Accessing osteocyte lacunar geometrical properties in human jaw bone on the submicron length scale...
11
Journal of Microscopy, Vol. 255, Issue 3 2014, pp. 158–168 doi: 10.1111/jmi.12147 Received 19 July 2013; accepted 14 May 2014 Accessing osteocyte lacunar geometrical properties in human jaw bone on the submicron length scale using synchrotron radiation μCT BERNHARD HESSE ∗ , ∗∗ , †, NILS M ¨ ANNICKE ∗ , ∗∗ , ALEXANDRA PACUREANU †, ‡,§, PETER VARGA ∗ , MAX LANGER †,§, PETER MAURER , FRANCOISE PEYRIN †, ‡, †† & KAY RAUM ∗ , †† ∗ Berlin-Brandenburg School for Regenerative Therapies and Julius Wolff Institut, Charit´ e-Universit¨ atsmedizin Berlin, Berlin, Germany †European Synchrotron Radiation Facility, Grenoble, France ‡Universit´ e de Lyon, CREATIS, CNRS UMR 5220, Inserm U1044, INSA-Lyon, Universit´ e Lyon 1, Lyon, France §Centre for Image Analysis and Science for Life Laboratory, Uppsala University, Uppsala, Sweden Klinik f ¨ ur Mund-, Kiefer- und Gesichtschirurgie, Klinikum Bremerhaven-Reinkenheide, Bremerhaven, Germany Key words. BRONJ, computed tomography, jaw bone, lacunae, synchrotron radiation. Summary The architectural properties of the osteocyte cell network pro- vide a valuable basis for understanding the mechanisms of bone remodelling, mineral homeostasis, ageing and patholo- gies. Recent advances in synchrotron microtomography en- able unprecedented three-dimensional imaging of both the bone lacunar network and the extracellular matrix. Here, we investigate the three-dimensional morphological properties of osteocyte lacunae in human healthy and bisphosphonate- related osteonecrotic jaw bone based on synchrotron X-ray computed tomography images, with a spatial isotropic voxel size of 300 nm. Bisphosphonate-related osteonecrosis of the jaw is a relatively new disease with increasing incidence, which remains poorly understood. A step forward in eluci- dating this malady is to assess whether, and how, the mor- phology of the osteocyte lacunar network is modified in the affected jaw tissue. We evaluate thousands of cell lacunae from five specimens of which three originate from patients diagnosed with bisphosphonate-associated osteonecrosis. In this exploratory study, we report three-dimensional quantita- tive results on lacunar volumes (296–502 μm 3 ), shape (ap- proximated by an ellipsoidal shape with principal axes a > b > c, such that a = 2.2b and a = 4c) and spatial distribu- tion (i.e., 50% of the mineralized matrix volume is located within 12 μm to the closest lacunar boundary) at submicron resolution on such specimens. We observe that the average ** Bernhard Hesse and Nils M ¨ annicke contributed equally to this work. †† Francoise Peyrin and Kay Raum contributed equally to this work. Correspondence to: Kay Raum, Julius Wolff Institut and Berlin-Brandenburg School for Regenerative Therapies, Charit´ e – Universit¨ atsmedizin Berlin, Augustenburger Platz 1, 13353 Berlin, Germany. Tel: +49 30 450 539 503; fax: +49 (0)30 450 559938; e-mail: [email protected] lacunar volumes of the bisphosphonate-related osteonecrotic jaw specimens were within the range of volumes found in the two specimens originating from healthy donors and conclude that lacunar volumes are not the key element in the course of bisphosphonate-related osteonecrotic jaw. In three out of five specimens we observe lacunar volume sizes in segmented osteons to be significantly different compared to lacunar vol- umes in the adjacent tissue regions. Furthermore, we quantify the number of lacunae containing small dense objects (on av- erage 9%). In contrast to lacunar morphology we report the lacunar density (16 000–50 000 per mm 3 ) to be different in jaw bone tissue compared to what has been reported in femoral sites. Introduction Osteocytes are the most abundant bone cells, embedded in small cavities (lacunae) of the extracellular matrix during the deposition of new tissue in remodelling. They are intercon- nected and communicate via cell processes extending in slen- der tunnels called canaliculi. Lacunae are some hundreds of μm 3 in size, while the diameter of the canaliculi in human bone is in the range of 200–900 nm (Marotti et al., 1995). Osteocytes are believed to play a pivotal role in controlling the resorption and the formation processes of remodelling through osteoclast and osteoblast activity, respectively, driven by biological and mechanical signals (Bonewald, 2011). However, the details of mechanosensation and mechanotransduction processes are not fully understood yet (Wang et al., 1993; Zhou et al., 2009; Schneider et al., 2010; Klein-Nulend et al., 2013). The mor- phology of the lacuno-canalicular network (LCN) plays a cru- cial role in mechanosensation (Knothe Tate, 2003, 2011; C 2014 The Authors Journal of Microscopy C 2014 Royal Microscopical Society
Transcript of Accessing osteocyte lacunar geometrical properties in human jaw bone on the submicron length scale...

Journal of Microscopy, Vol. 255, Issue 3 2014, pp. 158–168 doi: 10.1111/jmi.12147
Received 19 July 2013; accepted 14 May 2014
Accessing osteocyte lacunar geometrical properties in humanjaw bone on the submicron length scale using synchrotronradiation μCT
B E R N H A R D H E S S E ∗, ∗∗,†, N I L S M A N N I C K E ∗, ∗∗, A L E X A N D R A P A C U R E A N U†,‡, §, P E T E R V A R G A ∗,M A X L A N G E R†, §, P E T E R M A U R E R‖, F R A N C O I S E P E Y R I N†,‡,†† & K A Y R A U M ∗,††∗Berlin-Brandenburg School for Regenerative Therapies and Julius Wolff Institut, Charite-Universitatsmedizin Berlin, Berlin, Germany
†European Synchrotron Radiation Facility, Grenoble, France
‡Universite de Lyon, CREATIS, CNRS UMR 5220, Inserm U1044, INSA-Lyon, Universite Lyon 1, Lyon, France
§Centre for Image Analysis and Science for Life Laboratory, Uppsala University, Uppsala, Sweden
‖Klinik fur Mund-, Kiefer- und Gesichtschirurgie, Klinikum Bremerhaven-Reinkenheide, Bremerhaven, Germany
Key words. BRONJ, computed tomography, jaw bone, lacunae, synchrotronradiation.
Summary
The architectural properties of the osteocyte cell network pro-vide a valuable basis for understanding the mechanisms ofbone remodelling, mineral homeostasis, ageing and patholo-gies. Recent advances in synchrotron microtomography en-able unprecedented three-dimensional imaging of both thebone lacunar network and the extracellular matrix. Here, weinvestigate the three-dimensional morphological properties ofosteocyte lacunae in human healthy and bisphosphonate-related osteonecrotic jaw bone based on synchrotron X-raycomputed tomography images, with a spatial isotropic voxelsize of 300 nm. Bisphosphonate-related osteonecrosis of thejaw is a relatively new disease with increasing incidence,which remains poorly understood. A step forward in eluci-dating this malady is to assess whether, and how, the mor-phology of the osteocyte lacunar network is modified in theaffected jaw tissue. We evaluate thousands of cell lacunaefrom five specimens of which three originate from patientsdiagnosed with bisphosphonate-associated osteonecrosis. Inthis exploratory study, we report three-dimensional quantita-tive results on lacunar volumes (296–502 μm3), shape (ap-proximated by an ellipsoidal shape with principal axes a >
b > c, such that a = 2.2b and a = 4c) and spatial distribu-tion (i.e., 50% of the mineralized matrix volume is locatedwithin 12 μm to the closest lacunar boundary) at submicronresolution on such specimens. We observe that the average
**Bernhard Hesse and Nils Mannicke contributed equally to this work.††Francoise Peyrin and Kay Raum contributed equally to this work.Correspondence to: Kay Raum, Julius Wolff Institut and Berlin-Brandenburg School
for Regenerative Therapies, Charite – Universitatsmedizin Berlin, Augustenburger
Platz 1, 13353 Berlin, Germany. Tel: +49 30 450 539 503; fax: +49 (0)30 450
559938; e-mail: [email protected]
lacunar volumes of the bisphosphonate-related osteonecroticjaw specimens were within the range of volumes found in thetwo specimens originating from healthy donors and concludethat lacunar volumes are not the key element in the courseof bisphosphonate-related osteonecrotic jaw. In three out offive specimens we observe lacunar volume sizes in segmentedosteons to be significantly different compared to lacunar vol-umes in the adjacent tissue regions. Furthermore, we quantifythe number of lacunae containing small dense objects (on av-erage 9%). In contrast to lacunar morphology we report thelacunar density (16 000–50 000 per mm3) to be different injaw bone tissue compared to what has been reported in femoralsites.
Introduction
Osteocytes are the most abundant bone cells, embedded insmall cavities (lacunae) of the extracellular matrix during thedeposition of new tissue in remodelling. They are intercon-nected and communicate via cell processes extending in slen-der tunnels called canaliculi. Lacunae are some hundreds ofμm3 in size, while the diameter of the canaliculi in human boneis in the range of 200–900 nm (Marotti et al., 1995). Osteocytesare believed to play a pivotal role in controlling the resorptionand the formation processes of remodelling through osteoclastand osteoblast activity, respectively, driven by biological andmechanical signals (Bonewald, 2011). However, the details ofmechanosensation and mechanotransduction processes arenot fully understood yet (Wang et al., 1993; Zhou et al., 2009;Schneider et al., 2010; Klein-Nulend et al., 2013). The mor-phology of the lacuno-canalicular network (LCN) plays a cru-cial role in mechanosensation (Knothe Tate, 2003, 2011;
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society

L A C U N A R M O R P H O M E T R Y I N J A W B O N E 1 5 9
Anderson & Knothe Tate, 2008) and is related to bone tis-sue quality (Schneider et al., 2010) and has been reported tobe adapted to the anatomical location (Mishra & Knothe Tate,2003; Carter et al., 2013b). Further, given the tight relation-ship between bone diseases and remodelling, the osteocyte isbelieved to have special importance and has gained increas-ing attention recently. LCN morphology has been found tobe altered in various bone diseases (Mullender et al., 1996;Qiu et al., 2003; Mullender et al., 2005; van Hove et al.,2009). The osteocyte is a multifunctional cell: several recentstudies have provided evidence that it regulates phosphatemetabolism (Feng et al., 2013), and that it is directly involvedin the homeostasis metabolism of mineral by actively remod-elling its direct environment as shown in a murine lactatingmodel (Qing et al., 2012). Lacunar volume (Lc.V) has been re-ported to be altered in response to changes of the mechanicalenvironment and drug treatment; specifically, enlarged lacu-nae were observed in mice after space flight (Blaber et al., 2013)or after glucocorticoid treatment (Lane et al., 2006). More-over, both lacunar size and density were found to be altered innewly formed bone after antiresorptive and anabolic pharma-ceutical treatment in ovariectomized rats (Tommasini et al.,2012).
The distribution of osteocytes is thus not only crucial for theproper sensing of mechanical signals across the bone matrix,but also for easy access to mineral reservoirs. Distance of theextracellular tissue to the LCN is therefore of particular im-portance and has recently been demonstrated to be stronglyrelated to the thickness and orientation of mineral particles(Kerschnitzki et al., 2013).
Apoptosis, the process of programmed cell death, of osteo-cytes is believed to have an important role in initiating the re-modelling process (Jilka et al., 2013). In micropetrosis (Frost,1960), the lacuna is filled up with hypermineralized tissue.Appearance of highly mineralized occlusions (pearls) in thelacunae has been proposed to be an intermediate step of thisprocess (Carpentier et al., 2012) and has been observed in ag-ing (Busse et al., 2010) and bone diseases (Carpentier et al.,2012).
The LCN is an extensive, complex three-dimensional (3D)structure with submicrometric elements and is surroundedby the mineralized extracellular matrix. Its investigationhas therefore been limited by the available imaging tech-niques. Among the numerous modalities used towards thisend (reviewed in Webster et al., 2013), X-ray microtomog-raphy (μCT) techniques belong to the most promising ap-proaches and have been used recently to investigate the lacu-nae in healthy and diseased specimens (Vatsa et al., 2008;van Hove et al., 2009; Hannah et al., 2010; Carter et al.,2013a, b). When combined with a synchrotron source (SR-μCT), μCT enables nondestructive 3D imaging of bone tis-sue at submicron resolution and relatively large field of view(Langer et al., 2012; Pacureanu et al., 2012; Varga et al.,2013).
However, most (μCT-based) investigations of the LCN inhuman bone addressed long bones (van Hove et al., 2009;Hannah et al., 2010; Carter et al., 2013b; Dong et al., 2013),which have a regular osteonal structure that is well alignedalong the long axis (Arhatari et al., 2011). In contrast, thejaw bone has a more complex osteonal organization. Bispho-sphonate (BP) related osteonecrosis of the jaw (BRONJ) is asevere and most often irreversible side effect of bisphospho-nate treatment (Lesclous et al., 2009; Ruggiero et al., 2009;Otto et al., 2010; Meiller et al., 2012). Although multiple hy-potheses have been formulated recently, the underlying patho-physiological mechanisms are still not completely understood(Otto et al., 2010). A very recent publication reviewing 671publications concludes that ‘there is still no scientific datato sufficiently support any specific treatment protocol for themanagement of BRONJ’ (Kuhl et al., 2012). Insight into archi-tectural properties of both healthy and diseased tissue is how-ever a prerequisite for better understanding of this pathology.Therefore, the aim of this exploratory study was to accuratelyquantify the geometrical properties, such as size, shape anddistribution of osteocyte lacunae in healthy and BP treatedjaw from high resolution SR-μCT images. Furthermore, weinvestigate for the first time in 3D, small spheroidal hypermin-eralized structures (pearls) located inside the lacunae, whichmight be related to the pathological condition of the tissue.
Materials and methods
Specimen preparation
Five human jaw bone sections (cubes of about 1 mm3 in size)were extracted from three female donors suffering from BRONJ(aged 43, 63 and 76 years) during the treatments necessarydue to the course of the necrosis. Healthy control sampleswere obtained from debris during wisdom tooth removal fromtwo female donors of age 25 and 52. All sections originatedfrom similar anatomical regions, i.e. the proximal body of themandible. All patients signed an informed consent. Ethicalapproval was granted by the Arztekammer Bremen. After re-moval, the bone specimens were placed in tissueTec (SakuraFinetec, USA, Inc., Torrance, CA, USA) and stored frozen at–20°C until further processing. The specimens were selectedfrom a visually nonnecrotic region and cropped in frozen stageusing a cryotome (CM 3050 S, Leica, Germany) until theyreached a size of approximately 0.5 mm in diameter. The cutbone samples where then fixed in 70% ethanol for transportto the imaging site.
SR-μCT
SR-μCT measurements were performed in air at the ID 19experimental station at the European Synchrotron Radia-tion Facility using the settings established by Pacureanu etal. (2012). The energy of the X-ray beam was set to 19.1
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

1 6 0 B . H E S S E E T A L .
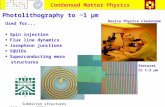
Fig. 1. (A) Virtual slice through the reconstructed 3D attenuation data, colourbar in units of 1 cm–1, scalebar 100 μm. The irregular features visibleinside the HC are likely due to remaining TissueTec or the vessel system. (B) Segmentation of the nonbone area (black), bone area (grey) and lacunae(white).
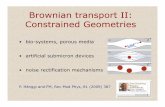
Fig. 2. Subregion from a reconstructed 3D image. (A) A single slice is shown. (B) Maximum intensity projection along z for a z-range of seven slices. (C)Minimum intensity projection along z for a z-range of seven slices. Two lacunae found to contain a pearl are indicated in (A) and (B). The size of eachpanel is 60 × 60 μm2. The colour bar is the same for all three panels.
keV. High flux with sufficiently narrow energy window couldbe achieved by a pink beam mode, using directly the firstharmonic of the undulator radiation. The X-rays were con-verted to visible light by a scintillator. A magnifying visi-ble light optics system and a CCD camera with 2048 pixel× 2048 pixel were used for detection. An effective pixel sizeof 300 × 300 nm2 was selected. Images were reconstructedwith a filtered back projection algorithm. The resulting fieldof view was about 0.6 mm in diameter and 0.6 mm inheight.
Image analysis
Data processing was performed using custom designed tool-boxes and functions written in C++ and Matlab R2009b(The Mathworks Inc., Natick, MA, USA; available on request).For visualization and manual selection of regions of interestthe software ZIBAmira (Zuse Institut Berlin, Berlin, Germany;Stalling D, 2005) was used.
Segmentation
Two binary masks corresponding respectively to the bone andlacunae 3D images were computed for each sample based onthresholding and 3D image processing methods. The thresh-olds were adjusted manually for a set of several subvolumesfrom different samples such that a good match with a visualsegmentation was achieved. Subsequently, the same thresh-old value was used for all samples. Using connected compo-nents analysis calculated with a connectivity of 16, the largestnonbone volume within the image was identified, includingHaversian canals as well as cavities (lacunae and all otherpores, e.g. cracks) connected to the edge of the sample, whileexcluding internal pores. The inverse of this domain was takenas the first mask, which defined the total volume (TV) of thesample. Bone volume (BV) denotes the TV minus the lacunae.
In the second step, the lacunae were segmented within theTV. Morphological operations with a 3D ball-shaped struc-turing element were used to smooth the lacunar shape and
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

L A C U N A R M O R P H O M E T R Y I N J A W B O N E 1 6 1
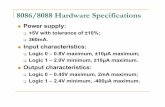
Fig. 3. (A) Minimum intensity projection of the reconstructed attenuation values along a z-range of 100 slices (30 μm). Panel (B) shows one slice of adistance map calculated for the 3D image. (C) Maximum intensity projection along z for 100 slices of the segmented lacunae, the colour code representsthe volume of each lacuna in μm3. (D) Same as (C) but only lacunae containing a pearl are shown. The scale bar represents 300 μm.
to exclude canaliculi connected to the lacunae. The result-ing image was labelled by 3D connected components analysisand was further filtered in order to remove canaliculi or otherkinds of small pores such as cracks (Figs. 1 and 3A). Lc.V wasquantified using the voxel count of the individual connectedcomponents. Objects with volumes larger than 50 μm3, butsmaller than 1400μm3, and with the anisotropy of their shape(defined by the ratios of square-roots of eigenvalues (EV) of thecovariance matrix) being smaller than 10, were defined as la-cunae (Figs. 3 C, D). In order to investigate lacunae propertiesoriginating from osteonal tissue exclusively, one or, if possible,two osteons per sample were segmented manually.
Detection of pearls inside lacunae
For each detected lacuna, the binary lacunar mask was eroded,multiplied by the corresponding raw data and binarized to getthe inner region of each lacuna. The threshold was selectedmanually and kept constant throughout the study. A con-
nected component analysis was performed on each lacunarregion to check whether it contains a dense object. If the size ofa connected component found within the lacunar region ex-ceeded 50 voxels (corresponding to 1.35 μm3) the object wasconsidered as a pearl and the housing lacuna denoted Lcpearl. Amanual verification on 100 randomly selected pearls from var-ious samples and locations was performed and no erroneousautomatic selections were found. Lacunae found to contain apearl are indicated in Figure 2.
Shape based description of lacunae
The shape of lacunae was quantified by eigenvalue analysisof the covariance matrix of each binary lacunar mask. Let,λ1 > λ2 > λ3 be the square-root of the EV and −→u1 ,−→u2,−→u3 bethe corresponding eigenvectors. Therefore −→u1 represents themajor orientation axis of each lacuna. The ratios of the square-root of the EV were used to describe the anisotropy of the lacunashape, namely λ1
λ2, λ1
λ3, λ2
λ3.
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

1 6 2 B . H E S S E E T A L .
Distance of the bone matrix to the lacunae
The distance of the extracellular tissue matrix to the osteocytelacunae was quantified with a Euclidean distance transform.For each voxel characterized as mineralized tissue the short-est distance to the nearest osteocyte lacuna was calculated(Fig. 3B). The histograms of the distance distribution werenormalized to the area under the curves. From the cumulativedistribution function the distances, in which 50% and 95%of the mineralized matrix are located are denoted as Lc.Dist50
and Lc.Dist95, respectively. The median of the distance mapfor elements bigger than zero is equal to Lc.Dist50.
Statistical analysis
Statistical analyses were performed using the Statistics toolboxof MATLAB. For each sample differences of Lc.Vs betweensegmented osteons and the adjacent regions were assessed byunpaired Student’s t-test. Furthermore, difference between theaverage Lc.Vs for each sample and average Lc.Vs of segmentedosteons was assessed by Student’s paired t-test. The low samplenumber did not allow a robust analysis of the effects of BRONJor age. All results were considered statistically significant forp < 0.05.
Results
A cross sectionalμCT image and the corresponding segmentedlacunar areas of a jaw bone sample are shown in Figures 1and 3. A distance map of the segmented lacunae is shown inFigure 3B.
For each sample, the lacunar density (N.Lc/BV), theLc.Dist50, the Lc.Dist95, the mean and standard deviation of theLc.V and the ratio of the square-roots of the EV are presentedin Table 1. All properties are shown separately for lacunaecontaining pearls as well as for lacunae located in osteonaltissue regions. Out of the in total analysed 19 208 lacunaeabout 9% were found to contain a pearl.
The segmented lacunae of osteons from two different donorsare illustrated in Figure 4. The histograms of the lacunae sizesof all samples are plotted in Figure 5. The overall mean sizefor all lacunae was found to be 380 ± 190 μm3. On average,lacunae were found to be flat shaped with the longest axis beingon average 4.1 times longer than the shortest axis, while theratio of the second longest axis is still 1.9 times longer thanthe shortest axis. The mean ratio of the longest to the secondlongest axis was found to be 2.3. The histograms of the ratiosof the square-roots of the EV are shown in Figure 6.
We found that 50% and 95% of the mineralized tissue islocated within less than 12 and 24 μm distance from theclosest lacuna on average, respectively (see Fig. 7).
In each sample, one or if possible two different osteons weresegmented and the Lc.Vs were compared to the adjacent tis-sue regions. The latter could be composed of both osteonal
and interstitial tissue. In three out of five samples we ob-serve significantly smaller Lc.Vs in the segmented osteonalregions (Table 1). Comparing the average Lc.Vs between thewhole samples and the segmented osteonal regions revealedthat osteonal regions contain significantly smaller lacunae(p = 0.01).
Discussion
In this exploratory study, we report geometrical propertiesof osteocyte lacunae in human jaw bone quantified from 3Dimages with submicron resolution by means of synchrotronradiation μCT. This setup allows investigation of several thou-sand lacunae within one field of view and a single tomographicscan. The size and shape measurements of the lacunae in jawbone were found to be in line with those reported for otherhuman bone sites (Hannah et al., 2010; Carter et al., 2013b;Dong et al., 2013).
Although we observe the same trend as reported by oth-ers (Carter et al., 2013a), that is that on average the Lc.Vsdecreased with donor age, statistical testing has not been per-formed due to the small sample number.
We observed that the average sizes of lacunae located insideosteonal tissue were different compared to the overall aver-age lacunar size (osteonal and interstitial tissue confounded),p = 0.01. In addition, for three out of four samples we re-port that the Lc.Vs are significantly smaller in the segmentedosteonal regions compared to Lc.Vs in the adjacent tissue re-gions. It must be noted that the result is hampered by the factthe regions outside the segmented osteonal tissue are in facttissue regions composed of both interstitial tissue and osteonaltissue; hence, the segmented osteonal regions are not nec-essarily the youngest bone tissue regions in each respectivesample.
Moreover, the average values of Lc.Vs of BRONJ specimenswere within in the range of sizes found for the two healthydonors. Although these observations need to be confirmed ina larger sample cohort, we anticipate the lacunar size not tobe a key factor for the development of BRONJ in jaw. However,we found the lacunar density to range from about 16 000 to50 000 per mm3, which is higher than the range reported forthe femoral site (Carter et al., 2013a; Dong et al., 2013). Inter-estingly, the lowest lacunar density was found in the samplefrom the youngest donor (25 years). The density was approx-imately 50% lower than in any of the four other specimens,suggesting either a very high variability within the jaw boneor an age-related effect. The high lacunar density of the jawbone in combination with other factors such as high boneturnover of jaw (Bertoldo et al., 2007) may be of interest forelucidating specific properties of jaw bone tissue that causeBRONJ to exclusively occur in this tissue.
The lacunar shape we report here expressed by the ratioof the square-root of EV is comparable with what has beenreported in other studies for human femoral bone (Carter
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

L A C U N A R M O R P H O M E T R Y I N J A W B O N E 1 6 3
Tab
le1
.Su
mm
ary
ofin
vest
igat
edpr
oper
ties
for
each
bon
esa
mpl
e.N
.Lc
den
otes
the
nu
mbe
rof
lacu
nae
,N.L
c/B
Vth
en
um
ber
ofla
cun
aepe
rbo
ne
volu
me
and
Lc.D
ist 5
0an
dLc
.Dis
t 95
the
dist
ance
toth
ela
cun
aein
wh
ich
50
%an
d9
5%
ofth
ebo
ne
volu
me
are
loca
ted,
resp
ecti
vely
.Lc.
Vde
not
esth
evo
lum
eof
the
lacu
nae
and
λi
stan
dsfo
rei
gen
valu
eio
fth
eco
vari
ance
mat
rix.
Th
esu
bscr
ipt
‘pea
rl’r
efer
sto
lacu
nae
that
wer
efo
un
dto
con
tain
ade
nse
min
eral
ized
obje
ct.T
he
prop
erti
esar
ere
port
edin
depe
nde
ntl
yfo
rla
cun
aeth
atw
ere
loca
ted
inos
teon
alti
ssu
e(O
T)
asw
ella
sfo
rth
ew
hol
esp
ecim
en.L
acu
nar
volu
mes
inse
gmen
ted
oste
onal
regi
onsh
ave
been
com
pare
dto
lacu
nar
volu
mes
inth
ead
jace
ntt
issu
e(n
amel
yth
en
onse
gmen
ted
tiss
ue
regi
ons)
.Sta
tist
ical
lysi
gnifi
can
tdi
ffere
nce
sar
ein
dica
ted
asfo
llow
s:*p
<0
.01
;**p
<0
.00
1.
N.L
c/B
VLc
.Dis
t 50
Lc.D
ist 9
5Lc
.VLc
.Vpe
arl
λ1
/λ2
λ1
/λ2
λ1
/λ3
λ1
/λ3
λ2
/λ3
λ1
/λ2
N.L
cN
.Lc p
earl
in1
mm
–3in
μm
inμ
min
μm
3St
din
μm
3st
dal
lLc
std
Lcpe
arl
std
allL
cst
dLc
pear
lSt
dal
lLc
std
Lcpe
arl
Std
Sam
ple
1k
All
tiss
ue
56
82
96
15
02
00
10
.22
0.9
42
92
20
53
82
33
2.1
0.9
1.9
0.8
3.9
1.6
3.4
1.3
2.0
0.7
1.9
0.6
(BR
ON
J,4
3y.
o.)
OT
65
51
18
47
00
0–
–3
78
**1
86
47
11
97
1.8
0.6
1.6
0.4
3.5
1.2
3.0
1.0
2.0
0.6
2.0
0.6
Sam
ple
2k
All
tiss
ue
50
81
50
94
63
00
10
.12
0.3
34
31
66
42
71
69
2.0
0.8
2.0
0.7
3.7
1.3
3.4
1.1
1.9
0.6
1.8
0.5
(BR
ON
J,7
6y.
o.)
OT
13
59
29
60
0–
–3
15
13
64
19
20
62
.51
.02
.10
.53
.91
.43
.20
.61
.60
.41
.60
.3Sa
mpl
e3
kA
llti
ssu
e2
81
21
24
30
80
01
1.6
21
.93
66
17
54
95
19
22
.00
.81
.70
.44
.01
.54
.11
.12
.10
.72
.50
.7(B
RO
NJ,
63
y.o.
)O
T7
53
43
30
20
0–
–3
37
15
04
75
19
72
.10
.81
.70
.44
.41
.44
.21
.22
.20
.72
.50
.8Sa
mpl
e3
gA
llti
ssu
e2
36
81
71
58
00
14
.62
9.6
50
22
34
67
62
78
3.0
1.2
2.1
0.6
5.0
1.7
3.7
1.2
1.7
0.5
1.8
0.5
(Hea
lth
y,2
5y.
o.)
OT
77
23
13
30
0–
–4
92
*2
29
69
11
39
3.3
1.3
2.7
0.8
5.5
1.7
4.3
1.8
1.7
0.5
1.6
0.3
Sam
ple
5g
All
tiss
ue
32
65
14
23
04
00
12
.82
6.7
29
61
53
42
42
19
2.3
1.0
1.9
0.8
4.1
1.7
3.4
1.5
1.9
0.6
1.7
0.5
(Hea
lth
y,5
2y.
o.)
OT
61
92
73
13
00
––
26
7**
12
03
91
16
32
.20
.91
.80
.44
.11
.53
.21
.02
.00
.61
.90
.5O
vera
llav
erag
eA
llti
ssu
e1
92
08
17
53
34
70
01
1.9
23
.93
83
18
94
95
21
12
.20
.91
.90
.74
.01
.53
.51
.21
.90
.61
.90
.6O
T2
93
42
00
30
28
03
71
17
24
62
19
22
.40
.91
.70
.44
.41
.53
.31
.02
.00
.62
.10
.6
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

1 6 4 B . H E S S E E T A L .
Fig. 4. Lacunae from two different osteons of different samples, projected closely along the osteon long axis and colour coded by lacunar volume. Scale-bar:50 μm.
200 400 600 800 10000
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Lc.V in µm3
P
sample 1ksample 2ksample 3ksample 3gsample 5g
200 400 600 800 10000
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Lc.Vpearl
in µm3
P
sample 1ksample 2ksample 3ksample 3gsample 5g
(B)(A)
Fig. 5. Histograms of lacunar volume for each specimen are shown, considering all lacunae (A) and the lacunae containing a pearl (B). All histogramsare normalized to the absolute volume of all lacunae.
0 5 100
0.05
0.1
0.15
0.2
λ1 / λ
2
P
0 5 100
0.05
0.1
0.15
0.2
λ2 / λ
3
0 5 100
0.05
0.1
0.15
0.2
λ1 / λ
3
sample 1ksample 2ksample 3ksample 3gsample 5g
(A) (B) (C)
Fig. 6. Normalized histograms of the ratios of the different eigenvalues are shown. (A) λ1/λ2, (B) λ2/λ3 and (C) λ1/λ3.
et al., 2013b;), given the assumption that EV (instead of thesquare-root of EV) were used to quantify the anisotropy. More-over, the observed lacunar sizes are in line with a recentstudy from (Dong et al., 2013). However, a precise compari-
son is hampered due to the different resolutions of the imagingtechniques. In this study, we worked with an isotropic voxel-size of 0.3 μm which is several times higher than the voxelsizes used in other studies investigating the 3D morphology of
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

L A C U N A R M O R P H O M E T R Y I N J A W B O N E 1 6 5
0 10 20 300
0.005
0.01
0.015
0.02
0.025
Distance in μm
P
0 5 10 15 20 25 300
0.2
0.4
0.6
0.8
1
Distance in μm
P
(A) (B)
Fig. 7. Histograms of the Euclidean distance transform (A) of the five investigated samples and their corresponding cumulative functions (B). Theallocation of the line-style can be seen in Figure 5.
osteocyte-lacunae (Hannah et al., 2010; Carter et al., 2013b;Dong et al., 2013).
We presented quantitative 3D data on how the bone matrixis located in terms of distance to the lacunar boundaries. Thedistances we found in human jaw were smaller than thosereported for femur (Dong et al., 2013) which is in line with thehigher lacunar density of jaw bone suggesting a higher poten-tial for interaction of the bone matrix with the cell network. Themeasure of Lc.Dist50 and Lc.Dist95 might give a superior de-scription of lacunae-to-matrix relationship compared to otherstandard parameters (such as porosity, density or distance toneighbours), since it combines lacunar density and spatial la-cunar distribution into one parameter. A similar approach wasused to describe changes in the vascular-trabecular interdis-tance in a rat model (Langer et al., 2011) where the authorsreported mean distances of about 20 to 80 μm and to quan-tify the interaction of the lacuno canalicular network and thematrix in ovine study (Kerschnitzki et al., 2013).
Finally, we analysed geometrical properties of lacunae thatcontained dense subcellular objects, denoted pearls. We ob-served that the specimens originating from patients suffer-ing from BRONJ contain a higher percentage of lacunae withpearls (�5–15%) than the healthy specimens (�1–4%). Thissuggests that the formation of such highly calcified structuresmight be related to the disease. Moreover, we observed thetrend that on average, lacunae containing pearls were largercompared to other lacunae. Those differences were observedboth for the whole sample and exclusively osteonal tissue.Nevertheless, it should be noted that during the automaticsegmentation we retained only pearls nonconnected to the la-cunar wall, and we defined minimum sizes for both the pearlsand the lacunae. This means that lacunae containing smallpearls attached to the lacunar wall and lacunae filled withmineral in a high proportion were not accounted for in thisstudy. Due to these segmentation criteria, the probability tosegment a pearl might be higher for larger lacunae and we ex-pect that images acquired at a higher spatial resolution could
reveal an increased incidence of lacunae with such highlymineralized small aggregates. We did not report the size ofthe mineralized object due to the limited spatial resolution andpartial volume effects which could make a small but very denseobject appear bigger. Additionally, it might be possible that infew cases phase artefacts caused by remnants of soft tissueinside the lacunae were falsely identified as pearls. However,we could verify that pearls indeed exist by imaging humancortical bone specimens at a higher resolution (50 nm) usingSR phase-nanoCT. The imaging setup for this technique hasbeen described elsewhere (Langer et al., 2012). In this phase-nanoCT image, pearls were segmented by simple thresholding(Fig. 8) and the cell lacuna with canaliculi was segmentedusing the method from (Pacureanu et al., 2010). Probably thesame kind of dense spherical structures can be seen in the sup-plementary movies in Langer et al. (2012). Moreover, densemineral-bearing vesicles of submicron sizes inside bone form-ing cells have also been reported in context of crystallizationpathways (Mahamid et al., 2011a). Osteoblasts and osteocytescontaining vesicles of about 1 μm diameter have been shownto contain several dense globules of about 80 nm diameter(Mahamid et al., 2011b).
Due to the resolution of the setup used in this study, wecannot resolve those fine structures and it remains unclear towhat extent the reported mineralized objects could be due tothe course of cell apoptosis or necrosis, or may also be affectedby such mineral-containing vesicles.
There are several limitations to this study. The number ofanalysed specimens was not sufficient and differences betweenindividual samples too high to elaborate the effect of BRONJand age. Furthermore, even though each analysed volumecontains several thousand lacunae, this number is relativelysmall compared to the total number of osteocytes in the jawbone, and it is unclear how large a representative volumeshould be for such analyses. In addition, the quantificationof lacunae does not reveal how many of these contained vi-able osteocytes. A further study should explore the diversity
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

1 6 6 B . H E S S E E T A L .
Fig. 8. ‘Pearls’ visualized with a higher resolution imaging technique (SR phase nano CT at 50 nm isotropic voxel-size). (A) Two perpendicular slices of aregion of interest from a reconstructed volume. Black colour corresponds to zero mass density and white colour corresponds to high mass density. In thecentre of the image the osteocyte lacuna is visible, containing several, spheroidal and very dense objects. The volume measures 711 × 900 × 450 (xyz)voxels with 50 nm pixel size. (B) Volume rendering of the lacuna and the canaliculi in (A), with the pearls found inside the lacuna rendered in red colour.
of properties in the human jaw bone in a larger number ofspecimens and at a higher resolution scale.
Nevertheless, we were able to present osteocyte lacunaeproperties in 3D on the submicron length scale including sev-eral thousands of lacunae from five different donors. The 3Ddata sets and the measurements at such high accuracy areunprecedented in human jaw bone. Moreover, the quantifica-tion of lacunae and of the mineralized structures found insidesome of them in healthy and BRONJ affected specimens, forma basis for more extended and in-depth future studies.
Conclusion
Based on five jaw bone samples originating from two healthysubjects and three patients suffering from BRONJ, we reportproperties of lacunae such as average volume (296–502 μm3)and the distribution of the volumes for each specimen, quan-tified by the standard deviation (153–234 μm3). The averageLc.Vs of the BRONJ specimens were within the range of vol-umes found in the two specimens originating from healthydonors. Within the limits of this study we observe that in threeout of five samples Lc.Vs found in segmented osteonal regionsare significantly smaller compared to the adjacent regions.The average shape of a lacuna can be described by one ellip-soid characterized by the axes a > b> c, such that a = 2.2band a = 4c. The lacunar density of jaw bone was found to varybetween 15 800 and 50 200 per mm3. Additionally, we quan-tify the spatial distribution of the lacunae by means of distancetransforms and find that on average 50% of the mineralizedmatrix volume is located within 11.9μm to the closest lacunarboundary. Furthermore, we describe the number density of la-
cunae containing mineralized objects and observe this featureto be highest in the three BRONJ specimens.
Acknowledgements
Authors thank the European Synchrotron Radiation Facilityfor allocated beam time within the experiment md583 andLTP md431 at the beamline ID19 and md672 at the beam-line ID22, the ZUSE Institute for providing ZIBAmira Software.B.H. and N.M. are thankful for being supported by the BSRT.This work has been conducted within the European AssociatedLaboratory ‘Ultrasound Based Assessment of Bone’ and wassupported by the Deutsche Forschungsgesellschaft (SPP1420,grants Ra1380/7 and Ge1894/3). This work was partiallysupported by the LabEX PRIMES (‘Physics Radiobiology Med-ical Imaging and Simulation’) of the Universite de Lyon andfunded by the French Agency Nationale de la Recherche.
Conflict of Interests
All authors state that they have no conflicts of interest.
References
Anderson, E.J. & Knothe Tate, M.L. (2008) Idealization of pericellular fluidspace geometry and dimension results in a profound underpredictionof nano-microscale stresses imparted by fluid drag on osteocytes. J.Biomech. 41, 1736–1746.
Arhatari, B.D., Cooper, D.M., Thomas, C.D., Clement, J.G. & Peele, A.G.(2011) Imaging the 3D structure of secondary osteons in human corti-cal bone using phase-retrieval tomography. Phys. Med. Biol. 56, 5265–5274.
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

L A C U N A R M O R P H O M E T R Y I N J A W B O N E 1 6 7
Bertoldo, F., Santini, D. & Lo Cascio, V. (2007) Bisphosphonates andosteomyelitis of the jaw: a pathogenic puzzle. Nat. Clin. Pract. Oncol. 4,711–721.
Blaber, E.A., Dvorochkin, N., Lee, C., et al. (2013) Microgravity inducespelvic bone loss through osteoclastic activity, osteocytic osteolysis, andosteoblastic cell cycle inhibition by CDKN1a/p21. PLoS One 8, e61372.
Bonewald, L.F. (2011) The amazing osteocyte. J. Bone Miner. Res. 26,229–238.
Busse, B., Djonic, D., Milovanovic, P., Hahn, M., Puschel, K., Ritchie,R.O., Djuric, M. & Amling, M. (2010) Decrease in the osteocyte lacunardensity accompanied by hypermineralized lacunar occlusion revealsfailure and delay of remodeling in aged human bone. Aging Cell 9,1065–1075.
Carpentier, V.T., Wong, J., Yeap, Y., Gan, C., Sutton-Smith, P., Badiei,A., Fazzalari, N.L. & Kuliwaba, J.S. (2012) Increased proportion ofhypermineralized osteocyte lacunae in osteoporotic and osteoarthritichuman trabecular bone: implications for bone remodeling. Bone 50,688–694.
Carter, Y., Thomas, C.D., Clement, J.G. & Cooper, D.M. (2013a) Femoralosteocyte lacunar density, volume and morphology in women acrossthe lifespan. J. Struct. Biol. 183, 519–526.
Carter, Y., Thomas, C.D., Clement, J.G., Peele, A.G., Hannah, K. & Cooper,D.M. (2013b) Variation in osteocyte lacunar morphology and densityin the human femur—a synchrotron radiation micro-CT study. Bone52, 126–132.
Dong, P., Haupert, S., Hesse, B., Langer, M., Gouttenoire, P.-J., Bousson,V. & Peyrin, F. (2013) 3D osteocyte lacunar morphometric propertiesand distributions in human femoral cortical bone using synchrotronradiation micro-CT images. Bone 60, 172–185.
Feng, J.Q., Clinkenbeard, E.L., Yuan, B., White, K.E. & Drezner, M.K.(2013) Osteocyte regulation of phosphate homeostasis and bone min-eralization underlies the pathophysiology of the heritable disorders ofrickets and osteomalacia. Bone 54, 213–221.
Frost, H.M. (1960) Micropetrosis. J. Bone Joint. Surg. Am. 42-A, 144–150.Hannah, K.M., Thomas, C.D., Clement, J.G., De Carlo, F. & Peele, A.G.
(2010) Bimodal distribution of osteocyte lacunar size in the humanfemoral cortex as revealed by micro-CT. Bone 47, 866–871.
Jilka, R.L., Noble, B. & Weinstein, R.S. (2013) Osteocyte apoptosis. Bone54, 264–271.
Kerschnitzki, M., Kollmannsberger, P., Burghammer, M., Duda, G.N.,Weinkamer, R., Wagermaier, W. & Fratzl, P. (2013) Architecture ofthe osteocyte network correlates with bone material quality. J. BoneMiner. Res. 28, 1837–1845.
Klein-Nulend, J., Bakker, A.D., Bacabac, R.G., Vatsa, A. & Weinbaum,S. (2013) Mechanosensation and transduction in osteocytes. Bone 54,182–190.
Knothe Tate, M.L. (2003) “Whither flows the fluid in bone?” An osteo-cyte’s perspective. J. Biomech. 36, 1409–1424.
Knothe Tate, M.L. (2011) Top down and bottom up engineering of bone.J. Biomech. 44, 304–312.
Kuhl, S., Walter, C., Acham, S., Pfeffer, R. & Lambrecht, J.T. (2012)Bisphosphonate-related osteonecrosis of the jaws—a review. Oral Oncol.48, 938–947.
Lane, N.E., Yao, W., Balooch, M., Nalla, R.K., Balooch, G., Habelitz, S.,Kinney, J.H. & Bonewald, L.F. (2006) Glucocorticoid-treated mice havelocalized changes in trabecular bone material properties and osteo-cyte lacunar size that are not observed in placebo-treated or estrogen-deficient mice. J. Bone Miner. Res. 21, 466–476.
Langer, M., Pacureanu, A., Suhonen, H., Grimal, Q., Cloetens, P. & Peyrin,F. (2012) X-ray phase nanotomography resolves the 3D human boneultrastructure. PLoS One 7, e35691.
Langer, M., Prisby, R., Peter, Z., Guignandon, A., Lafage-Proust, M.H. &Peyrin, F. (2011) Simultaneous 3D imaging of bone and vessel mi-crostructure in a rat model. Nuclear Science, IEEE Trans. 58, 139–145.
Lesclous, P., Abi Najm, S., Carrel, J.P., et al. (2009) Bisphosphonate-associated osteonecrosis of the jaw: a key role of inflammation? Bone45, 843–852.
Mahamid, J., Addadi, L. & Weiner, S. (2011a) Crystallization pathways inbone. Cells Tissues Organs 194, 92–97.
Mahamid, J., Sharir, A., Gur, D., Zelzer, E., Addadi, L. & Weiner, S. (2011b)Bone mineralization proceeds through intracellular calcium phosphateloaded vesicles: a cryo-electron microscopy study. J. Struct. Biol. 174,527–535.
Marotti, G., Ferretti, M., Remaggi, F. & Palumbo, C. (1995) Quantita-tive evaluation on osteocyte canalicular density in human secondaryosteons. Bone 16, 125–128.
Meiller, T., Almubarak, H., Weikel, D., Brahim, J. & Scheper, M. (2012)Bisphosphonate-associated osteonecrosis of the jaw: are we dealingwith a localized non-traditional calciphylaxis? Open Dent. J. 6, 5–7.
Mishra, S. & Knothe Tate, M.L. (2003) Effect of lacunocanalicular archi-tecture on hydraulic conductance in bone tissue: implications for bonehealth and evolution. Anat. Rec. A. Discov. Mol. Cell Evol. Biol. 273,752–762.
Mullender, M.G., Tan, S.D., Vico, L., Alexandre, C. & Klein-Nulend, J.(2005) Differences in osteocyte density and bone histomorphometrybetween men and women and between healthy and osteoporotic sub-jects. Calcif. Tissue Int. 77, 291–296.
Mullender, M.G., van der Meer, D.D., Huiskes, R. & Lips, P. (1996) Os-teocyte density changes in aging and osteoporosis. Bone 18, 109–113.
Otto, S., Hafner, S., Mast, G., et al. (2010) Bisphosphonate-related os-teonecrosis of the jaw: is pH the missing part in the pathogenesis puzzle?J. Oral Maxillofac. Surg. 68, 1158–1161.
Pacureanu, A., Langer, M., Boller, E., Tafforeau, P. & Peyrin, F. (2012)Nanoscale imaging of the bone cell network with synchrotron X-raytomography: optimization of acquisition setup. Med. Phys. 39, 2229–2238.
Pacureanu, A., Revol-Muller, C., Rose, J., Ruiz, M.S. & Peyrin, F. (2010)Vesselness-guided variational segmentation of cellular networks from3D micro-CT. In Biomedical Imaging: From Nano to Macro, 2010 IEEEInternational Symposium Rotterdam, The Netherlands.
Qing, H., Ardeshirpour, L., Pajevic, P.D., Dusevich, V., Jahn, K., Kato, S.,Wysolmerski, J. & Bonewald, L.F. (2012) Demonstration of osteocyticperilacunar/canalicular remodeling in mice during lactation. J. BoneMiner. Res. 27, 1018–1029.
Qiu, S., Rao, D.S., Palnitkar, S. & Parfitt, A.M. (2003) Reduced iliac cancel-lous osteocyte density in patients with osteoporotic vertebral fracture.J. Bone Miner. Res. 18, 1657–1663.
Ruggiero, S.L., Dodson, T.B., Assael, L.A., Landesberg, R., Marx, R.E. &Mehrotra, B. (2009) American Association of Oral and MaxillofacialSurgeons position paper on bisphosphonate-related osteonecrosis of thejaws–2009 update. J. Oral Maxillofac. Surg. 67, 2–12.
Schneider, P., Meier, M., Wepf, R. & Muller, R. (2010) Towards quantita-tive 3D imaging of the osteocyte lacuno-canalicular network. Bone 47,848–858.
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168

1 6 8 B . H E S S E E T A L .
Stalling, D.,Westerhoff, M. & Hege, H.-C. (2005) Amira: a highly interac-tive system for visual data analysis. The Visualization Handbook (ed. byH. C. Charles D), 749 pp. Elsevier, Oxford.
Tommasini, S.M., Trinward, A., Acerbo, A.S., De Carlo, F., Miller, L.M. &Judex, S. (2012) Changes in intracortical microporosities induced bypharmaceutical treatment of osteoporosis as detected by high resolutionmicro-CT. Bone 50, 596–604.
van Hove, R.P., Nolte, P.A., Vatsa, A., Semeins, C.M., Salmon, P.L.,Smit, T.H. & Klein-Nulend, J. (2009) Osteocyte morphology in hu-man tibiae of different bone pathologies with different bone min-eral density–is there a role for mechanosensing? Bone 45, 321–329.
Varga, P., Pacureanu, A., Langer, M., et al. (2013) Investigation of the3D orientation of mineralized collagen fibrils in human lamellar bone
using synchrotron X-ray phase nano-tomography. Acta. Biomater. 9,8118–8127.
Vatsa, A., Breuls, R.G., Semeins, C.M., Salmon, P.L., Smit, T.H.& Klein-Nulend, J. (2008) Osteocyte morphology in fibula andcalvaria—is there a role for mechanosensing? Bone 43, 452–458.
Wang, N., Butler, J.P. & Ingber, D.E. (1993) Mechanotransduction acrossthe cell-surface and through the cytoskeleton. Science, 260, 1124–1127.
Webster, D.J., Schneider, P., Dallas, S.L. & Muller, R. (2013) Studyingosteocytes within their environment. Bone 54, 285–295.
Zhou, X., Novotny, J.E. & Wang, L. (2009) Anatomic variations of thelacunar-canalicular system influence solute transport in bone. Bone45, 704–710.
C© 2014 The AuthorsJournal of Microscopy C© 2014 Royal Microscopical Society, 255, 158–168