AMYLINAMIDE, BONE CONSERVATION, AND PANCREATIC β CELLS
2
1026 Premise AMYLINAMIDE, BONE CONSERVATION, AND PANCREATIC &bgr; CELLS IAIN MACINTYRE Department of Chemical Pathology, Royal Postgraduate Medical School, Du Cane Road, London W12 ONN Summary Amylinamide is a potent osteoclast- inhibiting peptide that is co-secreted with insulin from the &bgr; cell. It induces profound hypocalcaemia in rats and rabbits and abolishes bone resorption by isolated osteoclasts in vitro. The non-amidated human peptide forms an insoluble fibrillar amyloid deposit that may interfere with &bgr;-cell function and precipitate type II diabetes. INTRODUCTION AMYLIN is a 37 aminoacid single-chain polypeptide first isolated as islet amyloid polypeptide from the islet amyloid of an insulinoma and of a diabetic catl and also as diabetes-associated peptide from the amyloid deposit of human type II diabetes.2 The peptide may be involved in the aetiology of type II diabetes.3 The nucleotide sequence of the corresponding cDNA indicates that amylin has all the characteristics of a secreted hormonal peptide and is likely to undergo amidation.4 Amylinamide has about 50% homo- logy with calcitonin gene-related peptide and a more remote resemblance to calcitonin. We synthesised amylinamide and examined its acute effects on plasma glucose after glucose infusion in rats and rabbits. Little or no effect was observed. A similar lack of effect was seen in man (S. R. Bloom). However, the amide had dramatic effects on calcium homoeostasis, causing severe hypocalcaemia in rats and rabbits.5 Furthermore amylinamide 0-25 nmol/1 completely abolished the bone- resorbing activity of isolated rat osteoclasts. In a comparison of the international reference preparation of human calcitonin with a second synthetic preparation of amylinamide (Bachem) (fig 1) (M. Zaidi and P. J. R. Bevis), the results supported our original findings. Amylinamide produced maximum hypocalcaemia in vivo and complete osteoclast inhibition in vitro. The concentration required was thirty-times that for calcitonin. However, amylinamide may be more abundant than calcitonin in normal plasma (M. W. Makgoba and S. J. Wimalwansa). These findings mean that amylinamide may be responsible for at least some of the plasma osteoclast-inhibiting activity formerly attributed solely to calcitonin. Amylinamide occurs in normal pancreas in many species, including man, and is localised with insulin within the same secretory granule in the 0 cell;6,7 presumably the two peptides are co-secreted. HYPOTHESIS These fmdings do not exclude an effect of amylinamide on normal carbohydrate metabolism in vivo, but give no support to a sole causal role in diabetes on the basis of the in-vitro metabolic effects.s On the other hand impairment of P-cell function by the formation of amyloid fibrils could influence the development of type II diabetes. The evidence, taken together, makes a case for amylinamide as a Dose concentration Fig I-Effect of human amylinamide (0) and international reference preparation of human calcitonin (.) on plasma calcium in rat (a) and bone resorption by isolated osteoclasts in vitro (b). Dose was pmol per rat; concentration in vitro was pmol/l. Mean (SE). new circulating bone-conserving peptide whose non- amidated form may precipitate as amyloid and impair P-cell function. Whether this amyloid formation represents abnormal processing or secretion of the hormone remains to be investigated. A simplified hypothesis of the role of amylinamide in normal calcium homoeostasis is shown in fig 2. Ingestion of food is followed by secretion of 0-cell-stimulating peptides such as glucose- dependent insulinotropic peptide (GIP). The consequent secretion of both insulin and amylinamide leads to increases not only in glycogen synthesis but also in bone formation. The second effect is the likely consequence of the combination of stimulation by insulin of bone collagen synthesis9 and inhibition of resorption by amylinamide. This maximises use of dietary calcium by diverting this element to the skeleton. Although it seems likely that gastrointestinal peptides will be an important stimulus for the co-secretion of insulin and amylinamide, other known insulin Fig 2-Hypothesis.
Transcript of AMYLINAMIDE, BONE CONSERVATION, AND PANCREATIC β CELLS

1026
Premise
AMYLINAMIDE, BONE CONSERVATION, ANDPANCREATIC &bgr; CELLS
IAIN MACINTYRE
Department of Chemical Pathology, Royal Postgraduate MedicalSchool, Du Cane Road, London W12 ONN
Summary Amylinamide is a potent osteoclast-
inhibiting peptide that is co-secreted withinsulin from the &bgr; cell. It induces profound hypocalcaemiain rats and rabbits and abolishes bone resorption by isolatedosteoclasts in vitro. The non-amidated human peptideforms an insoluble fibrillar amyloid deposit that mayinterfere with &bgr;-cell function and precipitate type IIdiabetes.
INTRODUCTION
AMYLIN is a 37 aminoacid single-chain polypeptide firstisolated as islet amyloid polypeptide from the islet amyloidof an insulinoma and of a diabetic catl and also as
diabetes-associated peptide from the amyloid deposit ofhuman type II diabetes.2 The peptide may be involved inthe aetiology of type II diabetes.3 The nucleotide sequenceof the corresponding cDNA indicates that amylin has all thecharacteristics of a secreted hormonal peptide and is likely toundergo amidation.4 Amylinamide has about 50% homo-logy with calcitonin gene-related peptide and a more remoteresemblance to calcitonin.We synthesised amylinamide and examined its acute
effects on plasma glucose after glucose infusion in rats andrabbits. Little or no effect was observed. A similar lack ofeffect was seen in man (S. R. Bloom). However, the amidehad dramatic effects on calcium homoeostasis, causingsevere hypocalcaemia in rats and rabbits.5 Furthermoreamylinamide 0-25 nmol/1 completely abolished the bone-resorbing activity of isolated rat osteoclasts. In a comparisonof the international reference preparation of humancalcitonin with a second synthetic preparation of
amylinamide (Bachem) (fig 1) (M. Zaidi and P. J. R. Bevis),the results supported our original findings. Amylinamideproduced maximum hypocalcaemia in vivo and completeosteoclast inhibition in vitro. The concentration requiredwas thirty-times that for calcitonin. However, amylinamidemay be more abundant than calcitonin in normal plasma(M. W. Makgoba and S. J. Wimalwansa). These findingsmean that amylinamide may be responsible for at least someof the plasma osteoclast-inhibiting activity formerlyattributed solely to calcitonin. Amylinamide occurs innormal pancreas in many species, including man, and islocalised with insulin within the same secretory granule inthe 0 cell;6,7 presumably the two peptides are co-secreted.
HYPOTHESIS
These fmdings do not exclude an effect of amylinamideon normal carbohydrate metabolism in vivo, but give nosupport to a sole causal role in diabetes on the basis of thein-vitro metabolic effects.s On the other hand impairment ofP-cell function by the formation of amyloid fibrils couldinfluence the development of type II diabetes. The
evidence, taken together, makes a case for amylinamide as a
Dose concentration
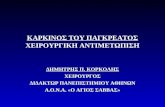
Fig I-Effect of human amylinamide (0) and internationalreference preparation of human calcitonin (.) on plasmacalcium in rat (a) and bone resorption by isolated osteoclasts invitro (b).
Dose was pmol per rat; concentration in vitro was pmol/l. Mean (SE).
new circulating bone-conserving peptide whose non-
amidated form may precipitate as amyloid and impair P-cellfunction. Whether this amyloid formation representsabnormal processing or secretion of the hormone remains tobe investigated.A simplified hypothesis of the role of amylinamide in normal
calcium homoeostasis is shown in fig 2. Ingestion of food is followedby secretion of 0-cell-stimulating peptides such as glucose-dependent insulinotropic peptide (GIP). The consequent secretionof both insulin and amylinamide leads to increases not only inglycogen synthesis but also in bone formation. The second effect isthe likely consequence of the combination of stimulation by insulinof bone collagen synthesis9 and inhibition of resorption byamylinamide. This maximises use of dietary calcium by divertingthis element to the skeleton. Although it seems likely that
gastrointestinal peptides will be an important stimulus for theco-secretion of insulin and amylinamide, other known insulin
Fig 2-Hypothesis.

1027
secretagogues such as glucose will clearly be involved. There is afurther important physiological implication, which is that secretionof amylinamide is likely to be a physiological response to calcitriol.There are specific high-affinity receptors for this potent calcium-regulating steroid in the P cell10 and calcitriol stimulates insulinsecretion." This stimulation of secretion should also extend to
amylinamide, which will have a significant consequence. The majoreffect of calcitriol is increased calcium absorption from the gut, butthis steroid also has a less desirable effect in enhancing boneresorption. Enhanced bone resorption will be minimised or
abolished by amylinamide, which will therefore act co-operativelywith calcitriol to direct to the skeleton the increased calcium
absorption produced by the active D metabolite. Interactions withparathyroid hormone and a co-operative action with calcitoninduring growth, pregnancy, and lactation are also possible.The most important consequence of our hypothesis is to provide
a possible explanation for the development of type I I diabetes by theimpairment of p-cell function by precipitated amylin. The fact thattype II diabetes does not occur12.13 where the aminoacid sequence of
amylinamide does not favour deposition strongly supports thisview. However, it is difficult to predict whether improved treatmentof type II diabetes will follow. Nevertheless measures might befound of preventing or even reversing the formation of isletamyloid.How might amylinamide be involved in disorders of
calcium homoeostasis? Amylinamide does not seem likely tobe involved in postmenopausal or senile osteosporosis but arole in the aetiology of the osteoporosis reported in type Idiabetes14 appears more plausible. Thus, a reduced
population of P cells produces a deficiency of amylinamideand insulin, with a consequent tilt in the balance of skeletalhomoeostasis towards bone loss. Could dietary calciumincrease amylinamide secretion? This possibility arisesbecause of the occurrence of amylinamide mRNA in thestomach and gastrointestinal tract, l5 which raises the
possibility of amylinamide secretion alone, without insulin,as a direct response to dietary constituents such as calcium.If so it might provide some explanation for the modesteffects of high dietary calcium in osteosporosis. If themetabolic effects of amylinamide on carbohydratemetabolism prove to be unimportant, a possible therapeuticrole for the peptide can be envisaged in those conditions inbone where calcitonin is already effective: hypercalcaemia,osteoporosis, and Paget’s disease.
These studies were supported in part by the Pinewood Foundation.
REFERENCES
1. Westermark P, Wemstedt C, Wilander E, Hayden DW, O’Brien TD, Johnson KH.Amyloid fibrils in human insulinoma and islets of Langerhans of the diabetic cat arederived from a neuropeptide-like protein also present in normal islet cells. ProcNatl Acad Sci USA 1987; 84: 3881-85
2 Cooper GJS, Willis AC, Clark A, Turner RC, Sim RB, Reid KBM. Purification andcharacterization of a peptide from amyloid-rich pancreases of type 2 diabeticpatients. Proc Natl Acad Sci USA 1987; 84: 8628-32.
3. Clark A, Cooper GJS, Lewis CE, et al. Islet amyloid formed from diabetes-associatedpeptide may be pathogenic in type-2 diabetes. Lancet 1987; ii: 231-34.
4. Sanke T, Bell GI, Sample C, Rubenstein AH, Sterner DF. An islet amyloid peptide isdenved from an 89-amino acid precursor by proteolytic processing. J Biol Chem1988; 263: 17243-46.
5 Datta HK, Zaidi M, Wimalawansa SJ, et al. In vivo and in vitro effects of amylin andamylin-amide on calcium metabolism in the rat and rabbit. Biochem Biophys ResCommun 1989; 162: 876-81.
6. Lukinius A, Wilander E, Westermark GT, Engstrom U, Westermark P. Co-localization of islet amyloid polypeptide and insulin in the B cell secretory granulesof the human pancreatic islets. Diabetologia 1989; 32: 240-44.
7 Johnson KH, O’Bnen TD, Hayden DW, et al. Immunolocalization of islet amyloidpolypeptide (IAPP) in pancreatic beta cells by means of peroxidase-antiperoxidase(PAP) and protein A-gold techniques. Am J Pathol 1988; 130: 1-8.
8. Leighton B, Cooper GJS Pancreatic amylin and calcitonin gene-related peptide causeresistance to insulin in skeletal muscle in vitro. Nature 1988; 335: 632-35.
9. Kream BE, Smith MD, Canalis E, Raisz LG. Characterization of the effect of insulinon collagen synthesis m fetal rat bone. Endocrinology 1985; 116: 296-302.
10 Norman AW, Roth J, Orci L. The vitamin D endocrine system: steroid metabolism,hormone receptors, and biological response (calcium binding). Endocr Rev 1982; 3:331-66.
11. Mayer E, Kadowaki S, Williams G, Norman AW. Mode of action of 1,25-dihydroxyvitamin D. In: Kumar R, ed. Vitamin D: basic and clinical aspects. TheHague: Martinus Nijhoff, 1984: 25-302.
12. Betsholtz C, Johnson KH, Werstermark P. ’Amylin’ hormone. Nature 1989; 338: 211.13. Leffert JD, Newgard CB, Okamoto H, Milburn JL, Luskey KL. Rat amylin. cloning
and tissue-specific expression in pancreatic islets. Proc Natl Acad Sci USA 1989;86: 3127-30.
14. Hui SL, Epstein S, Johnston CC Jr. A prospective study of bone mass in patients withtype I diabetes. J Clin Endocrinol Metab 1985; 60: 74-80.
15. Ferrier GJM, Pierson AM, Jones PM, Bloom SR, Girgis SI, Legon S. Expression ofthe rat amylin (IAPP/DAP) gene. J Mol Endocrinol 1989; 3: R1-R4.
Health Policy
ARE IN-VITRO FERTILISATION AND EMBRYOTRANSFER OF BENEFIT TO ALL?
MARSDEN G. WAGNER PATRICIA A. ST. CLAIR
Regional Office for Europe, World Health Organisation,Copenhagen, Denmark, and Department of Health Services, School
of Public Health and Community Medicine, University ofWashington, Seattle, Washington, USA
Summary The efficacy, safety, costs, and benefits ofin-vitro fertilisation and embryo transfer
(IVF/ET) have been reviewed. IVF/ET benefits only asmall proportion of infertile women, it is expensive, and hasserious health risks. Therefore policies for the managementof infertility in which most financial and manpowerresources are applied to prevention of infertility must bedeveloped. Health authorities should also requireaccreditation of IVF/ET programmes, certification of
providers, and ongoing monitoring of clinics. Full andaccurate information on IVF/ET must also be
disseminated, so that individuals seeking treatment forinfertility can make the best informed choice about their careand health authorities can decide the place of IVF/ET intheir infertility services.
INTRODUCTION
THE proliferation of in-vitro fertilisation and embryotransfer (IVF/ET) has sparked debate about its efficacy,safety, costs, and benefits.l No new technique shouldbecome standard until after rigorous evaluation. Until then,it must remain experimental, guided by the principlescovering research on human subjects .2 Evaluation involvesassessment of efficacy, safety, and costs, including indirectexpenditures on treatment of side-effects. This informationcan then be used to establish whether the new technique isappropriate in view of national policy and economicconstraints.2 IVF/ET and related assisted reproductiontechnologies have not been scrutinised in this way. Mostresearch has focused on perfecting the procedures. With fewexceptions,4e efficacy rates are reported for single clinics orfor data from clinics that participate voluntarily in pooling.There is a lack of randomised trials to ascertain the efficacyof IVF/ET compared with more established treatments forspecific classes of infertility, which seriously hampersevaluation.