An Evaluation of Time-Amplitude Sonography in Ocular Diagnosis* *From the Department of Surgery...
7
CORRECTION OF PTOSIS 1103 6. Hess, C: Eine Operationmethode gegen Ptosis. Arch. f. Augenh., 28 :22-26, 1894. 7. Friedenwald, J. S., and Guyton, J. S.: A simple ptosis operation: utilization of the frontalis by means of a single rhomboid-shaped suture. Am. J. Ophth., 31 :411-414, 1948. 8. Schimek, R. Α.: Symposium: Ptosis complications. Tr. A m Acad. Ophth., 63 :664, Oct. 1959. 9. Machek: An operation for ptosis with the formation of a fold in the upper lid. Arch. Ophth., 44 :539-544, 1915. 10. Fergus, A. F.: Ptosis operations. Tr. Ophth. Soc. U. Kingdom, 28 :184-190, 1908. 11. Roberts, J. B.: A new muscle "substitution" operation for congenital palpebral ptosis. Ophth. Ree., 25 :397-402, 1916. 12. Schimek, R. Α.: A new ptosis operation utilizing both levator and frontalis. Α Α Arch. Ophth., 54:92-99, 1955. 13. Spaeth, Ε. B. : Principles and Practice of Ophthalmic Surgery. Philadelphia, Lea, 1944, p. 387. 14. Ibid: p. 394. 15. Derby: Fascia lata hammock for repair of ptosis. Am. J. Ophth., 11: (May) 1928. 16. Berke, R. N.: Symposium: Ptosis complications. Tr. Am. Acad. Ophth., 63 :663 (Oct.) 1959. 17. Callahan, Α.: Surgery of the Eye. Springfield, 111., Thomas, 1956, p. 27. 18. Crawford, J. S.: Repair of ptosis using frontalis muscle and fascia lata. Tr. Am. Acad. Ophth., 59:672-678 (Sept.-Oct.) 1956. 19. Berke, R. N. : Symposium: Ptosis complications. Tr. Am. Acad. Ophth., 63 :667 (Oct.) 1959. 20. Peer, L. Α.: Transplantation of Tissues. Baltimore, Williams & Wilkins, 1955, v. 1, p. 57. 21. Curtin, B. J.: Surgical support of the posterior sclera. Am. J. Ophth., 49:1341-1350 (June) 1960. 22. Bick, M. W.: Surgical treatment of scleromalacia perforans. Am. J. Ophth., 46:598 (Oct.) 1958. 23. Wiener and Alvis: Surgery of the Eye. Philadelphia, Saunders, 1939, p. 326. 24. Spaeth, Ε. Β.: Principles and Practices of Ophthalmic Surgery. Philadelphia, Lee, 1944, pp. 394- 398. 25. Arruga, H. : Ocular Surgery. New York, McGraw-Hill, 1952. AN EVALUATION OF TIME-AMPLITUDE SONOGRAPHY IN OCULAR DIAGNOSIS* EDWARD W. PURNELL, M.D., AND ADNAN SOKOLLU, D.SC. Cleveland, Ohio Two methods of ultrasonic localization are used clinically. In both methods pulses of high frequency sound are sent into the eye, where they strike the ocular tissues and produce echoes. The two methods differ in the way these echoes are analyzed. In the simplest method echoes are represented by vertical deflections on an oscilloscope. This has been termed a time-amplitude display. In the more complex second method, the echoes modulate the intensity of the oscillo- scope beam and are displayed as a series of bright spots which can be integrated into a cross-sectional representation of the eye. This has been termed an intensity-modulated display. * From the Department of Surgery (Ophthal- mology), Western Reserve University School of Medicine. The purpose of our investigations was to evaluate the usefulness of time-amplitude sonography in ocular diagnosis. Oksala and Lehtinen 5 reported the method to be of value in differentiating between certain eye tu- mors. Baum and Greenwood 1-4 challenge this view and give evidence that the time-ampli- tude display when used alone is of little if any clinical value. Our investigations were conducted with a modified industrial ultra- sonic flaw detector similar to that used by Oksala. These instruments are relatively low in cost and simple in operation and maintenance. Since they are readily avail- able for widespread use in ocular diagnosis, we prejudiced our evaluation of time-ampli- tude sonography with the limitations im- posed by this equipment. The industrial ultrasonic flaw detector is
Transcript of An Evaluation of Time-Amplitude Sonography in Ocular Diagnosis* *From the Department of Surgery...

C O R R E C T I O N O F P T O S I S 1103
6. H e s s , C : Eine Operationmethode gegen Ptos is . Arch . f. Augenh. , 28:22-26, 1894. 7. Friedenwald, J. S., and Guyton, J. S . : A simple ptosis operation: utilization of the frontalis by
means of a s ingle rhomboid-shaped suture. A m . J. Ophth., 31 :411-414, 1948. 8. Schimek, R. Α . : Sympos ium: Ptos i s complications. Tr . A m Acad. Ophth., 63 :664 , Oct. 1959. 9. Machek: A n operation for ptosis with the formation of a fold in the upper lid. Arch. Ophth.,
44 :539-544, 1915. 10. Fergus , A . F . : P tos i s operations. Tr. Ophth. Soc. U . Kingdom, 28:184-190, 1908. 11. Roberts, J. B . : A new muscle "substitution" operation for congenital palpebral ptosis. Ophth. Ree. ,
25:397-402, 1916. 12. Schimek, R. Α . : A n e w ptosis operation uti l izing both levator and frontalis. Α Μ Α Arch. Ophth.,
54:92-99, 1955. 13. Spaeth, Ε . B. : Principles and Pract ice o f Ophthalmic Surgery. Philadelphia, Lea, 1944, p. 387. 14. Ibid: p. 394. 15. D e r b y : Fasc ia lata hammock for repair of ptosis. A m . J. Ophth., 1 1 : ( M a y ) 1928. 16. Berke, R. N . : Sympos ium: Ptos i s complications. Tr . A m . Acad . Ophth., 6 3 : 6 6 3 ( O c t . ) 1959. 17. Callahan, Α . : Surgery of the E y e . Springfield, 111., Thomas , 1956, p. 27. 18. Crawford, J. S . : Repair o f ptosis us ing frontalis muscle and fascia lata. Tr . A m . Acad. Ophth.,
59:672-678 (Sept . -Oct . ) 1956. 19. Berke, R. N . : Sympos ium: Ptos i s complications. Tr. A m . Acad. Ophth., 6 3 : 6 6 7 ( O c t . ) 1959. 20. Peer , L. Α . : Transplantation of Tissues . Baltimore, Wi l l iams & Wilkins , 1955, v. 1, p. 57. 21. Curtin, B . J . : Surgical support of the posterior sclera. A m . J. Ophth., 49:1341-1350 (June) 1960. 22. Bick, M. W . : Surgical treatment of scleromalacia perforans. A m . J. Ophth., 4 6 : 5 9 8 ( O c t . ) 1958. 23. W i e n e r and A l v i s : Surgery of the Eye . Philadelphia, Saunders, 1939, p. 326. 24. Spaeth, Ε . Β . : Principles and Pract ices of Ophthalmic Surgery. Philadelphia, Lee, 1944, pp. 394-
398. 25. Arruga, H . : Ocular Surgery. N e w York, McGraw-Hi l l , 1952.
A N E V A L U A T I O N O F T I M E - A M P L I T U D E S O N O G R A P H Y
I N O C U L A R D I A G N O S I S *
E D W A R D W . P U R N E L L , M . D . , A N D A D N A N S O K O L L U , D . S C .
Cleveland, Ohio
Two methods of ultrasonic localization are used clinically. In both methods pulses of high frequency sound are sent into the eye, where they strike the ocular tissues and produce echoes. The two methods differ in the way these echoes are analyzed. In the simplest method echoes are represented by vertical deflections on an oscilloscope. This has been termed a time-amplitude display. In the more complex second method, the echoes modulate the intensity of the oscillo-scope beam and are displayed as a series of bright spots which can be integrated into a cross-sectional representation of the eye. This has been termed an intensity-modulated display.
* From the Department of Surgery (Ophthal-m o l o g y ) , Western Reserve Univers i ty School o f Medicine.
The purpose of our investigations was to evaluate the usefulness of time-amplitude sonography in ocular diagnosis. Oksala and Lehtinen5 reported the method to be of value in differentiating between certain eye tu-mors. Baum and Greenwood 1 - 4 challenge this view and give evidence that the time-ampli-tude display when used alone is of little if any clinical value. Our investigations were conducted with a modified industrial ultra-sonic flaw detector similar to that used by Oksala. These instruments are relatively low in cost and simple in operation and maintenance. Since they are readily avail-able for widespread use in ocular diagnosis, we prejudiced our evaluation of time-ampli-tude sonography with the limitations im-posed by this equipment.
The industrial ultrasonic flaw detector is

1104 E D W A R D W . P U R N E L L A N D A D N A N S O K O L L U
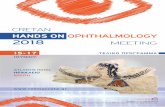
Fig . 1. (Purnel l and Soko l lu ) . Comparison of rectified-pulse and high frequency display, ( a ) Recti -fied pulse display, cornea and anterior surface of lens. Scale in mm. ( b ) H i g h frequency display of same echoes. Each large division equals 0.75 mm. Frequency, 10 mc.
properly termed a "rectified-pulse" display unit, for the patterns shown on the oscillo-scope screen are deflections triggered by echoes of predetermined amplitude. Un-wanted echoes of low amplitude can be eliminated from the display by increasing the amplitude required for an oscilloscopic deflection. On the other hand, significant information may be lost if all echoes of low amplitude are rejected. In adjusting the trigger circuit, the operator must use dis-cretion based on his knowledge of the struc-tures being examined.
In evaluating the industrial flaw detector
we compared the rectified-pulse display with its high frequency display on a second oscilloscope. The high frequency oscilloscope indicated all oscillations of the receiving crystal and was not dependent on amplitude for excitation. Figure 1 compares a triggered-pulse display of the anterior segment with the display obtained on the high frequency oscilloscope. The high frequency display is biphasic and shows all the oscillations in a single echo pulse. An echo of low amplitude is seen posterior to the double corneal echo on the high frequency display. This echo was "rejected" by the triggered-pulse circuit.

T I M E - A M P L I T U D E S O N O G R A P H Y 1105
R E S U L T S
A . P R E L I M I N A R Y C L I N I C A L T R I A L S
Our preliminary clinical experience was obtained with a Sperry Reflectoscope modi-fied by increasing the sensitivity and reduc-ing the time constant of the trigger circuit. Design principles of the transducers and de-tails of the circuitry will be published in a separate report. Patients with optically de-monstrable intraocular lesions were studied so that ophthalmoscopic and sonic findings could be compared.
Gross anatomic abnormalities, such as bullous detachments and intraocular foreign bodies, could be detected easily by echoes from normally echo-free areas. However, even when the sound beam was directed to-ward the lesion with the aid of an ophthal-moscope, large retinal detachments could not always be localized or oriented to the proper quadrant. Known foreign bodies and flat detachments often could not be observed, or were found after prolonged manipulation of the scanning axis. In addition, scans of normal eyes frequently revealed abnormal peaks and isolated echoes from the area of the posterior pole, indicating tumor or flat detachment where none existed.
Compound echoes with no anatomic cor-relation were observed consistently at the lens periphery and occasionally posterior to the cornea. Echoes from key landmarks, such as the lens and posterior sclera, ap-peared and disappeared with such rapidity when the transducer was moved that abnor-mal echoes could not be oriented easily.
B . S T U D I E S W I T H E N U C L E A T E D A N I M A L E Y E S
In an attempt to gain more experience with the interpretation of time-amplitude recordings, we conducted experiments on enucleated animal eyes under conditions where the scanning axis could be controlled precisely. The scanning transducer was held above the eye in a plane perpendicular to the optical axis by a compound cathetom-
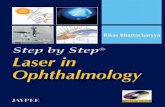
Fig . 2 (Purnel l and Soko l lu ) . Cathethometer used for fine movements of transducer. T h e eye is firmly held in its cradle by vacuum.
eter with vernier micrometers (fig. 2) . In this way we could move and measure the position of the transducer in either the horizontal or the vertical direction while noting changes in the time-amplitude dis-play.
Deviations of 0.1 mm. along the hori-zontal plane caused marked alterations in the time-amplitude display. Variations in the number of echoes and in their range and amplitude indicated that echoes were return-ing randomly from various tissue planes of the cornea, lens, and posterior coats.
In Figure 3 the reflecting surfaces of the anterior segment of the cat eye are plotted as the transducer was moved horizontally in a plane perpendicular to the optical axis. Each circle in this diagram represents one signal on the oscilloscope, regardless of amplitude, plotted at its appropriate depth. The cornea is represented by seven different

E D W A R D W . P U R N E L L A N D A D N A N S O K O L L U 1106
«MIHHI
Fig . 3 (Purnei l and Soko l lu ) . Anterior segment of cat eye ; each circle represents a triggered-pulse deflection as transducer w a s moved in horizontal direction. Zero depth represents the uppermost re-flecting surface of the cornea on the optical axis .
reflecting surfaces. Echoes were reflected by 14 different reflecting surfaces in the lens.
Movements of the transducer along the optical axis caused minor changes in ampli-tude, but did not affect the number of echoes recorded or the distances between them. Deviation of the transducer as little as three degrees from the vertical axis caused almost complete loss of the sonogram.
This method of scanning affords maxi-mum accuracy in transducer-tissue orienta-tion when one depends upon external land-
marks. However, only a small segment of the eye was displayed sonically. In Figure 3 large areas of the cornea and lens are not represented. The transducer had to be ro-tated constantly to view these curved struc-tures.
False echoes (echoes without anatomic correlation) were frequently observed in the enucleated eyes. The nature of these echoes became more apparent when they were displayed on the high frequency oscillo-scope. W e identified the following types of false echoes:
1. Multiple echoes from a single surface or "ghost images." Ghost images of the cornea occur when echoes from the cornea rebound off the crystal surface and are re-flected a second time. They may be recog-nized as false echoes when the transducer-to-eye distance is altered, and they may be eliminated by keeping this distance greater than the length of the desired scanning field.
2. Trailer echoes due to internal reflection at target. False echoes occur from internal reflections between two reflecting surfaces. These echoes appear in the display behind the first order echoes at a distance equal to that between the two surfaces, and appear as trailers to the first order echo.
An example is shown in Figure 1, in the high frequency display of the cornea. A small false echo is located posterior to the two large echoes from the anterior and pos-terior corneal surfaces.
Figure 4 shows internal reflections from a thin glass slide used as a model of the cor-nea. The triggered-pulse display shows two dissimilar compound pips, the second one being a ghost image of the first. Small changes in amplitude of the internally re-flected echoes give the ghost image a differ-ent configuration on the triggered-pulse dis-play, so that it might be interpreted as an echo from some deeper structure. However, similar high frequency displays from the two images suggest that the second echo is a ghost.

T I M E - A M P L I T U D E S O N O G R A P H Y 1107
Fig . 4 ( P u m e l l and S o k o l l u ) . Comparison of rectified pulse ( a ) and high frequency displays ( b ) and ( c ) demonstrating internal reflections f rom a glass slide model. Small changes in amplitude g ive second order echo pattern a n e w configuration in triggered-pulse display. Patterns of the first ( b ) and second ( c ) order echoes are similar in con-figuration on high frequency display, suggest ing second order echo is a "false echo."
3. Trailer echoes due to internal reflec-tions and oscillations at the transducer. A similar false echo may be produced by in-ternal reflections and oscillations at the transducer. In Figure 5 the first corneal echo rebounds from the back surface of the trans-ducer and appears on the oscilloscope be-hind the first order pulse at a distance de-pendent on the crystal thickness.
4. False echoes due to irregularities in signal pulse. Ideally, the signal pulse should be of shortest possible duration. However, to obtain a display from deep eye structures or inclined surface planes with commercial triggered-pulse apparatus, the pulse ampli-tude and duration must be increased. The high energy required causes distortion in the receiver system, and when the transducer
Fig . S (Purnel l and Soko l lu ) . H i g h frequency display showing "trailer" echo due to internal reflection and oscil lations at crystal.

1108 E D W A R D W . P U R N E L L A N D A D N A N S O K O L L U
Fig . 6 (Purnei l and Soko l lu ) . H i g h frequency displays revealing distortion of eye echo pattern as signal pulse artifacts are superimposed, ( a ) P a t -tern from anterior segment showing two corneal echoes and one lens echo, ( b ) A s transducer is moved closer to eye, false echoes appear behind corneal echoes, ( c ) Transducer closer to eye. Lens echo appears double, ( d ) Transducer almost touching eye. Corneal echoes are distorted and false echoes are present anterior to altered lens echo, ( e ) A l l corneal echoes are "shadowed" by signal pulse when transducer touches cornea. T h e lens echo is distorted and fol lowed by three arti-facts. Display is composed entirely of false echoes.
is close to the eye these distortions appear as echoes from within the eye. Figure 6 shows distortions in the echograms of the anterior segment as the transducer is moved closer to the eye. At point of contact with the eye, three false echoes are seen in the vitreous.
D I S C U S S I O N
Our unfavorable results in clinical trials seem to be based on three related inade-quacies of the method: (1 ) Inability to in-terpret the data because of uncertain tissue-
transducer orientation. ( 2 ) Inability to ob-tain echoes from known lesions. ( 3 ) Inabil-ity to recognize and reject "echoes" with no anatomic correlation.
Echoes from the intraocular tissues will not be displayed if the plane of the crystal is more than a few degrees off the per-pendicular to the reflecting surfaces. The scanning axis must be reoriented constantly, making a correlation between echoes and the reflecting surfaces difficult or impossible. This difficulty in relating the displayed echo to the proper intraocular structure is an in-adequacy of the time-amplitude method whether the echoes are displayed as trig-gered-pulse or high frequency representa-tions on the oscilloscope.
False echoes were more readily identified on the high frequency display. With the in-dustrial triggered-pulse equipment we found that these echoes were included or excluded by the operator according to his knowledge of structures in the scanning axis. With the transducer close to or touching the eye, al-most any desired display could be formu-lated from false echo artifacts. For this reason we feel that magnification of the triggered-pulse pattern, as was done by Oksala and Lehtinen,5 is probably mislead-ing. A variety of triggered-pulse patterns can be produced by a single reflecting sur-face.
We agree with Baum and Greenwood's

T I M E - A M P L I T U D E S O N O G R A P H Y 1109
analysis of the inadequacy of the time-ampli-tude method when used alone in clinical diagnosis.4 Furthermore, we agree with these authors that the availability and low cost of industrial ultrasonic flaw detectors may mis-lead many into trying the method, with un-rewarding and disappointing results.
It would appear that the clinical value of the time-amplitude display system is limited to supplementing data obtained by means of
the two-dimensional intensity-modulated sys-
tem. S U M M A R Y
Clinical trials of ultrasound visualization with a simple time-amplitude display system were disappointing. We believe the system, used alone, has little if any clinical value because of problems of orientation and false echoes.
2065 Adelbert Road (6).
R E F E R E N C E S
1. Baum, G , and Greenwood, I . : T h e application of ultrasonic locating techniques to ophthalmology. Α Μ Α Arch. O p h t h , 60:263-279, 1958.
2. : Ultrasound in ophthalmology. A m . J. O p h t h , 49:249-261 , 1960. 3. : Ul trasonography: A n aid in orbital tumor diagnosis. Α Μ Α Arch. O p h t h , 65:180-194, 1960. 4. : A critique of time-amplitude ultrasonography. Α Μ Α Arch . O p h t h , 65:353-365, 1961. 5. Oksala, A , and Lehtinan, Α . : Acoust ic biomicroscopy of intraocular tumors. A m . J. O p h t h , 5 1 :
1203-1211, 1961.
T H E G U N N P U P I L SIGN*
R O B E R T C. D R E W S , M . D .
Saint Louis, Missouri
In 1904, Mr. R . Marcus Gunn said that ". . . In the early stages, so long as the diag-nosis rested merely on subjective symptoms, retro-ocular neuritis was liable to be con-fused with functional amblyopia, but a care-ful examination of the character of the re-action of the pupil to light should always serve to distinguish between them. The re-action was invariably impaired when there was decided amblyopia from neuritis, while it remained normal in cases of functional origin."1
The finding of a Gunn pupil sign in an eye with obvious disease is redundant in-formation and the test has found little appeal for clinicians. It is the purpose of this paper to point out that the Gunn pupil sign and its
* From the Department of Ophthalmology and the Oscar Johnson Institute, Wash ing ton U n i v e r -sity School of Medicine. T h i s work w a s per-formed while the author w a s stationed at the U . S. Nava l Hospital, Great Lakes , Illinois. Opinions or assertions are the private ones of the writer and are not to be construed as official or reflecting the v i e w s of the N a v y Department or the N a v a l Serv -ice at large.
modifications (the pseudoanisocoria of Kes-tenbaum2 and the swinging flashlight test of Levatin3) make excellent objective screening tests for visual dysfunction anterior to the lateral geniculate bodies. In military service, especially in a hospital associated with a large recruit training center, many patients are seen where malingering enters the dif-ferential diagnosis. I have found that the presence or absence of the Gunn pupil sign is a rapid and easy objective method for gaining considerable insight into this sort of problem.
The cases presented in this paper were seen on the eye service of the U. S. Naval Hospital, Great Lakes, Illinois, during an 18-month period. They serve to illustrate the usefulness of the test. They do not represent all the patients with pertinent findings (for instance, a large number of patients seen with amblyopia ex anopsia and a negative Gunn pupil sign are not listed) but special care was taken to record all cases which seemed to be exceptional (table 1) .











![A Role for PPAR/ in Ocular Angiogenesisdownloads.hindawi.com/journals/ppar/2008/825970.pdf · nal dehydrogenases [14]. ATRA has its own family of high-affinity nuclear receptors,](https://static.fdocument.org/doc/165x107/606b30d521266277443bb5cb/a-role-for-ppar-in-ocular-a-nal-dehydrogenases-14-atra-has-its-own-family-of.jpg)