α2-macroglobulin expression in neuritic-type plaques in patients with Alzheimer's disease
5
Neurobiology of Aging, Vol. 14, pp. 233-237, 1993 0197-4580/93 $6.00 + .00 Printed in the U.S.A. All rights reserved. Copyright © 1993 Pergamon Press Ltd. oL2-Macroglobulin Expression in Neuritic-Type Plaques in Patients With Alzheimer's Disease DOMINIQUE VAN GOOL*, BART DE STROOPERt, FRED VAN LEUVENt, ERIK TRIAU$ AND RENE DOM *1 Departments of *Neuropathology, and ~Human Genetics University Hospital, Gasthuisberg, Leuven, Belgium -~Psychogeriatric Nursing Home "De Wingerd", Leuven, Belgium Received 9 July 1992; Accepted 8 January 1993 VAN GOOL, D., B. DE STROOPER, F. VAN LEUVEN, E. TRIAU AND R. DOM. ct2-Macroglobulinexpressionin neuritic-type plaques in patients with Alzheimer'sdisease, NEUROBIOL AGING 14(3) 233-237, 1993.--Because it has been suggested that et2M could be involved in the generation of amyloid peptide, attention was given to a possible association of t~2M expression and amyloid accumulation in the brain. Therefore, we investigated the presence of the proteinase inhibitor a2-macroglobulin (ct2M) in the cerebra of 4 patients with Alzheimer's Disease (AD). One case of a patient with Down's syndrome, 2 cases of patients with Dementia of the Lewy Body type (DLB), 1 case of an aged, clinically nondemented person who displayed many amyloid plaques, and 3 normal aged control brains were also studied. The results obtained by immunocytochemistry with monoclonal antibodies directed against two different epitopes of human ot2M showed an association of ~t2M, only with neuritic-type plaques in patients with AD. No ~x2M immunoreactivity was found in either preamyloid-type plaques or burned out-type plaques in AD, DLB, or aged nondemented controls. The results do not support a direct role of this proteinase inhibitor in the formation of amyloid. Because tx2M is observed to be associated with reactive microglia in the outer border of the neuritic plaques, the data suggest that et2M could be a marker for an inflammatory cellular process in these neuritic plaques. Neuropathology et2-macroglobulin Dementia lmmunocytochemistry Alzheimer's Lewy Body disease SEVERAL lines of evidence suggest a possible imbalance be- tween proteinases and proteinase inhibitors as a primary phenom- enon in Alzheimer's Disease (AD) (12). The neurofibrillary tan- gles strongly react with antibodies to ubiquitin (23). This peptide marks proteins for intracellular ATP-dependent proteolysis (21). The amyloid plaques, on the other hand, contain proteinases such as cathepsin B and D (6) and proteinase inhibitors like protease nexin 1 (22) and ot 1-antichymotrypsin (I). Moreover, the amyloid peptide 13A4, the main component of the amyloid plaques and the congophilic angiopathy, is derived from the amyloid precursor protein (APP) by an unknown proteo- lytic process (3,11,28,29). Because secretion of APP must include a cleavage step in the amyloid sequence by a hypothetical secre- tase, generation of the amyloid peptide 13A4 and normal secretion of APP are mutually exclusive processes (3,11,28). Inhibition of the secretase by proteinase inhibitors such as etl- antichymotrypsin, et2M, or the Kunitz proteinase inhibitor domain which is present in some forms of APP derived by alternative splicing of a common mRNA precursor (9,15,16,19,24), could prevent secretion of APP. Uncleaved APP is degraded in the en- dosomal-lysosomal pathway toward 13A4 containing fragments (13,14). Evidence for this attractive hypothesis was advanced by the observation that et2M but not od-antichymotrypsin, inhibited the secretion of APP in neural cells in vitro (12). Furthermore, im- munoreactivity was also found with polyclonal antibodies against a2M in the brain of AD patients, which was absent in normal brain (4). Based on these observations and on limited experimental ev- idence for the induction of et2M synthesis in neural cells by stim- ulation with interleukin 6, the hypothesis was advanced that a (sub)acute phase reaction, with a2M as one of the important me- diators could be responsible for at least some of the lesions in AD brain (4,5,12). The current study was undertaken to investigate whether the amyloid deposits in AD are indeed accompanied by the appearance of ct2M. Two well characterized mouse monoclonal antibodies against two different epitopes of human et2M (8,26,27) were used to study the expression of this broad spectrum proteinase inhibitor in the brain of AD patients and of normal older age matched patients. The study was extended to include other conditions with accumulation of amyloid peptide type [3A4 in the brain: Down's syndrome, Dementia of the Lewy Body type (DLB) and normal aged nondemented controls. METHOD Ct~ses Four patients (aged 71,74,76,76) had AD based on clinical and neuropathological features. The fifth patient (age 75) had Down's syndrome and displayed all neuropathological features of AD. Requests for reprints should be sent to R. Dom, Ph.D., Department of Neuropathology, University Hospital, Gasthuisberg, B, 3000 Leuven, Belgium. 233
Transcript of α2-macroglobulin expression in neuritic-type plaques in patients with Alzheimer's disease
Neurobiology of Aging, Vol. 14, pp. 233-237, 1993 0197-4580/93 $6.00 + .00 Printed in the U.S.A. All rights reserved. Copyright © 1993 Pergamon Press Ltd.
oL2-Macroglobulin Expression in Neuritic-Type Plaques in Patients With Alzheimer's Disease
D O M I N I Q U E V A N G O O L * , B A R T DE S T R O O P E R t , FRED VAN L E U V E N t , ERIK T R I A U $ A N D RENE DOM *1
Departments of *Neuropathology, and ~Human Genetics University Hospital, Gasthuisberg, Leuven, Belgium -~Psychogeriatric Nursing Home "De Wingerd", Leuven, Belgium
Received 9 July 1992; Accepted 8 January 1993
VAN GOOL, D., B. DE STROOPER, F. VAN LEUVEN, E. TRIAU AND R. DOM. ct2-Macroglobulin expression in neuritic-type plaques in patients with Alzheimer's disease, NEUROBIOL AGING 14(3) 233-237, 1993.--Because it has been suggested that et2M could be involved in the generation of amyloid peptide, attention was given to a possible association of t~2M expression and amyloid accumulation in the brain. Therefore, we investigated the presence of the proteinase inhibitor a2-macroglobulin (ct2M) in the cerebra of 4 patients with Alzheimer's Disease (AD). One case of a patient with Down's syndrome, 2 cases of patients with Dementia of the Lewy Body type (DLB), 1 case of an aged, clinically nondemented person who displayed many amyloid plaques, and 3 normal aged control brains were also studied. The results obtained by immunocytochemistry with monoclonal antibodies directed against two different epitopes of human ot2M showed an association of ~t2M, only with neuritic-type plaques in patients with AD. No ~x2M immunoreactivity was found in either preamyloid-type plaques or burned out-type plaques in AD, DLB, or aged nondemented controls. The results do not support a direct role of this proteinase inhibitor in the formation of amyloid. Because tx2M is observed to be associated with reactive microglia in the outer border of the neuritic plaques, the data suggest that et2M could be a marker for an inflammatory cellular process in these neuritic plaques.
Neuropathology et2-macroglobulin Dementia lmmunocytochemistry Alzheimer's Lewy Body disease
SEVERAL lines of evidence suggest a possible imbalance be- tween proteinases and proteinase inhibitors as a primary phenom- enon in Alzheimer's Disease (AD) (12). The neurofibrillary tan- gles strongly react with antibodies to ubiquitin (23). This peptide marks proteins for intracellular ATP-dependent proteolysis (21). The amyloid plaques, on the other hand, contain proteinases such as cathepsin B and D (6) and proteinase inhibitors like protease nexin 1 (22) and ot 1-antichymotrypsin (I).
Moreover, the amyloid peptide 13A4, the main component of the amyloid plaques and the congophilic angiopathy, is derived from the amyloid precursor protein (APP) by an unknown proteo- lytic process (3,11,28,29). Because secretion of APP must include a cleavage step in the amyloid sequence by a hypothetical secre- tase, generation of the amyloid peptide 13A4 and normal secretion of APP are mutually exclusive processes (3,11,28). Inhibition of the s e c r e t a s e by p r o t e i n a s e i n h i b i t o r s such as e t l - antichymotrypsin, et2M, or the Kunitz proteinase inhibitor domain which is present in some forms of APP derived by alternative splicing of a common mRNA precursor (9,15,16,19,24), could prevent secretion of APP. Uncleaved APP is degraded in the en- dosomal-lysosomal pathway toward 13A4 containing fragments (13,14).
Evidence for this attractive hypothesis was advanced by the observation that et2M but not od-antichymotrypsin, inhibited the secretion of APP in neural cells in vitro (12). Furthermore, im-
munoreactivity was also found with polyclonal antibodies against a2M in the brain of AD patients, which was absent in normal brain (4). Based on these observations and on limited experimental ev- idence for the induction of et2M synthesis in neural cells by stim- ulation with interleukin 6, the hypothesis was advanced that a (sub)acute phase reaction, with a2M as one of the important me- diators could be responsible for at least some of the lesions in AD brain (4,5,12).
The current study was undertaken to investigate whether the amyloid deposits in AD are indeed accompanied by the appearance of ct2M. Two well characterized mouse monoclonal antibodies against two different epitopes of human et2M (8,26,27) were used to study the expression of this broad spectrum proteinase inhibitor in the brain of AD patients and of normal older age matched patients. The study was extended to include other conditions with accumulation of amyloid peptide type [3A4 in the brain: Down's syndrome, Dementia of the Lewy Body type (DLB) and normal aged nondemented controls.
METHOD
Ct~ses
Four patients (aged 71,74,76,76) had AD based on clinical and neuropathological features. The fifth patient (age 75) had Down's syndrome and displayed all neuropathological features of AD.
Requests for reprints should be sent to R. Dom, Ph.D., Department of Neuropathology, University Hospital, Gasthuisberg, B, 3000 Leuven, Belgium.
233

234 VAN GOOL ET AL.
Cases 6 and 7 (aged 65 and 71) were diagnosed as having De- mentia of the DLB (18). The 8th patient (aged 75) had no clinical signs of dementia nor any other neurological nor psychiatric dis- ease but showed by neuropathological investigation a large num- ber of amyloid plaques (preamyloid- and burned out-type), with- out neurofibrillary tangles and without angiopathy. Three other aged control patients (aged 68,68,70) without neuropsychiatric symptoms were included in the study. Except for a few neurofi- brillary tangles in the hippocampus, they displayed no further neuropathological changes.
Histology and lmmunocytochemistry
Sections of the hippocampus and of temporal and parietal neo- cortical areas from the cerebra of those 11 subjects were investi- gated. Formalin-fixed paraffin embedded sections were stained with Haematoxylin-Eosin, Trichroom-Masson, Kluver- Barera, Cresyl-Violet, Congo-red, and modified Bielschowsky silverstain- ing. Immunostaining was carried out with monoclonal antibodies following the P.A.P. method (Sternberger et al., 1970) after pre- treatment of the sections with 50% formic acid for 7 min.
Monoclonal antibodies F44etB2 and F4413A7 to human ct2- Macroglobulin have been described previously (8,27). They react with two different epitopes as described by Delain et al. (8). Both are detected only on complex form et2M, while the epitope of F44etB2 has been mapped on the receptor binding domain of ot2M (8,27). The Mabs were purified from ascites fluid by ammonium sulfate precipitation (2,5 M) and gel filtration (ACA 34/44, LKB). Antibodies against APP (Boehringer-Mannheim) and against [3A4 (BDS and FVL, unpublished observations) were used. Antibodies against Tau (Biomakor) and Ubiquitin (Dakopatts) were used to investigate the neurofibrillary pathology and Lewy bodies. Kpl (Dako), a monoclonal antibody against microglia, was used to investigate the microglial reaction in the plaques.
To compare the different stainings, serial sections were taken for all the different antibodies. Tau, ubiquitin, 13A4, APP, et2M, and Kpl were compared with each other and with the silver stain- ing.
Control experiments were carried out by omission of the pri- mary antibody and by the use of other monoclonal mouse anti- bodies which remained negative. (anti-Heparansulfate antibody IC7) (17).
RESULTS
Description and Quantification of Amyloid and Neurofibrillary Pathology
In the four cerebra of the Alzheimer patients and also in the cerebrum of the patient with Downs syndrome, many preamyloid plaques, neuritic plaques, and burned out plaques were visualised with Bielschowsky silverstaining. In 2 cases, there was an intense amyloid angiopathy, visualised with congo-red staining. The dif- ferent types of plaques and the amyloid angiopathy stained with antibodies against 13A4 protein. APP antibodies also stained senile plaques in AD and some plaques in DLB. Many neurofibrillary tangles were visualized with antibodies against tau and ubiquitin. Tau staining also demonstrated the presence of numerous neuritic plaques. In the cases with DLB, abundant Lewy bodies were found with ubiquitin antibodies localized in the substantia nigra, the locus coereleus but also in the archi- and in the neocortex. Numerous amyloid plaques from the burned out and the preamy- loid type could be visualized with APP-antibodies and [3A4- antibodies. All these plaques remained tan-negative. In 1 control case with many preamyloid- and burned out-type plaques, the
plaques stained with antibodies against APP and [3A4 peptides. In the other 3 control cases, no amyloid plaques were observed. In the hippocampal area, a few neurofibrillary tangles were present.
In the hippocampus and in temporo-parietal neocortex, amy- loid plaques and neurofibrillary tangles were counted in all 11 cases. The terminology used for the amyloid plaques is based on the neuropathological concept of Ulrich et al. (25). Plaques and tangles were counted after silver staining and 13A4 immunostain- ing (neuritic, burned out, and preamyloid plaques), and after tau staining (neuritic plaques). In each region, multiple microscopical fields were chosen at random and countings were carried out. The mean and the SD were calculated. The magnitude of the micro- scope was 100" and the surface of one field was 1,07 mm 2. Table 1 shows the mean number of lesions per field in different brain regions. It is clear that AD and Down patients are characterized by neurofibrillary pathology (tangles - neuritic-type plaques) while controls and cases with DLB do not present those lesions.
tx2 M-lmmunocytochemistry
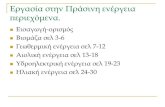
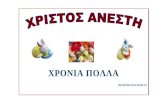
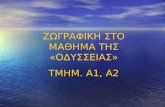
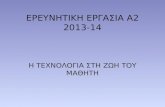
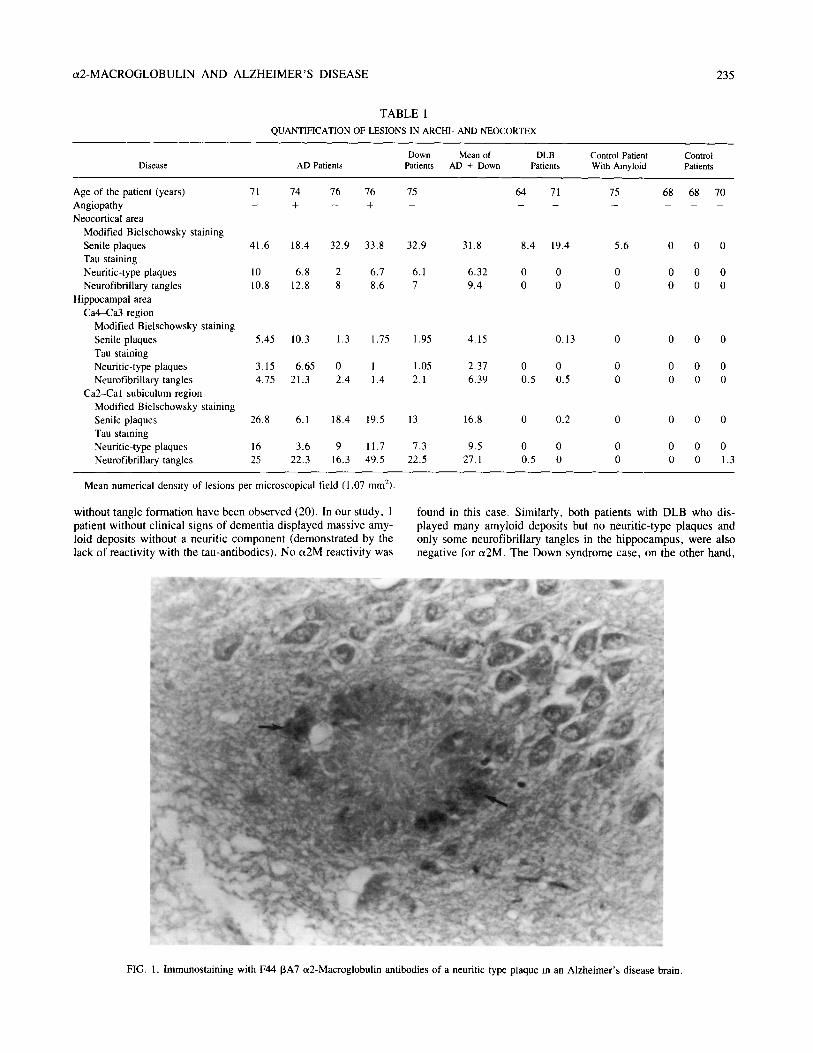
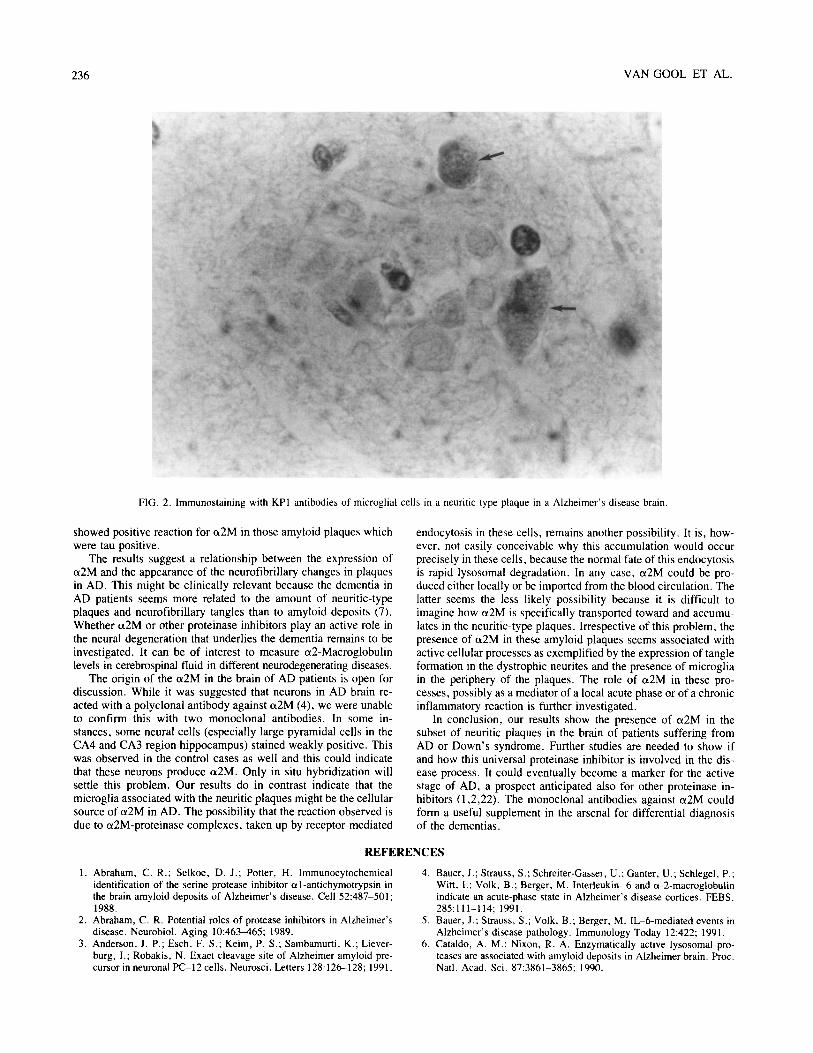
The two different monoclonal ct2-Macroglobulin antibodies showed the same immunoreactivity. Positive staining was only observed in neuritic-type plaques, as well in the neocortex as in the hippocampus. In these plaques, the ct2M staining was clearly lo- cated in a halo around the amyloid core (Fig. 1). In some lesions, the positive reaction occured in microglial cells which were situ- ated in and around these neuritic plaques (Fig. 2). These cells were also ubiquitin-positive but remained tau negative. The neurofibril- lary tangles themselves were et2M-negative. The amyloid core of the plaques and also the amyloid angiopathy remained negative. Plaques from the preamyloid type or from the burned out type, which did not react with antibodies against tau were also negative for a2-Macroglobulin.
In the cases with DLB we failed to detect any positive reaction with et2M antibodies, which correlates with the lack of neurofi- brillary changes and neuritic-type plaques.
In all the 11 cases reported here, a weak positive reaction with et2M-antibodies was present in the pyramidal cells of the hippo- campus, especially in the CA4 and CA3 region. Because both control and AD cases show this reactivity, it indicates that a weak a2-Macroglobulin staining in these neurons is present normally and is not altered in AD.
DISCUSSION
A possible relationship has been proposed between the amyloid formation in brains of patients with AD and the presence of the potent broad spectrum proteinase inhibitor et2M (4,5,12).
Our data obtained by immunohistochemistry with two different monoclonal antibodies demonstrate that et2M is indeed present in amyloid plaques of AD brain but only in the neuritic-type plaques containing neurofibrillary material and thus positive staining with tau antibodies. We were not able to demonstrate any reactivity with the anti-et2M antibodies in preamyloid deposits or in burned out-type plaques, although these stained clearly with a monoclonal antibody against precursor amyloid protein and with polyclonal antibodies against [3A4- peptide. Because preamyloid deposits are thought to be the first step in the formation of the amyloid plaques, the absence of immunoreactivity for et2M in these deposits does not support a role for ot2M in the formation of the amyloid peptide. This is in agreement with our biochemical findings (10).
In contrast, the presence of ot2M in AD seems associated with the appearance of neurofibrillary changes in the plaques. Several diseases are known where production of amyloid from the 13A4- type occurs without the appearance of neurofibrillary tangles or neuritic plaques. Also in normal, elderly people, amyloid deposits
c t2 -MACROGLOBULIN A N D A L Z H E I M E R ' S DISEASE 235
TABLE 1
QUANTIFICATION OF LESIONS IN ARCHI- AND NEOCORTEX
Down Mean of DLB Control Patient Control Disease AD Patients Patients AD + Down Patients With Amyloid Patients
Age of the patient (years) 71 74 76 76 75 64 71 75 68 68 70 Angiopathy - + - + . . . . . Neocortical area
Modified Bielschowsky staining Senile plaques Tan staining Neuritic-type plaques Neurofibrillary tangles
Hippocampal area Ca4--Ca3 region
Modified Bielschowsky staining Senile plaques Tau staining Neuritic-type plaques Neurofibrillary tangles
Ca2-Cal subiculum region Modified Bielschowsky staining Senile plaques Tau staining Neuritic-type plaques Neurofibrillary tangles
41.6 18.4 32.9 33.8 32.9 31.8 8.4 19.4 5.6 0 0 0
10 6.8 2 6.7 6.1 6.32 0 0 0 0 0 0 10.8 12.8 8 8.6 7 9.4 0 0 0 0 0 0
5.45 10.3 1.3 1.75 1.95 4.15 0.13 0 0 0 0
3.15 6.65 0 1 1.05 2.37 0 0 0 0 0 0 4.75 21.3 2.4 1.4 2.1 6.39 0.5 0.5 0 0 0 0
26.8 6.1 18.4 19.5 13 16.8 0 0.2 0 0 0 0
16 3.6 9 11.7 7.3 9.5 0 0 0 0 0 0 25 22.3 16.3 49.5 22.5 27.1 0.5 0 0 0 0 1.3
Mean numerical density of lesions per microscopical field (1.07 mm2).
without tangle formation have been observed (20). In our study, 1 patient without clinical signs of dement ia displayed massive amy- loid deposits without a neuritic component (demonstrated by the lack o f reactivity with the tau-antibodies). No ot2M reactivity was
found in this case. Similarly, both patients with DLB who dis- played many amyloid deposits but no neurit ic-type plaques and only some neurofibrillary tangles in the h ippocampus , were also negative for a2M. The Down syndrome case, on the other hand,
FIG. 1. lmmunostaining with F44 [3A7 a2-Macroglobulin antibodies of a neuritic type plaque in an Alzheimer's disease brain.
236 VAN GOOL ET AL.
FIG. 2. Immunostaining with KPI antibodies of microglial cells in a neuritic type plaque in a Alzheimer's disease brain.
showed positive reaction for et2M in those amyloid plaques which were tau positive.
The results suggest a relationship between the expression of ct2M and the appearance of the neurofibrillary changes in plaques in AD. This might be clinically relevant because the dementia in AD patients seems more related to the amount of neuritic-type plaques and neurofibrillary tangles than to amyloid deposits (7). Whether ot2M or other proteinase inhibitors play an active role in the neural degeneration that underlies the dementia remains to be investigated. It can be of interest to measure a2-Macroglobulin levels in cerebrospinal fluid in different neurodegenerating diseases.
The origin of the ot2M in the brain of AD patients is open for discussion. While it was suggested that neurons in AD brain re- acted with a polyclonal antibody against a2M (4), we were unable to confirm this with two monoclonal antibodies. In some in- stances, some neural cells (especially large pyramidal cells in the CA4 and CA3 region hippocampus) stained weakly positive. This was observed in the control cases as well and this could indicate that these neurons produce ot2M. Only in situ hybridization will settle this problem. Our results do in contrast indicate that the microglia associated with the neuritic plaques might be the cellular source of a2M in AD. The possibility that the reaction observed is due to et2M-proteinase complexes, taken up by receptor-mediated
endocytosis in these cells, remains another possibility. It is, how- ever, not easily conceivable why this accumulation would occur precisely in these cells, because the normal fate of this endocytosis is rapid lysosomal degradation. In any case, et2M could be pro- duced either locally or be imported from the blood circulation. The latter seems the less likely possibility because it is difficult to imagine how et2M is specifically transported toward and accumu- lates in the neuritic-type plaques. Irrespective of this problem, the presence of et2M in these amyloid plaques seems associated with active cellular processes as exemplified by the expression of tangle formation in the dystrophic neurites and the presence of microglia in the periphery of the plaques. The role of o~2M in these pro- cesses, possibly as a mediator of a local acute phase or of a chronic inflammatory reaction is further investigated.
In conclusion, our results show the presence of tx2M in the subset of neuritic plaques in the brain of patients suffering from AD or Down's syndrome. Further studies are needed to show if and how this universal proteinase inhibitor is involved in the dis- ease process. It could eventually become a marker for the active stage of AD, a prospect anticipated also for other proteinase in- hibitors (1,2,22). The monoclonal antibodies against o~2M could form a useful supplement in the arsenal for differential diagnosis of the dementias.
REFERENCES
1. Abraham, C. R.; Selkoe, D. J.; Potter, H. Immunocytochemical identification of the serine protease inhibitor ~l-antichymotrypsin in the brain amyloid deposits of Alzheimer's disease. Cell 52:487-501; 1988.
2. Abraham, C. R. Potential roles of protease inhibitors in Alzheimer's disease. Neurobiol. Aging 10:463-465; 1989.
3. Anderson, J. P.; Esch, F. S.; Keim, P. S.; Sambamurti, K.; Liever- burg, I.; Robakis, N. Exact cleavage site of Alzheimer amyloid pre- cursor in neuronal PC-12 cells. Neurosci. Letters 128:126-128; 1991.
4. Bauer, J.; Strauss, S.; Schreiter-Gasser, U.; Ganter, U.; Schlegel, P.; Witt, I.; Volk, B.; Berger, M. Interleukin- 6 and a-2-macroglobulin indicate an acute-phase state in Alzheimer's disease cortices. FEBS. 285:111-114; 1991.
5. Bauer, J.; Strauss, S.; Volk, B.; Berger, M. IL-6-mediated events in Alzheimer's disease pathology. Immunology Today 12:422; 1991.
6. Cataldo, A. M.; Nixon, R. A. Enzymatically active lysosomal pro- teases are associated with amyloid deposits in Alzheimer brain. Proc. Natl. Acad. Sci. 87:3861-3865; 1990.

a2-MACROGLOBULIN AND ALZHEIMER'S DISEASE 237
7. Delacourte, A.; Flament, S.; Dibe, E. M.; Hublau, P.; Sablonnirre, B.; Hrmon, B.; Shrrrer, V.; D6fossez, A. Pathological proteins tan 64 and 69 are specifically expressed in the somatodindritic domain of the degenerating cortical neurons during Alzheimer's disease. Acta Neuropathol. 80:111-117; 1990.
8. Delain, E.; Barray, M.; Tapon-Bretaudiere, J.; Pochon, F., Marynen, P.; Cassiman, J. J.; Van Den Berghe, H.; Van Leuven, F. The mo- lecular organization of human alpha-2- macroglobulin: An immuno- electron microscopic study with monoclonal antibodies. J. Biol. Chem. 263:2981-2989; 1988.
9. De Strooper, B.; Van l_euven, F.; Van Den Berghe, H. The amyloid 13 protein precursor of proteinase nexin 2 from mouse is closer related to its human homolog than previously reported. Biochim. Biophys. Acta 1129:141-143; 1991.
10. De Strooper, B.; Van Leuven, F.; Van Den Berghe, H. ~2- Macro- globulin and other proteinase inhibitors do not interfere with the se- cretion of amyloid precursor protein in mouse neuroblastoma cells. FEBS. 308:50-53; 1992.
11. Esch, F. S.; Keim, P. S.; Beattie, E. S.; Blacher, R. W.; Culwell, A. R., Oltersdorf, T.; McClure, D.; Ward, P. J. Cleavage of amyloid 13 peptide during constitutive processing of its precursor. Science 248: 1122-1123; 1990.
12. Ganter, U.; Strauss, S.; Jonas, U.; Weidemann, A.; Beyreuther, K.; Volk, B.; Berger, M.; Bauer, J. Alpha 2-macroglobulin synthesis in interleukin-6-stimulated human neuronal (SH-SY5Y neuroblastoma) cells. FEBS. 282:127- 131; 1991.
13. Golde, T. E.; Estus, S.; Younkin, L. H.; Selkoe, D. J.; ¥ounkin, S. G. Processing of the amyloid protein precursor to potentially amy- loidogenic derivates. Science. 255:728-730; 1992.
14. Haass, C.; Koo, E. H.; Mellon, A.; Hung, A. Y.; Selkoe, D. J. Tar- geting of cell-surface &amyloid precursor protein to lysosomes: AI- teruative processing into amyloid-bearing fragments. Nature 357:500- 502; 1992.
15. Kang, J.; Lemaire, H. G., Unterbeck, A.; Salbaum, J. M.; Masters, C. L.; Grzeschik, K.; Multhaup, G.; Beyreuther, K.; M~iller-Hill, B. The precursor of Alzheimer's disease amyloid A4 protein resembles a cell-surface receptor. Nature 325:733-734; 1987.
16. Kitaguchi, N.; Takahashi, Y.; Tokushima, Y.; Shiojiri, S.; Ito, H. Novel precursor of Alzheimer's disease amyloid protein shows pro- tease inhibitory activity. Nature 331:539-540; 1988.
17. Lories, V.; Cassiman, J. J.; Van Den Berghe, H.; David, G. Multiple distinct membrane heparan sulfate proteoglycans in human lung fi- broblasts. J. Biol. Chem. 264:7009-7016;1989.
18. Neary, D. Non-Alzheimer's disease forms of cerebral atrophy. J. Neurol. Neurosurg. Psychiatry 53:929-93 l; 1990.
19. Ponte, P.; Gonzales-DeWhitt, P.; Schilling, G.; Miller, J.; Hsu, D.; Greenberg, G.; Davis, K.; Wallace, W.; Lieberburg, I.; Fuller, F.; Gordell, B. A new A4 amyloid mRNA contains a domain homologous to serine protease inhibitors. Nature 311:525-527; 1988.
20. Price, J. L.; Davis, P. B.; Morris, J. C.; White, D. L. The distribu- tion of tangles, plaques and related immunohistochemical markers in healthy aging and Alzheimer's disease. Neurobiol. Aging 12:295- 312; 1991.
21. Rechsteiner, M. Natural substrates of the ubiquitin proteolytic path- way. Cell 66:615-618; 1991.
22. Rosenblatt, D. E.; Geula, C.; Mesulam, M. Protease Nexin 1 immu- nostaining in Alzheimer's disease. Ann Neurol 26:628-634; 1989.
23. Tabaton, M.; Cammarata, S.; Mancardi, G.; Manetto, V.; Autilio- Gambetti, L.; Perry, G.; Gambetti, P. Ultrastructural localization of 13-amyloid, tau, and ubiquitin epitopes in extracellular neurofibrillary tangles. Proc. Natl. Acad. Sci. 88:2098-2102; 1991.
24. Tanzi, R. E.; McClatchey, A. I.; Lamperti, E. D.; Villa- Komaroff, L.; Gusella, J. F.; Neve, R. L. Protease inhibitor domain encoded by an amyloid protein precursor mRNA associated with Alzheimer's dis- ease. Nature 331:528- 529; 1988.
25. Ulrich, J. Recent progress in the characterization of the pathological hallmarks for Alzheimer's disease. Acta Neuropathol. Suppl. 129:5- 7; 1990.
26. Van Leuven, F. Human ct2-macroglobulin: Structure and function. TIBS. 7:185-187; 1982.
27. Van Leuven, F.; Marynen, P.; Cassiman, J. J.; Van Den Berghe H. Mapping of structure-function relationships in proteins with a panel of monoclonal antibodies. J. Immunol. Meth. 11:39--49; 1988.
28. Wang, R.; Meschia, J. F.; Cotter, R. J.; Sisodia, S. S. Secretion of the 13/A4 amyloid precursor protein. J. Biol. Chem. 266:16960- 16964; 1991.
29. Weidemann, A.; Kfnig, G.; Bunke, D.; Fischer, P.; Salbaum, J. M.; Masters, C. L.; Beyreuther, K. Identification, biogenesis, and local- ization of precursors of Alzheimer's disease A4 amyloid protein. Cell 57:115-126; 1989.