β2-agonists in asthma
4
43 LETTERS to the EDITOR &bgr;2-agonists in asthma SIR,-Dr Sears and colleagues (Dec 8, p 1391) and your accompanying editorial suggest that because of data generated with fenoterol inhaled &bgr;2-agonists as a drug class should not be prescribed as regular therapy since they may cause asthma control to worsen. On the basis of data generated during the development of salmeterol, a novel long-acting inhaled &bgr;2-agonist, we draw different conclusions. In a large placebo-controlled study in 675 patients’ with mild-to-moderate disease as defmed by FEV 60-90 % of predicted, we have proved that regular twice daily salmeterol produces significant improvements in asthma control as assessed by objective increase in lung function, reduction in requirement for additional bronchodilator, and reduction in waking episodes at night. These findings have been confirmed in a 12-week study in patients with more severe airways obstruction These improvements, although more striking with twice daily salmeterol, have also been seen when regular salbutamol has been used as a comparator.3A Why our programme has obtained results so different from those of Sears et al may be due to several factors, such as study design, drug tested, or a combination of both. Fenoterol differs from salbutamol and terbutaline in its extrapulmonary side-effects, as confirmed by Dr Wong and colleagues in the same issue of The Lancet, who reproduce the findings of Crane et al.5 We feel that extrapolation of data generated with fenoterol to all (3z-agonists is inappropriate since studies in large numbers of patients with salmeterol and salbutamol do not support the findings of Sears and colleagues. Department of Respiratory Medicine, Glaxo Group Research Ltd, Greenford UB6 0HE, UK J. B. D. PALMER M. M. JENKINS 1. Dahl R Salmeterol one month studies m asthmatic patients. Eur Resp J 1989, 2 (suppl 8): 677s. 2. Viskum K. Inhaled salmeterol improves control m moderate to severe asthmatics: a 3 month study. Eur Resp J 1990; 3: 839 3. Britton M. Salmeterol. three month comparison with salbutamol in asthmatic patients. Eur Resp J 1990; 3: 786. 4. Lundback B, Lmdstrom M. A 3 month comparison of salmeterol and salbutamol dry powder. Clin Exp Allergy 1990: 20 (suppl 1): 93. 5 Crane J, Burgess C, Beasley R. Cardiovascular and hypokalaemic effects of inhaled salbutamol, fenoterol and isoprenaline. Thorax 1989; 44: 136-40 SIR,-Your Dec 8 editorial (p 1411) refers to inhaled &bgr;2-agonists as "reliever" treatment whereas inhaled corticosteroids are contrasted as "preventer" treatment. This classification cannot be justified: several studies have found &bgr;2 -agonists to be preventers and inhaled corticosteroids as relievers. Sometimes you cite laboratory challenge studies to support the claim that inhaled &bgr;2-agonists have no influence on the underlying airways inflammation. However, when similar challenge studies show an influence of inhaled salmeterol on the late-phase reaction and subsequent enhanced bronchial reactivity, this finding is neglected because laboratory studies are not thought to reflect clinical asthma. Asthma is very difficult to treat but, as for any disease, symptomatic relief should be given, and treatment should not be withheld because of the possibility of relapse with more severe symptoms when the treatment is stopped. When this possibility exists it simply means that the treatment should not be stopped, at least not abruptly: withdrawal of corticosteroids can result in rapid and severe deterioration in asthma but this should not be used as an argument for not using these drugs in patients with asthma. The study by Dr Sears and colleagues (Dec 8, p 1391) gives a surprising result, at least for physicians who in their daily work treat asthma patients. A finding that regular treatment four times daily with inhaled fenoterol results in deterioration of asthma control needs confirmation. Concern generated by studies with the short-acting &bgr;2-agonist fenoterol is, surprisingly, extended to the long-acting salmeterol and formoterol. One,’ three,z-4 and twelve month (personal communication) studies with salmeterol have yielded none of the suggested adverse effects: on the contrary, compared with conventional, as necessary use of salbutamol, patients treated with salmeterol had less nocturnal symptoms, less daytime symptoms, improved morning and evening peak expiratory flow, and fewer exacerbations. Department of Respiratory Diseases, University Hospital of Aarhus, DK-8000 Aarhus C, Denmark RONALD DAHL 1. Dahl R. Salmeterol one month studies in asthmatic patients. Eur Resp J 1989, 2 (suppl 8): 677S 2. Bntton M. Salmeterol three month companson with salbutamol in asthmatic patients Eur Resp J 1990, 3 (suppl 10) 226S 3. Viskum K. Inhaled salmeterol improves control in moderate to severe asthmatics. a three month study. Eur Resp J 1990, 3 (suppl 10) 235S. 4 Lunback B, Lmdstrom M. A 3 month companson of salmeterol and salbutamol dry powder Clin Exp Allergy 1990, 20 (suppl 1). 93. SiR,—The evidence incriminating p-agonist therapy as a cause of increased asthma morbidity and, possibly, mortality is now so strong that doctors should alter their attitude to these drugs. Evidence that p-agonists can worsen asthma has been available for some years’ but Dr Sears and his colleagues now produce proof that regular treatment with a p-receptor agonist causes asthma to deteriorate compared with the same agent used on an "as necessary" basis. These fmdings should be regarded as an effect of p-agonists in general and not just the agent studied (fenoterol). Regular treatment with p-agonists must be discouraged and more emphasis placed upon the earlier use of anti-inflammatory agents, especially inhaled corticosteroids.2 Sears et al and your accompanying editorial express concern over the use of long-acting &bgr;2-agonists, such as salmeterol and formoterol. Salmeterol has recently been launched in the UK as a new type of &bgr;2-agonist "which provides long-lasting bronchodilatation and has anti-inflammatory activity". The manufacturer recommends regular treatment twice daily. The promotion of this drug as an agent with clinically relevant anti-inflammatory activity is potentially dangerous. Already one of my patients has had to be resuscitated after salmeterol was prescribed by his general practitioner, long-term oral corticosteroid therapy having been withdrawn. Salmeterol is a very effective bronchodilator with a prolonged duration of action which allows treatment to be given twice daily. However, Sears’ findings make it difficult for me to decide for which patients, if any, I should prescribe this drug. It should not, under any circumstances, be used as monotherapy. Salmeterol may have a role in patients in whom moderate or high-dose inhaled corticosteroid therapy has failed to control symptoms, especially nocturnal wakenings. The small minority of patients who require a combination of inhaled and oral steroids might also obtain some benefit from salmeterol.
Transcript of β2-agonists in asthma

43
LETTERS to the EDITOR
&bgr;2-agonists in asthmaSIR,-Dr Sears and colleagues (Dec 8, p 1391) and your
accompanying editorial suggest that because of data generated withfenoterol inhaled &bgr;2-agonists as a drug class should not be
prescribed as regular therapy since they may cause asthma controlto worsen. On the basis of data generated during the development ofsalmeterol, a novel long-acting inhaled &bgr;2-agonist, we drawdifferent conclusions.
In a large placebo-controlled study in 675 patients’ withmild-to-moderate disease as defmed by FEV 60-90 % of predicted,we have proved that regular twice daily salmeterol producessignificant improvements in asthma control as assessed by objectiveincrease in lung function, reduction in requirement for additionalbronchodilator, and reduction in waking episodes at night. Thesefindings have been confirmed in a 12-week study in patients withmore severe airways obstruction These improvements, althoughmore striking with twice daily salmeterol, have also been seen whenregular salbutamol has been used as a comparator.3AWhy our programme has obtained results so different from those
of Sears et al may be due to several factors, such as study design,drug tested, or a combination of both. Fenoterol differs fromsalbutamol and terbutaline in its extrapulmonary side-effects, asconfirmed by Dr Wong and colleagues in the same issue of TheLancet, who reproduce the findings of Crane et al.5 We feel thatextrapolation of data generated with fenoterol to all (3z-agonists isinappropriate since studies in large numbers of patients withsalmeterol and salbutamol do not support the findings of Sears andcolleagues.
Department of Respiratory Medicine,Glaxo Group Research Ltd,Greenford UB6 0HE, UK
J. B. D. PALMERM. M. JENKINS
1. Dahl R Salmeterol one month studies m asthmatic patients. Eur Resp J 1989, 2 (suppl8): 677s.
2. Viskum K. Inhaled salmeterol improves control m moderate to severe asthmatics: a 3month study. Eur Resp J 1990; 3: 839
3. Britton M. Salmeterol. three month comparison with salbutamol in asthmatic patients.Eur Resp J 1990; 3: 786.
4. Lundback B, Lmdstrom M. A 3 month comparison of salmeterol and salbutamol drypowder. Clin Exp Allergy 1990: 20 (suppl 1): 93.
5 Crane J, Burgess C, Beasley R. Cardiovascular and hypokalaemic effects of inhaledsalbutamol, fenoterol and isoprenaline. Thorax 1989; 44: 136-40
SIR,-Your Dec 8 editorial (p 1411) refers to inhaled &bgr;2-agonistsas "reliever" treatment whereas inhaled corticosteroids are
contrasted as "preventer" treatment. This classification cannot bejustified: several studies have found &bgr;2 -agonists to be preventers andinhaled corticosteroids as relievers.
Sometimes you cite laboratory challenge studies to support theclaim that inhaled &bgr;2-agonists have no influence on the underlyingairways inflammation. However, when similar challenge studiesshow an influence of inhaled salmeterol on the late-phase reactionand subsequent enhanced bronchial reactivity, this finding is
neglected because laboratory studies are not thought to reflectclinical asthma.Asthma is very difficult to treat but, as for any disease,
symptomatic relief should be given, and treatment should not bewithheld because of the possibility of relapse with more severesymptoms when the treatment is stopped. When this possibilityexists it simply means that the treatment should not be stopped, atleast not abruptly: withdrawal of corticosteroids can result in rapid
and severe deterioration in asthma but this should not be used as an
argument for not using these drugs in patients with asthma.The study by Dr Sears and colleagues (Dec 8, p 1391) gives a
surprising result, at least for physicians who in their daily work treatasthma patients. A finding that regular treatment four times dailywith inhaled fenoterol results in deterioration of asthma controlneeds confirmation.
Concern generated by studies with the short-acting &bgr;2-agonistfenoterol is, surprisingly, extended to the long-acting salmeteroland formoterol. One,’ three,z-4 and twelve month (personalcommunication) studies with salmeterol have yielded none of thesuggested adverse effects: on the contrary, compared with
conventional, as necessary use of salbutamol, patients treated withsalmeterol had less nocturnal symptoms, less daytime symptoms,improved morning and evening peak expiratory flow, and fewerexacerbations.
Department of Respiratory Diseases,University Hospital of Aarhus,DK-8000 Aarhus C, Denmark RONALD DAHL
1. Dahl R. Salmeterol one month studies in asthmatic patients. Eur Resp J 1989, 2 (suppl8): 677S
2. Bntton M. Salmeterol three month companson with salbutamol in asthmatic patientsEur Resp J 1990, 3 (suppl 10) 226S
3. Viskum K. Inhaled salmeterol improves control in moderate to severe asthmatics. athree month study. Eur Resp J 1990, 3 (suppl 10) 235S.
4 Lunback B, Lmdstrom M. A 3 month companson of salmeterol and salbutamol drypowder Clin Exp Allergy 1990, 20 (suppl 1). 93.
SiR,—The evidence incriminating p-agonist therapy as a cause ofincreased asthma morbidity and, possibly, mortality is now so
strong that doctors should alter their attitude to these drugs.Evidence that p-agonists can worsen asthma has been available forsome years’ but Dr Sears and his colleagues now produce proof thatregular treatment with a p-receptor agonist causes asthma todeteriorate compared with the same agent used on an "as necessary"basis. These fmdings should be regarded as an effect of p-agonists ingeneral and not just the agent studied (fenoterol). Regular treatmentwith p-agonists must be discouraged and more emphasis placedupon the earlier use of anti-inflammatory agents, especially inhaledcorticosteroids.2
Sears et al and your accompanying editorial express concern overthe use of long-acting &bgr;2-agonists, such as salmeterol andformoterol. Salmeterol has recently been launched in the UK as anew type of &bgr;2-agonist "which provides long-lastingbronchodilatation and has anti-inflammatory activity". Themanufacturer recommends regular treatment twice daily. Thepromotion of this drug as an agent with clinically relevant
anti-inflammatory activity is potentially dangerous. Already one ofmy patients has had to be resuscitated after salmeterol was
prescribed by his general practitioner, long-term oral corticosteroidtherapy having been withdrawn. Salmeterol is a very effectivebronchodilator with a prolonged duration of action which allowstreatment to be given twice daily. However, Sears’ findings make itdifficult for me to decide for which patients, if any, I should
prescribe this drug. It should not, under any circumstances, be usedas monotherapy. Salmeterol may have a role in patients in whommoderate or high-dose inhaled corticosteroid therapy has failed tocontrol symptoms, especially nocturnal wakenings. The smallminority of patients who require a combination of inhaled and oralsteroids might also obtain some benefit from salmeterol.

44
The reasons why regular bronchodilator therapy makes asthmaworse are conjectural but could be, as suggested by Sears et al, amanifestation of bronchodilatation allowing greater exposure toallergens or other factors which worsen asthma. If so, the longer theduration of action of the bronchodilator the worse one might expectthe adverse effects on asthma control to be.
I have been concerned for some time that treatment of asthmarather than an increase in prevalence of the disease has beenresponsible for the increase in mortality. I and many colleagues arevery worried about the potential dangers of long-acting &bgr;z-agonistswhich are claimed to have anti-inflammatory properties. Somegeneral practitioners may prescribe salmeterol or formoterol at atime when they would have formerly have introduced an inhaledsteroid; some patients might be misled by the apparent wellbeingproduced by a long-acting bronchodilator and stop inhaled
corticosteroids; and patients may use these drugs both 12-hourlyand for breakthrough symptoms, which could lead to greaterproblems than those already reported with fenoterol and perhaps totachyphylaxis also. Another concern is that if salmeterol does lead toa rise in mortality this might not be picked up until a major increaseis apparent in the Registrar General’s mortality statistics. I havebeen asking colleagues in hospital and in general practice whether,in the event of an asthma death, a report would be sent to theCommittee on Safety of Medicines (CSM) if the patient had beeninhaling salmeterol. Only one consultant colleague, who hasorganised an asthma deaths survey, would probably use the CSMyellow card in such a circumstance. When a patient has, say, a rashand is taking a new drug the adverse events would usually bereported. Death is rarely thought of as an adverse effect of a drugsince it is much more common to assume that death is due to diseaserather than treatment.
Sears and colleagues’ paper almost coincided with the UK launchof salmeterol. Clinicians persuaded to use regular p-agonist therapyin the form of salmeterol (or formoterol) must be very cautiousabout potential adverse effects and should be encouraged to recordall treatments taken by patients who die from asthma. In my opinionregular treatment with established bronchodilators (salbutamol,terbutaline, and fenoterol) should cease immediately.
Respiratory Unit,Northern General Hospital,Edinburgh EH5 2DQ, UK GRAHAM K. CROMPTON
1. Kraan J, Koeter GH, van der Mark TW, Sluiter HJ, deVries K. Changes in bronchialhyper-reactivity induced by four weeks of treatment with anti-asthmatic drugs inpatients with allergic asthma: a comparison between budesonide and terbutaline.J Allergy Clin Immunol 1985; 76: 628-36.
2. Bntish Thoracic Society, Research Unit of the Royal College of Physicians of London,King’s Fund Centre, and National Asthma Campaign. Guidelines for managementof asthma in adults I: Chronic persistent asthma. Br Med J 1990; 301: 651-53
SiR,—Two papers in your Dec 8 issue add to the evidence thatthe association between fenoterol and asthma death is likely to becausal1,2 and support moves to restrict severely the use of this drug.What is not yet clear is whether these studies should lead to changesin the use of other &bgr;z-agonists.Dr Wong and colleagues’ findings add to evidence that fenoterol
is more potent and less &bgr;z-selective than other commonly used&bgr;z-agonists. These properties were known before fenoterol wasintroduced,3-5 as was the fact that fenoterol could cause death inbaboons when infused in doses previously given to man.6 All&bgr;z-agonists are potentially hazardous; the degree of hazard dependson dose, selectivity, and clinical setting. Isoprenaline and fenoterol(both associated with epidemics of asthma mortality) cause strikingincreases in heart rate and inotropy; this would greatly increaseoxygen demand, which may be harmful in the face of hypoxaemia.Although high doses of isoprenaline do not produce seriousventricular arrhythmias when given to animals with normal bloodgas tension, much smaller doses may cause fatal cardiac depressionduring hypoxaemia.7Dr Sears and colleagues suggest that regular fenoterol use may
increase the risk of asthma death by increasing asthma severity.They suggest that their findings relate to all &bgr;z-agonists, but there isvery little evidence for this. The regular use of fenoterol greatlyreduces baseline airway calibre,8,9 and this happens more frequently
with fenoterol than with terbutaline." Our studies of drug therapyand asthma death show a much increased risk with fenoterol thanwith salbutamol. The magnitude of chronic side-effects of fenoteroland isoprenaline may differ from those of other &bgr;z-agonists, just asthere are differences in acute side-effects.These studies should lead to a modification of asthma
management-towards earlier inhaled anti-inflammatory therapywith a return to the originally intended use of inhaled &bgr;z-agonists,for symptomatic relief. However, in redefining the use of
&bgr;z-agonists in asthma, it is important to emphasise that there arepharmacological differences as well as similarities. Recent workimplies not only that all &bgr;z-agonists should be used less often, butalso that some should preferably not be used at all.
Department of Medicine,Wellington School of Medicine,Wellington, New Zealand
JULIAN CRANECARL BURGESSRICHARD BEASLEYNEIL PEARCE
1. Grainger J, Woodman K, Pearce NE, et al. Prescribed fenoterol and death fromasthma m New Zealand, 1981-1987. a further case-control study. Proceedings ofthe British Thoracic Society winter meeting 1990. Thorax (in press) (abstr).
2. Pearce NE, Beasley R, Burgess C, Grainger J, Crane J. Confounding by seventy doesnot explain the association between fenoterol and asthma death Med J Aust NZ1990; 20 (suppl 1): 515 (abstr).
3. Wagner J, Reinhardt D, Schumann HJ. Comparison of the bronchodilator andcardiovascular actions of isoprenaline, Th 1165a, terbutaline and salbutamol in catsand isolated organs preparations. Res Exp Med 1973, 162: 49-62.
4. Apperley GH, Daly MJ, Levy GP. Selectivity of beta adrenoceptor agonists andantagonists on bronchial, skeletal, vascular and cardiac muscle m the anaesthetizedcat. Br J Pharmacol 1976, 57: 235-46.
5. Brittain RT, Dean CM, Jack D. Sympathomimetic bronchodilator drugs. PharmacolTher Bull 1976; 2: 423-62
6. Cohen E, van As A, Quirk C. A haemodynamic study of fenoterol (berotec) in thebaboon Med Proc 1972; 18: 24-27.
7. Collins JM, McDevitt DG, Shanks RG, Swanton JG The cardiotoxicity of
isoprenaline during hypoxia. Br J Pharmacol 1969; 36: 35-45.8. Van Arsdel PP, Schaffrin RM, Rosenblatt J, et al. Evaluation of oral fenoterol in
chronic asthmatic patients Chest 1978; 73: 997-98.9. Plummer AL. The development of drug tolerance to beta 2 adrenergic agents Chest
1978; 73: 949-57.10. Trembath PW, Greenacre JK, Anderson M, et al. Comparison of four weeks’
treatment with fenoterol and terbutaline aerosols m adult asthmatics. J Allergy ClinImmunol 1979; 63: 395-400.
SIR,—Two articles and an editorial in your Dec 8 issue raiseseveral important issues, and I agree that we need to redefine the useof &bgr;z-agonists in asthma. However, great care needs to be takenwhen extrapolating from studies of existing &bgr;2-agonists such asfenoterol to the newer, long-acting agents salmeterol andformoterol. Dr Sears and colleagues’ finding of no benefit fromregular fenoterol can be contrasted with clinical trials on twice-dailysalmeterol, where a significant reduction in morbidity was achieved,thus demonstrating efficacy in chronic asthma.1.2 In studies
comparing regular salmeterol with regular salbutamol, over 3months, improvements in lung function and reduction in symptomswere also seen in the patients on salbutamol. Therefore we do havepositive evidence for benefit in controlling asthmatic symptomsfrom the use of chronic &bgr;z-agonist therapy.The other reason for hoping that the new, long-acting agents may
have a different role from those in current use stems from the effectof salmeterol on the inflammation associated with asthma. Thenewer &bgr;2-agonists may turn out to have a significant additionalnon-bronchodilator activity.3-5 Such a claim does not seem possiblefor &bgr;2-agonists in current use.Asthma therapy still remains largely dependent on
bronchodilators, with &bgr;2-agonists having a substantial role. Inhaled&bgr;2-agonists are frequently used to relieve symptoms but
increasingly are also given for regular treatment of chronic asthma,in company with oral bronchodilators. It is against this prescribinghabit that your editorial’s arguments for anti-inflammatory therapyto be used as primary treatment for chronic asthma must be seen.These arguments are well rehearsed and simply come down to thefact that it is better to treat the underlying inflammation and thusminimise bronchoconstriction. This view has been incorporatedinto British Thoracic Society guidelines6 and into a consensusconference held in Canada last year.’ 7

45
The early use of and central role of anti-inflammatory treatmentdoes not, however, mean that bronchodilators can be solely reservedfor relief of symptoms. Regular anti-inflammatory treatment
frequently does not eliminate symptoms and &bgr;z-agonists are oftenrequired to relieve coexisting bronchoconstriction. Under thesecircumstances long-acting potent 0,-agonists might simplifytreatment and make it more effective when used in conjunction withanti-inflammatory medication. In the clinical trials of salmeterolthis effect was clearly seen in the substantial reduction in morbidityobserved in patients recruited already taking inhaled steroids.
National Heart and Lung Institute,London SW3 6LY, UK T. J. H. CLARK
1. Britton M Salmeterol: three month companson with salbutamol in asthmatic patients.Eur Resp J 1990; 3 (suppl 10): 226S (S797).
2. Lundbeck B, Lindstrom M. A three month comparison of salmeterol and salbutamoldry powder. Clin Exp Allergy 1990; 20 (suppl 1) 38. 93.
3 Twentyman O, Finnerty JP, Harris A, Palmer J, Holgate ST Protection againstallergen induced asthma by salmeterol. Lancet 1990; 336: 1338-42.
4 Butchers PR, Cousins SA, Vardey CJ. Salmeterol a potent and long acting inhibitor ofthe release of inflammatory and spasmogenic mediators from human lung. Br JPharmacol 1987; 92 (suppl): 745P.
5 Fuller RW, Baker AJ. Anti-inflammatory effects of salmeterol. Eur Resp J 1990; 3(suppl 1): 226s.
6. British Thoracic Society. Guidelines for the managment of asthma in adults I. Chronicpersistent asthma. Br Med J 1990; 301: 651-53.
7 Hargreave FE, Dolovich J, Newhouse MT, eds. The assessment and treatment ofasthma: a conference report. J Allergy Clin Immunol 1990; 85: 1098-111.
SiR,—The conclusion by Dr Wong and colleagues (Dec 8, p1396) that "until further data are available fenoterol should not berecommended for use in asthma in the doses currently advised in theBritish National Formulary" seems difficult to justify. The BNFdose is 1 or 2 puffs three or four times daily.l In Wong’s studysalbutamol, terbutaline, and fenoterol in a single dose of 2 puffsproduced equal bronchodilator effects and apparently similar andinsignificant heart rate, QTc’ tremor, and serum potassiumresponses. It was only at higher doses (particularly a cumulativedose of 26 puffs) that any separation of systemic effects betweenfenoterol and the other agonists emerged. Wong et al seem to bearguing that if a drug shows adverse effects at multiples of therecommended dose the recommended dose itself must be unsafe: onthat argument many commonly used drugs, such as paracetamoland digoxin, would be unsafe. The data sheet for fenoterol statesthat "patients should be warned not to exceed the recommendeddose".2 If, as Wong et al suggest, the British Thoracic Society isrecommending the use of up to 50 puffs of these drugs in themanagement of acute asthma3 then what is needed is alteration ofthat policy-not promotion of the concept that fenoterol is unsafe atconventional dosage. This study demonstrated no clinical harm,even at the highest dosage. Wong et al present no data for theirargument that the drug will be more toxic in more severe asthmaticpatients who may also be hypoxic. Indeed we have shown thatasthmatic patients who take conventional doses of inhaledsalbutamol on a regular basis demonstrate down-regulation ofsystemic &bgr;z-adrenoceptors and blunting of the responses to highconcentrations of inhaled salbutamol acutely. What is not yet clearis how acute corticosteroid administration to patients inexacerbation may affect these responses.Wong et al rightly conclude that in their mild asthmatic patients
the doses of agonists used have resulted in the FEV, responsesbeing at the top of the dose-response curve, so that conclusionsabout relative potency cannot be drawn. Thus they cannot comparethe systemic effects at equipotent bronchodilator doses. However,the dose-response curves for heart rate and tremor for salbutamoldo not appear to have reached the steep part of the curve between 2and 8 puffs. This, rather than loss of (32-selectivity of fenoterol,probably explains the apparent difference in gradient between theheart rate curves for fenoterol and salbutamol: the gradients forfenoterol from 2 to 26 puffs and for salbutamol from 8 to 26 puffsappear similar. If fenoterol were more potent than salbutamol itwould not be necessary to evoke loss of selectivity to account for thegreater fenoterol effects. (32 agonists increase heart rate by at leasttwo mechanisms—direct cardiac &bgr;[adrenoceptor stimulationS andreflex vagal withdrawal following (32-receptor mediated peripheral
vasodilatation with consequent fall in diastolic blood pressure.6Since Wong et al did not measure blood pressure, they cannotexclude this latter possibility, and they present no credible data tosupport loss of &bgr;z-adrenoceptor selectivity of fenoterol.The evaluation of the role of fenoterol in the increased asthma
morbidity in New Zealand has been complicated by disagreementamongst pharmacoepidemiologists about interpretation of case-control studies.7og The debate will not be served by poorly designedstudies such as this one which are misinterpreted and from whichunsubstantiated conclusions are drawn. There seems to be no goodreason for not using inhaled fenoterol in the way recommendedboth by the BNF and data sheet, provided warnings are heeded bydoctors and patients.
Department of Clinical Pharmacology,University of Dundee,Ninewells Hospital and Medical School,Dundee DD1 9SY, UK
B. J. LIPWORTHD. NEWNHAMD. G. MCDEVITT
1. British National Formulary. London: British Medical Association/RoyalPharmaceutical Society of Great Britain, 1990: 125
2. ABPI. Data sheet compendium. London DataPharm, 1990: 214-153. British Thoracic Society. Guidelines for management of asthma in adults: II. Acute
severe asthma. Br Med J 1990; 301: 797-99.4. Lipworth BJ, Struthers AD, McDevitt DG. Tachyphylaxis to systemic but not
airways responses during prolonged therapy with high-dose inhaled salbutamol inasthmatics. Am Rev Respir Dis 1989; 140: 586-92
5. Hall JA, Petch MC, Brown MJ. Intracoronary injections of salbutamol demonstratethe presence of functional &bgr;2-adrenoceptors in the human heart. Circ Res 1989; 65:546-53
6. Arnold JMO, McDevitt DG. Contribution of the vagus to the haemodynamicresponses following intravenous boluses of isoprenaline. Br J Clin Pharmacol 1983;15: 423-29.
7. Crane J, Pearce N, Flatt A, et al. Prescribed fenoterol and death from asthma in NewZealand, 1981-1983. case control study. Lancet 1989; i: 917-22.
8. Pearce N, Grainger J, Atkinson M, et al. Case control study of prescribed fenoterol anddeath from asthma in New Zealand 1977-1981. Thorax 1990; 45: 170-75
SIR,-Dr Twentyman and colleagues (Dec 1, p 1338) reportfindings with salmeterol, after bronchial allergen challenge, whichsuggest that this long-acting (32 agonists may have anti-
inflammatory effects in vivo. Salmeterol is a potent inhibitor of therelease of inflammatory mediators, including spasmogeniccysteinyl-leukotrienes, from antigen-stimulated human lungfragments in vitro.1 We have been comparing the efficacy ofsalmeterol with that of the short-acting &bgr;z-agonist salbutamolagainst allergen-induced bronchoconstriction and have also lookedat the effects of these drugs on urinary leukotriene E4 (L TE4)excretion after allergen challenge. L TE4 is the stable urinarymetabolite of leukotrienes C4 and D and represents an integratedassessment of endogenous cysteinyl-leukotriene generation. Inatopic individuals urinary LTE4 is raised following allergenchallenge .2Twelve atopic asthmatics, seven of them males with FEV1 above
60% predicted and PCzo for histamine below 32 mg/ml, inhaledsalmeterol 50 ug, salbutamol 200 Jlg, or placebo in a randomised
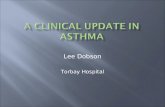
Urinary L TE4 excretion after allergen challenge.
P = placebo; SM = salmeterol, S8 = salbutamol.
*p=0037 (SM vs P), **p=0-01 (SB vs P).

46
double-blind fashion 15 min before allergen challenge. Airwaycalibre was monitored by FEV, for 4 h after the end of the challenge.Salbutamol and salmeterol completely abolished the early phase ofbronchoconstriction in the first 120 min after challenge: the areaunder the FEV1-time curve was inhibited by a mean of 90% forsalbutamol and 119% (net bronchodilatation) for salmeterol
(p < 0-005 vs placebo). However, in the second 120 min salbutamoldid not differ significantly from placebo while salmeterol providedsustained bronchodilation throughout the 240 min. Neithersalbutamol nor salmeterol significantly altered LTE4 excretion inthe first 2 h after challenge but caused modest reductions in thesecond 2 h collection (figure). There was no significant differencebetween the two &bgr;z-agonists during either collection period. Thelonger duration of action of salmeterol over salbutamol cannot beexplained in terms of any striking difference in effect on endogenouscysteinyl-leukotriene generation. This also suggests that
02-adrenergic stimulation of the airway smooth muscle rather thanthe mast cell may be functionally more important in vivo.The issue of salmeterol’s putative anti-inflammatory effects in
vivo is important but is not resolved by either Twentyman’s studyor ours. This will require more direct observation of other featuresof airway inflammation in asthma such as its effects on
inflammatory cell influx and cell activation markers in bronchialbiopsy specimens.
Department of Clinical Pharmacology,Royal Postgraduate Medical School,London W12 0NN, UK
KEVIN M. O’SHAUGHNESSYIAN K. TAYLORRICHARD W. FULLER
1. Butchers PR, Vardey CJ, Johnson M. Salmeterol: a potent and long-acting inhibitor ofinflammatory mediator release from human lung. Br J Pharmacol (in press).
2. Taylor GW, Taylor IK, Black P, et al. Urinary leukotreine E4 after antigen challengeand in acute asthma and allergic rhinitis. Lancet 1989; i: 584-88.
SiR,—Your Dec 8 editorial misses the point of our study (Dec 1,p 1338) when it states that "Bronchodilatation lasted up to 9 hours,with protection against non-specific bronchial reactivity for up to 32hours". Our study 1, in which no allergen was administered,showed that bronchodilatation and functional antagonism ofbronchoconstriction did not extend to 32 hours after salmeteroladministration. Study 2 then showed that salmeterol protectedagainst the allergen-induced increase in bronchial responsiveness at32 and 34 hours. This is an important point and implies thatsalmeterol has an additional action distinct from bronchodilatationand functional antagonism and can inhibit an effect of allergen thatis normally associated with pulmonary inflammation and worseningasthma svmntoms
Chest Medical Unit,Papworth Hospital,Papworth Everard CB3 8RE, UK O. P. TWENTYMAN
Medicine 1,Southampton General Hospital J. P. FINNERTY
1. Hargreave FE, Dolovich J, O’Byme PM, Ramsdale EH, Daniel EE. The origin ofairway hyperresponsiveness J Allergy Clin Immunol 1986, 78: 825-32
SIR,-Dr Twentyman and colleagues (Dec 1, p 1338), in theirpaper on the long-acting p-agonist salmeterol in asthma, interprettheir data as showing a complete inhibition of both the early and lateresponses after allergen challenge. They base this claim upon thefailure of antigen to cause significant bronchoconstriction whencompared with a prechallenge baseline. However, in administeringa potent and long-acting bronchodilator agent they have alteredbaseline forced expiratory volume (FEV 1) and histamine
responsiveness such that the late response is only evident bycomparison with a saline challenge. If this comparison is made, alate reaction is clearly demonstrated by changes in both airflowobstruction and histamine challenge, which parallel those afterplacebo. Salmeterol causes prolonged bronchodilation.1 The fall inFEV1 seen 35-95 h after allergen challenge is therefore surprisingand provides further evidence that a late reponse is occurring. Asimilar decline in PC2. histamine of 2-2 doubling dilutions is seenbetween 1-5 and 7-5 h after challenge whereas there was apparentlyno significant change after saline control.
It is likely that salmeterol is causing long-acting functionalantagonism of asthmatic responses because of its action at
&bgr;z-receptors. The parent compound, salbutamol, is not generallyconsidered to be an anti-inflammatory agent although it preventsmast cell degranulation.3 The suggestion that salmeterol may have anovel and as yet undetermined effect on the underlyinginflammatory process in asthma should be treated with somecaution. The claim that salmeterol has a potent anti-inflammatoryaction could lead to a dangerous decrease in steroid prescribing.
Salmeterol administration was associated with an improvementin FEV and PCzo histamine 32 h post allergen challenge. This is theonly tangible evidence of a true anti-inflammatory action. AsTwentyman et al point out, stimulation of the P-receptor dependson the pharmacological profile of the drug used. Because of itsuniquely long duration of action, simple comparison of salmeterolwith conventional P-agonists is unjustified. Although modificationof the late phase response may occur, it is misleading to claim itscomplete inhibition on the data presented in this study.Section of Respiratory Medicine,Department of Medicine and Pharmacology,University of Sheffield,Royal Hallamshire Hospital,Sheffield S10 2JF, UK
TREVOR ROGERSKATHARINE HIGGINSALYN MORICE
1. Ullman A, Svendmyr N. Salmeterol, a new long acting inhaled beta 2 adrenoceptoragonist comparison with salbutamol in adult asthmatic patients. Thorax 1988, 56:674-78
2 Cockcroft DW, Murdock KY. Comparative effects of inhaled salbutamol, sodiumcromoglycate and beclomethasone dipropionate on allergen-induced earlyasthmatic responses, late asthmatic responses and increased bronchial
responsiveness to histamine J Allergy Clin Immunol 1987, 79: 734-40.3. Howarth PH, Durham SR, Lee TH, Kay AB, Church MK, Holgate ST. Influence of
albuterol, cromolyn sodium and ipratropium bromide on the airway and circulatingmediator responses to allergic bronchial provocation in asthma. Am Rev Respir Dis1985; 132: 986-92
Recurrence after first seizure
SiR,—The National General Practice Study of Epilepsy (Nov 24,p 1271) might leave the casual reader with the impression that therisk of recurrence after a first seizure is at least 78% within three
years. The study group states that they have largely overcomeselection bias but it is not clear how many patients were referredimmediately after the first event.The diagnosis "definite epileptic seizures" was made on all
available information, including recurrence pattern, up to 6 monthsafter the index seizure. What would have been the outcome in
respect of accuracy of diagnosis and risk of recurrence if the
diagnosis had been made immediately after the index seizure? Sucha procedure would seem to be more relevant clinically.Most patients had had several seizures (9% had had 10 or more)
before they were enrolled. Including these patients (with a
recurrence rate of 100%) in a study of the prognosis after a firstseizure will certainly lead to gloomy results. The risk of recurrencefor patients admitted after the first seizure (46%, group C) is ofmore practical importance, and accords with hospital-basedstudies.12
This study is of great importance for the epidemiology of epilepsybut application to clinical practice-for example, on the dilemmawhether or not to start antiepileptic drug treatment after a firstseizure-seems hazardous. The risk of recurrence in patients seenwith a first seizure by a general practitioner or referred to a hospitalwill probably be far lower than 78%.
Department of Neurology,University Hospital,Rotterdam Dijkzigt,3015GD Rotterdam, Netherlands C. A. VAN DONSELAAR
Department of Public Health and Social Medicine,Erasmus University, Rotterdam J. D. F. HABBEMA
1 Hopkins A, Garman A, Clarke C. The first seizure in adult life. value of clinicalfeatures, electroencephalopathy, and computerised tomographic scanning in
prediction of seizure recurrence. Lancet 1988, i : 721-26
2. van Donselaar CA, Geerts AT, Schimsheimer RJS. Idiopathic first seizure in adultlife who should be treated? Br Med J (in press)