High Dose Irradiation of Possible FCAL Sensors at the S-DALINAC

(mHs
LABORATORY INVESTIGATION
A Dual-inhibition Study on Vascular Smooth
Muscle Cells with Meclofenamic Acid and
�-irradiation for the Prevention of Restenosis
Alexander Sauter, MD, Alexis Landers, MD, Helmut Dittmann, MD,Maren Pritzkow, BEng, Benjamin Wiesinger, MD, Melanie Bayer, MD,
Rudiger Bantleon, PhD, Jorg Schmehl, MD, Claus D. Claussen, MD, andRainer Kehlbach, PhD
ABSTRACT
PURPOSE: Restenosis is still one of the major limitations after angioplasty. A therapeutic treatment combining �-irradiation andpharmacologic cyclooxygenase-2 inhibition was employed to study the impact on vascular smooth muscle cells (SMCs).
MATERIALS AND METHODS: The effects of meclofenamic acid in combination with yttrium-90 (90Y) on cell growth, clonogenicactivity, cell migration, and cell cycle distribution of human aortic SMCs were investigated. Treatment was sustained over a periodof 4 days and recovery of cells was determined until day 20 after initiation. The hypothesis was that there is no difference betweencontrol and treated groups.
RESULTS: A dose-dependent growth inhibition was observed in single and combined treatment groups for meclofenamic acid and�-irradiation. Cumulative radiation dosage of 8 Gy completely inhibited colony formation. This was also observed for 200 �Mmeclofenamic acid alone or in combination with minor �-irradiation dosages. Results of the migration tests showed also a dosedependency with additive effects of combined therapy. Meclofenamic acid 200 �M alone and with cumulative �-irradiation dosagesresulted in an increased G2/M-phase share.
CONCLUSIONS: Incubating human SMCs with meclofenamic acid and 90Y for a period of 4 d (ie, 1.5 half-life times) resulted inan effective inhibition of smooth muscle cell proliferation, colony formation, and migration.
ABBREVIATIONS
PDGF � platelet-derived growth factor, PTA � percutaneous transluminal angioplasty, SMC � smooth muscle cell
sim3m
ahctpipmdc
Percutaneous transluminal angioplasty (PTA) in combina-tion with stent implantation is a very well establishedmethod for the therapy of atherosclerotic disease in coro-nary and noncoronary arteries, first described by Gruntzigin 1974 (1). It is a safe therapy that improves the quality oflife of patients (2). However, restenosis after angioplasty is
From the Departments of Diagnostic and Interventional Radiology (A.S.,B.W., R.B., J.S., C.D.C., R.K.), Nuclear Medicine (H.D., M.P.), and PediatricsM.B.), Eberhard-Karls-University, WaldhÖrnlestr. 22, 72072 Tubingen, Ger-
any; and Department of Oral and Maxillofacial Surgery (A.L.), Evangelicospital, Hattingen, Germany. Received September 16, 2009; final revi-ion received November 22, 2010; accepted December 4, 2010. Address
correspondence to R.K.; E-mail: [email protected]
None of the authors have identified a conflict of interest.
© SIR, 2011
J Vasc Interv Radiol 2011; 22:623–629
iDOI: 10.1016/j.jvir.2010.12.015
till among the main limitations of this procedure. This isllustrated by recent studies revealing 36-month actuarial pri-ary patency rates of 54.3% in femoropopliteal PTA (3) and
7.6% for PTA only versus 45.3% for PTA with stent place-ent after a 9–24-month follow-up (4).
The mechanisms underlying restenosis are complexnd consist of inflammatory and thrombotic events, intimalyperplasia, and vessel recoil (5). Vascular smooth muscleells (SMCs) are important players in hyperplasia forma-ion (6). Stimulated by vascular injury after PTA or stentlacement, these cells of media origin migrate predom-nantly to the intima (7–9). This process is driven byhysical factors including blood flow, shear stress, andatrix stiffness, as well as promigratory (eg, platelet-
erived growth factor [PDGF]) and antimigratory mole-ules (10 –12).
Two main approaches to reduce restenosis have been
nvestigated. Drug-eluting stents coated with antiprolifera-
eidhn
Brt
mnws
p
mda(8oh3flF0dfoiMMoaatswd
cswe
POatpCd(m
CTcptempAwse
624 � Meclofenamic Acid and �-irradiation for Restenosis Prevention Sauter et al � JVIR
tive pharmaceutical agents like sirolimus or paclitaxel havebeen shown to be associated with good outcomes in coro-nary vessels (13,14). However, the femoropopliteal seg-ment poses limitations for this procedure (15). Currently, apaclitaxel-eluting non–polymer-based stent (Zilver PTX;Cook, Bloomington, Indiana) is undergoing evaluation in amulticenter trial. Preliminary data showed a 94% event-freesurvival rate and a 96% rate of freedom from target lesionrevascularization for the 6-month interim follow-up (16).Although coronary and infrapopliteal vessels are anatomi-cally similar, the infrainguinal vascular beds are geneti-cally and physically diverse. The superficial femoralartery is a long and large vessel that is exposed to axial,longitudinal, and rotational forces. These factors mightinfluence the efficacy of a drug, the dosing, the elutionrates, and stent fracture (15). The second approach in-cludes the use of intravascular brachytherapy (especially�-radiation sources) (17), but limitations like the “edgeffect” may occur (18,19). The lack of studies illuminat-ng the combination of �-irradiation and antiproliferativerugs encouraged us to perform an investigation in auman aortic SMC in vitro model comparing meclofe-amic acid (20) and �-irradiation.
MATERIALS AND METHODS
Cell Culture and IrradiationHuman aortic SMCs (ATCC, Rockville, Maryland) werecultured in a 1:1 ratio of Waymouth MB 752/1 and HamF12 media (Invitrogen, Karlsruhe, Germany). The culturemedium was supplemented with 20% fetal calf serum (In-vitrogen) as well as 100 IU/mL penicillin and 100 �g/mLstreptomycin. Only cells from passages 19 or 20 were usedthroughout the experiments. The passage number describesthe overall culturing period of cells with approximately twopopulation doublings per passage. The cells used in ourexperiments grow stably until approximately passage 30before senescence begins. The cells were characterized with�-actin (monoclonal mouse antihuman smooth muscle ac-tin; DAKO, Hamburg, Germany), a specific cytoskeletalmarker for SMCs. Except when administering the radionu-clide and when performing the different assays, cells werekept in standard air incubators (Thermo Fisher Scientific,Dreieich, Germany) at 37°C, 5% CO2, and humidity greaterthan 95%. After incubation with yttrium-90 (90Y, CIS Bio,
erlin, Germany), the irradiated cells were kept in a sepa-ate incubator, maintaining the same environmental condi-ions.
Meclofenamic acid (Sigma-Aldrich, Munich, Ger-any), a nonsteroidal antiinflammatory drug, is an anthra-
ilic acid derivate that inhibits the cyclooxygenase path-ay (21) with additional vasodilative effects (22,23). A
tock solution of 10�2 M was kept at �20°C and finalconcentrations of 10 �M, 25 �M, 50 �M, 100 �M, and200 �M in culture medium were added for the incubation
eriod of 4 d. c
Yttrium-90 (�max, 2.28 MeV; half-life, 64.1 h; maxi-um tissue range, 11 mm; mean tissue range, 2.5 mm),
elivered as solution in 0.04 M HCl, was filtered sterilend applied to the cells. The effects of different dosesdoses administered over a period of 4 d: 2 Gy, 4 Gy, and
Gy) alone or in combination with meclofenamic acidn human aortic SMC growth were examined. In detail,uman aortic SMCs were plated (day �2) with a density of0,000 cells in 6.7 mL culture medium in 25-cm2 cultureasks with ventilated caps (Falcon; Becton Dickinson,ranklin Lakes, New Jersey). Two days after plating (day), culture medium was replaced by 90Y-containing me-ium for the irradiation groups and nonradioactive mediumor the control and meclofenamic acid groups. The amountf radioactivity needed to achieve the intended cumulativerradiation dose within 4 d was calculated analogous to the
edical Internal Radiation Dose Committee concept withIRDOSE version 3.1 software (24). This concept was
riginally developed for organ dose calculations, so somedjustments to the in vitro conditions had to be made. It wasssumed that the irradiation dose to a monolayer cell cul-ure adherent at the bottom of the culture flask is 50% of theelf-dose in the supernatant (2.67-mm thickness). The latteras derived from the ratio of the 2.67-mm spheroid self-ose and the maximum self-dose.
After 4 d (ie, day 4) culture medium was removed,ells were washed twice by rinsing with phosphate-bufferedaline solution (Invitrogen), and nonradioactive mediumas applied. Further culture medium change was conducted
very 4 d.
roliferation Kineticsn days 4, 8, 12, 16, and 20 after initial “pharmaceutical”
nd/or radionuclide exposure, cells were harvested byrypsinization (trypsin–ethylene diamine tetraacetic acid/hosphate-buffered saline solution 0.05%/0.02%; Promo-ell, Heidelberg, Germany). The absolute cell number wasetermined with the use of an electronic cell counterCoulter Counter Z1; Beckmann Coulter, Krefeld, Ger-any).
lonogenic Activityhe clonogenic activity of the cells was determined witholony formation assays on days 4, 12, and 20 after initialharmacon and/or radionuclide exposure. The differentime points have been chosen to investigate whether recov-ry occurred. Cells were seeded at 500 cells/well in 2 mLedium in six-well plates (Falcon; Becton Dickinson). The
lates were incubated at 37°C in a 5% CO2 atmosphere.fter 10 d, the assays were stopped and the cells were fixedith 3.5% formaldehyde and 70% ethanol and subsequently
tained with Coomassie blue. The total number of coloniesxceeding 50 cells per colony was counted by light micros-
opy (Zeiss, Gottingen, Germany).
mhmtomR
c1D
SDhusdsI
R
CPehcndd(1tdnsc1l1sa
a enden
Volume 22 � Number 5 � May � 2011 625
Migration AssayThe migratory ability of human aortic SMCs was investi-gated in a 24-well compound chamber (Falcon; BectonDickinson) with 8 �M pore membrane inserts after the 4-dtreatment period. Cells were washed, trypsinized, and fi-nally seeded at a density of 310,000 cells/mL in the mem-brane inserts with 0.5 mL cell culture medium containing20% fetal calf serum. Medium (0.8 mL) containing 20%fetal calf serum was added to the lower compartment ofthe plate. One group was additionally stimulated with 25ng/mL PDGF-BB (R&D Systems, Wiesbaden, Germany)as a chemoattractant in the lower compartment to imitatethe stimulation of cells after PTA, whereas the othergroup received no PDGF. After incubating the plates for4 h at 37°C in a humidified 5% CO2 atmosphere, the
embrane inserts were fixed (ethanol 70%, formalde-yde 3.5%, 10 min respectively) and stained with Coo-assie blue after mechanically removing the cells at-
ached to the upper surface. The cells on the lower sidesf the inserts were counted with the use of a lighticroscope (magnification �100; Zeiss) and a Fuchs–osenthal counting chamber.
Cell Cycle AnalysisCell cycle distribution was analyzed by using a flow cy-tometer (FACSort; Becton Dickinson) and combined label-ing with bromodeoxyuridine and propidium iodide. Ondays 4, 12, and 20 after the beginning of the treatment, 20�M bromodeoxyuridine solution was added to the culturesfor 60 min. Cells were then washed with phosphate-suf-fered saline solution, harvested by trypsinization, and re-suspended in 70% ethanol for storage. For analysis, cellswere incubated with a murine antibromodeoxyuridine anti-body (Becton Dickinson) as primary antibody and a fluo-rescein isothiocyanate–labeled rabbit antimouse antibody(DAKO) as secondary antibody. The total amount of DNA
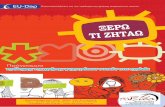
Figure 1. Proliferation kinetics of human aortic SMCs with meccid treatment (b). Values shown are means � SD of three indep
was stained with propidium iodide. Distribution pattern of p
ells in the different cell cycle phases were examined for04 events by using the CellQuest Pro program (Bectonickinson).
tatistical Analysisata are expressed as means � SD or means � SEM. Theypothesis was that there is no difference between thentreated control group and the treated group. Statisticalignificance was assessed with analysis of variance, andifferences were considered significant at P � .05. Fortatistical analysis, SigmaPlot 11 software (Systat, Chicago,llinois) was used.
ESULTS
ell Proliferationroliferation kinetics were assessed over a period of 20 d tovaluate the long-term effects on mitogenic activity ofuman aortic SMCs under different treatments. For betteromparability of the multiple approaches, absolute cellumbers were related to the corresponding control group onay 20. The control group showed a steady increase fromay 0 (absolute cell number, 60,530 � 6,710) to day 20absolute cell number, 1,325,100 � 85,230). Between day2 and day 20, a plateau phase was reached. Single-agentreatment with meclofenamic acid presented a dose-depen-ent effect (Fig 1a). Groups treated with 10 �M meclofe-amic acid showed only a slight growth reduction (notignificant; P � .05) compared with their correspondingontrols. On day 20, these cells (absolute cell number,,379,470 � 15,590) slightly exceeded the control (abso-ute cell number, 1,325,100 � 85,230). On days 8, 12, and6, treatment with 25 �M meclofenamic acid showed aignificant difference (P �.05). Concentrations of 50 �Mnd 100 �M meclofenamic acid resulted in a stronger
mic acid treatment alone (a) or �-irradiation and meclofenamict experiments. *P � .05 versus control by analysis of variance.
lofena
roliferative suppression. At the highest concentration (200

�cgsdtnrpmilGmdralrtta
CCfng1g(T�crctb
MCcim2�tcwcmsnab
trol by analysis of variance.
626 � Meclofenamic Acid and �-irradiation for Restenosis Prevention Sauter et al � JVIR
M), a cytostatic effect with no further proliferation oc-urred. Cells in the irradiated groups (2 Gy, 4 Gy, 8 Gy)rew more slowly than controls (Fig 1b). The 2-Gy grouphows a sigmoid curve and approximates the controls onay 20 (not significant; P � .05). Regarding the combina-ion with meclofenamic acid, the 2 Gy and 50 �M meclofe-amic acid groups showed a delayed exponential growthate without reaching a plateau within the examinationeriod. The combination of 2 Gy �-irradiation and 50 �Meclofenamic acid resulted in a supraadditive effect. Add-
ng higher meclofenamic acid concentrations led to nearlyinear growth with the greatest supraadditive effect in the 2y, 100 �M meclofenamic acid groups. The 2 Gy, 200 �Meclofenamic acid groups were entirely suppressed. On
ay 20, the absolute cell numbers in the 4-Gy groupseached only 20% of control. Nevertheless, meclofenamiccid caused additional suppressive effects, illustrated byower proliferation in the combined groups. With increasingadiation dosages to 8 Gy, the absolute cell numbers inhese groups were only 12% of the controls. Consequently,he additional impact of meclofenamic acid is low and nodditive effects can be expected (data not shown).
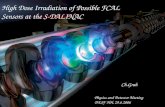
lonogenic Activityolony-forming assays are presented in dose-dependent
ashion as logarithmic surviving fractions (treated colonyumbers divided by control colony numbers). Radiatedroups in combination with 50 �M meclofenamic acid and00 �M meclofenamic acid are shown. On day 4, all treatedroups showed a significant (P � .05) dose dependencyFig 2a). No colonies are found beyond a threshold of 4 Gy.he ability for colony formation was lost at 4 Gy and 100M meclofenamic acid. Figure 2b reveals an exerted re-overing effect and a flatter curve after 12 d. For day 20, theegenerative potential of the cells is seen in Figure 2c, asolonies (without meclofenamic acid treatment) are de-ected beyond 8 Gy and curves are less steep than 8 defore.
igratory Activityell migration with and without PDGF stimulation de-reased with increasing doses of meclofenamic acid andrradiation (Fig 3). Regarding the stimulated group, treat-ent with 200 �M meclofenamic acid, 2 Gy �-irradiation/
00 �M meclofenamic acid, 4 Gy �-irradiation, 4 Gy-irradiation/200 �M meclofenamic acid, 8 Gy �-irradia-
ion, and 8 Gy �-irradiation/200 �M meclofenamic acidould reduce migration significantly (P � .05) comparedith controls. Regarding possible synergistic effects of the
ombination therapy, only the 2 Gy �-irradiation/200 �Meclofenamic acid disclosed an additive effect. The other
timulated groups revealed only infraadditive effects. In theonstimulated groups, 2 Gy/200 �M, 4 Gy/200 �M, 8 Gy,nd 8 Gy/200 �M were significantly (P � .05) different,
Figure 2. For colony formation assays, cells were seeded (a)
directly after the 4-day treatment period, (b) at day 12, or (c) atday 20 after initiation. Surviving fractions of human aortic SMCcolonies after irradiation or combined treatment were calcu-lated on the basis of colony counts and plating efficiency. Nocolonies could be detected under 200 �M treatment. Data barsrepresent the mean surviving fraction � SEM of 18 parallel datasets from three independent experiments. *P � .05 versus con-
ut effects were only infraadditive.

Micp
i2irgc
sAdabhacSfaptMae
erbmrc
abfmiitiFallrsde1
a�psoSapTto
aaa
Volume 22 � Number 5 � May � 2011 627
Cell Cycle AnalysisRepresentative dot plots of the cell cycle analysis on day 4after initial treatment of the control (Fig 4a) and the 200�M
eclofenamic acid group (Fig 4b) are shown. The signif-cant (P � .05) diminishing S-phase portions on d 4 areoncordant with the decreased cell counts seen in theroliferation kinetic. An exception is the 50 �M
meclofenamic acid group. On d 20, especially the 4-Gygroups showed a higher but not significant (P �.05)amount of S-phase cells as the control, revealing theregenerative capacity of SMCs. Directly after the end ofthe treatment, G2/M phase is elevated in the 8 Gy and/or200 �M meclofenamic acid groups, leading to a signif-cant (P � .05) long-lasting G2/M phase arrest for the00 �M and 4 Gy/200 �M treatment assays. Correspond-ng to these data, G1 phase portions of these cells areeduced (Fig 4c,4d). The low-dose meclofenamic acidroups are not significantly different (P � .05) fromontrol (data not shown).
DISCUSSION
The mechanisms underlying restenosis formation after an-gioplasty are considered to be complex (5). As a result ofvascular damage and a consequent release of promigratoryfactors (eg, PDGF), vascular SMCs migrate and proliferatetoward the intima, causing a narrowing of the vessel lumen.The high degree of plasticity and the absence of a terminaldifferentiation of the vascular SMCs also contribute to thedevelopment and progression of other vascular diseasessuch as atherosclerosis, cancer, and hypertension (6–12). Inrecent years, two main approaches have been attempted toreduce restenosis.
Several pharmacologic studies (25–31) were per-formed to evaluate systemic and local (eg, drug-eluting
Figure 3. The number of migrated cells decreased under in-creasing treatment doses, revealing a more sensitive responseunder PDGF-BB stimulation. Values shown are means � SD ofsix membranes from three independent experiments. *P � .05versus control by analysis of variance.
stents) therapies. Mitotic inhibitors like paclitaxel have c
hown to be beneficial in vivo (25) and in vitro (26).nother promising group of inhibitors are anthranilic aciderivates, including tranilast (27–29) and meclofenamiccid (20). In clinical practice, meclofenamic acid haseen used as a nonsteroidal antiinflammatory agent in-ibiting the cyclooxygenase-2 pathway (30). Schober etl (20) showed meclofenamic acid reduces proliferation,lonogenic activity, and migration of human aorticMCs in a dose-dependent manner. Antiproliferative ef-ects are caused by a combination of a G2/M phase blocknd a downregulation of the p44/42 mitogen-activatedrotein kinase. As described for tranilast, antiprolifera-ive effects such as inhibition of interleukin-1�–induced
CP-1 production and other chemokine inhibitions arelso likely for meclofenamic acid (31). In addition, toxicffects could be ruled out (20).
The good outcome in patients treated with sirolimus-luting stents in coronary vessels is not applicable in pe-ipheral vessels like the superior femoral artery. There is noenefit to the use of sirolimus-eluting stents versus bareetal stents (32). Promising are new developments with
efined drug application and absorption points for drug-oated balloons and bioabsorbable stents (16,25).
Intravascular brachytherapy is the second approachgainst restenosis formation (17). In coronary vessels, Sil-er et al (33) showed a clinical benefit after a 2-yearollow-up with �-irradiation compared with placebo treat-ent. This was also demonstrated in diabetic patients, but
ts association with a frequent occurrence of late thrombosiss a major limitation (34). Other disadvantages of brachy-herapy consist of the edge effect (18,19) and unintentionalrradiation caused by the �-component of some radiators.or phosphorus P 32, the edge effect can be explained withhalf-life of 14.3 d and a �max of 1.71 MeV. This long-
asting irradiation with low energies causes growth stimu-ation on the edges. However, proliferation at the edgeegion also occurs at minor rates without irradiation inirolimus-eluting stent therapy (35) or is caused by the stentesign of bare metal stents (36). A radiator with a reduceddge effect is 188Re (half-life, 16.9 h; �max, 2.12 MeV), but88Re has the aforementioned �-component. Yttrium-90 aspure �-source (half-life, 64.1 h; �max, 2.28 MeV) has no-component and therefore has advantages in clinical ap-lication. Besides the radiator, it is also important to con-ider stent geometry. Pure �-radiators, for example, seemnly to be recommended in cases of thin-strut stents (37). Ineptember 2008, two companies (ITM, Munich, Germany;nd FlowMedical, Garching, Germany) received a Euro-ean approval for intravascular brachytherapy with 188Rh.his is promising for the development of new techniques in
his field, not only for the vasculature but also for treatmentf refractory bronchial strictures (38).
The advantages and disadvantages of the two differentpproaches have encouraged us to investigate the effects ofcombined therapy with meclofenamic acid and �-irradi-
tion on human aortic SMCs, resulting in an effective
ontrol of human aortic SMC proliferation and migration in
rp
bt
R
o
628 � Meclofenamic Acid and �-irradiation for Restenosis Prevention Sauter et al � JVIR
vitro. A combination of 4 Gy �-irradiation with 100 �Mmeclofenamic acid attains encouraging benefits for reduc-ing SMC-induced restenotic processes.
The present results reflect the effects on monoculturesof human aortic SMCs. As intimal hyperplasia is a multi-cellular event, the present study is only an incomplete invitro representation of these processes. The effects on othercell types like endothelial cells have to be examined and invivo experiments in animals should be carried out to inves-tigate efficiency, side effects, and outcomes of the treatmentschemata. An in vivo experiment would also consider thecomplex differentiation pathway of vascular SMCs andtheir heterogeneous origin (39).
Combined treatment with meclofenamic acid and �-ir-adiation has clear synergistic effects in the inhibition of
Figure 4. Representative dot plots of cell cycle analysis on d 4groups. Green represents cells in G1 phase, blue in S phase, andd 4 (c) and d 20 (d) after initial treatment. Data shown are means
f variance.
roliferation and migration of human aortic SMCs. We
elieve that such a treatment might be useful in overcominghe disadvantages of each stand-alone approach.
EFERENCES
1. Meier B, Bachmann D, Luscher T. 25 years of coronary angioplasty:almost a fairy tale. Lancet 2003; 361:527.
2. Keeling AN, Naughton PA, O’Connell A, Lee MJ. Does percutaneoustransluminal angioplasty improve quality of life? J Vasc Interv Radiol2008; 19:169–176.
3. Conrad MF, Cambria RP, Stone DH, et al. Intermediate results ofpercutaneous endovascular therapy of femoropopliteal occlusive dis-ease: a contemporary series. J Vasc Surg 2006; 44:762–769.
4. Kasapis C, Henke PK, Chetcuti SJ, et al. Routine stent implantation vs.percutaneous transluminal angioplasty in femoropopliteal artery disease:a meta-analysis of randomized controlled trials. Eur Heart J 2008; 30:
itial treatment in control (a) and 200 �M meclofenamic acid (b)
G2/M phase. Summarized data for the different treatments one independent experiments. *P � .05 versus control by analysis
after inred in
of thre
44–55.

1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
Volume 22 � Number 5 � May � 2011 629
5. Dangas G, Fuster V. Management of restenosis after coronary inter-vention. Am Heart J 1996; 132:428–436.
6. Gerthoffer WT. Mechanisms of vascular smooth muscle cell migration.Circ Res 2007; 100:607–621.
7. Murry CE, Gipaya CT, Bartosek T, Benditt EP, Schwartz SM.Monoclonality of smooth muscle cells in human atherosclerosis. Am JPathol 1997; 151:697–705.
8. Clowes AW, Clowes MM, Fingerle J, Reidy MA. Regulation of smoothmuscle cell growth in injured artery. J Cardiovasc Pharmacol 1989;14(Suppl 6):S12–S15.
9. Reidy MA, Fingerle J, Lindner V. Factors controlling the developmentof arterial lesions after injury. Circulation 1992; 86:III43–III46.
10. Li C, Wernig F, Leitges M, Hu Y, Xu Q. Mechanical stress-activatedPKCdelta regulates smooth muscle cell migration. FASEB J 2003; 17:2106–2108.
1. Peyton SR, Putnam AJ. Extracellular matrix rigidity governs smoothmuscle cell motility in a biphasic fashion. J Cell Physiol 2005; 204:198–209.
2. Ward MR, Tsao PS, Agrotis A, Dilley RJ, Jennings GL, Bobik A. Lowblood flow after angioplasty augments mechanisms of restenosis: in-ward vessel remodeling, cell migration, and activity of genes regulatingmigration. Arterioscler Thromb Vasc Biol 2001; 21:208–213.
3. Pendyala L, Jabara R, Shinke T, et al. Drug-eluting stents: present andfuture. Cardiovasc Hematol Agents Med Chem 2008; 6:105–115.
4. Kumbhani DJ, Bavry AA, Kamdar AR, Helton TJ, Bhatt DL. The effectof drug-eluting stents on intermediate angiographic and clinical out-comes in diabetic patients: insights from randomized clinical trials. AmHeart J 2008; 155:640–647.
5. Tepe G. Drug-eluting stents for infrainguinal occlusive disease: prog-ress and challenges. Semin Vasc Surg 2006; 19:102–108.
6. Ansel GM, Lumsden AB. Evolving modalities for femoropopliteal inter-ventions. J Endovasc Ther 2009; 16:II82–III97.
7. Waksman R, Cheneau E, Ajani AE, et al. Intracoronary radiation therapyimproves the clinical and angiographic outcomes of diffuse in-stent re-stenotic lesions: results of the Washington Radiation for In-Stent Reste-nosis Trial for Long Lesions (Long WRIST) Studies. Circulation 2003;107:1744–1749.
8. Voisard R, Hob J, Baur R, Herter T, Hannekum A, Hombach V. Edgerestenosis: impact of low dose irradiation on cell proliferation and ICAM-1expression. BMC Cardiovasc Disord 2006; 6:32.
9. Albiero R, Nishida T, Adamian M, et al. Edge restenosis after implan-tation of high activity (32)P radioactive beta-emitting stents. Circulation2000; 101:2454–2457.
0. Schober W, Kehlbach R, Gebert R, et al. Meclofenamic acid for inhibi-tion of human vascular smooth muscle cell proliferation and migration: anin vitro study. Cardiovasc Intervent Radiol 2002; 25:57–63.
1. Matsell DG, Gaber LW, Malik KU. Cytokine stimulation of prostaglan-din production inhibits the proliferation of serum-stimulated mesangialcells. Kidney Int 1994; 45:159–165.
2. Yeung SY, Pucovsky V, Moffatt JD, et al. Molecular expression and
pharmacological identification of a role for K(v)7 channels in murinevascular reactivity. Br J Pharmacol 2007; 151:758–770.3
3. Garcia-Villalon AL, Amezquita YM, Monge L, Fernandez N, Salcedo A,Dieguez G. Endothelin-1 potentiation of coronary artery contractionafter ischemia-reperfusion. Vascul Pharmacol 2008; 48:109–114.
4. Stabin MG. MIRDOSE: personal computer software for internal doseassessment in nuclear medicine. J Nucl Med 1996; 37:538–546.
5. Tepe G, Zeller T, Albrecht T, et al. Local delivery of paclitaxel to inhibitrestenosis during angioplasty of the leg. N Engl J Med 2008; 358:689–699.
6. Wiskirchen J, Schober W, Schart N, et al. The effects of paclitaxel on thethree phases of restenosis: smooth muscle cell proliferation, migration, andmatrix formation: an in vitro study. Invest Radiol 2004; 39:565–571.
7. Fukuyama J, Ichikawa K, Hamano S, Shibata N. Tranilast suppressesthe vascular intimal hyperplasia after balloon injury in rabbits fed on ahigh-cholesterol diet. Eur J Pharmacol 1996; 318:327–332.
8. Fukuyama J, Ichikawa K, Miyazawa K, Hamano S, Shibata N, Ujiie A.Tranilast suppresses intimal hyperplasia in the balloon injury model andcuff treatment model in rabbits. Jpn J Pharmacol 1996; 70:321–327.
9. Karakayali F, Haberal N, Tufan H, et al. Evaluation of neointimal hyper-plasia on tranilast-coated synthetic vascular grafts: an experimentalstudy. J Invest Surg 2007; 20:167–173.
0. Epstein SE, Speir E, Unger EF, Guzman RJ, Finkel T. The basis ofmolecular strategies for treating coronary restenosis after angioplasty.J Am Coll Cardiol 1994; 23:1278–1288.
1. Chikaraishi A, Hirahashi J, Takase O, et al. Tranilast inhibits interleukin-1beta-induced monocyte chemoattractant protein-1 expression in ratmesangial cells. Eur J Pharmacol 2001; 427:151–158.
2. Duda SH, Bosiers M, Lammer J, et al. Drug-eluting and bare nitinolstents for the treatment of atherosclerotic lesions in the superficialfemoral artery: long-term results from the SIROCCO trial. J EndovascTher 2006; 13:701–710.
3. Silber S, Popma JJ, Suntharalingam M, et al. Two-year clinical fol-low-up of 90Sr/90 Y beta-radiation versus placebo control for the treat-ment of in-stent restenosis. Am Heart J 2005; 149:689–694.
4. Syeda B, Schukro C, Kirisits C, et al. Randomized blinded clinical trial ofintracoronary brachytherapy with 90Sr/Y beta-radiation for the preventionof restenosis after stent implantation in native coronary arteries in dia-betic patients. Radiother Oncol 2006; 78:60–66.
5. Sakurai R, Ako J, Morino Y, et al. Predictors of edge stenosis followingsirolimus-eluting stent deployment (a quantitative intravascular ultra-sound analysis from the SIRIUS trial). Am J Cardiol 2005; 96:1251–1253.
6. Yazdani SK, Berry JL. Development of an in vitro system to assessstent-induced smooth muscle cell proliferation: a feasibility study. J VascInterv Radiol 2009; 20:101–106.
7. Wilczek K, Petelenz B, Strzala A, Marczewska B, Traczyk M, Polonski L.Dose perturbation caused by stents: experiments with a model 90Sr/90Ysource. Cardiovasc Intervent Radiol 2007; 30:981–991.
8. Kim JH, Shin JH, Song HY, et al. Liquid (188)Re-filled balloon dilationfor the treatment of refractory benign airway strictures: preliminary ex-perience. J Vasc Interv Radiol 2008; 19:406–411.
9. Dennis JE, Charbord P. Origin and differentiation of human and murinestroma. Stem Cells 2002; 20:205–214.


![I]Iodine- -CIT · COSTIS (Compact Solid Target Irradiation System) solid target holder. COSTIS is designed for irradiation of solid materials. IBA Cyclotron COSTIS Solid Target ...](https://static.fdocument.org/doc/165x107/5e3b25610b68cc381f725e57/iiodine-costis-compact-solid-target-irradiation-system-solid-target-holder.jpg)