/3 secretion in vitro. Eur. J.Clin. Invest. 22, 396-402.
4L METCALFE, K.A., HITMAN, G.A., POCIOT, F., BERGHOLDT,R., TOUMILHETO-WOLF, E., TOUIMILHETO, J., VIS-VANATHAN, M., RAMACHANDRAN, A., NERUP, J., and THEDIME STUDY GROUP. (1995). A trans-racial study of associa-tion between IDDM and the interleukin-1 receptor type 1 gene.Diabetologia 38 (Suppl.l), 279 (abstract).
42. metcalfe, k.a., hitman, g.a., fennessy, m.j.,McCarthy, m.l, tuomiletho, j., tuomtletho-wolf, e.,and THE DIME STUDY GROUP. (1995). In Finland insulin gene re-
gion encoded susceptibility to IDDM exerts maximum effect whenthere is low HLA-DR associated risk. Diabetologia 38, 1223-1229.
93
43. EWENS, W.J., and SPIELMAN, R.S. (1995). The transmission dis-equilibrium test—History, subdivision and admixture. Am. J. Hum.Genet. 57, 455^164.
44. THOMSON, G (1995). Analysis of complex human genetictraits—An ordered notation method and new tests for mode of in-heritance. Am. J. Hum. Genet. 57, 474-486.
45. THOMSON, G. (1995). Mapping disease genes—Family-based as-
sociation. Am. J. Hum. Genet. 57, 487^198.
Address reprint requests to:Dr. Flemming Pociot
Steno Diabetes CenterDK-2820 Gentofte
Denmark
Received 23 July 1996/Accepted 4 October 1996







![Post-mortem histopathology underlying β-amyloid PET ...€¦ · A recent phase III trial of [18F]flutemetamol positron emission tomography (PET) imaging in 106 end-of-life subjects](https://static.fdocument.org/doc/165x107/6128f3e918ccd57368713d6a/post-mortem-histopathology-underlying-amyloid-pet-a-recent-phase-iii-trial.jpg)





