Adverse reactions to β-lactam antimicrobials
19
Click here to load reader
Transcript of Adverse reactions to β-lactam antimicrobials

1. Introduction
2. Beta-lactams: structure and
function
3. Allergic adverse events
4. Hematological adverse events
5. Hepatobiliary adverse events
6. Renal adverse events
7. Neurological adverse events
8. Gastrointestinal adverse
events excluding C.
difficile-associated diarrhea
9. C. difficile-associated disease
10. Adverse reactions associated
with specific agents
11. Management of allergic
reactions of
b-lactam antibiotics
12. Expert opinion
Review
Adverse reactions to b-lactamantimicrobialsPhilippe Lagace-Wiens† & Ethan Rubinstein†University of Manitoba, Faculty of Medicine, Department of Medical Microbiology and Infectious
Diseases, Winnipeg, Manitoba, Canada
Introduction: Beta-lactam antibiotics are among the most clinically useful
antimicrobials used in medicine. Unfortunately, adverse events related to
their use remain poorly understood by many clinicians and, in particular, the
misdiagnosis of b-lactam allergy and misunderstanding of crossreactivity
among members of the b-lactam antibiotics may effectively eliminate a whole
class of antimicrobials from use and require the use of broader spectrum
agents with less well-established safety profiles.
Areas covered: This review describes the range, diagnosis and management of
adverse events associated with b-lactam antimicrobials, particularly focusing
on recognition, diagnosis and management of true allergy and risk of cross-
sensitivity between b-lactam antibiotics. A literature review was undertaken
using PubMed, focusing primarily on literature published in the past 10 years
relating to b-lactam adverse events and allergy.
Expert opinion: Beta-lactams are generally safe drugs and serious adverse
events are rare and allergy is overdiagnosed. Accurate diagnosis can usually
be achieved through careful history and in some instances skin or in vitro test-
ing is required. Even among individuals with true immediate-type allergy to
penicillin, most cephalosporins are readily tolerated and desensitization is
usually an option in cases where no alternate antimicrobials are available.
Other allergic reactions (Type II, III and IV) are rare and avoidance of the cul-
prit agent is generally recommended. Nonallergic or morbilliform rashes are
generally not allergic in nature and should not prompt drug or class avoid-
ance. Other adverse events are frequently dose-related and can be avoided
by appropriate dosing and consideration of renal function.
Keywords: adverse event, allergy, antibiotic, antimicrobial, beta-lactam, carbapenem,
cephalosporin, crossreactivity, drug-related, hypersensitivity, penicillin, rash, review, side effect
Expert Opin. Drug Saf. (2012) 11(3):381-399
1. Introduction
Beta-lactams are the most commonly prescribed antimicrobial in both the hospital andcommunity settings and remain one of the safest antimicrobials prescribed [1]. How-ever,b-lactam antibiotics do carry the risk of adverse events, including rare allergic reac-tions and even rarer adverse events affecting hematological, renal and neurologicalsystems [2]. Beta-lactam antibiotics were first used in significant quantities during theSecond World War and have been continuously used, developed and modified sincethen. Given the long history of use, surprisingly little was known about the nature ofadverse events related to their use until relatively recently, and for this reason, manyclinicians do not fully understand the nature of these adverse events. Misdiagnosis ofb-lactam-related adverse events constitutes a significant problem to the clinician, partic-ularly when these limit the use of these otherwise useful agents [3]. The key tomanagingboth serious and insignificant adverse reactions is the understanding of the various typesof reactions that exist, and particularly the true existence, diagnosis and managementof b-lactam allergy. Although there are class-specific adverse events that are well
10.1517/14740338.2012.643866 © 2012 Informa UK, Ltd. ISSN 1474-0338 381All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

documented, the recent understanding of the intimate linkbetween structural components of b-lactam agents and adverseevents, including crossreactivity, has lead to a deeper under-standing of the mechanisms by which adverse events occur forspecific agents, and in particular, the very low prevalence ofcross-sensitization between penicillins and cephalosporins [4],supporting the use of most cephalosporins even in individualswith documented allergy [5].In addition to adverse events directly related to the antibi-
otic itself, recent developments in the epidemiological studyof Clostridium difficile-associated disease (CDAD) have dem-onstrated that some of these agents may be associated with ahigher risk of CDAD than others [6]. A better understandingof these risks is of paramount importance for the moreeffective use of antimicrobials in general, including b-lactams.Lastly, if a true b-lactam allergy is documented and con-
firmed, a number of strategies to manage the allergy havebeen developed [7]. These range from the strategic use of struc-turally unrelated b-lactam antibiotics to desensitization [8].When b-lactam therapy is needed or superior, these approachesallow clinicians to use them despite allergy.
2. Beta-lactams: structure and function
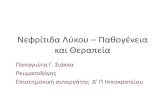
The prototype b-lactam is penicillin, a natural compoundfirst isolated in 1928 by Alexander Fleming from the moldPenicillium notatum. The structure of penicillin core and rep-resentative penicillins is illustrated in Figure 1. Modificationsof side chains of this natural compound eventually led tothe discovery of various related compounds with differentpharmacodynamic and pharmacokinetic properties, antimi-crobial spectra and side-effect profiles [7,9]. Modifications ofthe penicillin ‘core’ have focused on the variable side chain
of carbon 7 (frequently called ‘R1’ or simply ‘R’) in order toimprove activity (particularly against gram-negative isolates),oral bioavailability and pharmacodynamic properties [10].The side-chain substitutions are also of critical importanceto allergic reactivity (and crossreactivity) because they serveas minor allergic determinants [3,7-9].
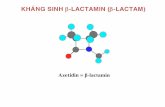
Cephalosporins were also developed from a natural productproduced by molds of the genus Cephalosporium (now Acremo-nium spp.). Although there are a number of structural similari-ties between penicillins and cephalosporins, including theb-lactam ring, a number of differences must be highlighted.Firstly, there are two variable side chains commonly targetedtomodify the structure of cephalosporins [7,11]. Carbon 7 substi-tutions (‘R1’) tend to modify the antimicrobial spectrum andbioavailability while modifications of position 3 (‘R2’) tendto provide useful pharmacological properties (e.g., longer halflife) [10]. In addition to side-chain differences, the sulfur ringof the cephalosporin nucleus is a six-membered dihydrothiazinering compared to the five-membered thiazolidine ring of peni-cillins [11]. In addition to providing relative stability to penicil-linases, this structure also goes through different degradationpathways. The b-lactam ring of penicillins spontaneously opensin physiologic conditions forming a stable penicilloyl groupacid (which is the major antigenic determinant of penicillins)that can bind to protein conjugates and create antigenic hapt-ens. Contrary to this, due to their structural difference, theb-lactam and dihydrothiazine rings of cephalosporins are rap-idly fragmented into unstable compounds that generally donot have structural similarity to the penicillin allergic determi-nants [3,11,12]. The cephalosporin nucleus and representativecephalosporins are presented Figure 2.
Monobactams are a separate class of b-lactam antibiotics ofwhich aztreonam is the only commercially available agent [7].Newer monobactams, including orally bioavailable agents arein development. Monobactams differ structurally from otherb-lactams in that they possess only a b-lactam ring withoutan accompanying ring [7]. Their structure is such that theyhave activity only against gram-negative pathogens. They arenot metabolized into structures chemically resembling penicil-loyl acids or minor determinants of penicillin allergy andtherefore no immunological crossreactivity occurs with thisagent [13].
Carbapenems were initially isolated from Streptomycessp. and are structurally related to other b-lactams. Theycontain a b-lactam ring bound to a five-membered ringand two variable chains [7]. Structurally, they differ frompenicillins by the absence of sulfur atom in the five-membered ring and by the substitution of the nitrogen inposition R1 for a carbon (hence the name carbapenem).The primary result of this chemical structure is the extraor-dinary stability of the agent against b-lactamase hydrolysis.Substitutions to the side chains of carbapenems have pro-duced agents with activity against a slightly different spec-trum of pathogens, as well as altered the pharmacodynamicproperties [14].
Article highlights.
. Beta-lactams are generally safe drugs and adverseevents are overdiagnosed.
. Patients with immediate-type hypersensitivity topenicillins can safely be given many second- orthird-generation cephalosporins.
. Patients with primary cephalosporin allergies will oftentolerate structurally unrelated cephalosporins.
. Nonspecific morbilliform rashes following beta-lactam administration are usually not allergic in natureand are not a contraindication to their use.
. Patients with severe desquamating reactions due tobeta-lactams should generally not be re-exposed to theoffending agent.
. Nonallergic adverse events are frequently dose-related orspecific to certain agents.
. Clostridium difficile-associated diarrhea is frequentlyassociated with broad-spectrum antimicrobial use andcephalosporins are often implicated.
This box summarizes key points contained in the article.
P. Lagace-Wiens & E. Rubinstein
382 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

The function of b-lactam antibiotics is similar for all classes(penicillins, monobactams, cephalosporins and carbapenems).The agents are analogs of D-alanyl-D-alanine which forms theterminal part of crosslinking peptides (commonly pentapepti-des) required to form crosslinks between the peptidoglycans inbacterial cell walls. In bacteria, during cell wall synthesis andturn-over, these peptides are bound to enzymes known aspenicillin-binding proteins (PBP) that facilitate transpeptida-tion resulting in the formation and maintenance of bacterialcell walls. Beta-lactam antibiotics bind to these PBPs as substrateanalogs and inhibit transpeptidation resulting in damage to thecell-wall integrity. Although all b-lactams function in this fash-ion, b-lactam antibiotics differ somewhat in their affinity tothe different PBPs present in bacteria, which partially explainsthe variation in antimicrobial spectrum. For example, althoughcloxacillin or cephalexin are potent inhibitors of staphylococcalPBP2 resulting in good activity against wild-type Staphylococcusaureus, they have no activity against Enterococcus spp., becausethe latter rely principally on PBP6 for transpeptidation whichis poorly inhibited by these agents. On the other hand, penicillinand amoxicillin are inhibitors of both PBP2 and PBP6, resultingin activity against both organisms (provided a b-lactamase is notpresent). Furthermore, the exact structure, polarity and sidechains of b-lactams may also affect their ability to enter the
periplasmic space of gram-negative organisms, which may resultin a limitation in the spectrum of activity.
3. Allergic adverse events
Allergic reactions are among the most common adverse eventsreported following b-lactam administration. The reportedrate of penicillin allergy ranges between 1 and 10% and theincidence of life-threatening allergy to penicillin is estimatedbetween 0.01 and 0.05% [15]. To gain an understanding ofb-lactam allergy and more importantly of immunologicalcrossreactivity, an understanding of the immunochemistry ofb-lactams is critical.
3.1 Immunochemistry of b-lactamsThe immunochemistry of penicillin, the prototype b-lactam,is well characterized. Penicillins, and closely related com-pounds, are rapidly metabolized into benzylpenicilloyl [16]. Thismetabolite, which accounts for the metabolism of > 95% ofnative penicillin, is known as the ‘major determinant’ ofpenicillin allergy because it is responsible for the majority of aller-gies [7,16]. The metabolite is stable and readily binds to proteinconjugates creating potentially immunogenic haptens [3]. Theremaining metabolites, including penilloate, penicilloate and
Penicillin nucleus Penicillin V
Amoxicillin
Piperacillin
HN
N
SCH3
CH3
R
O
O
H
COOH
O HN
N
S
OOH
O
O
O
HN
N
S
OH
O
HO
NH2
H
OHN
N
O
S
OOH
H
NH
N
NO
O
O
O
Figure 1. Structure of penicillin nucleus and representative penicillins.
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 383
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

N
71
3
S
R2
O OH
O
HHN
R1
O
N
N N
N
O
HN
N
S
N
S
N
S
H
O
O OH
S
HN
N
S
O
OO
O
H
O OH
O
HN
N
S
OH
O
O
H
NH2
S O
NH
N
S
O NH2
OHO
O
O
O H
O
OHN
N
S
O NH2
O
O
NO
HO O
S
N
HN
N
S
O
OO
O
H
O OH
H2N
NO
S
N
HN
N
S
N+O
O
H
O O-
NO
OH
O
H2N
Cephalosporin nucleus
Cephalothin Cefazolin
Cephalexin Cefoxitin
Cefuroxime Cefotaxime
Ceftazidime
Figure 2. Structure of cephalosporin nucleus and representative cephalosporins.
P. Lagace-Wiens & E. Rubinstein
384 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

native penicillin are collectively referred to asminor determinants,which account for a minority of allergic reactions [7]. In addition,semi-synthetic penicillins also produce metabolites that areunique, including parts of the C-7 side chain which may act assensitizers [7]. An important step to understanding the immuno-chemistry of penicillins and other b-lactams is that hypersensitiv-ity to any one penicillin determinant does not typically confercrossreactivity to other determinants, including unique metabo-lites or side-chain determinants of semisynthetic penicillins andother b-lactams because they are structurally unrelated [9]. Forexample, an individual may have an allergy mediated by a metab-olite of the amoxicillin R1 side chain without having an allergy topenicillin (which has no such side chain) [3]. On the reverse, anallergy to the major determinant of penicillin generally meansallergy to amoxicillin because the two agents share this particulardeterminant.
The immunochemistry of cephalosporins is less well charac-terized, but recent developments have shed considerable lighton the mechanism by which allergy to these agents develops.Like penicillin, a metabolite similar to benzylpenicilloyl is gener-ated in vivo, cephalosporoyl. However, unlike benzylpenicilloyl,this metabolite is highly unstable and undergoes rapid fragmen-tation in the dihydrothiazine (six-membered) ring [11]. This frag-mentation results in the formation of molecules that have nostructural resemblance to benzylpenicilloyl or to the minordeterminants [3,8,12]. The relevance of this fragmentation isthus that the crossreactivity between penicillin-allergic andcephalosporin-allergic patients is not usually due to sensitizationto major or minor determinants of penicillin. However, it hasbeen shown in various experimental studies supported by clinicalevidence that the resulting fragments, which may include frag-ments of the cephem nucleus, and more importantly parts ofthe side chains of the cephalosporins, act as haptens and maylead to sensitization [11]. Indeed, recent in vitro studies and clin-ical observations have shown that cephalosporin side chains (orportions thereof) constitute the major determinants of cephalo-sporin allergy [3]. Therefore, crossreactivity between cephalo-sporins and penicillins is generally mediated by similaritiesin side-chain structures rather than the structure of theirb-lactam core.
The immunochemistry of carbapenems has not been fullyelucidated. The carbapenems have significant structural similar-ity with penicillins. Their principal metabolite, a stable carba-penoyl compound, is structurally similar to benzylpenicilloyland capable of binding to amino acid residues (e.g., glycine)thereby forming haptens [17,18]. These biochemical similaritiessuggest similar immunochemistry to the penicillins and ahigher risk of crossreactivity. Immediate-type hypersensitivitieshave been demonstrated in both native carbapenems and theirprimary carbapenoyl metabolites [19].
Monobactams are unique b-lactams formed by only ab-lactam ring and a side chain. As such, both the nativemoleculeand its metabolites have no structural similarity to those of pen-icillins or carbapenems [19]. However, like cephalosporins, themetabolites of monobactams, especially side-chain determinants
can act as haptens, and sensitization to side chains has beendocumented [19]. Lack of immunological crossreactivity betweenaztreonam and monobactams with structurally different sidechains and a near-complete crossreactivity between aztreonam-directed antibodies and ceftazidime (which has an identicalside chain) suggest that side chain is the major determinant ofmonobactam allergy [19].
3.2 Types of hypersensitivity reactionsPatient claims of penicillin allergy are often unfounded andresult in elimination of a potentially useful class of drugs astreatment options [15]. It is worth noting that a significant pro-portion of patients claim that any adverse event (includingnonallergic events) or intolerance constitutes an ‘allergic reac-tion’ [3,8]. For example, adverse events such as gastrointestinalintolerance, diarrhea and headache are frequently called aller-gies although they are more likely common side effects orcaused by the disease state being treated [20]. Further complicat-ing the issue of allergic reactions is the frequent development ofrash in association with certain viral infections, particularlywhen treated with amoxicillin [12,20]. As many as 70 -- 100%of individuals with concurrent Epstein--Barr virus (EBV) infec-tion develop such a rash, and concurrent infections like acutehuman immunodeficiency virus (HIV), cytomegalovirus(CMV) and herpes simplex virus (HSV) have also been associ-ated with this phenomenon [21]. Cutaneous reactions are alsopart of the Jarisch--Herxheimer reaction seen with the treat-ment of spirochete infections, particularly Borrelia recurrensis.Such idiopathic morbilliform rashes are not allergies. Lastly,some bacterial infections may produce rashes, particularlyfollowing treatment, which may be misdiagnosed as allergy.The toxin-mediated scarlet rash following streptococcalpharyngitis is one such example.
True allergic reactions are mediated by antibodies orimmune cells. Coombs and Gell categorized allergic reactionsinto four groups on the basis of their pathophysiology and theimmune mediators involved [7,22]. Beta-lactams can be impli-cated in any of these four reaction types. Type I reactions(immediate type hypersensitivity) are of the greatest concernbecause they are rapidly progressive, potentially fatal andtend to become more severe with repeated exposures [7].They are mediated by IgE class antibodies and result in thedegranulation of mast cells, producing large amounts of vaso-active substances and histamine [22]. Although anaphylaxis isthe most severe form of type I reaction angioedema, urticaria,laryngeal edema, wheezing and hypotension are more com-mon findings. Pruritis, an urticarial rash, hive or angioedemais highly suggestive of a type I hypersensitivity [20,22]. Type IIreactions are primarily mediated by IgG and complement. Intype II reactions, cytotoxic IgG bind to circulating red cellsand platelets, and both complement and the lymphoreticularsystem contribute to the excess destruction of red cells andplatelets [7,22]. In type III reactions, IgG and/or IgM com-plexes form and precipitate in tissues. Common syndromesare drug fever, immune-complex glomerulonephritis and
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 385
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

serum sickness [23]. Type IV reactions are T cell mediated andresult in delayed hypersensitivity. Recent findings have sug-gested that separate components of the cellular immuneresponse activated by the drug antigen result in a variety ofdistinct clinical presentations of type IV delayed hypersensi-tivity reactions, including among others contact hypersensitiv-ity, hepatitis, bullous exanthems and eosinophilia [24]. A fifthcategory of adverse drug reactions includes idiopathic reac-tions that are not clearly immune mediated [20]. Examples ofsuch adverse reactions are morbilliform rashes and maculo-papular rashes, neither of which is IgE mediated. Tables 1
and 2 describe hypersensitivity reactions to b-lactams accord-ing to Coombs and Gell classification as well as by timeof onset.
3.2.1 Beta-lactams and immediate- and accelerated-
type hypersensitivity (‘type I’)The prevalence of immediate ‘Type I’ allergy to penicillins andb-lactams is not precisely known. Although the reported rate ofsuspected penicillin allergy ranges from 1 to 10% [25,26], thetrue incidence of demonstrable IgE-mediated allergy to penicil-lin (by skin test) in this population is between 10 and 20%[15,27]. The prevalence of severe (anaphylactic) type I reactionto penicillin is estimated at 0.01 -- 0.05% [15,28]. Equivalentdata for cephalosporins is not as readily available, but reportsof anaphylaxis from cephalosporins are extremely rare, reportedat between 0.0001 and 0.1% [11,29]. Reactions such as urticaria,rash, exanthem and pruritus occur in 1 -- 3% of the generalpopulation that receive cephalosporins [3,5].Type I reaction to b-lactam antimicrobials are mediated by
the presence of IgE directed against a structural component ofthe molecule [7,22]. Haptens, produced by the metabolism ofb-lactam drugs, bind to circulating serum proteins and createsensitizing antigens (see the section ‘Immunochemistry ofb-lactams’) [30]. Presentation of these antigens to a sensitizedhost results in the rapid degranulation of mast cells with a releaseof vasoactive substances and histamine [30]. The symptoms of atype I reaction are usually readily recognizable and include urti-caria, angioedema, wheezing, laryngeal edema, apprehension,hypotension or anaphylaxis [7,22,30]. Nearly all type I (IgE medi-ated) reactions occur within 72 hours of drug administration.The onset of pruritis within 72 hours of the initiation of ab-lactam drug is suggestive of a milder type I reaction [7]. Mor-billiform rashes, particularly in the absence of pruritus are nottypical of type I reactions, particularly if they occur after72 hours [3,5,8]. With the exception of rare delayed urticaria(readily diagnosed by the pruritic wheals), nearly all type Ireactions occur within 72 hours of administration [12].Immediate and accelerated type I allergic reactions are
typically the most serious allergic reactions because of therapidity in which they progress, the potentially fatal natureof the reaction and the fact that they may become moresevere with repeated exposures [12]. Individuals with a severe(anaphylactic) reaction to a b-lactam antibiotic should notbe given an identical drug or, in the case of penicillins, other
penicillins unless done so by an expert for purposes ofevaluation or desensitization. The risk of crossreactivity withcephalosporins and other b-lactams will be discussed later.
3.2.2 Beta-lactams and delayed cytotoxic
antibody-mediated reactions (type II)Type II reactions occur when circulating antibodies (IgG andIgM) directed to the surface of circulating blood cells (leucocytes,platelets of red cells) bind result in either an increased destructionof the cells by the reticuloendothelial system or direct destructionthrough complement-mediated cytopathic effects. These reac-tions are typically delayed and occur > 72 hours after expo-sure [7,22]. The most common type II reaction associated withb-lactams is hemolysis associated with IgG or IgM antibodiesdirected at cell surface-adsorbed b-lactams [22]. The antibodiesattach to the cell-adsorbed antigen and lead to increased clearing(and hemolysis by complement) of the red cells. Such cytopeniascan occur with all cell types. Although data on prevalence ofthese reactions is not available, it is known that drug-inducedhemolytic anemia occurs at a rate of approximately one per amillion population and that 70 -- 80% of cases are associatedwith antimicrobials, particularly penicillins and cephalo-sporins [31-36]. Drug-induced neutropenia occurs relatively rarely,with an incidence of 2 -- 15 cases per million, and although a sig-nificant proportion of these are associated with b-lactams, it is notknown howmany are associated with type II reactions as opposedto marrow toxicity [37]. Immune-mediated thrombocytopenia isuncommonly associated with b-lactam drugs [38-40].
Type II reactions are drug-specific, and crossreactivitybetween cephalosporins and penicillins does not appear tooccur [3,12]. The offending drug should be avoided and thereare no skin-test equivalents to determine the likelihood ofsuch a reaction [7,22].
3.2.3 Antibody complex-mediated reactions (type III)These delayed reactions occur when the b-lactam induces the for-mation of antibody--antigen complexes that precipitate in tissuesand activate complement resulting in a variety of clinical syn-dromes including serum sickness and small-vessel vasculitis,potentially affecting any end organ [23]. Typical manifestationsinclude fever, malaise, nausea, vomiting, diarrhea, abdominalpain, arthralgias, myalgias, lymphadenopathy, glomerulonephri-tis and rash [23]. Although antimicrobials, particularly penicillin,are common culprits, the incidence of serum sickness associatedwith penicillin is very low, 7 -- 40/100,000 prescriptions [23]. Itis important to distinguish the difference between true type IIIreaction and serum sickness-like reactions, which do not involveantibody complexes but rather a poorly understood idiopathicphenomenon associated with some antimicrobials, particularlycefaclor [41].
3.2.4 Delayed-type T-cell-mediated hypersensitivity
(type IV)Delayed-type (type IV) hypersensitivity to b-lactam antibioticsoccurs, but the incidence is not known. There are several
P. Lagace-Wiens & E. Rubinstein
386 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

reports of contact dermatitis and pustulosis associated withb-lactam use [42-48] and additional reports of systemic symptomsin association with cell-mediated hypersensitivities [7,22,49-51].Other phenomena such as Stevens--Johnson syndrome (SJS)and toxic epidermal necrolysis are presumed to be immunemediated, but the precise role of T cells is not clear. Eosinophilia,bullous exanthems and immune hepatitis may also be the resultof T-cell activation and cytokine expression in response to ab-lactam allergen [24]. It may be difficult to distinguish latetype IV systemic reactions from other hypersensitivities, butskin patch testing has proven useful for the diagnosis of derma-titis and other delayed hypersensitivity reactions caused byb-lactam drugs [52].
3.2.5 Idiopathic hypersensitivity reactionsThe group of delayed hypersensitivity reactions that do not fallunder the Coombs and Gell classification schemes are collec-tively known as idiopathic reactions [3]. These include non-pruritic morbilliform and maculopapular rashes. These occurin 3 -- 7% of children taking amoxicillin [12]. These do notappear to be IgE mediated but the mechanism of occurrence isnot understood. The occurrence of these rashes does not consti-tute a contraindication to represcription [12]. Other idiopathicconditions such as SJS, toxic epidermal necrolysis, drug reaction(or rash) with eosinophilia and systemic symptoms (DRESS)and erythema multiforme have been reported with aminopeni-cillin, cephalosporin and other b-lactams but their incidence isvery low, and it is difficult to determine the attributablerisk [52-57]. The culprit drugs should generally be avoided in thesecases. However, unlike in adults where SJS is usually a delayedhypersensitivity to a drug, it is typically related to infectiouscauses in children. As such, some experts recommend that chil-dren with SJS in association with b-lactam administration, neg-ative responses in late-reading intradermal and patch tests with ahighly suspected or proven infectious cause of the SJS may beoffered b-lactams [58]. The DRESS syndrome is a potentiallylife-threatening syndrome including a severe skin eruption,fever, hematologic abnormalities (eosinophilia or atypical lym-phocytes), and internal organ involvement that has been associ-ated with b-lactam antibiotics. It appears to be very rare,although the true incidence in relation to b-lactams is unknown.Although reactivation of human herpes viruses has been impli-cated in the disease, the exact pathophysiology is not establishedand rechallenge, either for diagnostic or therapeutic purposes isnot recommended [59].
3.3 Crossreactivity between b-lactamsCrossreactivity between the b-lactams does occur; however,with the exception of crossreactivity within members ofthe penicillin group, its prevalence is exaggerated by manyclinicians [3].
Table 1. Gell and Coombs Classification of hypersensitivity reactions.
Classification Time of onset Mediator Clinical signs Utility of
skin test
Comments
Allergic immediate(Type I)
< 1 h IgE Anaphylaxis, hypotension, laryngealedema, wheezing, angioedema,urticaria
Yes Parenteral more likelythan oral. Fatal in1/50,000 -- 100,000.Rarely 1 -- 72 h
Late (Type II) > 72 h Clearance/hemolysis of RBCs andplatelets
No IgE not involved
Type III > 72 h IgG, IgM,immunecomplexes
Serum sickness No Tissue lodging of immunecomplexes, drug fever.IgE not involved
Type IV > 72 h T cells Contact dermatitis No IgE not involvedIdiopathic Usually > 72 h ? Maculopapular or morbilliform
rashesNo Occurs in 1 -- 4% of
b-lactam recipients.
Adapted from [12].
Table 2. Early, accelerated and late hypersensitivity
reactions to b-lactams.
Timing Examples of reactions
Immediate toaccelerated,IgE mediated(< 1 h to 72 h)
UrticariaLaryngeal edemaBronchospasmHypotensionLocal swellingAngioedema
Delayed (> 72 h) Morbilliform rashMaculopapular rashSerum sickenessUrticaria (rarely late)Stevens--JohnsonsyndromeInterstitial nephritisPulmonary infiltrationVasculitisHemolytic anemiaNeutropeniaThrombocytopenia
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 387
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

3.3.1 Penicillins and cephalosporinsThe issue of crossreactivity between b-lactams, particularlybetween penicillins and cephalosporins has been one of contro-versy which has been resolved only recently. The widely cited‘10%’ crossreactivity between the two agents appears to origi-nate from publications by Dash [60] and Petz [61,62] whoreported allergic reactions to cephalosporins in 7.7 -- 8.1% ofpenicillin allergic patients. A number of flaws existed with theseearly studies, namely that the definitions of penicillin allergywere loose (patient report), cephalosporin preparations werecrude and contained penicillin, the importance of cephalospo-rin structure was not known at the time and the authors didnot consider that penicillin-allergic individuals are, at baseline, three times more likely to experience an adverse allergicreaction to any unrelated drug [3,63]. Further confusion is addedby reports of in vitro crossreactivity between antibodies directedto the agents that do not predict hypersensitivity [3,62].A more recent meta-analysis of the true crossreactivity risk in
properly characterized and defined penicillin allergies has paintedquite a different picture [4]. In this study, the authors identified sixtrials (47,284 patients) evaluating the crossreactivity betweenpenicillins and cephalosporins in patients with a reported historyof penicillin or amoxicillin allergy and four trials (1,831 patients)who had undergone penicillin skin testing. The results clearlyindicated that in the presence of a history of allergy to penicillinor amoxicillin, there was an increased risk of allergy only to ceph-alothin, cephaloridine and cephalexin (all first-generation agents)while no increased risk of allergy existed for cefprozil, cefpodox-ime, ceftazidime and cefuroxime [4]. Further studies into themetabolism of cephalosporins and monoclonal antibodiesdirected to cephalosporins demonstrated that the side chains ofthe cephalosporin constitute the major determinant of allergicreactions (see ‘Immunochemistryofb-lactams’ section) [3,29,64-69].As such, crossreactivity between penicillin and/or amoxicillin andcephalosporins appears to be driven by side-chain similaritiesbetween the agents. Penicillin, for example, shares a significantsimilarity in its C-7 side chain to cefoxitin, cephalothin and ceph-alodrine and a significant crossreactivity is expected betweenthese agents. Likewise, cephalexin and amoxicillin share similarside chains and crossreactivity occurs [4]. The meta-analysis byPichichero [4] supports this observation and also partially explainsthe initial observations by Dash and Petz [60,61]. Similarly, ceph-alosporins with side chains dissimilar to penicillin or amoxicillinare not associated with an increased risk of allergic reactionsin penicillin or amoxicillin allergic individuals [4]. Table 3 indi-cates the relationship between side-chain chemical structures ofcephalosporins and penicillins.
3.3.2 Crossreactivity between cephalosporinsSuperficially, the risk of allergic crossreactivity between cepha-losporins should be high given their similar structure. However,the reported crossreactivity between cephalosporins is actuallyquite low [70]. The explanation for this is the significant hetero-geneity between side chains of different cephalosporins, whichare the major determinants of allergy. As such, the risk of
crossreactivity between cephalosporins with dissimilar sidechains (both side chains must be dissimilar) is extremelylow [3,65,70]. Therefore, individuals with a non-anaphylacticallergy to cephalosporins could be offered another cephalospo-rin with dissimilar side chains [70]. Table 3 indicates the relation-ship between side-chain chemical structures of cephalosporinsand penicillins.
3.3.3 Crossreactivity between other b-lactam
antibioticsAllergy to penicillin appears to confer some increased risk ofcarbapenem allergy. The exact risk remains controversial andstudies demonstrated a risk of allergic reactions ranging from0.9% to 47.4% [19]. Many of these studies had loose definitionsof allergy and used variable methods for determination forallergy (skin tests, test doses, native carbapenem vs. metabolitesetc.) and the wide range of results appears to be partly explainedby the way allergies are defined and the manner in which theyare verified. However, the studies that have used both standardpenicillin skin tests and in-house carbapenem skin tests todetermine allergy, followed by a trial dose of carbapenemsuggest a crossreactivity around 1%, with all carbapenemskin-test negative patients tolerating the dose [71-73]. As such,a recommendation could be made to skin test penicillin allergicpatients with the carbapenem and using the carbapenem inpatients with no reaction to the skin test [19].
Aztreonam and other monobactams have a unique struc-ture that appears to be weakly immunogenic and does notcrossreact with penicillin and cephalosporins and can safelybe given to patients with documented allergy to theseagents [19]. Isolated hypersensitivity to aztreonam does occurand is associated with antibodies directed to the aztreonamside chain [19]. Because ceftazidime and aztreonam have iden-tical side chains, there is a documented crossreactivity betweenthese two agents and ceftazidime allergy should preclude theuse of aztreonam and vice versa [19].
3.4 Diagnosis of type I hypersensitivity to b-lactamsType I hypersensitivity reactions have a defined and predictablecourse and can usually be readily recognized by history. Immedi-ate hypersensitivity reactions usually occur within one hour ofexposure, butmay occur up to 72 hours after. There are rare casesof delayed urticarial reactions after 72 hours. The symptomsinclude urticaria, pruritus, anaphylaxis, angioedema, erythema(diffuse or localized), bronchospasm, laryngeal edema, hyperper-istalsis, hypotension or arrhythmias [20]. Skin tests, whichprovide an objective means of assessing IgE-mediated allergicreactions are available and standardized only for penicillin, wheremajor and minor determinants are used to assess risk ofIgE-mediated reactions (see the ‘Immunochemistry of b-lactams’section). Although skin testing is only positive in 43 --85%of individuals with a history of penicillin allergy and ispositive in 15 -- 55% of individuals without allergy, a negativetest has a very strong predictive value (~ 99%) for toleratingpenicillin [20].
P. Lagace-Wiens & E. Rubinstein
388 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

Penicillin skin tests do not reliably predict allergy to ceph-alosporins unless there is a side-chain similarity between pen-icillin and the cephalosporin in question (Table 3) [3]. Tocompound the issue of cephalosporin skin testing, there areno standardized antigens and many of the antigenic determi-nants caused by their degradation are not well known [11,70].However, some allergists advocate skin tests using the wholeantibiotic, and such tests have been used for the diagnosis ofimmediate reactions to these antibiotics, but their sensitivityand specificity are not defined [11]. Additional discussion onthe precise diagnosis of allergic reactions to b-lactams, includ-ing type I, II, III and IV reactions should be achieved using acareful clinical history, judicious use of in vivo (skin-prick andpatch and drug challenge) and in vitro (specific IgE determi-nation, radioallergosorbent test (RAST), histamine release,cellular antigen stimulation (CAST), and basophil activation)tests, the discussion of which is beyond the scope of this man-uscript. Interested readers are directed to a number of recentreviews on the topic [58,74-78].
4. Hematological adverse events
In general, hematologic adverse effects are uncommon unlessthe b-lactam agents are administered in large doses and forprolonged periods.
4.1 AgranulocytosisAgranulocytosis is a rare complication of drugs in general, and b-lactams are extremely rare causes of this disorder. Total incidencevaries between 2.4 and 15.4 per million population/year in theUS to 6/million/year in France [79,80]. This incidence increaseswith age, as only 10%of cases are reported in children and youngadults, and more than half of these episodes occur in peopleover 60 years of age. This observation is probably reflecting thehigher medication use associated with old age. In one cohorttwo out of three episodes were in individuals over the age of65 [80]. Beta-lactam antibiotics are considered to be responsiblefor ~ 25% of all cases of drug-induced agranulocytosis andsevere neutropenia.
For b-lactam antibiotics-associated agranulocytosis, themedian exposure time before the onset of agranulocytosis was22 days for oxacillin and nafcillin, 25 days for penicillin G and19 days for cefapirin [81]. The median time for normalization ofthe neutrophil count following cessation of b-lactam therapywas short for penicillin G and oxacillin (4 days) and longer fornafcillin and cefapirin (8 days) [81]. In a comprehensive studyevaluating the association of piperacillin with neutropenia andagranulocytosis, it was determined that among 13,816 patientsenrolled in non-neutropenic fever studies, the occurrenceof piperacillin-induced neutropenia was very low: only fivepatients (0.04%) developed neutropenia; none died. The USFDA Adverse Event Reporting System (AERS) database wasalso screened and the authors identified 366 unique cases ofpiperacillin- or piperacillin-tazobactam-induced hematologicalabnormalities, including neutropenia (n = 183, 50%),T
able
3.Groupsofcephalosp
orinsandb-lactamswithsimilarC3andC7sidech
ains.
Sim
ilarC-7
sidech
ain.Cross
reactions
betw
eenagents
within
onegroupis
possible
Sim
ilarC-3
sidech
ain.Cross
reactionsbetw
eenagents
within
onegroupis
possible
Group1
Group2
Group3
Group1
Group2
Group3
Group4
Group5
Group6
Group7
Penicillin
Amoxicillin
Cefepim
eCefadroxil
Cefm
etazole
Cefotaxime
Ceftibuten
Cefuroxime
Cefdinir
Ceftazidim
eCephalothin
Ampicillin
Ceftizoxime
Cephalexin
Cefoperazone
Cephalothin
Ceftizoxime
Cefoxitin
Cefixime
Cefsulodin
Cephalodrine
Cefaclor
Cefpirome
Cephadrine
Cefotetan
Cephapirin
Cefoxitin
Cephadrine
Cefotaxime
Cefamandole
Cephalexin
Cefpodoxime
Cefadroxil
Ceftriaxone
Cefatrizine
Cefetamet
Cefeteram
Adaptedfrom
[3,12].
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 389
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

leukopenia, (n = 99, 27%), agranulocytosis (n = 58, 15.8%), andothers. In 62 cases, patients received between 1 and 14 days oftherapy (mean 7.7 + 4.1 days). Overall, there were 82 (22.4%)deaths. The authors concluded that while piperacillin-associatedneutropenia is rare; cases may arise after treatment durationshorter than 14 days [82]. Agranulocytosis was described withceftriaxone (6 reports), cephalothin (3 reports), cephapirin(4 reports), cefipime (3 reports) and isolated case reports havebeen associated with amoxicillin--clavulanate, cefamandole,cephalexin, cephadrine, penicillin G-procaine, and piperacillin(summarized in reference [81]).The clinical features of agranulocytosis are general malaise,
often including chills, myalgia, or arthralgia and nonspecificsore throat, and severe deep infections.Without intervention, most patients (> 60%) develop sep-
ticemia while some have evidence of pneumonia as well asanorectal, skin or oropharyngeal infections and finally septicshock. As in cancer chemotherapy, the occurrence of infectiondepends on the degree and duration of neutropenia. Whenantibiotics are administered preemptively, the patient’s com-plaints and the physical findings may be attenuated and fevermay be the only sign [37]. In elderly patients the clinical man-ifestations are generally more severe, with septicemia or septicshock appearing in at least two-thirds. In these patients, ane-mia and thrombocytopenia are often accompanying theagranulocytosis [37].The pathogenesis of agranulocytosis caused by b-lactam
antibiotics is uncertain. Clinical observations, studies in volun-teers and patients, and laboratory experiments have suggestedthat idiosyncratic drug-induced neutropenia or agranulocytosisis mediated by immunoallergic and toxic mechanisms [83]. Inmany cases, neutropenia occurs after prolonged exposure,resulting in a decreased granulocyte production by a hypoplas-tic bone marrow. In other cases, a repeated intermittent expo-sure is implied suggesting, but not proving, autoimmunemechanism [84]. In other cases direct damage to the bonemarrow plays a role [85].Leukopenia has been described with carbenicillin, ticarcil-
lin, as well as with azlocillin, mezlocillin, and piperacil-lin [86,87]; the carboxypenicillins are considered to be morefrequently associated with neutropenia than the other agents.Neutropenia has been reported after the use of cefotaxime forover 2 weeks and is reversible upon drug discontinuation.Methicillin-associated neutropenia (< 500/mm3) is relativelycommon in children (16/124; 13%), usually appearing after10 days of methicillin therapy or longer involving both neu-trophils and lymphocytes usually reverting to normal aftercessation of therapy [88]. Reversible neutropenia has alsobeen reported with imipenem-cilastatin [89].
4.2 Hemolytic anemiaHemolytic anemia seems to be rare with b-lactam antibiotics,with a notable exception of very high-dose administration ofthese agents (e.g., penicillin G in doses exceeding 20 millionunits/day).
Two types of hemolysing antibodies have been described.One type reacts with red blood cells (RBCs) only in the pres-ence of the drug and/or its metabolites, and predominantlycauses complement-mediated intravascular hemolysis. The sec-ond type binds to RBCs, regardless of the presence of drug, andtypically belongs to the IgG class. These do not activate com-plement, but rather cause Fc-mediated extravascular hemolysis.Some drugs may stimulate the production of both types of anti-bodies [90]. To date ~ 26 patients with piperacillin-inducedhemolytic anemia have been described, all adults. In 30%,infections associated with cystic fibrosis were the indicationfor piperacillin therapy. All patients had positive direct anti-globulin test for both IgG and IgM classes, the relevance ofwhich is questionable in the pathogenesis of this condition.Only one patient died [82]. Ceftriaxone has also been describedto cause hemolytic anemia in several patients, and in some thedirect anti-globulin test of IgG type was positive [88]. Further-more, hemolytic anemia has been described with cefotaxime,cefpodoxime, ceftazidime, and other newer cephalosporins [35].Altogether, and based on the number of reports, these newercephalosporins are considered relatively the frequent causes ofdrug-induced hemolytic anemia [89].
4.3 Thrombocytopenia and thrombocytopathyPatients with drug-induced thrombocytopenia commonlypresent with petechiae, purpura and thrombocytopenia withplatelet counts of < 20 � 109. Occasionally fever and chillsmay herald the onset. Usually the thrombocytopenia becomesevident after 10 days of drug application but occasionallyalready on the first day. Characteristically, platelet count beginsto rise within a few days after drug discontinuation. In rarercase several weeks will pass before the count begins to rise again,possibly because of the generation of antibiotic-independentIgG anti-platelet auto-antibodies [91]. Table 5 presents b-lactamantibiotics described to cause drug-induced immune thrombo-cytopenia. Typically, thrombocytopenia related to b-lactamadministration occurs as a result of high serum levels in thesetting of large doses or improperly dosed agents in the settingof renal failure.
Specifically, azlocillin is known to be associated with throm-bocytopenia, and cefotaxime administration was associatedwith thrombocytopenia in 29/764 (3.8%) of patients in oneseries [92]. However, this rate was not observed in otherseries [93]. Methicillin-associated thrombocytopenia is rare,and methicillin-dependent antiplatelet antibodies have beendetected in a few patients with this condition [94].
4.4 EosinophiliaEosinophils are produced in the bone marrow from stem cells(CD34+ multipotential myeloid progenitors) in response toeosinophilopoietic cytokines and growth factors includingIL-3, GM-CSF and IL-5. The normal count of circulatingeosinophils in the peripheral blood is 125/mm3 for adultsand 225/mm3 for children < 12 years. Eosinophilia has beenreported with Imipenem-Cilastatin, but was not associated
P. Lagace-Wiens & E. Rubinstein
390 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

with clinical manifestations. Eosinophilia may occur with anyb-lactam (or other) antibiotic and usually has no clinicalrelevance unless clearly associated with allergic phenomena [89].
5. Hepatobiliary adverse events
Penicillins, including ampicillin, have been known to cause vary-ing degrees of hepatotoxicity both of the acute hepatitis and cho-lestatic types [95]. The exact mechanism of the toxicity is notknown but believed to be of allergic nature. The risk is estimatedto be 1:100.000. Amoxicillin-clavulanate has led to cholestaticjaundice occasionally with a fatal outcome [96,97]. The hepaticdamage may be noticed weeks after therapy has been discontin-ued. The process may last for many weeks tomonths, but a com-plete recovery, provided there is no rechallenge is the rule [98].Predisposing factors for the development of jaundice includeadvanced age, male sex and a longer treatment duration.
However, hepatotoxicity has also been described in children,including the ‘vanishing duct syndrome’ [99].
Most cephalosporins cause mild elevations of liver enzymes,increase in transaminases are recorded in 1.4% of patients,alkaline phosphatase in 7 -- 9% and of bilirubin in2.2% [92]. Azlocillin and piperacillin cause elevation of liverenzymes in 0.9% and 3% of patients respectively [90]; occa-sionally, severe cholestatic jaundice has also beenobserved [100]. Repeated challenge may cause a more severeclinical picture [90]. Ceftriaxone is somewhat different as10 -- 40% of the drug is excreted in the bile resulting in con-centrations that may be ~ 150 higher than the blood levels.Ceftriaxone binds to calcium salts producing a precipitatethat may form biliary sludge and pseudolithiasis, particularlyin children, but also in adults with impaired gall bladder emp-tying [101,102]. In addition, mild elevations of liver enzymemay also be caused by ceftriaxone, which are readily reversible
Table 4. Groups of cephalosporins with dissimilar C3 and C7 side chains.
Dissimilar C-7 side chain.
Crossreactions between C-7 portions
of the agents within the group is
unlikely
Dissimilar C-3 side chain. Crossreactions between C-3 portions of the
agents within the group is unlikely
Group 1 Group 2
Cefazolin Cefotiam CeftrizineCefotetan Ceftazidime CefotiamCefuroxime Cephapirin CefpodoximeCefdinir Cefixime CefprozilCefoperazone Ceftibuten Ceftibuten
Moxolactam CeftriaxoneCefonicidCefepimeCefazolinCephaloridineCefaclor
Adapted from [3,12].
Table 5. Beta-lactam antibiotics described as a cause of drug-induced immune thrombocytopenia.
Agent Platelet
count < 20 � 109Re-challenge
performed
In vitro
testing
Mechanism
Amoxicillin + + Drug-dependent binding to specific plateletprotein
Ampicillin + + Increase in drug-dependent-platelet-associatedIgG in patent serum
Methicillin + + + IgG nonspecific platelet function end point usedPenicillin + + Like ampicillinPiperacillin + + + Like ampicillinCephamandole +Ceftazidime + + Like methicillinCephalothin + + + Like amoxicillinCeftizoxime + Like methicillin
Adapted from [152].
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 391
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

following drug discontinuation. Liver enzyme elevations havealso been noted during imipenem-cilastatin therapy with noparticular consequences [103]. The same has also been observedfor methicillin [104] as well as for all other anti-staphylococcalpenicillins. It is believed that nafcillin has the lowest rate ofsuch complications among these agents [105]. The carboxype-nicillins are also associated with cholestasis and with increasedliver enzymes and it is believed that ticarcillin is associatedwith less hepatotoxicity than carbenicillin [106].
6. Renal adverse events
The modern b-lactam antibiotics are remarkably safe from therenal point of view provided they are administered in regulartherapeutic doses. In the past, nephrotoxicity was regularly seenwith cephaloridine, but this compound is no longer on the mar-ket.With ampicillin, a few cases of interstitial nephritis have beendescribed, not uncommonly accompanied by a skin rash thussuggesting an allergic basis for this effect [107]. Higher doses(> 200 mg/kg/day) are more likely to be associated with nephro-toxicity [108]. High doses of methicillin have also been incrimi-nated as a cause of interstitial nephritis, characterized byhematuria, proteinuria, sterile pyuria, renal insufficiency andeosinophiluria accompanied by fever, rash and eosinophilia,again suggesting an allergic etiology [109,110]. Renal biopsy dem-onstrates heavy interstitial infiltrates with lymphocytes, plasmacells and eosinophil infiltrationwith sparing of the glomeruli [111].Interstitial nephritis has to be differentiated from hemorrhagiccystitis which can also be caused by methicillin [112]. Mostpatients with methicillin–induced interstitial nephritis willrecover slowly once the agent is withdrawn; in severe cases pred-nisone has led to a more rapid normalization of renal func-tions [110]. Substitution of methicillin with another b-lactamantibiotic is not recommended since crossreactivity mayoccur [112]. Immunohistochemical investigations in such a casedisclosed binding to the kidney tissues of the hapten of methicil-lin dimethoxyphenyl-penicilloyl with immunoglobulins [113].Thus, it appears that when methicillin binds as a hapten to thebasal basement of the tubular cell and changes its antigenicity,the induced antibodies are then directed against both the haptenand the transformed basal membrane inducing the nephritis [114].Interstitial nephritis induced by methicillin appears to be morecommon when large doses are administered for prolonged peri-ods [115] and also appears to be more common with methicillinthan with other penicillins [116]. Nephrotoxicity may appear afterhigh and prolonged use of imipenem-cilastatin, due to thecilastatin component, which is not a b-lactam molecule [14].
7. Neurological adverse events
All b-lactam antibiotics, when administered in high doses,may cause seizures in experimental animals and in humans,particularly in the presence of an underlying brain diseasesuch as idiopathic epilepsy [117] or when a medical condition(such as meningitis) increases the agent’s penetration of the
blood--brain barrier. In such instances, the brain is exposedto particularly high concentrations of the agent. The patho-physiologic mechanism is the epileptogenic activity of theb-lactam molecule itself on the neurons. Convulsions can beanticipated with high IV doses of ampicillin when serum lev-els exceed 800 µg/ml but have also been described withconventional dosages.
Penicillin in high dosages has rarely been reported to causebenign intracranial hypertension, likely secondary to cere-bral vasculitis [118]. Carbenicillin, piperacillin, piperacillin-tazobactam and ticarcillin in high doses or in conventionaldoses in patients with compromised renal function have alsoproduced seizures [119,120].
Cefotaxime-associated brain toxicity has been reported in0.3% of > 2000 patients [92]. The major clinical manifesta-tions of this toxicity were hallucinations, vertigo, disorienta-tion as well as headache. No seizures were reported with theuse of cefotaxime. Cephalexin in high doses has been associ-ated with diplopia, tinnitus, ataxia and even grand malseizures [121,122].
8. Gastrointestinal adverse events excludingC. difficile-associated diarrhea
Oral, and less commonly, systemically administered b- lactamantibiotics can cause nausea, vomiting and diarrhea of moderateseverity. Ampicillin-associated diarrhea appears to bemore com-mon in children (8%) and more often with ampicillin than withamoxicillin [123]. The rate of diarrhea in adults is 5 -- 20% and ishigher in the older age group [124]. Occasionally one may findovergrowth of yeast in the intestine leading to diarrhea and mal-absorption as a result of prolonged oralb-lactam therapy. Amox-icillin has significantly better bioavailability and is thus less likely(2%) to cause diarrhea than ampicillin [125]. With amoxicillin-clavulanate, the rate of gastrointestinal adverse events is relatedto the clavulanic acid component of the combination and seemsto be lower when the twice-daily 875/125mg and 2000/125mgdoses of amoxicillin-clavulanate are given than with the conven-tional dose [126]. Nevertheless, the rate of diarrhea associatedwith the combination is higher than with amoxicillin alone [127].It has been estimated that with a conventional dosage of500/125 mg three times daily, the rate of upper gastrointestinalevents is 2.5%, nausea 1.4% and diarrhea 3.4% among38,500 patients [128].
The cephalosporins like cefazolin and cephalothin may beassociated with C.difficile diarrhea even after a single dose(see the section ‘C.difficile-associated disease’). For cefuroximeaxetil-treated patients, the rate of gastrointestinal adverseeffects were diarrhea 2 -- 10.2%, nausea 0 -- 5%, vomiting1 -- 5%, abdominal pain 2 -- 2.8% and dizziness 0.8 -- 3%,regardless of whether the patients received 5 or 10 days’therapy. The gastrointestinal tolerability of cefuroxime axetilwas better than that of amoxicillin-clavulanate [129]. Withcefotaxime, diarrhea has been observed in 0.44 -- 0.79% ofpatients, vomiting in 0.7%, abdominal pain in 0.1% and
P. Lagace-Wiens & E. Rubinstein
392 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

mucosal candidiasis in 0.28% [93]. Ceftriaxone causes a sub-stantial alteration in the colonic flora with suppression ofgram-negative bacilli and overgrowth of enterococci andyeast, more so than with other cephalosporins [130]. Cepha-lexin, an oral cephalosporin, is associated with diarrhea inup to 5% of patients. Dyspepsia, candidiasis anorexia andanal pruritus have also been described but are less com-mon [131]. The isoxazolyl penicillins (cloxacillin, oxacillin,methicillin and flucloxacillin) are rarely associated with gas-trointestinal effects. Piperacillin-tazobactam is associatedwith diarrhea in 3.8 -- 4/6% of cases, and more often thanwith piperacillin alone [132,133]. Ertapenem is associated withan incidence of 1.7 -- 7.0% diarrhea, 0.7 -- 8% nausea and0.9% vomiting. These adverse events have similar incidencein patients treated with meropenem and imipenem and notmuch different from placebo in various clinical trials [14].
9. C. difficile-associated disease
The risk of CDAD, ranging from diarrhea to toxic megaco-lon and death is often overlooked as an adverse event associ-ated with antibiotic use, including b-lactams. The clinicaldisease and pathophysiology have been extensively reviewedelsewhere [6,80,134,135]. The primary effect of antimicrobialson the development of CDAD is the alteration of gut flora,particularly the destruction of ‘beneficial’ anaerobic flora [6].Depending on the study, cephalosporins and extended spec-trum penicillins have been implicated as significant risks forthe development of CDAD [6]. Although there has been alack of well-designed prospective studies to assess the indi-vidual risks associated with antibiotic classes, numerousstudies have suggested that third-generation (oximino-)cephalosporins are consistently associated with high relativerisks of CDAD [6,136-138]. Clinicians should consider thiswhen prescribing b-lactam (and other) antimicrobials andreduce the duration, dose and spectrum of antibiotic therapywhen possible.
10. Adverse reactions associated with specificagents
Although many adverse events related to b-lactam use are classspecific, some unusual adverse events are associated with spe-cific antimicrobial agents which have restricted their use.While many of these agents are no longer in routine use,some are still regularly used and clinicians should be awareof the potential adverse events associated with their use.
10.1 CefaclorCefaclor is a second-generation oral cephalosporin released in1979 [139]. The primary recipients have been children withmild to moderate respiratory tract infections [139]. Soon afterits release, cefaclor was associated with a significant numberof adverse drug reactions characterized by onset of urticaria,erythema multiforme-like rash, arthralgia or arthritis, and
pruritus sparing of the mucous membranes [139]. This illnesshas similar clinical presentation to classic serum sickness,but the circulating immune complexes are absent and nephri-tis does not occur and is thus coined ‘serum sickness-like reaction’. The reaction appears to occur in up to 3.4%of recipients and resolves spontaneously after discontinuationof the drug [140]. It is not associated with adverse reaction toother cephalosporins [139,141,142]. The reaction may be associ-ated with inherited defects in the metabolism of reactive inter-mediates or metabolites or other genetic predispositions inaffected individuals [141]. Most serum sickness-like reactionsto cefaclor and other b-lactams in children are associatedwith negative responses in non-immediate-reading skin testsand do not relapse during subsequent treatments with theinitially suspected b-lactams [58].
10.2 Thiomethyl tetrazole side-chain agentsCephalosporins and oxalactams with a thiomethyl tetrazole(MTT) side chain are known to have unique adverse effectsthat have severely limited their clinical use. The agents thathave been in routine use are cefamandole, cefotetan, cefo-perazone and moxalactam. The thiomethyl tetrazole groupis a known acetaldehyde dehydrogenase inhibitor and istherefore associated with disulfiram-like reactions andacute ethanol sensitivity [143]. Thiomethyl tetrazole antibi-otics are also metabolized into thiomethyl tetrazoledimmers that inhibit glutamate synthesis resulting in acuteprothrombin deficiency (warfarin-like reaction) and risk ofbleeding [143]. The condition is reversible with vitamin Kadministration [143].
10.3 Ceftriaxone calcium precipitation and bile
sludgeCeftriaxone therapy is associated with the formation of biliarysludge and pseudolithiasis, particularly in children [144-146].Reports in adults are infrequent but asymptomatic sludgingdoes occur [146]. The mechanism of biliary sludging and pre-cipitation is related to the excretion of significant quantitiesof ceftriaxone into the bile as a divalent anion [146]. The pres-ence of calcium ions in bile results in the formation of aninsoluble precipitate which results in thickening and occasion-ally stone formation [146]. The reaction is dependent ondose and children are more prone to experiencing it [146].The sludging typically resolves after discontinuation oftherapy [146]. Incidences of renal calculi produced throughthe same mechanism have also been reported [145].
The possibility of ceftriaxone spontaneously precipitatingwhen infused concurrently or in succession with calcium-containing infusions and causing end-organ damage hasbeen studied and remains controversial. The FDA issued awarning indication that such combinations should beavoided, but review of available data in adults did not substan-tiate the risk [147]. Until further research is done, avoiding thiscombination is prudent, particularly in children where therisk has not been studied [147].
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 393
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

11. Management of allergic reactions ofb-lactam antibiotics
The first step is to recognize the relationship between the adverseeffects and the administered drug. This may not be as simple as itmay seem, since a patient who receives a large number of drugswith several underlying conditions and complicating issues mayhave a number of potential etiologies for any given adverse event.A high rate of vigilance needs to be maintained and a low thresh-old of suspicion for adverse events is needed. Unfortunately, onlyin a minority of cases are laboratory tests diagnostic, as is the casewith methicillin-induced nephropathy and immediate-typehypersensitivity to penicillin. In most instances, clinical judg-ment remains the best tool physicians have. When suspicion ofa b-lactam-associated adverse event is noted, the first step wouldbe to discontinue the offending agent or a change to a drug of adifferent chemical class. In most instances, a cephalosporin canbe considered in penicillin allergic patients, and in some instan-ces, a different cephalosporin can be considered in cephalosporinallergy as discussed previously. In most cases this step is sufficientto reverse the condition over a period of several days. In someinstances, a later challenge with the same agent has been recom-mended for agents that are vital and that the patient will needwith high likelihood in the future. In very severe cases, for exam-ple SJS and renal failure, a trial of corticosteroids needs to beconsidered carefully. If a life-threatening adverse reaction to ab-lactam antibiotic requires a change of antibiotic class, consider-ationmust be given to the intended target organism for an appro-priate choice of an alternate antimicrobial to be made. Althoughdefinitive treatment should be guided by susceptibility testing,agents such as vancomycin, macrolides or clindamycin usuallyhave similar activity against gram-positive organisms for whichpenicillins and early cephalosporins are used while fluoroquino-lones, sulfonamides and aminoglycosides frequently have similaractivity against gram-negative organisms for which extendedspectrum penicillins and cephalosporins are used. Clindamycinor metronidazole may be considered as alternative options incases where b-lactams are used for anaerobic infections.In immediate-type allergic reactions, skin testing may add
some certainty to the diagnosis, but limitation of skin testingexists and many clinicians erroneously assume that negativeskin tests mean tolerance to all b-lactams. This is especiallyfalse for primary cephalosporin allergy, which cannot be pre-dicted using penicillin skin testing. For cephalosporin aller-gies, cephalosporin skin-testing can be considered fordiagnosis but is not yet well standardized as a diagnosticmethod. Other in vitro diagnostic tests of IgE-mediatedhypersensitivity to b-lactams can be considered but havebeen reported to have low sensitivity (43 -- 75%) and specific-ity (67 - 83%) [58,148,149]. Re-challenge after a negative skintest in a clinical setting capable of managing potentially severeimmediate-type hypersensitivities is considered the gold stan-dard for the diagnosis of immediate-type b-lactam allergy andshould be considered in individuals in whom b-lactamtherapy may be required in the future.
If an immediate allergic reaction to an agent is identifiedclinically either by skin testing or through an in-vitro assayand if the agent is critically needed for optimal treatment of apatient, then desensitization is recommended. Desensitizationhas been reviewed extensively elsewhere [7], but consists ofincremental increases from very small doses to therapeuticdoses in regular increments. Patients are usually pre-treatedwith antihistamines and monitored for allergic reactions.Desensitized patients can continue to receive therapeutic doseson a regular schedule, but any interruption in dosing meansanother desensitization course will be required.
Management of non-immediate reactions to b-lactams hasbeen reviewed elsewhere and varied according to the exactmechanism of hypersensitivity. These may vary from com-plete cessation and avoidance and supportive managementof symptoms with corticosteroids (in serum-sickness reac-tions) to reassurance, as might be the case with nonspecificor presumed infection-related morbilliform rashes [7,15,150,151].
12. Expert opinion
Adverse events related to b-lactam antibiotics are commonlyreported. Among the potentially serious adverse events, the cli-nician is most commonly faced with reported patient allergy orrash to b-lactam antibiotics. Since 90% of such reports cannotbe substantiated by skin and/or in vitro testing, it behooves theclinician to recognize scenarios that are more likely to reflecttrue allergy. Important questions to ask in order to determinewhether a true allergy exists are the timing of onset of the reac-tion with respect to drug administration, how long ago thereaction occurred, the exact symptoms (including urticaria,pruritus, edema etc.), concomitant medications and subsequentreactions to related drugs. Most true allergies can also generallybe separated from nonspecific drug rash: rashes associated withviral infections and hypersensitivity reactions other than type Ireactions (type II -- IV).
Once true allergy has been accurately suspected, the courseof action most clinicians take is the complete avoidance ofb-lactam antimicrobials, including cephalosporins. Unfortu-nately, this approach was founded by flawed early observations,and has proven to be incorrect. It has become evident that cross-reactions between penicillin or amoxicillin and cephalosporinsare due to similarities in side chains between the penicillin andcephalosporin. For patients truly allergic to penicillin, the riskof a reaction from a cephalosporin with side chains that differfrom penicillin or amoxicillin (e.g., cefuroxime, cefpodoxime,cefdinir, ceftriaxone etc.) is as low as the risk of a reaction toany unrelated drug and their use is justified and defensible byavailable evidence. As such, patients with penicillin allergy cansafely be given cephalosporins provided there is no structural sim-ilarity between the side chains of the cephalosporin molecule.Similarly, crossreaction between cephalosporins is not class spe-cific but rather side-chain specific, and cephalosporins with dif-ferent C-3 and C-7 side chains from the culprit agent can safelybe prescribed to individuals with a cephalosporin allergy.
P. Lagace-Wiens & E. Rubinstein
394 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

Unfortunately, individuals with true penicillin allergy are threetimes more likely to develop de novo allergies to unrelatedcompounds, which may appear to be crossreactions when thedrug in question is a structurally unrelated cephalosporin. TypeII or III reactions, allergic renal and hepatic toxicities, as well assevere reactions such as SJS are agent specific, and the offendingagent and closely related agents should generally be avoided, asshould any skin testing using the culprit agent. Possible excep-tions include non-immediate-reading skin testing of childrenwith suspected infectious causes of SJS and possibly when multi-ple drugs are simultaneously suspected as causes of the severecutaneous reactions. Such non-immediate reading of skin testingshould be performed under the guidance of an expert in these set-tings. When penicillins or cephalosporins are the single or bestavailable option for treatment of a condition (e.g., syphilis inregnancy and streptococcal endocarditis) in an allergic patient,desensitization is the recommended over administrationof a potentially suboptimal therapy. Desensitization is contrain-dicated in patients with severe (or potentially severe) skinreactions, such as acute generalized exanthematic pustulosis, toxicepidermal necrolysis, drug-induced SJS and DRESS.
Other adverse events related to the use of b-lactamsinclude agent-specific adverse events and a variety of adverseevents related to other body systems. With the exception ofceftriaxone, most of the agents associated with frequent and
agent-specific adverse events are no longer in routine use, andtheir use has largely been supplanted by other agents.Nonallergicadverse events are primarily dose-related and careful dosing,accounting for diminished renal function, and frequentre-evaluation of dose in critically ill patients with tenuous renalfunction will prevent most of these dose-related effects. Finally,a small proportion of nonallergic adverse events appear to be idi-opathic and not dose-related. Some of these, such as interstitialnephritis and SJS associated with b-lactamsmay actually be aller-gic in origin. In such cases, it is better to avoid the offendingdrug altogether. These instances are rare. In summary, althoughb-lactam drugs have documented and potentially seriousside effects, when proper dosing and a careful selection ofb-lactams in allergic patients is considered, they remainremarkably safe and very useful agents.
Declaration of interest
P Lagace-Wiens: Accepted honoraria from Bayer, travelgrants from Siemens Healthcare Diagnostics and Sanofi-Pasteur. Owns shares in A Zeneca and B Daltonics as partof a diversified portfolio. Research funds from Novexel S.A. and A Zeneca. E Rubinstein states no conflict of interestand has received no payment in the preparation ofthis manuscript.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Smith RG. Penicillin and cephalosporin
drug allergies: a paradigm shift. J Am
Podiatr Med Assoc 2008;98:479-88.. Reviews the evidence for using selected
cephalosporins in
penicillin-allergic individuals.
2. Cunha BA. Antibiotic side effects.
Med Clin North Am 2001;85:149-85. General review of antimicrobial
adverse events.
3. Pichichero ME. Use of selected
cephalosporins in penicillin-allergic
patients: a paradigm shift.
Diagn Microbiol Infect Dis
2007;57:13S-8S
4. Pichichero ME, Casey JR. Safe use of
selected cephalosporins in
penicillin-allergic patients:
a meta-analysis. Otolaryngol Head
Neck Surg 2007;136:340-7.. Definitive meta-analysis supporting the
use of cephalosporins in
penicillin-allergic individuals.
5. Pichichero ME. Cephalosporins can be
prescribed safely for penicillin-allergic
patients. J Fam Pract 2006;55:106-12
6. Blondeau JM. What have we learned
about antimicrobial use and the risks for
Clostridium difficile-associated diarrhoea?
J Antimicrob Chemother
2009;63:238-42
7. Yates AB. Management of patients with a
history of allergy to beta-lactam
antibiotics. Am J Med 2008;121:572-6
8. DePestel DD, Benninger MS,
Danziger L, et al. Cephalosporin use in
treatment of patients with penicillin
allergies (2003). J Am Pharm Assoc
2008;48:530-40
9. Baldo BA, Pham NH, Zhao Z.
Chemistry of drug allergenicity.
Curr Opin Allergy Clin Immunol
2001;1:327-35
10. Andes DR, Craig WA. Cephalosporins.
In: Mandell GL, Bennett JE, Dolin R,
editors. Principles and Practice of
Infectious Diseases. Elsevier;
Philadelphia, PA: 2009. p. 323-39
11. Moreno E, Macias E, Davila I, et al.
Hypersensitivity reactions to
cephalosporins. Expert Opin Drug Saf
2008;7:295-304
12. Pichichero ME. A review of evidence
supporting the American Academy of
Pediatrics recommendation for
prescribing cephalosporin antibiotics for
penicillin-allergic patients. Pediatrics
2005;115:1048-57. Review of evidence supporting the use
of cephalosporins in
penicillin-allergic individuals.
13. Cunha BA. Antibiotic selection in the
penicillin-allergic patient. Med Clin
North Am 2006;90:1257-64
14. Zhanel GG, Wiebe R, Dilay L, et al.
Comparative review of the carbapenems.
Drugs 2007;67:1027-52
15. Park MA, Li JT. Diagnosis and
management of penicillin allergy.
Mayo Clin Proc 2005;80:405-10. Review of the diagnosis and
management of penicillin allergy.
16. Schafer JA, Mateo N, Parlier GL,
Rotschafer JC. Penicillin allergy skin
testing: what do we do now?
Pharmacotherapy 2007;27:542-5
17. Wong BK, Sahly Y, Mistry G, et al.
Comparative disposition of [14C]
ertapenem, a novel carbapenem
antibiotic, in rat, monkey and man.
Xenobiotica 2004;34:379-89
18. Harrison MP, Haworth SJ, Moss SR,
et al. The disposition and metabolic fate
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 395
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

of 14C-meropenem in man. Xenobiotica
1993;23:1311-23
19. Frumin J, Gallagher JC. Allergic
cross-sensitivity between penicillin,
carbapenem, and monobactam
antibiotics: what are the chances?
Ann Pharmacother 2009;43:304-15
20. Salkind AR, Cuddy PG, Foxworth JW.
The rational clinical examination. Is this
patient allergic to penicillin? An
evidence-based analysis of the likelihood
of penicillin allergy. Jama
2001;285:2498-505. Evidence-based approach to clinical
diagnosis of penicillin allergy.
21. Jappe U. Amoxicillin-induced exanthema
in patients with infectious
mononucleosis: allergy or transient
immunostimulation? Allergy
2007;62:1474-5
22. Yates AB, deShazo RD. Allergic and
nonallergic drug reactions. South Med J
2003;96:1080-7
23. Clark BM, Kotti GH, Shah AD,
Conger NG. Severe serum sickness
reaction to oral and intramuscular
penicillin. Pharmacotherapy
2006;26:705-8
24. Pichler WJ. Immune mechanism of drug
hypersensitivity. Immunol Allergy Clin
North Am 2004;24:373-97.v-vi
25. Kerr JR. Penicillin allergy: a study of
incidence as reported by patients. Br J
Clin Pract 1994;48:5-7
26. Ahlstedt S. Penicillin allergy–can the
incidence be reduced? Allergy
1984;39:151-64
27. Sogn DD, Evans R III, Shepherd GM,
et al. Results of the national institute of
allergy and infectious diseases
collaborative clinical trial to test the
predictive value of skin testing with
major and minor penicillin derivatives in
hospitalized adults. Arch Intern Med
1992;152:1025-32
28. Idsoe O, Guthe T, Willcox RR,
de Weck AL. Nature and extent of
penicillin side-reactions, with
particular reference to fatalities from
anaphylactic shock. Bull World
Health Organ 1968;38:159-88
29. Kelkar PS, Li JT. Cephalosporin
allergy. N Engl J Med
2001;345:804-9
30. Shepherd GM. Hypersensitivity reactions
to drugs: evaluation and management.
Mt Sinai J Med 2003;70:113-25
31. Shariatmadar S, Storry JR, Sausais L,
Reid ME. Cefotetan-induced immune
hemolytic anemia following prophylaxis
for cesarean delivery. Immunohematol
2004;20:63-6
32. Kunzmann S, Thomas W, Mayer B,
et al. Immune-mediated severe hemolytic
crisis with a hemoglobin level of 1.6 g/dl
caused by anti-piperacillin antibodies in a
patient with cystic fibrosis. Infection
2010;38:131-4
33. Kakaiya R, Cseri J, Smith S, et al. A case
of acute hemolysis after ceftriaxone:
immune complex mechanism
demonstrated by flow cytometry.
Arch Pathol Lab Med 2004;128:905-7
34. Barton LL. Cefuroxime-induced immune
hemolysis. J Pediatr
2004;144:690; author reply
35. Garratty G. Drug-induced immune
hemolytic anemia. Hematology Am Soc
Hematol Educ Program 2009;(1):73-9
36. Arndt PA, Garratty G, Hill J, et al. Two
cases of immune haemolytic anaemia,
associated with anti-piperacillin, detected
by the ’immune complex’ method.
Vox Sang 2002;83:273-8
37. Andres E, Maloisel F. Idiosyncratic
drug-induced agranulocytosis or acute
neutropenia. Curr Opin Hematol
2008;15:15-21
38. Kurokawa I. A case of purpuric drug
eruption due to cefaclor. Int J
Antimicrob Agents 2002;20:393-4
39. Kaufman DW, Kelly JP, Johannes CB,
et al. Acute thrombocytopenic purpura in
relation to the use of drugs. Blood
1993;82:2714-18
40. Abate G, Godbole K, Springston C.
Piperacillin/tazobactam--induced
petechial rash. Ann Pharmacother
2010;44:1345-6
41. King BA, Geelhoed GC.
Adverse skin and joint reactions
associated with oral antibiotics in
children: the role of cefaclor in serum
sickness-like reactions. J Paediatr
Child Health 2003;39:677-81
42. Yesudian PD, King CM. Occupational
allergic contact dermatitis from
meropenem. Contact Dermat 2001;45:53
43. Kim YH, Ko JY, Kim YS, Ro YS. A case
of allergic contact dermatitis to clavulanic
acid. Contact Dermat 2008;59:378-9
44. Rosso R, Mattiacci G, Bernardi ML,
et al. Very delayed reactions to
beta-lactam antibiotics. Contact Dermat
2000;42:293-5
45. Hausermann P, Bircher AJ. Immediate
and delayed hypersensitivity to
ceftriaxone, and anaphylaxis due to
intradermal testing with other
beta-lactam antibiotics, in a previously
amoxicillin-sensitized patient.
Contact Dermat 2002;47:311-12
46. de Thier F, Blondeel A, Song M. Acute
generalized exanthematous pustulosis
induced by amoxycillin with clavulanate.
Contact Dermat 2001;44:114-15
47. Conde-Salazar L, Guimaraens D,
Gonzalez MA, Mancebo E. Occupational
allergic contact urticaria from
amoxicillin. Contact Dermat
2001;45:109
48. Andre MC, Silva R, Filipe PL, et al.
Systemic contact allergy to penicillin
after prick and intradermal tests.
Ann Allergy Asthma Immunol
2011;106:174-5
49. Yawalkar N, Hari Y, Frutig K, et al. T
cells isolated from positive epicutaneous
test reactions to amoxicillin and
ceftriaxone are drug specific and
cytotoxic. J Invest Dermatol
2000;115:647-52
50. Song EK, Seon JK, Jeong MS.
Delayed-type hypersensitivity reaction to
piperacillin/tazobactam in a patient with
an infected total knee replacement.
J Bone Joint Surg Br 2010;92:1596-9
51. Romano A, Torres MJ, Quaratino D,
et al. Diagnostic evaluation of delayed
hypersensitivity to systematically
administered drugs. Allergy
1999;54(Suppl 58):23-7
52. Romano A, Viola M, Gaeta F, et al.
Patch testing in non-immediate drug
eruptions. Allergy Asthma Clin Immunol
2008;4:66-74
53. Narayanan VS, Mamatha GP, Ashok L,
Rajashekar N. Steven Johnson syndrome
due to I.V Ceftriaxone--a case report.
Indian J Dent Res 2003;14:220-3
54. Thestrup-Pedersen K, Hainau B,
Al’Eisa A, et al. Fatal toxic epidermal
necrolysis associated with ceftazidine and
vancomycin therapy: a report of two
cases. Acta Derm Venereol
2000;80:316-17
55. Lopez S, Blanca-Lopez N,
Cornejo-Garcia JA, et al. Nonimmediate
reactions to betalactams. Curr Opin
Allergy Clin Immunol 2007;7:310-16
P. Lagace-Wiens & E. Rubinstein
396 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

56. Lissia M, Mulas P, Bulla A, Rubino C.
Toxic epidermal necrolysis (Lyell’s
disease). Burns 2010;36:152-63
57. Forman R, Koren G, Shear NH.
Erythema multiforme, Stevens-Johnson
syndrome and toxic epidermal necrolysis
in children: a review of 10 years’
experience. Drug Saf 2002;25:965-72
58. Ponvert C, Perrin Y, Bados-Albiero A,
et al. Allergy to betalactam antibiotics in
children: results of a 20-year study based
on clinical history, skin and challenge
tests. Pediatr Allergy Immunol
2011;22:411-18
59. Cacoub P, Musette P, Descamps V,
et al. The dress syndrome: a literature
review. Am J Med 2011;124:588-97
60. Dash CH. Penicillin allergy and the
cephalosporins. J Antimicrob Chemother
1975;1:107-18
61. Petz LD. Immunologic cross-reactivity
between penicillins and cephalosporins:
a review. J Infect Dis
1978;137(Suppl):S74-S9
62. Petz LD. Immunologic reactions of
humans to cephalosporins.
Postgrad Med J 1971;47(Suppl):64-9
63. Smith JW, Johnson JE, Cluff LE. Studies
on the epidemiology of adverse drug
reactions. II. An evaluation of penicillin
allergy. N Engl J Med
1966;274:998-1002
64. Baumgart KW, Baldo BA.
Cephalosporin allergy. N Engl J Med
2002;346:380-1
65. Blanca M, Mayorga C, Torres MJ, et al.
Side-chain-specific reactions to
betalactams: 14 years later.
Clin Exp Allergy 2002;32:192-7
66. Miranda A, Blanca M, Vega JM, et al.
Cross-reactivity between a penicillin and
a cephalosporin with the same side
chain. J Allergy Clin Immunol
1996;98:671-7
67. Blanca M, Vega JM, Garcia JJ, et al.
Immediate hypersensitivity reactions to
penicillin and related antibiotics.
Clin Exp Allergy 1989;19:556-8
68. Blanca M, Perez E, Garcia J, et al.
Anaphylaxis to amoxycillin but good
tolerance for benzyl penicillin. In vivo
and in vitro studies of specific IgE
antibodies. Allergy 1988;43:508-10
69. Blanca M, Fernandez J, Miranda A, et al.
Cross-reactivity between penicillins and
cephalosporins: clinical and immunologic
studies. J Allergy Clin Immunol
1989;83:381-5
70. Madaan A, Li JT. Cephalosporin allergy.
Immunol Allergy Clin North Am
2004;24:463-76.vi-vii
71. Romano A, Viola M,
Gueant-Rodriguez RM, et al. Brief
communication: tolerability of
meropenem in patients with
IgE-mediated hypersensitivity to
penicillins. Ann Intern Med
2007;146:266-9
72. Romano A, Viola M,
Gueant-Rodriguez RM, et al. Imipenem
in patients with immediate
hypersensitivity to penicillins. N Engl
J Med 2006;354:2835-7
73. Atanaskovic-Markovic M, Gaeta F,
Medjo B, et al. Tolerability of
meropenem in children with
IgE-mediated hypersensitivity to
penicillins. Allergy 2008;63:237-40
74. Romano A, Blanca M, Torres MJ, et al.
Diagnosis of nonimmediate reactions to
beta-lactam antibiotics. Allergy
2004;59:1153-60. Review of the diagnosis of non-Type I
allergic reactions to penicillin.
75. Fox S, Park MA. Penicillin skin testing
in the evaluation and management of
penicillin allergy. Ann Allergy
Asthma Immunol 2011;106:1-7
76. Bousquet PJ, Gaeta F,
Bousquet-Rouanet L, et al. Provocation
tests in diagnosing drug hypersensitivity.
Curr Pharm Des 2008;14:2792-802
77. Brockow K, Romano A. Skin tests in the
diagnosis of drug hypersensitivity
reactions. Curr Pharm Des
2008;14:2778-91
78. Blanca M, Romano A, Torres MJ, et al.
Update on the evaluation of
hypersensitivity reactions to betalactams.
Allergy 2009;64:183-93
79. Strom BL, Carson JL, Schinnar R, et al.
Descriptive epidemiology of
agranulocytosis. Arch Intern Med
1992;152:1475-80
80. Andres E, Maloisel F, Kurtz JE, et al.
Modern management of
non-chemotherapy drug-induced
agranulocytosis: a monocentric cohort
study of 90 cases and review of the
literature. Eur J Intern Med
2002;13:324-8
81. Andersohn F, Konzen C, Garbe E.
Systematic review: agranulocytosis
induced by nonchemotherapy drugs.
Ann Intern Med 2007;146:657-65
82. Scheetz MH, McKoy JM, Parada JP,
et al. Systematic review of
piperacillin-induced neutropenia.
Drug Saf 2007;30:295-306
83. Andres E, Zimmer J, Affenberger S,
et al. Idiosyncratic drug-induced
agranulocytosis: update of an old
disorder. Eur J Intern Med
2006;17:529-35
84. Claas FH. Immune mechanisms leading
to drug-induced blood dyscrasias. Eur J
Haematol Suppl 1996;60:64-8
85. Guest I, Uetrecht J. Drugs that induce
neutropenia/agranulocytosis may target
specific components of the stromal cell
extracellular matrix. Med Hypotheses
1999;53:145-51
86. Kerr RO, Cardamone J, Dalmasso AP,
Kaplan ME. Two mechanisms of
erythrocyte destruction in
penicillin-induced hemolytic anemia.
N Engl J Med 1972;287:1322-5
87. Mayer B, Yurek S, Salama A.
Piperacillin-induced immune hemolysis:
new cases and a concise review of the
literature. Transfusion 2010;50:1135-8
88. Seltsam A, Salama A.
Ceftriaxone-induced immune haemolysis:
two case reports and a concise review of
the literature. Intensive Care Med
2000;26:1390-4
89. Salama A. Drug-induced immune
hemolytic anemia. Expert Opin Drug Saf
2009;8:73-9
90. Gooding PG, Clark BJ, Sathe SS.
Piperacillin: a review of clinical
experience. J Antimicrob Chemother
1982;9(Suppl B):93-9
91. Nieminen U, Kekomaki R.
Quinidine-induced thrombocytopenic
purpura: clinical presentation in relation
to drug-dependent and drug-independent
platelet antibodies. Br J Haematol
1992;80:77-82
92. Smith CR. Cefotaxime and
cephalosporins: adverse reactions in
perspective. Rev Infect Dis
1982;4(Suppl):S481-8
93. Young JP, Husson JM, Bruch K, et al.
The evaluation of efficacy and safety of
cefotaxime: a review of 2500 cases.
J Antimicrob Chemother
1980;6(Suppl A):293-300
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 397
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

94. Schiffer CA, Weinstein HJ, Wiernik PH.
Letter: methicillin-associated
thrombocytopenia. Ann Intern Med
1976;85:338-9
95. Koklu S, Yuksel O, Filik L, et al.
Recurrent cholestasis due to
ampicillin. Ann Pharmacother
2003;37:395-7
96. Ersoz G, Karasu Z, Yildiz C, et al.
Severe toxic hepatitis associated with
amoxycillin and clavulanic acid. J Clin
Pharm Ther 2001;26:225-9
97. Thomson JA, Fairley CK, Ugoni AM,
et al. Risk factors for the development of
amoxycillin-clavulanic acid associated
jaundice. Med J Aust 1995;162:638-40
98. Cundiff J, Joe S. Amoxicillin-clavulanic
acid-induced hepatitis. Am J Otolaryngol
2007;28:28-30
99. Smith LA, Ignacio JR, Winesett MP,
et al. Vanishing bile duct syndrome:
amoxicillin-clavulanic acid associated
intra-hepatic cholestasis responsive to
ursodeoxycholic acid. J Pediatr
Gastroenterol Nutr 2005;41:469-73
100. Hargreaves JE, Herchline TE. Severe
cholestatic jaundice caused by
mezlocillin. Clin Infect Dis
1992;15:179-80
101. Shiffman ML, Keith FB, Moore EW.
Pathogenesis of ceftriaxone-associated
biliary sludge. In vitro studies of
calcium-ceftriaxone binding and
solubility. Gastroenterology
1990;99:1772-8
102. Michielsen PP, Fierens H,
Van Maercke YM. Drug-induced
gallbladder disease. Incidence, aetiology
and management. Drug Saf
1992;7:32-45
103. Calandra GB, Wang C, Aziz M,
Brown KR. The safety profile of
imipenem/cilastatin: worldwide clinical
experience based on 3470 patients.
J Antimicrob Chemother
1986;18(Suppl E):193-202
104. Berger M, Potter DE. Pitfall in diagnosis
of viral hepatitis on haemodialysis unit.
Lancet 1977;2:95-6
105. Maraqa NF, Gomez MM,
Rathore MH, Alvarez AM. Higher
occurrence of hepatotoxicity and rash in
patients treated with oxacillin,
compared with those treated with
nafcillin and other commonly used
antimicrobials. Clin Infect Dis
2002;34:50-4
106. Graft DF, Chesney PJ. Use of
ticarcillin following
carbenicillin-associated hepatotoxicity.
J Pediatr 1982;100:497-9
107. Woodroffe AJ, Weldon M, Meadows R,
Lawrence JR. Acute interstitial nephritis
following ampicillin hypersensitivity.
Med J Aust 1975;1:65-8
108. Lee HA, Hill LF. The use of ampicillin
in renal disease. Br J Clin Pract
1968;22:354-7
109. Woodroffe AJ, Thomson NM,
Meadows R, Lawrence JR. Nephropathy
associated with methicillin
administration. Aust N Z J Med
1974;4:256-61
110. Galpin JE, Shinaberger JH,
Stanley TM, et al. Acute interstitial
nephritis due to methicillin. Am J Med
1978;65:756-65
111. Cogan MC, Arieff AI. Sodium wasting,
acidosis and hyperkalemia induced by
methicillin interstitial nephritis. Evidence
for selective distal tubular dysfunction.
Am J Med 1978;64:500-7
112. Yow MD, Taber LH, Barrett FF, et al.
A ten-year assessment of
methicillin-associated side effects.
Pediatrics 1976;58:329-34
113. Baldwin DS, Levine BB,
McCluskey RT, Gallo GR.
Renal failure and interstitial
nephritis due to penicillin and
methicillin. N Engl J Med
1968;279:1245-52
114. Flax MH. Editorial: drug-induced
autoimmunity. N Engl J Med
1974;291:414-15
115. Sanjad SA, Haddad GG, Nassar VH.
Nephropathy, an underestimated
complication of methicillin therapy.
J Pediatr 1974;84:873-7
116. Neu HC. Antistaphylococcal
penicillins. Med Clin North Am
1982;66:51-60
117. Serdaru M, Diquet B, Lhermitte F.
Generalized seizures and ampicillin.
Lancet 1982;2:617-18
118. Schmitt BD, Krivit W. Benign
intracranial hypertension associated
with a delayed penicillin reaction.
Pediatrics 1969;43:50-3
119. Kallay MC, Tabechian H, Riley GR,
Chessin LN. Neurotoxicity due to
ticarcillin in patient with renal failure.
Lancet 1979;1:608-9
120. Malanga CJ, Kokontis L, Mauzy S.
Piperacillin-induced seizures.
Clin Pediatr (Phila) 1997;36:475-8
121. Erikssen J, Midtvedt T, Bergan T.
Treatment of urinary tract infections
with cephalexin. Scand J Infect Dis
1970;2:53-8
122. Saker BM, Musk AW, Haywood EF,
Hurst PE. Reversible toxic psychosis after
cephalexin. Med J Aust 1973;1:497-8
123. Feder HM Jr. Comparative tolerability of
ampicillin, amoxicillin, and
trimethoprim-sulfamethoxazole
suspensions in children with otitis media.
Antimicrob Agents Chemother
1982;21:426-7
124. Gurwith MJ, Rabin HR, Love K.
Diarrhea associated with clindamycin and
ampicillin therapy: preliminary results of
a cooperative study. J Infect Dis
1977;135(Suppl):S104-10
125. Knudsen ET. Amoxil and Talpen.
Br Med J 1977;1:903
126. White AR, Kaye C, Poupard J, et al.
Augmentin (amoxicillin/clavulanate) in
the treatment of community-acquired
respiratory tract infection: a review of the
continuing development of an innovative
antimicrobial agent.
J Antimicrob Chemother
2004;53(Suppl 1):i3-20
127. Bush LM, Johnson CC. Ureidopenicillins
and beta-lactam/beta-lactamase inhibitor
combinations. Infect Dis Clin North Am
2000;14:409-33.ix
128. Neu HC, Wilson AP, Gruneberg RN.
Amoxycillin/clavulanic acid: a review of
its efficacy in over 38,500 patients from
1979 to 1992. J Chemother
1993;5:67-93
129. Scott LJ, Ormrod D, Goa KL.
Cefuroxime axetil: an updated review of
its use in the management of bacterial
infections. Drugs 2001;61:1455-500
130. de Vries-Hospers HG, Tonk RH,
van der Waaij D. Effect of intramuscular
ceftriaxone on aerobic oral and faecal
flora of 11 healthy volunteers. Scand J
Infect Dis 1991;23:625-33
131. Mitropoulos IF, Rotschafer JC,
Rodvold KA. Adverse events associated
with the use of oral cephalosporins/
cephems. Diagn Microbiol Infect Dis
2007;57:67S-76S. General review of adverse events
associated with cephalosporins.
P. Lagace-Wiens & E. Rubinstein
398 Expert Opin. Drug Saf. (2012) 11(3)
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.

132. Bow EJ, Rotstein C, Noskin GA, et al.
A randomized, open-label, multicenter
comparative study of the efficacy and
safety of piperacillin-tazobactam and
cefepime for the empirical treatment of
febrile neutropenic episodes in patients
with hematologic malignancies.
Clin Infect Dis 2006;43:447-59
133. Kuye O, Teal J, DeVries VG, et al.
Safety profile of piperacillin/tazobactam
in phase I and III clinical studies.
J Antimicrob Chemother
1993;31(Suppl A):113-24
134. Voth DE, Ballard JD. Clostridium
difficile toxins: mechanism of action and
role in disease. Clin Microbiol Rev
2005;18:247-63
135. Knoop FC, Owens M, Crocker IC.
Clostridium difficile: clinical disease and
diagnosis. Clin Microbiol Rev
1993;6:251-65
136. Yam FK, Smith KM. "Collateral
damage": antibiotics and the risk of
Clostridium difficile infection.
Orthopedics 2005;28:275-9
137. Loo VG, Poirier L, Miller MA, et al.
A predominantly clonal
multi-institutional outbreak of
Clostridium difficile-associated diarrhea
with high morbidity and mortality.
N Engl J Med 2005;353:2442-9
138. Gerding DN. Clindamycin,
cephalosporins, fluoroquinolones, and
Clostridium difficile-associated diarrhea:
this is an antimicrobial resistance
problem. Clin Infect Dis 2004;38:646-8
139. Isaacs D. Serum sickness-like reaction to
cefaclor. J Paediatr Child Health
2001;37:298-9
140. Levine LR. Quantitative comparison of
adverse reactions to cefaclor vs.
amoxicillin in a surveillance study.
Pediatr Infect Dis 1985;4:358-61
141. Kearns GL, Wheeler JG, Childress SH,
Letzig LG. Serum sickness-like reactions
to cefaclor: role of hepatic metabolism
and individual susceptibility. J Pediatr
1994;125:805-11
142. Boyd IW. Cefaclor-associated serum
sickness. Med J Aust 1998;169:443-4
143. Neu HC. Third generation
cephalosporins: safety profiles after
10 years of clinical use. J Clin Pharmacol
1990;30:396-403
144. Ozturk A, Kaya M, Zeyrek D, et al.
Ultrasonographic findings in ceftriaxone:
associated biliary sludge and
pseudolithiasis in children. Acta Radiol
2005;46:112-16
145. de Moor RA, Egberts AC,
Schroder CH. Ceftriaxone-associated
nephrolithiasis and biliary
pseudolithiasis. Eur J Pediatr
1999;158:975-7
146. Bickford CL, Spencer AP. Biliary sludge
and hyperbilirubinemia associated with
ceftriaxone in an adult: case report and
review of the literature. Pharmacotherapy
2005;25:1389-95
147. Steadman E, Raisch DW, Bennett CL,
et al. Evaluation of a potential clinical
interaction between ceftriaxone and
calcium. Antimicrob Agents Chemother
2010;54:1534-40
148. Qiao HL, Liu JH, Yang J, Dong ZM.
Relationships between skin test, specific
IgE and levels of cytokines in patients
with penicillin allergy. Int J Clin Pract
2005;59:895-9
149. Fontaine C, Mayorga C, Bousquet PJ,
et al. Relevance of the determination of
serum-specific IgE antibodies in the
diagnosis of immediate beta-lactam
allergy. Allergy 2007;62:47-52
150. Rosario NA, Grumach AS. Allergy to
beta-lactams in pediatrics: a practical
approach. J Pediatr (Rio J)
2006;82:S181-8
151. Bryson EO, Frost EA, Rosenblatt MA.
Management of the patient reporting an
allergy to penicillin. Middle East
J Anesthesiol 2007;19:495-512
152. Bougie DW, Wilker PW, Birenbaum JA.
Drug-dependent antibody. What binds
where. J Thromb Haemost
2003;1:abstract OC023
AffiliationPhilippe Lagace-Wiens†1,2 MD FRCPC DTMH
& Ethan Rubinstein3,4 MD LLB†Author for correspondence1Medical Microbiologist, Clinical Microbiology,
Diagnostic Services of Manitoba,
Saint-Boniface Hospital,
Winnipeg, Manitoba, Canada2University of Manitoba,
Faculty of Medicine,
Department of Medical Microbiology and
Infectious Diseases,
L4025-409 Tache Ave. Winnipeg,
Manitoba, R2H 2A6, Canada
Tel: +204 237 2483; Fax: +204 237 7678;
E-mail: [email protected] of Manitoba,
Department of Internal Medicine,
Faculty of Medicine,
Winnipeg, Manitoba, Canada4H.E. Sellers Research Chair in Infectious
Diseases, Head, Section of Infectious Diseases,
University of Manitoba,
Department of Medical Microbiology and
Infectious Diseases,
Faculty of Medicine,
Winnipeg, Manitoba, Canada
Adverse reactions to b-lactam antimicrobials
Expert Opin. Drug Saf. (2012) 11(3) 399
Exp
ert O
pin.
Dru
g Sa
f. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
ealth
Sci
ence
Lea
rnin
g C
tr o
n 09
/12/
12Fo
r pe
rson
al u
se o
nly.